Atrial Fibrillation: Past, Present and Future Mohammad Shenasa MD, FACC O’Connor Hospital, San...
151
Atrial Fibrillation: Past, Present and Future Mohammad Shenasa MD, FACC O’Connor Hospital, San Jose, CA 5th Congress of Cardiologists and Angiologists of Bosnia and Herzegovina Bosnia M. Shenasa 2010
-
Upload
evelin-tuckett -
Category
Documents
-
view
214 -
download
0
Transcript of Atrial Fibrillation: Past, Present and Future Mohammad Shenasa MD, FACC O’Connor Hospital, San...

Atrial Fibrillation:Past, Present and Future
Mohammad Shenasa MD, FACCO’Connor Hospital, San Jose, CA
5th Congress of Cardiologists and Angiologists of Bosnia and Herzegovina
BosniaMay 2010
M. Shenasa 2010
Avicenna, Persian physician, philosopher & poet980-1037 AD
M. Shenasa 2010
M. Shenasa 2010

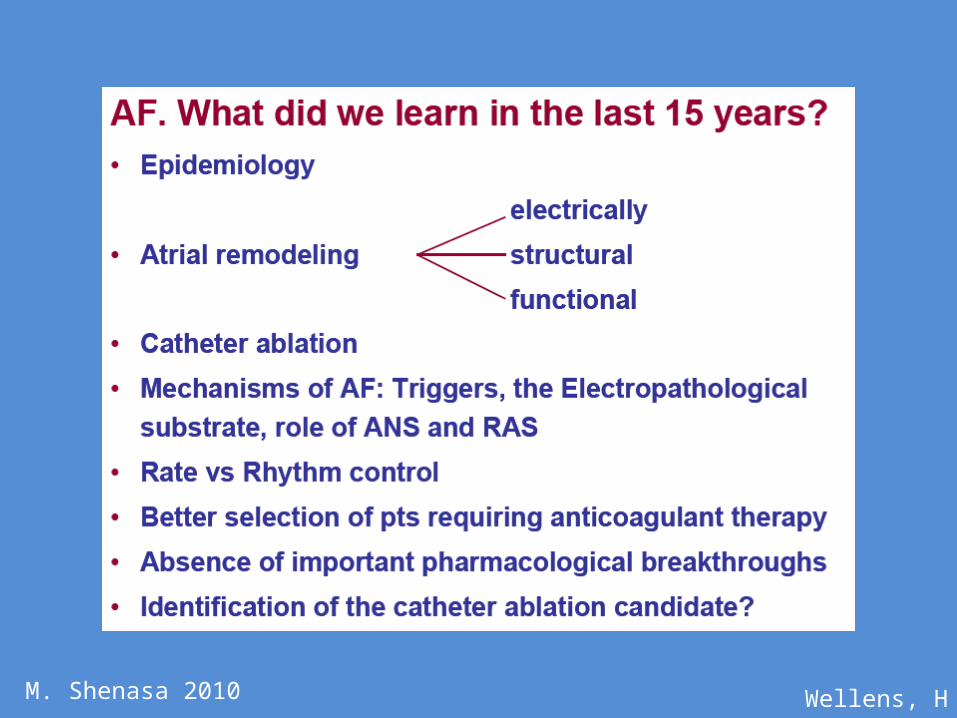
Lecture Highlights • Epidemiology• Mechanisms • Heart Failure and AF• Asymptomatic AF• Stroke and AF • Inflammation and AF• AF and Remodeling • AF and Fibrosis
• New and Atrial specific Antiarrhythmics
• Upstream Therapies in AF
• AF and Ablation • Future Directions
M. Shenasa 2010

2008-2009
2008: 2,4692009: 2,528
AFPast, Present, Future
M. Shenasa 2010

Atrial Fibrillation: Medicare Data
• AFib is a highly prevalent disease and associated with significant cardiovascular morbidity and morality
• AFib costs Medicare more than $15.7 billion annually due to costly complications
• Screening and diagnosis of AFib is limited in Medicare population
• Estimated by 2050, 15 million Americans will suffer from AF and its adverse consequences
• Conclusion– A need exists for Medicare to find ways to reduce overall
costs and improve the quality of care for AFib patients
M. Shenasa 2010
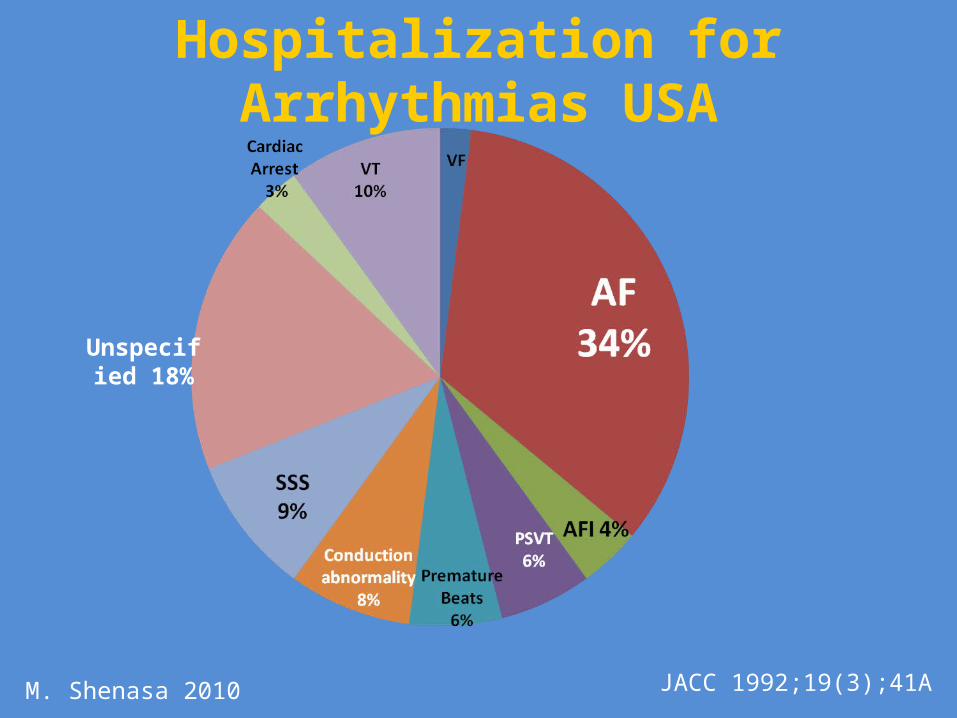
Unspecified 18%
Hospitalization for Arrhythmias USA
JACC 1992;19(3);41AM. Shenasa 2010
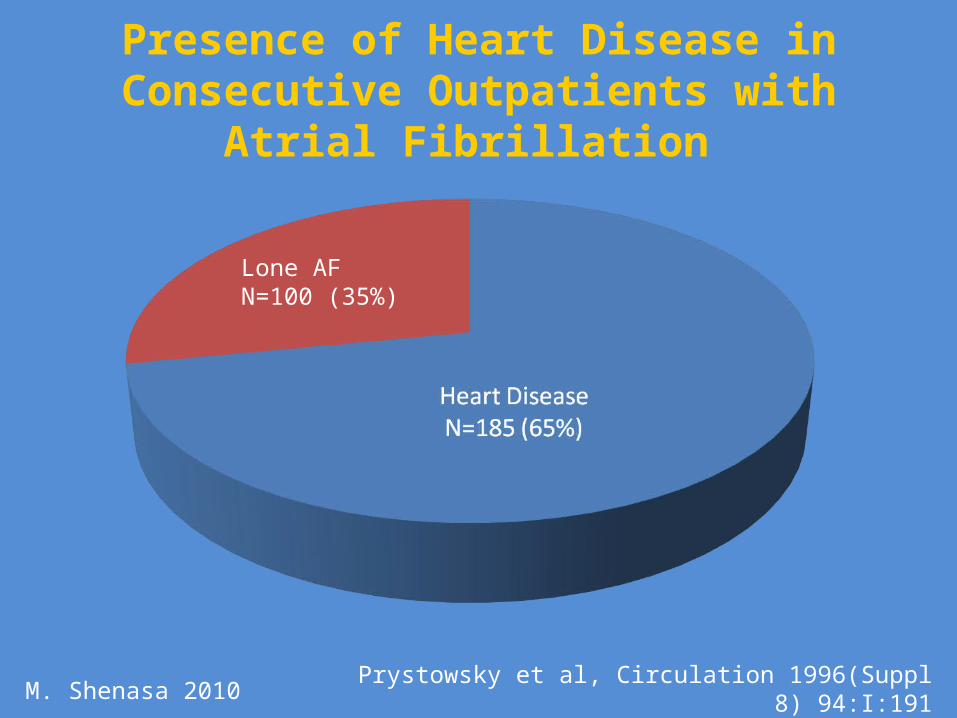
Presence of Heart Disease in Consecutive Outpatients with Atrial Fibrillation
Lone AFN=100 (35%)
Prystowsky et al, Circulation 1996(Suppl 8) 94:I:191M. Shenasa 2010
Wellens, HM. Shenasa 2010
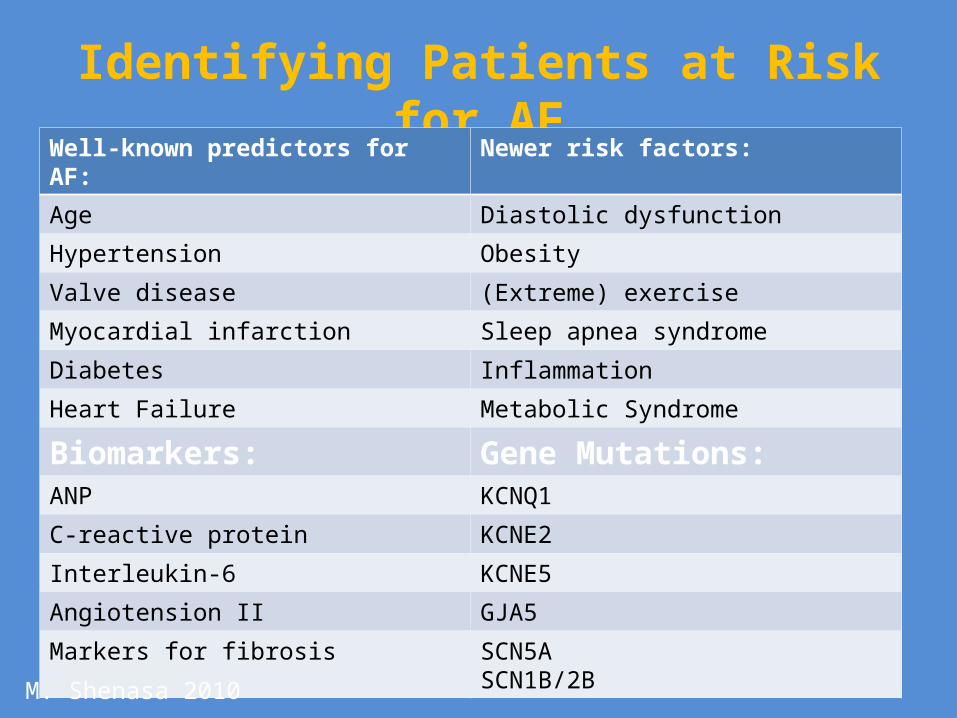
Identifying Patients at Risk for AFWell-known predictors for AF: Newer risk factors:
Age Diastolic dysfunction
Hypertension Obesity
Valve disease (Extreme) exercise
Myocardial infarction Sleep apnea syndrome
Diabetes Inflammation
Heart Failure Metabolic Syndrome
Biomarkers: Gene Mutations:ANP KCNQ1
C-reactive protein KCNE2
Interleukin-6 KCNE5
Angiotension II GJA5
Markers for fibrosis SCN5ASCN1B/2B
M. Shenasa 2010

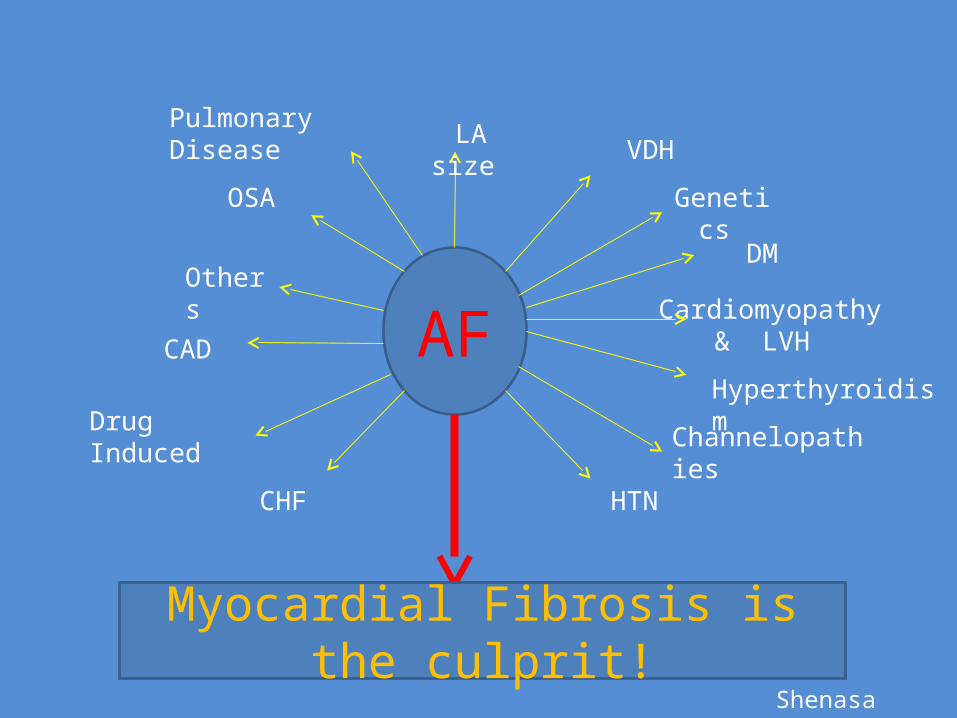
AF
LA size VHD
DM
HTNCardiomyopathy& LVH
CHF
CAD
OSA
Atrial Fibrosis Others
ChannelopathiesDrug Induced
Hyperthyroidism
Pulmonary Disease
Genetics
M. Shenasa 2010
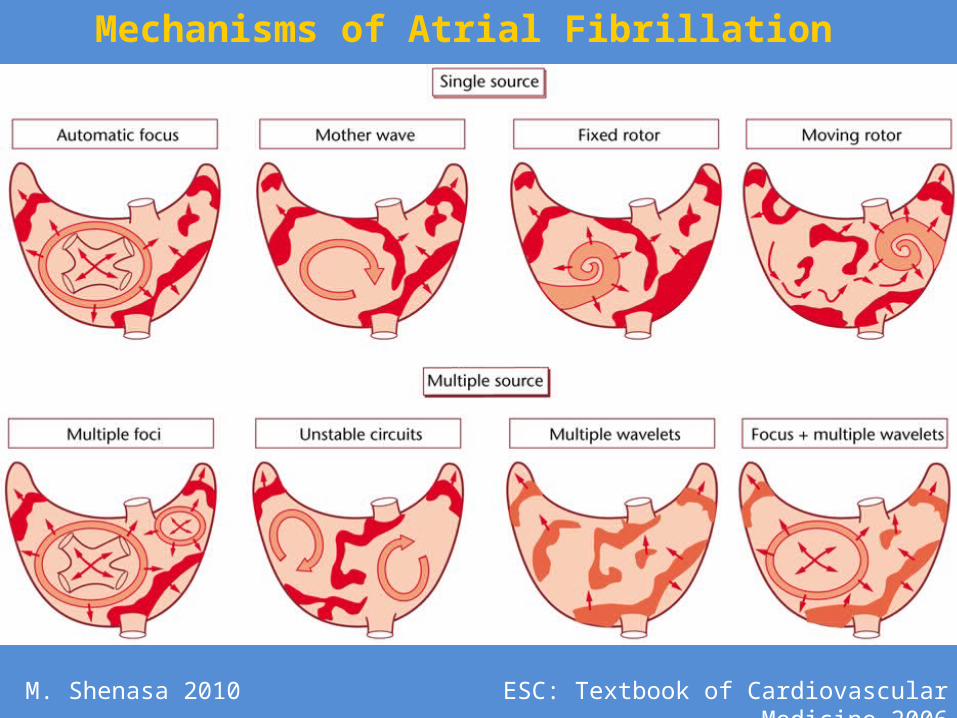
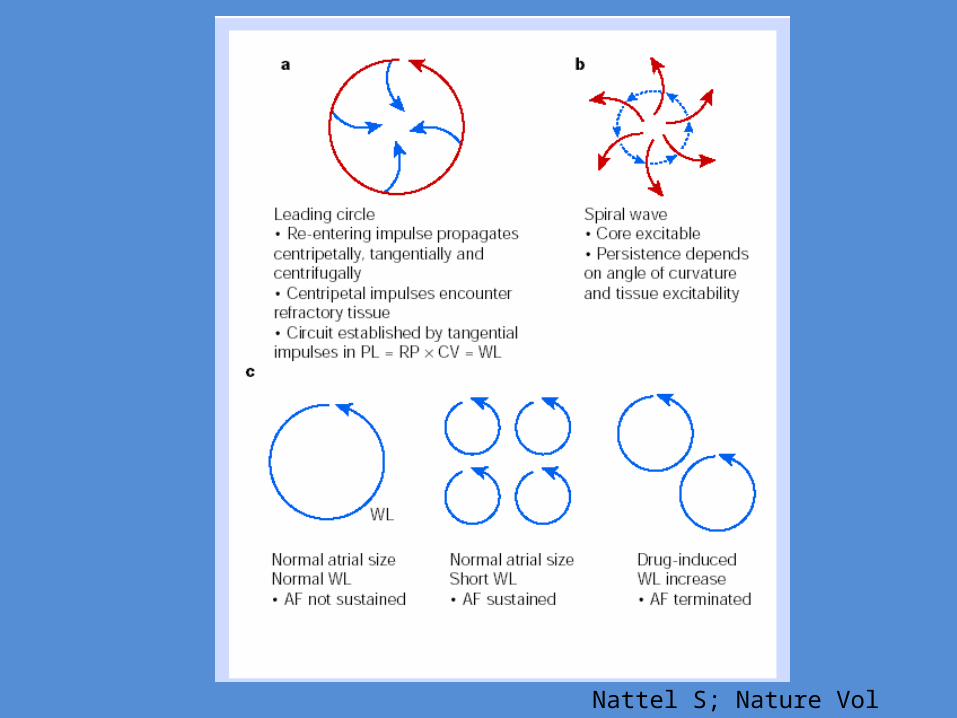
Mechanisms of Atrial Fibrillation
ESC: Textbook of Cardiovascular Medicine 2006M. Shenasa 2010
Cardiology Clinics 2009; 27:79-93 (
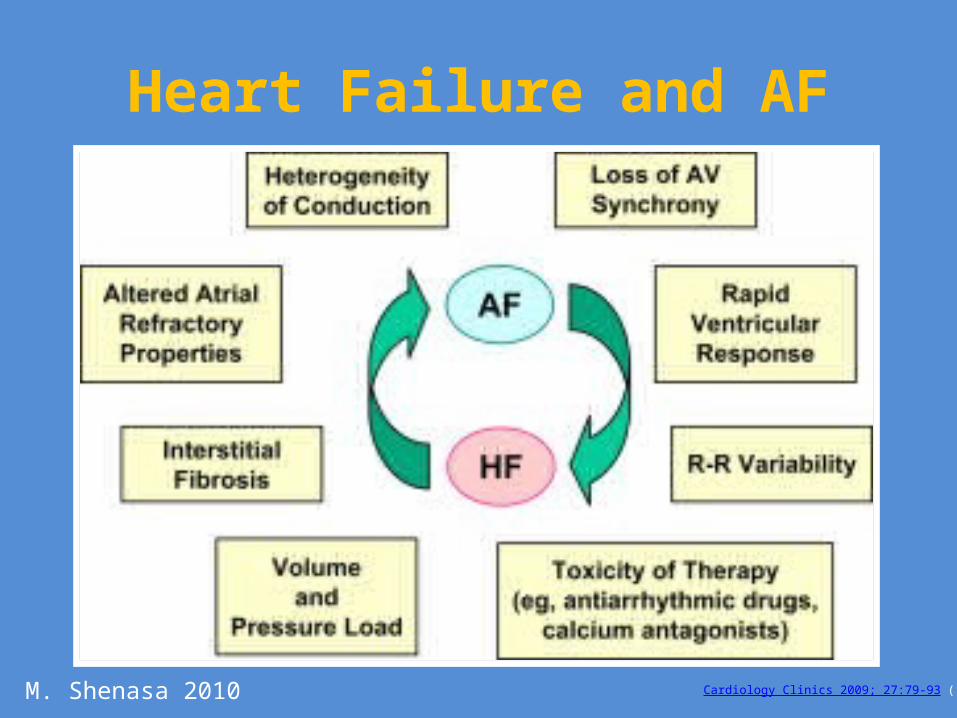
Heart Failure and AF
M. Shenasa 2010
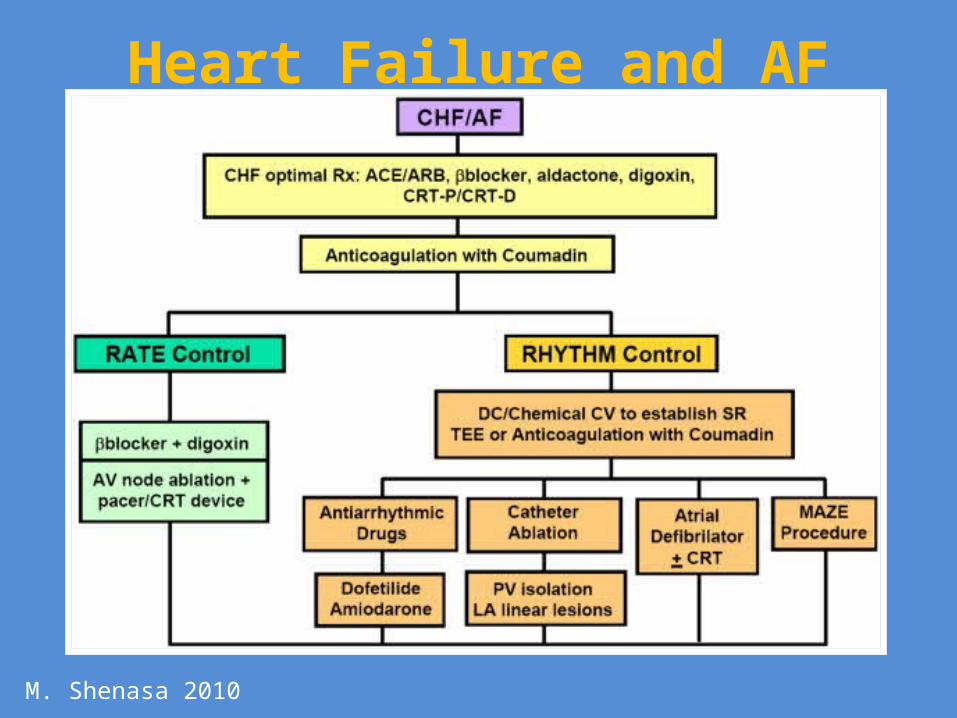
Heart Failure and AF
M. Shenasa 2010
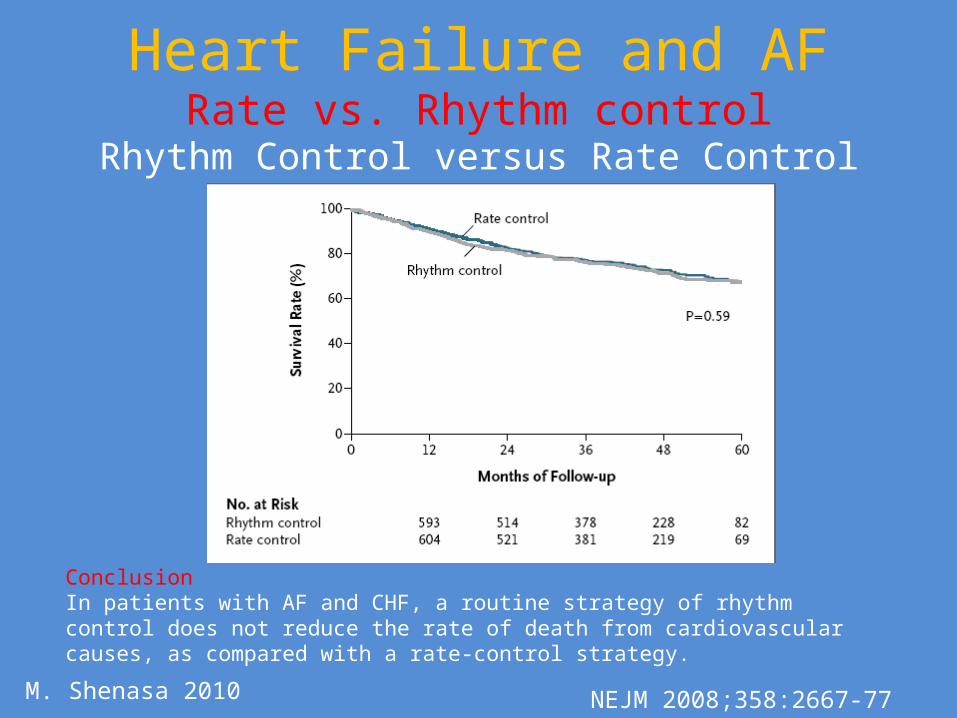
Heart Failure and AFRate vs. Rhythm control
Rhythm Control versus Rate Control for AF & HF.
Conclusion In patients with AF and CHF, a routine strategy of rhythm control does not reduce the rate of death from cardiovascular causes, as compared with a rate-control strategy.
M. Shenasa 2010 NEJM 2008;358:2667-77

Heart Failure and AFMaintenance of Sinus Rhythm and Survival in Patients With CHF and AF
Talajic, M. et al. JACC 2010;55:1796-1802
Conclusion:A rhythm-control strategy or the presence of sinus rhythm are not associated with better outcomes in patients with AF and CHF.
M. Shenasa 2010
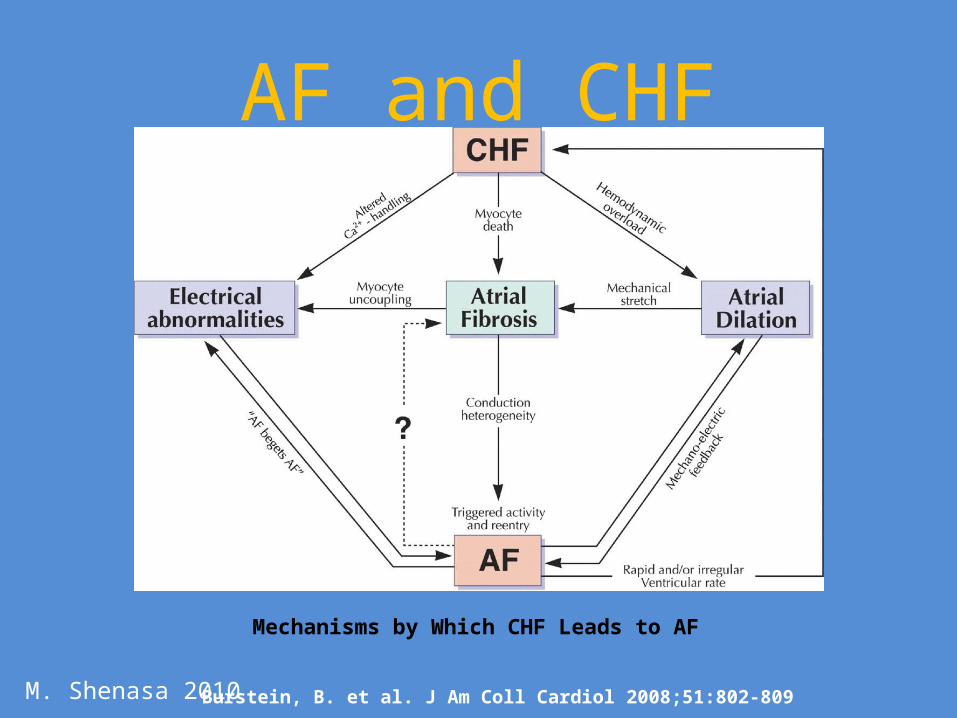
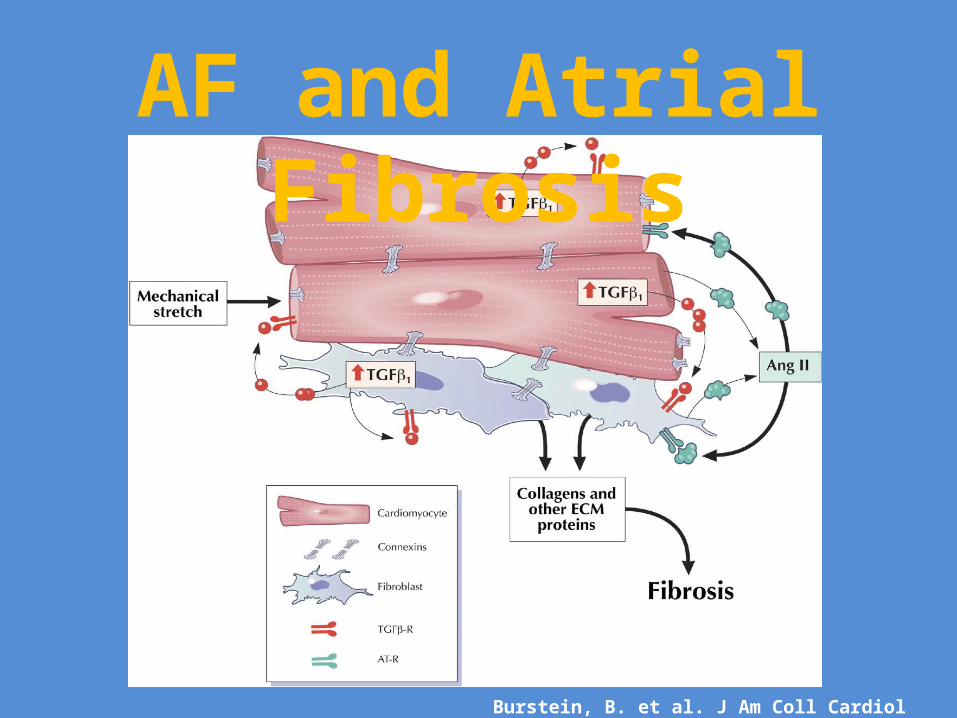
Burstein, B. et al. J Am Coll Cardiol 2008;51:802-809
Mechanisms by Which CHF Leads to AF
AF and CHF
M. Shenasa 2010
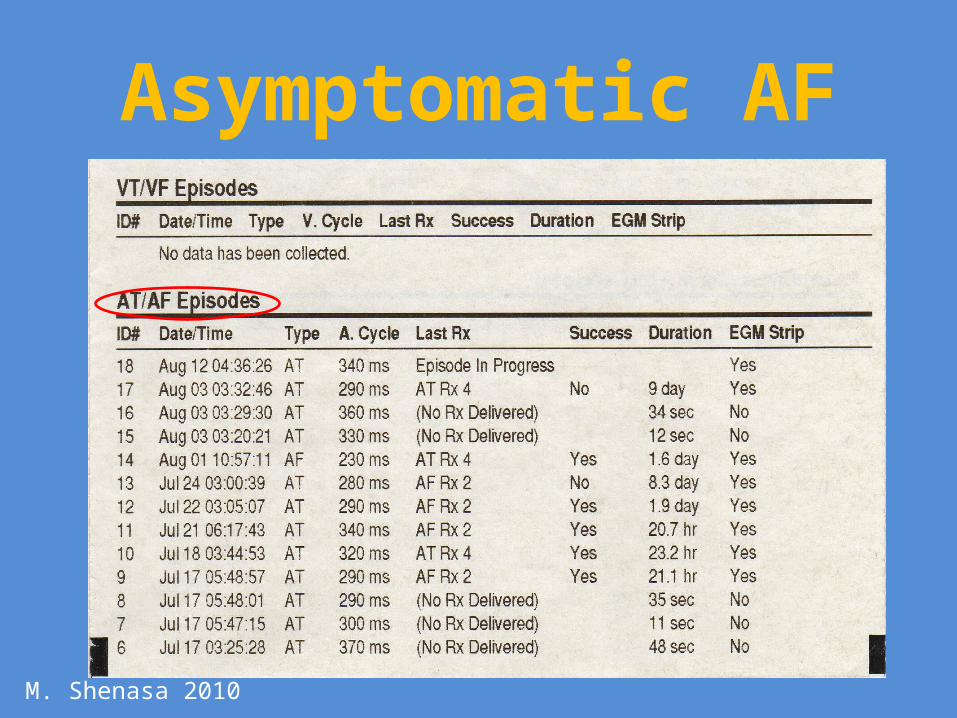
Asymptomatic AF
M. Shenasa 2010

Stroke and AFHeart Disease and Stroke
• Stroke affects about 795,000 individuals annually in the US only.
• 1 every 40 seconds.• Third leading cause of death• Number 1 cause of disability• 87% are ischemic stroke i.e. embolic• 13% are hemorrhagic stroke• 1 in 15 people develop brain aneurysm in their life• Ruptured aneurysm are 30,000 cases of hemorrhagic
stroke. • Silent stroke cognitive decline, dementia and
Alzheimer's are associated with AFM. Shenasa 2010

M. Shenasa 2010

Silent Atrial Fibrillation
195 Patients
86(44%)CHB
No Hx of AF
109 (55%)Hx of AF in SR at the
time of impact
35 (40%) Silent AF
Duration <1 min to 2 weeks
68 (62%)Silent AF
9/35 (25%) permanent AF in F/U
19/68 (30%) permanent AF
M. Shenasa 2010

Inflammation and AFMarkers for inflammation
1.) High Sensitivity C-reactive protein (hs-CRP)2.) Interleukin (IL)-63.) White cell count4.) Tumor necrosis factor alpha (TNFα)Others Cause of inflammation • Oxidative Stress• Endothelial dysfunction • Coexisting co-morbid risk factors & others
M. Shenasa 2010
Inflammation and AFHypothesis:
• Ang-II may play a key role in pathogenesis of AF only in a subset of patients
• ACEIn and ARB may prevent and treat AF in those patients with elevated serum ACE and Ang-II activity.
Courtesy of A. Sovari
Inflammation and AFInflammation
Fibrosis Atrial Fibrillation?Intracardiac and extracardiac markers of inflammation during atrial fibrillation.
Markers of inflammation before and after curative ablation of atrial flutter.
Marcus G.M., et al Heart Rhythm 2008;5:215-221
Normalization of inflammation markers after AF ablation and cardioversion suggests inflammation is the effect rather than the cause.
M. Shenasa 2010
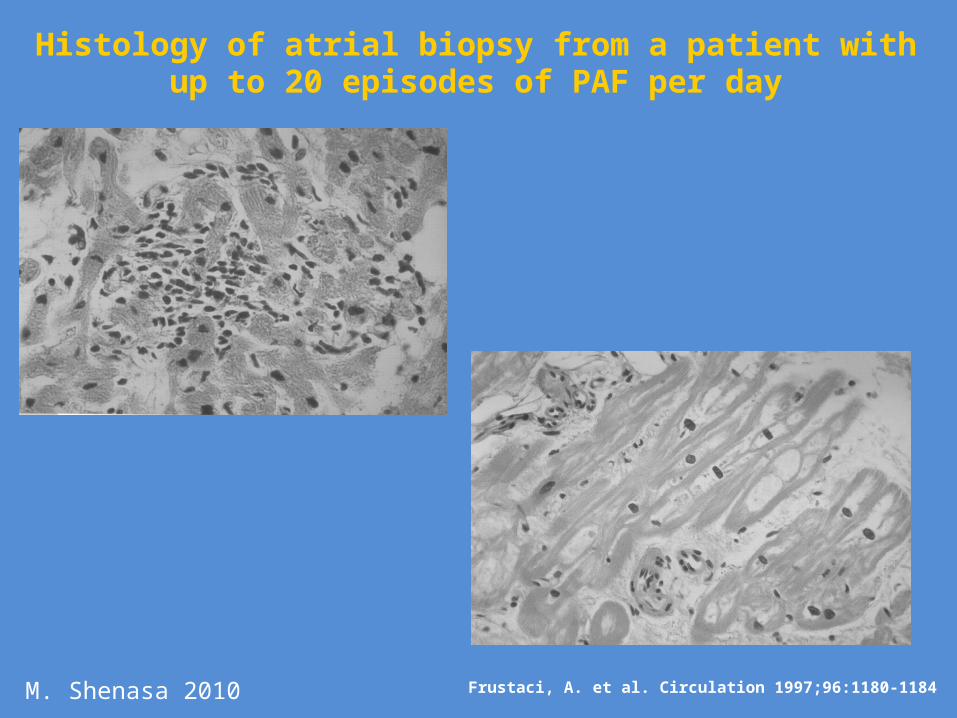
Frustaci, A. et al. Circulation 1997;96:1180-1184
Histology of atrial biopsy from a patient with up to 20 episodes of PAF per day
M. Shenasa 2010
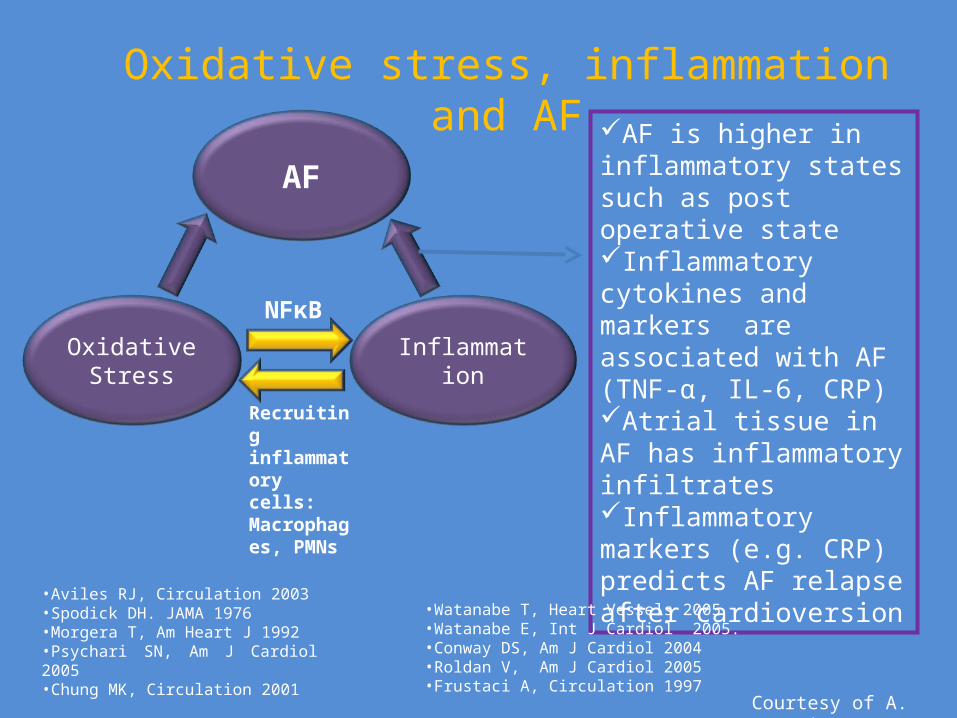
Oxidative Stress Inflammation
NFκB
Recruiting inflammatory cells: Macrophages, PMNs
AF is higher in inflammatory states such as post operative stateInflammatory cytokines and markers are associated with AF (TNF-α, IL-6, CRP)Atrial tissue in AF has inflammatory infiltratesInflammatory markers (e.g. CRP) predicts AF relapse after cardioversion
•Aviles RJ, Circulation 2003•Spodick DH. JAMA 1976•Morgera T, Am Heart J 1992•Psychari SN, Am J Cardiol 2005•Chung MK, Circulation 2001
•Watanabe T, Heart Vessels 2005•Watanabe E, Int J Cardiol 2005.•Conway DS, Am J Cardiol 2004 •Roldan V, Am J Cardiol 2005 •Frustaci A, Circulation 1997
Oxidative stress, inflammation and AF
AF
Courtesy of A. Sovari
Inflammation and AF• AF is clearly associated with increased level of inflammatory
markers. • Atrial biopsies with in patients with AF have also confirmed the
presence of inflammation • There is also evidence supporting a link between inflammation
and AF, and some of the drug therapies, such as the ACE-inhibitors, ARBs, Steroids, fish oils, and vitamin C, that might be efficacious in the prevention of AF by modulating inflammatory pathways.
• However, randomized trial and longitudinal studies are needed to confirm the direct relationship between AF and inflammation
M. Shenasa 2010

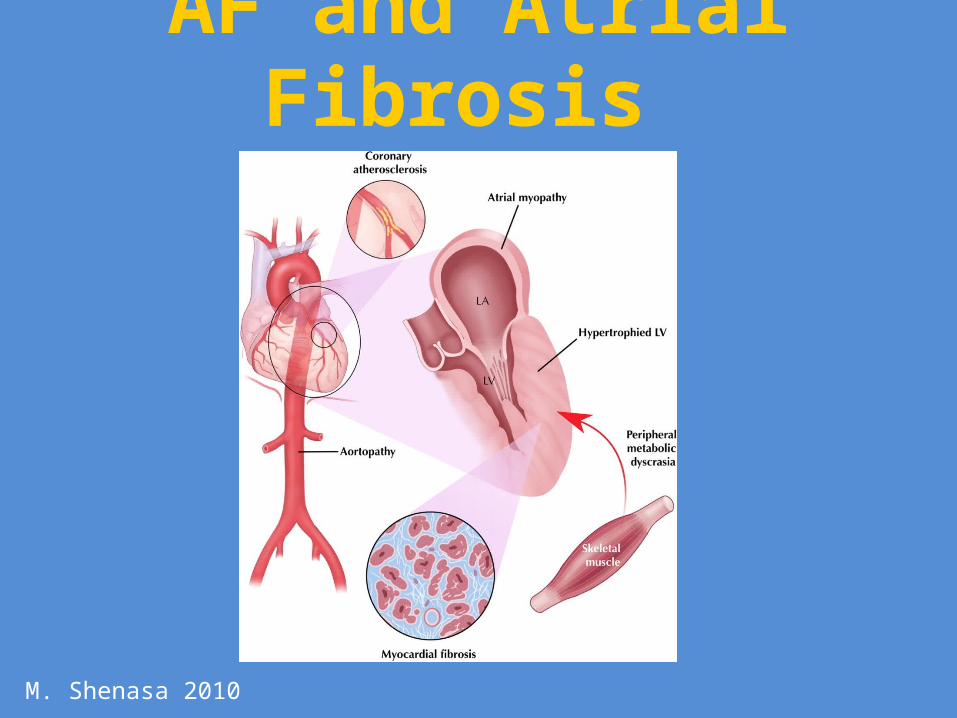
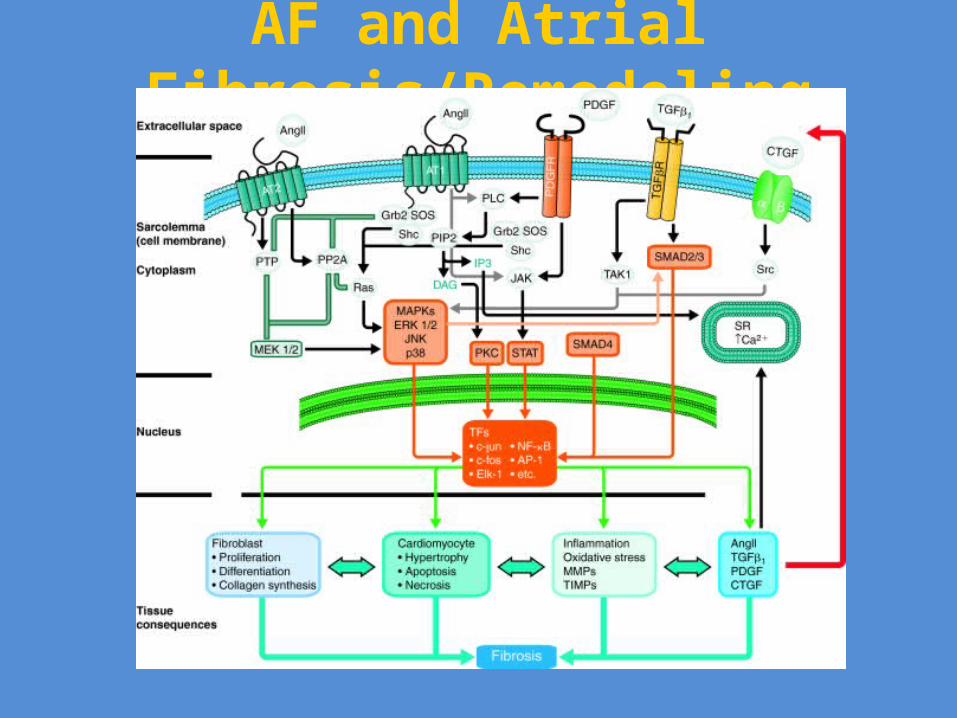
AF and Atrial Fibrosis
AF Fibrosis?After age 65, 5% per year develop
atrial myocardium fibrosis
M. Shenasa 2010
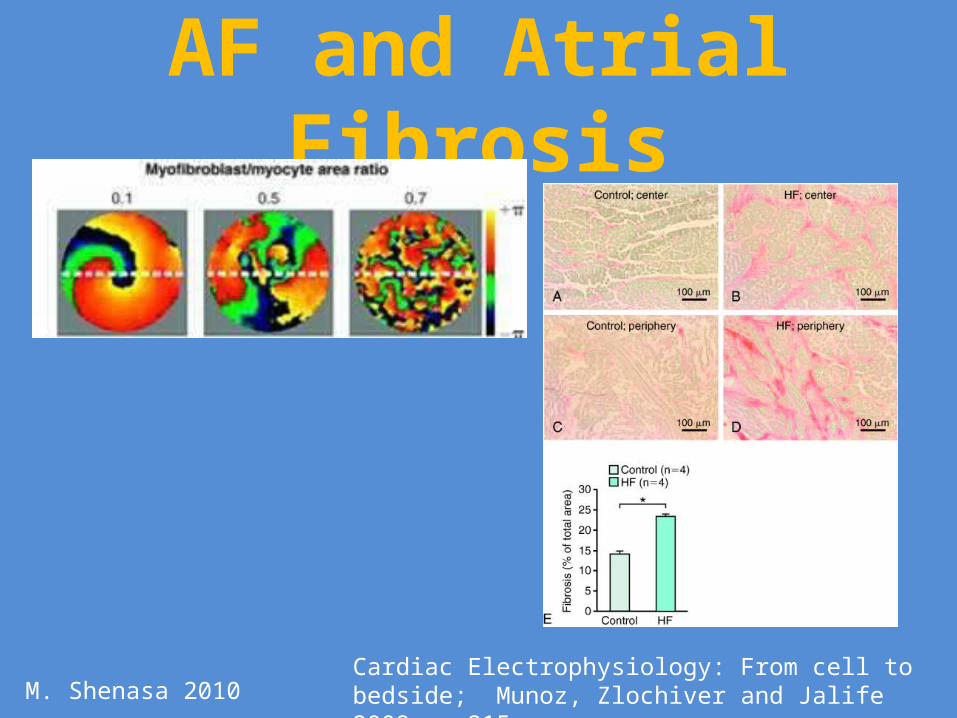
AF and Atrial Fibrosis
Cardiac Electrophysiology: From cell to bedside; Munoz, Zlochiver and Jalife 2009 pp 215M. Shenasa 2010
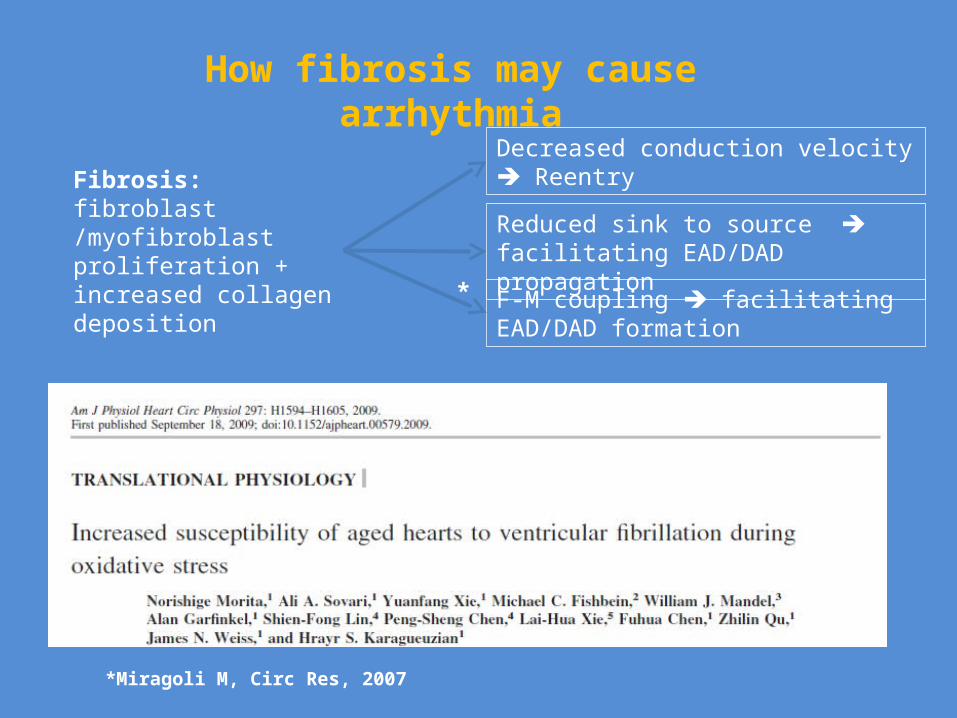
Fibrosis: fibroblast /myofibroblast proliferation + increased collagen deposition
Decreased conduction velocity Reentry
Reduced sink to source facilitating EAD/DAD propagation
F-M coupling facilitating EAD/DAD formation
How fibrosis may cause arrhythmia
*Miragoli M, Circ Res, 2007
*

AF and Atrial Fibrosis
AF
LA size VDH
DM
HTN
Cardiomyopathy& LVH
CHF
CAD
OSA
Others
ChannelopathiesDrug Induced
Hyperthyroidism
Pulmonary Disease
Shenasa 2010
Myocardial Fibrosis is the culprit!
Genetics
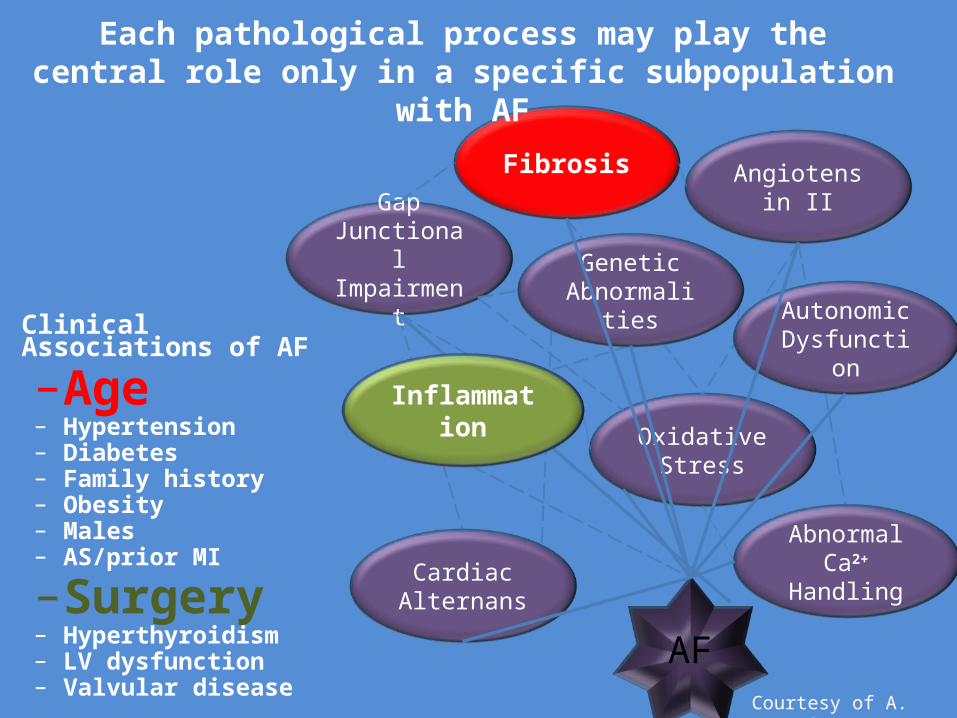
Oxidative Stress
Fibrosis
Gap Junctional
Impairment
Cardiac Alternans
Abnormal Ca2+ Handling
Angiotensin II
AF
Autonomic Dysfunction
Genetic Abnormalities
• Clinical Associations of AF
–Age– Hypertension– Diabetes– Family history– Obesity– Males– AS/prior MI
–Surgery– Hyperthyroidism– LV dysfunction– Valvular disease
Inflammation
Each pathological process may play the central role only in a specific subpopulation with AF
Courtesy of A. Sovari

The main result: AF recurred in 51.4% in valsartan group, 52.1% in placebo group
Disappointment or a lesson in chess?

AF and Remodeling
M. Shenasa 2010

Atrial remodeling in AFElectrical remodeling
• Atrial remodeling refers to the changes in atrial properties and function that promote AF. Rapid atrial activation provokes both a shortening of the atrial action potential and refractory period, as well as an impaired rate adaption with reduced wave length, thereby enhancing the risk for functional reentry.
Europace 2009;11:860-885
M. Shenasa 2010
Atrial remodeling in AF Structural remodeling
• LA dilatation and increasing atrial fibrosis. Increased atrial pressure and volume related to structural heart disease. HTN or aging will cause ultra structural changes in the heart and leads to activation of fibroblasts, enhanced collagen depositions and fibrosis, which in term result in electrical remodeling.
M. Shenasa 2010
M. Shenasa 2010

New Antiarrhythmics for AF
M. Shenasa 2010
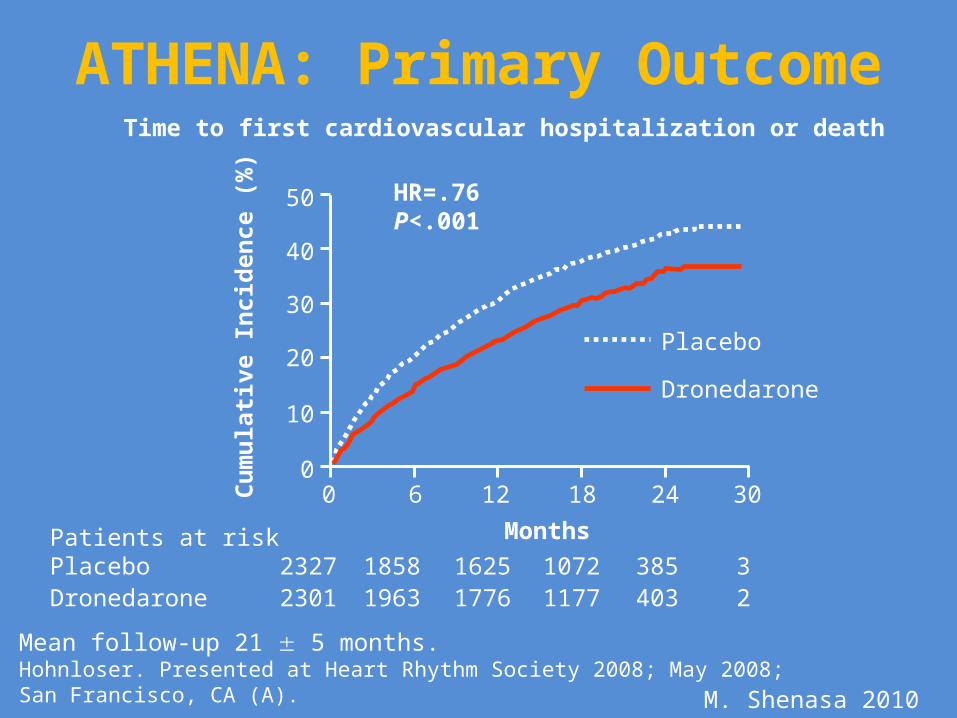
ATHENA: Primary OutcomeTime to first cardiovascular hospitalization or death
Mean follow-up 21 5 months.Hohnloser. Presented at Heart Rhythm Society 2008; May 2008; San Francisco, CA (A).
Patients at riskPlacebo 2327 1858 1625 1072 385 3Dronedarone 2301 1963 1776 1177 403 2
0
10
20
30
40
50
0 6 12 18 24 30
Cu
mu
lati
ve I
nci
den
ce (
%) HR=.76
P<.001
Months
Placebo
Dronedarone
M. Shenasa 2010
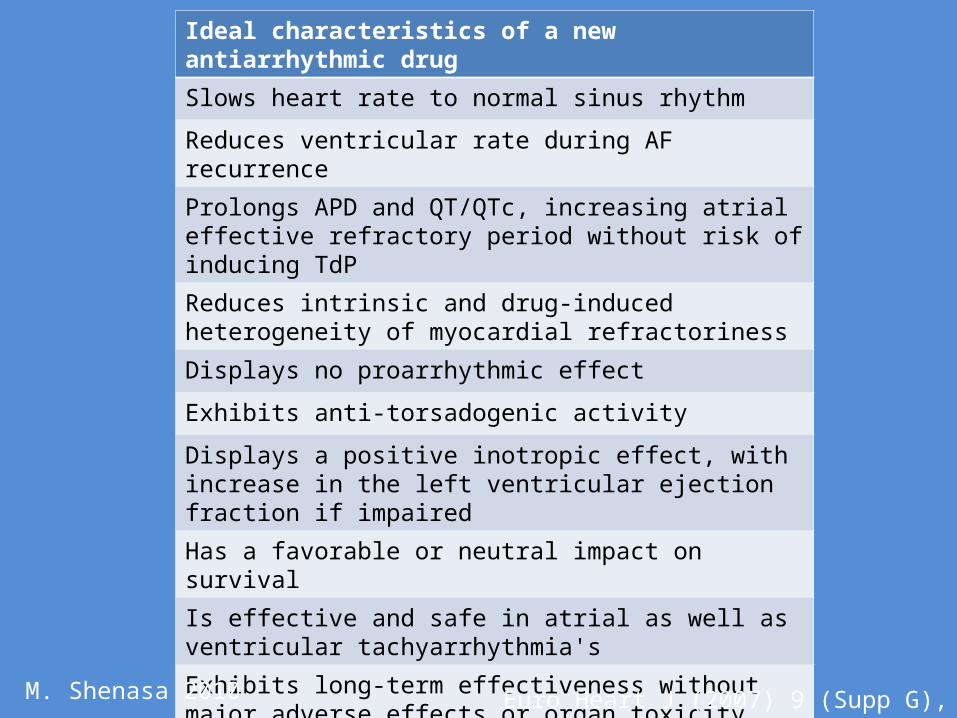
Ideal characteristics of a new antiarrhythmic drug
Slows heart rate to normal sinus rhythm
Reduces ventricular rate during AF recurrence
Prolongs APD and QT/QTc, increasing atrial effective refractory period without risk of inducing TdP
Reduces intrinsic and drug-induced heterogeneity of myocardial refractoriness
Displays no proarrhythmic effect
Exhibits anti-torsadogenic activity
Displays a positive inotropic effect, with increase in the left ventricular ejection fraction if impaired
Has a favorable or neutral impact on survival
Is effective and safe in atrial as well as ventricular tachyarrhythmia's
Exhibits long-term effectiveness without major adverse effects or organ toxicity
Is not incompatible with other frequently used essential cardioactive drugs
Euro Heart J (2007) 9 (Supp G), G17-G25M. Shenasa 2010

Lancet 2006;367:262-72
Atrial Specific Antiarrhythmic Therapy
M. Shenasa 2010
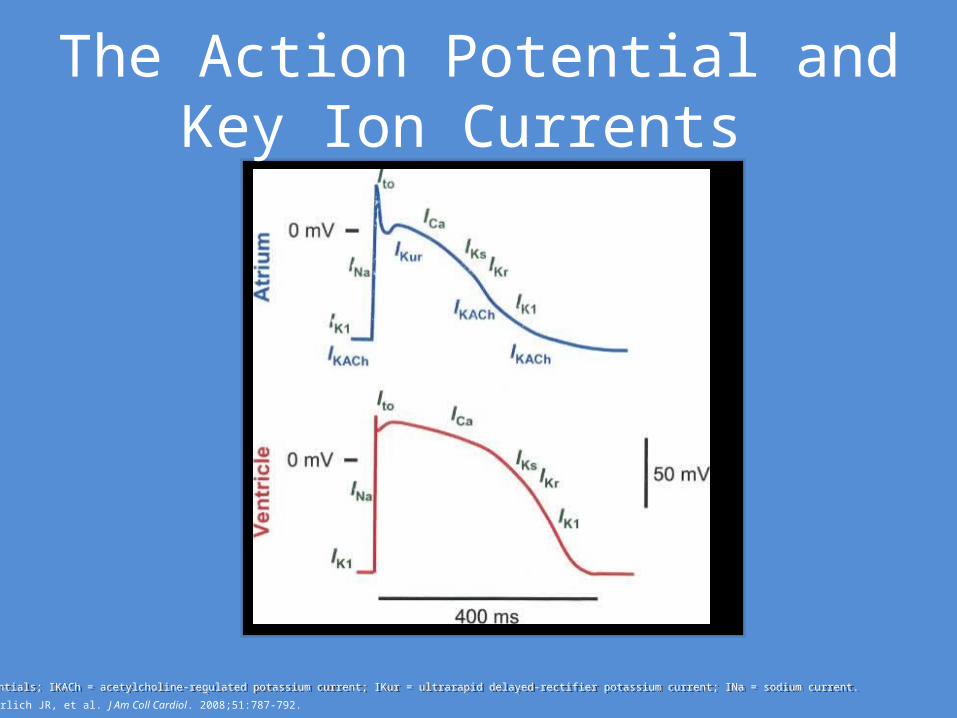
The Action Potential and Key Ion Currents
Ehrlich JR, et al. J Am Coll Cardiol. 2008;51:787-792.
APs = action potentials; IKACh = acetylcholine-regulated potassium current; IKur = ultrarapid delayed-rectifier potassium current; INa = sodium current.APs = action potentials; IKACh = acetylcholine-regulated potassium current; IKur = ultrarapid delayed-rectifier potassium current; INa = sodium current.
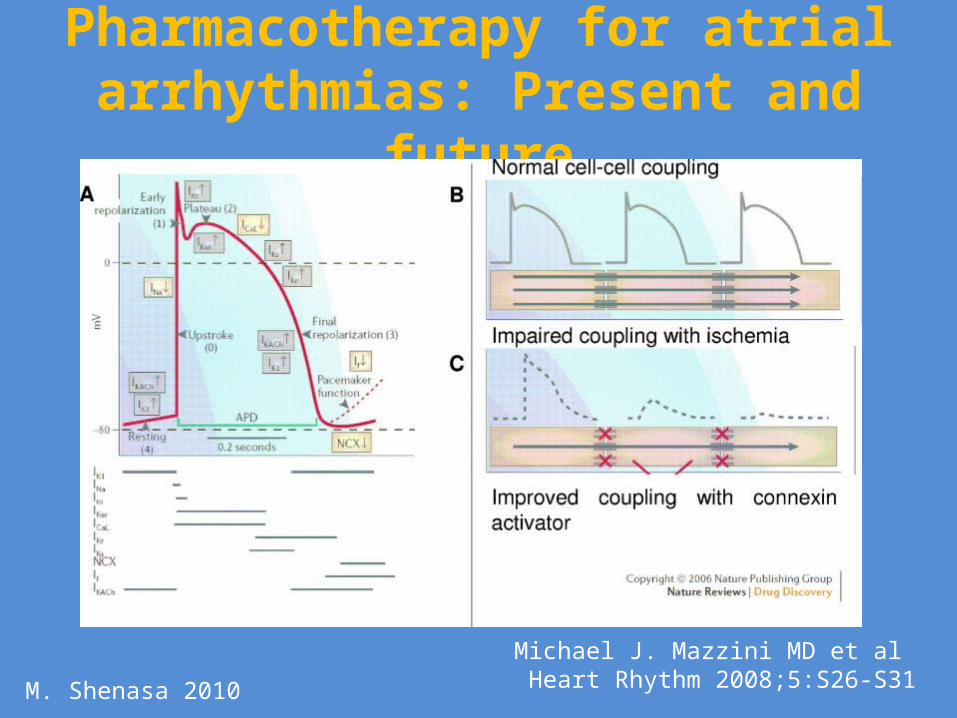
Pharmacotherapy for atrial arrhythmias: Present and future
Michael J. Mazzini MD et al Heart Rhythm 2008;5:S26-S31M. Shenasa 2010
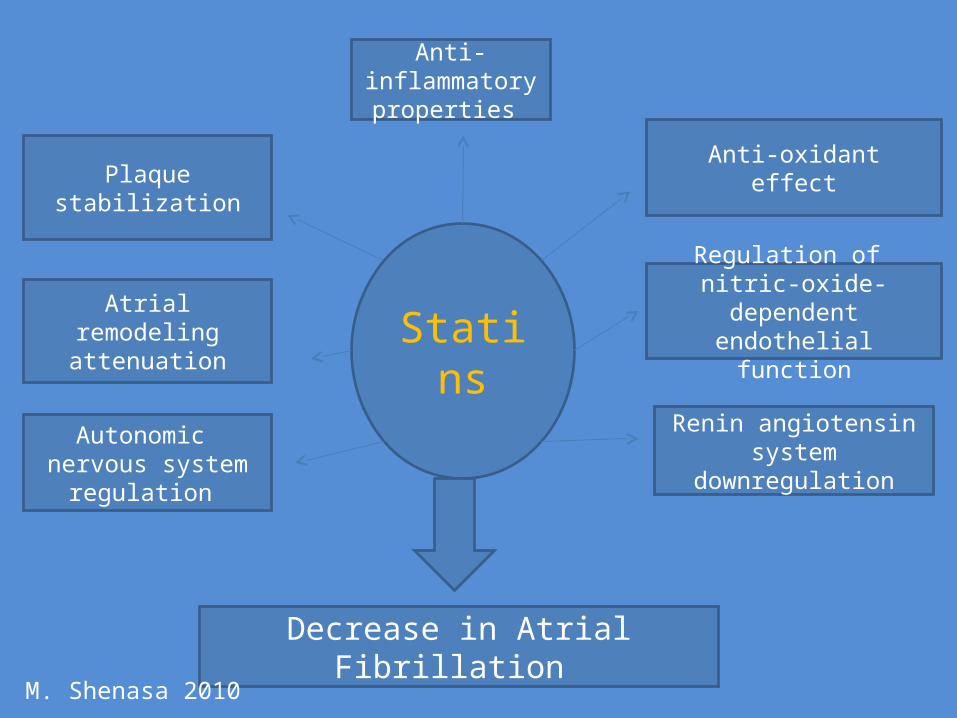
Statins
Renin angiotensin system downregulation
Regulation of nitric-oxide-dependent
endothelial function
Anti-oxidanteffect
Anti-inflammatory properties
Plaquestabilization
Autonomic nervous system
regulation
Atrial remodelingattenuation
Decrease in Atrial Fibrillation M. Shenasa 2010

Ablation of AFCurrent Controversies
• Definition• Cure?• Procedural endpoints• Anticoagulation and Anti arrhythmic therapy post
ablation• Outcomes • Follow ups• Guidelines • Cost
M. Shenasa 2010

AF and Ablation
Haïssaguerre M et al, (N Engl J Med 1998;339;659-66.)
Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins.
M. Shenasa 2010

M. Shenasa 2010

Marine, J. E. JAMA 2007;298:2768-2778.
Pattern of Myocardium on Left Atrium and Pulmonary Veins (PV) and Representative Electroanatomical Map of Left Atrium in Patient Receiving Successful Ablative Therapy
M. Shenasa 2010
Questions?• Why do some patients have numerous paraxsysmol AF
without ever developing persistent forms, while other progress to sustained forms of AF within a short time?
• If muscle sleeves are present in the pulmonary veins in everyone, why do some develop AF and other do not?
• Does a “natural” functional electrical block between pulmonary veins and the left atrial myocardium exist, and would this protect against AF?
• Why does “focal” AF develop at age 30 in one patient and age 70 in another?
• Why do periods of frequent AF paroxysms alternate in unpredictable patterns with periods of sinus rhythm in most patients?
M. Shenasa 2010

Catheter-Based Management of AF
Valderrabano, M JMDHC 2;2007:24-29M. Shenasa 2010

Courtesy of U.Penn
AF and Ablation
M. Shenasa 2010
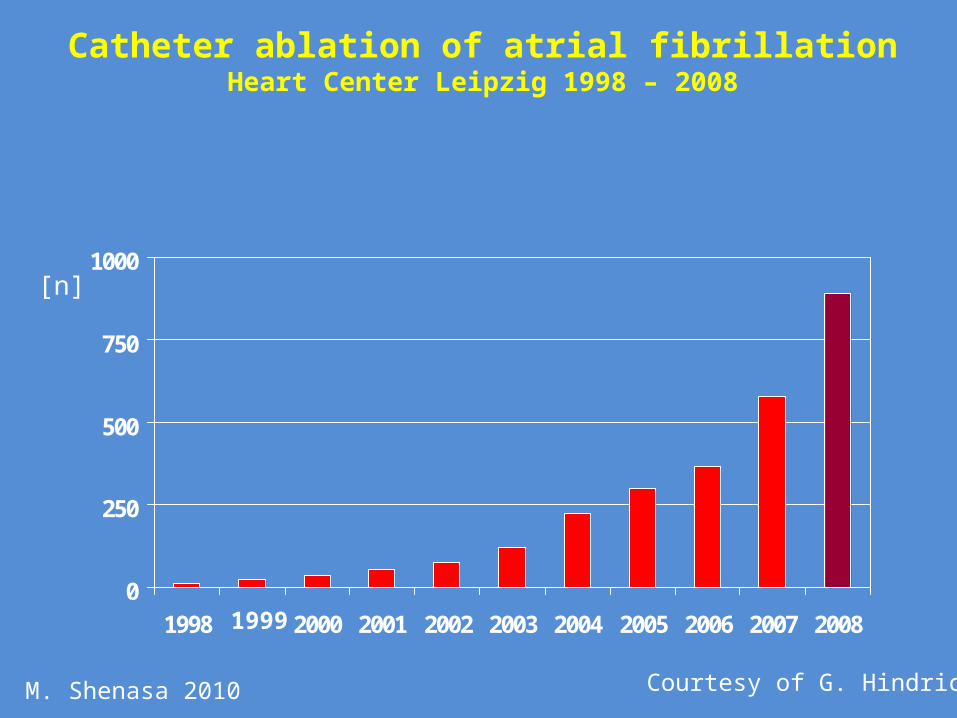
Catheter ablation of atrial fibrillationHeart Center Leipzig 1998 – 2008
[n]
0
250
500
750
1000
1998 2000 2001 2002 2003 2004 2005 2006 2007 20081999
Courtesy of G. HindricksM. Shenasa 2010

AF and AblationPlumonary vein Ablation in Atrial Fibrillation
Hype or Hope?Hein Wellens
Circ:2000;102:2562-2564
Circumferential Radiofrequency Ablation of Pulmonary Vein Ostia
A New Anatomic Approach for Curing Atrial Fibrillation Carlo PapponeCirc:2000;102:2619-2628
Controversies In Cardiovascular Medicine Should atrial fibrillation ablation be considered first-line therapy fow some patients?
(Circulation 2005; 112:1231)

Criteria for patient selection
1. Patients’ expectations: symptom relief, freedom from anticoagulation, freedom from antiarrhythmic therapy, resolution of tachycardia-induced myopathy
2. Failure of prior antiarrhythmic therapy or prior procedures
3. Pattern of atrial fibrillation: paroxysmal vs. chronic4. Presence of structural heart disease: left atrial size,
left ventricular dysfunction, hypertrophic cardiomyopathy
5. Duration of atrial fibrillation
Valderrabano, M JMDHC 2;2007:24-29M. Shenasa 2010
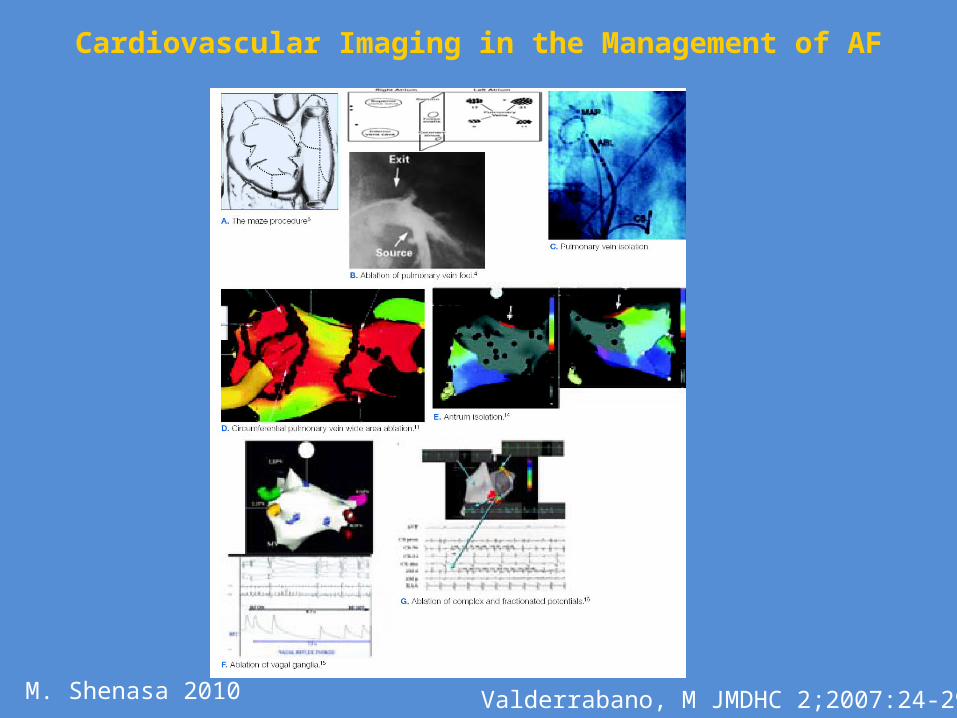
Cardiovascular Imaging in the Management of AF
Valderrabano, M JMDHC 2;2007:24-29M. Shenasa 2010

Future Trials in AFibCABANA
( Catheter Ablation versus Anti-Arrhythmias Drugs for Afib)
NIH sponsored Multicenter /Randomized Comparing catheter ablation with rhythm control
therapy Endpoints: Afib recurrences and Mortality
outcomes
M. Shenasa 2010
Catheter Ablation versus Antiarrhythmic Drug Therapy for Atrial Fibrillation
(CABANA)• Randomized trial comparing ablation to best drug therapy
(rate or rhythm control)• 1⁰ endpoint: mortality (powered for 30% mortality reduction
assuming 12% 3-year mortality in drug group)• 2 ⁰ endpoint: QOL, AF recurrence, composite MAE• Enrollment criteria: age ≥ 65 years, or <65 years with ≥ 1 risk
factor for stroke • Ablation technique to include PVI ± additional procedures
(lines, CFAE, focal triggers) • Planned 3,000 patients, 120 enrolling centers• Pilot phase completed 2008, full study started fall 2009
M. Shenasa 2010


Future Development in AF Ablation
• Mapping and Imaging• Remote Catheter Navigation• Molecular Imaging • Genetic Engineering • Stem Cell Therapy• Energy Source
– Laser, Radiation, Ultrasound • Eventually noninvasive mapping and ablation
M. Shenasa 2010

Genetics of AF
• Familial AF: KCNQ1 gene– Familial auricular fibrillation reported by Wolff, L,
1943• Nonfamilial AF: KCNE1• Genes of potassium: KCNE1• Genes of sodium channel subunits: SCN5A• Genes of sarcoplasmic reticulum calcium ATPase:
SERCA2• Renin-angiotensin system: RAS• Genes related to inflammation
JACC 2008;52:241-50M. Shenasa 2010

• ACC/AHA/ESC 2006 Guidelines for the Management of Patients With Atrial Fibrillation.
• HRS/EHRA/ECAS Expert Consensus Statement on Catheter and Surgical Ablation of Atrial Fibrillation: Recommendation for Personnel, Policy, Procedures and Follow-up
Fuster, V: Circulation, Aug 2006; 114: e257 - e354.
Calkins H, et al Heart Rhythm 2007;4:816-861
M. Shenasa 2010

Cardiology Clinics 2009; 27:201-216M. Shenasa 2010

Management Decision in AF
AblationAblationAntiarrhythmic
Antiarrhythmic
Rate ControlRate ControlRate ControlRate Control
AnticoagulationAnticoagulation
M. Shenasa 2010
Conclusion• All Atrial Fibrillation patients are not the same. • Atrial Fibrillation is not a disease. It is a
symptom like fever, syncope and etc. • Atrial Fibrillation should be treated based on
etiologies rather than mechanisms. • Prevention should be the first line of therapy.
Most importantly focusing on fibrosis and inflammation.
M. Shenasa 2010

Thank you
M. Shenasa 2010
Stroke and AFHeart Disease and Stroke
• Stroke affects about 795,000 individuals annually in the US only.
• 1 every 40 seconds.• Third leading cause of death• Number 1 cause of disability• 87% are ischemic stroke i.e. embolic• 13% are hemorrhagic stroke• 1 in 15 people develop brain aneurysm in their life• Ruptured aneurysm are 30,000 cases of hemorrhagic
stroke. • Silent stroke cognitive decline, dementia and
Alzheimer's are associated with AFM. Shenasa 2010

Wish list for the next mapping system
• Enough reality of correct anatomical representation
• Ability to incorporate ablation catheter into anatomy
• Real-time• Lesion quantification • Reduce radiation exposure • Increase success rate• Ultimate imaging is Visual imaging • Technology begets technology like an arm race
M. Shenasa 2010
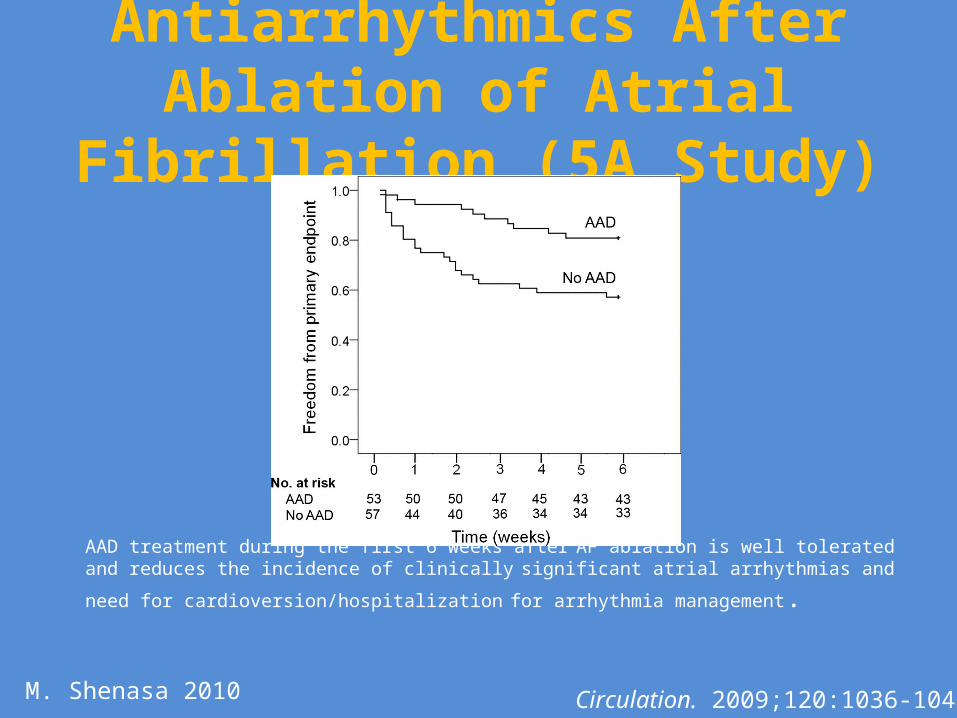
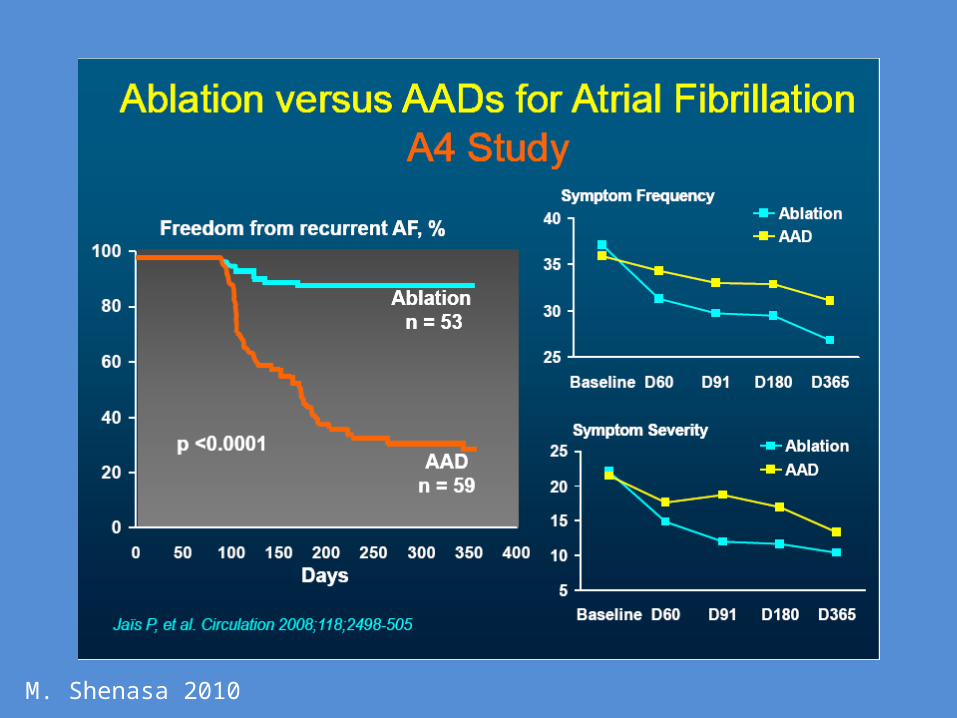
Antiarrhythmics After Ablation of Atrial Fibrillation (5A Study)
AAD treatment during the first 6 weeks after AF ablation is well tolerated and reduces the incidence of clinically significant atrial arrhythmias and need for
cardioversion/hospitalization for arrhythmia management.
Circulation. 2009;120:1036-1040M. Shenasa 2010
M. Shenasa 2010
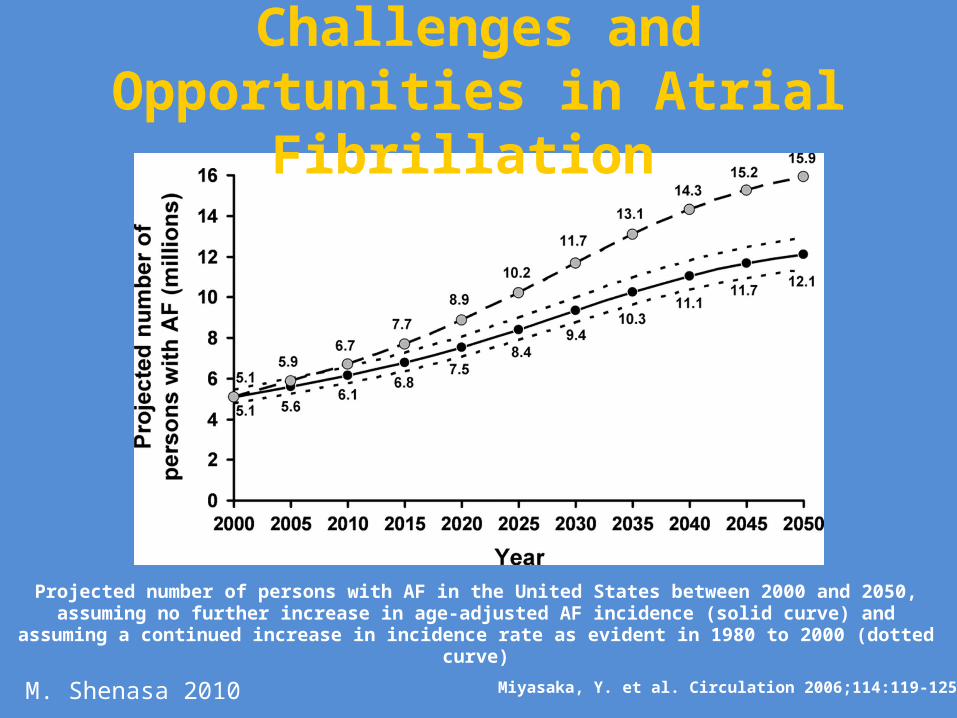
Miyasaka, Y. et al. Circulation 2006;114:119-125
Projected number of persons with AF in the United States between 2000 and 2050, assuming no further increase in age-adjusted AF incidence (solid curve) and assuming
a continued increase in incidence rate as evident in 1980 to 2000 (dotted curve)
Challenges and Opportunities in Atrial Fibrillation
M. Shenasa 2010
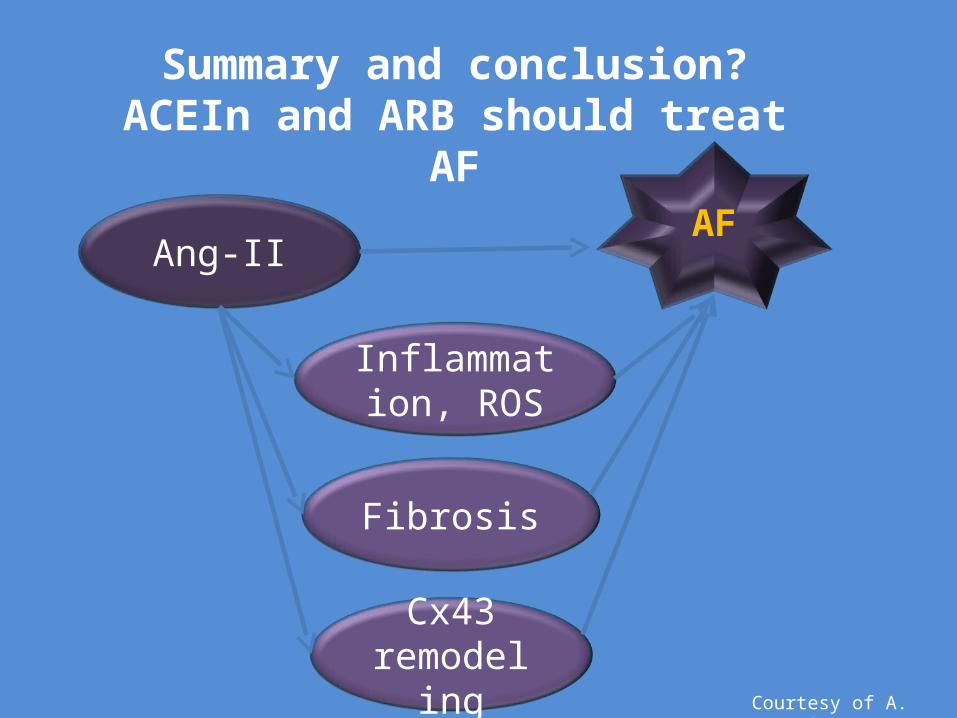
Fibrosis
Inflammation, ROS
Cx43 remodeling
Ang-IIAF
Summary and conclusion?ACEIn and ARB should treat AF
Courtesy of A. Sovari
Best therapy is the one that is not needed

Ideal antiarrhythmic drug
• Completely safe• Completely effective• Fun and easy to take• Makes you live longer • Cheaper than aspirin
Immortilide for arrhythmias
Take one per life time
M. Shenasa 2010
Raman, S. V. J Am Coll Cardiol 2010;55:91-96
AF and Atrial Fibrosis
M. Shenasa 2010

Angiotensin II-dependent cellular signalling via type 1 and type 2 receptors.
Goette A , Lendeckel U Europace 2008;10:238-241
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author 2008. For permissions please email: [email protected]

Gap Junctions
Gap junctions are intercellular channels some 1.5–2 nm in diameter. These permit the free passage between the cells of ions and small molecules (up to a molecular weight of about 1000 daltons). They are constructed from 4 (sometimes 6) copies of one of a family of a transmembrane proteins called connexins. Because ions can flow through them, gap junctions permit changes in membrane potential to pass from cell to cell
M. Shenasa 2010
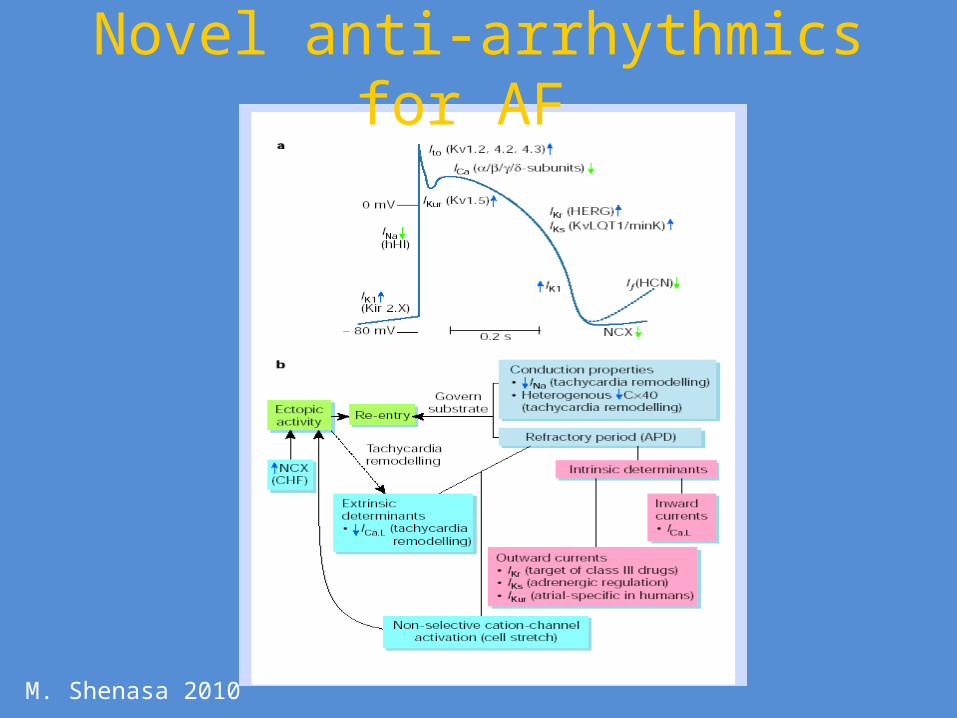
Novel anti-arrhythmics for AF
M. Shenasa 2010
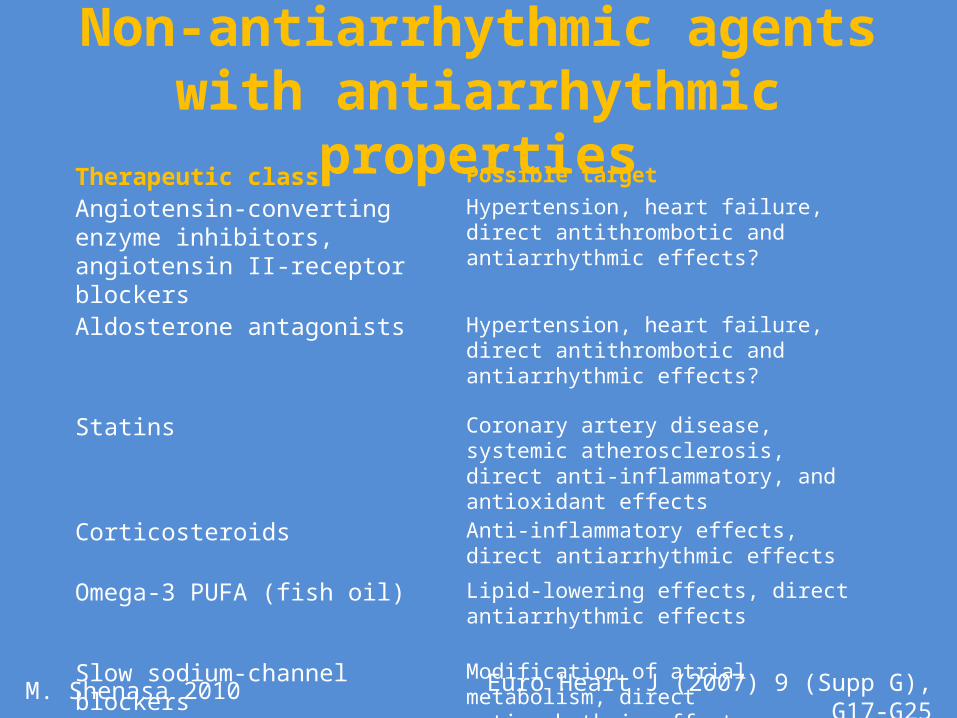
Non-antiarrhythmic agents with antiarrhythmic properties
Therapeutic class Possible target
Angiotensin-converting enzyme inhibitors, angiotensin II-receptor blockers
Hypertension, heart failure, direct antithrombotic and antiarrhythmic effects?
Aldosterone antagonists Hypertension, heart failure, direct antithrombotic and antiarrhythmic effects?
Statins Coronary artery disease, systemic atherosclerosis, direct anti-inflammatory, and antioxidant effects
Corticosteroids Anti-inflammatory effects, direct antiarrhythmic effects
Omega-3 PUFA (fish oil) Lipid-lowering effects, direct antiarrhythmic effects
Slow sodium-channel blockers Modification of atrial metabolism, direct antiarrhythmic effect
Euro Heart J (2007) 9 (Supp G), G17-G25M. Shenasa 2010

Concepts to Consider
• Selective ion channel blocker• Multi-channel blockade (like amiodarone)• Atrial channel selective (usually “relative”)• Substrate based
– Gap junction conduction– Fibrosis– Inflammation
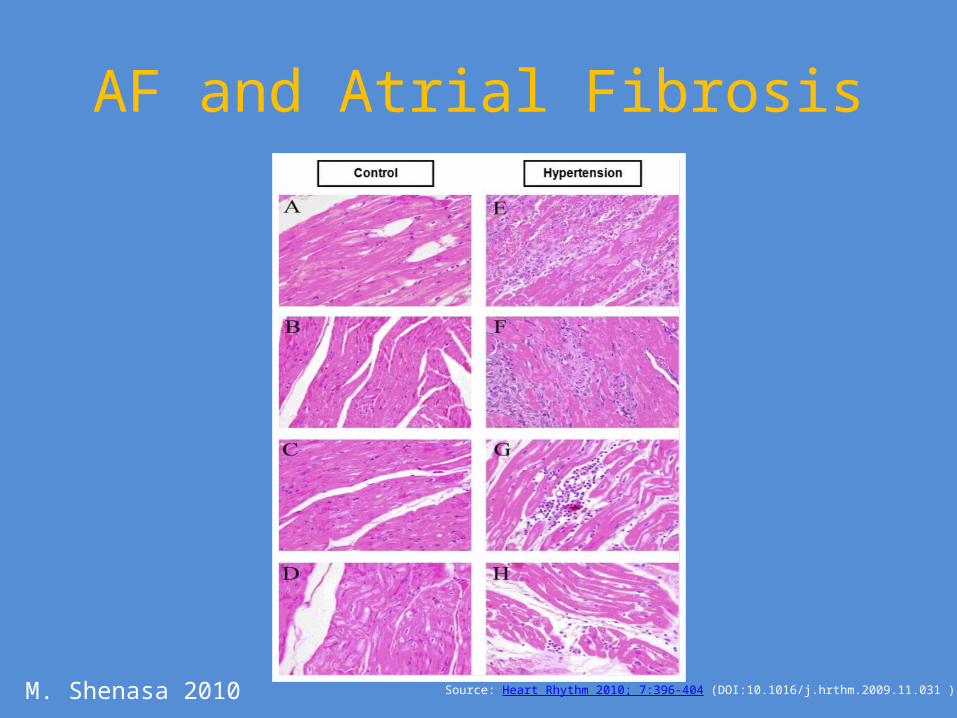
Source: Heart Rhythm 2010; 7:396-404 (DOI:10.1016/j.hrthm.2009.11.031 )
AF and Atrial Fibrosis
M. Shenasa 2010
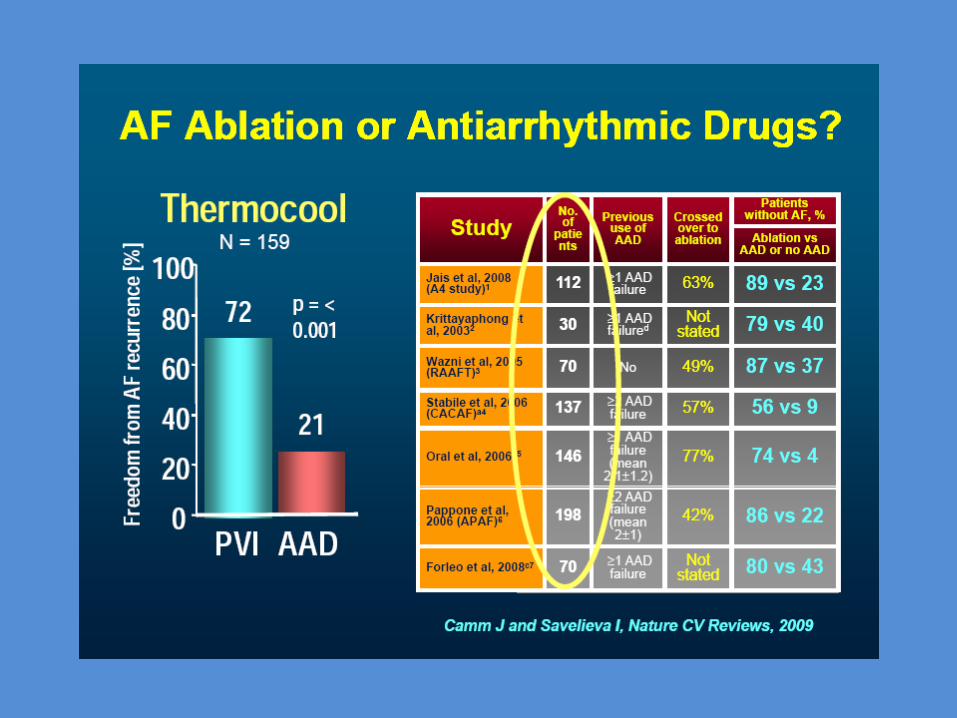

Comparison of Antiarrhythmic Drug Therapy and Radiofrequency Catheter Ablation in Patients With
Paroxysmal Atrial Fibrillation A Randomized Controlled Trial
David J. Wilber MD et alJAMA 2010;303(4)333-340

Patient Flow Diagram
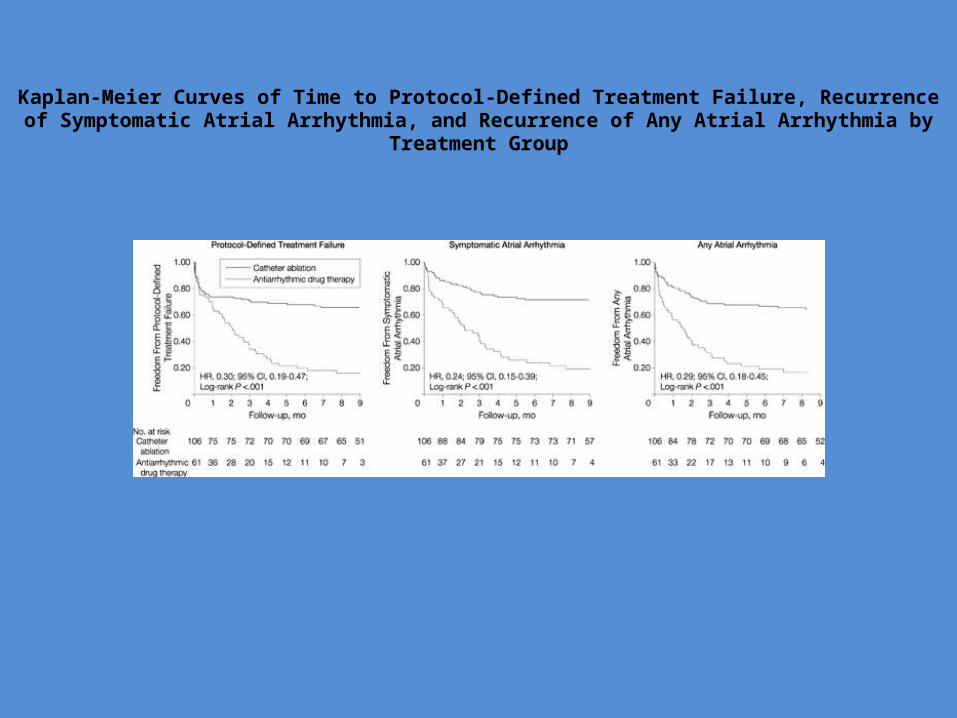
Kaplan-Meier Curves of Time to Protocol-Defined Treatment Failure, Recurrence of Symptomatic Atrial Arrhythmia, and Recurrence of Any Atrial Arrhythmia by Treatment Group

Conclusion
• Among patients with paroxysmal AF who had not responded to at least 1 antiarrhythmic drug, the use of catheter ablation compared with ADT resulted in a longer time to treatment failure during the 9-month follow-up period.
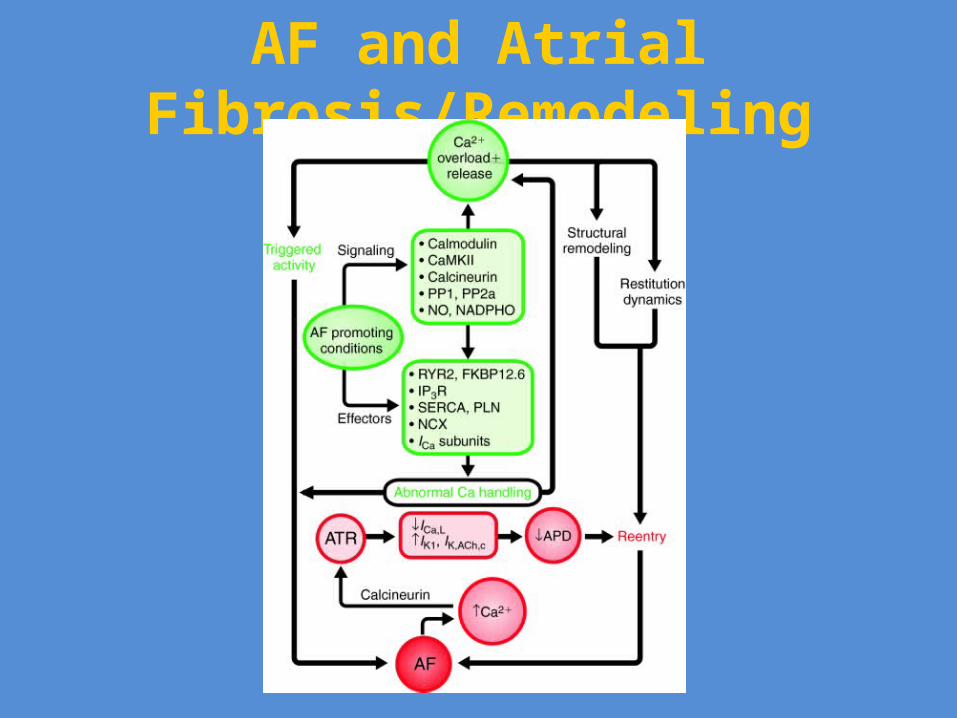
AF and Atrial Fibrosis/Remodeling
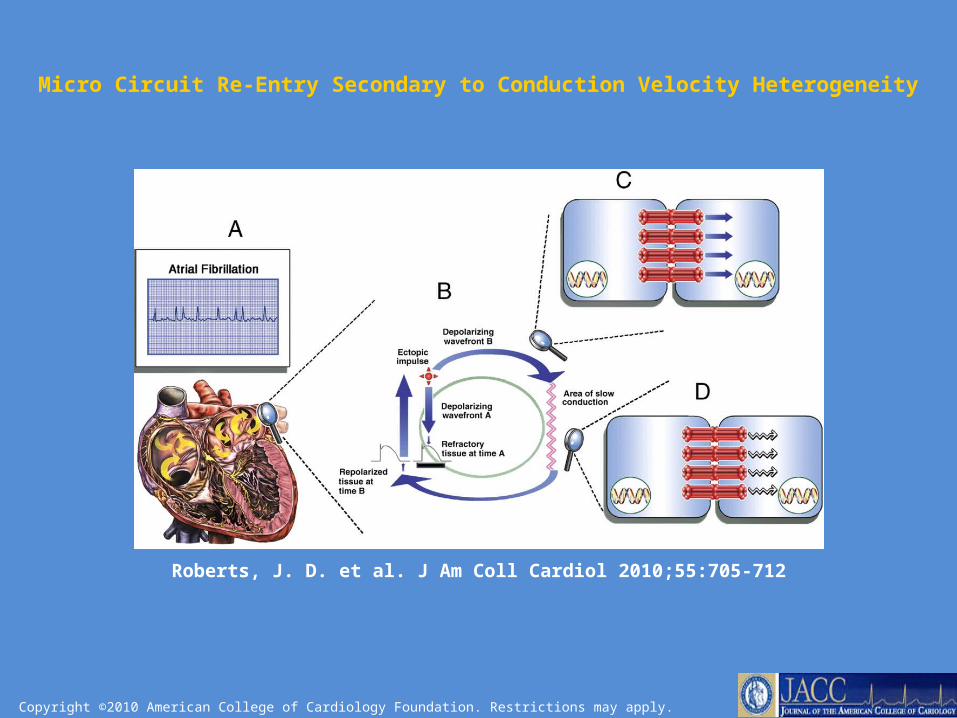
Copyright ©2010 American College of Cardiology Foundation. Restrictions may apply.
Roberts, J. D. et al. J Am Coll Cardiol 2010;55:705-712
Micro Circuit Re-Entry Secondary to Conduction Velocity Heterogeneity
Future Trials in AFib
CABANA ( Catheter Ablation versus Anti-Arrhythmias Drugs
for Afib)NIH sponsored Multicenter /Randomized Comparing catheter ablation with rhythm control
therapy Endpoints: Afib recurrences and Mortality
outcomes
The true prevalence of Asymptomatic “Silent” Atrial Fibrillation by its nature is unknown.
The interest in Silent Afib is emerging from symptomatic patients who are now closely followed after device implantations or ablative procedures.
It is estimated that the asymptomatic Afib are at least 6 folds greater than the symptomatic rate.
Cessation of anticoagulation in patients presumed to be in sinus rhythm associated with increased risk of stroke and death in the AFFIRM Trial.
What to do with silent Afib ( Asymptomatic)
Rhythm or Rate Control in Atrial Fibrillation
Evidence base5 prospective, controlled, randomized trials comparing 2
different strategies • PIAF: Pharmacological Interventions in Atrial Fibrillation • STAF: Strategies in Atrial Fibrillation ( pilot)• AFFIRM: Atrial Fibrillation Follow-up Investigation of Rhythm
Management• RACE: Rate Control versus Electrical Cardioversion of Atrial
Fibrillation • SAFE-T: Sotalol and Amiodarone for Effectiveness Trial

AFFIRM Trial• Atrial Fibrillation Follow-up Investigation of Rhythm
Management (AFFIRM)
• Sponsored by National Heart, Lung, and Blood Institute of the National Institutes of Health
• Randomized evaluation of treatment of AF by 1 of 2 strategies (rate control versus rhythm control and anticoagulation)
• Total of 4,160 patients followed for an average of 2.6 years

Nademanee, K. et al. J Am Coll Cardiol 2008;51:843-849
Can Sinus Rhythm Improve Survival?
Effects of Maintaining NSR After AF Ablation on Survival
Future Directions • Inflammation and AF• Fibrosis and AF• Genetics of AF• Role of Stem Cell in AF• Targeted therapy for AF i.e. anti-inflammatory, anti-
fibrosis • Development of atrial selective channel blockers• Upstream therapies i.e. ARB, ACE, Omega-3, and
statins• Patient Outcome and follow up

Future Directions Upstream TherapiesNon-antiarrhythmic
Omega-3 Fatty Acids and Cardiac Arrhythmias: Prior Studies and Recommendations for Future Research. A report from the National Heart, Lung, and Blood Institute and Office of Dietary Supplements Omega-3 Fatty Acids and Their role in Cardiac Arrhythmogenesis Workshop
Circulation 2007;116:e320-e335

Role of Inflammation in Initiation Perpetuation of Atrial Fibrillation
1.) Increased CRP levels2.) Hypercoagulapathy 3.) HMG-CoA4.) Statins 5.) Fish oil , Omega-3 and Vitamin C 6.) ACE and ARB7.) Glucocorticoids8.) Aldosterone blocking agents
Issac TT et al., JACC 2007;50:2021-8

Multimodality imaging plays an important role in the evaluation of atrial fibrillation patients, and in the management of atrial fibrillation.
Tops L F et al. Eur Heart J 2010;31:542-551
Unanswered Questions in AF Ablation
• Catheter ablation of paraxsysmol AF has the best outcome compared to permanent AF ablation: 80% (success rate 1 year) vs. 50%, particularly in a low risk population
• Image guidance • Balloon Cryoablation • Balloon-Based High-Intensity Focused Ultrasound ablation • Safety of AF Ablation• Continuation of anti-coagulation • Follow up and success rate, problem of silent recurrences

Future Development in Afib Ablation
• Mapping and Imaging• Remote Catheter Navigation• Molecular Imaging • Genetic Engineering • Stem Cell Therapy• Energy Source
– Laser, Radiation, Ultrasound • Eventually noninvasive mapping and ablation


Wellens, H
General Mechanisms of AF
1.) Multiple rapidly discharging foci2.) Focal sources with fibrillatory conduction3.) Multiple re-entrant circuit

AF and Atrial Fibrosis/Remodeling
The Future cardiac mapping/imaging would offer multi-modality virtual imaging including:
1.) Nuclear Perfusion and Functional Scans2.) Rotational Angiography3.) Structural, Functional, Coronary and Perfusion
Magnetic Resonance Imaging4.) Ultra Fast Computerized Tomography 5.) Neurocardiac Imaging 6.) 3-4 Dimensional Echocardiography7.) 3-D Biosense Electromagnetic Mapping8.) Intracardiac/Intravascular Ultrasound9.) Optical Coherence Tomography

Cardiac Mapping and EP in 2010
1.) In vivo optical mapping2.) Cardiac MR Spectroscopy3.) Laser Optical Spectroscopy4.) Near Infrared Spectroscopy5.) Molecular Imaging6.) Fluorescence Imaging7.) Genetic Engineering and Drug Delivery 8.) Biological Pacemakers 9.) Stem Cell Imaging

The Future of Atrial Fibrillation Ablation 1/2
1. Optical Mapping 2. Bioluminescence3. Diffused Optical Spectroscopy4. Magnetic Resonance Imaging5. Magnetic Resonance Spectroscopy (only
noninvasive)6. Diffusion Tensor Imaging7. Fiber Tracking8. Multimodality Mapping and Ablation
The Future of Atrial Fibrillation Ablation 2/2
9. Image Integration and Fusion10. CT Integration with Electroanatomical Mapping11. CT with rotational angiography 12. PET/CT integration 13. Intracardiac Echo14. Electro anatomical Mapping15. High intensity ultrasound mapping16. One-Stop Shop (integration of all multimodality
techniques)
Nattel S; Nature Vol 415, 2002

The History of Atrial Fibrillation: The Last 100 Years
ERIC N. PRYSTOWSKY, M.D.J Cardiovasc Electrophysiol, Vol. 19,
pp. 575-582, June 2008.


Fye W. N Engl J Med 2006;355:1412-1414
A Volunteer Sitting with His Arms in Saline-Filled Tubs with Wires Connected to Einthoven's Electrocardiograph
Fye W. N Engl J Med 2006;355:1412-1414
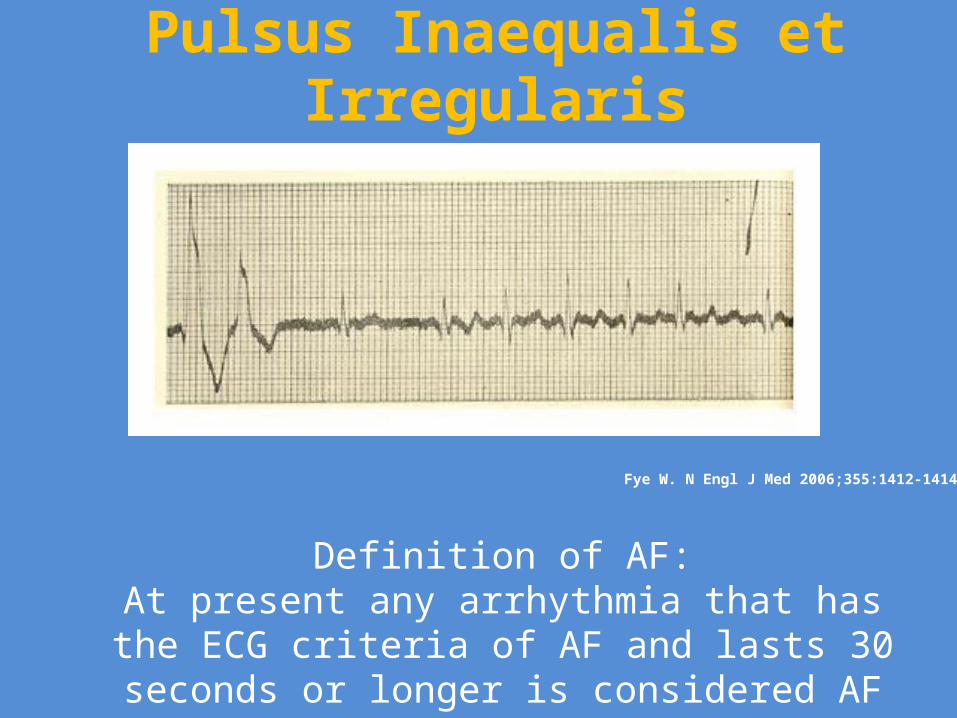
Pulsus Inaequalis et Irregularis
Definition of AF:At present any arrhythmia that has the ECG criteria of
AF and lasts 30 seconds or longer is considered AF

Heterogeneous conduction
Increased fibrosis
Triggered activity
Altered atrial refractoriness
Volume + pressure overload
Loss of atrial contraction
R-R variability
RapidVentricular rate
-energy depletion-Remodeling
-Ischemia-Abnormal Ca⁺
handling
AF
Heart failure
Heart Failure and AF

Camm, J

• Each year: – 795,000 new or recurrent stroke– 610,000 first attacks– 185,000 recurrent attacks
Circ 2010:121:9480954
Stroke and AFHeart Disease and Stroke: 2010

Stroke and AFHeart Disease and Stroke: 2010
• National Health and Nutrition Examination Survey– 2003-2006: 33.6% of US adults ≥ 20 years of age
have hypertension – 74,500,000 US adults with hypertension
• Hypertensive adults:– 78% are aware of condition – 68% using antihypertensive medications – 44% treated had their hypertension controlled
Circ 2010:121:9480954

Stroke and AFHeart Disease and Stroke: 2010
• Total serum cholesterol levels ≥ 240 mg/dL• 2006:• 17,200,000 diagnosed with diabetes , 7.7% of
the adult population • 6,100,000 undiagnosed diabetes • Paraxsysmol AF carries the same risk stroke as
persistent or permanent AF

Stroke and AFHeart Disease and Stroke: 2010
• Prevalence of overweight and obesity in the US adults (≥20 years of age) is 144,100,000
• 66.3% in 2006• 32.9% of US adults are obese• Children ages 2-19• 31.9% overweight and obese (23,500,000
children) • 16.3% are obese (12,000,000)
Circ 2010:121:9480954
Stroke and AFHeart Disease and Stroke: 2010
• Current usage of cardiovascular surgical and invasive procedures
• Operations and procedures increased • 33% from 5,444,000 to 7,235,000 annually• Total direct and indirect cost of CVD and stroke in the US for
2010 is estimated to be $503.2 billion – Cancer and benign neoplasms $228 billion – $93 billion in direct costs – 19billion in morbidity indirect
– $116 billion in mortality indirect
Circ 2010:121:9480954
Stroke and AFHeart Disease and Stroke
• Stroke affects about 795,000 individuals annually in the US only.
• 1 every 40 seconds.• Third leading cause of death• Number 1 cause of disability• 87% are ischemic stroke i.e. embolic• 13% are hemorrhagic stroke• 1 in 15 people develop brain aneurysm in their life• Ruptured aneurysm are 30,000 cases of hemorrhagic
stroke. • Silent stroke cognitive decline, dementia and
Alzheimer's are associated with AF

Role of inflammation and oxidative stress in AF
• Concentrations of inflammatory biomarkers were significantly increased in patients with AF and supports a strong association between AF and inflammation. Elevated inflammatory markers in patients with lone AF suggest that inflammation is associated with AF independent of comorbidities such as heart failure.
Heart Rhythm 2010;7:438-444
AF and Atrial Fibrosis/Remodeling

Kirchhof, P. et al. Eur Heart J 2009 30:2969-2980; doi:10.1093/eurheartj/ehp235

Silent Cerebral Infarction in Patients with Nonrheumatic Atrial Fibrillation • Silent cerebral infarction is frequently seen in
asymptomatic patients with AF. • Silent AF carries the same risk of stroke as
symptomatic AF.
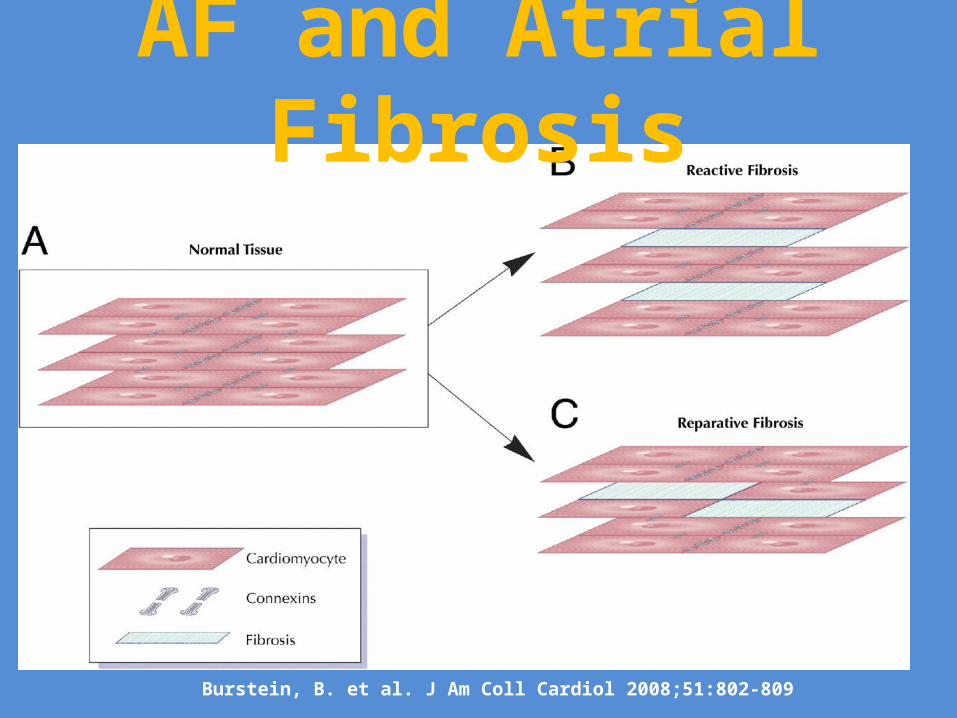
Burstein, B. et al. J Am Coll Cardiol 2008;51:802-809
AF and Atrial Fibrosis
Burstein, B. et al. J Am Coll Cardiol 2008;51:802-809
AF and Atrial Fibrosis

Roberts, J. D. et al. J Am Coll Cardiol 2010;55:705-712
Effect of Ion Channels on Atrial APD

AF and Ablation
Two Different sources of ectopy
Haïssaguerre, M Circ.2000;101:1409-1417

The role of imaging in AF ablation 1/3
EHJ 2010;31:542-551
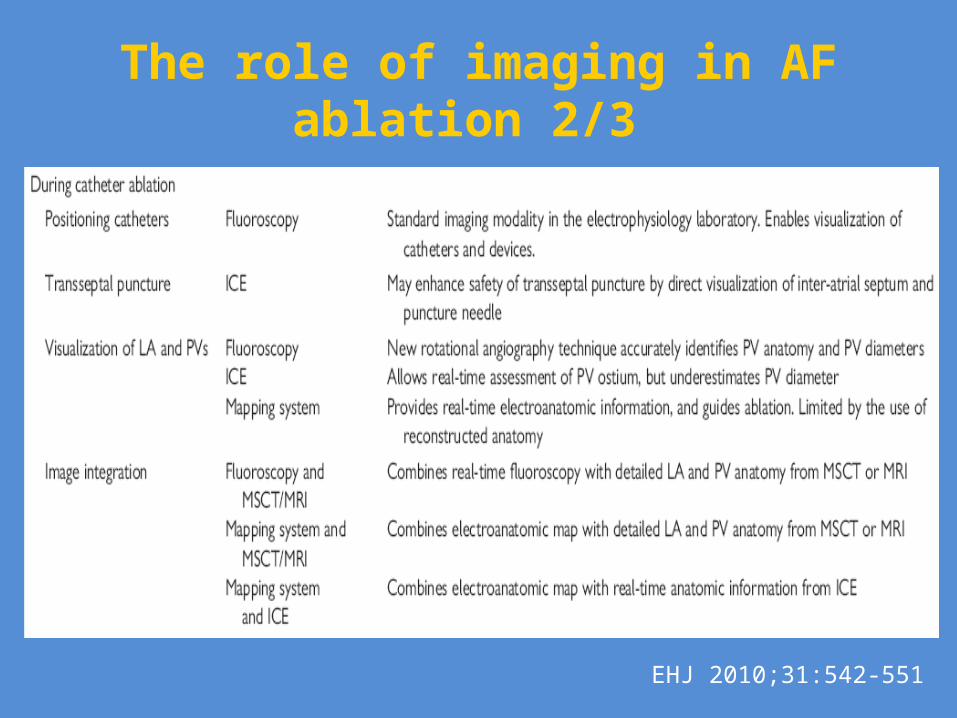
The role of imaging in AF ablation 2/3
EHJ 2010;31:542-551

The role of imaging in AF ablation 3/3
EHJ 2010;31:542-551

In whom and when can antiarrhythmic drug therapy be discontinued?
• Antiarrhythmic drug discontinuation may be reasonable in patients in whom concomitant conditions have been successfully treated or in whom prominent triggers have been eliminated.
• The problem remains with silent AF.

Inflammation and AFMarkers for inflammation
1.) High Sensitivity C-reactive protein (hs-CRP)2.) Interleukin (IL)-63.) White cell count4.) Tumor necrosis factor alpha (TNFα)Others Cause of inflammation • Oxidative Stress• Endothelial dysfunction • Coexisting co-morbid risk factors & others

Heart Failure and AF• High atrial rates particularly in
the presence of HF enhances Ca²+ influx which in term enhances in activation voltage dependent L-type Ca²+ channels

Stroke and AFHeart Disease and Stroke: 2010
• 2010: estimated 785,000 Americans will have a new coronary attack
• 470,000 will have a recurrent attack• 195,000 silent first myocardial infarctions/year• 25 seconds: American will have a coronary event • 1 minute: someone will die• Third cause of death• First cause of disability• Silent stroke will cause silent AF
Circ 2010:121:9480954

Atrial Fibrillation:Past, Present and Future II

Roberts, J. D. et al. J Am Coll Cardiol 2010;55:705-712


M. Shenasa 2010


Milestones in the management of Atrial Fibrillation
• Awareness of prognostic implications of AF• Prevention of thromboembolic strokes• Comparison of rate versus rhythm control
strategies• Catheter ablation to cure AF• New antiarrhythmic agents • Improving outcomes in AF
M. Shenasa 2010

Milestones in the management of AF• AF begets AF ( M. Allessi)• Moe GK: Atrial Fibrillation as a self-sustaining
arrhythmia independent of focal discharge. Am Heart J 1959;58:59-70
• Atrial remodeling • Left atrial isolation and Maze procedure (Cox)• Guiraudon corridor procedure (1985)• Tachycardia induced cardiomyopathy • AF ablation (M. Haissaguerre, NEJM 1998)• Role of Atrial fibrosis • Development of Atrial selective anti-arrhythmics • Percutaneous atrial appendage closure (Watchmen
device) M. Shenasa 2010

Cardiology Clinics 2009; 27:79-93
Heart Failure and AF
M. Shenasa 2010

Cumulative incidence of primary and secondary outcomes in treatment of Dronedarone with Placebo
M. Shenasa 2010 NEJM 2009;360:668-78.
M. Shenasa 2010
History of Atrial FibrillationScientific Era
• William Stokes (1854)• Wenckebach (1904)• Mackenzie (1907)• Sir Thomas Lewis (1909-1910) described details
of AF and reentry• Gordon Moe (1959) described the computer
model of multi-wavelet of reentry; Am Heart J 1946:67:200-20.
• Lown and colleagues (1962) first cardioversion for AF
M. Shenasa 2010
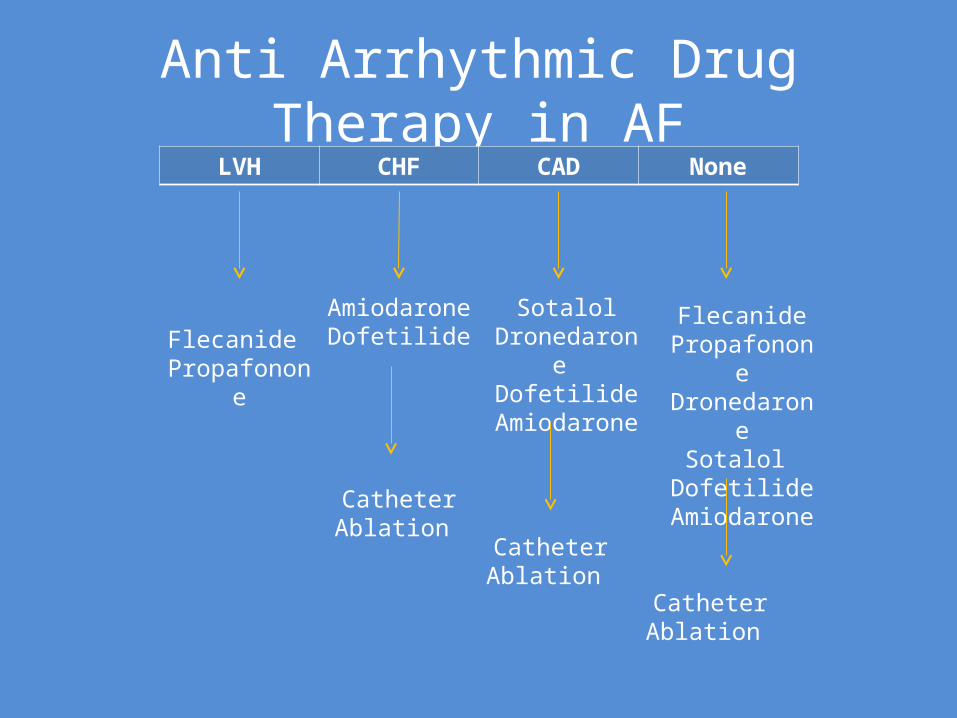
Anti Arrhythmic Drug Therapy in AFLVH CHF CAD None
Flecanide Propafonone
Amiodarone Dofetilide
Catheter Ablation
SotalolDronedarone
DofetilideAmiodarone
Catheter Ablation
FlecanidePropafononeDronedarone
Sotalol Dofetilide
Amiodarone
Catheter Ablation