Autism Research in Arkansas: On-going clinical trials and the Arkansas Autism Alliance
56
Autism Research in Arkansas: On-going clinical trials and the Arkansas Autism Alliance S. Jill James, PhD Professor, Department of Pediatrics Director, Autism Metabolic Genomics Laboratory Arkansas Children’s Hospital Research Institute University of Arkansas for Medical Sciences Little Rock, AR
description
Autism Research in Arkansas: On-going clinical trials and the Arkansas Autism Alliance. S. Jill James, PhD Professor, Department of Pediatrics Director, Autism Metabolic Genomics Laboratory Arkansas Children’s Hospital Research Institute University of Arkansas for Medical Sciences - PowerPoint PPT Presentation
Transcript of Autism Research in Arkansas: On-going clinical trials and the Arkansas Autism Alliance

Autism Research in Arkansas: On-going clinical trials
and the Arkansas Autism Alliance
S. Jill James, PhD
Professor, Department of PediatricsDirector, Autism Metabolic Genomics LaboratoryArkansas Children’s Hospital Research Institute
University of Arkansas for Medical SciencesLittle Rock, AR

OVERVIEW
Review of metabolic pathways: folate/methionine/glutathione
Efficacy of methylB12 and folinic acid treatment on glutathione redox status and core behaviors in autism
Parent Metabolic Profiles
Specific Aims of our 5 year NIH-funded study
Placebo-controlled double-blind cross-over study of broad spectrum nutritional supplementation
AAA and ATN in Arkansas

Homocysteine B6
Methionine Transsulfuration to Cysteine and Glutathione
THF: tetrahydrofolate
Methionine
Enzymes
5-CH3THF
THF
B12MS5,10-CH2THF
MTHFR
1

SAM
SAH
MTase
SAHH
Homocysteine B6
Methionine Transsulfuration to Cysteine and Glutathione
THF: tetrahydrofolate
Methionine
Adenosine
Enzymes
5-CH3THF
THF
B12MS5,10-CH2THF
MTHFR
Cell Methylation1
Methylation Potential(SAM/SAH)
2

SAM
SAH
MTase
SAHH
Homocysteine B6 CBS
Methionine Transsulfuration to Cysteine and Glutathione
THF: tetrahydrofolate
Cystathionine
Cysteine
GSH GSSG
Methionine
Adenosine
B6
Enzymes
B6
5-CH3THF
THF
B12MS5,10-CH2THF
MTHFR
Methylation Potential(SAM/SAH)
Cell Methylation1 2
3 Antioxidant Redox Potential (GSH/GSSG)

SAM
SAH
MTase
SAHH
Homocysteine B6 CBS
Methionine Transsulfuration to Cysteine and Glutathione
Cystathionine
Cysteine GSH GSSG
Methionine
Adenosine
B6
B6
5-CH3THF
THF
B12MS5,10-CH2THF
MTHFR
Cell Methylation1
1
2
3
Folate Cycle
Methionine Cycle
Transsulfuration Pathway
Methylation Potential(SAM/SAH)
2
3 Antioxidant Redox Potential (GSH/GSSG)

SAM
SAH
MTase
SAHH
Homocysteine B6Cystathionine
Cysteine GSH GSSG
Methionine
Adenosine 5-CH3THF
THF
B12MS5,10-CH2THF
Cellular MethylationReactions
Purines and Thymidylate
DNA SYNTHESIS
PROLIFERATION
METHYLATION
REDOX HOMEOSTASIS
Vital Importance of these Interdependent Metabolic Pathways
1 2
3

AN OPEN LABEL TRIAL OF METHYLCOBALAMINAND FOLINIC ACID IN AUTISTIC CHILDREN
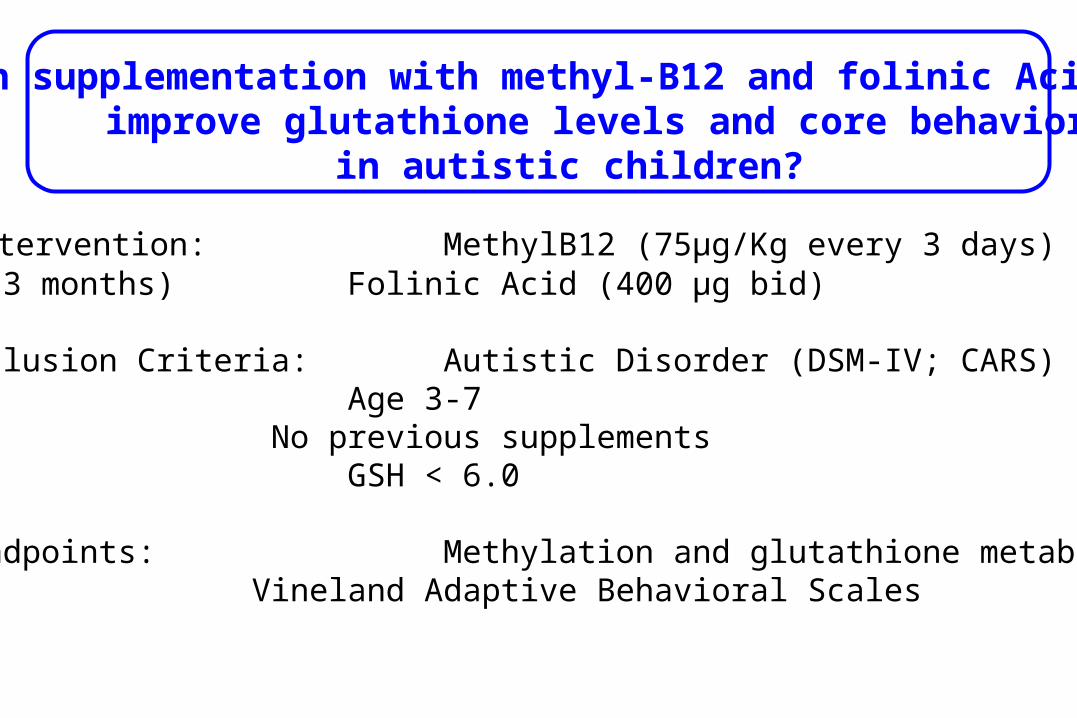
Intervention: MethylB12 (75µg/Kg every 3 days) (3 months) Folinic Acid (400 µg bid)
Inclusion Criteria: Autistic Disorder (DSM-IV; CARS) Age 3-7
No previous supplements GSH < 6.0
Endpoints: Methylation and glutathione metabolitesVineland Adaptive Behavioral Scales
Can supplementation with methyl-B12 and folinic Acid improve glutathione levels and core behaviors
in autistic children?

Each child served as their own control in the open label trial in which both parents and investigators were aware that the child was receiving supplements ofmethyl-B12 and folinic acid for a period of three months.
Plasma metabolites in the transmethylation and transsulfuration pathways were measured at baseline and again after the 3 month intervention period.
The study nurse administered and scored the Vineland Adaptive Behavior Scales parent questionnaire before and after the 3 month intervention.
STUDY DESIGN

SAM
SAH
MTase
SAHH
Homocysteine B6Cystathionine
Cysteine GSH GSSG
Methionine
Adenosine 5-CH3THF
THF
B12MS5,10-CH2THF
Cellular MethylationReactions
Purines and Thymidylate
DNA SYNTHESIS
1 2
3
Methyl B12
Folinic Acid
Folinic Acid
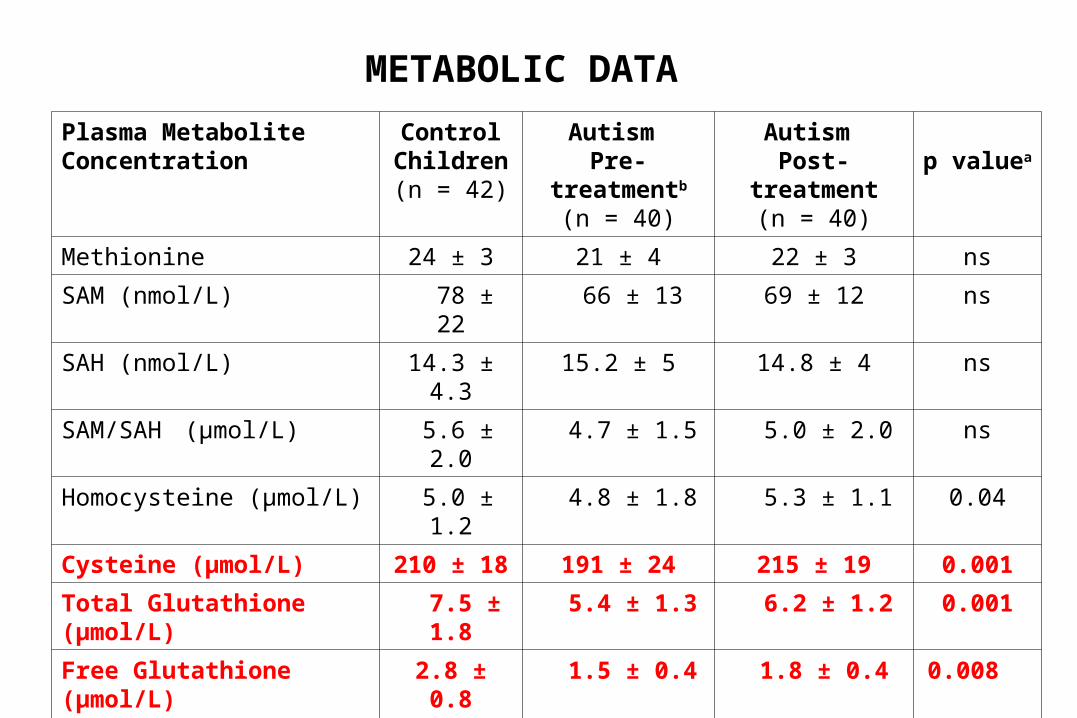
METABOLIC DATA
Plasma Metabolite Concentration
ControlChildren(n = 42)
Autism Pre-treatmentb
(n = 40)
Autism Post-treatment
(n = 40)p valuea
Methionine 24 ± 3 21 ± 4 22 ± 3 ns
SAM (nmol/L) 78 ± 22 66 ± 13 69 ± 12 ns
SAH (nmol/L) 14.3 ± 4.3 15.2 ± 5 14.8 ± 4 ns
SAM/SAH (µmol/L) 5.6 ± 2.0 4.7 ± 1.5 5.0 ± 2.0 ns
Homocysteine (µmol/L) 5.0 ± 1.2 4.8 ± 1.8 5.3 ± 1.1 0.04
Cysteine (µmol/L) 210 ± 18 191 ± 24 215 ± 19 0.001
Total Glutathione (µmol/L) 7.5 ± 1.8 5.4 ± 1.3 6.2 ± 1.2 0.001
Free Glutathione (µmol/L) 2.8 ± 0.8 1.5 ± 0.4 1.8 ± 0.4 0.008
GSSG (µmol/L) 0.18 ± 0.07 0.28 ± 0.08 0.22 ± 0.06 0.001
tGSH/GSSG 47 ± 18 21 ± 6 30 ± 9 0.001
fGSH/GSSG 17 ± 6.8 6 ± 2 9 ± 3 0.001a P value refers to treatment effect

Cysteine
0
50
100
150
200
250
300
Before After
µm
ol/L

0
1
2
3
4
5
6
7
8
9
10
Total Glutathione
Before After
µm
ol/L
x

0
0.1
0.2
0.3
0.4
0.5
0.6
GSSG
µm
ol/L
Before After

Total GSH/GSSG
0
10
20
30
40
50
60
Before After

SUMMARY OF METABOLIC RESULTS
1. All baseline metabolites were significantly different from age-matched controls (except for SAH)
2. The treatment did not significantly improve levels of methionine, SAM or SAM/SAH
3. The treatment did significantly improve cysteine, glutathione, and GSH/GSSG
4. Although significantly improved, glutathione and GSH/GSSG did not reach levels in control children
The Vineland Adaptive Behavior Scales (VABS) provides a numerical score for adaptive functioning in the areas of communication, socialization, daily living skills, motor skills, and an adaptive behavior composite (ABC) score.
The data are presented as the mean score for each category before and after intervention.
Behavioral Evaluation

Vineland Category
Baseline Score
(mean ± SD)
Post-Treatment
Score (mean ± SD)
Change in Score
(mean; 95% C I)
p value
Communication 65.3 ± 12.9
72.0 ± 15.5 6.7 (3.5, 10) <0.001
Daily Living Skills
67.0 ± 76 76.0 ± 17.7 9.0 (4.0, 14) <0.007
Socialization 68.2 ± 9.3 75.7 ± 14.7 7.5 (3.5, 11) <0.005
Motor Skills 75.6 ± 9.7 79.0 ± 14.7 3.3 (0, 8) 0.12
Composite Score
66.5 ± 9.2 73.9 ± 17.0 6.6 (2.3, 11) <0.003
BEHAVIOR SCORES
SUMMARY OF BEHAVIOR RESULTS
Although treatment with methylB12 and folinic acid significantly improved core behaviors, they did not reach standard scores for unaffected children (100 ± 15)
Improvement in measures of both metabolic and behavioral endpoints converge to suggest that some children may benefit from targeted nutritional intervention
CONCLUSIONS

What about the parents?
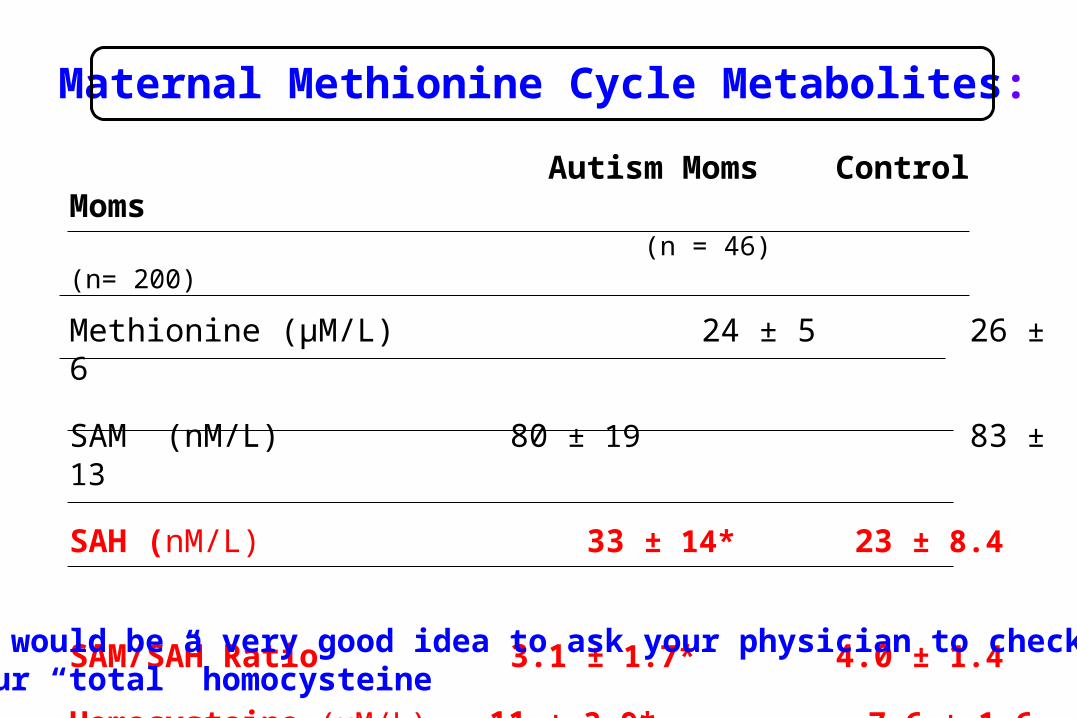
Autism Moms Control Moms (n = 46) (n= 200)
Methionine (µM/L) 24 ± 5 26 ± 6
SAM (nM/L) 80 ± 19 83 ± 13
SAH (nM/L) 33 ± 14* 23 ± 8.4
SAM/SAH Ratio 3.1 ± 1.7* 4.0 ± 1.4
Homocysteine (µM/L) 11 ± 3.9* 7.6 ± 1.6
*statistically significant
Maternal Methionine Cycle Metabolites:
It would be a very good idea to ask your physician to check your “total” homocysteine

Maternal Transsulfuration Metabolites
Autism Moms Control Moms
Cysteine (µM/L) 232 ± 40 231 ± 20
Total GSH (µM/L) 5.1 ± 1.7* 7.3 ± 1.5
Free GSH (µM/L) 1.5 ± 0.5* 2.6 ± 0.6
GSSG (µM/L) 0.30 ± 0.08* 0.24 ± 0.04
Total GSH/GSSG 17 ± 8 31 ± 10*
*statistically significant

Metabolite imbalance and the risk of being a mother of a child with
autism
Stratified GroupControlMothers
(N=200)
CaseMothers
(N=46)
Odds Ratio (Risk)
SAH >30µMol/L) 14% 54% 6.9
SAM/SAH <2.5 10% 54% 10.7
tGSH/GSSG <20 11% 65% 15.2
SAM/SAH <2.5 and tGSH/GSSG <20
3% 41% 46

It is not possible to determine from this data whether the abnormal metabolic profile in parents is genetically determined or whether it simply reflects the stress of living with an autistic child
IMPORTANT CAVEAT

METABOLIC BIOMARKERS OF AUTISM:PREDICTIVE POTENTIAL AND GENETIC SUSCEPTIBILITY
A 5 YEAR NIH-FUNDED STUDY (2006-2011)

Specific Aim 1: To determine whether the observed metabolite imbalance is associated with quantitative measures of autistic behavior
An expanded database of metabolic profiles will allow us to determine whether the severity and specificity of the metabolite imbalance is associated with the severity and specificity of behavioral abnormalities.
SPECIFIC AIM 1: METABOLITES AND BEHAVIOR

SPECIFIC AIM 2: PROSPECTIVE STUDY
Specific Aim 2: To investigate whether the abnormal metabolic profile precedes the diagnosis of autism among toddlers 18-30 months of age who are identified in developmental delay clinics to be at increased risk of developing autism.
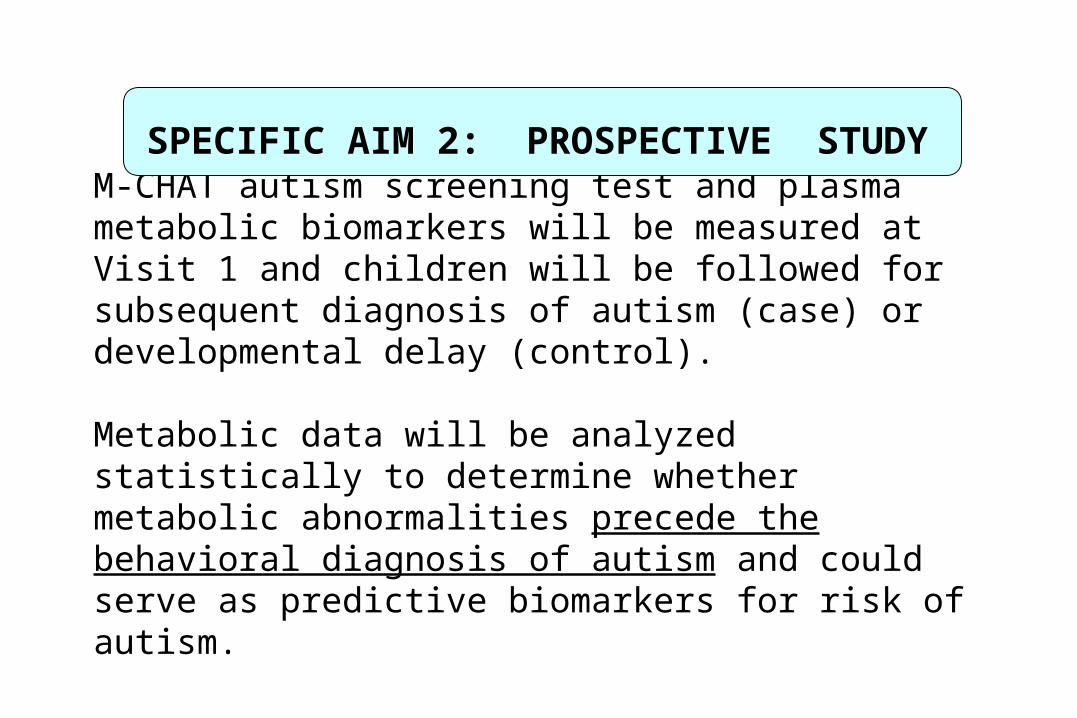
M-CHAT autism screening test and plasma metabolic biomarkers will be measured at Visit 1 and children will be followed for subsequent diagnosis of autism (case) or developmental delay (control).
Metabolic data will be analyzed statistically to determine whether metabolic abnormalities precede the behavioral diagnosis of autism and could serve as predictive biomarkers for risk of autism.
SPECIFIC AIM 2: PROSPECTIVE STUDY

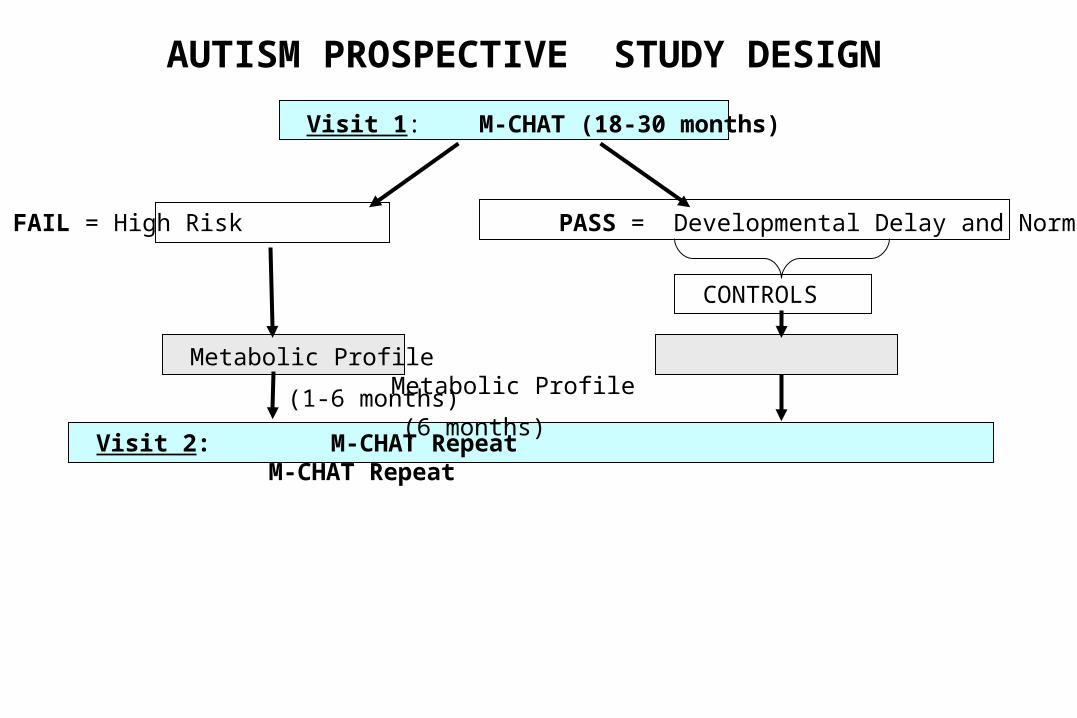
Visit 1: M-CHAT (18-30 months)
FAIL = High Risk PASS = Developmental Delay and Normal
CONTROLS
Metabolic Profile Metabolic Profile
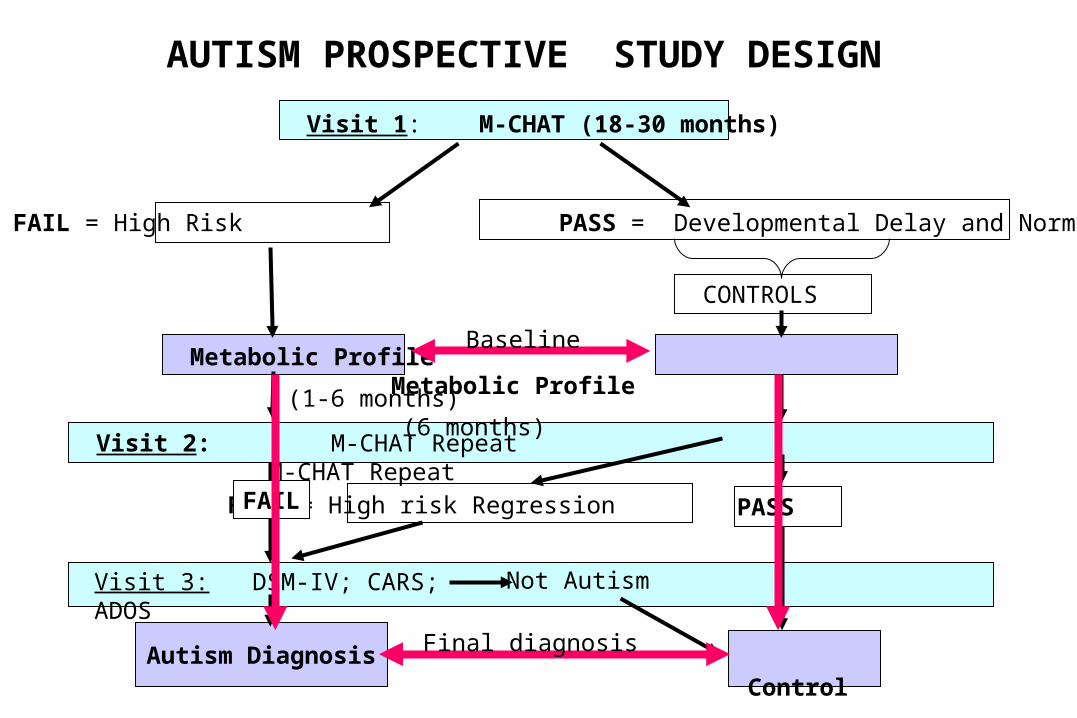
AUTISM PROSPECTIVE STUDY DESIGN
Visit 1: M-CHAT (18-30 months)
FAIL = High Risk PASS = Developmental Delay and Normal
CONTROLS
Visit 2: M-CHAT Repeat M-CHAT Repeat
(1-6 months) (6 months)
Metabolic Profile Metabolic Profile
AUTISM PROSPECTIVE STUDY DESIGN

Autism Diagnosis
Visit 1: M-CHAT (18-30 months)
FAIL = High Risk PASS = Developmental Delay and Normal
CONTROLS
Visit 2: M-CHAT Repeat M-CHAT Repeat
(1-6 months) (6 months)
Metabolic Profile Metabolic Profile
PASS
Visit 3: DSM-IV; CARS; ADOS
Control
Not Autism
AUTISM PROSPECTIVE STUDY DESIGN
FAIL

Autism Diagnosis
Visit 1: M-CHAT (18-30 months)
FAIL = High Risk PASS = Developmental Delay and Normal
CONTROLS
Visit 2: M-CHAT Repeat M-CHAT Repeat
(1-6 months) (6 months)
Metabolic Profile Metabolic Profile
FAIL = High risk Regression
Visit 3: DSM-IV; CARS; ADOS
Control
Not Autism
AUTISM PROSPECTIVE STUDY DESIGN
PASS FAIL
Autism Diagnosis
Visit 1: M-CHAT (18-30 months)
FAIL = High Risk PASS = Developmental Delay and Normal
CONTROLS
Visit 2: M-CHAT Repeat M-CHAT Repeat
(1-6 months) (6 months)
Metabolic Profile Metabolic Profile
FAIL = High risk Regression
Visit 3: DSM-IV; CARS; ADOS
Control
Not Autism
AUTISM PROSPECTIVE STUDY DESIGN
PASS FAIL
Baseline
Final diagnosis

If the metabolic profile is found to precede the behavioral diagnosis, subsequent studies would determine whether early intervention to normalize the metabolic profile can reduce or prevent the development of autism.
IMPLICATIONS OF AIM 2 AUTISM PROSPECTIVE STUDY

Specific Aim 3: To establish whether cells from children with autism exhibit evidence of increased oxidative stress and oxidative damage.
This mechanistic aim will determine whether lymphocytes from autistic children are inherently more vulnerable to oxidative stress than control cells
SPECIFIC AIM 3: CELLULAR CONSEQUENCES

Lymphoblastoid cell lines from autistic children withat least one affected sibling were compared with unaffected control lymphoblastoid cell lines*
Pairs of autistic and control cells lines were cultured under identical conditions. Rate of free radical generation, GSH/GSSG were measured at baseline and after exposure to thimerosal as oxidative stress.
EXPERIMENTAL PROCEDURES
*Preliminary data supported by SafeMinds

Cells from autistic children generate more free radicals than control cells
Relative Free Radical Generation (DCF)
0
100
200
300
400
500
600
700
800
900
0 0.3125 0.625 1.25 2.5
Thimerosal Concentration (uMol/L)
Vm
ax
RO
S R
ate
Control
Autistic

Cells from autistic children have lower GSH/GSSG ratio than control cells
Glutathione Redox Ratio (GSH/GSSG)
0
20
40
60
80
100
120
140
160
0 0.16 0.32 0.62 1.25 2.5
Thimerosal Concentration (uMol/L)
Control
Autistic

MITOCHONDRIAL REDOX IMBALANCE INLYMPHOBLASTOID CELL LINES
0
0.5
1
1.5
2
2.5
3
3.5
4
fGSH GSSG
0
2
4
6
8
10
12
14
16
18
Control Autistic
GSH/GSSG RATIOAutistic Control
(X 10)

Since both cell lines were cultured at the same time under identical conditions with identical media, the differences at baseline and after exposure to oxidant stress must reflect inherent genetic or epigenetic differences.
These results provide experimental evidence that cells from autistic children may be more sensitive to pro-oxidant environmental exposures.
CONCLUSION
SPECIFIC AIM 4: METABOLIC GENETICS
Specific Aim 4: Using a case-control design, we will determine whether the frequency of relevant genetic polymorphisms is increased among autistic children and whether specific genotypes are associated with the abnormal metabolic phenotype.
We have access to 500 trios (child, mother, father) from NIH genetic repository to look at relevant SNP frequencies and transmission

THF
5,10-CH2-THF
5-CH3-THF
B12
Cystathionine
DMG
Methionine
Homocysteine
SAM Methyl Acceptor
Methyltransferase
Methylated ProductMTHFR
TC II
SAH
Cysteine
Glutathione
Adenosine
GST
COMT
RFC
A Targeted Approach to Autism Genetics:Using the Metabolic Endophenotype as a
Guide to Candidate Genes
CBS
GCL

A RANDOMIZED DOUBLE-BLIND PLACEBO-CONTROLLED CROSS-OVER STUDY
Treating Oxidative Stress and the Metabolic Pathology of Autism

A significant proportion of autistic children have impaired methylation and antioxidant/detoxification capacity that results in chronic oxidative stress.
Targeted nutritional intervention that is designed to correct the metabolic imbalance will significantly improve their metabolic profile and improve measures of autistic behavior.
HYPOTHESIS

Specific Aim 1. We will screen children with a diagnosis of autism for evidence of impaired methylation (↓SAM/SAH) and impaired antioxidant capacity (↓GSH/GSSG)
Specific Aim 2. Children who exhibit evidence of impaired methylation and antioxidant capacity will be randomized into a double blind placebo-controlled cross-over trial of targeted nutritional intervention designed to correct metabolic deficiencies and to improve scores on standardized behavioral evaluation tests.
SPECIFIC AIMS

Thiols, Complete Lab, Thiols, Complete Lab, Thiols, Complete Lab, Behavioral Testing Behavioral Testing Behavioral Testing
B A
A BWASHOUT
A is supplement first, placebo secondB is placebo first, supplement second
RANDOMIZED DOUBLE-BLIND PLACEBO-CONTROLLED CROSS-OVER DESIGN
Children are randomly assigned to either the placebo first or the treatment firstfor 3 months before 1 month wash out period and cross-over
The supplements have been selected to impact three core cellular functions that are altered with chronic oxidative stress (www.clinicaltrials.gov)
1) Decreased SAM/SAH ratio and cellular methylation capacity
2) Antioxidant and detoxification support (mitochondrial and cytosolic)
3) Cell membrane integrity
1. Behavioral testing: ADOS; Vineland; PLS-2; SRSBehavioral testing will be videotaped and administered by PhD psychologists
2. Metabolic evaluation:Plasma: Thiol profile; CBC; amino acid profile, P5P,
HoloTCII; sulfate; nitrotyrosine; lactate/pyruvate; 25-
hydroxy vitamin D; uric acid; Urine: Sulfate, organic acids; creatinine; FIGlu, MMA Cellular: RBC membrane phospholipids; leukocyte
GSH/GSSG.
2. Immunologic evaluation: Flow cytometry for CRP, cytokine mRNA expression and protein levels for TNFα; g-IFN, IL-1; IL-4, IL-6; IL-10; IL-13; T-regs
OUTCOME MEASURES

AUTISM TREATMENT NETWORK (ATN) IN ARKANSAS

The ATN is a consortium of 15 national sites composed of experts in developmental pediatrics, neurology, genetics, metabolism, sleep, and gastroenterology who are dedicated to improving the standard of care of children with autism.
The ATN believes that treatment of medical issues can improve core behaviors and improve quality of life for children and adults with autismand their parents.
The ATN

Our Dream for Autism in Arkansas
Arkansas Autism Alliance (AAA)
UAMS/ACH/ACHRI

Clinical Evaluation & Treatment Center
Resource and Outreach Center Translational Research Center
UAMS/ACH/ACHRI Arkansas Autism Alliance

BEHAVIOR
(Genetic/Epigenetic) (Vulnerability/Resistance)
Multiple, AdditiveVariable Genes
Multiple, AdditiveVariable Factors
Necessary but Not Sufficient
Necessary but Not Sufficient
FROM EPIDEMIOLOGY TO MECHANISM
GENE EXPRESSION ENVIRONMENT

GENE EXPRESSION ENVIRONMENT
BEHAVIOR
(Genetic/Epigenetic) (Vulnerability/Resistance)
Necessary but Not Sufficient
Necessary but Not Sufficient
Metabolic Endophenotype (GSH/GSSG) (SAM/SAH)
Mechanism(Redox Imbalance; Methylation)
TREATMENTMultiple, AdditiveVariable Factors
Multiple, AdditiveVariable Genes
FROM EPIDEMIOLOGY TO MECHANISM

AcknowledgementsAutism Metabolic Genomics Laboratory
Stepan Melnyk, PhDStefanie JerniganAlena SavenkaShannon PalmerSarah Blossom, PhDLesya Pavliv
Study Nurses Nancy Chambers, Dana Schmidt, Amanda Hubanks, Nancy Lowery