Authors 1. Dr. Rayapati Dilip Kumar - Syncronei Medicalsyncronei.com/publication/pub6.pdf · 1. Dr....
14
Authors 1. 1. Dr. Rayapati Dilip Kumar Professor Department of Oral and Maxillofacial Surgery Dayananda Sagar College of Dental Sciences Dayananda Sagar Institutions Shavige Malleshwara Hills Kumaraswamy Layout. Bangalore 560 078; Karnataka INDIA 2. Dr.Honey Verma Post Graduate Student Department of Oral and Maxillofacial Surgery Dayananda Sagar College of Dental Sciences Dayananda Sagar Institutions Shavige Malleshwara Hills Kumaraswamy Layout. Bangalore 560 078; Karnataka INDIA Email: [email protected] 3. Dr.Prashanth N T Associate Professor, Department of Oral and Maxillofacial Surgery Dayananda Sagar College of Dental Sciences Dayananda Sagar Institutions Shavige Malleshwara Hills Kumaraswamy Layout. Bangalore 560 078; Karnataka INDIA 4. Dr.Shobha E S Professor, Department of Oral and Maxillofacial Surgery Dayananda Sagar College of Dental Sciences Dayananda Sagar Institutions Shavige Malleshwara Hills Kumaraswamy Layout. Bangalore 560 078; Karnataka INDIA
Transcript of Authors 1. Dr. Rayapati Dilip Kumar - Syncronei Medicalsyncronei.com/publication/pub6.pdf · 1. Dr....
Authors
1. 1. Dr. Rayapati Dilip Kumar
Professor
Department of Oral and Maxillofacial Surgery
Dayananda Sagar College of Dental Sciences
Dayananda Sagar Institutions
Shavige Malleshwara Hills
Kumaraswamy Layout. Bangalore 560 078; Karnataka
INDIA
2. Dr.Honey Verma
Post Graduate Student
Department of Oral and Maxillofacial Surgery
Dayananda Sagar College of Dental Sciences
Dayananda Sagar Institutions
Shavige Malleshwara Hills
Kumaraswamy Layout. Bangalore 560 078; Karnataka
INDIA
Email: [email protected]
3. Dr.Prashanth N T
Associate Professor, Department of Oral and Maxillofacial Surgery
Dayananda Sagar College of Dental Sciences
Dayananda Sagar Institutions
Shavige Malleshwara Hills
Kumaraswamy Layout. Bangalore 560 078; Karnataka
INDIA
4. Dr.Shobha E S
Professor, Department of Oral and Maxillofacial Surgery
Dayananda Sagar College of Dental Sciences
Dayananda Sagar Institutions
Shavige Malleshwara Hills
Kumaraswamy Layout. Bangalore 560 078; Karnataka
INDIA

QUALITATIVE AND QUANTITATIVE ANALYSIS OF BONE FORMATION IN THE PERI-IMPLANT
DEFECTS GRAFTED WITH POLYCAPROLACTONE (PCL) ALLOPLAST ENRICHED WITH
PLATELET RICH FIBRIN (PRF) - A CLINICAL AND RADIOLOGICAL STUDY.

INTRODUCTION
Dental rehabilitation of partially or totally edentulous patients with dental implants has become a widely accepted
mode of treatment with reliable long term results. Augmentation of edentulous jaws with bone grafts and implant
supported prosthesis has been under clinical research studies for many years. The availability of inadequate quantity
or quality of bone for the implant rehabilitation of edentulous jaws resulted in unsatisfactory prosthetic rehabilitation
from a functional and esthetic point of view and result in failure of these implants. Over the years, many techniques
have been introduced to gain bone volume and quality for placement of dental implants for prosthetic rehabilitation
.The gold standard is still autogenous bone, but intensive research strives to simplify the augmentation procedures,
constantly looking for alternative methods like use of alloplastic polymers. Bioresorbable polymers are widely used
in medical applications today and their potential use in implantology has been expanding rapidly. Polycaprolactone
(PCL) which belongs to the family of aliphatic polyesters has been widely used as a suture material and as a
contraceptive implant with drug eluting properties for the last 30 years.
Similarly Platelet rich fibrin (PRF) may be considered as a second generation platelet concentrate as the natural
concentrate is produced without any anticoagulants or gelifying agents. The biologic activity of the fibrin molecule
is enough in itself to account for the significant cicatricial capacity and the slow polymerization mode confers to the
PRF membrane that particularly favors the physiologic architecture to support the healing process around implants,
leading to good quantity and quality of bone formation in peri implant defects.
Assessing the densities of the cortical and trabecular bone and selecting the quality of bone for implant
placement is critical. With the introduction of computed tomography a new dimension was added in assessing the
bone to ascertain whether it is suitable to receive implants. The use of Pre-operative and Post -operative computed
tomographic scan aids was used to analyze the quantity and quality of bone present in pre implant phase and to
compare the amount of bone gained when peri –implant grafting has been done using Polycaprolactone and Platelet
rich fibrin.
Polycaprolactone in the mesh form customly designed to use in peri implant grafting is a relatively new
phenomenon in implant surgery .This study describes the role of Platelet rich fibrin when used in peri-implant
defects along with alloplast (poly caprolactone) .The clinical and radiological evaluation done pre-op and post –op
using computed tomographic scans allows a comprehensive evaluation of type and amount of bone formed in peri-
implant defects.
MATERIAL & METHODS
This study was designed to assess the quality and quantity of bone formation in the peri implant defects grafted with
PCL enriched with PRF clinically and radiologically .Study was conducted on patients selected for implant
supported prosthetic rehabilitation . Ten out patients with insufficient alveolar bone height in whom peri-implant
defect was observed intra operatively were considered for the study after a thorough preoperative work up by
clinical and radiological (CT scan) assessment.
A custom made case sheet was designed for the study to record the case history .All patients were informed about
the study and Informed consent was taken after the patients were explained about the need for placement of
alloplastic bone grafts along with Platelet rich fibrin. Preoperative CT scans were made in all patients to assess the
bone height and for selection of appropriate implants. Inter arch height and bucco lingual width of the edentulous
area was recorded on study models and surgical acrylic template was prepared. Prior to surgery, patients were
examined for fitness by clinical examination and routine hematological investigations.
Tapered design endosseous implants were used and allograft (SYNCRONIE MEDICAL INDIA) was shaped and
trimmed from a 2 x 2 cm mesh to appropriate size and was enriched with platelet rich fibrin , to fit around the
implant platform as a collar in the peri implant region. Clinical assessment of the patients were done on third day,
seventh day and third month post operatively for pain, swelling, infection, wound break down / soft tissue
dehiscence, implant exposure and implant mobility. CT scans were taken immediately post operatively and after
three months to assess the implant healing and bone regeneration. Volume wise measurements were done using
SIEMENS,SOMATOM definition AS with standard parameters (360 mAs,120 kV) by taking into consideration 1mm
AXIAL & PARAXIAL CUTS stable areas and the volume wise recordings were done.

PREPARATION OF GRAFTS(Fig 1.1-1.2)
Alloplast used in the study was POLYCAPROLACTONE mesh (syncronie) measuring 2 x 2 cm. The graft was
trimmed according to the platform size of the implant placed, using sterile ophthalmic scissors and suitable drill bit
of appropriate size to fit as collar around the implant .
PLATELET RICH FIBRIN PREPARATION(Fig 2.1-2.3)
Routine hematological investigations and informed consent were taken before withdrawal of blood for Platelet rich
fibrin preparation. Tourniquet was placed on the hand from which blood was to be drawn. In all patients, Cephalic
Vein in the ante cubital fossa was used for blood withdrawal.18-gauge needle was used for drawing blood,5 ml of
blood was drawn from the patient and placed in test tubes with no anticoagulant. The collected blood was
centrifuged at 2000 rpm for 10 min, and blood separated into three layers , red lower fraction containing red blood
cells, upper straw coloured cellular plasma and the middle fraction containing the fibrin clot. The upper straw
coloured layer was then removed and middle fraction was collected, separating the clot from underlying RBC,s .The
total dimensions of collected Platelet rich fibrin was 4 to 5 mm to be placed in the peri-implant defect.
.
SURGICAL PROCEDURE OF IMPLANT PLACEMENT(Fig 3.1-3.5)
In all cases Implants were placed under local anesthesia (2 % Lignocaine hydrochloride with 1:2,00,000
adrenaline).Crestal incision was given with No.15 blade followed by reflection of mucoperiosteal flap. Implant
osteotomy was performed using standard drill bits in sequence . Maintaining the parallelism sterile implant was
palced . After placement of cover screws, the peri implant area were assessed and deficient areas were grafted with
PCL enriched with PRF.
RADIOLOGICAL ASSESSMENT
Ct scans were done preoperatively to assess the bone height and for selection of appropriate implants. CT scans
were also done immediately post op to evaluate the measurements of peri-implant defect and three month post
operatively and assessed for implant healing and bone regeneration. CT Scans for all the patients was taken from the
same machine SIEMENS,SOMATOM definition AS with standard parameters (360 mAs,120 kV) .For quantitative
analysis Volume wise measurements were assessed in preoperative, immediate postoperative and three months
postoperative scans by using the VOLUME TOOL , SYNGO SOLARIS 7 software taking into consideration the
stable land marks like the mesial Cemento Enamel Junctions on either side of the edentulous regions, inferior border
of the mandible, apices of the adjacent teeth, lateral aspect of the piriform aperture and all the pre-operative and
post-operative volume wise measurements were compared and recorded.(FIG 4.1-4.3)
Qualitative analysis was done by measuring bone density of the bone formed in peri-implant defect area in terms of
hounsfield unit (HU) , using SYNGO BONE DENSITY TOOL in immediate post op and 3months post op CT scans
and were compared to assess quality of bone formed in the vicinity of implant.(Fig 5.1-5.2)
POST OPERATIVE PROCEDURE
Antibiotics (Cap. Amox 500mg t.i.d for five days) and anti-inflammatory drugs (Tab.Imol t.i.d for three days) were
prescribed along with oral hygiene maintenance instructions. Patients were checked for any pain/ swelling/
infection/ wound break down / soft tissue dehiscence in the implant region on third and seventh post-operative days.
Patients were recalled after seven days for suture removal. Permanent prosthesis was given after 3 months.
RESULTS
All patients were assessed clinically and radiologically. Radiological assessment was done using computed
tomograms. They were done pre operatively to assess the bone height, quality of bone and for selection of
appropriate length and diameter of the implants , Immediate post-operative CT scan was done to measure peri-
implant defect area and three months post operatively, before the commencement of prosthetic phase scans were

assessed for implant healing and bone regeneration in the peri-implant defect area. The immediate post op and the
third-month postoperative CT scans were compared. The measurements of the defect was calculated in terms of
volume in cm cube(cm3) in the computed tomograms using the VOLUME TOOL of the SYNGO SOLARIS 7
software, which gives accurate measurements volume wise. SYNGO SOLARIS software was used taking into
consideration the stable land marks in the scans like the Cemento -Enamel Junction of the teeth on either side of the
edentulous regions, inferior border of the mandible, coronoid and condylar process, lateral aspect of piriform
aperture and apices of the teeth on either side of the edentulous regions. Quality of bone formed in the peri- implant
area after three months was assessed by the SYNGO BONE DENSITY TOOL , which measured bone density in the
terms of hounsfield unit (HU). Comparison of values were done for the immediate post op and 3months post op CT
scans which revealed the type of bone formed in the vicinity of the implant. Radiological evaluations using CT scans
showed substantial increase in the volume wise bone measurements at the grafted regions (with PCL & PRF) at the
end of three months , the bone formed around the implant was of good quality with high density values . The
average volume of bone formed in peri-implant defect in single implant cases put together was approximately
around 1.50 cm 3
in the grafted regions and in multiple implant cases, around 3.5 cm 3 when compared with the pre-
operative values. The quality of bone formed 3 months post operatively was superior with high HU values when
compared with preoperative bone quality .The increased HU values on average ranged from 312 HU preoperatively
and 457 HU 3 months post operatively . In one of the case , loss of graft was recorded 1 week post operatively and
when the peri-implant area was assessed three months post operatively the volume of bone formed was less with low
HU values signifying poor quality of bone formed when compared with successfully grafted peri-implant areas.
Clinical evaluation on the third postoperative day showed pain and swelling in few cases . Implants were stable
clinically in the immediate postoperative period and after three months. Clinical evaluation done after three months
gave positive results and during the time of final prosthesis placement no complications related to the mechanical
components of anchorage units were noted. . Soft tissue healing was excellent. Patient satisfaction related to
aesthetics, comfort, function and recovery was good with eventual decrease in clinical symptoms like pain ,swelling,
& wound dehiscence considering the third post operative day to 3 months post operatively. In non of the patients
findings like implant exposure and implant mobility was recorded.
DISCUSSION
Polycaprolactone is a scaffold with a fully interconnected 3D matrix architecture. These scaffolds were hypothesized
to be suitable grafts for mandibular reconstruction because they:
1) eliminate the need for an autogenous donor site
2) are available in unlimited quantity and consistent quality
3) have a highly porous and honeycomb-like architecture that facilitates the infiltration of new
osteoid and bone trabeculae 8,9
4) do not evoke an undesirable prolonged inflammatory response9 and
5) can withstand local mechanical stresses10
.
Platelet rich fibrin was first used by Choukroun et al. in France and belongs to a new generation of platelet
concentrate1 . Simplified processing technique not requiring biochemical products for its preparation , makes it
superior to PRP . PRF can be used to promote wound healing ,bone growth, graft stabilization, wound healing and
hemostasis because the fibrin matrix is better organized , which more efficiently direct stem cell migration and the
healing program2,3
. The analysis of our results makes it possible to establish significant working parameters
concerning biologic PRF features. After comparison of our values with those obtained for volume of peri-implant
defect immediately post op and three months post op it is possible to consider that on the whole, PRF platelet
cytokines remain trapped in the fibrin meshes, and probably even in the fibrin polymers which promotes bone
formation in the peri implant area and promotes implant stability. In vitro release of growth factors from PRF and
the results of in vivo studies has now put forward a proposal to optimize the clinical application of PRF4. Such
studies have shown better results of PRF over PRP5. The findings by Wiltfang et al. from a series of clinical trials

showed encouraging results. Dohan et al proved a slower release of growth factors from PRF than PRP and observed
better healing properties with PRF. In a study by Bensaid et al6 it was observed that the cells are able to migrate
from the fibrin scaffold , while Kawamura and Urist demonstrated that PRF may act as a supportive matrix for bone
morphogenetic protein as well7, the same fact has been proved in our study through a good quality of bone which is
formed in the vicinity of implant where PRF had proven to be a scaffold concentrating growth factors to allow
osteogenic activity.
In this study, the PCL scaffolds were tested in combination with PRF for the treatment of peri implant defects with
respect to new bone formation, after 3 months of implantation. The quantitative and qualitative CT imaging analysis
showed that the PRF-treated defects had higher bone volume fraction when assessed three months post operatively.
The onset of new bone conduction can be attributed to the properties of the PCL scaffold itself. Scaffolds for peri
implant defects provided at least a temporary load-sharing, if not load-bearing, to withstand the forces of
mastication. The permeability to the scaffolds, both seeded it with bioactive substances and for cellular and vascular
infiltration when implanted11
. Besides possessing the above characteristics, the architecture of the PCL scaffolds
acted as a blotting medium to absorb any hematoma and subsequently promote blood clotting via the release of
calcium ions on its surface , necessary for normal wound healing12
.The other reason for the augmented bone volume
fraction measurement was the application of PRF which is an autologous plasma rich in growth factors that can
serve as local regulators for bone regeneration and hence exert a beneficial effect on bone healing in critical-size
defects13
.
Combining PCL and PRF, a controlled release of growth factors is possible14,15,16
. In our study,
implants has been placed successfully to regenerate new bone in a critical defect of peri implant area adopting the
strategy of a load-bearing 3D PCL scaffold with PRF . The harvesting of autogenous bone and its transplantation, so
far the only safe alternative , was thereby avoided. Based on these results and the effects of combination of the 3D
PCL with mesenchymal stem cells17
, it is clearly indicative of a real alternative to autogenous bone transplantation,
especially for patients with absolute or relative contraindication for bone removal. This must be considered
particularly with regard to the well known problems at the donor region and for the recipient patient as well.
Springer et al. and Macacci et al. have published similar positive results as to the combination of scaffolds18
and
stem cells19
, respectively. Considering comparative bone density assessed pre and post operatively in our study, the
bone generation capacity of both the grafts ( PCL & PRF ) can be explained. There are also important intra- and
inter-individual differences in patients due to their individual clinical situation in relation to quality and quantity of
bone formed. It could also be concluded that patient in whom peri implant defect was grafted with PRF & PCL had
minimum or limited post operative events characterized as swelling , pain , infection etc.
Our study group consisted of a limited number of patients with a limited follow up period. Hence
a more extensive study on more number of patients with a longer period of follow up is required to come to a
definitive conclusion. Regarding different scaffolds in combination with growth factors and for stem cells,
further research will be necessary to define the results of bone healing. Further clinical studies are necessary to
develop bone regeneration in vivo with different scaffolds in combination with growth factors and for stem cells
CONCLUSION
In the study conducted in the Department of Oral and Maxillofacial surgery, Dayananda Sagar College of Dental
Sciences, we assessed the efficacy of alloplast polycaprolactone(PCL)when used along with platelet rich
fibrin(PRF) in the Peri implant deficient regions. The results obtained suggested that Polycaprolactone enhances
early bone healing (3 months) when used along with platelet rich fibrin . Substantial increase in the volume wise
measurement of bone (using VOLUME TOOL , SYNGO SOLARIS 7) post operatively by computed tomograms after
three months was observed. Clinically no major complications were noted after 3months when assessed using
parameters like implant mobility, pain, infection, implant exposure. Our findings support the use of
Polycaprolactone as an alloplast along with platelet rich fibrin in peri implant deficient regions. It can be concluded
that PCL can be used efficaciously clinically and radiographically in the treatment of a peri- implant defect. PCL is
an efficient and readily available alloplast , found to be clinically effective and economical amongst available
regenerative materials and is more fruitful when used along with PRF. However due to limited sample size in our
study, considering future prospects a long term continuation , multicenter randomized, controlled clinical trial is in
process to know its clinical and radiographic effect over bone regeneration.

ILLUSTRATIONS AND TABLES
PREPARATION OF ALLOPLASTIC GRAFT MATERIAL (PCL)
Fig 1.1 Alloplastic graft sheet , polycaprolactone(PCL) (2 X 2 cm)
Fig 1.2 PCL trimmed to appropriate size to adapt in the peri implant defect

PREPARATION OF PLATELET RICH FIBRIN
Fig 2.1 Platelet rich fibrin prepared as a layer between RBCs below & Platelet poor plasma above.
Fig 2.2 PRF separated from underlying RBCs using sterile scissor
Fig 2.3 PRF membrane obtained after draining excess of serum in a sterile lint free cloth

SURGICAL PROCEDURE
Fig 3.1 Preoperative assessment of the edentulous area
Fig 3.2 Drilling done in sequence using burs along with External Irrigation
Fig 3.3 Preparation of osteotomy site
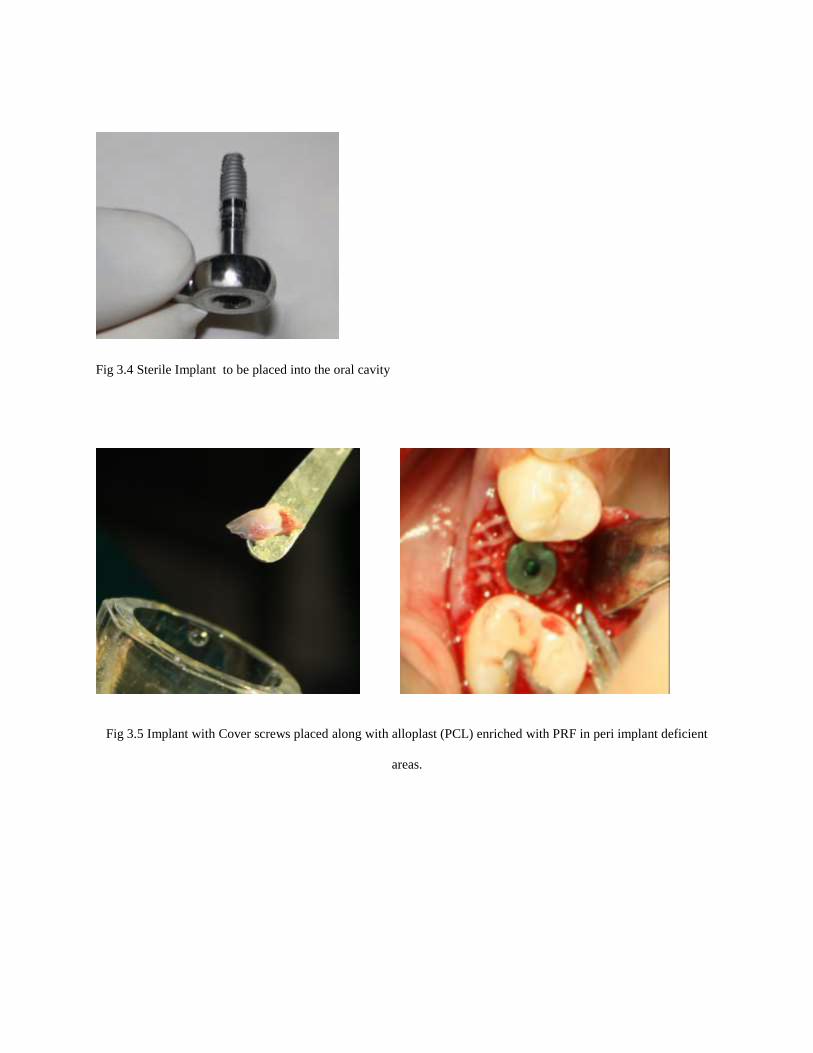
Fig 3.4 Sterile Implant to be placed into the oral cavity
Fig 3.5 Implant with Cover screws placed along with alloplast (PCL) enriched with PRF in peri implant deficient
areas.

QUANTITATIVE ANALYSIS OF BONE FORMED IN PERI IMPLANT DEFECT
Fig 4.1 Volume of implant
Fig 4.2 Volume of peri-implant defect (immediate post op)
Fig 4.3Volume of bone formed peri-implant area (3 months post op)
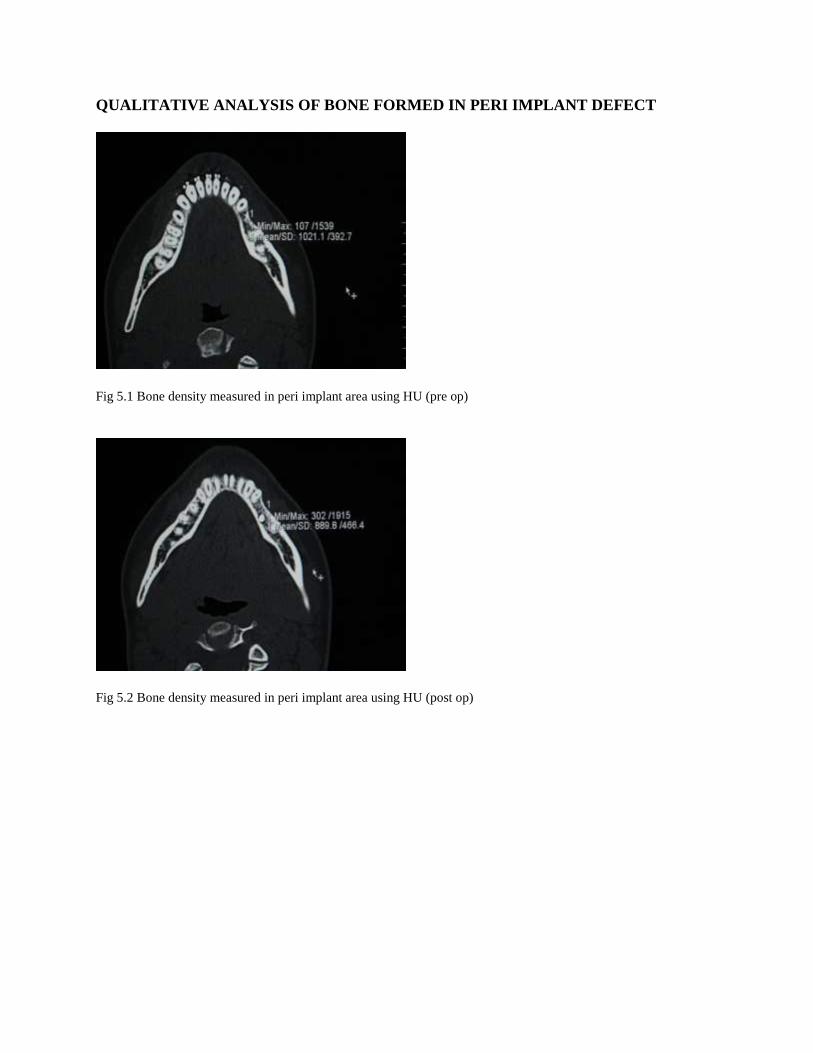
QUALITATIVE ANALYSIS OF BONE FORMED IN PERI IMPLANT DEFECT
Fig 5.1 Bone density measured in peri implant area using HU (pre op)
Fig 5.2 Bone density measured in peri implant area using HU (post op)

TABLES
RADIOLOGICAL ASSESSMENT OF PERI IMPLANT DEFECT IN TERMS OF QUALITY AND QUANTITY OF BONE. TABLE 1(Quality of bone)
Cases Implant
site
HU unit
/pre-op
HU
unit/3
months
post op
Inference
Case1 16 434 498 Quality of
bone formed
is superior comparatively
Case
2(loss of graft
recorded)
36 520 426 Quality of
bone formed is inferior
comparatively
Case 3 46 120 274 Quality of
bone formed is superior
comparatively
Case 4 35 107 302 Quality of bone formed
is superior
comparatively
Case 5 43 320 474 Quality of bone formed
is superior
comparatively
Case 6 26 207 362 Quality of
bone formed
is superior
comparatively
Case 7 47 520 574 Quality of
bone formed is superior
comparatively
Case 8 42 407 512 Quality of
bone formed is superior
comparatively
Case 9 31 313 372 Quality of bone formed
is superior
comparatively
Case 10 25 107 302 Quality of bone formed
is superior
comparatively
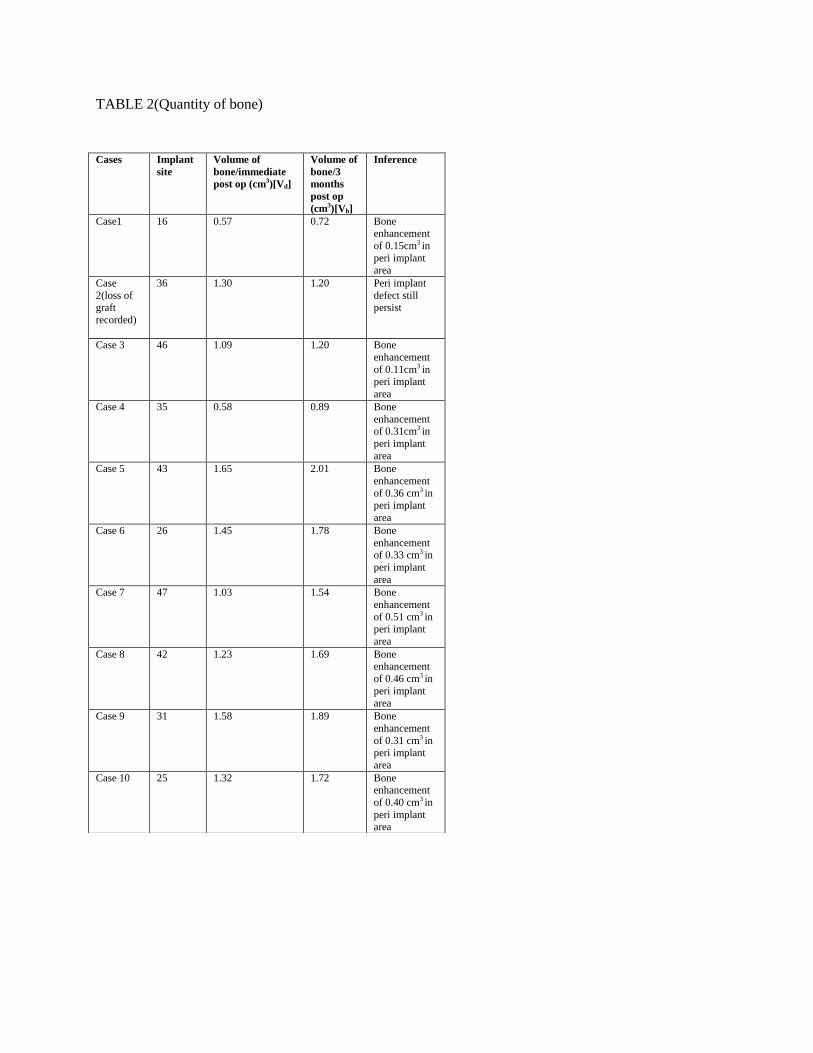
TABLE 2(Quantity of bone)
Cases Implant
site
Volume of
bone/immediate
post op (cm3)[Vd]
Volume of
bone/3
months
post op
(cm3)[Vb]
Inference
Case1 16 0.57 0.72 Bone enhancement
of 0.15cm3 in
peri implant area
Case
2(loss of
graft
recorded)
36 1.30 1.20 Peri implant
defect still
persist
Case 3 46 1.09 1.20 Bone
enhancement
of 0.11cm3 in peri implant
area
Case 4 35 0.58 0.89 Bone
enhancement of 0.31cm3 in
peri implant
area
Case 5 43 1.65 2.01 Bone
enhancement
of 0.36 cm3 in
peri implant
area
Case 6 26 1.45 1.78 Bone
enhancement of 0.33 cm3 in
peri implant
area
Case 7 47 1.03 1.54 Bone
enhancement
of 0.51 cm3 in peri implant
area
Case 8 42 1.23 1.69 Bone enhancement
of 0.46 cm3 in
peri implant
area
Case 9 31 1.58 1.89 Bone
enhancement
of 0.31 cm3 in peri implant
area
Case 10 25 1.32 1.72 Bone enhancement
of 0.40 cm3 in
peri implant area