Autism
77
Name the personality … what disorder they have ??? visual thinker Focused (IFE) Interaction, language, learning
Transcript of Autism

Name the personality … what disorder they have ???
visual thinker
Focused (IFE)
Interaction, language, learning

Topic: Autism
Spectrum Disordes
John matthews
Ng kar seng
James patrik
Ang ling kang

Autism spectrum disorder (ASD)
disorders in development of the brain Spectrum is
the range and severity of the difficulties vary
social interaction
social communicatio
n
Behavioralabnormalities
develops and diagnosed
before 3 years old age.
Boys more effected
then girls ratio 1:422 people
per 10000
Idiopatic and genetic
• Reciprocal social interaction
• Communication, • Restrictive and repetitive
stereotypical pattern of behaviour,
• Very well in certain skill • Abnormal play - little
symbolic play, ritualistic rigidity, preoccupations with parts of object
• Protoimperative pointing skill
• Protodeclarative pointing skill
• Totally aloof and not make eye contact
• Echolalia, pronoun reversal, nonsense rhyme
• Intellectual functioning can vary(75% MR)

social interaction
restricted, obsessional, idiosyncratic interest
awkward and clumsy and unusual posture and gait
facial expression and gesture
repetitive behaviour
No severe language impairment, high functioning
autism(11/10000)

Childhood disintegrative disorder
Heller dementia . Rare, unknown cause
2 – 4 years normal after that regression
start
motor stereotypies and seizure are often
language, play, social skill, imagination
bowel and bladder control may lost
Male > female
6 and 18 monthsNo responding
socially, repetitive hand movement,
Rare, mostly girls, due to genetic
mutation
Loss language skills
apnea and hyperventilation,
Loss coordination
highly irritability
Head growth slows down by
age 2
Better language
skills compare
ASFewer
repetitive behavior
s
Impaired social
interaction
Not severe
compare AS
Insufficient for a
diagnosis of autism
Have one Features of ASD

Psychopharmalogy
Problems Drugs
Repetitive behaviour, behavioural rigidity
Selective serotonin reuptake inhibitor (SSRI) like fluvoxamine and fluoxetine.
Aggressive and self- injury Alpha agonist (clonidine) and atypical antipsychotic (olanzapine)
Sleep dysfunction Melatonin and clonidine
Anxiety SSRI and buspirone.
Depression phenotype SSRI and venlafaxine
Bipolar phenotype Atypical antipsychotic (olanzapine) and lithium

Etiology
• Literature provides discussion of etiology to subtype ASD as either idiopathic or secondary.
• Patients with idiopathic autism are those who do not have a coexisting associated medical condition or syndrome known to cause autism.
• Patient with secondary autism are children with a known identifiable syndrome or medical disorder believed to play an etiological role in autism; this occurs in only 2% to 10% of cases. The presence of severe mental retardation, especially when associated with dysmorphic features, increases the likelihood of identifying a genetic etiology.

• Autistic spectrum disorder (ASD) is now believed to be biologically based neurodevelopmental disorders that are highly heritable.
• Because of the wide phenotypic spectrum, most experts believe that many genes are involved.
• Although ASD is believed to be mainly genetic in origin, the lack of 100% concordance in monozygotic twins indicates that environmental factors may modulate the phenotypic expression.
• Thus it has become increasingly apparent that the cause is multifactorial, with a variety of genetic and to a lesser extent, environmental factors playing a role.
Genetic Underpinning
• The exact cause of autism is unknown, but is believed to be multifactorial, with a strong genetic influence.
• There is a 92% concordance rate for monozygotic twins and 30% concordance rate for dizygotic twins for the broader spectrum of social and communication difficulties.
• In spite of these strong genetic underpinnings, the exact cause or causes are still unknown. • First, ASD appears to be complex heritable disorders
involving multiple genes; estimates based on family studies range from 5-20 genes.
• A second factor making genes identification more challenging is the variability in the autism phenotype.
• It is believed that multiple genes interact with varied environmental causes to produce the disorder, and that the causative genes may vary from one population to another.
• Because of the complex heterogeneity and the variable behavioral phenotype of autism, linkage studies have not identified specific chromosomal region that are universally believed to harbor the genes causing autism.
• Genetic syndromes associated with autism and coexisting mental retardation include:• Fragile X syndrome,
• Tuberous sclerosis,
• Phenylketonuria and
• Angelman syndrome.
• On these four entitles, the fragile X syndrome is the most common known genetic cause for the autistic phenotype.
• Children with severe congenital sensory impairments (visual and/or auditory) are also at risk for the development of symptoms consistent with autism, especially when appropriate early intervention is not provided.

• Compared with other disorders of a similar behavioral phenotype, certain genes are believed to be more strongly implicated in the heritability of autism, including chromosome 7q (seen in the similar behavioral phenotype of specific language impairment disorder), chromosome 2q and chromosome 15q11-13, both of which manifest traits of rigidity and stereotypical behaviors.

Environmental Factors
• Environmental influence may represent a “second hit” or “trigger” phenomenon; that is, they may modulate/ stimulate preexisting genetic factors to result in the manifestation of ASD in an individual child.
• Perinatal
• Postnatal

Perinatal
• Environmental factor should have their greatest effect during the prenatal period, especially early in gestation, because the developmental brain abnormalities associated with autism occur during the first and second trimesters.
• Factors already identified to play a role include maternal rubella or cytomegalovirus infections and treatment with valproate or thalidomide.
• Nelson and associates reported increased cord blood levels of brain-derived neurotrophic factor and other neurotrophins in newborns in whom ASD was later diagnosed, which may have implications regarding the mechanism of the characteristic early brain overgrowth.

• Some investigators feel that fetal toxin exposure might be implicated by studies that have demonstrated higher rates of autism in offspring of mothers who resided in urban settings during pregnancy.
• Among other factors, the strongest associations have been with threatened abortion and advanced maternal age.
• An association has been suggested between full-term neonatal encephalopathy and later diagnoses autism.

Postnatal• Postnatal causes of autism are less likely possibilities.
• Moderate environmental deprivation has not been found to play an etiological role in ASD. Although scientific evidence of no association between vaccines (especially MMR and thimerosal- or mercury-containing vaccine and autism continue to accumulate, many parents, as well as some professionals, remain unconvinced of the calidity of the evidence.

Neuroanatomical FindingBrain Growth• The head circumference of children with ASD is normal or
slightly smaller than normal at birth until 2 months of age.
• Longitudinal studies of children with autism showed an abnormally rapid increase in head circumference from 6-14 months of age, which was largely concluded by the end of the 2nd year of life.
• Growth appears to level off in late childhood in the majority; thus brain volume is not significantly different from that in controls by age 12 years, although (as measured by occipitofrontal circumference) may persist.

• MRI studies done at 2-4 year of age show that autistic toddlers have increased brain volume which characterized by increased volume of the cerebellum, cerebrum and amygdala compared with normal volumes.
• The abnormal growth in the first 2 year is most marked in the frontal, temporal, cerebellar and limbic regions of the brain, the areas of the brain responsible for higher-order cognitive, language, emotional and social functions, which are most impaired in ASD.
• It is believed that the early abnormal growth processes in the brain in the first 2 year of life underline the emergence of preclinical behavioral abnormalities seen in ASD.
• This period of early, accelerated brain growth appears to stop early in childhood and is followed by abnormally slow or arrested growth, resulting in areas of underdeveloped and abnormal circuitry in parts of the brain.

• Approximately one third of children with ASD meet criteria for macrocephaly, and 90% have greater than average brain volumes.
• Furthermore, increased cortical folding resulting in abnormal gyral patterns, reflecting increased volume, has been noted in affected children but not adolescents or adults.
• These findings appear very consistent, especially when study subjects are matched size lies in nonuniformchanges in the hippocampus, amygdala and cerebral white matter and less consistently, gray matter.
• It is most likely that it is the outer radiate zone, related to intrahemispheric synaptogenesis and connectivity that measures postnatally and produces the rapid growth in autism.

• Interestingly, parents of children with ASD can have macrocephaly in the absence of autism symptom.
• Thus, macrocephaly might be caused by a susceptibility gene that works in concert with other genes to produce ASD.
• ASD seems to be characterized by abnormalities of neural distribution and connectivity with excessive intrahemispheric connectivity and deficient interhemispheric connection (corpus callosum).

Cerebellar Purkinje Cells
• One of the most consistent findings over time has been the marked decrease in Purkinje cells noted in postmortem microscopic studies.
• The reduction in reelin may contribute abnormal regulation of neuronal layering and microscopic abnormalities found in the cerebellum.
• The absence of glial hyperplasia indicates the pathological process occurs early in brain is able to initiate a reaction to neuronal injury.

Olivary neurons
• Furthermore, the number of olivary neurons is preserved, which provides additional evidence that the process must occur before week 28 to 30 gestations.
• After this time, tight neuronal unions form between the two areas, and cell loss in the cerebellum would prompt an obligatory retrograde cell loss in the ascending olivaryneurons.
• Although it has long been known that the cerebellum played a role in motor learning, modulation, and coordination, there is growing evidence that it also plays a role in verbal processing, affective behavior and shifting of attention.

Decreased cell size, increased cell number and increased packing density in limbic structures
• Investigators have targeted the limbic system because it plays an important role in social behavior/cognition (amygdala) and associative social memory, especially relationships among the emotional aspects of an experience (hippocampus).
• Postmortem microscopic studies have consistently revealed abnormalities in cell number and size and packing density in both the amygdala and hippocampus.
Abnormal minicolumns in the cerebral cortex
• Minicolumns in some areas of the autistic frontal cortex were found to be smaller (representing an underdeveloped system) and had abnormal patterning.
• Both findings are consistent with deviant processes that occur very early in the second trimester.
• These anatomical abnormalities may result in deficient neuronal “insulation” and serve as the structural basis for increased neuronal “cross-talk” and overstimulation.
• This, in turn, may cause the sensory gating and processing difficulties found in some individuals with autism.
Hypoactivity in the fusiform gyrus during face recognition tasks
• The most consistent fMRI finding has been hypoactivity in the fusiform facial area, confirming the clinical impression that deficits in facial recognition are characteristic of ASD.
• fMRI has also demonstrated associated deficits in related areas of the “social brain”, such as the amygdala, which plays a critical role in emotional arousal and integration of emotional data.

• Persons with ASD appear to be less motivated to look at faces or to follow the point of conversational partners.
• Computerized eye tracking techniques have also revealed that they pay less attention to faces and more attention to inanimate details in the background.
• When they do look at the face, they target the mouth rather than the eyes.
• Because oral expressions provide less information about emotional states than the eyes, people with ASD often fail to detect meaningful social information during interactions.

Others neuroanatomical finding• Additional studies of neuroanatomy in children with ASD
have demonstrated anatomic changes in the anterior cingulate gyrus, an area of the brain associated with decision-making and the ascription of feelings and thoughts.
• Deficits in the reticular activating system, structural cerebellar changes, forebrain hippocampal lesions and neuroradiology abnormalities in the prefrontal and temporal lobe areas have been documented, and abnormal neurochemical findings have also been associated with ASD.
• In addition, the dopamine, catecholamine, and serotonin levels or pathways have been implicated.

• Other ASD symptom then might be explained by a dysregulation of axonal outgrowth, dendritic arborization and synaptic connectivity.
• Abnormalities described in cortical frontostriatalcircuits may be associated with ritualistic and repetitive behaviors.
• Volumetric sMRI studies of cortical systems serving language functions have revealed the absence of the usual left hemispheric hypertrophy (representing left brain dominance and language specialization).
• Instead of a larger left hemisphere (specifically, the Wernicke receptive language processing area), the planum temporale volumes were equal in subjects with autism.
• Furthermore, decreased gray matter in the left inferior prefontal gyrus or Broca’s area (expensive language center) resulted in actual reversal of the typical hemispheric asymmetry (left larger than right) in language- impaired subjects with autism.

How Is Autism Diagnosed?

Modified Checklist of Autism in Toddlers [M-CHAT]
• A list of informative questions about your child
• The answers can indicate whether he or she should be further evaluated by a specialist such as a developmental paediatrician, neurologist, psychiatrist or psychologist
Modified Checklist of Autism in Toddlers [M-CHAT]
• The original version, the M-CHAT, was developed by neuropsychologists Diana Robins and Deborah Fein and clinical psychologist Marianne Barton.
• The revision, which improves specificity, was released in December 2013
• The American Academy of Paediatrics (AAP) recommends that all children receive autism screening at 18 and 24 months of age, and the M-CHAT-R is one of the AAP’s recommended tools.

M-CHAT
• The M-CHAT Follow-Up Interview can be downloaded from:
• http://www2.gsu.edu/~psydlr
• Modified Checklist for Autism in Toddlers-Revised (M-CHAT-R™) can be done online at:
• http://www.autismspeaks.org/what-autism/diagnosis/mchat


M-CHAT Follow-up Interview
• The interview is designed to reduce the false positive rate
• It is highly recommended that M-CHAT users also incorporate the M-CHAT Follow-up Interview into the screening process
• Note that failing the follow-up interview does not diagnose ASDs; it indicates increased risk for ASDs.


Modified Checklist for Autism in Toddlers-Revised (M-CHAT-R™)
• screening children between 16 and 30 months of age that assesses risk for autism spectrum disorder (ASD)
• The M-CHAT-R's primary goal is to detect as many cases of ASD as possible.


• From birth to at least 36 months of age, every child should be screened for developmental milestones during routine well visits.
• When such a screening—or a parent—raises concerns about a child's development, the doctor should refer the child to a specialist in developmental evaluation and early intervention.
• These evaluations should include hearing and lead exposure tests as well as an autism-specific screening tool such as the M-CHAT. Among these screening tools are several geared to older children and/or specific autism spectrum disorders.

• A typical diagnostic evaluation involves a multi-disciplinary team of doctors including a paediatrician, psychologist, speech and language pathologist, physiotherapist and occupational therapist.
• Sometimes an autism spectrum disorder is diagnosed later in life, often in relation to learning, social or emotional difficulties.
• As with young children, diagnosis of adolescents and adults involves personal observation and interview by a trained specialist.
• Often, a diagnosis brings relief to those who have long struggled with difficulties in relating socially while not understanding the source of their difficulties. A diagnosis can also open access to therapies and assistive technologies that can improve function in areas of difficulty and, so, improve overall quality of life.
Pervasive Developmental Disorders Screening Test (PDDST)
• Purpose Assessment of autistic behaviours
• Is a parent-completed survey that targets children from birth-3 year of age and incorporates a 3-tiered approach: • 1 for the primary care clinic,
• 1 for the developmental clinic, and
• 1 for the multi-disciplinary autism clinic.
• All 3 tiers contain items that measure various aspects of language, social skills, pretend play, attachment, sensory responses, and motor stereotypies.

• In children with ASDs, intelligence, as measured by conventional psychologic testing, usually falls in the functionally retarded range; the deficits in language and socialization make it difficult to obtain an accurate estimate of the autistic child‘s intellectual potential.
• Some autistic children perform adequately in nonverbal tests, and those with developed speech may show adequate intellectual capacity.
• Autistic children also show deficits in their understanding of what the other person might be feeling or thinking, a so-called lack of a theory of mind.
• On some psychologic tests, children with autism pay more attention to specific details while overlooking the entire gestalt of the object, demonstrating a lack of central coherence.
DSM-5 Diagnostic Criteria• fifth edition of the Diagnostic and Statistical Manual of Mental Disorders
(DSM-5).
• As of May 2013, psychologists and psychiatrists will be using these criteria when evaluating individuals for these developmental disorders.
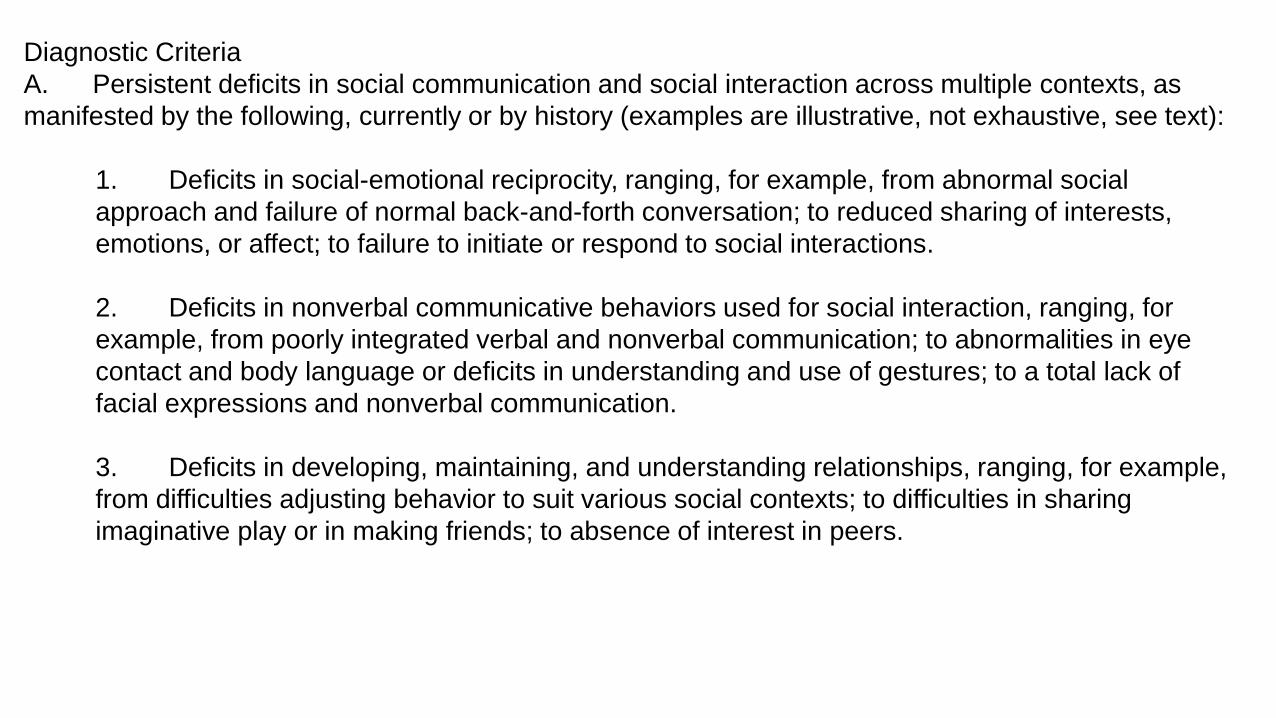
Diagnostic Criteria
A. Persistent deficits in social communication and social interaction across multiple contexts, as
manifested by the following, currently or by history (examples are illustrative, not exhaustive, see text):
1. Deficits in social-emotional reciprocity, ranging, for example, from abnormal social
approach and failure of normal back-and-forth conversation; to reduced sharing of interests,
emotions, or affect; to failure to initiate or respond to social interactions.
2. Deficits in nonverbal communicative behaviors used for social interaction, ranging, for
example, from poorly integrated verbal and nonverbal communication; to abnormalities in eye
contact and body language or deficits in understanding and use of gestures; to a total lack of
facial expressions and nonverbal communication.
3. Deficits in developing, maintaining, and understanding relationships, ranging, for example,
from difficulties adjusting behavior to suit various social contexts; to difficulties in sharing
imaginative play or in making friends; to absence of interest in peers.

B. Restricted, repetitive patterns of behavior, interests, or activities, as manifested by at least two of the
following, currently or by history (examples are illustrative, not exhaustive; see text):
1. Stereotyped or repetitive motor movements, use of objects, or speech (e.g., simple motor
stereotypies, lining up toys or flipping objects, echolalia, idiosyncratic phrases).
2. Insistence on sameness, inflexible adherence to routines, or ritualized patterns or verbal nonverbal
behavior (e.g., extreme distress at small changes, difficulties with transitions, rigid thinking patterns, greeting
rituals, need to take same route or eat food every day).
3. Highly restricted, fixated interests that are abnormal in intensity or focus (e.g, strong attachment to or
preoccupation with unusual objects, excessively circumscribed or perseverative interest).
4. Hyper- or hyporeactivity to sensory input or unusual interests in sensory aspects of the environment
(e.g., apparent indifference to pain/temperature, adverse response to specific sounds or textures, excessive
smelling or touching of objects, visual fascination with lights or movement).
Specify current severity:
Severity is based on social communication impairments and restricted repetitive patterns of
behavior (see Table on the next slide).
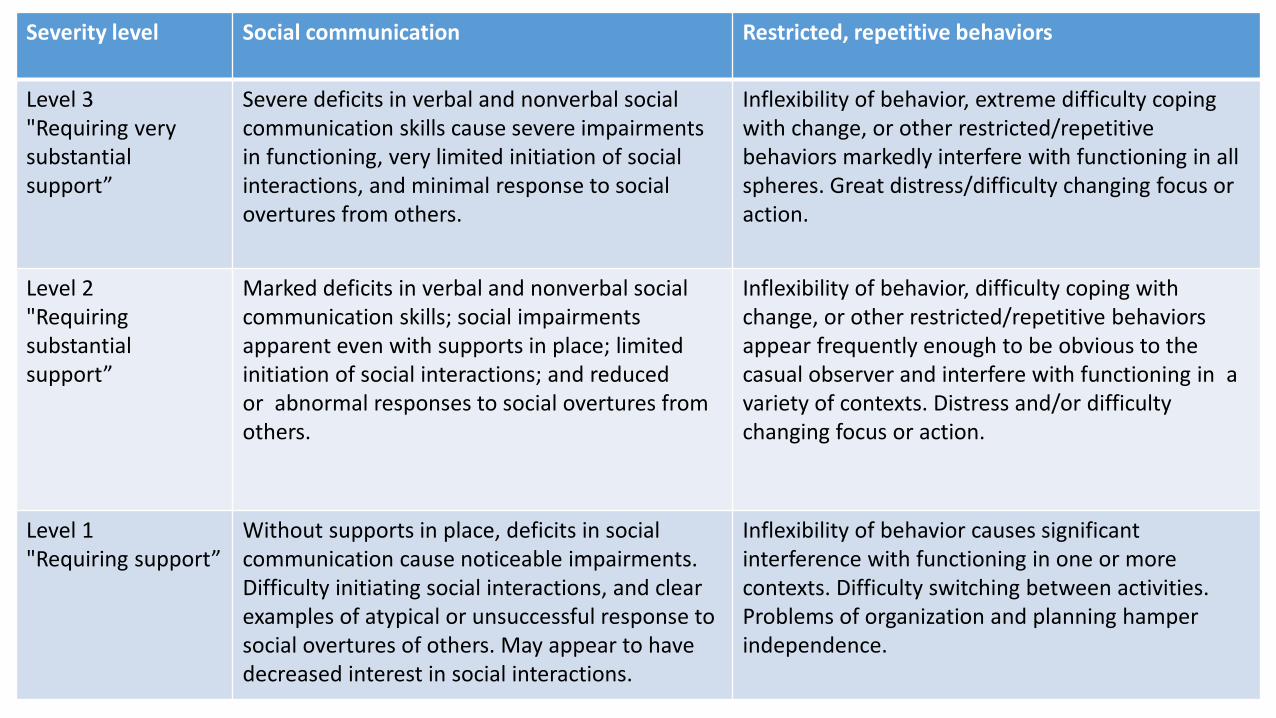
Severity level Social communication Restricted, repetitive behaviors
Level 3"Requiring very substantial support”
Severe deficits in verbal and nonverbal social communication skills cause severe impairments in functioning, very limited initiation of social interactions, and minimal response to social overtures from others.
Inflexibility of behavior, extreme difficulty coping with change, or other restricted/repetitive behaviors markedly interfere with functioning in all spheres. Great distress/difficulty changing focus or action.
Level 2"Requiring substantial support”
Marked deficits in verbal and nonverbal social communication skills; social impairments apparent even with supports in place; limited initiation of social interactions; and reduced or abnormal responses to social overtures from others.
Inflexibility of behavior, difficulty coping with change, or other restricted/repetitive behaviorsappear frequently enough to be obvious to the casual observer and interfere with functioning in a variety of contexts. Distress and/or difficulty changing focus or action.
Level 1"Requiring support”
Without supports in place, deficits in social communication cause noticeable impairments. Difficulty initiating social interactions, and clear examples of atypical or unsuccessful response to social overtures of others. May appear to have decreased interest in social interactions.
Inflexibility of behavior causes significant interference with functioning in one or more contexts. Difficulty switching between activities. Problems of organization and planning hamper independence.
C. Symptoms must be present in the early developmental period (but may not become fully manifest until
social demands exceed limited capacities, or may be masked by learned strategies in later life).
D. Symptoms cause clinically significant impairment in social, occupational, or other important areas of current
functioning.
E. These disturbances are not better explained by intellectual disability (intellectual developmental disorder) or
global developmental delay. Intellectual disability and autism spectrum disorder frequently co-occur; to make
comorbid diagnoses of autism spectrum disorder and intellectual disability, social communication should be below
that expected for general developmental level.

Treatment

• Each child or adult with autism is unique and, so, each autism intervention plan should be tailored to address specific needs.
• Intervention can involve behavioral treatments, medicines or both. Many persons with autism have additional medical conditions such as sleep disturbance, seizures and gastrointestinal (GI) distress.
• Addressing these conditions can improve attention, learning and related behaviors.
• Early intensive behavioral intervention involves a child's entire family, working closely with a team of professionals.
• In some early intervention programs, therapists come into the home to deliver services. This can include parent training with the parent leading therapy sessions under the supervision of the therapist. Other programs deliver therapy in a specialized center, classroom or preschool.

• Typically, different interventions and supports become appropriate as a
child develops and acquires social and learning skills.
• As children with autism enter school, for example, they may benefit from
targeted social skills training and specialized approaches to teaching.
• Adolescents with autism can benefit from transition services that
promote a successful maturation into independence and employment
opportunities of adulthood.

Early Intervention Therapies
• Lovaas Model based on Applied Behavior Analysis (ABA)
• Early Start Denver Model
• Parents and therapists also report success with other commonly used behavioral therapies, including Floortime, Pivotal Response Therapy and Verbal Behavior Therapy.

Applied Behavior Analysis [ABA]• Behavior analysis focuses on the principles that explain how learning
takes place. Positive reinforcement is one such principle.
• When a behavior is followed by some sort of reward, the behavior is more likely to be repeated.
• ABA is the use of these techniques and principles to bring about meaningful and positive change in behavior.
• These techniques can be used in structured situations such as a classroom lesson as well as in "everyday" situations such as family dinnertime or the neighborhood playground.
• Some ABA therapy sessions involve one-on-one interaction between the behavior analyst and the participant. Group instruction can likewise prove useful.

The Early Start Denver Model (ESDM)
• is a comprehensive behavioral early intervention approach for children with autism, ages 12 to 48 months.
• The program encompasses a developmental curriculum that defines the skills to be taught at any given time and a set of teaching procedures used to deliver this content.
• It is not tied to a specific delivery setting, but can be delivered by therapy teams and/or parents in group programs or individual therapy sessions in either a clinic setting or the child’s home.
• This early intervention program integrates a relationship-focused developmental model with the well-validated teaching practices of Applied Behavior Analysis (ABA).

Floortime• Takes place in a calm environment, can be at home or in a
professional setting.
• Formal treatment sessions range from two to five hours a day. They include training for parents and caregivers as well as interaction with the child. Therapists encourage families to use Floortime principals in their daily lives.
• Floortime sessions emphasize back-and-forth play interactions. This establishes the foundation for shared attention, engagement and problem solving. Parents and therapists help the child maintain focus to sharpen interactions and abstract, logical thinking.
• As children mature, therapists and parents tailor the strategies to match a child’s developing interests and higher levels of interaction.

Pivotal Response Treatment (PRT)
• Derived from applied behavioral analysis (ABA), it is play based and child initiated. Its goals include the development of communication, language and positive social behaviors and relief from disruptive self-stimulatory behaviors.
• Rather than target individual behaviors, the PRT therapist targets “pivotal” areas of a child's development. These include motivation, response to multiple cues, self-management and the initiation of social interactions.
• By targeting these critical areas, PRT will produce broad improvements across other areas of sociability, communication, behavior and academic skill building.
• Motivation strategies are an important part of the PRT approach. These emphasize “natural” reinforcement.

Verbal Behavior Therapy
• teaches communication using the principles of Applied BehaviorAnalysis(ABA) and the theories of behaviorist B.F. Skinner.
• By design, Verbal Behavior Therapy motivates a child, adolescent or adult to learn language by connecting words with their purposes. The student learns that words can help obtain desired objects or other results.
• Therapy avoids focusing on words as mere labels (cat, car, etc.) Rather, the student learns how to use language to make requests and communicate ideas.

Treatment Options for Toddlers and Preschool Children
• The child receives structured, therapeutic activities for at least 25 hours per week.
• Highly trained therapists and/or teachers deliver the intervention. Well-trained paraprofessionals may assist with the intervention under the supervision of an experienced professional with expertise in autism therapy.
• The therapy is guided by specific and well-defined learning objectives, and the child’s progress in meeting these objectives is regularly evaluated and recorded.
• The intervention focuses on the core areas affected by autism. These include social skills, language and communication, imitation, play skills, daily living and motor skills.
• The program provides the child with opportunities to interact with typically developing peers.
• The program actively engages parents in the intervention, both in decision making and the delivery of treatment.
• The therapists make clear their respect for the unique needs, values and perspectives of the child and his or her family.
• The program involves a multidisciplinary team that includes, as needed, a physician, speech-language pathologist and occupational therapist.
Medicines for Treating Autism’s Core Symptoms• Medicines for treating the three core symptoms of autism:
• communication difficulties
• social challenges
• repetitive behaviour
• Food and Drug Administration (FDA) has approved two drugs for treating irritability associated with the autism:• Risperidone
• Aripiprazole
• Relieving irritability often improves sociability while reducing tantrums, aggressive outbursts and self-injurious behaviors.

• Selective serotonin re-uptake inhibitors (SSRIs), including fluoxetine. Several of these medicines are FDA-approved for the treatment of anxiety disorders and depression, in children as well as adults. Although large clinical trials have yet to demonstrate their effectiveness, parents and clinicians have found that they can ease social diff
• Naltrexone, which is FDA-approved for the treatment of alcohol and opioid addictions. It can ease disabling repetitive and self-injurious behaviors in some children and adults with autism.

Physiotherapy management

• In a physiotherapy evaluation a child’s neuromuscular, musculoskeletal and cardiopulmonary systems are assessed.
• Therapists have to examine closely at a child’s ability to take in sensory input and control motor output.
• Facilitating and limiting factors for various gross motor skills like jumping, walking, running, stair climbing and kicking a ball will be assessed.
• During play, the therapist can observe how child uses the balance reactions, motor planning skills and protective reactions, as well as the strategies the child uses to move in and out of different positions.

• Posture is also looked at in a variety of positions and how the child’s posture affects their breath control, vocalizations and oral motor control.
• Muscle groups being overused and muscle groups which are underused are analysed. Joint range of motion especially for overused muscle groups like calf muscles for children who persistently walk on toes is measured. Joint laxity is also checked particularly for overstretched joints such as flat feet or children who often locks knees and elbows

During a Physical Therapy Treatment a child may work :• Improve postural control to increase stability during fine motor, gross
motor, and self-care activities.
• Improve static balance to improve motor control and attention and decrease impulsivity.
• Learn to perform the ideation, sequencing, timing and execution components of motor planning.
• Maximize sensory processing and organization skills to put into controlled motor skills.
• Lay down the foundations of gross motor skills to support participation in community and peer activities.

• Treating impairments in systems that affect motor function such as problems with respiratory control and coordination.
• Management of deformities and misalignments in the musculoskeletal system such as scoliosis, chest wall deformities, foot and ankle misalignments.
• Developing fitness program for older children with autism
Aquatic activities• It lays the scope for a large variety of activities.
• It is fun for the child.
• Working with both the support of water and against its resistance. This will help child work harder and longer without tiring. As the child gets fatigue the water supports their bodies allowing them to practice longer.
• Core muscle training is in play in order for the child to remain steady and stable in water. This promotes the core of movement development and most of the kicking and swimming strokes are good for developing core stability.
• Water pressure exerts continuous sensory input which can assist with proprioception or awareness of body in space.

Problems associated with teaching or managing autistic children • Social interaction - difficulty with social relationships, e.g. appearing
aloof and indifferent to others.
• Social communication - difficulty with verbal and non-verbal communication, e.g. not fully understanding the meaning of common gestures, facial expressions or tone of voice.
• Imagination - difficulty in the development of interpersonal skills and imagination, e.g. having a limited range of imaginative abilities, possibly copied and pursued rigidly and repetitively.
• Gross motor difficulties
• Fine motor difficulties

Therapy for children with autism
• Visual learning:• break down the skill (this is to ensure high rate of success eg: practice
climbing with a stepper before going up an actual staircase)
• model the action (“look at me” “do the same”)
• reinforce every little effort by the child (increase motivation)
• label the activity (“jumping” “clapping”)
• show clear pictures of the action (let the child see what we expect from him)
• Start with small parts and build up from there but know when to stop and give rest.

Auditory assistance:
• Some may need longer time to process auditory instructions, give them that time to process.
• if the child does not like noise/talking, try to use verbal commands as little as possible (model actions or use visuals)
• be consistent (start, 1,2,3,4,5, finish: always the same routine with little modifications if necessary)
• keep sentences short and clear (instead of saying ‘take a seat’ say ‘sit down’)
• Learning visually helps them to be less anxious, because they will be shown what they are going to do (eg. picture of jumping) and when it will be finished (start, 5 times, finish) and what will happen next (reinforcement: gets to play with favourite toy)
Studies on intervention for autistic children
• In a 16 week study, the impact of early yoga training program was assessed in school children with ASD. It was called ‘Get Ready To Learn Yoga” (GRTL) program to be undertaken by children daily with a control group just doing normal routine.
• Aberrant Behavior Checklist.
• Concluding results showed that classroom based physiotherapy interventions can help reduce behavioral deficiencies in ASD kids (Koenig, Buckley-Reen & Garg, 2012).

• 30 children from 5 to 16 with ASD were taught “Kata” and divided into control and intervention groups.
• After 14 weeks the intervention group showed a reduction in stereotypic behaviors with effects of training persisting after 30 days hiatus which no practice sessions were conducted (Bahrami, Movahedi, Marandi & Abedi, 2012).
Prognostic Indicators In Childhood
• Early joint attention and imitation skills.
• Decline is atypical features and improvements in adaptive behaviour have been reported for adolescents with ASD and a high IQ, with poorer outcomes evident in social skills and social impairments for young people with learning disability.
• 1/4th ASD children reported regression in skills.

• Early language regression before three years of age in children referred for paediatric neurology assessment, or those referred for ASD assessment has a high probability of being associated with an ASD diagnosis.
• Regression does not appear to be associated with worse prognosis during pre-school years.
• There have been not enough proper studies of later childhood or adolescent onset regression and it is not clear whether the phenomena are clinically the same