grant application & funding approval from Hoxworth Blood Center to the Heimlich Institute
11/6/2008
1
Respiratory EmergenciesAndi Marmor, MDNovember 6, 2008
� Upper Airway Emergencies� Upper Airway Infections� Anaphylaxis
� Lower Airway Emergencies� Asthma▪ New Guidelines▪ Medication update
� Foreign Body Aspiration
� Phoebastria (Phoebe) is a 16 mo girl who presents to the ED at 3am with fever, cough and difficulty breathing
� She has had a cold and cough for 2 days, then woke up “unable to breath” and making a “funny noise” at 2am
� Improved a bit on the way to the ED
� T = 38.9, O2 sat 99%, RR 40, HR 160� Frightened but alert, looking around, non-
toxic with supple neck� Rhinorrhea, no drooling, post OP exam
deferred� Clear lungs, moderate retractions and a slight
squeak heard on each inspiration
11/6/2008
2
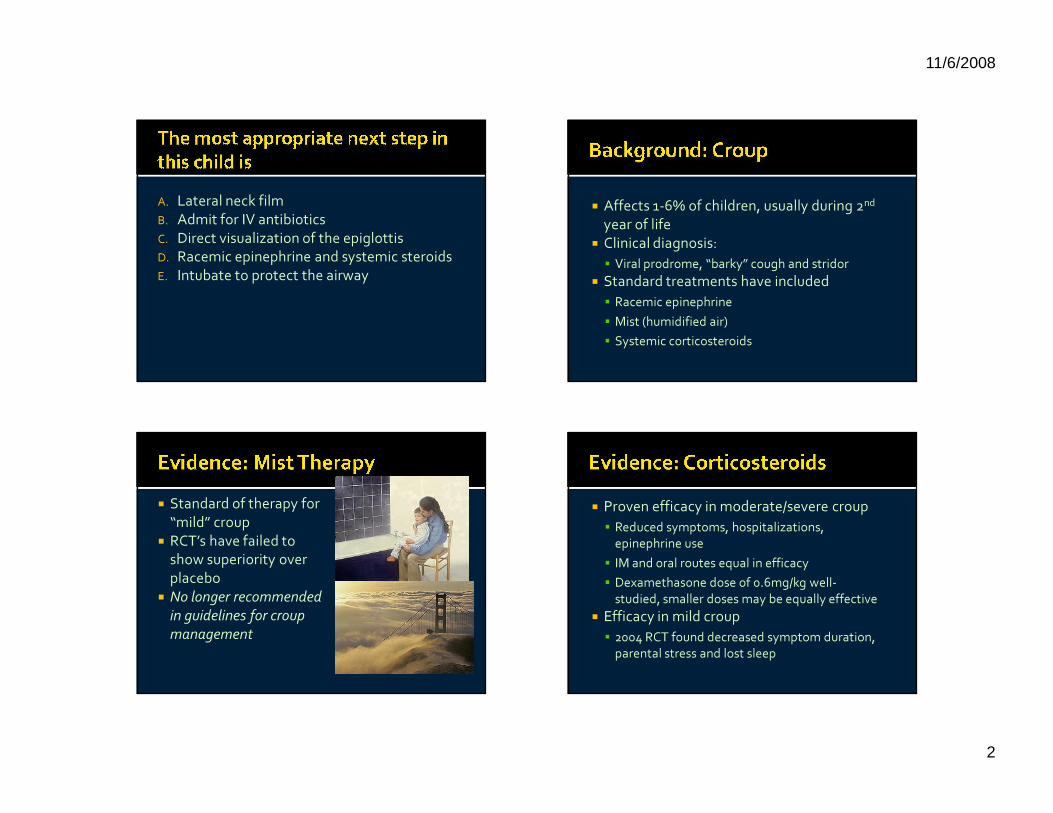
A. Lateral neck filmB. Admit for IV antibioticsC. Direct visualization of the epiglottisD. Racemic epinephrine and systemic steroidsE. Intubate to protect the airway
� Affects 1-6% of children, usually during 2nd
year of life� Clinical diagnosis: � Viral prodrome, “barky” cough and stridor
� Standard treatments have included� Racemic epinephrine� Mist (humidified air)� Systemic corticosteroids
� Standard of therapy for “mild” croup
� RCT’s have failed to show superiority over placebo
� No longer recommended in guidelines for croup management
� Proven efficacy in moderate/severe croup� Reduced symptoms, hospitalizations,
epinephrine use� IM and oral routes equal in efficacy� Dexamethasone dose of 0.6mg/kg well-
studied, smaller doses may be equally effective� Efficacy in mild croup� 2004 RCT found decreased symptom duration,
parental stress and lost sleep

11/6/2008
3
� Trial of mist therapy appropriate for mild cases
� Racemic epinephrine recommended for children with stridor at rest or severe upper airway obstruction� DC OK after steroids AND 3-4 h of observation
� Oral corticosteroids recommended in moderate croup and any time epi is given� May be beneficial in mild cases as well
A. Lateral neck filmB. Admit for IV antibioticsC. Direct visualization of the epiglottisD. Racemic epinephrine and systemic steroidsE. Intubate to protect the airway
NORMAL AP NECK STEEPLE SIGN
� You give Phoebe nebulized epinephrine, but her respiratory distress is worsening
� She is now fatigued, with cool extremities and an O2 sat of 94%
11/6/2008
4
A. EpiglottitisB. TracheitisC. Retropharyngeal abscessD. Foreign bodyE. Anaphylaxis
� Infectious:� Epiglottitis� Tracheitis� Retropharyngeal abscess/cellulitis
� Non-infectious� Foreign body aspiration� Anaphylaxis
� Infectious:� Epiglottitis� Tracheitis� Retropharyngeal abscess/cellulitis
� Non-infectious� Foreign body aspiration� Anaphylaxis
� Dramatic decline since Hib vaccination (1990)
� Causes: S. pneumonia, S. aureas > Hib� Diagnosis:� Clinical: Toxic, rapid progression, stridor, drooling� Lateral neck film: thumbprint sign� Direct visualization only in controlled setting
� Treatment: airway support and antibiotics
11/6/2008
5
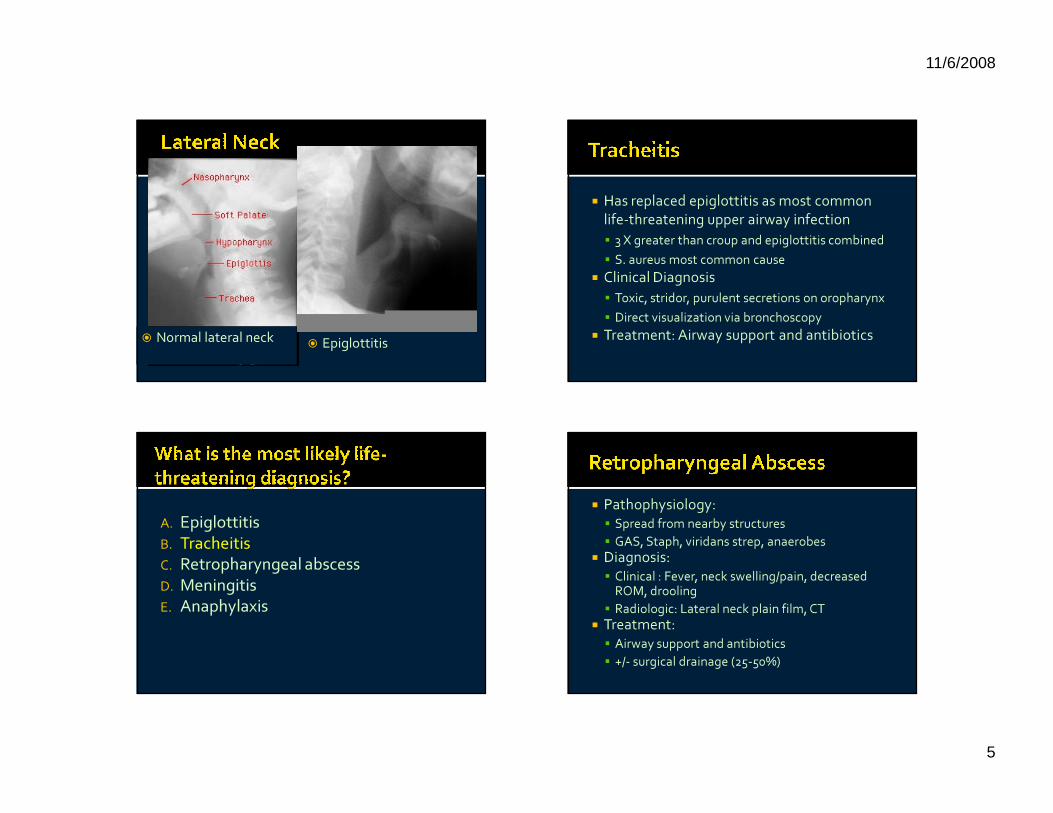
� Normal lateral neck � Epiglottitis
� Has replaced epiglottitis as most common life-threatening upper airway infection� 3 X greater than croup and epiglottitis combined� S. aureus most common cause
� Clinical Diagnosis� Toxic, stridor, purulent secretions on oropharynx� Direct visualization via bronchoscopy
� Treatment: Airway support and antibiotics
A. EpiglottitisB. TracheitisC. Retropharyngeal abscessD. MeningitisE. Anaphylaxis
� Pathophysiology:� Spread from nearby structures� GAS, Staph, viridans strep, anaerobes
� Diagnosis: � Clinical : Fever, neck swelling/pain, decreased
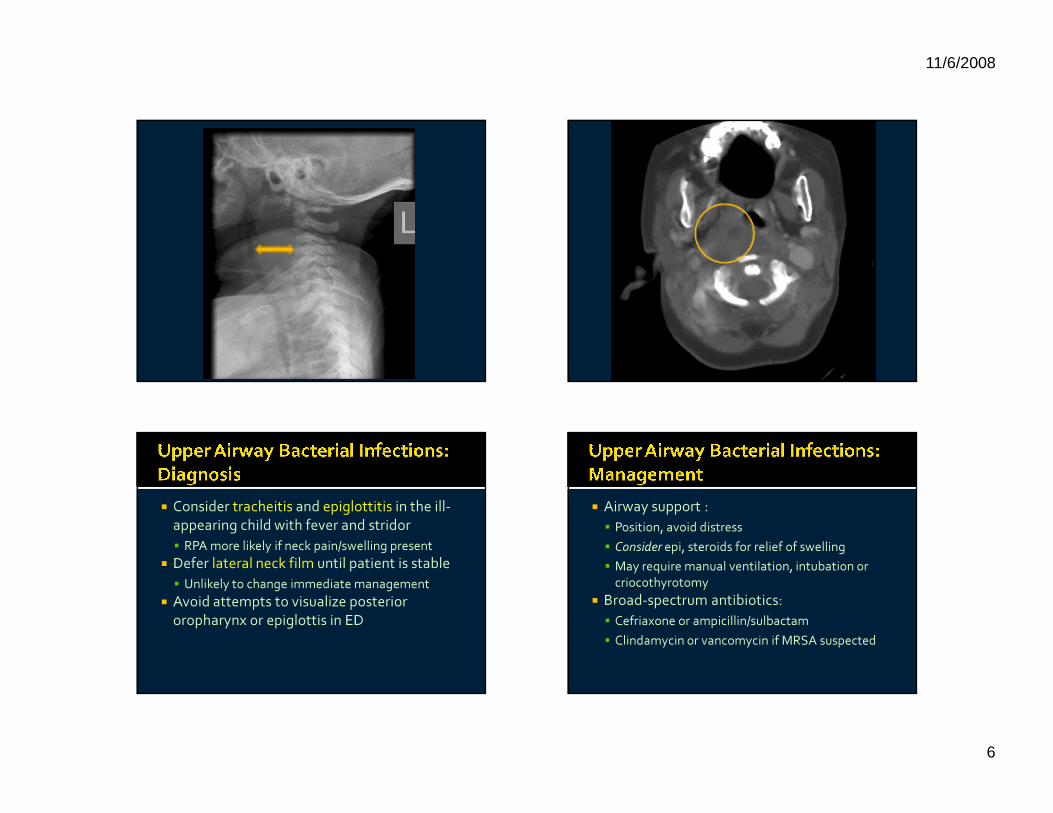
ROM, drooling� Radiologic: Lateral neck plain film, CT
� Treatment:� Airway support and antibiotics � +/- surgical drainage (25-50%)
11/6/2008
6
� Consider tracheitis and epiglottitis in the ill-appearing child with fever and stridor � RPA more likely if neck pain/swelling present
� Defer lateral neck film until patient is stable� Unlikely to change immediate management
� Avoid attempts to visualize posterior oropharynx or epiglottis in ED
� Airway support : � Position, avoid distress� Consider epi, steroids for relief of swelling� May require manual ventilation, intubation or
criocothyrotomy� Broad-spectrum antibiotics: � Cefriaxone or ampicillin/sulbactam� Clindamycin or vancomycin if MRSA suspected
11/6/2008
7
� Phalacrocorax (Phil) is a 14 month old boy who vomits and becomes unresponsive while with his mother in the waiting room
� In triage he is noted to have diffuse urticaria, swelling of his lips and eyelids, audible stridor and wheeze on auscultation
� He has a HR of 180, RR of 50, blood pressure of 100/60, and O2 sat of 99%
A. Give inhaled beta-agonists (albuterol) via nebulizer
B. Give IV methylprednisoloneC. Give IV diphenhydramineD. Give SC/IM epinephrineE. Give IV epinephrine
� Foods the most common cause in infants/ children
� History of allergy rare in infants� Fatality more likely:� History of atopy, asthma, peanut allergy, croup, or
urticaria
� Clinical diagnosis, labs not helpful� Symptoms occur 5-30 min after exposure� Cutaneous: itching, urticaria, flushing� Respiratory: upper/lower airway obstruction� GI: vomiting, diarrhea, abd pain� Cardiovascular: shock
� Biphasic course in 5-20%
11/6/2008
8
� ABC’s� IM Epinephrine: 0.01 mL/kg of a 1:1,000
solution (max =0.5 mg) � Beta-2 agonists if bronchospasm is present� Steroids: PO or IV� May blunt the late-phase response
� Antihistamines: may be more effective for cutaneous symptoms
A. Give inhaled beta-agonists (albuterol) via nebulizer
B. Give IV methylprednisoloneC. Give IV diphenhydramineD. Give SC/IM epinephrineE. Give IV epinephrine
� Observe for at least 6 to 8 hours� Discharge with injectable epinephrine� Consider in vitro (RAST) testing to identify
trigger
11/6/2008
9
� Amblyrhynchus (Ambly), a 6 yo girl, developed a URI a few days ago
� Increased coughing and trouble breathing since last night, despite using her albuterol every 4 hours.
� PMH: Asthma since age 3, no hospitalizations, but two ER visits in the past year
� VS: Afebrile, HR 120, R 45, O2 sat 97%. � Alert and awake, short sentences� Tachypneic, with increased work of
breathing, moderate retractions, very little air movement bilaterally, occasional wheeze
� You write her for 3 back-to-back duonebs(albuterol and ipratropium bromide)
� Her mother says, “can you write her for the new albuterol? her doctor told us it was better”
� R-enantiomer of albuterol � No demonstrated advantages over albuterol,
at equivalent doses: � 1.25 mg of levalbuterol=2.5 mg of racemic
albuterol� MAY have some advantage at lower doses
� More expensive, only approved for q8h use
� Routine use NOT recommended� Consider trial in select patients� Certain health plans: formulary outpatient
inhaler
11/6/2008
10
� Ambly is admitted overnight for frequent neb treatments and asthma teaching
� 2 months later she returns with another exacerbation, also requiring oral steroids
� Home from ward on beclomethasone 80mcg/puff, 1 puff bid
� She uses her albuterol twice a week during PE� Wakes up at night twice per week, uses her
albuterol and goes back to sleep
� You are concerned that her asthma control is sub-optimal
� However, you are intimidated by the “NEW ASTHMA GUIDELINES” you have been hearing about
� NHLBI released its 3rd Expert Panel Report (EPR-3) in August, 2007
� Assess asthma severity or control at each visit� Initiate or step up controller meds during
acute exacerbation� Inhaled corticosteroids (ICS) are first-line
medications for persistent asthma
� NHLBI released its 3rd Expert Panel Report (EPR-3) in August, 2007
� Assess asthma severity or control at each visit� Initiate or step up controller meds during
acute exacerbation� Inhaled corticosteroids (ICS) are first-line
medications for persistent asthma
11/6/2008
11
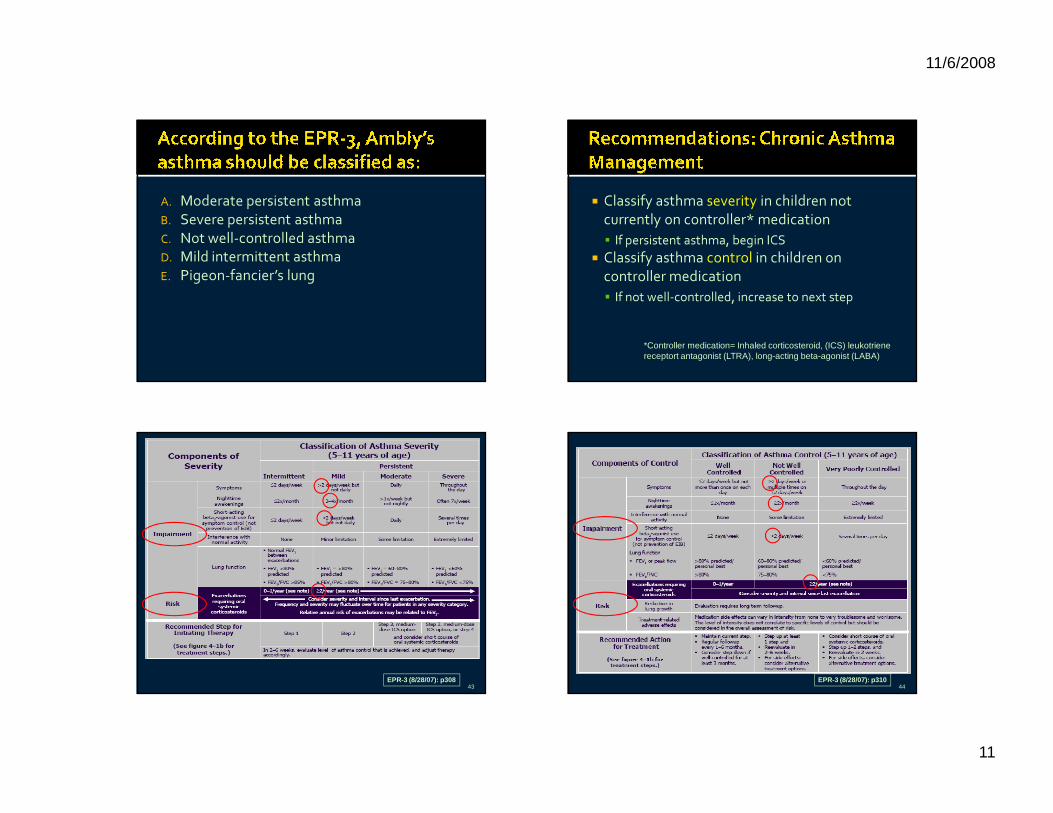
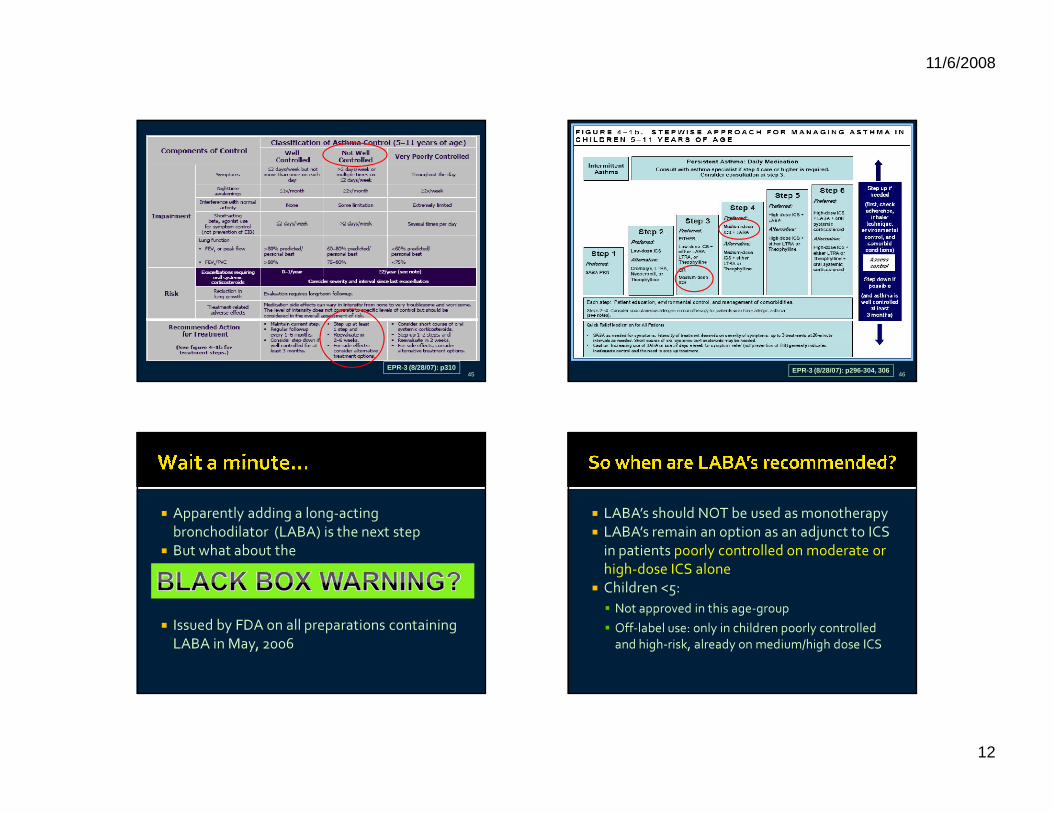
A. Moderate persistent asthmaB. Severe persistent asthmaC. Not well-controlled asthmaD. Mild intermittent asthmaE. Pigeon-fancier’s lung
� Classify asthma severity in children not currently on controller* medication� If persistent asthma, begin ICS
� Classify asthma control in children on controller medication� If not well-controlled, increase to next step
*Controller medication= Inhaled corticosteroid, (ICS) leukotriene receptort antagonist (LTRA), long-acting beta-agonist (LABA)
43EPR-3 (8/28/07): p308
44EPR-3 (8/28/07): p310
11/6/2008
12
45EPR-3 (8/28/07): p310
46EPR-3 (8/28/07): p296-304, 306
� Apparently adding a long-acting bronchodilator (LABA) is the next step
� But what about the
� Issued by FDA on all preparations containing LABA in May, 2006
� LABA’s should NOT be used as monotherapy� LABA’s remain an option as an adjunct to ICS
in patients poorly controlled on moderate or high-dose ICS alone
� Children <5:� Not approved in this age-group� Off-label use: only in children poorly controlled
and high-risk, already on medium/high dose ICS
11/6/2008
13
� You ask the medical student helping you with the case to refill Ambly’s albuterol, reminding her to write for the correct HFA inhaler that is covered by her insurance.
� She asks “what’s an HFA?”
A. Hooray for albuterolB. Having fun already?C. Happy flying artichokesD. Hydrofluoroalkane
� HFA propellant replaces ozone-toxic chlorofluorocarbons (CFC’s)
� HFA-MDI medication delivery to lungs, efficacy and safety comparable to CFC-MDI’s
� The old CFC-containing MDI’s are no longer available in pharmacies
11/6/2008
14
� Good seal over nose AND mouth
� One puff at a time� Count five breaths
� Fregata is an 18 month old toddler brought in because “his asthma suddenly got worse”
� Albuterol q4 hours for 2 days with a URI� Earlier in the day had choked on a piece of
popcorn. � Exam: alert and well-appearing, VS stable,
but tachypneic, with paroxysms of cough, during which he turns red
� Diffuse wheezing bilaterally
A. Blind finger sweepB. Heimlich maneuverC. Obtain inspiratory and expiratory chest filmsD. Obtain chest fluoroscopyE. Request rigid bronchoscopy
� Age: 1-3� More complications in young infants
� Foods most common objects� >90% in bronchi vs trachea
� Classic history in ~50%� Delay in diagnosis common, and associated
with morbidity
11/6/2008
15
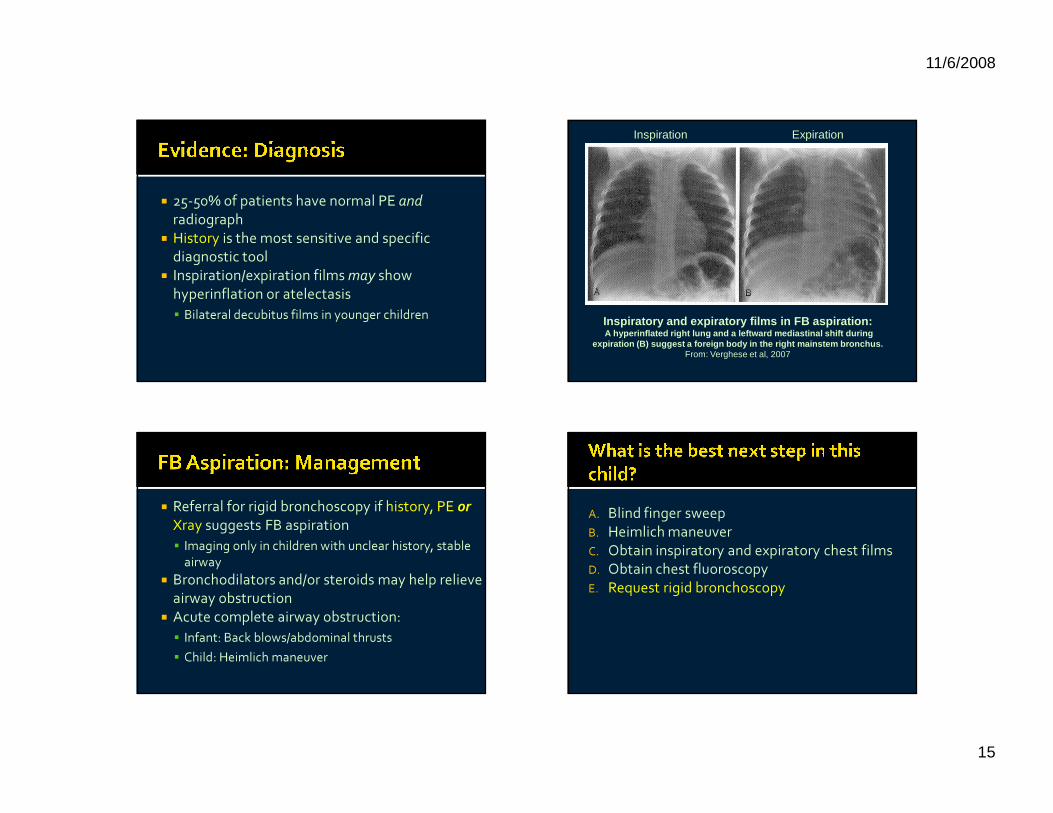
� 25-50% of patients have normal PE andradiograph
� History is the most sensitive and specific diagnostic tool
� Inspiration/expiration films may show hyperinflation or atelectasis� Bilateral decubitus films in younger children Inspiratory and expiratory films in FB aspiration:
A hyperinflated right lung and a leftward mediastinal shift during expiration (B) suggest a foreign body in the right mainstem bronchus.
From: Verghese et al, 2007
Inspiration Expiration
� Referral for rigid bronchoscopy if history, PE orXray suggests FB aspiration� Imaging only in children with unclear history, stable
airway� Bronchodilators and/or steroids may help relieve
airway obstruction� Acute complete airway obstruction: � Infant: Back blows/abdominal thrusts� Child: Heimlich maneuver
A. Blind finger sweepB. Heimlich maneuverC. Obtain inspiratory and expiratory chest filmsD. Obtain chest fluoroscopyE. Request rigid bronchoscopy
11/6/2008
16
� Clinical diagnosis most appropriate in most cases
� Lateral neck films may help narrow the diagnosis, but stabilize airway first
� Management for all: airway support and broad-spectrum antibiotics
� Consider in the child with upper airway obstruction without signs of infection
� IM epinephrine is the first-line drug
� History is the best diagnostic tool� Radiographs recommended only when
history is unclear, and airway is stable � Back blows/abdominal thrust or Heimlich
only for acute complete airway obstruction
� Albuterol still the first-line inhaled bronchodilator
� Classify EVERY ED patient according to 2007 guidelines
� Initiate or step up controllers based on classification
� Prescribe the correct HFA inhaler to ensure prompt receipt of medications
11/6/2008
17
Flightless CormorantPhalacrocorax harrisi
Waved AlbatrossPhoebastria irrorata
Magnificent FrigatebirdFregata magnificens
Galapagos Marine IguanaAmblyrhynchus cristatus
See you shortly for Part Two! Infectious and Neurologic EmergenciesAndi Marmor, MDNovember 6, 2008
11/6/2008
18
� The Febrile Child � Fever without a source� Meningitis
� ALTE� Diagnostic Testing and Disposition
� Imaging After Head Trauma
� Zalophus (Zal), a 2.5 mo old boy, presents to the ED with 2 days of fever
� On exam he is well-appearing, well-hydrated, febrile to 38.9
� No source can be found on exam or history� He is fully immunized for age, including his 1st
dose of PCV-7 1 week ago� He is uncircumcised
A. UA not needed because he is vaccinatedB. UA not needed because he is uncircumcisedC. Bag collection for urinalysisD. Catheter specimen for urinalysisE. Suprapubic tap for urinalysis
� Most common bacterial infection in FWS� Screen all infants<3 months of age with
T>38.5 and no source� Infants 3-24 months with FWS (T>39):� All girls� Uncircumcised boys < 12 mo of age� Circumcised boys < 6 mo of age
� Other factors to consider: length/height of fever, viral symptoms
11/6/2008
19
� Urine is collected for� Screening UA� Culture
� Cath urine accurate but invasive
� Bag may be less invasive� Contamination?
� Sensitivity: similar to cath specimen� Best NPV in low prior prob patients
� Specificity: lower than cath specimen� Bottom line:� If false positive results will negatively impact
patient, consider getting a cath instead
� At + threshold of >100,000 orgs, sens and spec are both ~85%
� Example:Prior prob PPV NPV
5% 23% 1%10% 40% 2%20% 60% 4%
� At + threshold of >100,000 orgs, sens and spec are both ~85%
� Example:Prior prob PPV NPV
5% 23% 1%10% 40% 2%20% 60% 4%
� The only clinically meaningful use of bag culture is to R/O UTI in low prevalence populations
11/6/2008
20
A. Testing not warranted because he is vaccinated
B. Testing not warranted because he is uncircumcised
C. Bag collection for urinalysisD. Catheter specimen for urinalysisE. Suprapubic tap for urinalysis
� You collect a cath urine on Zal and the dip is negative for LE and nitrites
� Now what?� Toss it?� Send it for culture?
� Leuk esterase� The most sensitive single test: 80-90%� Specificity is lower~ 70-85%
� Nitrites: high specificity (90-100%)� However, what you really want to know is the
Predictive Value � What is the chance of UTI if the UA is positive?� What is the chance of UTI is the UA is negative?
� Example: for LE onlyPrior prob PPV NPV5% 20% <1%10% 33% 1%20% 53% 3%
� Does the negative UA rule out UTI in our patient?
11/6/2008
21
� Example: for LE onlyPrior prob PPV NPV5% 20% <1%10% 33% 1%20% 53% 3%
� Does the negative UA rule out UTI in our patient?
� Not really!
� You collect a cath urine on Zal and the dip is negative for LE and nitrites
� Now what?� Toss it?� Send it for culture!
� There’s still no source for Zal’s fever, and you are concerned about occult serious bacterial infection (SBI)
A. Obtain a CBC/blood cx and LP; treat with ceftriaxoneB. Obtain a CBC/blood cx; treat with ceftriaxone if WBC
>15 or <5 C. Obtain a procalcitonin level, treat with ceftriaxone if >
0.12ng/dLD. Do not obtain any blood tests, as risk for SBI is very
lowE. Obtain a nasal RSV and flu test; obtain a CBC only if
this is negative
� Nearly 20% of febrile young childrenhave FWS
� A small proportion, although well-appearing, will have an occult serious bacterial infection (SBI) or urinary tract infection (UTI)� Vaccination with PCV-7 has drastically reduced
the risk of invasive pneumococcal disease (IPD)� Goal is to identify and treat children at
highest risk, without overtreating
11/6/2008
22
� Good response to PCV-7 after 2 doses� 2 wks to mount response
� Well-appearing, vaccinated children are at low risk for IPD/SBI (<0.5%)� Empiric CBC/blood cx NOT cost effective if rates
of SBI <0.5% (Lee, 2001) � Screen for UTI as for the unvaccinated child� Good follow up is essential!
� Neonates (< 1 month gestational age)� Full R/O sepsis workup and admission recommended
� 1 -3 months of age:� Screen for UTI in ALL young infants with FWS� WBC count still recommended: treat empirically if >15
or <5� > 3 months of age:� Consider age, partial vaccination and historical factors
(length/height of fever, presence of likely source, quality of follow up)
A. Obtain a CBC/blood cx and LP; treat with ceftriaxoneB. Obtain a CBC/blood cx; treat with ceftriaxone if WBC
>15 or <5 C. Obtain a procalcitonin level, treat with ceftriaxone if >
0.12ng/dLD. Do not obtain any blood tests, as risk for SBI is very
lowE. Obtain a nasal RSV and flu test; obtain a CBC only if
this is negative
A. Obtain a CBC/blood cx and LP; treat with ceftriaxoneB. Obtain a CBC/blood cx; treat with ceftriaxone if WBC
>15 or <5 C. Obtain a procalcitonin level, treat with ceftriaxone if >
0.12ng/dLD. Do not obtain any blood tests, as risk for SBI is very
lowE. Obtain a nasal RSV and flu test; obtain a CBC only if
this is negative
11/6/2008
23
� Various inflammatory mediators studied to predict SBI in young infants
� Mariaci et al– first large study in infants < 90 days
� Procalcitonin of <0.12ng/dL had sens of 95% and NPV of 96.5% for all SBI, and identified all cases of bacteremia
� Other studies recommend cutoff of 0.5, but have lower sensitivities
Pediatrics, Oct 2008; 122:701-710
A. Obtain a CBC/blood cx and LP; treat with ceftriaxoneB. Obtain a CBC/blood cx; treat with ceftriaxone if WBC
>15 or <5 C. Obtain a procalcitonin level, treat with ceftriaxone if >
0.12ng/dLD. Do not obtain any blood tests, as risk for SBI is very
lowE. Obtain a nasal RSV and flu test; obtain a CBC only if
this is negative
� A positive rapid viral test (RVT) significantly reduces probability of SBI/UTI
� RVT recommended when the results will change management� NPV best in infants with a low/mod probability of
SBI� Infants at high risk for UTI should be tested
for UTI regardless of viral diagnosis
� As the resident is setting up to place an IV and get labs, she notes that Zal is not looking well
� He appears lethargic with nuchal rigidity, and there is now a full fontanelle on exam
� You suspect meningitis
11/6/2008
24
A. Obtain a lumbar punctureB. Administer ampicillin, gentamicin and
acyclovir IVC. Administer dexamethasone 0.15mg/kg IVD. Administer ceftriaxone IVE. Administer ceftriaxone and vancomycin IV
� 1997 meta-analysis of trials since 1988:� Reduction in morbidity/mortality in both H.
influenza or S. pneumo meningitis (McIntyre)� Cochrane review 2007:� “Adjuvant corticosteroids are beneficial in the
treatment of children with acute bacterial meningitis”
� No studies have shown worse outcomes, serious adverse events or decreased antibiotic concentration in CSF
� Infants/children >6 weeks of age: � Steroids recommended prior to initiating
antibiotic therapy in suspected or proven meningitis due to S. pneumo or H. influenza
� Dexamethasone: 0.15mg/kg every 6 hours � No benefit shown for� Neonatal meningitis (eg: gram-neg, Listeria)� Developing countries� Steroids given after first dose of antibiotics
A. Obtain a lumbar punctureB. Administer ampicillin, gentamicin and
acyclovir IVC. Administer dexamethasone 0.15mg/kg IVD. Administer ceftriaxone IVE. Administer ceftriaxone and vancomycin IV
11/6/2008
25
A. Obtain a lumbar punctureB. Administer ampicillin, gentamicin and
acyclovir IVC. Administer dexamethasone 0.15mg/kg IVD. Administer ceftriaxone IVE. Administer ceftriaxone and vancomycin IV
� Combined treatment with a 3 cephalosporin and vancomycin recommended
� Some data suggests that a delay in administration of vancomycin for 2 hours may reduce risk of hearing loss without adverse effects
� Geochelone (Geo) is a 3 month old brought in by ambulance after he “stopped breathing”
� Taking a nap on his dad’s chest when he seemed to gag and made a funny noise.
� Face looked purple, he was limp and “not breathing”, dad thought he was dead
� He called for mom, who called 911, and in the commotion Geo gasped and started to cry
� PMH: Ex 34 weeker, home after 1 week obs for feeding and growing
� Exam: sleeping comfortably� VS: T 36.7 P 140 R 35 BP 80/40� Exam is entirely normal, including normal lung,
cardiac, abdominal and neurologic exam for age� This kid had an ALTE
11/6/2008
26
1. Apparent apnea2. Color change3. Change in muscle tone4. Choking/gagging5. Frightening to observer
� 2 major concerns� Risk of subsequent episodes▪ Varies from 0-24%, mortality <1%
� Underlying serious condition� 2 major questions� Diagnostic testing?� Admission?
A. Dad had to blow in his face to get him to breathe
B. The episode was associated with a recent feeding
C. Inability to find a cause for the ALTE in the EDD. Another event occurs in the EDE. His eyes appeared to roll back in his head
� Most common diagnoses:� GERD: 31%� Unknown: 23%� Seizure: 11%� LRTI: 8%� Other: metabolic disease, ENT disorder, toxin,
UTI, cardiac, abuse (each ~1%)� NOT related to SIDS
11/6/2008
27
� Most studies are of hospitalized infants� H and P diagnostic or guided testing in the
majority of cases (~70-100%)� H and P alone in 20-50%
� Which tests are most useful when H and P does not reveal diagnosis?� Brand (2005): 5 tests identified ALL cases � GER screen, UA/cx, head CT, WBC count,
pneumogram
� Claudius (2007): � ALL children who required hospitalization had h/o
multiple events, or were premature (NPV of 100%)� Other: social risks, prolonged/severe event, ill
appearance� Bonkowsky (2008):� Few predictors for abuse, epilepsy at presentation� 11% eventually diagnosed with abuse/neglect
A. Dad had to blow in his face to get him to breathe
B. The episode was associated with a recent feeding
C. Inability to find a cause for the ALTE in the EDD. Another event occurs in the EDE. His eyes appeared to roll back in his head
� Complete H and P in all patients: � Testing NOT needed if H and P reveals diagnosis� Focused testing based on H and P if not conclusive
� High yield testing targeted towards GERD, LRTI
� Admission� Ill appearance, severe /recurrent episodes,
premature, progressive condition� CONSIDER if dx unclear, high parental anxiety
11/6/2008
28
� Sula is a 9 month old boy brought in by his babysitter 30 minutes after he is knocked over in his high chair by the family dog � She had turned her back, heard a crash and found
Sula on the tile floor “stunned”, then he started to cry� She fed him 15 minutes later and he vomited
� Exam: VSS, somewhat fussy but consolable, he drinks from a bottle, has a non-focal neuro exam and a 1X2 cm abrasion on his forehead
A. Head CT scanB. Plain skull filmsC. Head UltrasoundD. Observation in ED for 4-6 hoursE. Discharge if caregiver is reliable
� Intracranial injury (ICI) occurs in ~3%-7% of children <18 with apparently minor HT
� Reasons for selective imaging strategies: � Minimize unnecessary radiation, sedation � Identify kids with clinically significant ICI
� Intracranial injury (ICI) occurs in ~3%-7% of children <18 with apparently minor HT
� Reasons for selective imaging strategies: � Minimize unnecessary radiation, sedation � Identify kids with clinically significant ICI
11/6/2008
29
� Children especially vulnerable to lifetime cancer risks from CT scan radiation� 16% of CT-attributable cancer deaths are in kids
� Estimates of lifetime cancer mortality risk attributable to CT scan: � 1 year old child: 0.07% (1/1500) from head CT� Children <15: of 600,000 head/abd scans done
yearly, 500 kids will die per year (0.35% increase over baseline yearly cancer mortality rate)
� The population of interest is those with GCS>13, and relatively minor mechanism
� 1999 AAP Guideline� NO symptoms and NO evidence of skull fracture� Imaging based on h/o LOC
� Brief LOC no longer considered predictive� Palchak, 2004: NO kids with Isolated LOC/amnesia
WITHOUT any other signs/symptoms had ICI
� Abnormal behavior� Concern for child abuse/unclear mechanism� Seizure?� Headache?� Vomiting?� Age <2
� Altered mental status/focal neurologic findings� Duh…
� Scalp hematoma� Evidence of skull fracture
11/6/2008
30
� UC Davis Rule1. Abn MS2. Evident skull fx3. Vomiting4. Scalp hematoma5. Headache
NPV: 99.7%
� UCLA Rule1. Abn MS2. Evident skull fx3. Hi-risk vomiting4. Scalp hematoma5. Severe/
progressive HA
NPV: 98%
� NEXUS II 1. Abn behavior2. Neuro deficit3. Altered alertness4. Evident skull fx5. Persist vomiting6. Scalp hematoma7. Coagulopathy
NPV: 99%
� UC Davis Rule1. Abn MS2. Evident skull fx3. Vomiting4. Scalp hematoma5. Headache
NPV: 99.7%
� UCLA Rule1. Abn MS2. Evident skull fx3. Hi-risk vomiting4. Scalp hematoma5. Severe/
progressive HA
NPV: 98%
� NEXUS II 1. Abn behavior2. Neuro deficit3. Altered alertness4. Evident skull fx5. Persist vomiting6. Scalp hematoma7. Coagulopathy
NPV: 99%
� Scan recommended in:� Any child with altered mental status, abnormal
neuro exam, or clinical evidence of skull fracture at the time of evaluation� Unclear mechanism or suspicion of child abuse
� Scan vs observe:� Those with persistent vomiting, severe headache
� Observe/DC without scan if:� No vomiting, no headache
� What about the child <2?
� Most guidelines suggest a “lower threshold” for imaging children <2 � Higher rates of ICI in those <3 mo (13%)� Higher rates of occult ICI▪ Up to 48% of infants with ICI asymptomatic (Greenes, 1999)
� Higher risk for skull fractures (6-30%)� Higher risk for non-accidental trauma
� Selective imaging more important in infants� Risks of sedation, radiation
11/6/2008
31
� Lack of symptoms NOT a good negative predictor of ICI in infants
� Historical predictors: � Younger age (<6 mo)� Fall >3 feet� Suspicion of abuse, or unclear mechanism
� Focal neurologic findings � Skull fracture (SF)� Positive predictive value 15-30% � Sensitivity best in young infants (60-100%)
� Scalp swelling/hematoma� 80-100% sensitive for SF� NPV for asymptomatic AND no scalp hematoma =
99.6% (Greenes, Palchak)
� Use history and exam to stratify into High, Intermediate or Low Risk
� High Risk (symptomatic) = Obtain CT scan� Altered MS/Focal neuro findings� Signs of skull fracture� Prolonged LOC or persistent vomiting
� Intermediate risk: Imaging or observation for 4-6 hours � Occult ICI most likely if:▪ <6 mo of age, scalp hematoma, higher force
mechanisms, unwitnessed, h/o abnormal behavior� Low Risk: may be discharged without CT� Asymptomatic AND no scalp hematoma AND no
risk factors
11/6/2008
32
� Intermediate risk: Imaging or observation for 4-6 hours � Occult ICI most likely if:▪ <6 mo of age, scalp hematoma, higher force
mechanisms, unwitnessed, h/o abnormal behavior� Low Risk: may be discharged without CT� Asymptomatic AND no scalp hematoma AND no
risk factors
� Reliable caregiver� No significant extracranial injuries or other
indications for admission� Normal neuro exam and normal mental
status� No suspicion for abuse or neglect
A. CT scanB. Plain skull filmsC. Head UltrasoundD. Observation for 4-6 hoursE. Discharge if caregiver is reliable
A. CT scanB. Plain skull filmsC. Head UltrasoundD. Observation for 4-6 hoursE. Discharge if caregiver is reliable
11/6/2008
33
� Well-appearing, vaccinated children (≥2 doses) are at low risk of invasive pneumococcal disease� Screen for UTI as recommended
� For young/unvaccinated infants, WBC is still recommended to stratify into high/low risk� Watch for more data on procalcitonin and other
mediators� A positive viral test reduces chance of SBI and UTI
and may change management in lower risk patients
� If patient is high risk, obtain cath specimen� Begin empiric therapy if UA positive� Send for culture anyway if negative
� In low/moderate risk patients, bag urine for UA is fine, but discard if negative
� Steroids should be given as soon as meningitis is suspected in infant >6 weeks� Follow promptly with LP/antibiotics
� Ceftriaxone/cefotaxime and vancomycin recommended as empiric antibiotics� Consider delay in vancomycin for 2 hours
� H and P +/- targeted testing likely to reveal diagnosis in majority of patients
� If diagnosis unclear, admission recommended for infants with � Multiple/severe episodes� Prematurity � Suspicion for child abuse or social concerns
11/6/2008
34
� Selective imaging the goal for all children� For children >2: � Abnormal MS/neuro exam or signs of skull fracture
the most important predictors of ICI� Decision rules may reduce unnecessary scans, but
need validation� For children < 2: � CT scan or observation recommended if symptomatic
or scalp hematoma/ signs of skull fracture� High-impact mechanism and unclear history are
additional risk factors
Giant TortoiseGeochelone elephantopus
Blue-footed BoobySula neboxuii
Galapagos Sea LionZalophus wollebaeki
� 5� 13� 26� 41� 55� 71� 83� 93� 103� 110
11/6/2008
35
� Okapi, an 8 mo old boy, has 3 days of runny nose, 2 d of fever to 39 and fussiness
� He is well-hydrated and well-appearing, but on exam the R eardrum is erythemetous, bulging and opaque
� Mom says he received amoxicillin for AOM 6 weeks ago
A. Observe without antibioticsB. Amoxicillin 40-50mg/kg/dayC. Amoxicillin 80-90mg/kg/dayD. Augmentin, since he has recurrent/ persistent
AOME. Azithromycin, since he has recurrent/
persistent OM
� Long history of management without antibiotics outside of U.S.
� Potential benefits of observation without antibiotics� Fewer side effects� Reduce bacterial resistance
� Potential downsides:� Longer duration of illness� More complications
11/6/2008
36
� Overall, the majority of children with AOM do well, whether or not they are treated with antibiotics
� However, antibiotics improve rates of cure� Randomized trial in UK:○ 70% vs 86% improved at 3 days
� AHRQ meta-analysis: ○ 12.3% lower clinical failure with antibiotics (NNT=8)○ 1 day shorter symptoms in 5-14% of children (NNT 7-20)
� Greatest difference found in children with more severe illness and younger age
� Rates have decreased in the post-antibiotic era� Rates higher in countries which do not treat with antibiotics� HOWEVER: � Rates of mastoiditis comparable (0.6 vs 0.2%) in children treated with/without antibiotics (AHRQ meta-analysis)� Majority of complicated cases treated with prior antibiotics
� Overall, little evidence supports use of antibiotics to reduce complications from AOM
� Recent AAP/AAFP guidelines based on review of available evidence
1. Consider diagnostic certainty in management2. Assess and treat pain in all children3. Consider observation without antibiotics in
selected children4. Specific antibiotics for initial/resistant infection5. Reduction of risk factors
� Recent AAP/AAFP guidelines based on review of available evidence
1. Consider diagnostic certainty in management2. Assess and treat pain in all children3. Consider observation without antibiotics in
selected children4. Specific antibiotics for initial/resistant infection5. Reduction of risk factors
11/6/2008
37
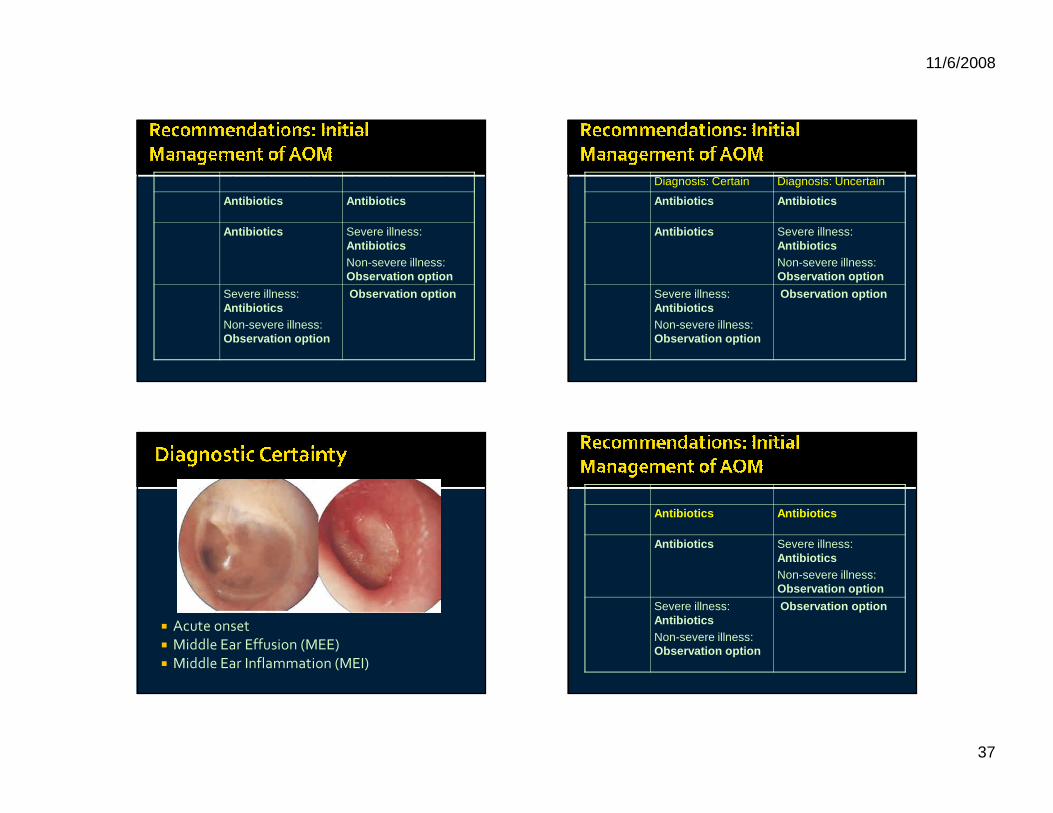
Age Diagnosis: Certain Diagnosis: Uncertain
<6 months Antibiotics Antibiotics
6 mo-2 yrs Antibiotics Severe illness: AntibioticsNon-severe illness:Observation option
>2 years Severe illness: AntibioticsNon-severe illness: Observation option
Observation option
Age Diagnosis: Certain Diagnosis: Uncertain
<6 months Antibiotics Antibiotics
6 mo-2 yrs Antibiotics Severe illness: AntibioticsNon-severe illness:Observation option
>2 years Severe illness: AntibioticsNon-severe illness: Observation option
Observation option
� Acute onset� Middle Ear Effusion (MEE)� Middle Ear Inflammation (MEI)
Age Diagnosis: Certain Diagnosis: Uncertain
<6 months Antibiotics Antibiotics
6 mo-2 yrs Antibiotics Severe illness: AntibioticsNon-severe illness:Observation option
>2 years Severe illness: AntibioticsNon-severe illness: Observation option
Observation option
11/6/2008
38
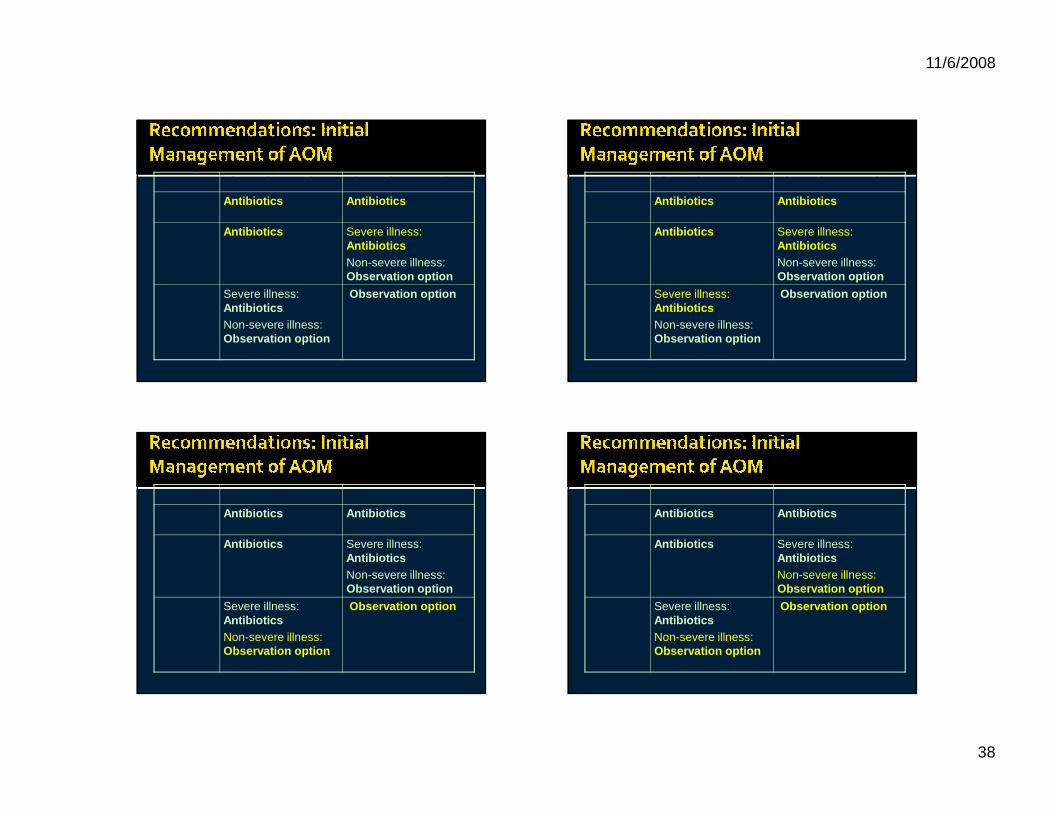
Age Diagnosis: Certain Diagnosis: Uncertain
<6 months Antibiotics Antibiotics
6 mo-2 yrs Antibiotics Severe illness: AntibioticsNon-severe illness:Observation option
>2 years Severe illness: AntibioticsNon-severe illness: Observation option
Observation option
Age Diagnosis: Certain Diagnosis: Uncertain
<6 months Antibiotics Antibiotics
6 mo-2 yrs Antibiotics Severe illness: AntibioticsNon-severe illness:Observation option
>2 years Severe illness: AntibioticsNon-severe illness: Observation option
Observation option
Age Diagnosis: Certain Diagnosis: Uncertain
<6 months Antibiotics Antibiotics
6 mo-2 yrs Antibiotics Severe illness: AntibioticsNon-severe illness:Observation option
>2 years Severe illness: AntibioticsNon-severe illness: Observation option
Observation option
Age Diagnosis: Certain Diagnosis: Uncertain
<6 months Antibiotics Antibiotics
6 mo-2 yrs Antibiotics Severe illness: AntibioticsNon-severe illness:Observation option
>2 years Severe illness: AntibioticsNon-severe illness: Observation option
Observation option
11/6/2008
39
�Family agrees with plan�Able to observe and assess child�Communication/transportation available
� Based on Okapi’s age (6 mo to 2 years), high fever and certain diagnosis, you decide he should be managed with initial antibiotic therapy
� What is the best initial choice for antibiotics?
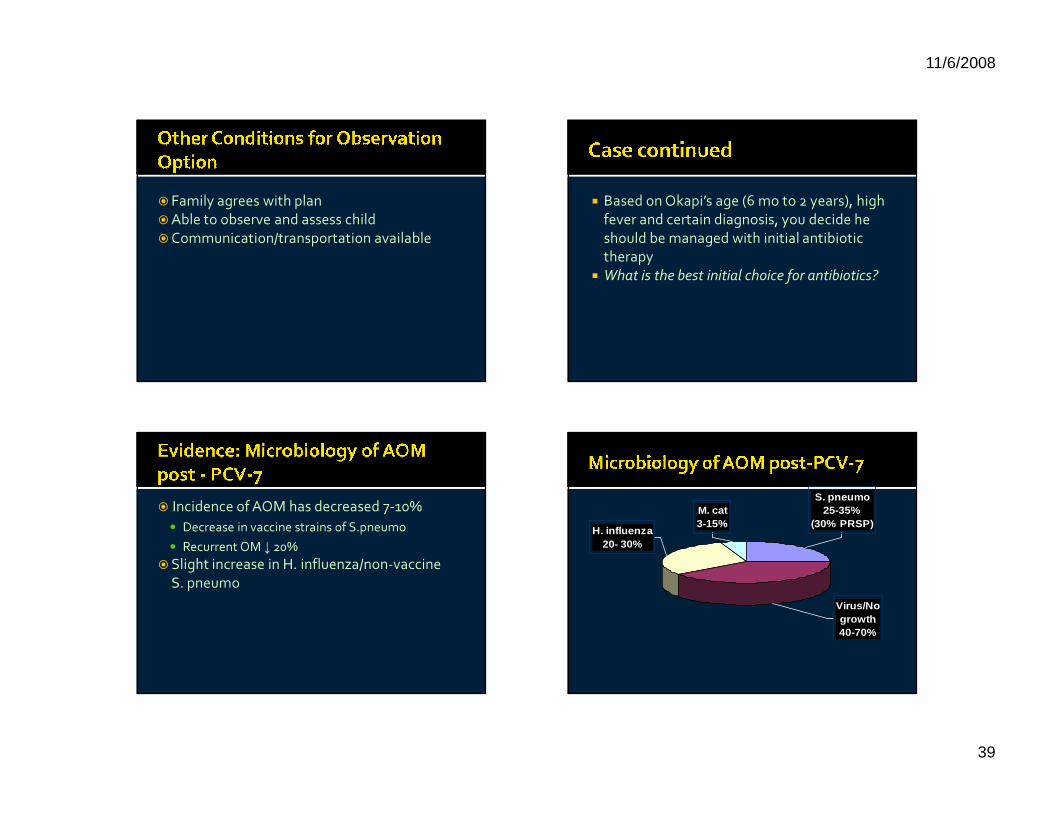
� Incidence of AOM has decreased 7-10%� Decrease in vaccine strains of S.pneumo� Recurrent OM ↓ 20%
�Slight increase in H. influenza/non-vaccine S. pneumo
Virus/No growth 40-70%
H. influenza 20- 30%
M. cat 3-15%
S. pneumo 25-35%
(30% PRSP)
11/6/2008
40
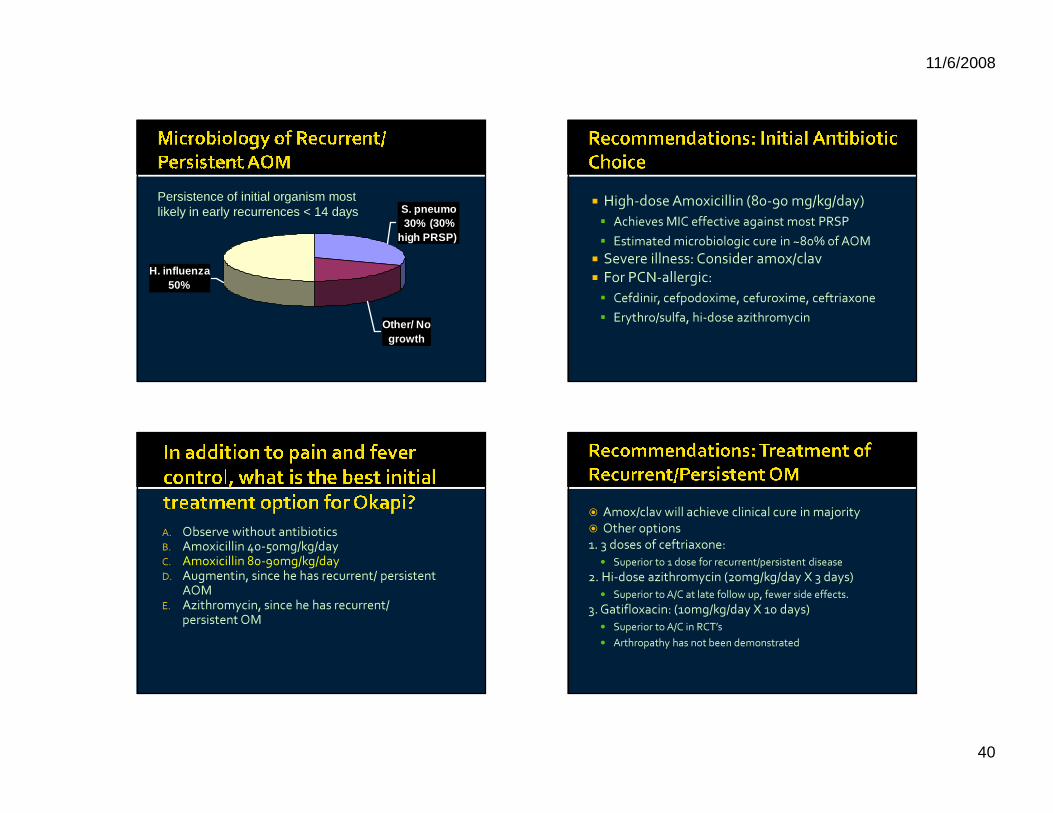
S. pneumo 30% (30%
high PRSP)
Other/ No growth
H. influenza 50%
Persistence of initial organism most likely in early recurrences < 14 days
� High-dose Amoxicillin (80-90 mg/kg/day)� Achieves MIC effective against most PRSP � Estimated microbiologic cure in ~80% of AOM
� Severe illness: Consider amox/clav� For PCN-allergic:� Cefdinir, cefpodoxime, cefuroxime, ceftriaxone� Erythro/sulfa, hi-dose azithromycin
A. Observe without antibioticsB. Amoxicillin 40-50mg/kg/dayC. Amoxicillin 80-90mg/kg/dayD. Augmentin, since he has recurrent/ persistent
AOME. Azithromycin, since he has recurrent/
persistent OM
� Amox/clav will achieve clinical cure in majority� Other options1. 3 doses of ceftriaxone: � Superior to 1 dose for recurrent/persistent disease
2. Hi-dose azithromycin (20mg/kg/day X 3 days)� Superior to A/C at late follow up, fewer side effects.
3. Gatifloxacin: (10mg/kg/day X 10 days)� Superior to A/C in RCT’s� Arthropathy has not been demonstrated
11/6/2008
41
� 1 point each for anorexia, fever, nausea/vomiting, leukocytosis, L shift, migration of pain
� 2 points each for RLQ pain on cough/percussion/hopping, and RLQ tenderness
� Score ≥6 considered: go to surgery� Reported PPV 96/NPV 99 (in same cohort
used to derive the rule!)
� 1 point each for migration, anorexia, nausea/vomiting, rebound pain, fever, left shift
� 2 points each for RLQ tenderness and WBC > 10K
� Score ≥7 considered “probable appendicitis” (9-10= very probable)
� Reported PPV: 92%/NPV 46%
� 8 criteria with increasing point values (gender, severe pain, vomiting, fever, migration, RLQ pain, guarding, rebound)
� Score > 21: PPV 73%� Score < 15: NPV 96%
� 588 patients evaluated by a surgeon for suspected appendicitis
� 34% of them had appendicitis� Alvarado and PAS scores did not perform well
enough to send pt straight to surgery