August 2017 Lunch and Learn Fractures and External Causes · 2017-08-10 · Human Bone...
79
August 2017 Lunch and Learn Fractures and External Causes
Transcript of August 2017 Lunch and Learn Fractures and External Causes · 2017-08-10 · Human Bone...

August 2017 Lunch and LearnFractures and External Causes
Housekeeping Items• All attendees are muted to eliminate background
noise
• Questions will be addressed at the end of the session via “Questions” queue
• Session recording will be provided in the coming day along with a PDF of the slides
• Attendees will receive an certificate of attendance
• AHIMA CEUs can be applied for immediately
• AAPC CEUs will be available in the next several weeks (an email notification will be provided when this is finalized)
Ms. Scott is the current director of coding quality and professional development at TrustHCS. She has vast management, education, coding and auditing expertise. She has over 10 years of management experience, a combined 15 years educating, and 26 years of coding and auditing experience. Throughout her management and coding experience she has also performed coding compliance audits and DRG validation reviews. Her engagements with other HIM professionals have focused on guiding coding efforts to increase accuracy and timeliness. She has experience working with a wide range of HIM departments. This experience allows her to combine her knowledge with real-world experience to drive HIM department efforts and programs.
Today’s PresenterNena Scott, MSEd, RHIA, CCS, CCS-P, CCDS

ObjectivesAfter completing this education participants will:
• Have refreshed their knowledge and understanding of the anatomy and physiology related to fractures.
• Have increased their knowledge and understanding of the coding guidelines in reference to fractures and external causes.
• Have an understanding of the coding of fractures and external causes ICD-10-CM and procedures in ICD-10-PCS.

Anatomy of Skeletal System

Anatomy of Skeletal System
6

Skeletal SystemConsists of 206 bones
22 bones in skull
4 bones in pectoral girdle
6 bones in middle ear
60 bones in upper limbs
1 hyoid bone
60 bones in lower limbs
26 bones in vertebral column
2 bones in pelvic girdle
25 bones in thoracic cage
7

Parts of the Skeletal SystemAxial Skeleton – Forms the longitudinal part of the body (80 bones)
• Skull (cranium and facial bones)
• Hyoid bone (anchors tongue and muscles associated with swallowing)
• Vertebral column (vertebrae and disks)
• Bony thorax (ribs and sternum)
• 80 bones
Appendicular Skeleton (126 bones)
• Pectoral girdle (clavicles and scapulae)
• Upper limbs (arms, wrists, hands)
• Pelvic girdle (ischium, ilium, and pubic bones form the coxae which attach posteriorly to the sacrum and coccyx)
• Lower limbs (leg, ankles, feet)
8

Human Bone Classification• Long – long longitudinal axes and expanded ends. (e.g., forearm and thigh bones)
• Short – somewhat cubelike, with their lengths and widths roughly equal. (e.g., wrist and ankle bones)
• Flat – platelike structures with broad surfaces. (e.g., rib, scapulae and some of the skull bones)
• Irregular – variety of shapes and are usually connected to several other bones. (e.g., vertebrae and many facial bones)
• Sesamoid or round – small and nodular and are embedded within tendons adjacent to joints, where the tendons are compressed. (e.g., kneecap (patella))
9

Anatomy of the Skull
10
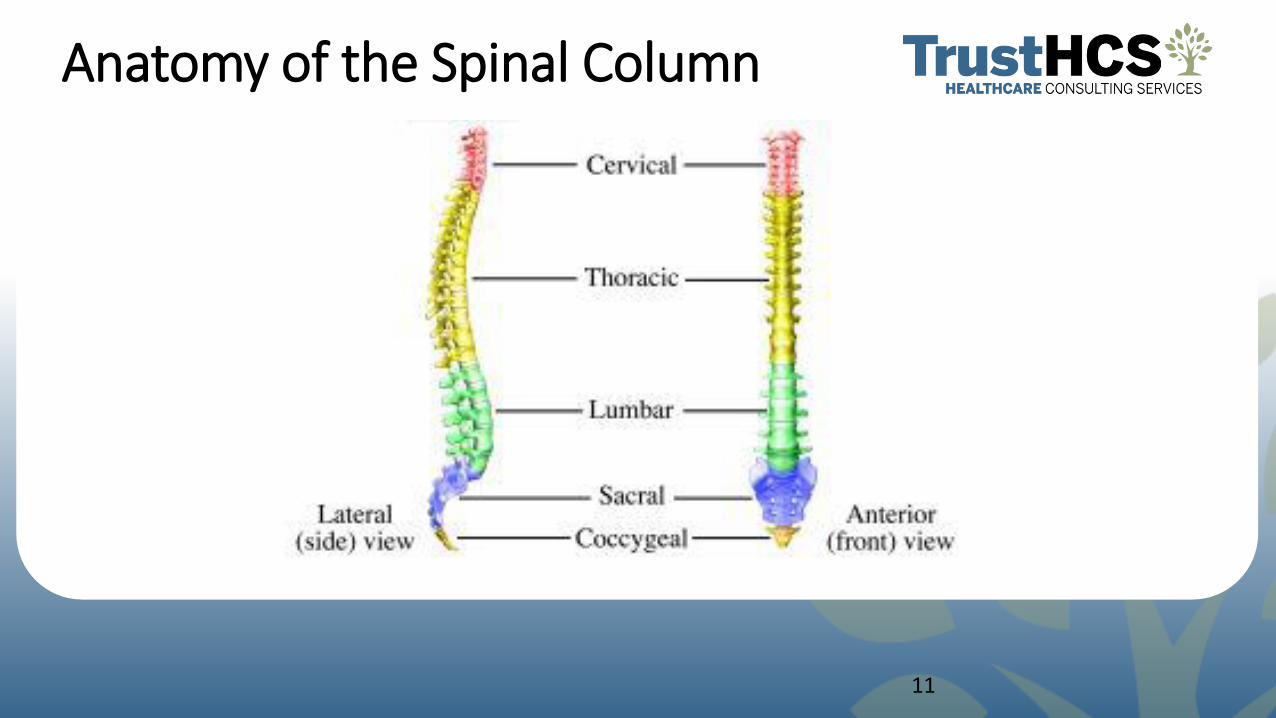
Anatomy of the Spinal Column
11
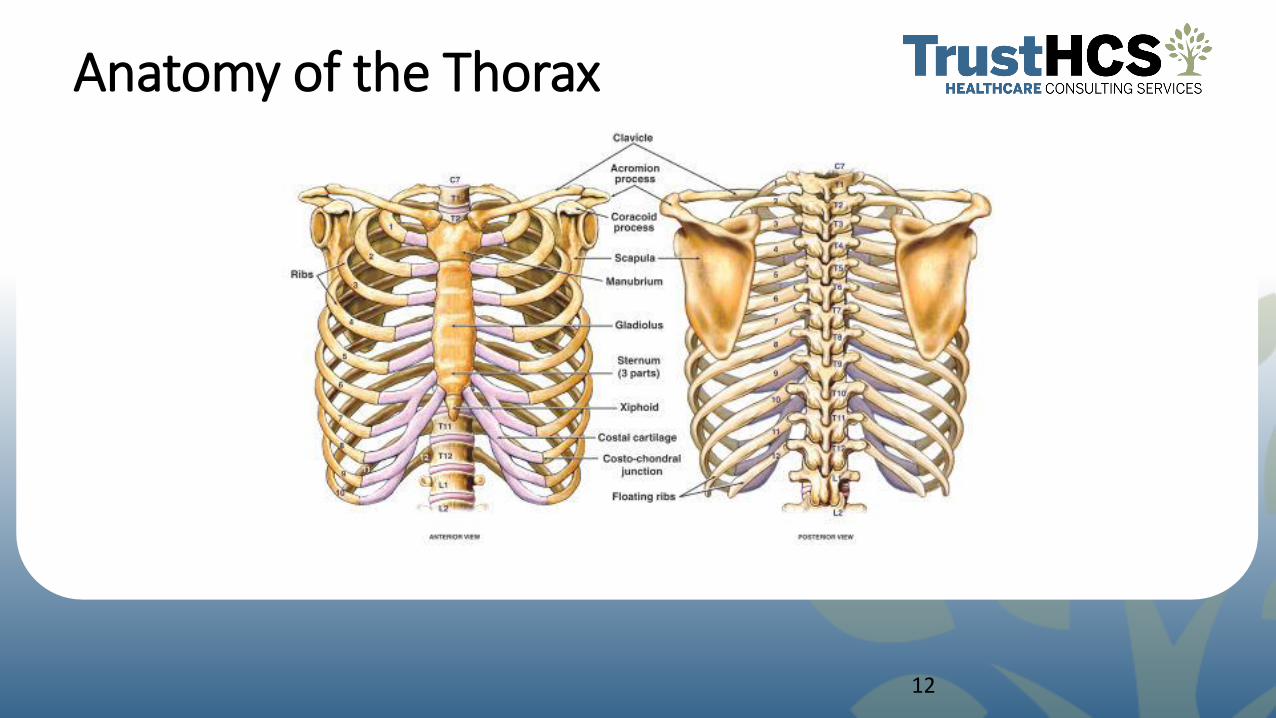
Anatomy of the Thorax
12

Anatomy of the Pectoral Girdle
13

Anatomy of the Pelvis
14

Anatomy of the Upper Limbs
15

Anatomy of the Lower Limbs
16

Fractures

Open vs. Closed Fractures
18

Portions of the Fractured Bone –Not the Bone Involved
Condyle
• Round prominence at the end of a bone, most often part of a joint
Coronoid Process
• “like a crown”--upper part of a bone
Ramus
• “a branch”
Symphysis
• Connected by broad flattened disks of fibrocartilage, which adhere to the ends of each bone, as in the articulations between the bodies of the vertebrae
19

Coding Guidelines

Coding of Traumatic Fractures
• The principles of multiple coding of injuries should be followed in coding fractures.
• Fractures of specified sites are coded individually by site in accordance with both the provisions within categories S02, S12, S22, S32, S42, S49, S52, S59, S62, S72, S79, S82, S89, S92 and the level of detail furnished by medical record content.
• Fractures not indicated as open or closed should be coded to closed.
• Fractures not indicated whether displaced or not displaced should be coded to displaced.
21

Initial vs. Subsequent Encounter
• Traumatic fractures are coded using the appropriate 7th character for initial encounter (A, B, C) while the patient is receiving active treatment for the fracture. These initial encounter codes relate only to those traumatic fracture that utilize the Gustilo Open Fracture Classification.
• The appropriate 7th character for initial encounter should also be assigned for a patient who delayed seeking treatment for the fracture or nonunion.
• Fractures are coded using the appropriate 7th character for subsequent care for encounters after the patient has completed active treatment of the fracture and is receiving routine care for the fracture during the healing or recovery phase.
22

Initial vs. Subsequent Encounter
• Care for complications of surgical treatment for fracture repairs during the healing or recovery phase should be coded with the appropriate complication codes.
• Care of complications of fractures, such as malunion and nonunion, should be reported with the appropriate 7th character for subsequent care with nonunion (K, M, N,) or subsequent care with malunion (P, Q, R).
• A code from category M80, not a traumatic fracture code, should be used for any patient with known osteoporosis who suffers a fracture, even if the patient had a minor fall or trauma, if that fall or trauma would not usually break a normal, healthy bone.
23

Coding GuidelinesExternal Causes of Morbidity

External Cause Coding Guidelines
External cause code used for length of treatment
• Assign the external cause code, with the appropriate 7th character (initial encounter, subsequent encounter or sequela) for each encounter for which the injury or condition is being treated.
Use the full range of external cause codes
• Use the full range of external cause codes to completely describe the cause, the intent, the place of occurrence, and if applicable, the activity of the patient at the time of the event, and the patient’s status, for all injuries, and other health conditions due to an external cause.
25
External Cause Coding Guidelines Assign as many external cause codes as necessary
• Assign as many external cause codes as necessary to fully explain each cause. If only one external code can be recorded, assign the code most related to the principal diagnosis.
The selection of the appropriate external cause code
• The selection of the appropriate external cause code is guided by the Alphabetic Index of External Causes and by Inclusion and Exclusion notes in the Tabular List.
26

External Cause Coding Guidelines
External cause code can never be a principal diagnosis • An external cause code can never be a principal (first-listed) diagnosis. Combination external cause codes• Certain of the external cause codes are combination codes that identify sequential
events that result in an injury, such as a fall which results in striking against an object. The injury may be due to either event or both. The combination external cause code used should correspond to the sequence of events regardless of which caused the most serious injury.
No external cause code needed in certain circumstances • No external cause code from Chapter 20 is needed if the external cause and intent are
included in a code from another chapter (e.g. T36.0X1- Poisoning by penicillins, accidental (unintentional)).
27

Use of Nonprovider Documentation for External Cause of Morbidity
Coding Clinic, First Quarter 2014: Page 19
Question:
External causes of morbidity coding may require up to four codes to identify the cause of injury, the intent of the injury (accident versus intentional), the place of injury, and the person's status at the time of injury. Can you please clarify whether coders must use physician documentation or if coders can use information from non-provider documentation, such as nurse's notes, documentation from ambulance transport, etcetera? It seems that it would be labor intensive to expect a physician to restate documentation that may have already been provided by ambulance transport or the emergency room nurse. Would you please address this issue nationally so everyone can be consistent?
Answer:
Coders should use information contained in the official medical record. Codes for external causes of morbidity are assigned based on physician documentation; however, if the physician does not document external cause information, coders may use documentation available from nonphysicians. If there is conflict between the physician and nonphysician documentation, the physician's documentation takes precedence.
Place of Occurrence Guideline • Codes from category Y92, Place of occurrence of the external cause, are secondary
codes for use after other external cause codes to identify the location of the patient at the time of injury or other condition.
• A place of occurrence code is used only once, at the initial encounter for treatment. No 7th characters are used for Y92. Only one code from Y92 should be recorded on a medical record. A place of occurrence code should be used in conjunction with an activity code, Y93.
• Do not use place of occurrence code Y92.9 if the place is not stated or is not applicable.
29

Activity Code • Assign a code from category Y93, Activity code, to describe the activity of the patient at
the time the injury or other health condition occurred. • An activity code is used only once, at the initial encounter for treatment. Only one code
from Y93 should be recorded on a medical • record. An activity code should be used in conjunction with a place of occurrence code,
Y92. • The activity codes are not applicable to poisonings, adverse effects, misadventures or
sequela . • Do not assign Y93.9, Unspecified activity, if the activity is not stated. • A code from category Y93 is appropriate for use with external cause and intent codes if
identifying the activity provides additional information about the event.
30

Place of Occurrence, Activity, and Status Codes Used with Other External Cause Code
When applicable, place of occurrence, activity, and external cause status codes are sequenced after the main external cause code(s).
Regardless of the number of external cause codes assigned, there should be only one place of occurrence code, one activity code, and one external cause status code assigned to an encounter.
31

If the Reporting Format Limits the Number of External Cause Codes
If the reporting format limits the number of external cause codes that can be used in reporting clinical data, report the code for the cause/intent most related to the principal diagnosis.
If the format permits capture of additional external cause codes, the cause/intent, including medical misadventures, of the additional events should be reported rather than the codes for place, activity, or external status.
32

Multiple External Cause Coding Guidelines
More than one external cause code is required to fully describe the external cause of an illness or injury. The assignment of external cause codes should be sequenced in the following priority: If two or more events cause separate injuries, an external cause code should be assigned for each cause. The first-listed external cause code will be selected in the following order:
• External codes for child and adult abuse take priority over all other external cause codes.
• External cause codes for terrorism events take priority over all other external cause codes except child and adult abuse.
• External cause codes for cataclysmic events take priority over all other external cause codes except child and adult abuse and terrorism.
• External cause codes for transport accidents take priority over all other external cause codes except cataclysmic events, child and adult abuse and terrorism.
33

Multiple External Cause Coding Guidelines
• Activity and external cause status codes are assigned following all causal (intent) external cause codes.
• The first-listed external cause code should correspond to the cause of the most serious diagnosis due to an assault, accident, or self-harm, following the order of hierarchy listed above.
34

Unknown or Undetermined Intent Guideline
If the intent (accident, self-harm, assault) of the cause of an injury or other condition is unknown or unspecified, code the intent as accidental intent. All transport accident categories assume accidental intent.
Use of undetermined intent
• External cause codes for events of undetermined intent are only for use if the documentation in the record specifies that the intent cannot be determined.
35

Sequelae (Late Effects) of External Cause Guidelines
Sequelae external cause codes Sequela are reported using the external cause code with the 7th character “S” for sequela. These codes should be used with any report of a late effect or sequela resulting from a previous injury. Sequela external cause code with a related current injuryA sequela external cause code should never be used with a related current nature of injury code. Use of sequela external cause codes for subsequent visits Use a late effect external cause code for subsequent visits when a late effect of the initial injury is being treated. Do not use a late effect external cause code for subsequent visits for follow-up care (e.g., to assess healing, to receive rehabilitative therapy) of the injury when no late effect of the injury has been documented
36

Skull Fractures and Intracranial InjuriesFractures of the skull and facial bones are classified to category S02.
• Fourth character indicates the area of the skull or face fractured.
• Fifth character provides additional specificity, such as the specific bone or the type of fracture.
Intracranial injury involves open wound of the head (S01.-) or a fracture of the skull (S02.-), these are coded separately, as instructed by the notes in the Tabular List. Codes for intracranial injury (S06.-) have additional characters to indicate:
• The type of injury, location, and the level of consciousness.
• Whether a loss of consciousness was associated with the injury
• Whether there was loss of consciousness of any duration with death due to brain injury or due to any other cause, prior to regaining consciousness.
37
Coding Example #1
A 22-year-old man was brought to the Emergency Room after being struck by a football while playing during a college football game. He was knocked unconscious for 10 minutes. At the Emergency Room the physician ordered a CT scan of the brain. The final diagnosis was concussion. How would this scenario be coded?
38

Coding Example #1
Code #1
Diagnosis: Concussion
Step 1 Go to the alphabetic index and look up the main term and subterm(s)
Concussion
Step 2 Verify code in external cause tabular list
Placeholder will be needed for the 5th characters
7th character will identify the episode of care (e.g., initial, subsequent, sequela)
S06.0X1A Concussion, with loss of consciousness of 30 minutes or less, initial encounter
39


Coding Clinic, Fourth Quarter 2016: Page 67
ICD-10-CM New/Revised Codes: Concussion
Codes in subcategory S06.0, Concussion, identifying loss of consciousness greater than 30 minutes (6th character of 2, 3, 4, 5, 6, 7 and 8) have been deleted. The excludes1 note has also been revised as follows:
From concussion with other intracranial injuries classified in category S06- code to specified intracranial injury
To concussion with other intracranial injuries classified in subcategories S06.1- to S06.6- , S06.81- and S06.82- code to specified intracranial injury

Coding Clinic, Fourth Quarter 2016: Page 67
Question:
How should a case documented as concussion with loss of consciousness of 45 minutes be coded? There was no documentation of intracranial injury.
Answer:
Assign code S06.0X9, Concussion with loss of consciousness of unspecified duration, with the appropriate 7th character.
Coding Example #1
Code #2
Diagnosis: Struck by football
Step 1 Go to the external causes, alphabetic index look up the main term and subterm(s)
Struck (accidentally) by; ball; football
Step 2 Verify code in external cause tabular list
Placeholders will be needed for the 6thcharacters.
The 7th character will identify the episode of care (e.g., initial, subsequent, sequela)
W21.01XA Struck by football, initial encounter
43

Coding Example #1
Code #3
Diagnosis: Place of Occurrence Football Field
Step 1 Go to the external causes, alphabetic index look up the main term and subterm(s)
Place of Occurrence; football field
Step 2 Verify code in external cause tabular list
Y92.321 Football field as the place of occurrence of the external cause
45


Coding Example #1
Code #4
Diagnosis: Activity Football
Step 1 Go to the external causes, alphabetic index look up the main term and subterm(s)
Activity; football (American) NOS; tackle
Step 2 Verify code in external cause tabular list
Y93.61 Activity, American tackle football
47


Coding Example #2
A 42-year-old female presented to the Emergency Room after falling from a step ladder while trying to change a light bulb in the kitchen of her single family home. The patient stated she had no loss of consciousness. She did complain of severe neck pain. The physician ordered an x-ray of the cervical spine which revealed a fracture of the second cervical vertebra.
The diagnosis documented by the physician was fracture to cervical vertebra.
How would this scenario be coded?
49

Coding Example #2
Code #1
Diagnosis: Fracture cervical vertebra
Step 1 Go to the alphabetic index and look up the main term and subterm(s)
Fracture, traumatic; vertebra, vertebral; cervical; second –see Fracture, traumatic; neck; cervical vertebra; second; specified type NEC
Step 2 Verify code in external cause tabular list
7th character will identify the episode of care (e.g., initial, subsequent, sequela)
S12.100A Unspecified displaced fracture of second cervical vertebra, initial encounter for closed fracture
50


Fracture of Dens

Coding Example #2
Code#2
Diagnosis: Fall from ladder
Step 1 Go to the External Causes, Alphabetic Index and look up the main term and subterm(s)
Fall, falling; from, off, out of; ladder
Step 2 Verify code in external cause tabular list
Placeholders will be needed for the 4th, 5th and 6thcharacters.
7th character will identify the episode of care (e.g., initial, subsequent, sequela)
W11.XXXA Fall on and from ladder, initial encounter
53


Coding Example #2
Code #3
Diagnosis: Place of Occurrence, kitchen
Step 1 Go to the external causes, alphabetic index and look up the main term and subterm(s)
Place of Occurrence; residence; house, single family; kitchen
Step 2 Verify code in external cause tabular list
Y92.010 Kitchen of single-family (private) house as the place of occurrence of the external cause
55


Coding Example #2
Code#4
Diagnosis: Activity, household maintenance
Step 1 Go to the external causes, alphabetic index and look up the main term and subterm(s)
Activity; maintenance; household NEC
Step 2 Verify code in external cause tabular list
Y93.E9 Activity, other interior property and clothing maintenance
57


Clarification: Use of Activity Codes for Subsequent EncountersCoding Clinic, Third Quarter 2015: Page 40 Question:
One of the examples on the use of the 7th character published in the First Quarter 2015 issue of Coding Clinic page 8 indicated that "the activity code is not assigned again as activity codes are used only at the initial encounter for treatment." We understand that this is consistent with the Official Coding Guideline I.C.20.a.8.c. However, there is also guideline I.C.20.a.2 which states "…assignment of the 7th character for external cause should match the 7th character of the code assigned for the associated injury or condition for the encounter."
Why wasn't the activity code assigned for the example in the First Quarter 2015, such as the patient who presents to the emergency department (ED) after an injury playing lacrosse and then follows up with the local orthopedist for treatment of the fracture? In that example, the patient was still receiving active treatment with the local orthopedist and the 7th character "A, initial encounter" was assigned to the injury code, but the activity code was only assigned for the ED encounter. Does "initial encounter" in the context of the 7th character for injury codes have a different meaning from "initial encounter" as used in the application of the activity codes?
Clarification: Use of Activity Codes for Subsequent Encounters
Answer:
Yes, "initial encounter" has different meanings. The 7th character for initial encounter is assigned while the patient is receiving active treatment for the condition. As shown in the example in question, the 7th character "A" for initial encounter was assigned for the ED visit, as well as for the visit to the orthopedist because the patient was still receiving active treatment during both visits. However, in the context of external cause codes, activity codes can only be used once for the first time the patient is seen for this problem, and it does not need to correlate to the assignment of the 7th character for "initial encounter" in the injury code.

Coding Example #3
A 10-year-old female is seen for continued pain related to her elbow fracture. Six weeks ago, this patient injured her elbow when she fell while skating at the local roller rink. After further evaluation, the attending physician found a nonunion of the previously displaced right distal humerus fracture. She will be scheduled for surgery in the next two days. How would this scenario be coded?
61

Coding Example #3
Code #1
Diagnosis: Fracture humerus, lower end
Step 1 Go to the external causes, alphabetic index and look up the main term and subterm(s)
Fracture, traumatic; humerus; lower end
Step 2 Verify code in external cause tabular list. 6th character will identify the laterality. 7th character will identify the episode of care (e.g., initial, subsequent, sequela)
S42.401K Unspecified fracture of lower end of right humerus, subsequent encounter for fracture with nonunion
62

Coding Example #3
Code #2
Diagnosis: Fall from skates
Step 1 External Causes, Alphabetic Index look up the main term and subterms
Fall, falling; involving; skates – see Accident, transport, pedestrian, conveyance; roller skates; fall
Step 2 Verify code in external cause tabular list7th character will identify the episode of care (e.g., initial, subsequent, sequela)
V00.121D Fall from non-in-line roller-skates, subsequent encounter
63

Gustilo ClassificationICD-10-CM categories S52, Fracture of forearm, S72, Fracture of femur, and S82, Fracture of lower leg, including ankle, have additional seventh character extension (B, C, E, F, H, J, M, N, Q, R) to identify open fractures with the Gustilo classification. The classification is as follows:
Type Description
I Lower energy, wound less then 1 cm
II Wound greater than 1 cm with moderate soft issue damage
III High energy wound greater than 1 cm with extensive soft tissue damage
IIIA Adequate soft tissue cover
IIIB Inadequate soft tissue cover
IIIC Associated with arterial injury
64

Coding Example #4
This 35-year-old female patient was a driver involved in an automobile accident when she was rear-ended by another car on the interstate highway. She was brought into the hospital by the EMTs on a backboard and after proper splinting to the right arm. She was seen in the emergency room complaining of pain in the arm and the neck. Radiological exam indicated a type II compound fracture of the shafts of the right radius and ulna. After CT scan of the head and neck, which was negative for fracture, the patient was removed from the backboard. She was treated for a displaced, type II compound fracture of the shaft of the right radius and ulna. She also received a collar for her cervical strain. How would this scenario be coded?
65

Coding Example #4
Code #1
Diagnosis: Fracture radius shaft, compound
Step 1 Go to the alphabetic index and look up the main term and subterm(s)
Fracture, traumatic; radius; shaft
Step 2 Verify code in tabular list. 6th character will identify the laterality7th character will identify the episode of care and the specific type of fracture(e.g., initial, subsequent, sequela)
S52.301B Unspecified fracture of shaft of right radius, initial encounter for open fracture type I or II
66

Coding Example #4
Code #2
Diagnosis: Fracture ulna shaft, compound
Step 1 Go to the alphabetic index look up the main term and subterm(s) Fracture, traumatic; ulna; shaft
Step 2 Verify code in tabular list.
6th character will identify the laterality7th character will identify the episode of care and the specific type of fracture(e.g., initial, subsequent, sequela)
S52.201B Unspecified fracture of shaft of right ulna, initial encounter for open fracture type I or II
68


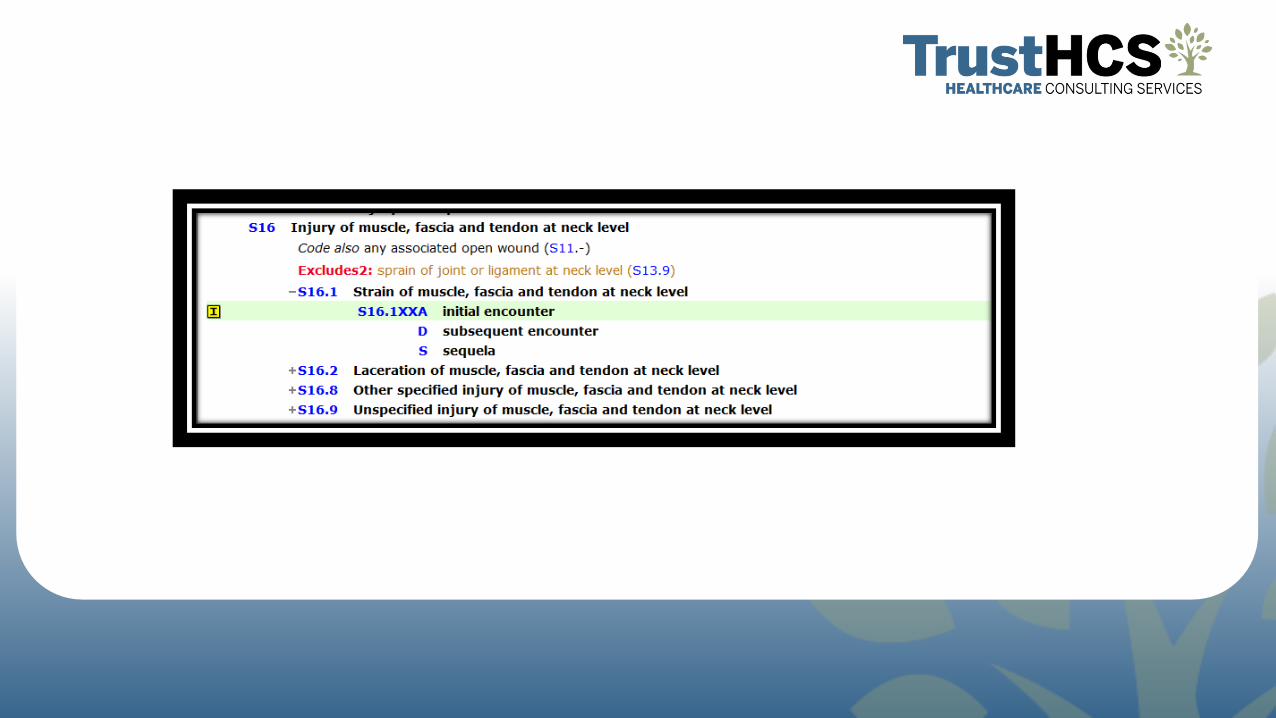
Coding Example #4Code #3
Diagnosis: Cervical strain
Step 1 Go to the alphabetic index and look up the main term and subterm(s)
Strain; cervical
Step 2 Verify code in tabular list.
Placeholders will be needed for the 5th and 6th characters. 7th character will identify the episode of care (e.g., initial, subsequent, sequela)
S16.1XXA Strain of muscle, fascia and tendon at neck level, initial encounter
70
Coding Example #4
Code #4
Diagnosis: MVA, driver
Step 1 Go to the external causes, alphabetic index and look up the main term and subterm(s)
Accident; transport; car occupant; driver; collision; car
Step 2 Verify code in external cause tabular list
Placeholders will be needed for the 5th and 6th characters.
7th character will identify the episode of care (e.g., initial, subsequent, sequela)
V43.52XA Car driver injured in collision with other type car in traffic accident, initial encounter
72

Coding Example #4Code #5
Diagnosis: Place of Occurrence, highway
Step 1 Go to the external causes, alphabetic index and look up the main term and subterm(s)
Place of Occurrence; highway
Step 2 Verify code in external cause tabular list
Y92.411 Interstate highway as the place of occurrence of the external cause
74


ICD-10-PCS

Example – 0QSC04ZReduction of a displaced fracture
What body part/bone, approach, and device?
77

Thank YouFor Your Time and Attention!
References
• Detailed Instructions for Appropriate ICD-10-CM Coding. (2016). West Valley City, UT: OptumInsight.
• Frazier, M. S., & Drzymkowski, J. W. (2008). Essential of Human Disease and Conditions. St. Louis, MO: Elsevier.
• Leon-Chisen, N. (2017). ICD-10-CM and ICD-10-PCS Coding Handbook.Chicago, IL: AHA Press.
• Porter, R. S., & Kaplan, J. L. (2016). The Merck Manual of Diagnosis and Therapy. New Jersey: Merck.
79






![Practical Use of Emergency Tourniquets to Stop Bleeding in ... · limb involved (right or left limb, upper or lower extremity, limb regions [forearm, arm, leg, thigh]), patient nationality](https://static.fdocuments.in/doc/165x107/5ee0c803ad6a402d666be44b/practical-use-of-emergency-tourniquets-to-stop-bleeding-in-limb-involved-right.jpg)