Attenuated form of Lysosomal Storage Disease in a Medieval ... · Kircher SG (2017) Attenuated form...
6
Central Bringing Excellence in Open Access JSM Biochemistry & Molecular Biology Cite this article: Kircher SG (2017) Attenuated form of Lysosomal Storage Disease in a Medieval Skeleton from Austria. JSM Biochem Mol Biol 4(2): 1025. *Corresponding author Susanne Gerit Kircher, Center of Pathobiochemistry and Genetics, Medical University of Vienna, Institute of Medical Chemistry and Institute of Medical Genetics, Waehringerstrasse 10, A-1090 Vienna, Austria, Tel: 43-1- 40160-56512 or -38077; Fax: 43-1-40160-956531; Email: Submitted: 16 April 2017 Accepted: 24 May 2017 Published: 26 May 2017 ISSN: 2333-7109 Copyright © 2017 Kircher OPEN ACCESS Keywords • Medieval skeleton • Dysostosis multiplex • Lysosomal storage diseases • Mucopolysaccharidosis • Mucolipidosis • Glycoproteinosis • Harris lines Short Communication Attenuated form of Lysosomal Storage Disease in a Medieval Skeleton from Austria Susanne Gerit Kircher* Center of Pathobiochemistry and Genetics, Medical University of Vienna, Austria Abstract Introduction: Forty years ago, a medieval skeleton from the 9 th century was found near Pitten, Austria. The skeleton´s burial position at the edge of the cemetery, the presence of multiple skeletal changes typical of mucopolysaccharidosis and its similarity to a painting by Virchow R 200 years ago have previously been interpreted to indicate Pfaundler-Hurler disease, the early name for mucopolysaccharidosis type I. Materials and methods: These previous findings were re-evaluated and compared with those for another medieval male skull without lysosomal storage disease but with syphilitic changes. Of special interest was the shape of the skull and face, as well as the typical bony lesions observed in dysostosis multiplex. X-rays of the tibial bones revealed the so-called Harris lines similar to those observed in Morquio syndrome in early reports by Morquio L. Results: Many parts of the skeleton showed signs consistent with dysostosis multiplex: mid-face hypoplasia with a broad nasal bridge, prominent jaw, osteosclerosis of the skull with scaphoid form, elongated sella turcica, signs of premature synostosis of the coronary suture, kyphoscoliosis, platyspondyly with ovoid-like vertebrae and more severe changes in the thoraco-lumbar region, broad iliac wings, severe joint changes in the hypoplastic acetabulae and markedly flat heads of the femoral bones in the varus-position, and shortening of the long bones, thus resulting in a moderate, short stature. Discussion: On the basis of the individual´s age and current knowledge of lysosomal storage diseases, this young man most probably had an attenuated form of one disease of this group of disorders. The burial of a disabled individual may indicate intellectual disability, as well as severe deficit in vision, hearing or immobility, which are observed in untreated adult patients with mucopolysaccharidoses or several other lysosomal storage disorders. ABBREVIATIONS LSD: Lysosomal Storage Disease; MPS: Mucopolysaccharidosis; ML: Mucolipidosis; T: Thoracic Vertebra, L: Lumbar Vertebra INTRODUCTION Between 1970 and 1973, in the southern region of Lower Austria in Pitten, near Neunkirchen, a medieval graveyard from the 9 th century was found. One of the discovered skeletons (tomb number 126a) was of interest for further investigations [1]. First, its position at the extreme south-eastern edge of the cemetery indicated that the individual had a disease with mental retardation, because such persons were buried without any church consecrations until the 20 th century. The second reason for further investigations of this skeleton, which had been examined by X-rays and histological analysis of the epiphyses and growth plates 40 years ago, was the multiple skeletal findings interpreted as a heritable skeletal disease, including multiple changes involving all parts of the skeleton. The diagnosis was thought to be mucopolysaccharidosis type I, previously described as Pfaundler-Hurler disease. The skeleton was initially classified as a female but was ultimately identified as belonging to a young man between 20 to 30 years of age. The body length was calculated to be 157 cm, which was less than the typical mean body length of adult men in the early medieval time (165.1 – 179.1 cm) [1,2]. Increased knowledge of the skeletal findings recognized as dysostosis multiplex , as well as clinical understanding of patients with attenuated disease courses of lysosomal storage diseases (LSDs), prompted re-evaluation of the initial findings and revision on the basis of clinical experience and scientific knowledge. MATERIALS AND METHODS The bones preserved included: the skull, 2 scapulae, the sternum, both clavicles, the complete spine (7 cervical, 12 thoracic and 5 lumbar vertebrae), 12 pairs of ribs, the pelvis and os sacrum, the right and left humeri, the right ulna and
Transcript of Attenuated form of Lysosomal Storage Disease in a Medieval ... · Kircher SG (2017) Attenuated form...

CentralBringing Excellence in Open Access
JSM Biochemistry & Molecular Biology
Cite this article: Kircher SG (2017) Attenuated form of Lysosomal Storage Disease in a Medieval Skeleton from Austria. JSM Biochem Mol Biol 4(2): 1025.
*Corresponding author
Susanne Gerit Kircher, Center of Pathobiochemistry and Genetics, Medical University of Vienna, Institute of Medical Chemistry and Institute of Medical Genetics, Waehringerstrasse 10, A-1090 Vienna, Austria, Tel: 43-1-40160-56512 or -38077; Fax: 43-1-40160-956531; Email:
Submitted: 16 April 2017
Accepted: 24 May 2017
Published: 26 May 2017
ISSN: 2333-7109
Copyright© 2017 Kircher
OPEN ACCESS
Keywords•Medieval skeleton•Dysostosis multiplex•Lysosomal storage diseases•Mucopolysaccharidosis•Mucolipidosis•Glycoproteinosis•Harris lines
Short Communication
Attenuated form of Lysosomal Storage Disease in a Medieval Skeleton from AustriaSusanne Gerit Kircher*Center of Pathobiochemistry and Genetics, Medical University of Vienna, Austria
Abstract
Introduction: Forty years ago, a medieval skeleton from the 9th century was found near Pitten, Austria. The skeleton´s burial position at the edge of the cemetery, the presence of multiple skeletal changes typical of mucopolysaccharidosis and its similarity to a painting by Virchow R 200 years ago have previously been interpreted to indicate Pfaundler-Hurler disease, the early name for mucopolysaccharidosis type I.
Materials and methods: These previous findings were re-evaluated and compared with those for another medieval male skull without lysosomal storage disease but with syphilitic changes. Of special interest was the shape of the skull and face, as well as the typical bony lesions observed in dysostosis multiplex. X-rays of the tibial bones revealed the so-called Harris lines similar to those observed in Morquio syndrome in early reports by Morquio L.
Results: Many parts of the skeleton showed signs consistent with dysostosis multiplex: mid-face hypoplasia with a broad nasal bridge, prominent jaw, osteosclerosis of the skull with scaphoid form, elongated sella turcica, signs of premature synostosis of the coronary suture, kyphoscoliosis, platyspondyly with ovoid-like vertebrae and more severe changes in the thoraco-lumbar region, broad iliac wings, severe joint changes in the hypoplastic acetabulae and markedly flat heads of the femoral bones in the varus-position, and shortening of the long bones, thus resulting in a moderate, short stature.
Discussion: On the basis of the individual´s age and current knowledge of lysosomal storage diseases, this young man most probably had an attenuated form of one disease of this group of disorders. The burial of a disabled individual may indicate intellectual disability, as well as severe deficit in vision, hearing or immobility, which are observed in untreated adult patients with mucopolysaccharidoses or several other lysosomal storage disorders.
ABBREVIATIONSLSD: Lysosomal Storage Disease; MPS: Mucopolysaccharidosis;
ML: Mucolipidosis; T: Thoracic Vertebra, L: Lumbar Vertebra
INTRODUCTIONBetween 1970 and 1973, in the southern region of Lower
Austria in Pitten, near Neunkirchen, a medieval graveyard from the 9th century was found. One of the discovered skeletons (tomb number 126a) was of interest for further investigations [1]. First, its position at the extreme south-eastern edge of the cemetery indicated that the individual had a disease with mental retardation, because such persons were buried without any church consecrations until the 20th century. The second reason for further investigations of this skeleton, which had been examined by X-rays and histological analysis of the epiphyses and growth plates 40 years ago, was the multiple skeletal findings interpreted as a heritable skeletal disease, including multiple changes involving all parts of the skeleton.
The diagnosis was thought to be mucopolysaccharidosis type I, previously described as Pfaundler-Hurler disease. The skeleton was initially classified as a female but was ultimately identified as belonging to a young man between 20 to 30 years of age. The body length was calculated to be 157 cm, which was less than the typical mean body length of adult men in the early medieval time (165.1 – 179.1 cm) [1,2]. Increased knowledge of the skeletal findings recognized as dysostosis multiplex , as well as clinical understanding of patients with attenuated disease courses of lysosomal storage diseases (LSDs), prompted re-evaluation of the initial findings and revision on the basis of clinical experience and scientific knowledge.
MATERIALS AND METHODSThe bones preserved included: the skull, 2 scapulae, the
sternum, both clavicles, the complete spine (7 cervical, 12 thoracic and 5 lumbar vertebrae), 12 pairs of ribs, the pelvis and os sacrum, the right and left humeri, the right ulna and

CentralBringing Excellence in Open Access
Kircher (2017)Email:
JSM Biochem Mol Biol 4(2): 1025 (2017) 2/6
radius, both femora and patellae, and both tibiae and fibulae [1]. Unfortunately, neither the hand nor the foot bones could be found. For the assessment and categorization of the skeletal changes, the calculations, measurements, angles and indices used were based on previous studies investigating medieval graves in Central Europe [1,3,4]. Further investigations using electron microscopy and histology were performed in a subsequent report to elucidate any bony-cartilaginous pathology of the epiphyses [5].
In this report, descriptions of the pathologic bone morphology were revised and compared with the typical skeletal changes known as dysostosis multiplex observed in a group of lysosomal storage diseases, such as mucopolysaccharidoses (MPS), mucolipidoses (ML) and glycoproteinoses, e.g. alpha-mannosidosis or GM1-gangliosidosis. The bone morphology, X-rays and comparisons with other ancient or medieval skeletons with diseases associated with inflammation, life-style, trauma, tumors or other genetic diseases from prior literature research confirmed the observations from the skeleton to be consistent with multi-systemic characteristics of dysostosis multiplex . In the context of knowledge of attenuated disease courses in LSDs, the possible diagnosis may be MPS, ML or a glycoproteinosis.
To highlight the specific changes in the skull, the forms and shapes, especially those of the facial bones, were compared with those of another skull of a man aged 40 – 50 years and found in another grave yard in Lower Austria (Falkenstein), which has been dated to the 16th – 18th century [6]. Skull morphology and cranial indices may change over centuries and do not allow for an unbiased comparison with findings in patients from recent times [7].
RESULTSAs described by Szilvássy and Kritscher in 1983, the
skull of the young adult man was relatively heavy, owing to excessive bone density (weight 754 grams), with accentuated parietal bones. Via X-rays, a thickening of the skull bones and a flattened elongated sella turcica (‘shoe-shapedʼ sella) was observed [1]. The head circumference was 53.2 cm, which was relatively enlarged as compared with the body length. The facial skeleton was relatively small compared with the cranial bones but relatively broad with deeply sunken nasal bones thus suggesting mid-face hypoplasia with a broad nose. There was some frontal bossing as compared with the facial shape of the other male skeleton, as well as a prominent maxillary bone and an even more prominent mandibular bone (Figure 1A and B). This characteristic profile reminded Kritscher and coauthors of a face illustrated by Virchow 200 years ago (Figure 2) [7]. Virchow diagnosed this female patient with cretinism, but in the author´s view, the patient showed a high degree of similarity to a patient with Pfaundler-Hurler disease, the previous name for mucopolysaccharidosis type I [1]. The relatively enlarged head (macrocephaly), thickened cortical bone/calvarium, J-shaped sella turcica and facial anomalies with a broad flat nasal bridge, and obtuse mandibular angle with prognatism are typical radiological findings in dysostosis multiplex and have been observed in several LSDs, in virtually all patients with all types of MPS and ML and also alpha-mannosidosis or GM1-gangliosidosis [9-11]. In a study of 78 patients with attenuated Scheie forms of
MPS I, 84-87% of the bone deformities, such as kyphosis, gibbus, scoliosis and hip dysplasias, were found to be consistent with dysostosis multiplex [12]. In another study, dysostosis multiplex was identified in 90% of patients with alpha-mannosidosis and in all patients with the adult form of GM1-gangliosidosis with increasing age [13,14].
The vertebral bodies were highly flattened, with a porous-like structure and ovoid-shape in the thoracic spine and with wedge-shaped vertebrae from L1-L3, thus resulting in a kyphoscoliotic bending [1,5]. These changes, especially in the region of the thoracolumbar spine (T12), are also characteristic of dysostosis multiplex , thus leading to the thoracolumbar kyphosis observed in MPS patients (Figure 3A and B) [10,11,15]. There is no precise description of the odontoid process of the second vertebra, which is mainly hypoplastic or aplastic in MPS IV (Morquio disease) as well as in others MPS types. The os sacrum in the medieval skeleton revealed signs of spina bifida which might be an additional finding and not related to the genetic skeletal dysplasia.
The iliac wings are broad, and all pelvic bones have an abnormal shape with flat acetabulae presenting many irregularities in the joint surfaces [1,5]. Both femoral heads showed strong flattening with a spongy appearance, which was interpreted as epiphyseal dysplasia and coxa vara positioning. Although bilateral flattening of the epiphyses of both femoral heads is a constant finding in dysostosis multiplex, several MPS-patients with MPS IVA have normal ilia but poor formation of the acetabular roofs [15].
In general, the long bones of the Austrian male medieval skeleton appeared to be shortened with several open epiphyseal
A)
B)
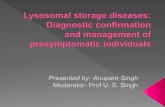
Figure 1 (A) Lateral view of a young adult male skull from the early Medieval Ages highly suspected to have LSD/MPS. There is mid-face hypoplasia combined with frontal bossing and a prominent maxilla and even more prominent mandibular bone. Tooth irregularities include relatively large teeth. A relatively small frontal bone with a scaphoid-like form of the skull and prominent temporal bones are observed as in premature craniosynostosis. - (B) Skull of an adult male with syphilitic lesions aged from the late Medieval Ages. The shape of the face is different, with high and rounded frontal bones. There are no signs of mid-face hypoplasia.

CentralBringing Excellence in Open Access
Kircher (2017)Email:
JSM Biochem Mol Biol 4(2): 1025 (2017) 3/6
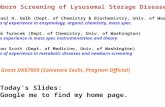
Figure 2 Early drawing by Rudolf Virchow: Kretin aus Unterfranken. The ʼgestaltʼ is reminiscent of a patient with Pfaundler-Hurler-disease (mucopolysaccharidosis type 1).
A) B)
Figure 3 (A): Vertebral spine with platyspondyly and irregular curvature (kyphoscoliosis). There are more severe changes in the thoracolumbar region as often observed in patients with dysostosis multiplex. – (B) Lateral view of the severely abnormal vertebral bone T12, with an irregular wedge-like anterior part and porous bone structure.
plates, thus indicating decreased disproportionate growth and non-simultaneous bone maturation. In X-rays of the long tubular bones (except the humeral bones), Szilvássy and Kritscher have identified so-called Harris lines, numerous transverse lines on the proximal and distal ends in the growth zones of the epiphyses, which were first described by Harris [9]. These radiological changes were interpreted as signs of perturbed ossification of the cartilage cells (Figure 4). Interestingly, the identified lines can be observed in an X-ray from the proximal end of one tibial bone, illustrated in a report from Morquio of a 14-year-old female diagnosed with mucopolysaccharidosis [7]. Multiple defects/erosions and irregular growth plates in the distal femoral and proximal tibial bones have been highlighted in the description of dysostosis multiplex typical for MPS or as the underlying cause for gonarthrosis in other LSDs [10]. Osteoblastic and chondroblastic changes with osteoclastic giant cells and slightly decreased bone mass, as well as disorganized repair around subchondral bone plates, have also been described in ML III alpha/beta [18].
The sternum was separated at the manubrium and three segments of the corpus, and all epiphyses were open. From these four bone fragments, it was not possible to recognize any abnormality generally observed in MPS, such as pectus carinatum or excavatum, which is commonly observed in MPS IV (Morquio disease).
In dysostosis multiplex, the clavicles bones are found to be short and thickened, and the ribs are thickened or paddle-shaped [10]. In the Austrian medieval skeleton, no pathological findings of the clavicles or ribs were identified. This might be a finding inconsistent with dysostosis multiplex, because this discrepancy has also been observed in a retrospective study of 5 patients with MPS IVA and 3 patients with MPS VI in which several patients showed no changes in their clavicles or ribs [15].
Unfortunately, because the investigated Austrian medieval skeleton´s hands and feet were not discovered, they could not provide other typical signs of dysostosis multiplex, such as hypoplastic and irregularly-shaped metacarpal and metatarsal bones [10,19].
DISCUSSIONEven skeletons from several thousand years ago can provide
Figure 4 X-ray of the proximal part of both tibial bones. Note the horizontal lines (Harris lines) observed in skeletal diseases with inborn disturbances of osteochondrotic maturation.

CentralBringing Excellence in Open Access
Kircher (2017)Email:
JSM Biochem Mol Biol 4(2): 1025 (2017) 4/6
insights into bone pathology and the events that occured during the life of the individual. One observation in a 5,000- year-old skeleton of a young man found in Pontecagnano, Italy, has revealed signs of double-skull trepanation and femur fracture, thus resulting in chronic osteomyelitis [20]. Several archaeological findings from medieval skeletons have provided insights into diseases such as meningiomatous hyperostosis, as detected in a skull found near the Rochester Cathedral in Great Britain [21]. Three other medieval skeletons found in West-England have provided evidence of erosive peripheral arthritis of different disease-associated origins [22]. In another medieval skeleton from the 11th – early 12th century from the leprosarium cemetery near Winchester, it was possible to isolate DNA of Mycobacterium leprae from a young Pilgrim man who suffered from leprosy [23]. In a medieval skeleton from the 13th – 15th century from Estremoz, Portugal, very specific skeletal changes in the vertebral bodies with congenital fusions and division abnormalities have been interpreted as Klippel-Feil syndrome in a man between 30 to 45 years of age [24].
Numerous attempts have been made to corroborate skeletal dysplasias in ancient specimens on the basis of clinical and radiological findings together with present knowledge of genetic diseases and their characteristic signs. Indeed, conditions such as achondrogenesis, achondrodysplasia, thanatophoric dysplasia, osteogenesis imperfecta and other genetic disorders have been well documented, particularly in recent studies on the collection at the Vrolik museum in Amsterdam [25]. However, even findings of diseases in skeletons from ancient graves are not unique or new. The first illustrations of a possible Maroteaux-Lamy case, another type of mucopolysaccharidosis (MPS VI), were reported by Pachajoa in a collection of pottery from the Tumaco-Tolita culture: these pieces were found on the coast of Colombia-Ecuador and dated between 300 B.C. until 600 A.C., approximately 2,000 years ago [26].
Mucopolysaccharidosis has also been described as one of the differential diagnoses for the humerus varus found in a sub-adult skeleton from a medieval graveyard near Orléans in France [27]. These changes in the femoral head very closely resemble the observations of Legg-Calvé-Perthes disease in bones found in archaeological material in a Langobard cemetery in Moravia and dated from the 5th to 6th century, in which the differential diagnosis of a mucopolysaccharidosis was discussed [28]. In that report, the hip joints were not as flattened as in the presently described skeleton. Parts of an adult skeleton, found in Eunpyeong, near Seoul, South Korea, - from an individual with dwarfism - with many signs of skeletal dysplasia, has provided evidence of a skeletal dysplasia, in which the differential diagnosis of a lysosomal disease has been reported [29].
The Austrian medieval skeleton was found at the extreme south-eastern edge of the cemetery, thus indicating that the individual had a disease with mental retardation. In other early medieval graves, the position of burial appears to be sufficient to conclude the social position of the individual and rites, such as early medieval Muslim skeletons found in the northern areas of the Pyrenees on the Iberian Peninsula [30].
Even in other parts of Lower Austria, there have been discoveries of skeletons thought to present with skeletal signs
of mucopolysaccharide diseases. In 2004, in the course of railway construction near the village of Saladorf (Tullnerfeld), a burial field with 28 skeletons from the late Antiquity period (4th century A.D.) was discovered [31]. The age of these findings was estimated on the basis of the simultaneous geological discovery of coins from this time. In this area around Tulln, one of the auxiliary camps of the Roman legions Lauriacum, Vindobona and Petronell-Carnumtum served as a village for smaller units of soldiers. Around this time, the original rite of burning was slowly transitioning to burying the dead with linen shirts and jewelry. Among these 28 skeletons, 5 children younger than three years of age were found. In one of these skeletons of a child younger than six months of age (grave number 1781b), a strongly thickened squama temporalis of the pars petrosa and a thickened mandibular bone suspicious of a mucopolysaccharidosis have been found and compared with bones from Pottenbrunn [2]. The bones from Pottenbrunn in Lower Austria, assigned to the early Middle Ages, included 9 different skeletons of children with a bone pathology interpreted as mucopolysaccharidosis (personal communication and 32). In all these cases, a final diagnosis of MPS I (Hurler syndrome) or MPS IV (Morquio syndrome) could not be made.
In this more than 1,100-year-old Austrian medieval skeleton, there were many signs consistent with dysostosis multiplex, such as a J-shaped sella turcica in a macrocephalic skull with hyperostosis, frontal bossing, mid-face hypoplasia, a prominent jaw, platyspondyly of the spine with ovoid-shaped vertebrae and significantly more pronounced changes in the thoracolumbar region, skeletal involvement with disproportionate growth retardation and severe bilateral Perthes-like changes in the hip joints. Together, these observations led to the diagnosis of skeletal dysplasia associated with MPS, ML and several other glycoproteinoses, such as alpha-mannosidosis or GM1-gangliosidosis. In all these disorders, attenuated disease courses allow patients to reach an age of several decades. Given the individual´s estimated age of more than twenty years, the author does not agree with the diagnosis of a (Pfaundler-) Hurler type of MPS, but instead suggest an attenuated form of lysosomal disorder, for instance of mucopolysaccharidosis. If MPS type I were present, it may have been attenuated Scheie-disease (MPS IS), although these patients with MPS IS often present with micrognathy and no mental retardation. The list of possible differential diagnoses should still include MPS II (Hunter disease), MPS III (Sanfilippo disease), MPS IV (Morquio disease), and MPS VI (Maroteaux-Lamy disease), because all of these conditions may be present in adult patients. Of these, patients with Sanfilippo, the neuropathic form of Hunter´s disease and even the rare MPS VII (Sly disease) or other lysosomal diseases with dysostosis multiplex, such as glycoproteinoses or ML, are associated with mental retardation. But it cannot be excluded, that any other form of severly impaired functions may have developed, stigmatizing the patient to be retarded, from a loss of hearing or visual function, or the immobility that can be expected because of the severe hip changes.
CONCLUSIONMedieval skeletons offer new insights into diseases described
long after the individual´s deaths. Indeed, it wasn´t until 1918, that the Austrian medical doctor Professor Meinhard von

CentralBringing Excellence in Open Access
Kircher (2017)Email:
JSM Biochem Mol Biol 4(2): 1025 (2017) 5/6
Pfaundler presented, together with his colleague Doctor Gertrud Hurler, the first cases of Pfaundler-Hurler disease, later known as mucopolysacharidosis type IH [33,34]. The original X-rays of these first patients with MPS I, first termed Pfaundler-Hurler disease, show impressive similarities to the presented skeleton from Saladorf, which is, to our knowledge, the first nearly complete skeleton with typical signs of dysostosis multiplex observed for lysosomal storage diseases, especially in the group of mucopolysaccharidoses [35]. Diseases with skeletal changes consistent with dysostosis multiplex and characteristic of lysosomal diseases such as mucopolysaccharidoses, can be carefully classified, documented and even investigated through X-ray analysis, as shown in this skeleton from the early medieval period.
In Austria, a male skeleton more than 1,100-years old was recovered, dating from the early Middle Ages. The many signs of skeletal changes observed in this skeleton showing dysostosis multiplex suggested an underlying mucopolysaccharidosis as well as other entities from the group of lysosomal storage diseases. However, the platyspondyly and very severe changes in the hip joints at the young adult age, the prominent lower jaw and the rather large teeth were highly reminiscent of patients with attenuated forms of Morquio disease (MPS IV).
ACKNOWLEDGEMENTSI am very grateful to Dr. Herbert Kritscher, Vice-Director of the
National Museum of Natural Art, Vienna, Austria and publisher of the ´Annalen des Naturhistorischen Museums´ for the permission to reproduce all the pictures he published in earlier articles.
CONFLICT OF INTERESTI declare that I have no financial interest or any other conflict
of interest. The reproduction of all figures was in accordance with and with written informed consent from Dr. Kritscher, who generated these photos and X-rays from the medieval skeletons for the publications citied.
REFERENCES1. Szilvássy J, Kritscher H. Ein frühmittelalterliches Skelett mit Pfaundler-
Hurler-Syndrom. Ann Naturhist Mus Wien. 1981; 85/A: 73-84.
2. Pail P. Demographie und Paläopathologie einer spätantiken Bevölkerung Pannoniens und Norikums am Beispiel der Gräberfelder Mannersdorfa.d.Leitha und Saladorf (Niederösterreich). Magisterthesis Universität Wien. 2009.
3. Szilvássy J. Der mongolische Einschlag im Gräberfeld von Zwölfaxing, NÖ. Mitt Anthropolog Ges Wien. 1975; 106: 34-41.
4. Szilvássy J. Altersschätzung an den sternalen Gelenkflächen der Schlüsselbeine. Beitr Gerichtl Med. 1977; 35: 343-345.
5. Schultz M, Kritscher H, Szilvássy J. Weitere Untersuchungen an einem frühmittelalterlichen Skelett mit Pfaundler-Hurler-Syndrom. Ann Naturhist Mus Wien. 1984; 86/A: 89-93.
6. Bauer G, Szilvássy J, Kritscher H. Ein mittelalterlicher Karnerschädel und eine linke Tibia aus Falkenstein, Niederösterreich, mit Syphilis. Ann Naturhist Mus Wien. 1983; 85/A: 59-72.
7. Woon-Joon L, Woo EJ, Oh CS, Yoo JA, Kim YS, Jong HH, et al. Bio-Anthropological Studies on Human Skeletons from the 6th Century Tomb of Ancient Silla Kingdom in South Korea. PloS One. 2016; 11:
e0156632.
8. Virchow R. Gesammelte Abhandlungen zur wissenschaftlichen Medicin. Verlag Hamm (G.Grote´sche Buchhandlung).1862: 939-969.
9. Engel D. Dysostosismultiplex – Pfaundler-Hurlersyndrome. Arch Dis Child. 1939; 14: 217-230.
10. Palmucci S, Attinà G, Lanza ML, Belfiore G, Cappello G, Foti PV, et al. Imaging findings of mucopolysacharidoses: a pictorial review. Insights Imaging. 2013; 4: 443-459.
11. Xing M, Parker EI, Moreno-de-Luca A, Harmouche E, Terk MR. Radiological and clinical characterization of the lysosomal storage disorders: non-lipid disorders. Br J Radiol. 2014; 87: 20130467.
12. Thomas JA, Beck M, Clarke JTR. Childhood onset of Scheie syndrome, the attenuated form of mucopolysaccharidosis I. J Inherit Metab Dis. 2010. 33: 421-427.
13. Malm D, Nilssen O. Alpha-mannosidosis. Orphanet J Rare Diseases. 2008; 3: 21.
14. Kannebley JS, Silveira-Moriyama L, Bastos LOD, Steiner CE. Clinical Findings and Natural History in Ten Unrelated Families with Juvenile and Adult GM1 Gangliosidosis. J Inherit Metab Dis Reports. 2015; 24: 115-122.
15. Lachman RS, Burton BK, Clarke LA, Hoffinger S, Ikegawa S, Jin DK, et al. Mucopolysaccharidosis IVA (Morquio A syndrome) and VI (Maroteaux-Lamy syndrome): under-recognized and challenging to diagnose. Skeletal Radiol. 2014. 43: 359-369.
16. Harris HA. Lines of arrested growth in long bones in childhood; correlation of histological and radiographic appearance in clinical and experimental conditions. Brit J Radiol. 1931; 4: 561-588.
17. Morquio L. Arch MédEnf Paris. 1929; 32:129-135.
18. Kerr DA, Memoli VA, Cathey SS, Harris BT. Mucolipidosis Type III α/ß. The first characterization of This Rare Disease by Autopsy. Arch Pathol Lab Med. 2011; 135: 503-510.
19. Mankin HJ, Jupiter J, Trahan CA. Hand and foot abnormalities associated with genetic diseases. Hand. 2011; 6: 18-26.
20. Petrone P, Niola M, Di Lorenzo P, Paternoster M, Graziano V, Quaremba G, et al. Early Medical Skull Surgery for Treatment of Post-Traumatic Osteomyelitis 5,000 Years Ago. PLoS One. 2015; 10: e0124790.
21. Anderson T. An example of meningiomatous hyperostosis from medieval Rochester. Med Hist. 1992; 36: 207-213.
22. Rogers J, Watt I, Dieppe P. Arthritis in Saxon and medieval skeletons. Br Med J. 1981; 283: 1668-1670.
23. Roffey S, Tucker K, Filipek-Ogden K, Montgomery J, Cameron J, O´Connell T, et al. Investigation of a Medieval Pilgim Burial Excavated from the Leprosarium of St Mary Magdalen Winchester, UK. PLoSNegl Trop Dis. 2017; 11: e0005186.
24. Fernandez T, Costa C. Klippel-Feil syndrome with other associated anomalies in a medieval Portuguese skeleton (13th – 15th century). J Anat. 2007; 211: 681-685.
25. Oostra RJ, Baljet B, Dijkstra PF, Hennekam RCM. Congenital Anomalies in the Teratoligical Collection of Museum Vrolik in Amsterdam, The Netherlands. II: Skeletal Dysplasias. Am J Med Genet. 1998: 77; 116-134.
26. Pachajoa H, Rodriguez CA. Mucopolysaccharidoses type VI (Maroteaux-Lamy syndrome) in the pre-Columbian culture of Colombia. Colombia médica. 2014; 45: 85-88.
27. Kacki S, Duneufjardin P, Blanchard P, Castex D. HumerusVarus in a Subadult Skeleton from the Medieval Graveyard of La Madeleine

CentralBringing Excellence in Open Access
Kircher (2017)Email:
JSM Biochem Mol Biol 4(2): 1025 (2017) 6/6
Kircher SG (2017) Attenuated form of Lysosomal Storage Disease in a Medieval Skeleton from Austria. JSM Biochem Mol Biol 4(2): 1025.
Cite this article
(Orléans, France). Int J Osteoarchael. 2013; 23: 119-126.
28. Smrcka V, Marik I, Svenssonova M, Likovsky J. Legg-Calvé-Perthes Disease in Czech Archaeological Material, Case Reports. Clin Orthop Relat Res. 2009; 467: 293-297.
29. Woo EJ, Lee WJ, Hu KS, Hwang JJ. Paleopathological Study of Dwarfism-Related Skeletal Dysplasia in a Late Jeseon Dynasty (South Korean) Population. PLoS ONE. 2015; 10: e0140901.
30. Gleize Y, Mendisco F, Pemonge MH, Hubert C, Groppi A, Houix B, et al. Early Medieval Muslim Graves in France: First Archaeological, Anthropological and Palaeogenomic Evidence. PLoS ONE. 2016; 11: e148583.
31. Blesl C. Zeitschienen. FÖ Mat A. Bundesdenkmalamt. 2005; 107-125.
32. Teschler-Nicola M, Harkins K, Schamall D. Multiple Cases of Inherited Metabolic Disorder (Mucopolysaccharidosis) in a Medieval Population from Pottenbrunn, Lower Austria. Presented at the 34th Annual Meeting of the Paleopathology Association, Philadelphia, Pennsylvania. 2007.
33. Wiskott A. In memoriam Meinhard von Pfaundler. Gedenkrede. Z Kinderheilkunde. 1966; 96: 97-105.
34. Hurler G. Über einen Typ multipler Abartungen, vorwiegend am Skelettsystem. Z Kinderheilkunde (Berlin). 1919; 24: 220-234.
35. Ullrich O. Die Pfaundler-Hurlersche Krankheit. In Ergebnisse der Inneren Medizin und Kinderheilkunde, Herausgeber: M.v.Pfaundler, A. Schittenhelm, Springer-Verlag Berlin. 1943; 63: 933-1000.