Attention Deficit Hyperactivity Disorder – ADHD: The Essentials This AAPA Chapter Lecture Series...
64
Attention Deficit Hyperactivity Disorder – ADHD: The Essentials This AAPA Chapter Lecture Series program is supported by an educational grant from McNeil Pediatrics, Division of Ortho- McNeil-Janssen Pharmaceuticals, Inc., administered by Ortho-McNeil Janssen Scientific Affairs, LLC.
-
Upload
clarissa-baldwin -
Category
Documents
-
view
220 -
download
6
Transcript of Attention Deficit Hyperactivity Disorder – ADHD: The Essentials This AAPA Chapter Lecture Series...

Attention Deficit Hyperactivity Disorder – ADHD: The Essentials
This AAPA Chapter Lecture Series program is supported by an educational grant from McNeil
Pediatrics, Division of Ortho-McNeil-Janssen Pharmaceuticals, Inc., administered by Ortho-
McNeil Janssen Scientific Affairs, LLC.

The Story of Fidgety Phillip by Heinrich Hoffmann
• "Let me see if Philip can
Be a little gentleman; Let me see if he is able To sit still for once at table." Thus spoke, in earnest tone, The father to his son; (cont…….)

Faculty Disclosure Statement
1. In the past 12 months, I have not had a significant financial interest or other relationship with the manufacturer(s) of the product(s) or provider(s) of the service(s) that will be discussed in my presentation.
2. This presentation will not include discussion of pharmaceuticals or devices that have not been approved by the FDA and I will not be discussing unapproved or “off-label” uses of pharmaceuticals or devices.

Learning Objectives1. List the criteria for diagnosis of ADHD.2. Discuss the prevalence of ADHD and its impact
on society.3. Discuss one screening tool used to diagnose and
assess control of ADHD.4. Review all FDA-approved medications for
treatment of ADHD.5. Describe the risks and benefits of using stimulant
medications to treat ADHD.

Pre-test Question #1
1. According to the DSM IV, how long must symptoms of inattention/ hyperactivity be present before considering a diagnosis of ADHD?a. 2 months b. 6 monthsc. 12 moths d. 24 months

Pre-test Question #2
2. What is the estimated prevalence of ADHD among school-aged children in the United States?a. 1-3%b. 4-8%c. 11-14%d. 15-18%

Pre-test Question #3
3. Which of the following is considered a Broadband Screening tool useful in screening for ADHD?a. BASC Monitor Rating Scaleb. Connors Rating Scale (long form) c. ACTeRS Boys and Girls Formd. Vanderbilt Assessment Scales

Pre-test Question #4
4. Which of the following is NOT a criterion for initiation of pharmacotherapy?a. Diagnostic tools confirm diagnosisb. Age 6 or olderc. Blood chemistries within normal range for age d. Normal cardiac examination

Pre-test Question #5
5. Of the following drugs used to treat ADHD, which drug does NOT carry the option of a “drug holiday”?a. Lisdexamphetamine(Vyvanse)b. Methylphenidate(Concerta, Ritalin, etc.)c. Dextroamphetamine(Dexedrine)d. Atomoxetine(Strattera)

Epidemiology of ADHD
• Affects 4-6% of children• Persists into adolescence and adulthood
– 4.4% estimated current adult ADHD• Stimulant Usage
– 1.5 – 2 million American children – 2-3 fold increase over last 30 years– Greater use in females and adolescents
• The total excess cost of ADHD in the US in 2000 was $31.6 billion

Case Study
• DC is a 10 y.o. male that is being seen in your office for evaluation of ADHD. His mother is concerned because his grades have started slipping, and he seems to have a hard time completing his assignments. She also notes that he fidgets a lot and can’t seem to sit still, unless he is playing a video game. DC’s father thinks that he is just “a typical boy”, and needs to apply himself better.

Core Symptoms
INATTENTION
HYPERACTIVITY/IMPULSTIVITY

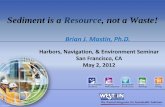
Core Symptoms• Hyperactivity
– Hyperactivity symptoms peak at age 4• Impulsivity
– Peak at age 4, but remain throughout life• Inattention
– Generally appear at 8-9 yo and tend to be lifelong
• DSM IV criteria: Symptoms must be present for at least 6 months to make ADHD diagnosis
Eur Child Adolesc Psychiatry. 2004;13 Suppl 1:I7-30

1. Often fails to give close attention to details 2. Difficulty sustaining attention in tasks or play activities. 3. Does not seem to listen when spoken to directly. 4. Does not follow through on instructions and fails to finish
schoolwork, chores, or duties in the workplace.5. Difficulty organizing tasks6. Avoids tasks that require sustained attention.7. Loses necessary things8. Distracted by external stimuli9. Is forgetful
American Psychiatric Association, Diagnostic and statistical manual of mental disorders, 4th ed. Washington, D.C., 1994. Copyright © 1994 American Psychiatric Association
INATTENTION: CORE SYMPTOM AREAS

1. Fidgets with hands or feet or squirms in seat.2. Leaves seat in classroom.3. Runs about or climbs excessively in situations in which it is
inappropriate.4. Difficulty playing or engaging in leisure activities quietly.5. “On the go" or often acts as if "driven by a motor." 6. Talks excessively. 7. Blurts out answers 8. Difficulty awaiting turn. 9. Interrupts or intrudes on others
American Psychiatric Association, Diagnostic and statistical manual of mental disorders, 4th ed. Washington, D.C., 1994
HYPERACTIVITY/IMPULSTIVITY

INATTENTION
IMPULSIVITY
AGE
HYPERACTIVITY
ADHD: Course of the Disorder

Diagnosis: Questions to ask
• How is your child doing in school?• Has you child had any learning difficulties?• Does your child seem happy in school?• Do you think your child has any behavioral
problems?• Does your child have difficulty completing
assignments?
www.uptodate.com accessed on 3/18/10

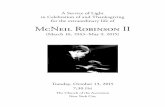
ADHD SubtypesADHD,
Inattentive Type 40%Academic
impairments
ADHD, Hyperactive-
Impulsive Type10%
Behavioral impairments
ADHD, Combined Type 50%
Academic/behavioral
impairments

Noah welcomes his sister Juliette

ADHD Prevalence And Its Impact On Society
PrevalancePhysical/Medical RiskComorbid psych disorder

Prevalence• School-age children: 8-10%
– One the most common childhood disorders• Male: female ratio is 2:1 - 4:1
– Higher ratio for hyperactive subtype• Whites, males, those with older teachers are more likely to be
diagnosed• Lower rates on West coast• Declines with age??
Clinical practice guideline: diagnosis and evaluation of the child with attention-deficit/hyperactivity disorder. American Academy of Pediatrics. Pediatrics 2000; 105:1158.
Green, M, Wong, M, Atkins, D, et al. Diagnosis of Attention Deficit/Hyperactivity Disorder: Technical Review 3. US Department of Health and Human Services, Agency for Health Care Policy and Research; Rockville, MD, 1999.
Taylor, E, Sergeant, J, Doepfner, M, Gunning, B. Clinical guidelines for hyperkinetic disorder. European Society for Child and Adolescent Psychiatry. Eur Child Adolesc Psychiatry 1998; 7:184.
Prevalence, Recognition, and Treatment of Attention-Deficit/Hyperactivity Disorder in a National Sample of US Children. Arch Pediatr Adolesc Med. 2007 Sep;161(9):857-64.

ADHD Physical/Medical Risk
• Seizures – 2.5X greater• Sleep problems(39%-56%)• Developmental coordination disorder(50%+)• Reduced Physical fitness, Strength, Stamina• Accident proness(57%+)• 2x-3x the medical cost of a normal child

Comorbid Psychiatric Conditions
• 50% of children with ADHD have one or more comorbid condition.– Oppositional defiant disorder (40%)– Conduct disorder (20%)– Depression & mood disorders (15%)– Anxiety disorder (25%)– Learning disabilities (25%)
J Am Acad Child Adolesc Psychiatry 2001 Feb;40(2):147-58.

Prognosis
• Education• Employment• Peer relationships• Substance Use• Injuries • Driving

Prognosis• Education
– Impaired academic functioning– Persist into adulthood
• Employment– Lower status jobs– Poorer performance
• Peer relationships

Prognosis
• Substance Use– Increased prevalence?
• Injuries – Greater risk for intentional or unintentional
injury• Driving
– Twice as likely to be involved in a MVC

Pathogenesis and Screening in ADHD.
Broadband/Narrow ScreeningGeneticsNeuroanatomyCathecholamine Imbalance

Case Study
• MA is a 7 year old male in your clinic whose mother suspects that her son has ADHD. How would you evaluate if this child has ADHD?

Screening
Broadband screening• Rely on parent- , teacher-, or child-completed
questionnaires• Rule out a broad range of possible diagnoses.Narrow screening• Directed toward a specific diagnosis• >90% accuracy in diagnosing ADHD
Arch Dis Child. 2005 Oct;90(10):1010-5

Pathogenesis
• Disorder of multiple causes
• Causes may compound each other
• Genetics• Neuroanatomy
– Frontalstriatial cerebellar cicuit
• Catecholamine imbalance

ADHD Risk Factors
• PRENATAL– Maternal smoking– Maternal Etoh– Cocaine user – polydrug– Pesticides?
• POSTNATAL– Head trauma, tumors– Lead posioining – affinitiy for dopamine receptors– ALL – Inattentive type

Case Study
RW has the diagnosis of ADHD. Her mother wonders about the treatment options, and is concerned about the side effects of ADHD medications. What can you tell her about the medications available and the side effects of the stimulant medication you are about to prescribe?

Treatment of ADHD
MedicationBehavioral therapy

Treatment
• Behavioral• Pharmacological

Behavioral Therapy
• Maintaining a daily schedule• Provide logical choices for schoolwork and
toys• Setting small reasonable goals• Rewarding positive behavior• Using charts• Limit choices• Cognitive therapy??

Criteria for Initiation of Pharmacotherapy• Diagnostic assessment confirms ADHD.• Child age is greater than 6?• Parents accept pharmacotherapy as contribution to
management• Child has a normal cardiac exam• Administration of medication will be reliable• Consider a specialist:
– Child with Tourette syndrome– Child with a pervasive developmental delay– Child with seizures – Caridiac question
An auditable protocol for treating attention deficit/hyperactivity disorder. Arch Dis Child 2001; 84:404.

Prior to Commencement
• Discuss: fears/questions• Discuss: risk/benefit of treatment• Discuss: trial and error period• Medication delivery: 5 P’s
– Patch, pump, pellet, pill, prodrug

Stimulant Medications• Generally thought of as first line treatment• Methylphenidate
– Short acting: Ritalin, Methylin, Focalin– Intermediate: Metadate, Methylin ER– Long acting: Concerta, Daytrana(patch)
• Amphetamines– Short acting: Dextroamphetamine/amphetamine
(Adderall), Dextroamphetamine sulfate (Dextrostat, Dexedrine)
– Long acting: Lisdexamfetamine (Vyvanase), Adderall XR

Stimulant Medication: Side Effects
• Monitor blood pressure, heart rate• Appetite Reduction/Weight Loss• Final height ?• Insomnia• Tics• Rare: Headache/abdominal pain• Rare: Depression/withdrawn behavior

Initial CV Risk Assessment
• Personal history, focusing on cardiovascular events
• Family history of cardiac problems
• Physical exam• Cardiac consultation if
irregularities are suspected
• EKG ?

Non-Stimulant Therapy• Atomoxetine (Strattera) • Alpha-adrenergic agents
– Guanfacine (Tenex)– Clonidine (Catapres)
• Anti-depressant (non-SSRI, non-tricyclic)– Buproprion (Wellbutrin)

Atomoxetine (Strattera)• Selective norepinephrine reuptake inhibitor• May work via norepinephrine transporter• In randomized studies: as effective as
methylphenidate• May be given as single daily dose or bid• Currently recommended as second-line only

Adverse Side Effects: Atomoxetine
• Nausea• Sedation• Tics• Liver Injury• Suicidal Thinking• Cardiovascular

Other Medications
• Antidepressants– TCA– Bupropion
• Alpha 2 adrenergic agonist– Clonidine– Guanfacine hydrochloride

Alpha-2-adrenergic agonists
• Not routinely prescribed• Clonidine
– Not as effective as stimulants– Patient profile– Side effects
• Guanfacine hydrochloride– Patient profile– Side effects
J Am Acad Child Adolesc Psychiatry 1999 Dec;38(12):1551-9.

Alpha-2 Agonist
• Drowsiness may occur• Rare: depression• Rare: hypotension, cardiac arrhythmia• Aggression

Antidepressants
• TCA– Inhibit the reuptake of norepinephrine and serotonin– Second line therapy– Cardiac side effects
• Bupropion– Blocks the reuptake of norepinephrine and dopamine– More stimulant properties than TCAs– Side effects- lowers seizure threshold
J Am Acad Child Adolesc Psychiatry 1996 Oct;35(10):1314-21.

Low-dose Antidepressants
• Bupropion, Desipramine, and imipramine• Limited evidence base• Not as frequently used• Side-effects: rare with low-dose• Risk of idiosyncratic effect such as arrhythmia

MEDICATION MANAGEMENT
TitrationMaintenanceDrug HolidaysTermination

Medication Monitoring
• For stimulant-naïve patient– Initially every 1-2 weeks– Titrate medication dosage as needed based
on efficacy and side effects
• Routinely every 4-6 months (at least twice a year)– Evaluate medication efficacy, side effects– Physical examination

Titration• Optimal dose and frequency are determined• The timing of dose administration in relationship to meals
and expectations is important.• Medication should be started on a weekend day.• Dosing history varies on clinical picture• During titration, have a standardized assessment of effect.• Monitor at least 2-4 weeks• Monitor the child's height, weight, blood pressure, and
pulse.• Switching medication classes
JAMA 1998 Apr 8;279(14):1100-7

Maintenance
• Begins once optimal dose achieved.• Regular monitoring
– Vitals– Adjust dose– Monitor for side effects
J Am Acad Child Adolesc Psychiatry. 2007 Jul;46(7):894

Drug Holidays
• Definition
• Not an option for children who are taking atomoxetine.
• Inattentive type

Termination of Medication
• Duration of pharmacologic therapy is highly individualized
• Ongoing evaluation of the risk-benefit analysis• Long-term side effects and drug dependence
do not occur with stimulant medications or atomoxetine
• Other medications, follow prescribing guidelines
J Clin Psychopharmacol 2004 Feb;24(1):30-5.

Things you may have heard…
• Food additives• Refined sugar• Essential fatty acids• Iron deficiency• Pesticides

Resources for Families• CHADD: Children and Adults with ADD
– www.chadd.org• NAMI: National Alliance for the Mentally Ill
– www.nami.org• ADDA: National Attention Deficit Disorder
Association– www.add.org
• NIMH: National Institute of Mental Health– www.nimh.nih.gov/publicat/adhd.cfm

More Resources for Families
• United States Department of Education– www.ed.gov/offices/OSERS
• Society for Developmental and Behavioral Pediatrics– www.dbpeds.org/handouts
• American Academy of Child and Adolescent Psychiatry (AACAP)– www.aacap.org/publications/factsfam/noattent.htm

Post-test Question #1
1. According to the DSM IV, how long must symptoms of inattention/ hyperactivity be present before considering a diagnosis of ADHD?a. 2 months b. 6 monthsc. 12 moths d. 24 months

Post-test Question #2
2. What is the estimated prevalence of ADHD among school-aged children in the United States?a. 1-3%b. 4-6%c. 11-14%d. 15-18%

Post-test Question #3
3. Which of the following is considered a Broadband Screening tool useful in screening for ADHD?a. BASC Monitor Rating Scaleb. Connors Rating Scale (long form) c. ACTeRS Boys and Girls Formd. Vanderbilt Assessment Scales

Post-test Question #4
4. Which of the following is NOT a criterion for initiation of pharmacotherapy?a. Diagnostic tools confirm diagnosisb. Age 6 or olderc. Blood chemistries within normal range for age d. Normal cardiac examination

Post-test Question #5
5. Of the following drugs used to treat ADHD, which drug does NOT carry the option of a “drug holiday”?a. Lisdexamphetamine(Vyvanse)b. Methylphenidate(Concerta, Ritalin, etc.)c. Dextroamphetamine(Dexedrine)d. Atomoxetine(Strattera)

Thank you for attending this AAPA Chapter Lecture Series program supported by an educational grant from
McNeil Pediatrics, Division of
Ortho-McNeil-Janssen Pharmaceuticals, Inc., administered by
Ortho-McNeil Janssen Scientific Affairs, LLC