Atopic Eczema 2

of 27
-
Upload
pierre-charles-wood -
Category
Documents
-
view
222 -
download
0
Transcript of Atopic Eczema 2
-
8/8/2019 Atopic Eczema 2
1/27
Childhood
ECZEMANICE
Guidelines 2007
Dr Ellie Day (ST5 Paediatrics)
July 16th 2010
Royal Surrey County Hospital
-
8/8/2019 Atopic Eczema 2
2/27
Definition
General term for skin inflammation
Chronic inflammatory itchy skin condition characterisedby:
pruritus dry, scaly skin
erythema
swelling, cracking, weeping, crusting
lichenification
superadded infections
Relapsing & Remitting course
Flare ups
-
8/8/2019 Atopic Eczema 2
3/27
Pathophysiology
Normal skin has a high water content and is flexible andelastic
epidermis provides barrier function
stratum corneum contains layers of lipid
In Eczema, skin barrier function is disturbed water is more readily able to evaporate
stratum corneum cells dry out & shrink
cracks appear and act as portal of entry
Evidence suggests genetic component resulting in skin
barrier breakdown
8/10 children where both parents have eczema
Pathophysiology still poorly understood
likely multifactoral
-
8/8/2019 Atopic Eczema 2
4/27
Statistics
Usually occurs before the age of 5 Adult onset possible but uncommon
1 in 6 UK school age children have eczema
2 out of 3 children will outgrow it by teenage years
1 in 20 adults have it
Affects all races
Ratio 1:1.4 (male to female)
Has significant morbidity
Incidence and prevalence on the rise climate change pollution
allergies
diet
-
8/8/2019 Atopic Eczema 2
5/27
Atopic Eczema
May occur with other atopic diseases;
asthma
allergic rhinitis
acute allergic reactions to food urticaria
-
8/8/2019 Atopic Eczema 2
6/27
Differential Diagnoses
Seborrheic dermatitis / eczema
yellow, oily, scaly patches
Face, scalp, ears
cradle cap, dandruff
Contact dermatitis / eczema
localised reaction (erythema, itching, burning)
contact with irritant
Allergic Contact dermatitis / eczema
red, itchy, weepy
contact with allergen
Scabies
Ringworm
Psoriatic plaque
-
8/8/2019 Atopic Eczema 2
7/27
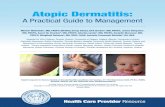
Presentation Age & duration
influencesdistribution and
appearance
Infancy;
face,scalp,extensor
surfaces,nappy
area spared.
Children;
longstandingflare ups
localised to the
flexures
-
8/8/2019 Atopic Eczema 2
8/27
Morbidity/Mortality
Significant cause of morbidity
Incessant itch and loss of work days in adults
In children,enormous psychological burden to families
and loss of school days Mortality is extremely RARE !
-
8/8/2019 Atopic Eczema 2
9/27
Diagnostic criteria
An itchy skin condition (or parental report of scratching) inlast 12 months plus any 3 of the following:
History of involvement of the skin creases
History of flexural dermatitis
(or dematitis of cheeks +/or extensor areas in child
-
8/8/2019 Atopic Eczema 2
10/27
10
Assessment
Detailed history time of onset / pattern / severity
response to past / current Rx
possible triggers dietary history
growth & development
impact on child & family
history of atopy (personal / family)
Tools POEM / CDLQI / Visual analogue scales
10
-
8/8/2019 Atopic Eczema 2
11/27
Management:
General Measures1. Adopt an holistic approach severity
quality of life
impact on activities / sleep
2. Identify and manage trigger factors
irritants
skin infections
food / inhalent allergens
3. General measures keep fingernails short
Avoid perfumed / lathering products
? Role for antihistamines
-
8/8/2019 Atopic Eczema 2
12/27
Management -a stepped approach
1. EMOLLIENTS
moisturising, washing, bathing combination of products or one for all
2.TOPICAL STEROIDS
Tailor potency to severity & body site Short term use
3. INFECTIVE EXACERBATIONS
Recognition How to access appropriate treatment
Special reference to recognition of eczema herpeticum
4.EDUCATION
Patient & Parents Verbal & Written
Practical demonstrations
-
8/8/2019 Atopic Eczema 2
13/27
Other Forms of Rx
Antihistamines Not for routine use
trial of non sedating if severe itching
consider 1-2 week trial of sedating if significant sleep
disturbance
Bandages & Dressing
localised medicated or dry dressings
NOT for infected areas
Topical calcineurin inhibitors
tacrolimus and pimecrolimus
NOT for mild eczema or as 1st line
Children aged >2 yrs
Phototherapy & Systemic treatments
-
8/8/2019 Atopic Eczema 2
14/27
Management -
Dermatological Referral Diagnosis is / has become uncertain
Failure to control
No of flare ups despite treatment
adverse reaction to treatment
Contact allergic dermatitis is suspected
persistent atopic eczema
facial, eyelid, hand eczema
Significant social / psychological problems
Severe and recurrent infections
Perceived benefit from specialist advice
-
8/8/2019 Atopic Eczema 2
15/27
15
Emollients 1
In eczema, normal skin barrier function is disturbed Use of regular moisturisers will help to rehydrate &
restore barrier
reduce itching & scratching
prevent skin penetration
reduce inflammatory / infective triggers
Regular use helps prevent flare-ups & need for steroids
LOTIONS are light & non greasy
mildly affected large areas or hairy areas
CREAMS are also non-greasy but thicker
for moist or weeping lesions
OINTMENTS are thick, occlusive and greasy
dry, lichenified or scaly lesions15
-
8/8/2019 Atopic Eczema 2
16/27
Emollients 2 Mode of action:
Occlusive
Humectant (contain urea, lactic acid...)
Keratolytics (contain urea, lactic acid, glycolic acid
For everyday moisturising, washing & bathing
used more often and in larger amounts than other treatments
used in conjunction with other treatments
used instead of soaps, detergent based products, shampoos
Used on the whole body even when clear
Advise liberal use & prescribe accordingly (250 - 500g
weekly) Review repeat prescriptions at least annually
Examples:
Dibrobase, Doublebase, Epaderm, Cetraban,
Aveeno, Oilatum
-
8/8/2019 Atopic Eczema 2
17/27
17
Topical Steroids 1
Suppress inflammation & control / relieve the symptoms indirectly reduce risk of infection
Rebound may occur on discontinuation
Divided into 4 strengths: (depends on steroid & formulation)
MILD- Hydrocortisone 0.1-2.5% [Dioderm]
MODERATE
- Betamethasone valerate 0.025% [Betnovate-RD]
- Clobetasone butyrate 0.05% [Eumovate]
POTENT
- Mometasone furoate 0.1% [Elocon]
- Betamethasone valerate 0.1% [Betnovate]
VERY POTENT
- Clobetasol propionate [Dermovate] 17
-
8/8/2019 Atopic Eczema 2
18/27
Topical Steroids 2
Benefits outweigh the risks WHEN applied correctly only on active areas
Prescribe a strength of topical steroids to match severityof the eczema & its anatomical location
Avoid potent steroids on face or neck of children under 1 yr
Avoid using for > 2 weeks at a time Avoid prescribing very potent steroids without specialist advice
Do not use potent topical steroids for more than 2 wks inchildren under 1 year
For maintenance step down a potency class from whatwas used for controlling the flare
Exclude secondary infection if no result within 2 weeks
Consider weekend treatment in children with >2 flaresper months
usual steroid 2days/week on weekly basis
-
8/8/2019 Atopic Eczema 2
19/27
19
Topical Steroids 2
Choice of steroid combined with other agents alsoavailable
Antimicrobial Fucidin H, Canesten HC, Trimovate, Fucibet
Crotamiton (anti itch) Eurax-Hydrocortisone
Urea (humectant moisturiser) Calmurid HC Salicyclic Acid (keratolytic) Diprosalic
19
-
8/8/2019 Atopic Eczema 2
20/27
Infected Eczema Lesions can become infected
staphylococcus +/or streptococcus (usually)
Characterised by:
weeping,
crusts, pustules,
failure to respond to treatment,
fever,malaise and possibly sepsis
Start treatment as soon as possible and continue for 48
hrs after symptoms subside
Topical antibiotics for localised infection
Systemic antibiotics if widespread or not responding
Flucloxacillin (Erythromycin / Clarithromycin)
If coexisting with a flare,consider topical steroid or
steroid/abx combinations (eg fucibet)
-
8/8/2019 Atopic Eczema 2
21/27
21
Eczema Herpeticum
Consider HSV infection areas of rapidly worsening, painful eczema
fever, lethargy, distress
clustered cold sore - like blisters
punched out erosions which may coalesce & crust
not responding to usual treatment
Treat with systemic aciclovir immediately
+/- antibiotics
Consider opthalmological / dermatological advice
-
8/8/2019 Atopic Eczema 2
22/27
22
NICE Guidelines 2007
22
-
8/8/2019 Atopic Eczema 2
23/27
23
NICE Guidelines 2007
23
-
8/8/2019 Atopic Eczema 2
24/27
24
ALLERGY
Consider food allergy
immediate reaction to a food
moderate / severe uncontrolled atopic eczema
above + history of gut dysmotility or failure to thrive Consider inhalent allergy
seasonal flares
associated asthma, rhinitis
>3 yrs with facial eczema consider allergic contact dermatitis
previously controlled
reaction to topical treatments
24
-
8/8/2019 Atopic Eczema 2
25/27
25
ALLERGY 2
Offer 6-8 week trial of extensively hydrolysed or amino
acid formula in bottle fed infants < 6 months with
uncontrolled > moderate eczema
Avoid partially hydrolysed, soya protein or other speciesmilk if suspect CMPI
It is not known if altering a breastfeeding mothers diet is
effective in reducing the severity of symptoms but can
consider a trial if strongly suspect
25
-
8/8/2019 Atopic Eczema 2
26/27
26
NICE Guidelines 2007
26
-
8/8/2019 Atopic Eczema 2
27/27
Acknowledgements
NICE Guideline- CG57
emedicine.org
Cks.nhs.uk