Learned helplessness and generalization - Stanford University
Upload
mocanu-elenaCategory
view
215download
1Abstract
Objective: To investigate the association between helplessness, disability and disease activity with
health-related quality of life (HRQoL) in a multi-ethnic cohort of rheumatoid arthritis (RA) patients
in Singapore.
Methods: This cross-sectional study was conducted at Tan Tock Seng Hospital, Department of
Rheumatology, Allergy and Immunology, from October 2010 to October 2011. All patients fulfilled
the American College of Rheumatology 1987 criteria for RA. Socio-demographics, clinical and
patient-reported outcome (PRO) variables were collected. HRQoL outcomes were Short-Form 36
(SF-36) physical and mental component summary scores (PCS and MCS) and Short-Form 6
Dimensions (SF-6D) utilities. Stepwise multiple linear regression analyses were performed using
HRQoL outcomes as dependent variables in separate models and with adjustment for helplessness
(Rheumatology Attitudes Index, RAI), disability (Health Assessment Questionnaire, HAQ) and
disease activity (Disease Activity in 28 joints, DAS28) followed by socio-demographic, clinical and
PRO variables.
Results: Complete data was provided by 473 consenting subjects (mean (SD) age: 60.02 (11.04)
years, 85% female, 77% Chinese). After adjustment for all measured covariates, only RAI and
HAQ scores remained significantly associated with SF-36 MCS (: -0.9, p
!!
2
Introduction
Rheumatoid arthritis (RA) is a chronic debilitating disease with an estimated 1% prevalence in the
population [1]. Health-related quality of life (HRQoL) is a multidimensional measure of a patients
well-being, including physical well-being, social well-being, emotional well-being and functional
abilities [2]. The course of RA results in financial burdens and drastic psychosocial and physical
changes to the patients, thus affecting their HRQoL [3]. In recent years, there has been a shift of
focus from traditional indicators of disease activity and prognosis to a more holistic measure of
patient outcome using HRQoL instruments [4]. Furthermore, it has been shown that current efficacy
endpoints such as joint counts and laboratory tests, such as C-reactive protein, are poorer predictors
of overall HRQoL of patients compared to patient-reported outcomes (PRO)[5].
Although there are several studies on the HRQoL of RA patients in North Asia, Europe and
Northern America [6-13], the findings from these populations may not be readily generalizable to
Southeast Asia, as HRQoL is heavily influenced by cultural, economic and social issues [14]. For
example, depressed elderly Asians residing in Canada and the United States were significantly more
likely to report more external locus of control and self-blaming attributions than depressed
Caucasians [15] and this may alter the relationship between sense of helplessness and HRQoL
among Asians. Furthermore, there is a dearth of literature on RA patients in Southeast Asia and
existing studies have their limitations. The study by Sadamoto et al [11] utilised the Lorishs face
scale which is not widely used in clinical practice or research, while the studies by Kojima et al [13]
and Linde et al [10] involved subjects with lower disease activity, who are not representative of the
general RA patient population. Studies by Standfield et al [12] and Cho S-K et al [8] may not have
accounted for all possible confounding factors, as acknowledged by the authors. Hence, our study is
likely to fill a gap in current literature by studying the relationships between sense of helplessness,
disability and disease activity and HRQoL in RA patients in Singapore, an island city state in
Southeast Asia, We hypothesized that subjects with a higher sense of helplessness would report
poorer mental and overall HRQoL while those with greater disability or higher disease activity
would report poorer physical, mental and overall HRQoL as measured by the SF-36 and the Short-
Form 6 Dimensions (SF-6D)..
!!
3
Methods
Patients and data collection
A cross-sectional study involving RA patients from the Department of Rheumatology, Allergy and
Immunology at Tan Tock Seng Hospital (TTSH) was carried out from October 2010 to October
2011. All patients fulfilled the 1987 American College of Rheumatology (ACR) criteria for RA [16].
This study was approved by the Institutional Review Board and all subjects provided written
informed consent.
Clinical variables were scored by the attending rheumatologists. Socio-demographic and PRO
variables were collected using a set of self-administered and pre-tested English and Chinese
language questionnaires. For a very small group of subjects who can understand but cannot read,
the survey was interviewer-administered. Socio-demographic variables collected included gender,
age, race, education level and marital status. Clinical variables included the number of co-
morbidities, duration of morning stiffness, ACR functional status, physicians global assessment
(DGA, higher score indicates poorer disease status) of RA, RA disease activity in 28 joints (DAS28)
[17] and medications. PRO variables included patients global assessment of RA activity and pain
intensity on visual analogue scale (0-100mm, higher value denoting worse PGA and greater pain
intensity), HAQ (range 0-3) [18,19], RAI (range 15-75) [20], SF-36 [21,22], and SF-6D [23,24] for
assessment of functional status, helplessness and quality of life respectively.
RAI
RAI is a 15-item self-administered survey to measure the sense of helplessness which may arise due
to the unpredictable nature of the rheumatic disease [20]. The RAI was previously found to exhibit
good psychometric properties in Singapore. The response options range from 1 (strongly disagree)
to 5 (strongly agree) [25] with reversed scoring for 9 questions. The total RAI score ranges from 15
to 75 with higher scores indicating a greater sense of helplessness.
!!
4
SF-36
The SF-36 is a self-reported generic HRQoL survey that has also been used widely in Singapore
[26]. It comprises 8 health domains including physical functioning, physical role functioning,
emotional role functioning, bodily pain, general health, vitality, social functioning and mental
health. The 8 domains may be further collapsed into the physical component summary (PCS) and
the mental component summary (MCS) scores [21]. PCS and MCS are norm-based scores with a
mean of 50 and standard deviation of 10, with higher scores indicating better HRQoL. This means
that someone with a score of 40 is one standard deviation below the average score of the Singapore
general population while someone with a score of 60 is one standard deviation above the average
score of the Singapore general population. A difference of 5 points [26] is usually defined as the
minimally important difference (MID) but MID of 3 points has also been suggested [22].
SF-6D
The SF-6D is a preference based HRQoL questionnaire derived from the SF-36 [23] and comprises
6 single-item dimensions including physical function, role limitation, social function, pain, mental
health and vitality. The response option for each item ranges from 4 to 6 levels, thus describing
18,000 possible health states. The utility scores of SF-6D range from 0.30 to 1.00 with a score of
1.00 designated perfect health and a score of 0.3 representing the worst possible health state. A
MID of 0.041 for SF-6D has been proposed [24].
Statistical Analyses
Descriptive statistics was presented and stratified by gender and race. Mean and standard deviations
(SD) were presented. Differences between genders were assessed using Chi-squared test for
categorical variables, and Students t-test or Mann-Whitney U-test for normally and non-normally
distributed continuous variables, respectively. Differences between races were assessed using Chi-
squared test for categorical variables, and analysis of variance (ANOVA) or Kruskal-Wallis test for
normally and non-normally distributed continuous variables, respectively.
!!
5
Univariable regression analyses were conducted and only variables that had p values less than 0.1
were included in the subsequent multiple linear regression analyses. Stepwise multiple linear
regression analyses were performed with SF-36 PCS, SF-36 MCS and SF-6D utility scores as
dependent variables in separate models. Given that we hypothesized that helplessness, functional
status and disease activity are associated with HRQoL outcomes, we introduced RAI, HAQ and
DAS28 scores separately as independent variables one at a time to each of the three dependent
variables (model series 1). Only the variable(s) that has/ have statistically significant association(s)
with the dependent variable is/are retained in the next series of model. In model series 2, socio-
demographic covariates such as age, gender, race, marital status and education level were added to
the variables that were statistically significant in model series 1. In model series 3, clinical
covariates such as ACR functional class status, DGA, number of medications, number of co-
morbidities and duration of morning stiffness were added to model series 2. In model series 4, PRO
covariates such as PGA and pain intensity were added to model series 3. To avoid multicollinearity
in the model, a variable is only included if the variance inflation factor is less than 10 [27].
Adjusted R-square was used to compare across the models.
All statistical analyses were carried out using STATA SE version 12.1 for Windows (Stata Corp,
College Station, TX).
!!
6
Results
Subjects
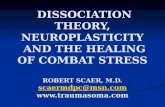
Of the 708 subjects recruited, 198 subjects did not have complete HRQoL data, 22 subjects did not
have complete socio-demographic, clinical and other PRO data and 15 subjects who were not
ethnically Chinese, Malay or Indian were excluded (Figure 1). Subjects that were excluded had
better General Health Assessment (GHA) (3.0212.57 vs 9.7219.09, p
!!
7
HAQ score was statistically significant across all HRQoL outcomes without adjustment of covariate
(p
!!
8
Discussion In this study among multi-ethnic Southeast Asian patients with RA, as hypothesized, sense of
helplessness and disability are inversely associated with the HRQoL of RA patients. Furthermore,
helplessness was more strongly associated with mental HRQoL than with physical HRQoL [28].
Therefore, clinicians may consider emphasizing self-management skills so as to improve the mental
HRQoL of RA patients [29]. Interestingly, our hypothesis with regard to disease activity was not
supported by our findings.
We observed that there was initially an association between disease activity and HRQoL but this
was abolished after adjusting for PRO covariates in PCS and SF-6D. In MCS, the association was
abolished after adjusting for clinical variables. The observation that PRO covariates explain much
of the association between disease activity and HRQoL would suggest that it might be feasible to
replace the cumbersome DAS28 measurements with simpler PRO tools.
Our study supported the hypothesis that RA patients with higher HAQ have lower HRQoL. This
relationship was strong across all 3 HRQoL measures: SF-36 PCS, SF-36 MCS and SF-6D. This
finding is consistent with other studies and supports the recommendation that measuring disability
be made part of daily clinical practice [9]. In fact, among all independent variables, regression
coefficients were the largest for HAQ (6.0 points with SF-36 PCS, 7.0 points with SF-36 MCS and
0.081 points with SF-6D) and exceeded the minimal clinically important difference for all 3
measures. The relationship of pain was also seen across all 3 HRQoL measures. This was consistent
with published literature although it was not in our original hypotheses [30,31].
In this study, we demonstrated that RAI, HAQ and DAS28 scores were more strongly associated
with SF-36 MCS than with SF-36 PCS and SF-6D. The HAQ is a generic measure that was
designed to assess the difficulty in performing activities of daily living. It is interesting that it
should be more strongly correlated with MCS compared to PCS as there is a published study that
showed a stronger association to PCS than MCS [32]. We observed that RA has a greater impact on
PCS (49.3210.16) than MCS (53.7012.99). It appears that a more refined RA-specific measure of
physical functioning may be needed if the impact of RA on physical functioning is to be fully
captured. While the SF-36 may suffice, a RA-specific measure may be more sensitive and
responsive compared to the generic SF-36.
!!
9
As SF-6D is an overall measure of HRQoL, it is not surprising that the factors associated with SF-
6D scores reflects a combination of factors associated with PCS and MCS.
Limitations
There are several limitations in our study. First, the cross-sectional design does not allow us to draw
any causal relationship between the factors and HRQoL. However, this study provides the basis for
a future prospective, longitudinal study to identify predictors of HRQoL in RA. Second, our
subjects were recruited from a tertiary care setting, thus our findings may not be generalizable to
patients with milder conditions who are being followed up in the primary care setting. Nonetheless,
we observed that the HAQ and DAS28 scores of our population are lower than many published
overseas studies. Third, we did not observe any significant association between the number of co-
morbidities and HRQoL outcomes and this may suggest that alternative approaches to account for
comorbidities should be explored [33]. Last, this study did not capture socioeconomic status data.
Nonetheless, previous studies have shown that beta coefficient associated with socioeconomic
status tends to be smaller than with comorbidities [7,34].
The study sample was restricted to subjects with complete HRQoL, socio-demographic, clinical and
PRO data. The individuals excluded had better GHA, PGA, and pain score with shorter duration of
morning stiffness. This may limit the generalizability of our data and additional studies focusing on
this group of excluded subjects may need to be conducted.
Conclusions
We found that RAI and HAQ scores, but not DAS28 scores, are significantly associated with
HRQoL of RA patients in Singapore. Greater emphasis on managing disability and providing
psychosocial support should supplement clinical management so that HRQoL of RA patients can
improve and better treatment outcomes achieved.
Acknowledgement
This study is supported by a grant from the National Healthcare group (NHG)-SIG/PTD/06044
!!
10
References
1.!Shapira!Y,!Agmon1Levin!N,!Shoenfeld!Y!(2010)!Geoepidemiology!of!autoimmune!rheumatic!diseases.!Nat!Rev!Rheumatol!6!(8):4681476.!doi:10.1038/nrrheum.2010.86!
2.!Cella!DF!(1994)!Quality!of!life:!concepts!and!definition.!J!Pain!Symptom!Manage!9!(3):1861192!3.!Cadena!J,!Vinaccia!S,!Prez!A,!Rico!MI,!Hinojosa!R,!Anaya!J1M!(2003)!The!impact!of!disease!activity!on!the!
quality!of!life,!mental!health!status,!and!family!dysfunction!in!colombian!patients!with!rheumatoid!arthritis.!J!Clin!Rheumatol!9!(3):1421150!
4.!Guillemin!F!(2000)!Functional!disability!and!quality1of1life!assessment!in!clinical!practice.!Rheumatology!(Oxford)!39!(suppl!1):17123!
5.!Eichler!HG,!Mavros!P,!Geling!O,!Hunsche!E,!Kong!S!(2005)!Association!between!health1related!quality!of!life!and!clinical!efficacy!endpoints!in!rheumatoid!arthritis!patients!after!four!weeks!treatment!with!anti1inflammatory!agents.!Int!J!Clin!Pharmacol!Ther!43!(5):2091216!
6.!Marra!CA,!Lynd!LD,!Esdaile!JM,!Kopec!J,!Anis!AH!(2004)!The!impact!of!low!family!income!on!self1reported!health!outcomes!in!patients!with!rheumatoid!arthritis!within!a!publicly!funded!health1care!environment.!Rheumatology!(Oxford)!43!(11):139011397.!doi:10.1093/rheumatology/keh334!
7.!Langley!PC,!Mu!R,!Wu!M,!Dong!P,!Tang!B!(2011)!The!impact!of!rheumatoid!arthritis!on!the!burden!of!disease!in!urban!China.!J!Med!Econ!14!(6):7091719.!doi:doi:10.3111/13696998.2011.611201!
8.!Cho!S1K,!Kim!D,!Jun!J1B,!Bae!S1C,!Sung!Y1K!(2012)!Factors!influencing!quality!of!life!(QOL)!for!Korean!patients!with!rheumatoid!arthritis!(RA).!Rheumatol!Int:1110.!doi:10.1007/s0029610111235216!
9.!Rupp!I,!Boshuizen!HC,!Roorda!LD,!Dinant!HJ,!Jacobi!CE,!van!den!Bos!G!(2006)!Poor!and!good!health!outcomes!in!rheumatoid!arthritis:!the!role!of!comorbidity.!J!Rheumatol!33!(8):148811495!
10.!Linde!L,!Sorensen!J,!Ostergaard!M,!Horslev1Petersen!K,!Rasmussen!C,!Jensen!DV,!Hetland!ML!(2009)!What!factors!influence!the!health!status!of!patients!with!rheumatoid!arthritis!measured!by!the!SF112v2!health!survey!and!the!Health!Assessment!Questionnaire?!J!Rheumatol!36!(10):218312189.!doi:10.3899/jrheum.090134!
11.!Sadamoto!K,!Fukuya!H,!Saito!E!(2001)!What!is!the!factor!that!most!influences!QOL!among!rheumatoid!arthritis!patients?!Mod!Rheumatol!11!(1):52155.!doi:10.1007/s101650170044!
12.!Standfield!L,!Norris!S,!Harvey!C,!Elliot!L,!Riordan!J,!Hall!S,!Day!R,!Nash!P,!Thirunavukkarasu!K,!Robertson!J,!Palmer!T!(2010)!Relationship!between!rheumatoid!arthritis!disease!severity,!health1related!utility,!and!resource!use!in!australian!patients:!A!cross1sectional,!multicenter!study.!Clin!Ther!32!(7):132911342.!doi:10.1016/j.clinthera.2010.07.006!
13.!Kojima!M,!Kojima!T,!Ishiguro!N,!Oguchi!T,!Oba!M,!Tsuchiya!H,!Sugiura!F,!Furukawa!TA,!Suzuki!S,!Tokudome!S!(2009)!Psychosocial!factors,!disease!status,!and!quality!of!life!in!patients!with!rheumatoid!arthritis.!J!Psychosom!Res!67!(5):4251431.!doi:10.1016/j.jpsychores.2009.01.001!
14.!Kagawa1Singer!M!(2011)!Impact!of!culture!on!health!outcomes.!J!Pediatr!Hematol!Oncol!33:S901S95!10.1097/MPH.1090b1013e318230dadb!
15.!Fry!PS,!Grover!SC!(1982)!Cognitive!Appraisals!of!Life!Stress!and!Depression!in!the!Elderly:!A!Cross1Cultural!Comparison!of!Asians!and!Caucasians.!Intl!J!Psychol!17!(114):4371454.!doi:10.1080/00207598208247455!
16.!Arnett!FC,!Edworthy!SM,!Bloch!DA,!McShane!DJ,!Fries!JF,!Cooper!NS,!Healey!LA,!Kaplan!SR,!Liang!MH,!Luthra!HS,!Medsger!TA,!Mitchell!DM,!Neustadt!DH,!Pinals!RS,!Schaller!JG,!Sharp!JT,!Wilder!RL,!Hunder!GG!(1988)!The!american!rheumatism!association!1987!revised!criteria!for!the!classification!of!rheumatoid!arthritis.!Arthritis!Rheum!31!(3):3151324.!doi:10.1002/art.1780310302!
17.!Fransen!J,!van!Riel!PLCM!(2009)!The!disease!activity!score!and!the!EULAR!response!criteria.!Rheum!Dis!Clin!North!Am!35!(4):7451757.!doi:10.1016/j.rdc.2009.10.001!
18.!Koh!ET,!Seow!A,!Pong!LY,!Koh!WH,!Chan!L,!Howe!HS,!Lim!TH,!Low!CK!(1998)!Cross!cultural!adaptation!and!validation!of!the!Chinese!Health!Assessment!Questionnaire!for!use!in!rheumatoid!arthritis.!J!Rheumatol!25!(9):170511708!
!!
11
19.!Bruce!B,!Fries!J!(2003)!The!Stanford!Health!Assessment!Questionnaire:!Dimensions!and!practical!applications.!Health!Qual!Life!Outcomes!1!(1):20!
20.!Callahan!LF,!Brooks!RH,!Pincus!T!(1988)!Further!analysis!of!learned!helplessness!in!rheumatoid!arthritis!using!a!"Rheumatology!Attitudes!Index".!J!Rheumatol!15!(3):4181426!
21.!Ware!(1993)!Manual!and!interpretation!guide.!Nimrod!Press,!Boston!22.!Hays!RD,!Morales!LS!(2001)!The!RAND136!measure!of!health1related!quality!of!life.!Ann!Med!33!(5):3501
357.!doi:doi:10.3109/07853890109002089!23.!Brazier!J,!Roberts!J,!Deverill!M!(2002)!The!estimation!of!a!preference1based!measure!of!health!from!the!
SF136.!J!Health!Econ!21!(2):2711292.!doi:10.1016/s016716296(01)0013018!24.!Walters!SJ,!Brazier!JE!(2005)!Comparison!of!the!minimally!important!difference!for!two!health!state!
utility!measures:!EQ15D!and!SF16D.!Qual!Life!Res!14!(6):152311532.!doi:10.1007/s1113610041771310!25.!Thumboo!J,!Feng!P1H,!Chan!S1P,!Boey!M1L,!Thio!S1t,!Fong!K1Y!(2002)!A!Chinese!version!of!the!
Rheumatology!Attitudes!Index!is!a!valid!and!reliable!measure!of!learned!helplessness!in!patients!with!SLE.!Lupus!11!(2):88194.!doi:10.1191/0961203302lu156oa!
26.!Koh!ET,!Leong!KP,!Tsou!IYY,!Lim!VH,!Pong!LY,!Chong!SY,!Seow!A,!Group!ftTTSHRAS!(2006)!The!reliability,!validity!and!sensitivity!to!change!of!the!Chinese!version!of!SF136!in!oriental!patients!with!rheumatoid!arthritis.!Rheumatology!(Oxford)!45!(8):102311028.!doi:10.1093/rheumatology/kel051!
27.!Obrien!R!(2007)!A!Caution!Regarding!Rules!of!Thumb!for!Variance!Inflation!Factors.!Qual!Quant!41!(5):6731690.!doi:10.1007/s1113510061901816!
28.!Brady!TJ!(2003)!Measures!of!self1efficacy,!helplessness,!mastery,!and!control:!The!Arthritis!Helplessness!Index!(AHI)/Rheumatology!Attitudes!Index!(RAI),!Arthritis!Self1Efficacy!Scale!(ASES),!Children's!Arthritis!Self1Efficacy!Scale!(CASE),!Generalized!Self1Efficacy!Scale!(GSES),!Mastery!Scale,!Multi1Dimensional!Health!Locus!of!Control!Scale!(MHLC),!Parent's!Arthritis!Self1Efficacy!Scale!(PASE),!Rheumatoid!Arthritis!Self1Efficacy!Scale!(RASE),!and!Self1Efficacy!Scale!(SES).!Arthritis!Care!Res!(Hoboken)!49!(S5):S1471S164.!doi:10.1002/art.11413!
29.!Chui!DYY,!Lau!JSK,!Yau!ITY!(2004)!An!outcome!evaluation!study!of!the!Rheumatoid!Arthritis!Self1Management!Programme!in!Hong!Kong.!Psychol!Health!Med!9!(3):2861292.!doi:10.1080/13548500410001721855!
30.!Jakobsson!ULF,!Hallberg!IR!(2002)!Pain!and!quality!of!life!among!older!people!with!rheumatoid!arthritis!and/or!osteoarthritis:!a!literature!review.!J!Clin!Nurs!11!(4):4301443.!doi:10.1046/j.136512702.2002.00624.x!
31.!Rupp!I,!Boshuizen!HC,!Dinant!HJ,!Jacobi!CE,!van!den!Bos!GA!(2006)!Disability!and!health1related!quality!of!life!among!patients!with!rheumatoid!arthritis:!association!with!radiographic!joint!damage,!disease!activity,!pain,!and!depressive!symptoms.!Scand!J!Rheum!35!(3):1751181.!doi:10.1080/03009740500343260!
32.!Mikuls!T,!Saag!K,!Criswell!L,!Merlino!L,!Cerhan!JR!(2003)!Health!related!quality!of!life!in!women!with!elderly!onset!rheumatoid!arthritis.!J!Rheumatol!30!(5):9521957!
33.!Rupp!I,!Boshuizen!HC,!Jacobi!CE,!Dinant!HJ,!van!den!Bos!G!(2004)!Comorbidity!in!patients!with!rheumatoid!arthritis:!effect!on!health1related!quality!of!life.!J!Rheumatol!31!(1):58165!
34.!Thumboo!J,!Fong!KY,!Machin!D,!Chan!SP,!Soh!CH,!Leong!KH,!Feng!PH,!Thio!S,!Boey!ML!(2003)!Quality!of!life!in!an!urban!Asian!population:!the!impact!of!ethnicity!and!socio1economic!status.!Soc!Sci!Med!56!(8):176111772!
!
!
!
!
!
!
!
!
!
!
! !
! ! !
!
!
!
!
!
! !
Recruitment October 2010-October 2011
N=708
Complete HRQoL data N=510
Complete HRQoL and covariate data
N=488
Exclusion of other races N=473
198 subjects with missing HRQoL data
7 subjects with missing education level data 1 subject with missing morning stiffness data
1 subject with missing DGA data 1 subject with missing PGA data
2 subjects with missing HAQ score 8 subjects with missing RAI score
2 subjects with missing ACR functional status
15 subjects who were not Chinese, Malays or Indians
Figure 1. Patient exclusion chart Abbreviations: Health-related quality of life (HRQoL), physicians global assessment (DGA), patients global assessment (PGA), patient reported outcomes (PRO), health assessment questionnaire (HAQ), rheumatology attitudes index (RAI), American College of Rheumatology (ACR)
Table 1. Socio-demographics, clinical and PRO variables in overall population and between genders Feature Mean SD (%) P value Total
(N=473) Male
(N=70) Female
(N=403)
Socio-demographic variables Age (years) 60.0211.04 62.2610.33 59.6311.12 0.066 Race
Chinese Malay Indian
366 (77) 47 (10) 60 (13)
50 (72) 12 (17) 8 (11)
316 (78)
35 (9) 52 (13)
0.092
Marital Status Single Married Widowed Divorced
64 (13)
339 (71) 51 (11) 19 (4)
4 (6)
62 (88) 4 (6) 0 (0)
60 (15)
277 (69) 47 (12) 19 (4)
0.007*
Educational Level No formal education Primary Secondary Polytechnic/Pre-U Tertiary education
91 (19)
121 (25) 193 (41) 46 (10) 22 (5)
9 (13)
11 (16) 33 (47) 15 (21)
2 (3)
82 (20)
110 (27) 160 (40)
31 (8) 20 (5)
0.001*
Clinical variables ACR functional status
I Normal II Limited in social activities III Limited in vocational activities IV Wheel-chair or bedridden
326 (69) 112 (24)
26 (5) 9 (2)
50 (72) 10 (14) 9 (13) 1 (1)
276 (69) 102 (25)
17 (4) 8 (2)
0.010*
DGA 3.607.89 4.176.96 3.518.04 0.266 Number of medications 3.801.71 3.741.77 3.811.70 0.774 Number of co-morbidities 2.431.84 2.902.03 2.361.80 0.041* Minutes of morning stiffness 12.7449.86 11.9847.44 12.9250.44 0.258 DAS28 score 2.320.86 2.450.96 2.300.84 0.261 PRO variables PGA 22.0426.58 23.9128.38 21.7126.27 0.615 Pain intensity 14.2722.59 13.3719.99 14.4223.03 0.772 HAQ score 0.290.49 0.280.43 0.300.50 0.889 RAI score 35.906.65 36.646.14 35.776.73 0.216 SF-36 PCS 49.3210.16 50.139.80 49.1810.22 0.287 SF-36 MCS 53.7012.99 53.2512.77 53.7813.04 0.872 SF-6D index 0.810.12 0.810.13 0.810.12 0.937 Data shown as mean SD or n (%). *p
Table 2. Socio-demographics, clinical and PRO variables in overall population and among races Feature Mean SD (%) P value Total
(N=473) Chinese (N=366)
Malay (N=47)
Indian (N=60)
Socio-demographic variables Age (years) 60.0211.04 60.4411.21 58.929.99 58.2810.06 0.425 Gender Male Female
70 (15)
403 (85)
50 (14)
315 (86)
12 (26) 35 (74)
8 (13)
52 (87)
0.092
Marital Status Single Married Widowed Divorced
64 (13)
339 (71) 51 (11) 19 (4)
55 (15)
263 (72) 40 (11)
8 (2)
1 (2)
35 (75) 5 (11) 6 (12)
8 (14)
41 (68) 6 (10) 5 (8)
0.003*
Educational Level No formal education Primary Secondary Polytechnic/Pre-U Tertiary education
91 (19)
121 (25) 193 (41) 46 (10) 22 (5)
75 (21) 91 (25)
140 (38) 40 (11) 20 (5)
7 (15)
11 (24) 26 (55)
3 (6) 0 (0)
9 (15)
19 (32) 27 (45)
3 (5) 2 (3)
0.201
Clinical variables ACR functional status
I Normal II Limited in social activities III Limited in vocational activities IV Wheel-chair or bedridden
326 (69) 112 (24)
26 (5) 9 (2)
254 (69) 87 (24) 21 (6) 4 (1)
27 (57) 15 (32)
4 (9) 1 (2)
45 (75) 10 (17)
1 (1) 4 (7)
0.028*
DGA 3.607.89 3.547.89 4.137.35 3.608.42 0.485 Number of medications 3.801.71 3.771.70 4.111.54 3.721.83 0.414 Number of co-morbidities 2.431.84 2.391.85 2.341.59 2.801.96 0.334 Minutes of morning stiffness 12.7449.86 12.7748.98 8.9331.29 15.8365.85 0.874 DAS28 score 2.320.86 2.300.86 2.370.74 2.390.97 0.604 PRO variables PGA 22.0426.58 21.9226.01 22.0927.57 22.7529.52 0.936 Pain intensity 14.2722.59 14.0321.96 11.1321.13 18.1826.92 0.216 HAQ score 0.290.49 0.280.48 0.350.45 0.360.57 0.177 RAI score 35.906.65 35.926.55 35.266.30 36.307.56 0.781 SF-36 PCS 49.3210.16 49.6210.32 47.629.86 48.839.34 0.127 SF-36 MCS 53.7012.99 53.6013.32 53.9111.81 54.1511.97 0.980 SF-6D utilities 0.810.12 0.810.12 0.800.12 0.820.11 0.913 Data shown as mean SD or n (%). *p
Table 3. Univariable association between RAI, HAQ and DAS28 Scores on HRQoL outcomes Model Series 1 SF-36 PCS
Regression coefficient
SF-36 MCS Regression Coefficient
SF-6D Regression
Coefficient (x10-2) RAI score -0.5*** -1.3*** -1.0*** DAS28 score -3.0*** -4.4*** -4.0*** HAQ score -8.2*** -12.7*** -11.8*** ***p
Table 4. Stepwise, multivariable association between RAI, HAQ, DAS28 Scores, socio-demographic, clinical and psychosocial variables on HRQoL outcomes
*P