Asthma management from a solo QTIP practice prospective
23
Mariana Ciobanu, MD,FAAP Mariana Ciobanu, MD,FAAP Carolina Pediatrics-Cheraw Carolina Pediatrics-Cheraw QTIP July 2012 Collaborative meeting QTIP July 2012 Collaborative meeting Asthma management Asthma management from a solo QTIP from a solo QTIP practice practice prospective prospective
-
Upload
wing-clayton -
Category
Documents
-
view
18 -
download
2
description
Mariana Ciobanu , MD,FAAP Carolina Pediatrics-Cheraw QTIP July 2012 Collaborative meeting. Asthma management from a solo QTIP practice prospective. - PowerPoint PPT Presentation
Transcript of Asthma management from a solo QTIP practice prospective
Mariana Ciobanu, MD,FAAPMariana Ciobanu, MD,FAAP
Carolina Pediatrics-CherawCarolina Pediatrics-Cheraw
QTIP July 2012 Collaborative meetingQTIP July 2012 Collaborative meeting
Asthma management Asthma management from a solo QTIP from a solo QTIP practice prospectivepractice prospective
To better understand how to To better understand how to differentiate between infants who differentiate between infants who wheeze and go on to develop asthma wheeze and go on to develop asthma and those who wheeze but do not go and those who wheeze but do not go on to have asthmaon to have asthma
To discuss management strategies To discuss management strategies for treating children with a high risk for treating children with a high risk of developing asthmaof developing asthma
To discuss possible prevention To discuss possible prevention therapies for asthma in children four therapies for asthma in children four years old or youngeryears old or younger
ObjectivesObjectives
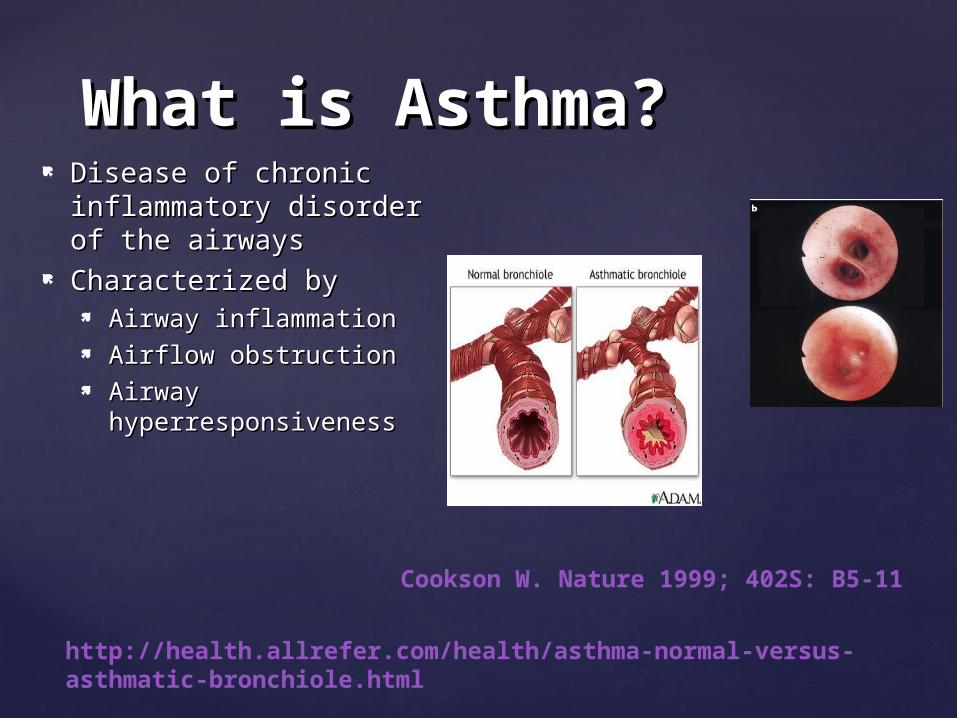
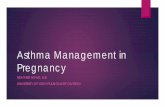
What is Asthma?What is Asthma? Disease of chronic Disease of chronic
inflammatory disorder of inflammatory disorder of the airwaysthe airways
Characterized byCharacterized by Airway inflammationAirway inflammation Airflow obstructionAirflow obstruction Airway Airway
hyperresponsivenesshyperresponsiveness
http://health.allrefer.com/health/asthma-normal-versus-asthmatic-bronchiole.html
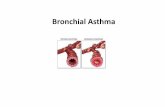
Cookson W. Nature 1999; 402S: B5-11
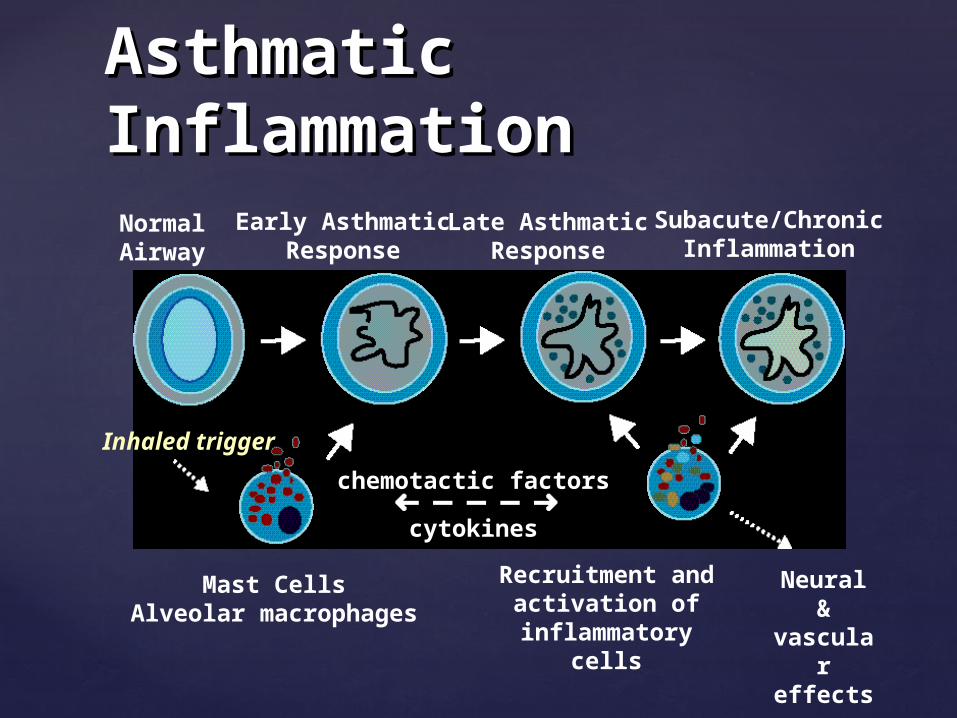
Asthmatic Asthmatic InflammationInflammation
NormalAirway
Mast CellsAlveolar macrophages
Recruitment andactivation of
inflammatory cells
Subacute/ChronicInflammation
Neural &vascular effects
Late AsthmaticResponse
Early AsthmaticResponse
chemotactic factors
cytokines
Inhaled trigger
Asthma is a complex traitAsthma is a complex trait Heritable and environmental factors contribute to its Heritable and environmental factors contribute to its
pathogenesis. Viral infections appears have an pathogenesis. Viral infections appears have an expanding role as well.expanding role as well.
Onset appears early in life and severity remains Onset appears early in life and severity remains constantconstant
Multiple interacting genesMultiple interacting genes At least 20 distinct chromosomal regions with linkage to At least 20 distinct chromosomal regions with linkage to
asthma and asthma related traits have been identified: asthma and asthma related traits have been identified: Chromosome 5q Chromosome 5q , ADAM33, ADAM33 , , PHF11PHF11
What Causes What Causes Asthma?Asthma?
Potential Risk Potential Risk FactorsFactors11
Host factorsHost factors Genetic predispositionGenetic predisposition AtopyAtopy Airway Airway
hyperresponsivenesshyperresponsiveness GenderGender Race/EthnicityRace/Ethnicity
Environmental factorsEnvironmental factors Indoor allergensIndoor allergens Outdoor allergensOutdoor allergens Occupational sensitizerOccupational sensitizer
Environmental factors Environmental factors (cont)(cont) Tobacco smokeTobacco smoke Air pollutionAir pollution Respiratory infectionsRespiratory infections Socioeconomic statusSocioeconomic status Family sizeFamily size Diet and drugsDiet and drugs ObesityObesity
1Masoli M, et al. The Global Burden of Asthma: Executive Summary of the GINA Dissemination Committee Report. Allergy 2004; 59: 469-78.

Clinical diagnosis supported by the Clinical diagnosis supported by the certain historical, physical and certain historical, physical and laboratory findingslaboratory findings History of episodic symptoms of airflow obstruction History of episodic symptoms of airflow obstruction
(e.g.. breathlessness, wheezing, and (e.g.. breathlessness, wheezing, and COUGHCOUGH)-)-response to therapy!response to therapy!
Physical: wheeze, hyperinflationPhysical: wheeze, hyperinflation Laboratory: exhaled nitric oxide (eNO), spirometry Laboratory: exhaled nitric oxide (eNO), spirometry
Exclude other possibilitiesExclude other possibilities
Diagnosing Asthma-Diagnosing Asthma-Not EasyNot Easy
AsthmaAsthma Congenital Anomalies with airway impingement: Congenital Anomalies with airway impingement:
Vascular rings, tracheobronchial obstruction, Vascular rings, tracheobronchial obstruction, mediastinal mass mediastinal mass
Bronchopulmonary dysplasia Bronchopulmonary dysplasia Cystic fibrosis Cystic fibrosis Gastroesophageal reflux Gastroesophageal reflux Aspiration Aspiration Foreign Body Aspiration Foreign Body Aspiration Heart Failure Heart Failure Sinusitis and allergic rhinitisSinusitis and allergic rhinitis Bronchiolitis Bronchiolitis Pertussis Pertussis Tuberculosis Tuberculosis Immune system Disorders Immune system Disorders
Differential Diagnosis Differential Diagnosis WheezingWheezing
Group 1: Low Lung function: children Group 1: Low Lung function: children improve within a few years and "outgrow" improve within a few years and "outgrow" their asthmatheir asthma
Group 2: Non-Atopic, viral-induced asthma: Group 2: Non-Atopic, viral-induced asthma: also outgrow asthma after a somewhat also outgrow asthma after a somewhat longer period of time (nonatopic longer period of time (nonatopic wheezing).wheezing).
Group 3: Atopic Asthma: in contrast, Group 3: Atopic Asthma: in contrast, children who will go on to develop children who will go on to develop persistent wheezing beyond infancy and persistent wheezing beyond infancy and early childhood usually have a family early childhood usually have a family history of asthma and allergies and present history of asthma and allergies and present with allergic symptoms very early in life with allergic symptoms very early in life (atopy-associated asthma).(atopy-associated asthma).
Wheezing in InfantsWheezing in Infants
Diagnosing Asthma in Young Diagnosing Asthma in Young Children – Asthma Predictive Children – Asthma Predictive IndexIndex
>> 4 episodes/yr of 4 episodes/yr of wheezing lasting more wheezing lasting more than 1 day affecting than 1 day affecting sleep in a child with one sleep in a child with one MAJOR or two MINOR MAJOR or two MINOR criteriacriteria
Major criteriaMajor criteria Parent with asthmaParent with asthma Physician diagnosed Physician diagnosed
atopic dermatitisatopic dermatitis Minor criteriaMinor criteria
Physician diagnosed Physician diagnosed allergic rhinitisallergic rhinitis
Eosinophilia (Eosinophilia (>>4%)4%) Wheezing apart from Wheezing apart from
coldscolds
1Adapted from Castro-Rodriquez JA, et al. AJRCCM 2000; 162: 1403
Identify precipitating factors (pets, ETS, Identify precipitating factors (pets, ETS, mold second hand smoking exposure)mold second hand smoking exposure)
Identify comorbid conditions that may Identify comorbid conditions that may aggravate asthma (GERD, allergies etc)aggravate asthma (GERD, allergies etc)
Assess the patient/families knowledge Assess the patient/families knowledge and self management skillsand self management skills
Classify asthma severity using the Classify asthma severity using the Guidelines from the NHLBI (Expert Guidelines from the NHLBI (Expert Panel)Panel)
Asthma Diagnosis Asthma Diagnosis MadeMade
Use Impairment and RiskUse Impairment and Risk ImpairmentImpairment
Symptoms: night time symptoms, reliever Symptoms: night time symptoms, reliever use (SABA), miss school/work, quality of use (SABA), miss school/work, quality of life, ACT screenlife, ACT screen
Lung function- spirometry (FEV0.5), eNOLung function- spirometry (FEV0.5), eNO RiskRisk
Recurrent exacerbations including ED Recurrent exacerbations including ED visits and hospitalization (may be normal visits and hospitalization (may be normal between events)between events)
At times, hard to differential between At times, hard to differential between impairment and risk impairment and risk
Assessing Asthma Assessing Asthma SeveritySeverity
Break down into intermittent, mild, Break down into intermittent, mild, moderate, or severe persistent asthma moderate, or severe persistent asthma depending on symptoms of impairment depending on symptoms of impairment and riskand risk
Once classified, use the 6 steps depending Once classified, use the 6 steps depending on the severity to obtain asthma control on the severity to obtain asthma control with the lowest amount of medicationwith the lowest amount of medication
Controller medications (inhaled steroids) Controller medications (inhaled steroids) should be considered if >4 should be considered if >4 exacerbations/year, 2 episodes of oral exacerbations/year, 2 episodes of oral steroids in 6 months, or use of SABA’s steroids in 6 months, or use of SABA’s (albuterol) more then twice a week(albuterol) more then twice a week
Classifying Asthma Classifying Asthma Severity in Children 0-4 Severity in Children 0-4 Years of AgeYears of Age
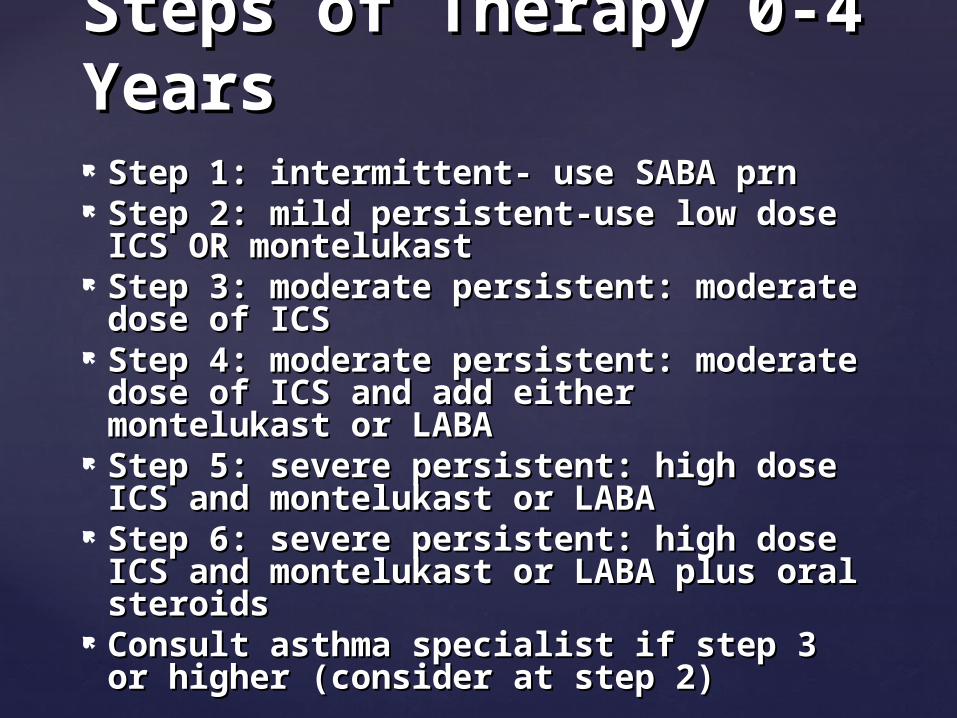
Step 1: intermittent- use SABA prnStep 1: intermittent- use SABA prn Step 2: mild persistent-use low dose Step 2: mild persistent-use low dose
ICS OR montelukastICS OR montelukast Step 3: moderate persistent: moderate Step 3: moderate persistent: moderate
dose of ICSdose of ICS Step 4: moderate persistent: moderate Step 4: moderate persistent: moderate
dose of ICS and add either dose of ICS and add either montelukast or LABAmontelukast or LABA
Step 5: severe persistent: high dose Step 5: severe persistent: high dose ICS and montelukast or LABAICS and montelukast or LABA
Step 6: severe persistent: high dose Step 6: severe persistent: high dose ICS and montelukast or LABA plus oral ICS and montelukast or LABA plus oral steroidssteroids
Consult asthma specialist if step 3 or Consult asthma specialist if step 3 or higher (consider at step 2)higher (consider at step 2)
Steps of Therapy 0-4 Steps of Therapy 0-4 YearsYears
Asthma ManagementAsthma Management
Goals of therapyGoals of therapy Prevent symptomsPrevent symptoms Maintain (near) “normal” PFMaintain (near) “normal” PF Maintain normal activity Maintain normal activity Prevent exacerbations & minimize ER Prevent exacerbations & minimize ER
visits/hospitalizationsvisits/hospitalizations Optimal drug tx, minimal problems Optimal drug tx, minimal problems Patient/family satisfaction Patient/family satisfaction
Monitor carefully- every 3-6 months Monitor carefully- every 3-6 months if stable, more often if not(1 wk f/u if stable, more often if not(1 wk f/u app after an acute episode)app after an acute episode)
If stable after 3 months, try to If stable after 3 months, try to reduce therapy (usually by 25-50%)reduce therapy (usually by 25-50%)
Inhaled steroids are safe even in the Inhaled steroids are safe even in the young at mild to moderate doses young at mild to moderate doses with only a slight decrease in with only a slight decrease in growth velocity. Higher doses have growth velocity. Higher doses have been shown to affect growth, cause been shown to affect growth, cause cataracts and reduce bone densitycataracts and reduce bone density
Response to therapy is very Response to therapy is very important in this age group!important in this age group!
Maintaining ControlMaintaining Control

Managing Asthma: Managing Asthma: Asthma Action PlanAsthma Action Plan
Develop with a physician Develop with a physician
Tailor to meet individual needsTailor to meet individual needs
Educate patients and families about all aspects Educate patients and families about all aspects of planof plan Recognizing symptomsRecognizing symptoms Medication benefits and side effectsMedication benefits and side effects Proper use of inhalers and Peak Expiratory Flow Proper use of inhalers and Peak Expiratory Flow
(PEF) meters(PEF) meters
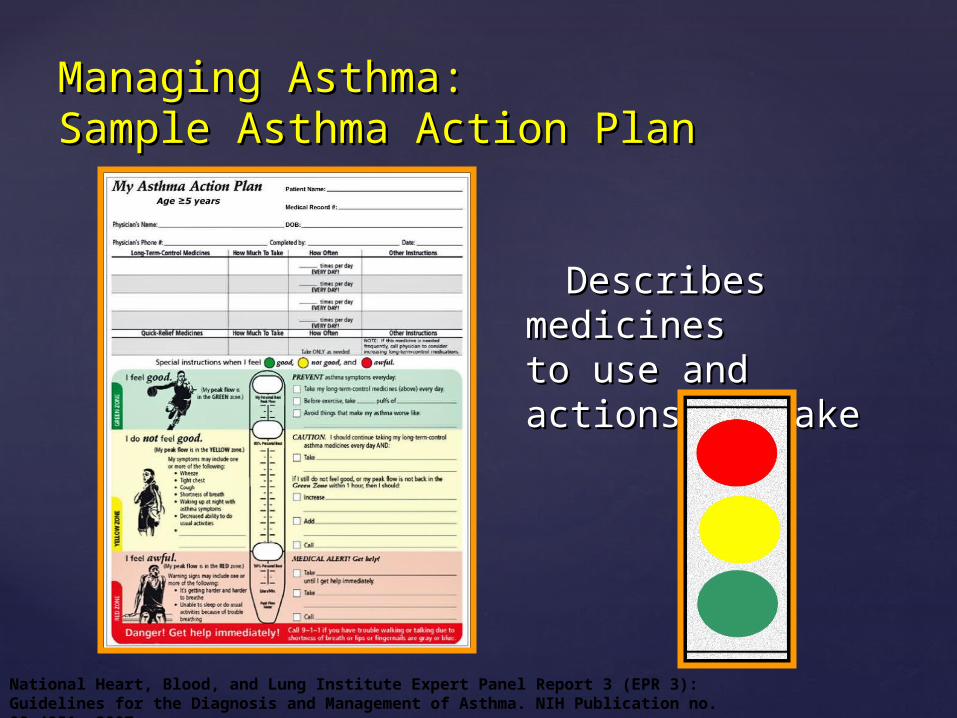
Managing Asthma: Managing Asthma: Sample Asthma Action PlanSample Asthma Action Plan
Describes medicines Describes medicines to use and actions to to use and actions to taketake
National Heart, Blood, and Lung Institute Expert Panel Report 3 (EPR 3): Guidelines for the Diagnosis and Management of Asthma. NIH Publication no. 08-4051, 2007.
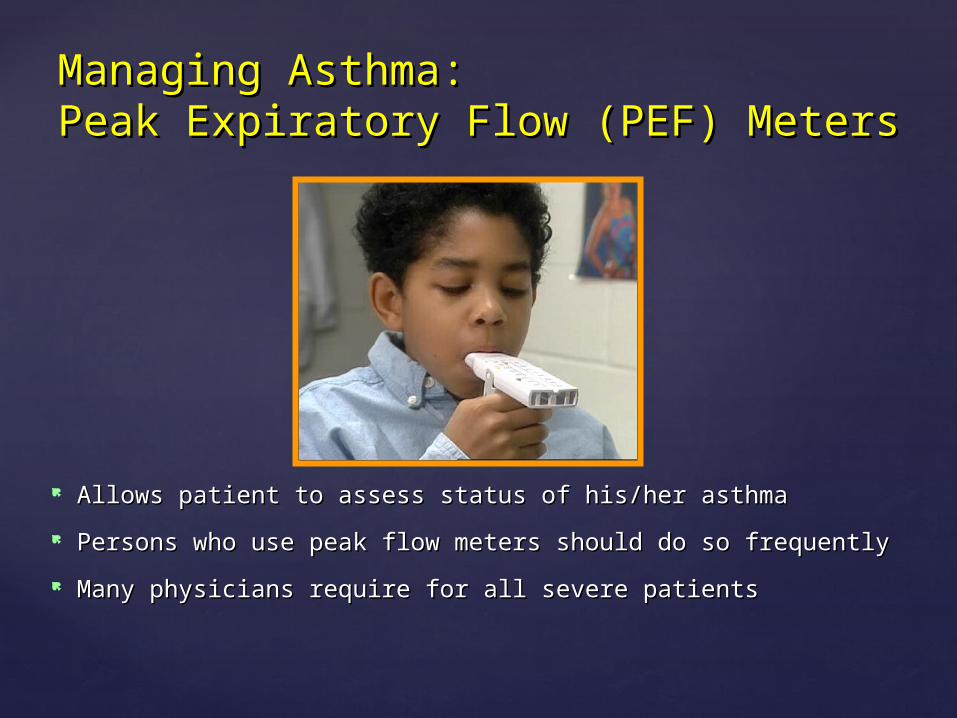
Managing Asthma: Managing Asthma: Peak Expiratory Flow (PEF) MetersPeak Expiratory Flow (PEF) Meters
Allows patient to assess status of his/her asthma Allows patient to assess status of his/her asthma
Persons who use peak flow meters should do so frequentlyPersons who use peak flow meters should do so frequently
Many physicians require for all severe patientsMany physicians require for all severe patients

Control chronic and nocturnal symptomsControl chronic and nocturnal symptoms Maintain normal activity levels and exerciseMaintain normal activity levels and exercise Maintain near-normal pulmonary functionMaintain near-normal pulmonary function Prevent acute episodes of asthmaPrevent acute episodes of asthma Minimize emergency department (ED)Minimize emergency department (ED)
visits and hospitalizationsvisits and hospitalizations Avoid adverse effects of asthma medicationsAvoid adverse effects of asthma medications
Asthma: Goals of Asthma: Goals of TreatmentTreatment11
11Global Initiative for Asthma. GINA workshop report: global Global Initiative for Asthma. GINA workshop report: global strategy for asthma management and prevention. Available at: strategy for asthma management and prevention. Available at: http://www.ginasthma.org. Accessed October 13, 2006.. Accessed October 13, 2006.
There has been remarkable progress in There has been remarkable progress in pharmacotherapy, education and pharmacotherapy, education and environmental measures in treating environmental measures in treating asthmaasthma
However, no single action has been However, no single action has been demonstrated to decrease the risk of demonstrated to decrease the risk of developing asthmadeveloping asthma
Genetic and environmental influences-key!Genetic and environmental influences-key! Exposure to microbial products- Hygiene?Exposure to microbial products- Hygiene? Low level of lung function present in Low level of lung function present in
preschoolers with asthmapreschoolers with asthma Prevention will depend on factors Prevention will depend on factors
influencing the development and influencing the development and progression of asthmaprogression of asthma
Asthma PreventionAsthma Prevention