ASV Galileo
43
ASV use and algorithm ASV use and algorithm HAMILTON MEDICAL AG Switzerland February 2001
-
Upload
alvyandani -
Category
Documents
-
view
56 -
download
1
description
asv galileo
Transcript of ASV Galileo

ASV use and algorithmASV use and algorithm
HAMILTON MEDICAL AGSwitzerland
February 2001

ContentsContents
•Introduction
•Clinical use of ASV
•Functional description of ASV
•Scientific basis

IntroductionIntroduction
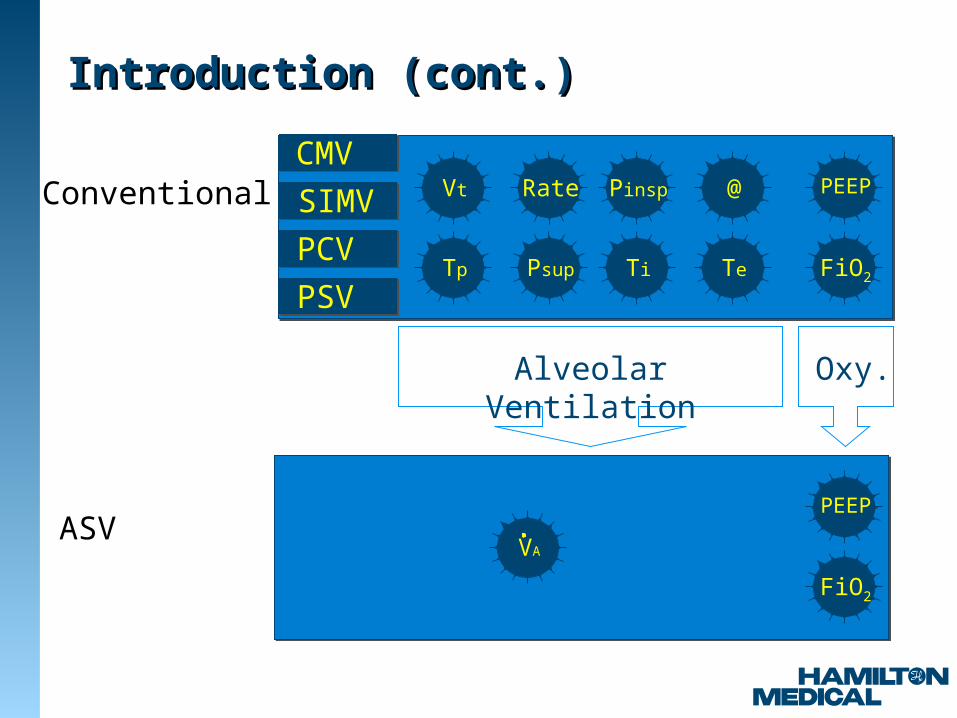
b) The obvious but difficult solutionRemove as many knobs as possible while still giving the user control over the pertinent parameters
a) Problems with conventional ventilatorsToo many knobs, too many controls, very few guidelines for setting controls
c) Definitions of pertinent parameters V'A To control pH/PaCO2 and WOB PEEP To control FRC and thus PaO2
FiO2 To control PaO2
Tp
Rate
Psup
Pinsp
Ti Te
@
FiO2
PEEPVt
FiO2
PEEP
VA
CMV
SIMV
PCV
PSV
Alveolar Ventilation Oxy.
Conventional
ASV
Introduction (cont.)Introduction (cont.)
Uses of ASVUses of ASV
•As start-up procedure only
•To critique the actual settings
•During weaning with and w/o protocol
•For post-cardiac surgery patients only
•For all patients, including ARDS
•As start-up procedure only
•To critique the actual settings
•During weaning with and w/o protocol
•For post-cardiac surgery patients only
•For all patients, including ARDS

How to use ASV clinically (1)How to use ASV clinically (1)
1) Set Body Wt of patient and high Pressure limit to 45 mbar (will yield Pmax < 35 mbar)
2) Set %MinVol to 100% (except COPD)
3) Set PEEP & FiO2 according to clinical requirements
4) Connect patient
How to use ASV clinically (2)How to use ASV clinically (2)
5) Ventilate for some minutes and assess blood gases and/or WOB (clinically)
6) Adjust %MinVol to meet pH/PaCO2 targets or WOB targets
7) Adjust PEEP and FiO2
8) Review high Pressure limit setting, consider changes only in exceptions
9) Observe Ppeak and fSpont trends
Repeat steps 5-9 until you consider extubation

Set high Pressure limit, Body Wt, %MinVol
Ventilate patient
Check blood gases and clinical statusPlot Pinsp, fTotal, fSpont trend
Set alarms
Consider weaning complete
fSpont and
ABG OK?
Yes
No
Prepare GALILEO
Pinsp< 8 cmH2O
No
Yes
Optimize %MinVol
Consider reducing %MinVol
Practical usePractical use

Optimize %MinVolOptimize %MinVolsee Operator‘s Manual p.D-13 and D-14see Operator‘s Manual p.D-13 and D-14
%MinVol change Remarks
Normal art. blood gases None
High PaCO2 Increase %MinVol Pay attention to
inspiratory pressures
Low PaCO2 Decrease %MinVol Pay attention to Pmean,
CO2 status
High respiratory drive Consider Increase in
%MinVol
Consider sedation,
analgesia, other treatment
Low O2 saturation None Consider PEEP and/or
FiO2 increase

How to monitor the patientHow to monitor the patient
• Target graphics window shows
– ASV target MinVol, Vt, f
– Actually achieved values for MinVol, Vt, f
– Safety limits for Vt and f
– Check feasibility of %MinVol settings
• Trends show
– level of support provided by the ventilator vs. level of patient activity

ASV Target Graphics ASV Target Graphics WindowWindow

How to monitor the patient: How to monitor the patient: Trend and trackTrend and track
Pinsp
fSpont
I I I I I I I
1h 2h 3h 4h


Tp
Rate
Psup
Pinsp
Ti Te
@
FiO2
PEEPVt
FiO2
PEEP
VA
CMV
SIMV
PCV
PSV
Alveolar Ventilation Oxy.
Conventional
ASV
How does ASV work?How does ASV work?
0
500
1000
1500
2000
0 20 40 60
f (b/min)
Vt (
ml)
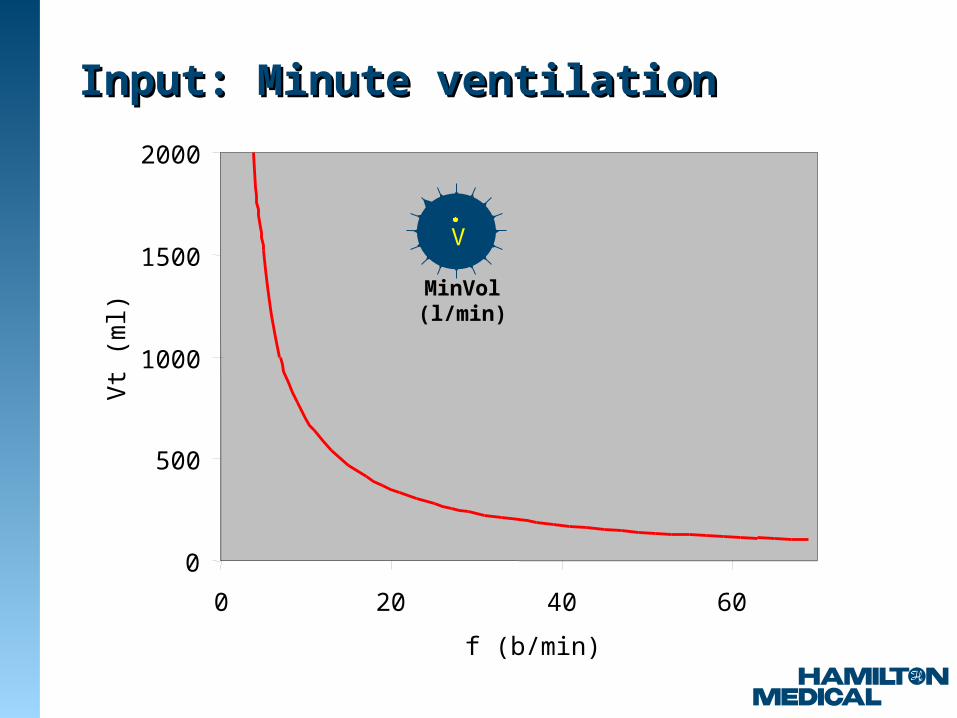
Input: Minute ventilationInput: Minute ventilation
MinVol (l/min)
V
ASV is a "servant" to achieve a preset ASV is a "servant" to achieve a preset MinVol while respecting boundary MinVol while respecting boundary
conditions.conditions.
"Maintain at least 100% of normal ventilation, take spontaneous breathing into account,
prevent tachypnea,prevent AutoPEEP,
prevent excessive dead space ventilation,fully ventilate in apnea or low drive,
give control to patient in case breathing activityis okay, and do this without exceeding a 35 mbar
plateau pressure."
Command to servantCommand to servant
Functional description of ASVFunctional description of ASVsee also see also
flow chart in ASV brochureflow chart in ASV brochureAppendix D of Operator‘s ManualAppendix D of Operator‘s Manual
ASV User‘s GuideASV User‘s Guide
1) Calculation of minute ventilation
2) Application of lung-protective rules
3) Optimal breath pattern
4) Approach the target
0
500
1000
1500
2000
0 20 40 60
f (b/min)
Vt (
ml)
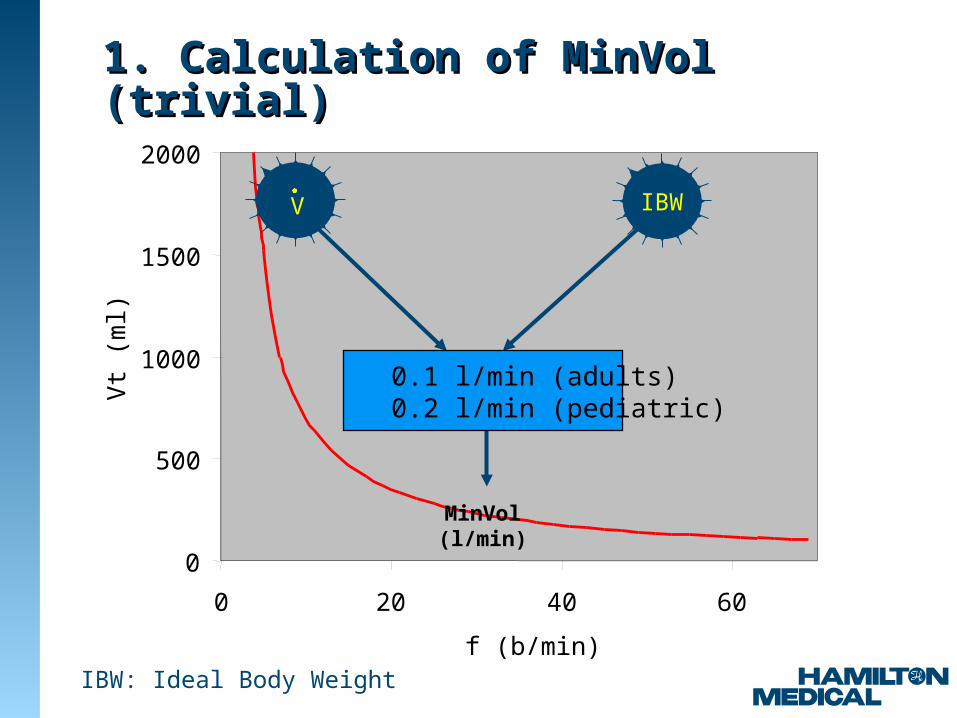
1. Calculation of MinVol (trivial)1. Calculation of MinVol (trivial)
MinVol (l/min)
0.1 l/min (adults)0.2 l/min (pediatric)
IBWV
IBW: Ideal Body Weight

2. Lung-protective rules 2. Lung-protective rules (boundary conditions)
0
500
1000
1500
2000
0 20 40 60
f (b/min)
Vt (
ml)
DD
AA
CC
BB
5 test breaths
10*Vd10*Vd
5 b/min5 b/min 20/RCexp20/RCexp
2*Vd2*Vd
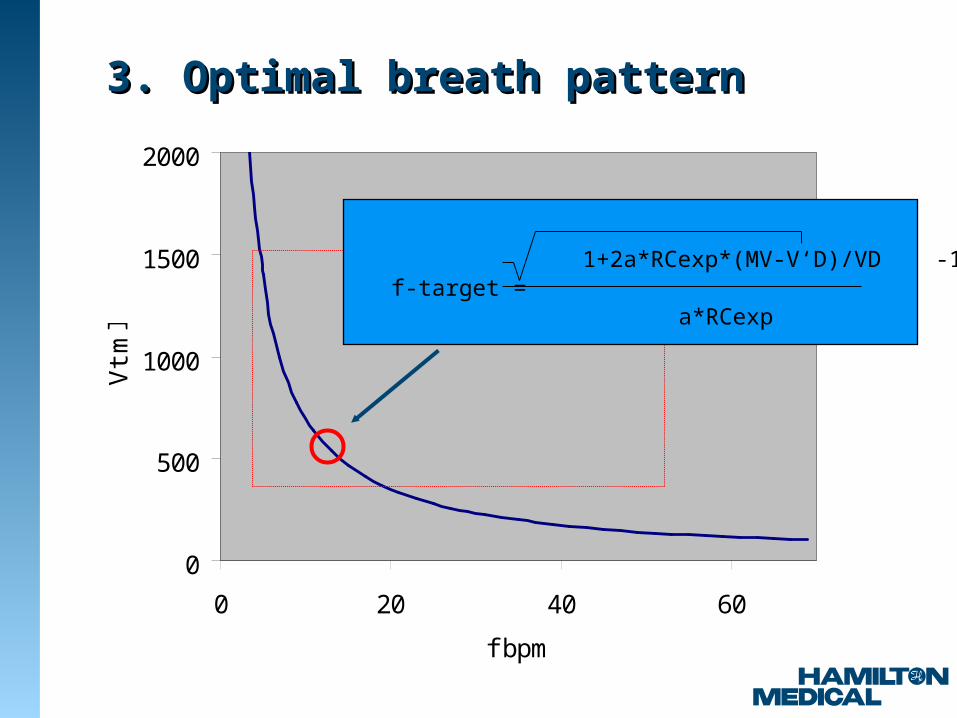
3. Optimal breath pattern 3. Optimal breath pattern
0
500
1000
1500
2000
0 20 40 60
f bpm
Vt m
l
1+2a*RCexp*(MV-V‘D)/VD -1f-target =
a*RCexp

0
500
1000
1500
2000
0 20 40 60
f bpm
Vt m
l
5 test breaths
4. Adjust Pinsp & fSIMV to meet target4. Adjust Pinsp & fSIMV to meet target
0
500
1000
1500
2000
0 20 40 60
f bpm
Vt m
l
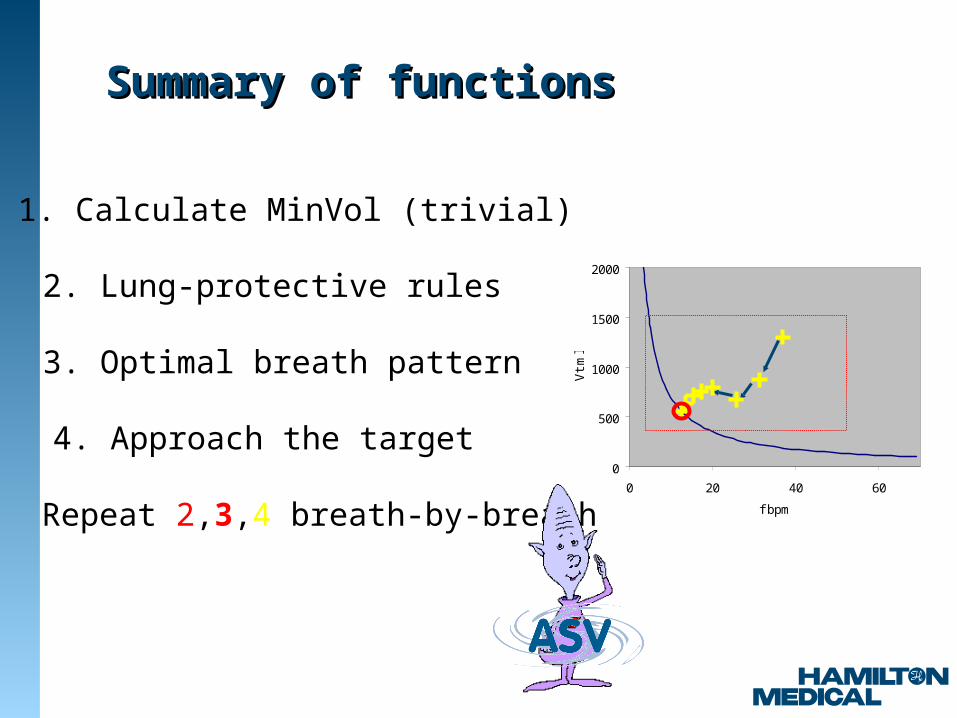
2. Lung-protective rules
1. Calculate MinVol (trivial)
4. Approach the target
3. Optimal breath pattern
Repeat 2,3,4 breath-by-breath
Summary of functionsSummary of functions

Scientific basisScientific basis
Choice of breathing pattern
Role of RCexp
Machine- or patient-triggered Dead space ventilation
Effects of PSL
Scientific basis (1)Scientific basis (1)
Choice of breathing pattern
Role of RCexp
Dead space ventilationMachine- or patient-triggered
Effects of PSL
FSIMPVFSIMPV

Fully Synchronized Intermittent Mandatory Pressure Ventilation (FSIMPV)
Fully Synchronized Intermittent Mandatory Pressure Ventilation (FSIMPV)
Machine- or patient-triggered Machine- or patient-triggered ventilationventilation
• Machine- and/or patient-triggered.
• Gas delivery is pressure-controlled for both the mandatory and the spontaneous breaths. Pressure levels are identical.
• Mandatory breaths are time-cycled if they were NOT triggered by the patient, spontaneous breaths are flow-cycled.
Control settings are: inspiratory pressure, respiratory rate, I:E ratio, pressure ramp, and expiratory trigger sensitivity. Other controls include
FiO2 and PEEP/CPAP.
"FSIMPVFSIMPV"
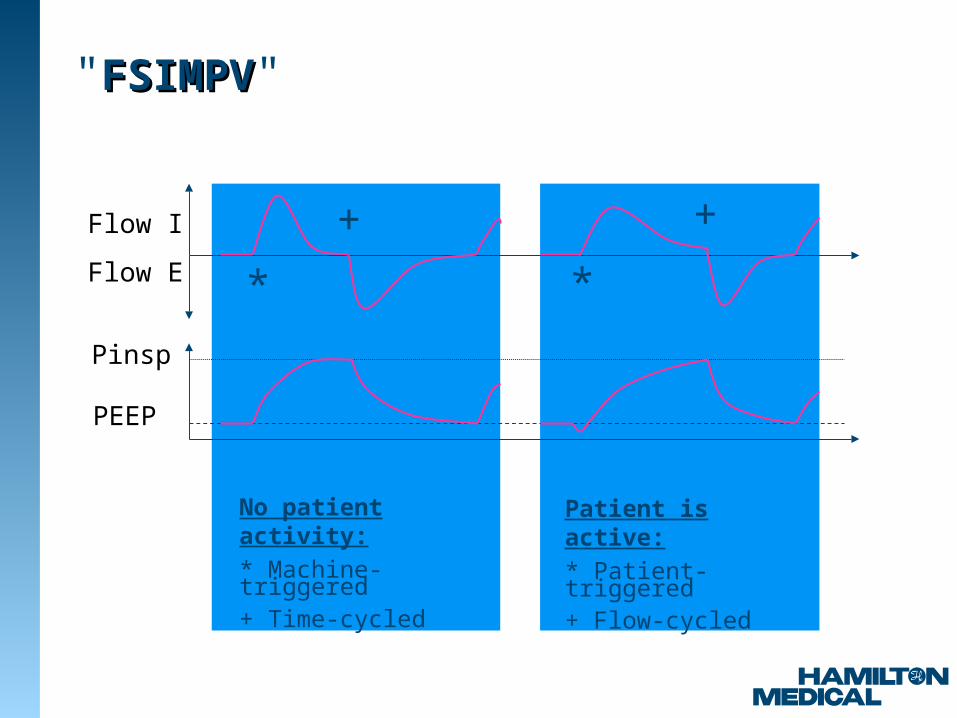
"FSIMPVFSIMPV"
Pinsp
PEEP
No patient activity:
* Machine-triggered+ Time-cycled
Patient is active:
* Patient-triggered+ Flow-cycled
Flow I
Flow E * *
+ +

"FSIMPVFSIMPV"
Ti To adjust I:E
f To adjust the rate
Pinsp To adjust Vt and fspont
PEEP To control FRCFiO2 To control PaO2
Scientific basis (2)Scientific basis (2)
Choice of breathing pattern
Role of RCexp
Dead space ventilationMachine- or patient-triggered
Effects of PSL
FSIMPVFSIMPV
Flow-volume loopFlow-volume loop

Flow, volume, and pressure tracings: Dynamic hyperinflationFlow, volume, and pressure tracings: Dynamic hyperinflation
-750-500-250
0250500750
V'a
w (
ml/s
)
0 1 2 3 4 5 6 7 8 9 10 11
-1000
100200300400500600700
Vol
(m
l)
0 1 2 3 4 5 6 7 8 9 10 11
05
101520253035
Paw
(cm
H2O
)
0 1 2 3 4 5 6 7 8 9 10 11
Time (s)

-100
0
100
200
300
400
500
600V
ol
(ml)
-1200 -800 -400 0 400 800
V'aw (ml/s)
I
E
Expiratory time constantExpiratory time constantExpiratory time constantExpiratory time constant

Scientific basis (3)Scientific basis (3)
Choice of breathing pattern
Role of RCexp
Dead space ventilationMachine- or patient-triggered
Effects of PSL
FSIMPVFSIMPV
Flow-volume loopFlow-volume loop
Minimal WOB (Otis)Minimal WOB (Otis)

Scientific basis (4)Scientific basis (4)
Choice of breathing pattern
Role of RCexp
Dead space ventilationMachine- or patient-triggered
Effects of PSL
FSIMPVFSIMPV
Flow-volume loopFlow-volume loop
Minimal WOB (Otis)Minimal WOB (Otis)
Radford 2.2 ml/kgRadford 2.2 ml/kg

0
50
100
150
200
250
0 50 100 150 200 250
Height (cm)
Vd
(m
l)
Vd (Hart)Vd - female (Radford)Vd - male (Radford)
Dead space guesstimationDead space guesstimation

Scientific basis (5)Scientific basis (5)
Choice of breathing pattern
Role of RCexp
Dead space ventilationMachine- or patient-triggered
Effects of PSL
FSIMPVFSIMPV
Flow-volume loopFlow-volume loop
Minimal WOB (Otis)Minimal WOB (Otis)
Radford 2.2 ml/kgRadford 2.2 ml/kg
Vt and fVt and f
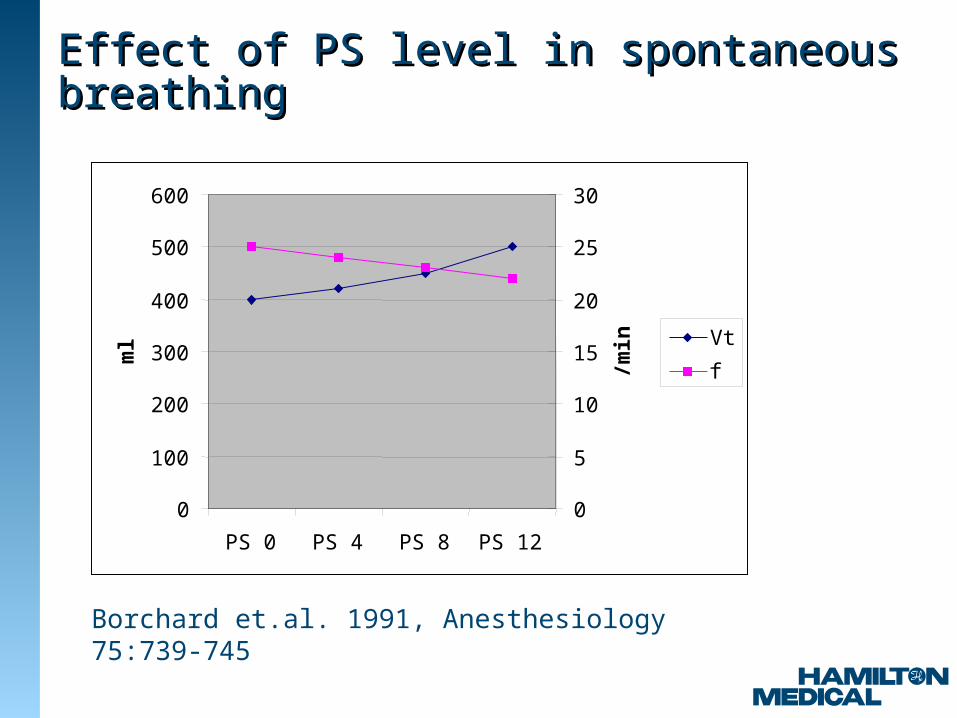
Effect of PS level in spontaneous breathingEffect of PS level in spontaneous breathing
Borchard et.al. 1991, Anesthesiology 75:739-745
0
100
200
300
400
500
600
PS 0 PS 4 PS 8 PS 12
ml
0
5
10
15
20
25
30
/min Vt
f
0
100
200
300
400
500
600
700
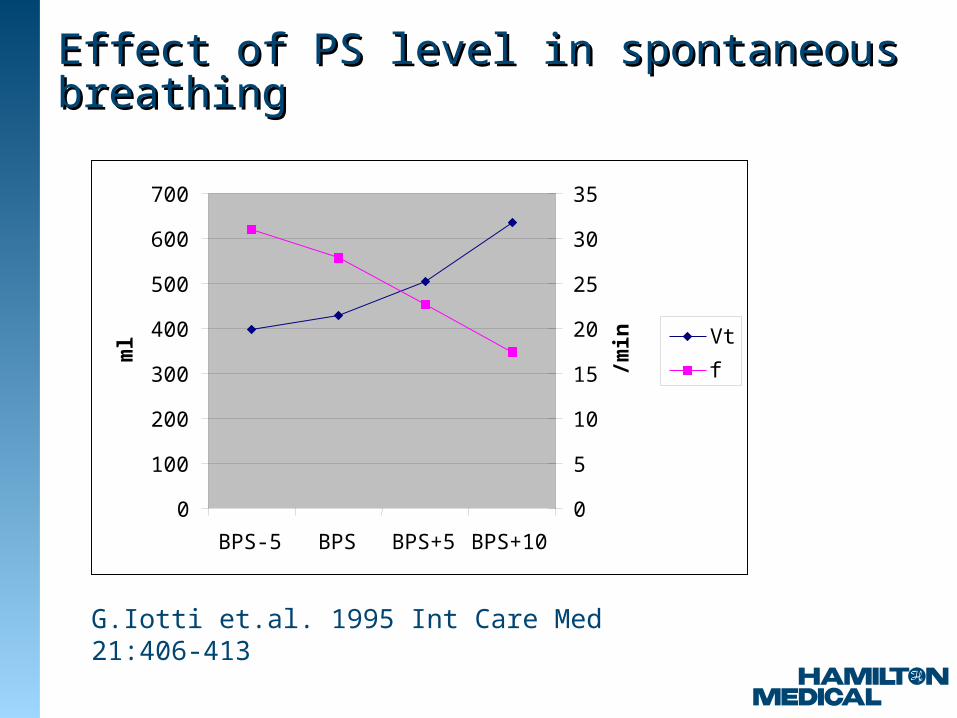
BPS-5 BPS BPS+5 BPS+10
ml
0
5
10
15
20
25
30
35
/min Vt
f
Effect of PS level in spontaneous breathingEffect of PS level in spontaneous breathing
G.Iotti et.al. 1995 Int Care Med 21:406-413

Scientific basis: SummaryScientific basis: Summary
Choice of breathing pattern
Role of RCexp
Dead space ventilationMachine- or patient-triggered
Effects of PSL
FSIMPVFSIMPV
Flow-volume loopFlow-volume loop
Minimal WOB (Otis)Minimal WOB (Otis)
Radford 2.2 ml/kgRadford 2.2 ml/kg
Vt and fVt and f
•ASV works in passive and in active patients
•ASV promotes weaning from minute one
•ASV employs lung-protective strategies to minimize complications from AutoPEEP and thus barotrauma
•ASV prevents tachypnea, apnea, excessive dead space ventilation, and excessive breaths
•ASV adapts continuously to the needs of the patient
BenefitsBenefits

When technology is masterWhen technology is masterwe shall reach disasterwe shall reach disaster
fasterfasterPiet Hein






![asv[s]:// @.blob.core.windows.net/ fs.azure.account.key.accountname enterthekeyvaluehere.](https://static.fdocuments.in/doc/165x107/56649e8f5503460f94b9405a/asvs-blobcorewindowsnet-fsazureaccountkeyaccountname-enterthekeyvaluehere.jpg)