Atypical vascular lesion of the breast - VGR-Dvgrd.org/archive/cases/2010/avl/Atyical vascular...
4
CASE REPORT Atypical vascular lesion of the breast Joshua Mandrell, MD, Sheetal Mehta, MD, and Stacy McClure, MD Maywood, Illinois Atypical vascular lesions (AVLs) are vascular proliferations that develop after surgery and radiation for breast carcinoma and may represent precursors to angiosarcoma. AVLs are not well-known entities and currently lack official prognostic factors and guidelines for surgical treatment. We report the case of a patient who developed an AVL, vascular type, 4 years after lumpectomy and radiation therapy for ductal carcinoma in situ of the breast. The patient underwent wide local excision with 1-cm margins with subsequent pathologic examination confirming complete excision of the residual atypical vascular proliferation. This case highlights the importance of close cutaneous surveillance in patients with a history of surgery and radiation for breast carcinoma, and a low threshold for biopsy. More studies are needed to further delineate the risk of AVLs progressing to angiosarcoma and to identify histologic features or immunophenotypic markers, which may be predictive of this risk. Furthermore, formal treatment recommendations for these enigmatic entities would be helpful. ( J Am Acad Dermatol 2010;63:337-40.) Key words: angiosarcoma; atypical vascular lesion; dermatologic surgery; vascular neoplasms; pathology. A typical vascular lesions (AVLs) develop as one or more small erythematous to viola- ceous macules or papules after radiation therapy for breast carcinoma. 1 Although the specific type, technique, and dosage of prior radiation has not been specifically analyzed, all AVLs are observed within the radiation field. The latency period for development of these lesions ranges from 1 to 20 years after radiation, although presentation within 3 to 6 years is most common. 1,2 The effects of radiation therapy are typically divided into acute or early changes that occur within days to weeks and delayed or late changes that occur within months to years. Early radiation-induced changes occur secondary to necrosis of the rapidly dividing keratinocytes. 3 Dilation of capillaries and increased vascular perme- ability leads to erythema. 3 Decreased activity in hair follicles and sweat glands can lead to hair loss and xerosis, respectively. 3 By 3 to 4 weeks, warmth, tenderness, and edema can occur in addition to erythema. 3 Thrombosis of vessels, hemorrhage, des- quamation, exudation, hyperpigmentation, and ulceration can also occur. 3 Typical late radiation- induced changes seen within the skin include hya- linization of dermal collagen fibers, swelling of endothelial cells, telangiectatic dilation of dermal vessels, and proliferation and hyalinization of deeper vessels. 4,5 Because such skin changes usually stop within 3 years of radiation therapy, observed changes after this period should alert the clinician. 5,6 We report the case of a patient who developed an AVL and suggest that more guidelines would be beneficial to help clinicians treat these patients. CASE REPORT A 63-year-old woman with a medical history of hypertension, hypercholesterolemia, and estrogen receptor-positive, ductal carcinoma in situ of the right breast presented to the dermatology clinic for evaluation of an asymptomatic, unchanging macule of the right breast that had been present for 6 months. The patient had a history of right breast lumpectomy with axillary node dissection and adju- vant chemotherapy and radiation (32 treatments of external beam radiation therapy for a total of 5000 cGy) 4 years before presentation. She was currently taking the estrogen antagonist anastrozole. Physical examination revealed a 6-mm violaceous macule Abbreviations used: AVL: atypical vascular lesion LT: lymphatic type VT: vascular type From the Loyola University Medical Center. Funding sources: None. Conflicts of interest: None declared. Reprints not available from the authors. Correspondence to: Joshua Mandrell, MD, Department of Dermatology, Loyola University Medical Center, Bldg 54, Room 101, 2160 S First Ave, Maywood, IL 60153. E-mail: [email protected]. Published online February 8, 2010. 0190-9622/$36.00 ª 2010 by the American Academy of Dermatology, Inc. doi:10.1016/j.jaad.2009.08.017 337
Transcript of Atypical vascular lesion of the breast - VGR-Dvgrd.org/archive/cases/2010/avl/Atyical vascular...

CASE REPORT
Atypical vascular lesion of the breast
Joshua Mandrell, MD, Sheetal Mehta, MD, and Stacy McClure, MD
Maywood, Illinois
From
Fund
Conf
Repr
Corre
D
Ro
jm
Publ
0190
ª 20
doi:1
Atypical vascular lesions (AVLs) are vascular proliferations that develop after surgery and radiation for breastcarcinoma and may represent precursors to angiosarcoma. AVLs are not well-known entities and currently lackofficial prognostic factors and guidelines for surgical treatment. We report the case of a patient who developedan AVL, vascular type, 4 years after lumpectomy and radiation therapy for ductal carcinoma in situ of the breast.The patient underwent wide local excision with 1-cm margins with subsequent pathologic examinationconfirming complete excision of the residual atypical vascular proliferation. This case highlights theimportance of close cutaneous surveillance in patients with a history of surgery and radiation for breastcarcinoma, and a low threshold for biopsy. More studies are needed to further delineate the risk of AVLsprogressing to angiosarcoma and to identify histologic features or immunophenotypic markers, which may bepredictive of this risk. Furthermore, formal treatment recommendations for these enigmatic entities would behelpful. ( J Am Acad Dermatol 2010;63:337-40.)
Key words: angiosarcoma; atypical vascular lesion; dermatologic surgery; vascular neoplasms; pathology.
Abbreviations used:
AVL: atypical vascular lesionLT: lymphatic typeVT: vascular type
Atypical vascular lesions (AVLs) develop asone or more small erythematous to viola-ceous macules or papules after radiation
therapy for breast carcinoma.1 Although the specifictype, technique, and dosage of prior radiation hasnot been specifically analyzed, all AVLs are observedwithin the radiation field. The latency period fordevelopment of these lesions ranges from 1 to 20years after radiation, although presentation within 3to 6 years is most common.1,2 The effects of radiationtherapy are typically divided into acute or earlychanges that occur within days to weeks and delayedor late changes that occur within months to years.Early radiation-induced changes occur secondary tonecrosis of the rapidly dividing keratinocytes.3
Dilation of capillaries and increased vascular perme-ability leads to erythema.3 Decreased activity in hairfollicles and sweat glands can lead to hair loss andxerosis, respectively.3 By 3 to 4 weeks, warmth,tenderness, and edema can occur in addition toerythema.3 Thrombosis of vessels, hemorrhage, des-quamation, exudation, hyperpigmentation, and
the Loyola University Medical Center.
ing sources: None.
licts of interest: None declared.
ints not available from the authors.
spondence to: Joshua Mandrell, MD, Department of
ermatology, Loyola University Medical Center, Bldg 54,
om 101, 2160 S First Ave, Maywood, IL 60153. E-mail:
ished online February 8, 2010.
-9622/$36.00
10 by the American Academy of Dermatology, Inc.
0.1016/j.jaad.2009.08.017
ulceration can also occur.3 Typical late radiation-induced changes seen within the skin include hya-linization of dermal collagen fibers, swelling ofendothelial cells, telangiectatic dilation of dermalvessels, and proliferation and hyalinization of deepervessels.4,5 Because such skin changes usually stopwithin 3 years of radiation therapy, observedchanges after this period should alert the clinician.5,6
We report the case of a patient who developed anAVL and suggest that more guidelines would bebeneficial to help clinicians treat these patients.
CASE REPORTA 63-year-old woman with a medical history of
hypertension, hypercholesterolemia, and estrogenreceptor-positive, ductal carcinoma in situ of theright breast presented to the dermatology clinic forevaluation of an asymptomatic, unchanging maculeof the right breast that had been present for 6months. The patient had a history of right breastlumpectomy with axillary node dissection and adju-vant chemotherapy and radiation (32 treatments ofexternal beam radiation therapy for a total of 5000cGy) 4 years before presentation. She was currentlytaking the estrogen antagonist anastrozole. Physicalexamination revealed a 6-mm violaceous macule
337

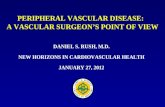
Fig 1. Low magnification (A) and high magnification(B) of a 6-mm violaceous macule of right breast.
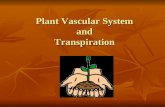
Fig 2. Low- (A) and high- (B) power image of hematox-ylin-eosin stain of atypical vascular lesion, vascular type.
J AM ACAD DERMATOL
AUGUST 2010
338 Case report
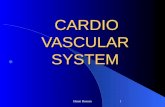
(Fig 1). A punch biopsy specimen revealed diffusedermal proliferation of well-formed capillary struc-tures with mild endothelial atypia (Fig 2). Stainingwas positive for the CD34 vascular marker andnegative for the D2-40 lymphatic marker (Fig 3). Adiagnosis of AVL, vascular type (VT), was made,consistent with the histologic appearance and thehistory of radiation. The patient underwent widelocal excision with 1-cm margins, with pathologicexamination confirming complete excision of theresidual atypical vascular proliferation.
REVIEWPatients who undergo conservative surgery and
radiation therapy for breast cancer have been ob-served to have various complications including pneu-monitis, arm edema, persistent breast or chest wallpain, breast fibrosis, fat necrosis, prolonged skinbreakdown, rib fracture, cardiac complications, neu-ropathy, vascular thrombosis, and vascular neo-plasms, including angiosarcoma and AVLs.7 The term‘‘atypical vascular lesion’’ was coined in 1994 byFineberg and Rosen,8 who described 4 women withcutaneous vascular proliferations after lumpectomyand radiation for breast carcinoma.1 They believedthese lesions to be benign and related to lymphaticobstruction after surgery and/or radiation-induceddilation of vascular channels.1,5 Others have used theterms ‘‘atypical hemangiomas,’’9 ‘‘acquired progress-ive lymphangioma,’’10 ‘‘benign lymphangiomatous
papules,’’11-13 ‘‘lymphangioma circumscriptum,’’14
and ‘‘benign lymphangioendothelioma’’8,14,15 todescribe the presumptive benign nature of the sameentity.
However, in their review of 42 cases, Brenn andFletcher14 concluded that AVLs were part of a con-tinuum and were in fact precursors to angiosarcomasthat warranted more aggressive treatment.1 Thisopinion was based primarily on a patient with aclassic AVL in whom serial biopsy specimens showedslow development of angiosarcoma during the next5 years.1,14 Other cases of malignant transformationto angiosarcomas are also reported in the litera-ture.14,16,17 However, despite such contradictory re-ports, the predominant consensus in the literatureremained that AVLs represented a benign entity.1
The natural course and malignant potential ofAVLs was once again called into question by a 2008report by Patton et al1 who reviewed 32 cases of AVLsafter surgery and radiation of the breast. The authorsdivided these into two histologic types: the lesscommon vascular type (VT) was observed to havea higher risk of development into angiosarcoma,

Fig 3. A, CD34 staining (vascular marker) is positive. B,D2-40 (lymphatic marker) is negative.
J AM ACAD DERMATOL
VOLUME 63, NUMBER 2
Case report 339
whereas the more common lymphatic type (LT) hada lower risk.1 VT lesions were characterized byirregular dispersed, pericyte-invested, capillary-sized vessels within the papillary or reticular dermis,which were often associated with extravasated eryth-rocytes or hemosiderin.1 These lesions resembledcapillary hemangiomas, with vessels displaying avascular immunophenotype (CD311, CD341, andD2-40e) although lacking a lobular organization.1
Although 4 of the 10 VT lesions showed endothelialatypia, they differed from angiosarcomas in that thevessels did not intercommunicate and did not displayendothelial multilayering.1 The lymphatic subtypeAVLs displayed thin-walled, variably anastomosinglymphatic vessels lined by attenuated or slightlyprotuberant endothelial cells.1 These vessels dis-played a lymphatic immunophenotype (CD311,D2-401, and CD341/e).1 Most of the original de-scriptions of AVLs seem to describe this LT entity witha discontinuous endothelial lining, absence of per-icytes, and smooth muscle actin and Ki67 negativ-ity.1,12,14,18 Of note, 6 of the VT AVLs displayed someoverlap with LT histology.1
In the clinicopathologic study by Patton et al,1
patients underwent biopsy alone, simple excision, oraggressive surgical therapy depending on physicianand patient preference. Therefore, knowledge of thetrue biological course of these lesions is still some-what limited. Of the 21 patients with LTAVLs who hadfollow-up, 5 patients developed local recurrences,and one developed several additional lymphaticAVLs and eventually a multifocal angiosarcoma.1 Ofthe 8 patients with VT AVLs who had follow-up, onehad local recurrences of VT AVLs and another devel-oped high-grade epithelioid angiosarcoma.1 Theauthors concluded that VT AVLs have the highestrisk for angiosarcoma transformation based on thedegree of endothelial atypia.1 This opinion seems tobe congruent with the observation of recurrencesand fatalities in patients with vascular lesions of thebreast with a capillary lobular pattern but withmoderately atypical endothelium reported as ‘‘post-irradiation angiosarcomas.’’1,19 Although the riskmay be smaller, it should be remembered that LTAVLs with unusual histologic features also have a riskof malignant transformation.1 It remains to be seenwhether LTAVLs are precursors to VTAVLs as part of acontinuum to angiosarcoma, or instead distinct enti-ties with their own inherent risk.1
In a study by the French Sarcoma Group, 20% ofpatients with AVLs experienced recurrence, afterbiopsy or excision with varying margins.2 The au-thors conceded that these new vascular lesions maynot represent true recurrences but rather new lesionswithin the same irradiated field or ‘‘field-effect
phenomenon.’’2 Other studies have observed thatup to 31% of patients develop further lesions withinthe radiation field.2,5,14,18 However, it should benoted that despite the more than 100 diagnosedcases of AVLs reported in the literature, no more than5 have progressed to angiosarcoma.1,2
Histologically, AVLs do display specific featuresthat separate them from the typical angiosarcoma.Fineberg and Rosen8 used these histologic findings todifferentiate AVLs from low-grade angiosarcoma. Incontrast to angiosarcoma, AVLs typically lack infiltra-tion into the subcutis, multilayering of endothelialcells, prominentnucleoli,mitoses, andhemorrhage.5,8
Others have observed that AVLs histologically displaydilated vascular spaces within the papillary dermiswith plump endothelial cells, differentiated from an-giosarcomaby lackof destructionof adnexa, localizedgrowth, and little penetration into reticular dermis orsubcutaneous tissue.5,8,11,12,14,18,20,21 Although angio-sarcomas usually lack chronic inflammation, circum-scription, and stromal projections into the lumen,these features are commonly seen in AVLs.5,8
Dissection of dermal collagen can be present in both

J AM ACAD DERMATOL
AUGUST 2010
340 Case report
entities.5,8,22,23 However, the clinical and histologicoverlap causes the diagnosis to remain challeng-ing.14,18,21,24 In fact, in a series of 11 patients withAVLs on biopsy specimen, 5 were reclassified asangiosarcoma after complete excision.5,21
AVLs remain challenging and enigmatic entities interms of diagnosis, natural history, and appropriatetherapy. Histologic features or immunophenotypicmarkers that could more specifically predict whichAVLs will develop into angiosarcoma would bevaluable. More research and controlled studies withcareful long-term follow-up are needed to furtherdelineate this risk. In addition, guidelines for treat-ment including recommendations regarding surgicalmargins would be beneficial, as current treatmentshave ranged from wide local excision with 1-cmmargins to mastectomy. In patients with breast can-cer and a history of surgery and radiation therapy,close monitoring of the skin for new vascular erup-tions, including macular lesions resembling a bruise(as in our patient), and a low threshold for biopsyshould be emphasized.
The authors would like to thank Drs Madhu Dahiyaand Eva Drinka for providing the histopathology images.
REFERENCES
1. Patton KT, Deyrup AT, Weiss SW. Atypical vascular lesions after
surgery and radiation of the breast: a clinicopathologic study
of 32 cases analyzing histologic heterogeneity and association
with angiosarcoma. Am J Surg Pathol 2008;32:943-50.
2. Gengler C, Coindre JM, Leroux A, Trassard M, Ranchere-Vince D,
Valo I, et al. Vascular proliferations of the skin after radiation
therapy for breast cancer: clinicopathologic analysis of a series
in favor of a benign process; a study from the French sarcoma
group. Cancer 2007;109:1584-98.
3. Mendelsohn FA, Divino CM, Reis ED, Kerstein MD. Wound care
after radiation therapy. Adv Skin Wound Care 2002;15:216,
218-24.
4. Weedon D. Skin pathology. 2nd ed. Edinburgh: Churchill
Livingstone; 2002.
5. Brodie C, Provenzano E. Vascular proliferations of the breast.
Histopathology 2008;52:30-44.
6. West JG, Qureshi A, West JE, Chacon M, Sutherland ML, Haghighi B,
et al. Risk of angiosarcoma following breast conservation: a clinical
alert. Breast J 2005;11:115-23.
7. Meric F, Buchholz TA, Mirza NQ, Vlastos G, Ames FC, Ross MI,
et al. Long-term complications associated with breast-con-
servation surgery and radiotherapy. Ann Surg Oncol 2002;9:
543-9.
8. Fineberg S, Rosen PP. Cutaneous angiosarcoma and atypical
vascular lesions of the skin and breast after radiation therapy
for breast carcinoma. Am J Clin Pathol 1994;102:757-63.
9. Hoda SA, Cranor ML, Rosen PP. Hemangiomas of the breast
with atypical histological features: further analysis of histolog-
ical subtypes confirming their benign character. Am J Surg
Pathol 1992;16:553-60.
10. Rosso R, Gianelli U, Carnevali L. Acquired progressive lym-
phangioma of the skin following radiotherapy for breast
carcinoma. J Cutan Pathol 1995;22:164-7.
11. Wagamon K, Ranchoff RE, Rosenberg AS, Jaworsky C. Benign
lymphangiomatous papules of the skin. J Am Acad Dermatol
2005;52:912-3.
12. Diaz-Cascajo C, Borghi S, Weyers W, Retzlaff H, Requena L,
Metze D. Benign lymphangiomatous papules of the skin
following radiotherapy: a report of five new cases and review
of the literature. Histopathology 1999;35:319-27.
13. Martın-Gonzalez T, Sanz-Trelles A, Del Boz J, Samaniego E.
Benign lymphangiomatous papules and plaques after radio-
therapy. Actas Dermosifiliogr 2008;99:84-6.
14. Brenn T, Fletcher CD. Radiation-associated cutaneous atypical
vascular lesions and angiosarcoma: clinicopathologic analysis
of 42 cases. Am J Surg Pathol 2005;29:983-96.
15. Guillou L, Fletcher CD. Benign lymphangioendothelioma
(acquired progressive lymphangioma): a lesion not to be
confused with well-differentiated angiosarcoma and patch
stage Kaposi’s sarcoma: clinicopathologic analysis of a series.
Am J Surg Pathol 2000;24:1047-57.
16. Hildebrandt G, Mittag M, Gutz U, Kunze ML, Haustein UF.
Cutaneous breast angiosarcoma after conservative treatment
of breast cancer. Eur J Dermatol 2001;11:580-3.
17. Di Tommaso L, Fabbri A. Cutaneous angiosarcoma arising
after radiotherapy treatment of a breast carcinoma: descrip-
tion of a case and review of the literature. Pathologica 2003;
95:196-202.
18. Requena L, Kutzner H, Mentzel T, Duran R, Rodrıguez-Peralto
JL. Benign vascular proliferations in irradiated skin. Am J Surg
Pathol 2002;26:328-37.
19. Di Tommaso L, Rosai J. The capillary lobule: a deceptively
benign feature of post-irradiation angiosarcoma of the skin:
report of three cases. Am J Dermatopathol 2005;27:301-5.
20. Bodet D, Rodriguez-Cano L, Bartralot R, Mollet J, Medina A,
Heras C, et al. Benign lymphangiomatous papules of the skin
associated with ovarian fibroma. J Am Acad Dermatol 2007;
56(Suppl):S41-4.
21. Mattoch IW, Robbins JB, Kempson RL, Kohler S. Post-radio-
therapy vascular proliferations in mammary skin: a clinico-
pathologic study of 11 cases. J Am Acad Dermatol 2007;57:
126-33.
22. Grunwald MH, Amichai B, Avinoach I. Acquired progressive
lymphangioma. J Am Acad Dermatol 1997;37:656-7.
23. Kim HS, Kim JW, Yu DS. Acquired progressive lymphangioma.
J Eur Acad Dermatol Venereol 2007;21:416-7.
24. Brenn T, Fletcher CD. Postradiation vascular proliferations: an
increasing problem. Histopathology 2006;48:106-14.