Australian optometric and ophthalmologic referral pathways for people with age-related macular...
8
RESEARCH PAPER Australian optometric and ophthalmologic referral pathways for people with age-related macular degeneration, diabetic retinopathy and glaucoma Clin Exp Optom 2014; 97: 248–255 DOI:10.1111/cxo.12119 Khalid F Jamous* § BSc(Optom) MOptom Isabelle Jalbert* OD MPH PhD Michael Kalloniatis* † MSc(Optom) PhD Mei Ying Boon* BOptom(Hons) PhD * School of Optometry and Vision Science and † Centre for Eye Health, University of New South Wales, Kensington, Australia § Department of Ophthalmology, Faculty of Medicine, King Saud University, Riyadh, Saudi Arabia E-mail: [email protected] Background: This study investigated the referral pathways offered to patients with age- related macular degeneration (AMD), diabetic retinopathy (DR) or glaucoma (GL) by ophthalmologists and optometrists. Methods: Australian ophthalmologists and optometrists were surveyed regarding referral decisions to other eye-care specialists (inter- or intra-professional), general medical practi- tioners (GPs), low vision rehabilitation (LVR) and support services. Thematic analysis and concept mapping were applied to highlight current and ideal referral pathways. Results: The survey was completed by 155 optometrists and 50 ophthalmologists and deemed representative of their respective professions in Australia. Not surprisingly, the vast majority of the participating optometrists (97 to 99 per cent) referred to ophthalmologists regardless of the underlying condition. Clear differences (Chi-square: p < 0.05) were observed in the referral patterns of optometrists and ophthalmologists to GPs and support services. General medical practitioner services were almost exclusively used for patients with DR, while AMD triggered a significantly higher referral rate to low vision rehabilitation and support services than the other two disorders. Conclusion: While ophthalmologists predominantly referred patients with AMD, DR or GL to low vision rehabilitation services, optometrists’ referrals were highly skewed toward ophthalmology. Referrals to other supporting services by the two groups were not greatly used. The perceived referral pathways by the two eye-care professionals suggested a unidi- rectional route, potentially highlighting the need for a more collaborative approach that facilitates optimal use of eye health care and allied services. Submitted: 13 March 2013 Revised: 6 September 2013 Accepted for publication: 14 September 2013 Key words: age-related macular degeneration, diabetic retinopathy, glaucoma, low vision rehabilitation, ophthalmologist, optometrist, referral pathways High-quality eye care involves optometrists and ophthalmologists working together with general practitioners (GPs), orthoptists and allied health care workers or professionals working for organisations providing low vision rehabilitation (LVR) and support services. 1–3 In Australia, this part of the health-care system is under substantial pres- sure due to the growing number of people with chronic eye disease, such as age-related macular degeneration (AMD), diabetic retinopathy (DR) and glaucoma (GL). 4–6 In addition, the ‘fragmented’ nature of the health-care system results in people with complex and chronic conditions frequently navigating through many potential routes to care on their own and reducing the efficiency of health-care delivery. 7 Co- management between different eye-care professionals was suggested as key to more efficient delivery of ocular health care. 8 Suit- able and timely delivery of eye health care can reduce visual loss and health-care costs, as preventative eye care is significantly less costly than subsequent disability. 9–11 Optometrists encompass a wide range of care, including performing vision and eye assessments, screening for, monitoring and treating eye disease, prescribing and supply- ing spectacles, contact lenses, low vision aids and therapeutic drugs. 12 They also initiate referrals for specialty care, rehabilitative and ancillary services in relation to health and function of the visual system, 13–15 making them essential in the development of co-management plans. Between optom- etrists and ophthalmologists in Australia, co-management plans have been proposed based on their respective training and areas of expertise. For example, proposed ‘shared care’ between local optometrists and hospital-based ophthalmologists can reduce patient waiting time for review and foster working partnerships to provide localised care for the benefit of patients. 16 Because of the systemic nature of some eye diseases, such as DR, GPs may also need to be included in patient management for further medical attention, such as diabetes control. In Australia, GPs can also facilitate referral to psychological counselling services and falls prevention clinics, so optometrists may wish to refer to GPs, particularly as visual impair- ment is associated with depression and increased falls risk. 17–19 Australian eye-care professionals are well placed to participate in a joint effort between CLINICAL AND EXPERIMENTAL OPTOMETRY Clinical and Experimental Optometry 97.3 May 2014 © 2013 The Authors 248 Clinical and Experimental Optometry © 2013 Optometrists Association Australia
Transcript of Australian optometric and ophthalmologic referral pathways for people with age-related macular...

RESEARCH PAPER
Australian optometric and ophthalmologic referral pathways forpeople with age-related macular degeneration,
diabetic retinopathy and glaucoma
Clin Exp Optom 2014; 97: 248–255 DOI:10.1111/cxo.12119
Khalid F Jamous*§ BSc(Optom) MOptomIsabelle Jalbert* OD MPH PhDMichael Kalloniatis*† MSc(Optom) PhDMei Ying Boon* BOptom(Hons) PhD* School of Optometry and Vision Science and† Centre for Eye Health, University of New SouthWales, Kensington, Australia§ Department of Ophthalmology, Faculty of Medicine,King Saud University, Riyadh, Saudi ArabiaE-mail: [email protected]
Background: This study investigated the referral pathways offered to patients with age-related macular degeneration (AMD), diabetic retinopathy (DR) or glaucoma (GL) byophthalmologists and optometrists.Methods: Australian ophthalmologists and optometrists were surveyed regarding referraldecisions to other eye-care specialists (inter- or intra-professional), general medical practi-tioners (GPs), low vision rehabilitation (LVR) and support services. Thematic analysis andconcept mapping were applied to highlight current and ideal referral pathways.Results: The survey was completed by 155 optometrists and 50 ophthalmologists anddeemed representative of their respective professions in Australia. Not surprisingly, the vastmajority of the participating optometrists (97 to 99 per cent) referred to ophthalmologistsregardless of the underlying condition. Clear differences (Chi-square: p < 0.05) wereobserved in the referral patterns of optometrists and ophthalmologists to GPs and supportservices. General medical practitioner services were almost exclusively used for patients withDR, while AMD triggered a significantly higher referral rate to low vision rehabilitation andsupport services than the other two disorders.Conclusion: While ophthalmologists predominantly referred patients with AMD, DR or GLto low vision rehabilitation services, optometrists’ referrals were highly skewed towardophthalmology. Referrals to other supporting services by the two groups were not greatlyused. The perceived referral pathways by the two eye-care professionals suggested a unidi-rectional route, potentially highlighting the need for a more collaborative approach thatfacilitates optimal use of eye health care and allied services.
Submitted: 13 March 2013Revised: 6 September 2013Accepted for publication: 14 September2013
Key words: age-related macular degeneration, diabetic retinopathy, glaucoma, low vision rehabilitation, ophthalmologist, optometrist,referral pathways
High-quality eye care involves optometristsand ophthalmologists working together withgeneral practitioners (GPs), orthoptists andallied health care workers or professionalsworking for organisations providing lowvision rehabilitation (LVR) and supportservices.1–3 In Australia, this part of thehealth-care system is under substantial pres-sure due to the growing number of peoplewith chronic eye disease, such as age-relatedmacular degeneration (AMD), diabeticretinopathy (DR) and glaucoma (GL).4–6 Inaddition, the ‘fragmented’ nature of thehealth-care system results in people withcomplex and chronic conditions frequentlynavigating through many potential routesto care on their own and reducing theefficiency of health-care delivery.7 Co-management between different eye-care
professionals was suggested as key to moreefficient delivery of ocular health care.8 Suit-able and timely delivery of eye health carecan reduce visual loss and health-care costs,as preventative eye care is significantly lesscostly than subsequent disability.9–11
Optometrists encompass a wide range ofcare, including performing vision and eyeassessments, screening for, monitoring andtreating eye disease, prescribing and supply-ing spectacles, contact lenses, low vision aidsand therapeutic drugs.12 They also initiatereferrals for specialty care, rehabilitative andancillary services in relation to health andfunction of the visual system,13–15 makingthem essential in the development ofco-management plans. Between optom-etrists and ophthalmologists in Australia,co-management plans have been proposed
based on their respective training and areasof expertise. For example, proposed ‘sharedcare’ between local optometrists andhospital-based ophthalmologists can reducepatient waiting time for review and fosterworking partnerships to provide localisedcare for the benefit of patients.16 Because ofthe systemic nature of some eye diseases,such as DR, GPs may also need to beincluded in patient management for furthermedical attention, such as diabetes control.In Australia, GPs can also facilitate referral topsychological counselling services and fallsprevention clinics, so optometrists may wishto refer to GPs, particularly as visual impair-ment is associated with depression andincreased falls risk.17–19
Australian eye-care professionals are wellplaced to participate in a joint effort between
C L I N I C A L A N D E X P E R I M E N T A L
OPTOMETRY
Clinical and Experimental Optometry 97.3 May 2014 © 2013 The Authors
248 Clinical and Experimental Optometry © 2013 Optometrists Association Australia

ophthalmologists and optometrists.20,21
Referrals should facilitate easy access to dif-ferent services and enhance early detectionand management of ocular disease. Threeprevalent eye diseases, AMD, DR and GLwere used to investigate these points. Ourstudy is the first attempt to sample attitudesof the two eye-care professional groups todetermine whether the traditional referralprocesses for people with AMD, DR and GLare generally consistent and interactive. Itshould benefit the patient by highlightingearly intervention, avoiding duplication ofservices and instituting cost-effective care. Itshould benefit the practitioners in buildingconfidence in the referral process and ensur-ing that no patient ‘falls through the cracks’.It should benefit the health-care system inminimising costs and expensive hospitalor ophthalmology time without sacrificingquality of care.
METHODS
Survey designA two-part questionnaire consisting of open-ended and closed questions was developedto survey Australian optometrists and oph-thalmologists (Appendix 1). Section 1explored the demographic characteristics ofclinicians, including age, gender, mode andlocation of practice and whether they pro-vided low vision services in their practice orconsider themselves as low vision service pro-viders. Section 2 determined the clinicians’referral patterns and referral criteria toother eye-care and allied services for peoplewith AMD, DR or GL. To determine thereferral pathway to low vision rehabilitationservices, a list of the major organisationsin Australia (for example, Vision Australia,Guide Dogs Australia et cetera) wasincluded. Similarly, to determine the refer-ral pathway to support services, a list wasincluded of the major support organisationsin Australia that are known to provide infor-mation and advice in relation to specificconditions (for example, Diabetes Australia,Glaucoma Australia and Macular Degenera-tion Foundation).
Sampling strategyHard copy and online versions of the surveywere approved by the Human ResearchEthics Advisory (HREA) panel at the Univer-sity of New South Wales. Optometrists wererecruited from the 2009 members’ directory
email list of Optometrists Association Aus-tralia (OAA). A total of 2,092 optometristswere invited electronically to participate inthe survey through a link to the online ques-tionnaire. Ophthalmologists were randomlyselected from the Yellow Pages business tel-ephone directory of Australia and publicdirectories of the major public hospitals inAustralia. A letter including a hard copy ofthe questionnaire, reply paid envelope andan invitation letter with the option to com-plete the questionnaire online was posted to353 ophthalmologists. All ophthalmologistswho participated in this study replied byhard copy.
AnalysisData were analysed using a mixed-methodsstrategy.22 Quantitative data obtained fromclosed-ended data was analysed using SPSS20 software (Version 20; SPSS Inc, Chicago,IL, USA) to conduct descriptive statistics.Chi-square analysis was used to determinesignificant differences among referrals todifferent services for AMD, DR or GL, withp-values of less than 0.05 being consideredsignificant. Qualitative data were analysedfor common themes reported by partici-pants. For example, answers reported byoptometrists that had a common idea suchas ‘visual field check up’, ‘assessment ofvisual field’ and ‘field testing’ were codedunder one theme—‘visual field testing’.Coded data were then entered into a data-base as factors and frequencies of occur-rence analysed.23
The perceptions of the ideal referralpathways for the three ocular conditionswere analysed with concept mapping. Therelationships between different concepts(that is, GPs, optometrists, ophthalmolo-gists, low vision rehabilitation services)were demonstrated using a diagram, whereconcepts were enclosed in circles or boxesand connected with arrows. This methodis a valid scientific tool of analysis in educa-tional research for visualising ideas orprocesses.24,25
RESULTS
Participant characteristicsOf 2,042 invitations confirmed to have beendelivered to optometrists, 155 responseswere received, resulting in a response rate ofeight per cent. For ophthalmologists, 344were successfully delivered and 50 responses
were returned producing a response rateof 15 per cent. The mean age and genderof participating optometrists and ophthal-mologists matched national averages.26
Although ophthalmologists who respondedwere primarily from New South Wales, therewere no significant differences betweenour cohorts and the national averages. Theresponding ophthalmologists were mostlyclassified as general ophthalmologists orthose with multiple subspecialties (60 percent), followed by retinal specialists (12 percent) and anterior segment specialists (eightper cent). None of the above characteristicshad a significant influence on the surveyoutcome (Table 1). Although the overallcharacteristics of the replying cohortswere comparable to national averages, thelower than expected response rates mayhave resulted in an incomplete assessmentregarding the nation as a whole. As data weregenerally consistent, it was considered animportant representation of the investigatedattitudes among eye-care specialists.
We also assessed the patient encounterrates for participating optometrists and oph-thalmologists for each condition. The major-ity of optometrists see five to nine AMDpatients per month and one to four patientswith DR or GL (Table 2A). Comparable dis-tributions were obtained for ophthalmolo-gists (p = 0.91, 0.99 and 0.99 for AMD, DRand GL, respectively) when assessed on anencounter per day rate (Table 2B).
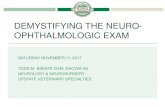
Referral patterns for individualswith AMD, DR or GLRegardless of the underlying condition,optometrists referred the majority ofpatients to ophthalmologists (Chi-square:p = 0.14) but rarely to another optometrist(Chi-square: p = 0.08; Figure 1A). Referralsto other providers were significantly depend-ent on the disorder (Chi-square: p < 0.05).GPs were consulted for only diabeticpatients, while AMD patients mostly referredto low vision rehabilitation and support ser-vices. Ophthalmologists’ referral behaviourwas not significantly different from that ofoptometrists (Figure 1B) with the exceptionof referrals to other ophthalmologists(2-tailed, paired Student’s t-test, p = 0.002).Overall, only the referral pattern to optom-etrists differed significantly between thetwo eye-care professions (Chi-square: p <0.05). With regard to referral to low visionrehabilitation services, the proportion ofophthalmologists referring patients withAMD to low vision rehabilitation services was
Australian optometric and ophthalmologic referral pathways Jamous, Jalbert, Kalloniatis and Boon
© 2013 The Authors Clinical and Experimental Optometry 97.3 May 2014
Clinical and Experimental Optometry © 2013 Optometrists Association Australia 249

significantly greater than the proportionreferring patients with DR or GL (Chi-square: p < 0.05). Vision Australia was themost commonly used organisation by oph-thalmologists (80/58/60 per cent for AMD/
DR/GL, respectively) and optometrists (67/47/44 per cent for AMD/DR/GL, respec-tively), followed by disease-specific groups—Macular Degeneration Foundation for AMD(14 per cent of ophthalmologists, 37 per
cent of optometrists), Diabetes Australia forDR (8 per cent of ophthalmologists, 28 percent of optometrists) and Glaucoma Aus-tralia for GL (26 per cent of ophthalmolo-gists, 32 per cent of optometrists). GuideDogs NSW/ACT was referred to by six to 14per cent of the practitioners. Ophthalmolo-gists also used the Royal Society for the Blind(10 to 14 per cent) while optometristsfavoured the Association for the Blind (8 to12 per cent). A number of other organisa-tions were used at much lower levels.
Referral criteria for individualswith AMD, DR or GLOptometrists’ referral criteria to ocularhealth care and supporting services for thethree conditions were analysed thematicallyand for frequency of occurrence (Table 3).Optometrists’ referral criteria to ophthal-mology were reported by many respondentsfor all three conditions (AMD = 134;DR = 135; GL = 130) and mainly based onfurther investigation or confirmation of adiagnosis, medical or surgical interventionsand treatment. Up to 110 responses indi-cated referring to ophthalmologists forreduced or altered vision or visual acuity.Few optometrists reported their criteria for
Demographic information Optometrists Ophthalmologists
National average Survey National average Survey
Total number of practitioners 4,414 155 887 50Age (years) Average 40.0 44.4 51.6 49.6
Male n.a.* 47.0 n.a.* 49.6Female n.a.* 41.1 n.a.* 47.0
Gender (%) Male 55.8 55.5 84.3 86.0Female 44.2 44.5 15.7 14.0
Location of practice (%) Metropolitan 78.8 66.5 84.4 96.0Rural/remote 21.2 33.5 15.6 4.0
State/Territory of location (%) New South Wales 37.7 38.0 36.4 52.0Victoria 22.1 26.5 25.9 24.0Queensland 20.0 19.3 17.0 8.0Western Australia 8.2 6.5 9.2 4.0South Australia 6.1 5.2 7.3 10.0Tasmania 2.7 1.9 2.2 0.0Australian Capital Territory 1.9 2.6 0.3 0.0Northern Territory 1.1 0.0 n.a.* 2.0
* n.a. = No data available
Table 1. Demographic characteristics of participating optometrists and ophthalmologists compared to national averages26
A Patients seen per month AMD DR GL
Rarely 9% 19% 6%1–4 19% 46% 48%5–9 31% 22% 30%
10–14 25% 9% 11%≥ 15 16% 4% 5%
B Patients seen per day AMD DR GL
Rarely 12% 20% 10%1–4 52% 58.7% 33.3%5–9 23.2% 18.5% 37.9%
10–14 6% 3.6% 9.2%≥ 15 6.8% 1.2% 9.6%
Table 2. For each of the three investigated disorders (A) optometrists and (B) ophthal-mologists indicated a range most closely representing the numbers of patients seen.Percentages of practitioners are shown for age-related macular degeneration (AMD),diabetic retinopathy (DR) and glaucoma (GL).
Australian optometric and ophthalmologic referral pathways Jamous, Jalbert, Kalloniatis and Boon
Clinical and Experimental Optometry 97.3 May 2014 © 2013 The Authors
250 Clinical and Experimental Optometry © 2013 Optometrists Association Australia

referring to the other services except for DR,where 90 respondents reported referral cri-teria to GPs for control of diabetes.
Agreement between optometrists andophthalmologists was observed regardingreferral criteria for low vision rehabilita-tion and support services, including areastargeting the effect of visual impairment(responses in bold and italics indicate crite-ria that were considered important by oph-thalmologists). In particular, optometristsand ophthalmologists particularly focusedon the use of adjunct services based on theremaining visual function as a consequenceof any of the three investigated disorders(Table 4).
Ideal service pathways for patientswith AMD, DR and GLFifty-nine per cent (n = 91) of optometristsdescribed an ideal referral pathway forpatients with AMD, DR and GL, while only 10per cent of the ophthalmologists reported
an opinion on this question. Responses werecategorised as ‘unidirectional’, if the indi-vidual service provider appeared in a distinctorder and patients were channelled fromone to the next. ‘Multidirectional’ pathwaysreferred to those scenarios where severalother services were activated by the sameprovider. Lastly, patients that were co-managed and thus repeatedly transferredbetween services, were labelled as ‘circular’.
There was complete agreement betweenoptometrists and ophthalmologists thatoptometrists or GPs should initiate thesepathways across the investigated disorders.GPs were preferred as initiators in 24.0 percent of scenarios and consequently trig-gered eye-specific care through referral toan optometrist. A particular deviation wasobserved with regard to DR (5.0 per cent ofthe above 24.0 per cent), for which multidi-rectional pathways included consultationswith podiatrists, endocrinologists and nutri-tionists at the same time. Of the remainder,
optometrists and GPs were presumedequally important as primary care providersin 2.7 per cent, while the balance was attrib-uted to optometrists as suggested firstresponder to problems related to AMD, DRand GL.
The majority (88.6 per cent) of reportedideal pathways included ophthalmologistssubsequent to the optometric assessment.This interaction was described as unidirec-tional by 64.6 per cent, while 24.0 per centenvisioned optometrists remaining the maincarers through back-referral by the ophthal-mologists. Alternatively, there was a sugges-tion that optometrists were to refer tolow vision rehabilitation services only (8.7per cent) or they are seen as equivalentwith ophthalmologists, creating a circularreferral pathway also including low visionrehabilitation services (2.7 per cent; AMDonly).
Finally, all proposed patient managementplans resulted in referrals to either low visionrehabilitation services only (62.4 per cent)or a combination of low vision rehabilitationand support services (37.6 per cent). Thisstep was supposed to be initiated by optom-etrists in 45.6 per cent of ideal pathway solu-tions, by ophthalmologists in 51.7 per centor by either for the remainder. It should benoted that 80 per cent of the ophthalmolo-gists suggested this step to be initiated bythem rather than an optometrist. Interest-ingly, low vision rehabilitation and supportservices were reported as the final destina-tion in a linear manner in 60.4 per cent ofscenarios, while only 39.6 per cent inte-grated them as part of a multidirectional(36.9 per cent) or circular (2.7 per cent)step, while consulting with other specialistsat the same time.
DISCUSSION
Previous studies indicate that more than 90per cent of referrals initiated by optometristswere to ophthalmological services for themanagement of AMD, DR or GL.27–29 This islikely to be influenced by the nature of theseconditions, significantly affecting a patient’svision and primarily requiring managementand treatment by an ophthalmologist.30–32
Considering the shortage of practising oph-thalmologists in Australia, high referral ratesto ophthalmologists is likely to compoundthe current shortfalls in the eye-caresystem.33 Rowe, MacLean and Shekelle34
indicated that many chronic cases may notrequire ophthalmological management or
AMD DR GLA
100%
80%
60%
40%
20%
0%
97%
8%4%
88%
49%
99%
5% 4%4%
52%
27%
99%
57%
67%
29%
AMD DR GLB
100%
80%
60%
40%
20%
0%
16% 14%
2%
94%
20%
28%
4%8%
72%
26%28%
68%
8% 10%
*
*
*
*
Ophthalmologists Optometrists GPs LVR services Support services
Figure 1. Distribution of referral decisionsThe proportions of (A) optometrists (n = 155) and (B) ophthal-mologists (n = 50) who refer patients with age-related maculardegeneration (AMD), diabetic retinopathy (DR) or glaucoma (GL)to other health-care and allied services. (CI = 95%, *p < 0.05)
Australian optometric and ophthalmologic referral pathways Jamous, Jalbert, Kalloniatis and Boon
© 2013 The Authors Clinical and Experimental Optometry 97.3 May 2014
Clinical and Experimental Optometry © 2013 Optometrists Association Australia 251

To optometristsAge-realed macular degeneration (AMD)(n = 10)
Diabetic retinopathy (n = 9) Glaucoma (n = 6)
Further eye testing (optical coherencetomography (OCT)
Further eye testing (OCT or retinalphotography) (7)
Visual field testing (5)
or retinal photography) (8) Dilated fundoscopy (5) Low vision aids (3)Dilated fundoscopy (5) Monitoring of diabetic retinopathy (2) Monitoring of glaucoma (1)Low vision aids (4)
To ophthalmologistsAMD (n = 134) Diabetic retinopathy (n = 135) Glaucoma (n = 130)
Reduction or change in vision or visualacuity (110)
Clinical sign of fundus changes (88) Abnormal status of optic disc (98)
Clinical sign of fundus changes (76) Proliferative diabetic retinopathy (61) Abnormal (IOP) (94)Diagnosis or suspicion of wet AMD (57) Moderate to severe non-proliferative diabetic
retinopathy (33)Visual field defects (67)
Diagnosis and treatment (44) Diagnosis and treatment Diagnosis and treatment (44)Further testing (OCT or angiogram) (37) Further testing (OCT or angiogram) (31) Further testing (OCT or pachymetry) (14)
NHMRC guidelines on DR (11) The NHMRC guidelines on glaucoma (7)A family history of glaucoma (2)
To general medical practitionersAMD (n = 5) Diabetic retinopathy (n = 90) Glaucoma (n = 5)
Provision of dietary supplements (3) For diabetes control (79) General health issues (4)General health issues (3) General health issues (17) For medical report (1)Arranging for further services, such ascommunity support services (1)
Arranging for further services, such ascounselling (6)
To support services (n = 68)AMD (n = 68) Diabetic retinopathy (n = 46) Glaucoma (n = 36)
Information & support (58) Information & support (37) Information & support (31)Patient’s request (25) Patient’s request (14) Patient’s request (10)
To low vision rehabilitation servicesAMD (n = 124) Diabetic retinopathy (n = 74) Glaucoma (n = 68)
Visual acuity problems (86) Visual acuity problems (40) Vision problems (46)Vision problems (36) Vision problems (22) Visual acuity problems (27)Low vision aids (31) Low vision aids (19) Orientation and mobility (22)Difficulties to perform activities of dailyliving (26)
Difficulties to perform activities of dailyliving (16)
Low vision aids (11)
Orientation and mobility (11) Orientation and mobility (7) Need for help in home (3)Occupational therapy (7) Occupational therapy (2) Need for help with social issues (2)Need for counselling (7)Patient or family’s request (6)
Table 3. Referral criteriaCriteria reported by optometrists influencing decisions for referrals to health and eye-care providers, indicating the total of responsesreceived in brackets (multiple responses were allowed). Responses in italics indicate criteria that were considered important byophthalmologists.n = number of participants replying to the respective category (please note that this does not correspond to the total number ofparticipants responding to the survey).
Australian optometric and ophthalmologic referral pathways Jamous, Jalbert, Kalloniatis and Boon
Clinical and Experimental Optometry 97.3 May 2014 © 2013 The Authors
252 Clinical and Experimental Optometry © 2013 Optometrists Association Australia

treatment if a condition is controlled.Optometrists could manage these con-trolled conditions, thereby reducing thepatient load on ophthalmological services.12
The proportions of optometrists referringpatients to GPs were very low except forpatients with DR (67 per cent). This is likelyto be due to optimal treatment of DR requir-ing active management of systemic diabetesand cardiovascular risk factors.35 GPs alsoprovide access to adjunct services, such ascounselling or falls prevention programs,which may benefit vision-impaired patientsand thus, low referral rates for AMD and GLto GPs suggest that these patients may bemissing out on these services.36 Even thoughwe did not define levels of visual loss in ourstudy, referrals to low vision rehabilitationand support services were primarily initiatedfor people with AMD (Figure 1). This maybe a consequence of the higher number ofpatients with AMD compared to DR and GLseen by eye-care specialists (Table 2), as wellas the potential for rapid deterioration ofvision with AMD progression.37–40 AMD isalso associated with significant functionalloss requiring multidisciplinary evaluation,especially among elderly patients.41 Educa-tion and awareness campaigns generated
by the Macular Degeneration Foundationin Australia may also have a significantcontribution.42
Visual field was a major criterion in theinvolvement of low vision rehabilitation(Table 4), as were visual fields in concord-ance with recommendations that difficultieswith mobility arise, if the visual field is lessthan 70° circular diameter and rehabilita-tion should be initiated once it is constrictedto 15°.43 This criterion may not be sufficient,as patients with GL may encounter difficul-ties with mobility even though their visualfields and visual acuities are relatively in-tact.44 Similarly, a study suggested that lowvision rehabilitation may be an effectivestrategy to help people with DR to cope withdifficulties in daily living activities.45 Thissuggests that these services are underusedto improve quality of life for people with DRand GL.
Envisioned referral pathwayTwo-thirds of the proposed referral path-ways did not distinguish between disordersand centred on the unidirectional optom-etrist to ophthalmologist relationship. GPswere included as primary care specialists in25 per cent of the scenarios but not taken
into consideration as referrers to low visionrehabilitation or support services. If theywere, this would open additional resourcesto the patient.46 Additional specialists such asendocrinologists, podiatrists and nutrition-ists were considered only in conjunctionwith a DR-specific pathway.47,48 Although thatcan be attributed to the systemic nature ofthe disease, a lack of collaboration betweenspecialists will result in isolated symptoma-tic treatments. Mapped pathways reflectedunidirectional thinking, suggesting there isnot much space for comparing notes andfeedbacks. Most noticeably, regardless of theinitiating party, allied health services, estab-lished to support core professionals, wereconsidered as an end point rather than anintegrated step during diagnosis and treat-ment of disorders of vision. Together withthe main focus of referral criteria on visualacuity and function, these services are likelyto be involved late in the patient’s diseaseprogression and therefore, may not providefull benefits to the patients.
CONCLUSION
Our study indicated that there is recognitionof all the major players contributing to thereferral process for the three investigatedconditions. Referrals by optometrists werehighly skewed toward ophthalmologists, sug-gesting that other eye-care players, such asGPs, other optometrists, low vision rehabili-tation and support services, may beunderused. In addition, the perceived refer-ral pathways were mostly unidirectional,highlighting the need for a more collabora-tive approach that facilitates optimal useof eye healthcare and allied service for themanagement and treatment of age-relatedmacular degeneration, diabetic retinopathyand glaucoma.
ACKNOWLEDGEMENTSKhalid F Jamous was supported by a scholar-ship from King Saud University at Riyadh,Saudi Arabia. This paper was presented inpart at the American Academy of OptometryAnnual meeting in Boston, USA in October2011. We thank Drs Andrew Whatham,Barbara Zangerl and Lisa Nivison-Smith fortheir valuable contribution in reviewing themanuscript.
REFERENCES1. Ratnarajan G, Newsom W, French K, Kean J, Chang
L, Parker M, Garway-Heath DF et al. The impact of
Vision and visual acuity problems
AMD Diabetic retinopathy GlaucomaVisual acuity (VA) (86) VA (40) VA (27)
VA worse than 6/12 (85) VA worse than 6/12 (35) VA worse than 6/12 (24)Near VA less than N5 (1) Poor VA (5) VA too poor to correct with
regular glasses (3)
Vision problems (36) Vision problems (22) Vision problems (46)
Significant visual lossaffecting independence andfunctional vision (32)
Significant visual lossaffecting independence andfunctional vision (18)
Significant visual field loss(less than 20 degree field ofview remaining) (n = 42)
Poor prognosis of visionrecovery (3)
Inability of patients to copewith regular eyeglassesalone (4)
Visual difficulties beyondthe scope of spectacles andsimple magnifiers (2)
Reduced contrast sensitivity(1)
Peripheral field lossaffecting mobility (1)Field loss crossinghorizontal meridian (i.e. anyinferior field loss) (1)
Table 4. Particular concerns regarding vision and visual acuity problemsThe reported visual parameters used as referral criteria to low vision rehabilitationservices for patients with age-related macular degeneration (AMD), diabetic retinopathyor glaucoma.
Australian optometric and ophthalmologic referral pathways Jamous, Jalbert, Kalloniatis and Boon
© 2013 The Authors Clinical and Experimental Optometry 97.3 May 2014
Clinical and Experimental Optometry © 2013 Optometrists Association Australia 253

glaucoma referral refinement criteria on referralto, and first-visit discharge rates from, the hospitaleye service: the Health Innovation & EducationCluster (HIEC) Glaucoma Pathways project. Oph-thalmic Physiol Opt 2013; 33: 183–189.
2. Department of Health and Ageing. Nationalframework for action to promote eye healthand prevent avoidable blindness and visionloss. Canberra: Commonwealth of Australia;2005. Available from: http://www.health.gov.au/internet/main/publishing.nsf/Content/EA9F52585145B878CA2572DD000C19FF/$File/ehframwork.pdf. [Accessed 13 July 2012].
3. Culham LE, Ryan B, Jackson AJ, Hill AR, Jones B,Miles C, Young JA et al. Low vision services forvision rehabilitation in the United Kingdom. Br JOphthalmol 2002; 86: 743–747.
4. Armstrong BK, Gillespie JA, Leeder SR, Rubin GL,Russell LM. Challenges in health and health carefor Australia. Med J Aust 2007; 187: 485–489.
5. Wagner EH, Austin BT, Davis C, Hindmarsh M,Schaefer J, Bonomi A. Improving chronic illnesscare: translating evidence into action. Health Aff(Millwood) 2001; 20: 64–78.
6. Australian Institute of Health and Welfare. Visionproblems among older Australians: AustralianInstitute of Health and Welfare; 2005. Availablefrom: http://www.aihw.gov.au/publications/aus/bulletin27/bulletin27-c00.pdf. [Accessed 2January 2009].
7. Hofmarcher MM, Oxley H, Rusticelli E. Improvedhealth system performance through better carecoordination, OECD Health Working Papers,OECD Publishing. 2007; No. 30.
8. Optometry Board of Australia. Guidelines for Useof Scheduled Medicines. Available from: http://www.optometryboard.gov.au/Search.aspx?q=guidelines%20glaucoma.[Accessed 4 October 2012]
9. Demers-Turco P. Providing timely and ongoingvision rehabilitation services for the diabeticpatient with irreversible vision loss from diabeticretinopathy. J Am Optom Assoc 1999; 70: 49–62.
10. Javitt JC, Aiello LP, Bassi LJ, Chiang YP, Canner JK.Detecting and treating retinopathy in patients withtype I diabetes mellitus. Savings associated withimproved implementation of current guidelines.Ophthalmology 1991; 98: 1565–1573.
11. Javitt JC, Aiello LP, Chiang Y, Ferris FL, Canner JK,Greenfield S. Preventive eye care in people withdiabetes is cost-saving to the federal government:implications for health-care reform. Diabetes Care1994; 17: 909–917.
12. Kiely PM. Optometrists Association Australia Uni-versal (entry-level) and Therapeutic CompetencyStandards for Optometry 2008. Clin Exp Optom2009; 92: 362–386.
13. Shuttleworth GN, Dunlop A, Collins JK, James CR.How effective is an integrated approach to lowvision rehabilitation? Two year follow up resultsfrom south Devon. Br J Ophthalmol 1995; 79: 719–723.
14. Lovie-Kitchin JE, Keeffe JE, Taylor HR. Referral tolow vision services by optometrists. Clin Exp Optom1996; 79: 227-233.
15. Junghans B, Jacobs R, Hendicott P, Cochrane A,Palagyi A. Delivering optometric graduatesready for practice beyond the cities and readyto serve an ageing population 2011. Availablefrom: http://www.olt.gov.au/project-delivering-optometric-graduates-ready-unsw-2007. [Accessed11 November 2012]
16. O’Connor PM, Harper CA, Brunton CL, Clews SJ,Haymes SA, Keeffe JE. Shared care for chroniceye diseases: perspectives of ophthalmologists,optometrists and patients. Med J Aust 2012; 196:646–650.
17. Department of Health and Ageing. NationalFramework for Action to promote eye health andprevent avoidable blindness and vision loss. 2005.Available from: http://www.health.gov.au/internet/main/publishing.nsf/Content/EA9F52585145B878CA2572DD000C19FF/$File/ehframwork.pdf. [Accessed 14 July 2012].
18. Lord SR, Tiedemann A, Chapman K, Munro B,Murray SM, Gerontology M, Ther GR et al. Theeffect of an individualized fall prevention programon fall risk and falls in older people: a randomized,controlled trial. J Am Geriatr Soc 2005; 53: 1296–1304.
19. Black AA, Wood JM, Lovie-Kitchin JE. Inferiorvisual field reductions are associated with poorerfunctional status among older adults with glau-coma. Ophthalmic Physiol Opt 2011; 31: 283–291.
20. Martin DP, Diehr P, Price KF, Richardson WC.Effect of a gatekeeper plan on health services useand charges: a randomized trial. Am J Public Health1989; 79: 1628–1632.
21. Kim JJ, Kim CM. Models for joint ophthalmology–optometry patient management. Curr OpinOphthalmol 2011; 22: 256–260.
22. Johnson RB, Onwuegbuzie AJ, Turner LA. Towarda definition of mixed methods research. J MixedMethods Res 2007; 1: 112–133.
23. Miles MB, Huberman AM. Qualitative Data Analy-sis: An Expanded Sourcebook: Thousand Oaks,California: Sage Publications, 1994.
24. Novak JD. Concept mapping: A useful tool forscience education. J Res Sci Teach 1990; 27: 937–949.
25. Davies M. Concept mapping, mind mapping andargument mapping: what are the differences anddo they matter? Higher Educ 2011; 62: 279–301.
26. AIHW. Australian Institute of Health and Welfare.Eye health labour force in Australia. Cat. no. PHE116. Canberra: AIHW, 2009.
27. Wood J, Jeffery M, Tame S. Glaucoma screening byoptometrists. Clin Exp Optom 1993; 76: 199–207.
28. Sheldrick JH, Ng C, Austin DJ, Rosenthal AR. Ananalysis of referral routes and diagnostic accuracyin cases of suspected glaucoma. OphthalmicEpidemiol 1994; 1: 31–39.
29. Pooley JE, Frost EC. Optometrists’ referrals to theHospital Eye Service. Ophthalmic Physiol Opt 1999;19 Suppl 1: S16–S24.
30. O’Shea JG. Age-related macular degeneration: aleading cause of blindness. Med J Aust 1996; 165:561.
31. Infeld DA, O’Shea JG. Glaucoma: diagnosis andmanagement. Postgrad Med J 1998; 74 (878): 709–715.
32. Barber AJ. A new view of diabetic retinopathy: aneurodegenerative disease of the eye. ProgNeuropsychopharmacol Biol Psychiatry 2003; 27: 283–290.
33. Pick ZS, Stewart J, Elder MJ. The New Zealandophthalmology workforce 2008. Clin ExperimentOphthalmol 2008; 36: 762–766.
34. Rowe S, MacLean CH, Shekelle PG. Preventingvisual loss from chronic eye disease in primary care.JAMA 2004; 291: 1487–1495.
35. Gardner TW, Antonetti DA, Barber AJ, LaNoue KF,Levison SW. Diabetic retinopathy: more thanmeets the eye. Surv Ophthalmol 2002; 47, Suppl 2:S253–S262.
36. Sims J, Kerse N, Naccarella L, Long H. Healthpromotion and older people: the role of thegeneral practitioner in Australia in promotinghealthy ageing. Aust N Z J Public Health 2000; 24:356–359.
37. Green J, Siddall H, Murdoch I. Learning to live withglaucoma: a qualitative study of diagnosis and theimpact of sight loss. Soc Sci Med 2002; 55: 257–267.
38. Chu J, Ali Y. Diabetic retinopathy: a review. DrugDevelop Res 2008; 69: 1–14.
39. Chopdar A, Chakravarthy U, Verma D. Age-relatedmacular degeneration. Br Med J 2003; 326 (7387):485–488.
40. Klein R, Klein BE, Linton KL. Prevalence of age-related maculopathy. The Beaver Dam Eye StudyOphthalmol 1992; 99: 933–943.
41. Lamoureux EL, Pallant JF, Pesudovs K, Rees G,Hassell JB, Keeffe JE. The effectiveness of low-visionrehabilitation on participation in daily living andquality of life. Invest Ophthalmol Vis Sci 2007; 48:1476–1482.
42. Macular Degeneration Foundation. MacularDegeneration Awareness Week, 2009. Availablefrom: http://www.mdfoundation.com.au/mdaw-past.aspx. [Accessed13 April 2011].
43. Lovie-Kitchin JE, Soong GP, Hassan SE, Woods RL.Visual field size criteria for mobility rehabilitationreferral. Optom Vis Sci 2010; 87: E948–E957.
44. Noe G, Ferraro J, Lamoureux E, Rait J, Keeffe JE.Associations between glaucomatous visual field lossand participation in activities of daily living. ClinExperiment Ophthalmol 2003; 31: 482–486.
45. Lamoureux EL, Hassell JB, Keeffe JE. The impactof diabetic retinopathy on participation in dailyliving. Arch Ophthalmol 2004; 122: 84–88.
46. Khan SA, Das T, Kumar SM, Nutheti R. Low visionrehabilitation in patients with age-related maculardegeneration at a tertiary eye care centre in south-ern India. Clin Experiment Ophthalmol 2002; 30: 404–410.
47. Pomeroy SEM, Cant RP. General practitioners’decision to refer patients to dietitians: insight intothe clinical reasoning process. Aust J Prim Health2010; 16: 147–153.
48. Woods CA. Working better with GPs: Lessons to belearned from a study of health care networks in themanagement of diabetes. Clin Exp Optom 2006; 89:1–2.
Australian optometric and ophthalmologic referral pathways Jamous, Jalbert, Kalloniatis and Boon
Clinical and Experimental Optometry 97.3 May 2014 © 2013 The Authors
254 Clinical and Experimental Optometry © 2013 Optometrists Association Australia

APPENDIX 1
Abbreviated version of questionnaire
The questionnaire was identical for optometrists and ophthalmologists except for question 3, where ophthalmologists were asked for theirsubspecialty (general ophthalmologists, retina, glaucoma, refractive surgery, cataract surgeon, neuropathology, paediatric, oculoplasticsurgeon, anterior segment, other). Additionally, questions 6, 9 and 12 of the questionnaire were asked in terms of patients per day, ratherthan per month on the ophthalmological version of the questionnaire to account for the anticipated larger number of patients. Thefull-length questionnaire includes appropriate space to answer each question and also a list of low vision rehabilitation organisations andsupport services.
Section 1 (Demographic information)1. Age: 20–29 30–39 40–49 50–59 ≥602. Gender: Male Female3. Mode of practice: (Tick all that apply)
Associate/Partner Sole practitioner FranchiseeIndependent Corporate/Franchise Other
4. State or territory of practice?ACT NSW NT QLD SA TAS VIC WA
5. Which areas do you provide services for?Metropolitan Rural Remote
Section 2:Age-related macular degeneration (AMD):6. On average, how many patients do you see in a month with AMD?
Rarely 1–2 3–5 6–10 11–20 ≥207. Which service(s) do you refer a patient with AMD to?
Optometrists Ophthalmologists LVR services Support services GPs Other;8. What are your criteria for referring patients with AMD to such services?
Diabetic retinopathy (DR):9. On average, how many patients do you see in a month with DR?
Rarely 1–2 3–5 6–10 11–20 ≥2010. Which service(s) do you refer a patient with DR to?
Optometrists Ophthalmologists LVR services Support services GPs Other;
11. What are your criteria for referring patients with DR to such services?Glaucoma:12. On average, how many patients do you see in a month with glaucoma?
Rarely 1–2 3–5 6–10 11–20 ≥2013. Which service(s) do you refer a patient with glaucoma to?
Optometrists Ophthalmologists LVR services Support services GPs Other;14. What are your criteria for referring patients with glaucoma to such services?15. When you refer patients with any one of these visual conditions (AMD, DR or glaucoma), do you provide them with information
or advice about the service or organisation that they are referred to?
16. Can you describe what you would consider is an ideal referral pathway for patients with AMD? _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _17. Can you describe what you would consider is an ideal referral pathway for patients with DR? _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _18. Can you describe what you would consider is an ideal referral pathway for patients with glaucoma? _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
Australian optometric and ophthalmologic referral pathways Jamous, Jalbert, Kalloniatis and Boon
© 2013 The Authors Clinical and Experimental Optometry 97.3 May 2014
Clinical and Experimental Optometry © 2013 Optometrists Association Australia 255