
AtlAutologous Chondrocyte Implantation · PDF file“ulcerated cartilage is a troublesome...
57
Atl Autologous Chondrocyte Chondrocyte Implantation Implantation Nehemia Blumberg
-
Upload
vuongquynh -
Category
Documents
-
view
216 -
download
2
Transcript of AtlAutologous Chondrocyte Implantation · PDF file“ulcerated cartilage is a troublesome...

A t lAutologous
ChondrocyteChondrocyte
ImplantationImplantation
Nehemia Blumberg

“ulcerated cartilage is a troublesome thing,
once destroyed, it is not repaired.”
Of the structure and disease of articulating cartilages. 1743
William Hunter (1718–1783)

Articular Cartilage Structure
SuperficialZone
ArticularSurface
MiddleZoneZone
Tidemark
DeepZone
CalcifiedC til
SubchondralBone
CartilageEach zone of has a characteristic composition and architecture relate directly to that zone’s function
Cartilage Form and Function
• Collectively, these highly specialized layers produce the superior
loading and minimal friction
• Chondrocytes constitute 2% of the total
l f d lt ti l tilvolume of adult articular cartilage
• Healthy chondrocytes are integral to cartilage survival

Cartilage Form and FunctionCartilage Form and Function

Response to Injury
Depends on the severity and depth:
• Low-energy “trivial” initiate a cascade toward gy
degeneration in the absence of visible changes
• Partial thickness
• Full-thickness subchondral bone

Cascade – “vicious cycle”
increased hydration
decreased proteoglycan concentrationinjure chondrocytes
decreased cartilage stiffnesslimit their repair capacity
increased force transmission to the subchondral bone
subchondral bone increases its stiffness
Higher impact loads to the cartilageg p g

Chondrocyte Response to InjuryChondrocyte Response to Injury
• proliferating & increasing matrix synthesis
l t f ti l tilavascular nature of articular cartilage
• can not restore the surface
• penetrate subchondral bone - higher repair capacity

Chondrocyte Response to InjuryChondrocyte Response to Injury
• bleeding & hematoma formation
• stem cell migration
• synthesis of type I collagen• synthesis of type I collagen
fibrocartilage

Clinically Point of ViewClinically Point of View
• partial thickness defects do not heal but rarely
i t d ith i ifi t li i l blassociated with significant clinical problems
• small full-thickness cartilage lesions can fill withsmall full thickness cartilage lesions can fill with
fibrocartilage & render a patient asymptomatic
• large full-thickness cartilage lesions result in pain &
disability

Goals of TreatmentGoals of Treatment
• restore the congtuity
• control the symptoms
• durability to stand load• durability to stand load
• prevent progression to OAprevent progression to OA

Indication for Autogenous gChondrocyte Implantation
t ti• symptomatic
large >2cm2• large >2cm2
full thickness lesion• full-thickness lesion
f l d l & t hl• femoral condyle & trochlear groovebetter then patella & tibia
• talus, shoulder, elbow, hip

EnvironmentEnvironmentPresence of coexisting knee pathology:
• ligamentous instability
• bony malalignment (TFJ, PFJ)
• meniscial mal-function
• Bone loos > 8mm
If untreated result in poorer patient outcome

Contra-indication for Autogenous gChondrocyte Implantation
• bipolar lesion
• OA• OA
• active inflammatory or infective arthritis

Autogenous Chondrocyte g yImplantation
The final determinant in assessing the
it bilit f h d l l i f ACIsuitability of a chondral lesion for ACI
comes at the time of arthroscopycomes at the time of arthroscopy

AutogenousChondrocyteChondrocyteImplantationpan arthroscopic biopsy:
i b f ll• precise number of cells30×106 cells/mL.
• suspension

AutogenousChondrocyteChondrocyteImplantationp
arthrotomic reimplantedarthrotomic reimplantedbeneath periosteal patch

Implantation of Trochlear Defect
2.85 cm2
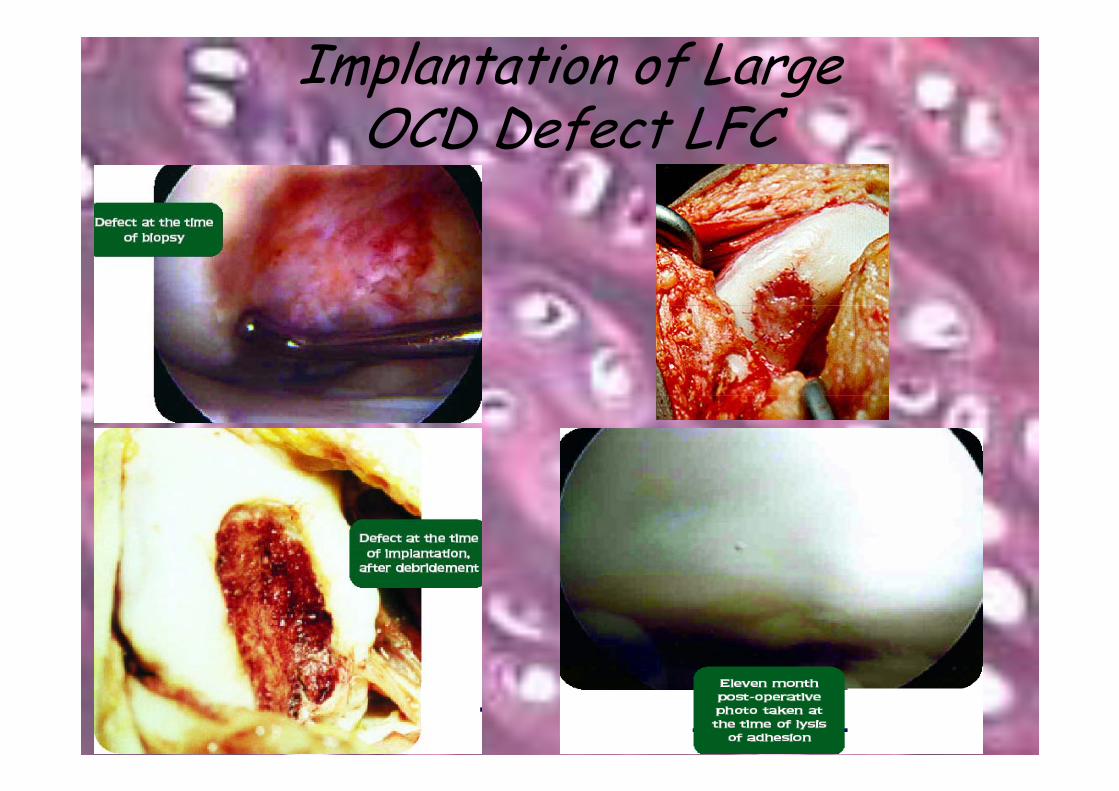
Implantation of LargeOCD Defect LFCOCD Defect LFC

Treating Coexisting PathologyTreating Coexisting PathologyWh t & Wh ?What & When?
Multifactorial:
• severity
• multiple coexisting pathology
• surgeon experiencesurgeon experience
• patient factors – work, rehabilitation
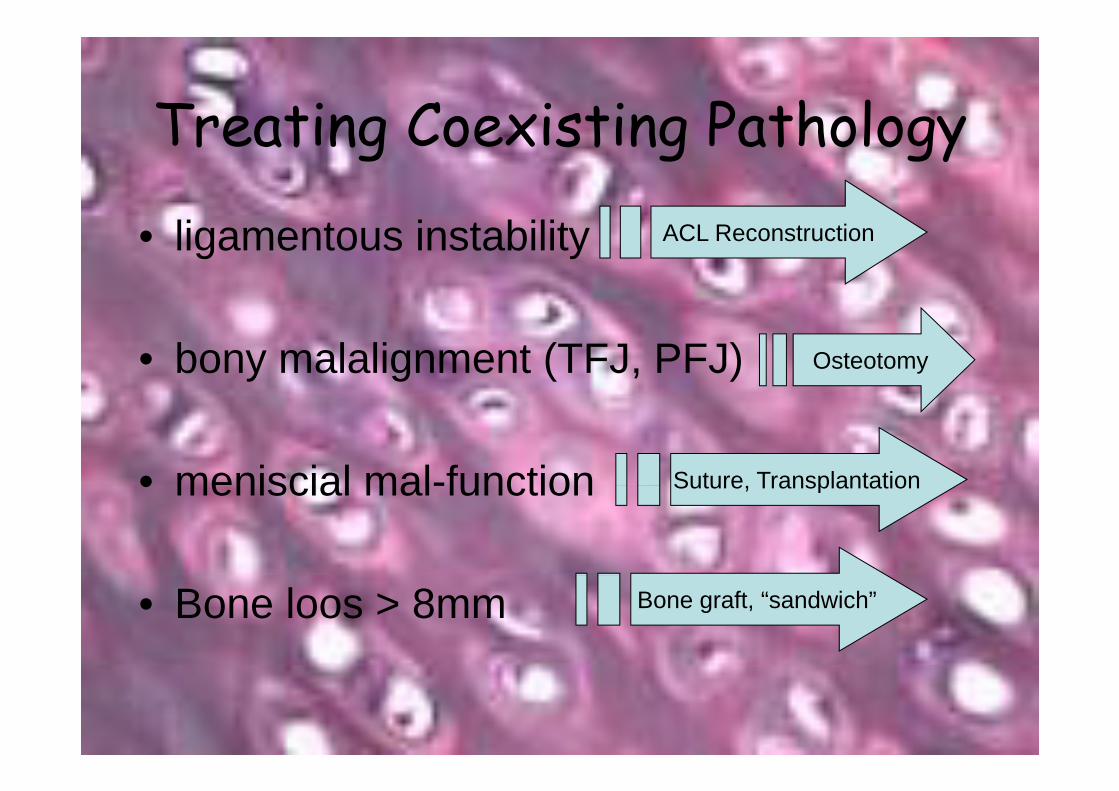
Treating Coexisting PathologyTreating Coexisting Pathology
• ligamentous instability ACL Reconstruction
• bony malalignment (TFJ, PFJ) Osteotomy
• meniscial mal-function Suture Transplantation• meniscial mal-function Suture, Transplantation
• Bone loos > 8mm Bone graft, “sandwich”

Concomitant or Staging?Concomitant or Staging?
One additional procedure doesn't increase complication ratep
ti B G fti• exception Bone Grafting:small: “sandwich”s a sa d clarge: open or arthroscopic grafting
4 6 months prior to ACI4-6 months prior to ACI

The Sandwich Technique
lesions that violate thesubchondral layersubchondral layer

Concomitant or Staging?Concomitant or Staging?200 ACI. Gillogly, 2002.g y,
• 55% concomitant procedure:anteromedialization of the tibial tubercleACL reconstruction HTOmeniscal transplant
• 12% staged procedure:bone graftHTO

Post-ACI rehabilitationcomplete fill not firmly attached to
subchondral bonesubchondral bone
equal to hostindentability which recoils
equal to hostcartilage
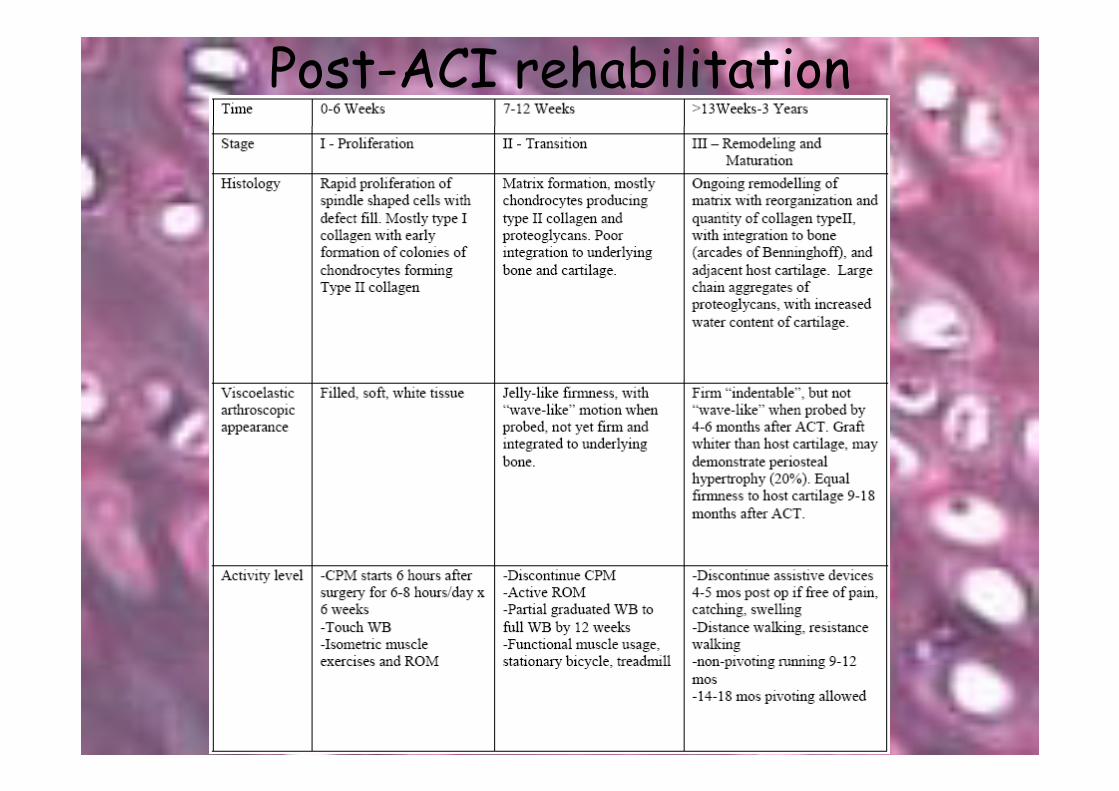
Post-ACI rehabilitation

Post ACI rehabilitationPost-ACI rehabilitationstimulus for regeneration without overstressingstimulus for regeneration without overstressing
• early motion (CPM)
• physical therapy: patellar mobility quadriceps strength romphysical therapy: patellar mobility, quadriceps strength, rom
• 3 months full weight bearing
• 6 months light-impact training
12 th hi h l l t• 12 months high-level sports

Periosteal FlapPeriosteal FlapIs not optimal:
• fixation of periost with stitches• Arthrotomy
Alternative:
• three-dimensional carrier• MACI - matrix-induced autologous chondrocyte implantation

Matrix-induced autologous gchondrocyte implantation
• bilayer membrane of collagena smooth side acts as a natural barriera porous side, seeded, faces bone
• seeded with cultured autologous chondrocytes• seeded with cultured autologous chondrocytes

Matrix-induced autologous h d i l ichondrocyte implantation
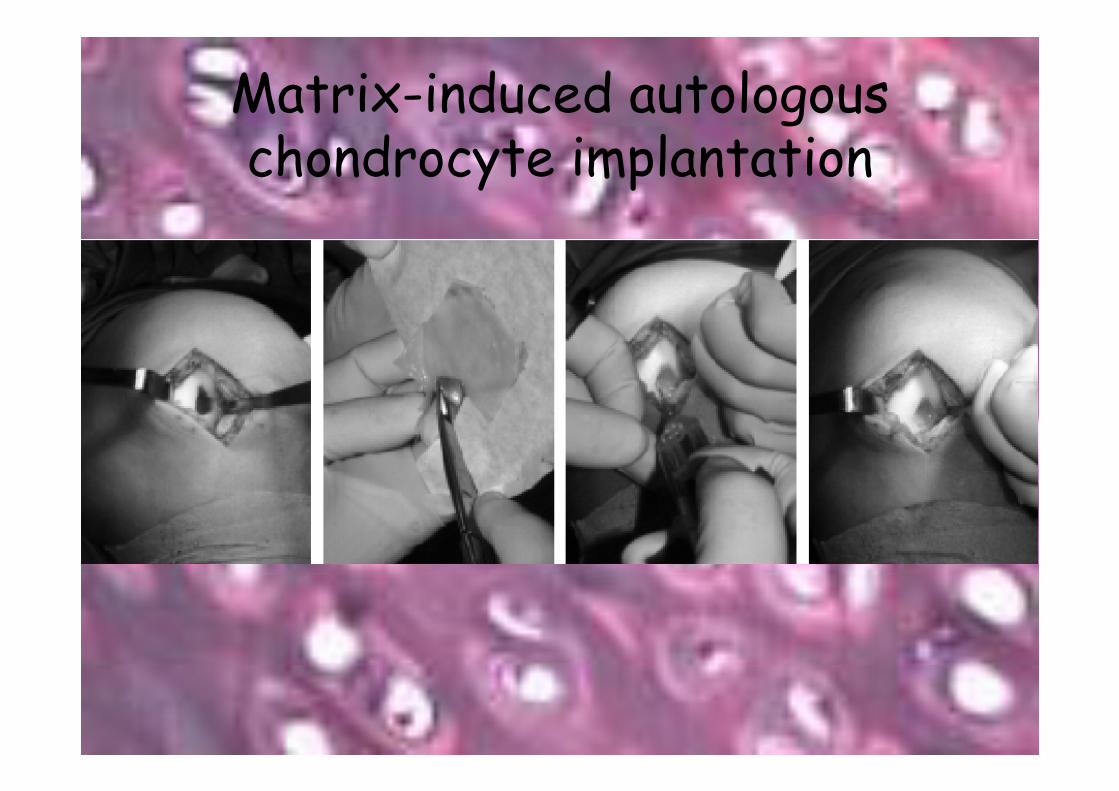
Matrix-induced autologous gchondrocyte implantation

Arthroscopic Matrix-induced pautologous chondrocyte implantation
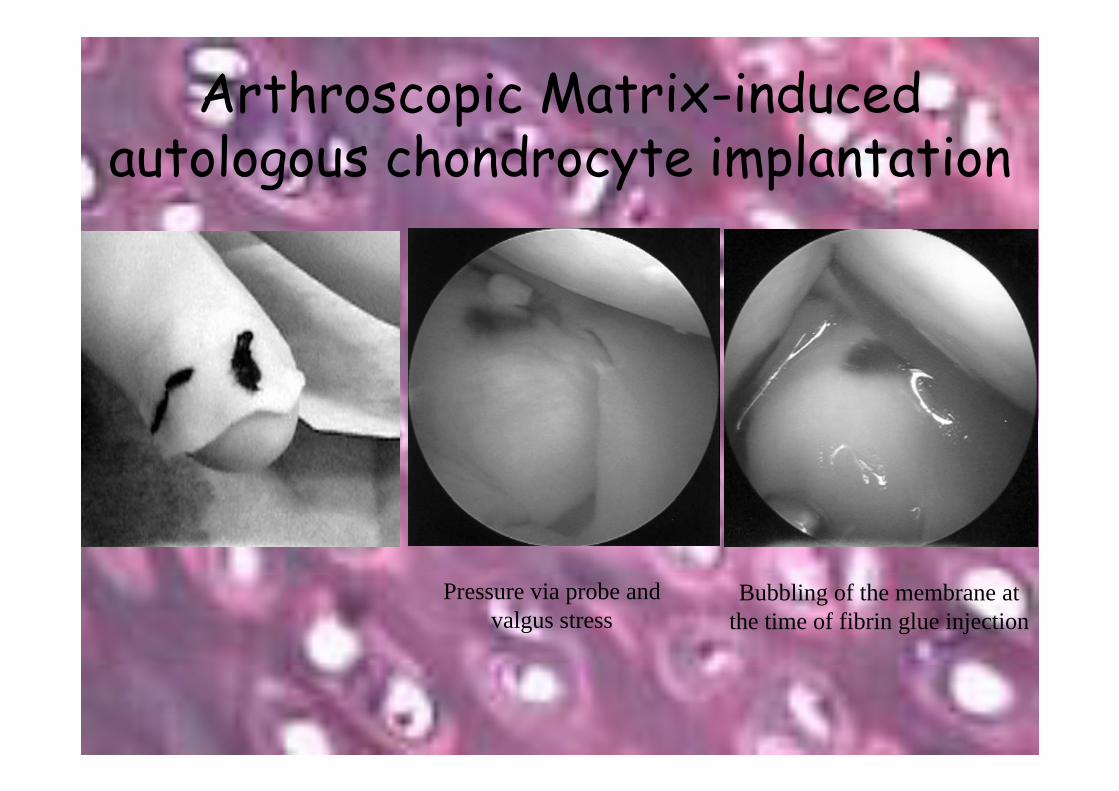
Arthroscopic Matrix-induced pautologous chondrocyte implantation
Bubbling of the membrane at the time of fibrin glue injection
Pressure via probe and valgus stress

Three-Dimensional CarrierSynthetic polymer scaffolds
Three Dimensional Carrier
... in the shape of a nose (left) is "seeded" with chondrocytes that replace the polymer with cartilage over time (right) to
make a suitable implant.

Three Dimensional CarrierThree-Dimensional Carrier
Light microscopy: migration and outgrowth of chondrocytes

Three Dimensional CarrierThree-Dimensional Carrier
Chondrograft before application

Three Dimensional CarrierThree-Dimensional Carrier

Three Dimensional CarrierThree-Dimensional CarrierStep 3
S di f ll ff ld
Step 2Cultivation of cells in monolayers for
2-3 weeks
Seeding of cells on scaffold
+
TMBio-molecules
Plasma protein (Fibrin)/Hyaluronic
id b d ff ld
Cartilage RepairFGF 2 variant
acid based scaffold

Three Dimensional CarrierThree-Dimensional Carrier

Clinical ResultsClinical Results• 80-90% good –excellent 5-7.5 ys.
knee score, VAS
• 75% hyaline-like tissue
Histology Excellent Good Fair Poor
Hyaline2
17%
6
50%
3
25%
1
8%17% 50% 25% 8%
Fib til1 2 2 1
Fibro cartilage17% 33% 33% 17%

Clinical ResultsClinical Results• able to return to military duty
• degenerative changes – lower scorehigher satisfactionhigher satisfaction
subgroup analysis: better if treat < 1 year• subgroup analysis: better if treat < 1 yearno difference: size, location (in femur) co procedure(in femur), co - procedure

Clinical ResultsClinical Results• 2 years as an indicator of future outcome
• grafts fail within the first 2 years
• graft survival ~100% between 3 - 8 years

Biomechanics & Durability• “We asked 18 randomly chosen patients”
• 11 patients agreed at a mean 54.3 months
• The mechanical characteristicsThe mechanical characteristics
Bi• Biopsy
Peterson Lars, et al. THE AMERICAN JOURNAL OF SPORTS MEDICINE,2002

Biomechanics & DurabilityBiomechanics & Durability

Periosteum or Collagen membrane?Periosteum or Collagen membrane?
70 ti t <50• 70 patients: <501 year postoperative
• ACI with periosteum: 18 (26%)• ACI with Collagen membrane: 52 (74%)• ACI with Collagen membrane: 52 (74%)
• Mean Modified Cincinnatti Rating Score:• Mean Modified Cincinnatti Rating Score:
ACI with Periosteum: 74 pointsACI with Periosteum: 74 pointsACI with Collagen membrane : 75 points

Complications
• arthrotomy: stiffnessthromboembolisminfection
• periosteal hypertrophy: 7-9 months“catching, pain”catching, pain
detachment• detachment
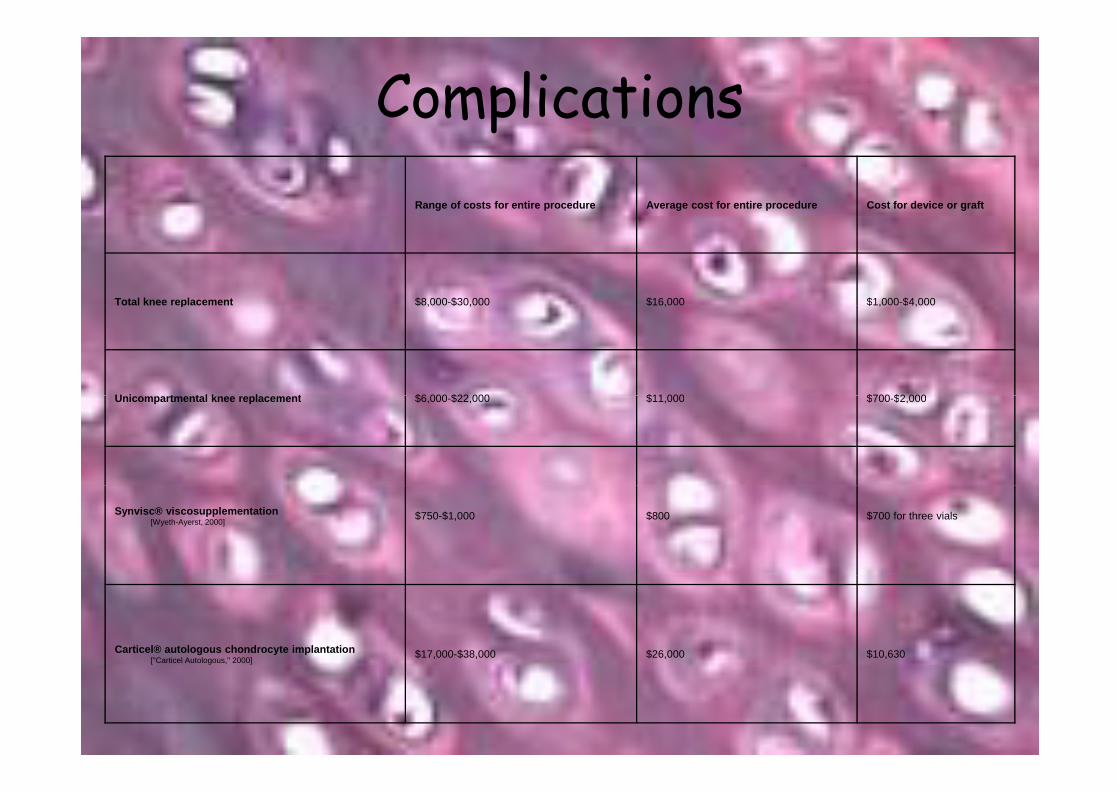
ComplicationspRange of costs for entire procedure Average cost for entire procedure Cost for device or graft
Total knee replacement $8,000-$30,000 $16,000 $1,000-$4,000p $ , $ , $ , $ , $ ,
U i t t l k l t $6 000 $22 000 $11 000 $700 $2 000Unicompartmental knee replacement $6,000-$22,000 $11,000 $700-$2,000
Synvisc® viscosupplementation[Wyeth-Ayerst, 2000]
$750-$1,000 $800 $700 for three vials
Carticel® autologous chondrocyte implantation["Carticel Autologous," 2000]
$17,000-$38,000 $26,000 $10,630

Cost Assumptions
Autologous chondrocyte transplantation for cartilage defectsg y p gin the knee joint. A West Midlands Development and Evaluation Service Report. University Hospital Birmingham. 1999

Cost Effectiveness(NHS) (QALY)
ACI £10 400 4 9ACI £10,400 4.9
Others £3,000 4.1
£7400 0.8
QALY Q li Adj d Lif Y• QALY Quality Adjusted Life Year
• At 10 years follow-up the base case analysis suggests anAt 10 years follow up the base case analysis suggests an incremental (additional) cost per QALY gain of approximately £9,000

A Randomized Trial
• ACI versus mosaicplasty for OCDJ Bone Joint Surg [Br] 2003g [ ]
• ACI versus MicrofractureACI versus MicrofractureJ Bone Joint Surg [Am] 2004

ACI versus MosaicplastyACI versus Mosaicplasty• 100 patients: 58 ACI
42 i l t42 mosaicplasty
• mean duration of symptoms 7.2 years
• mean follow-up 19 months (12 to 26)
• 1 ys.: 60 arthroscopy & biopsy

ACI versus MosaicplastyACI versus Mosaicplasty
Only lesions of the MFC treated by ACI, were significantly improved
International Cartilage Research Society (ICRS)

ACI versus MicrofractureACI versus Microfracture• 80 patients: 40 ACI
40 microfracture
• mean duration of symptoms 3 yearsmean duration of symptoms 3 years
follow up 12 24 months• follow-up 12 , 24 months
• 2 ys: 67 arthroscopy & biopsy

ACI versus MicrofractureACI versus Microfracture

ACI versus MicrofractureACI versus Microfracture
hyaline Fibrocartilage-hyaline
Fibrocartilage

ACI versus MicrofractureACI versus Microfractured ti b tt li i l lt• younger and more active - better clinical results
• subjective improvement better in the microfracture
• no difference regarding macroscopic & histological quality
• no association between histological quality & theno association between histological quality & the clinical outcome

Why?Why?d ti f t• mean duration of symptoms
• heterogenic
• “traditional ACI”
• short-term
• mechanical characteristics vs. histological quality


















