Assistant Professor Family Medicine Qassim Medical College 1429 - 1430.
57
Assistant Professor Family Assistant Professor Family Medicine Medicine Qassim Medical College Qassim Medical College 1429 - 1430 1429 - 1430
-
Upload
nora-alexander -
Category
Documents
-
view
220 -
download
0
Transcript of Assistant Professor Family Medicine Qassim Medical College 1429 - 1430.
Assistant Professor Family MedicineAssistant Professor Family Medicine
Qassim Medical CollegeQassim Medical College
1429 - 14301429 - 1430
Learning Objectives
To enable the student to:o Approach the most common skin lesionso Diagnose and differential diagnosis of the most
common skin problems. o Management of these cases in Family Practiceo Impact of psychological effect of these problems.o When to refer
A I5-year-old female comes to your office with " zits.“A I5-year-old female comes to your office with " zits.“She has been attempting to treat these with frequent She has been attempting to treat these with frequent washings with a buff puff and avoidance of cosmeticswashings with a buff puff and avoidance of cosmetics..
She is very distressed and breaks down crying. She is very distressed and breaks down crying. She is She is afraid thatafraid that "no boys will ever go out with someone "no boys will ever go out with someone with such an ugly face.“with such an ugly face.“
Her past history is unremarkable. Her past history is unremarkable. She is taking no medications at present. She is taking no medications at present. She has no allergies. She has no allergies. Her family history is unremarkable. Her family history is unremarkable. On physical examination the patient has multiple On physical examination the patient has multiple maculopapular-pustular lesions with comedones on her maculopapular-pustular lesions with comedones on her face and back.face and back.
No other abnormalities are found on examination.No other abnormalities are found on examination.
CASE STUDYCASE STUDY
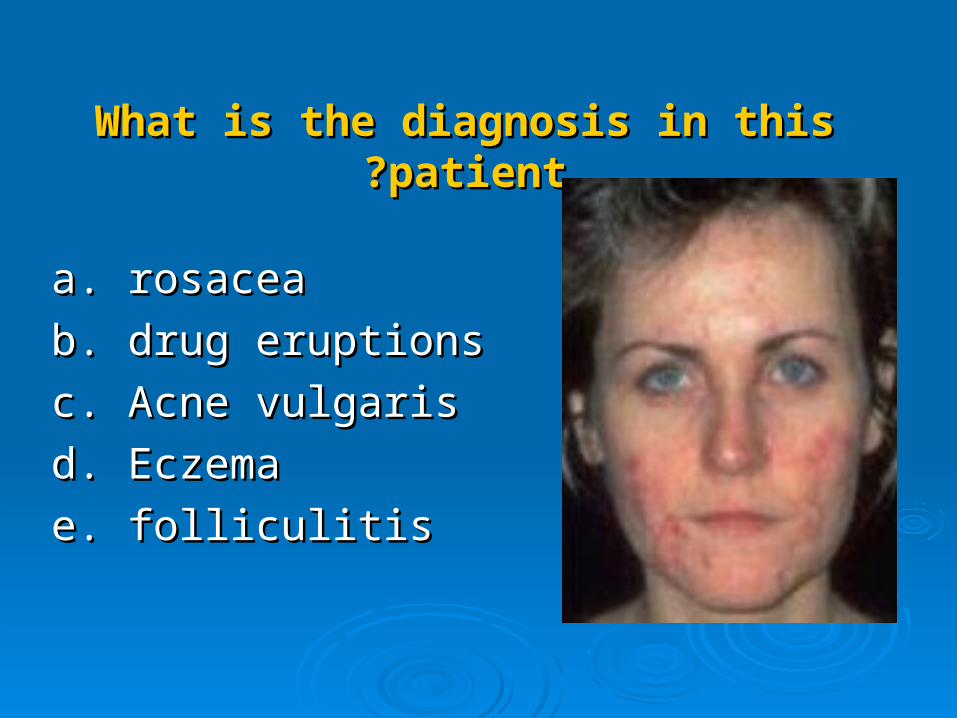
What is the diagnosis in this patientWhat is the diagnosis in this patient??
a. rosaceaa. rosacea
b. drug eruptions b. drug eruptions
c. Acne vulgarisc. Acne vulgaris
d. Eczemad. Eczema
e. folliculitise. folliculitis
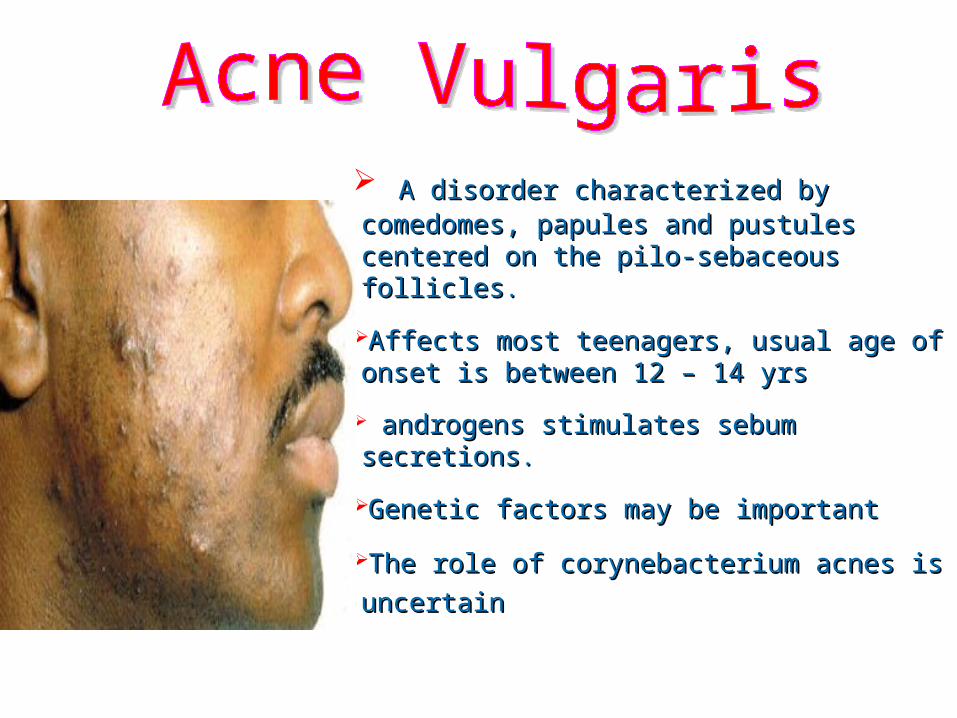
A disorder characterized by comedomes, A disorder characterized by comedomes, papules and pustules centered on the pilo-papules and pustules centered on the pilo-sebaceous folliclessebaceous follicles..
Affects most teenagers, usual age of onset Affects most teenagers, usual age of onset is between 12 – 14 yrsis between 12 – 14 yrs
androgens stimulates sebum secretionsandrogens stimulates sebum secretions..
Genetic factors may be importantGenetic factors may be important
The role of corynebacterium acnes is The role of corynebacterium acnes is
uncertainuncertain
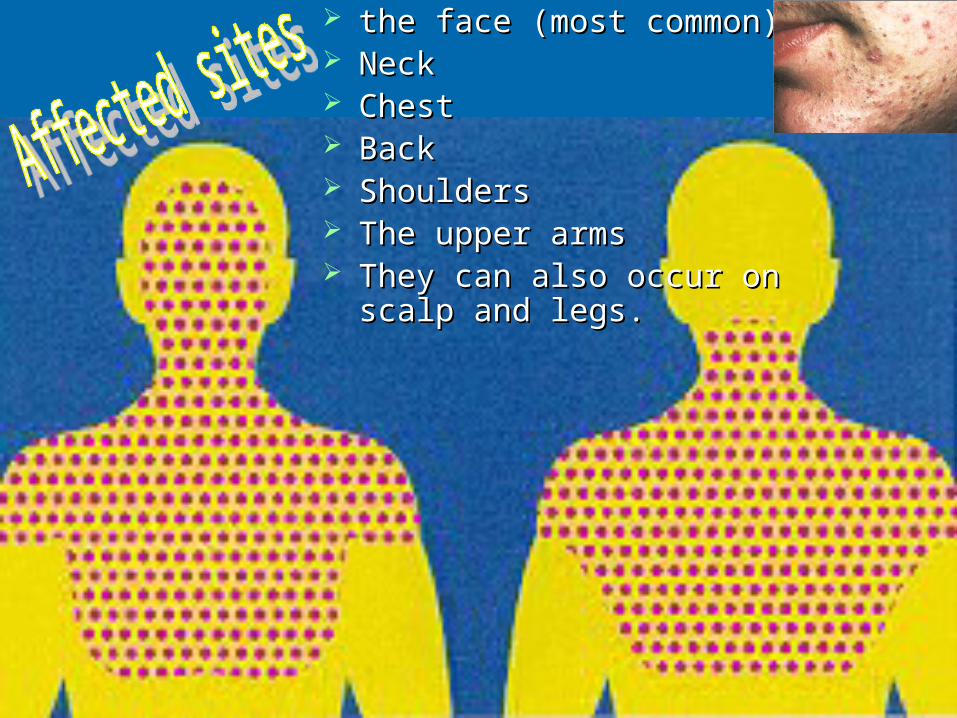
the face (most common)the face (most common) NeckNeck ChestChest BackBack ShouldersShoulders The upper armsThe upper arms They can also occur on scalp They can also occur on scalp
and legs. and legs.

Environmental factors: humidity and heavy Environmental factors: humidity and heavy sweating .sweating .
hormonal components of milk and/or other hormonal components of milk and/or other bioactive molecules in milk could exacerbate bioactive molecules in milk could exacerbate acneacne
acne severity did appear to have some acne severity did appear to have some correlation with stress around the time of correlation with stress around the time of school examinations ? !school examinations ? !
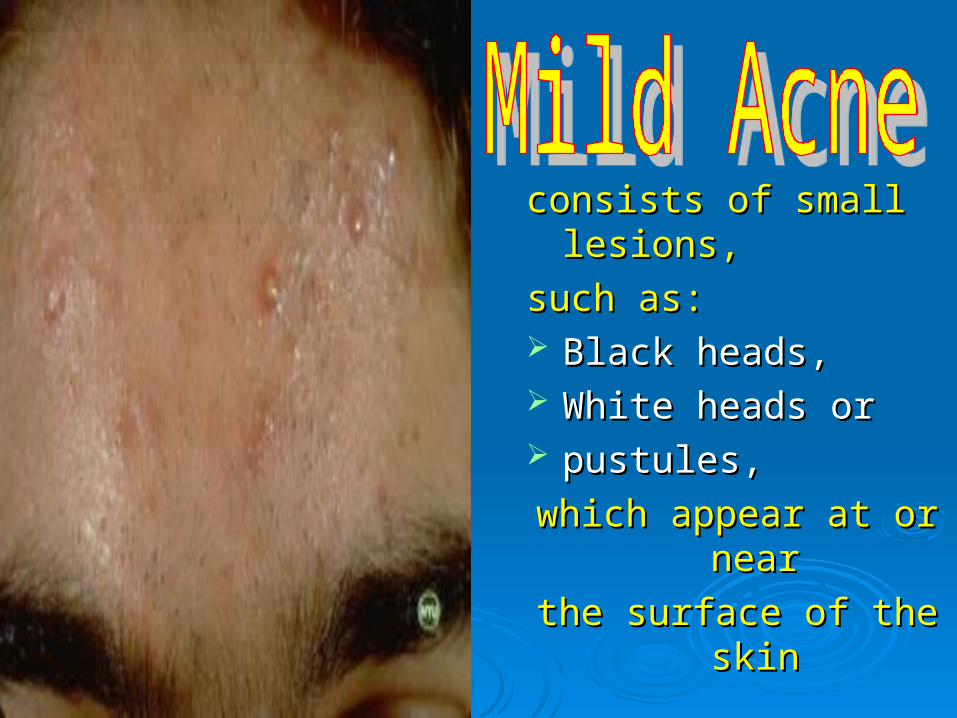
consists of small lesions, consists of small lesions,
such as: such as: Black heads, Black heads, White heads orWhite heads or pustules, pustules,
which appear at or nearwhich appear at or near
the surface of the skinthe surface of the skin
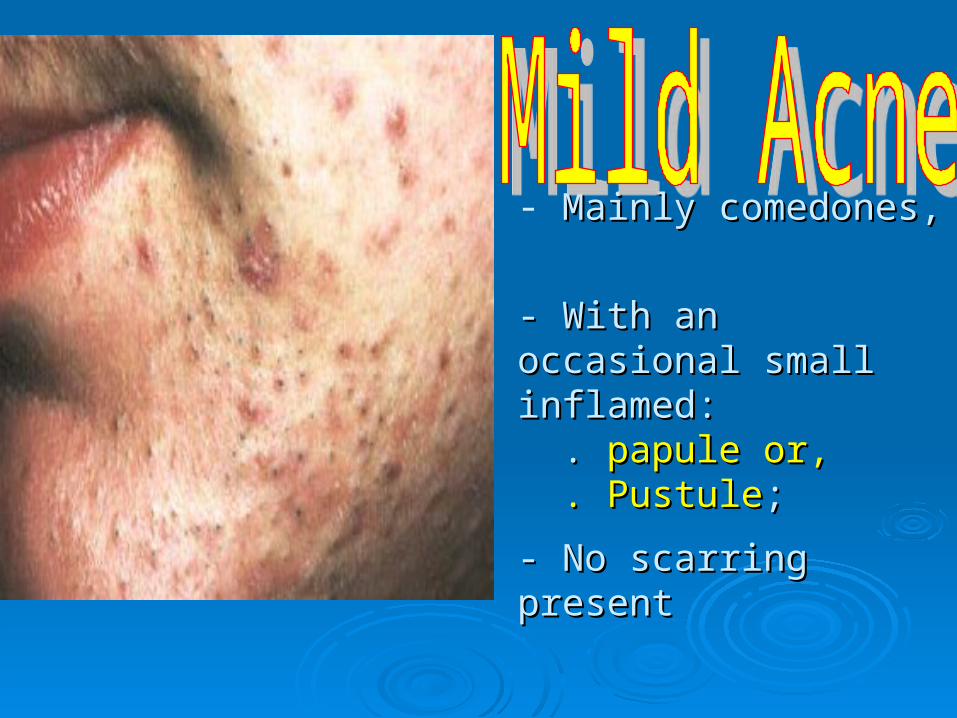
- Mainly comedones, Mainly comedones,
- With an occasional small - With an occasional small inflamed: inflamed: . . papule or, papule or, . Pustule . Pustule; ;
- No scarring present- No scarring present
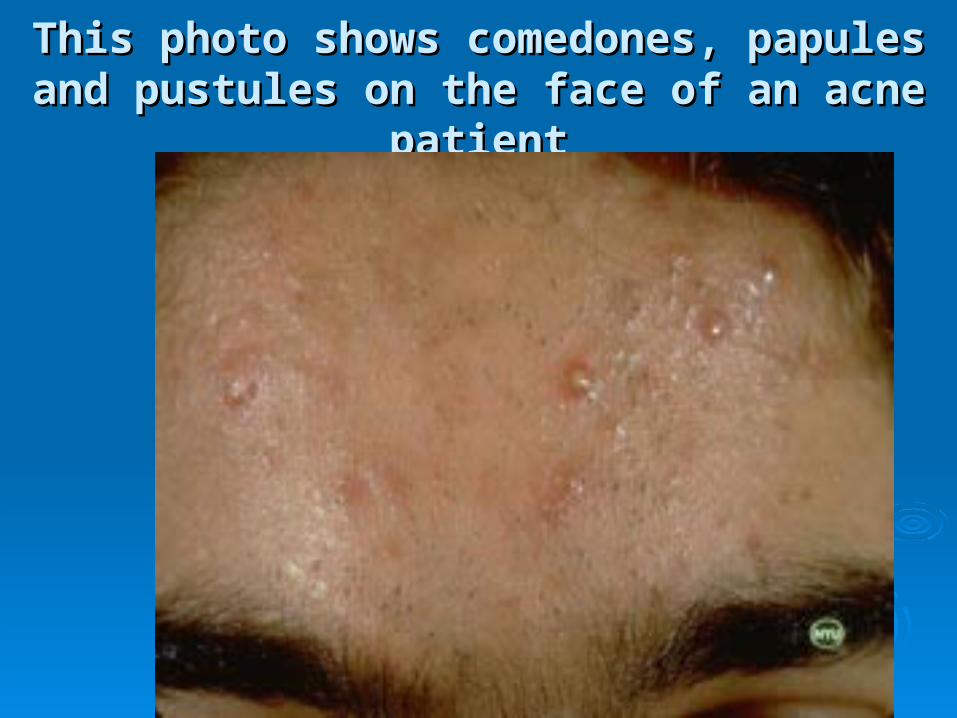
This photo shows comedones, papules and This photo shows comedones, papules and pustules on the face of an acne patientpustules on the face of an acne patient

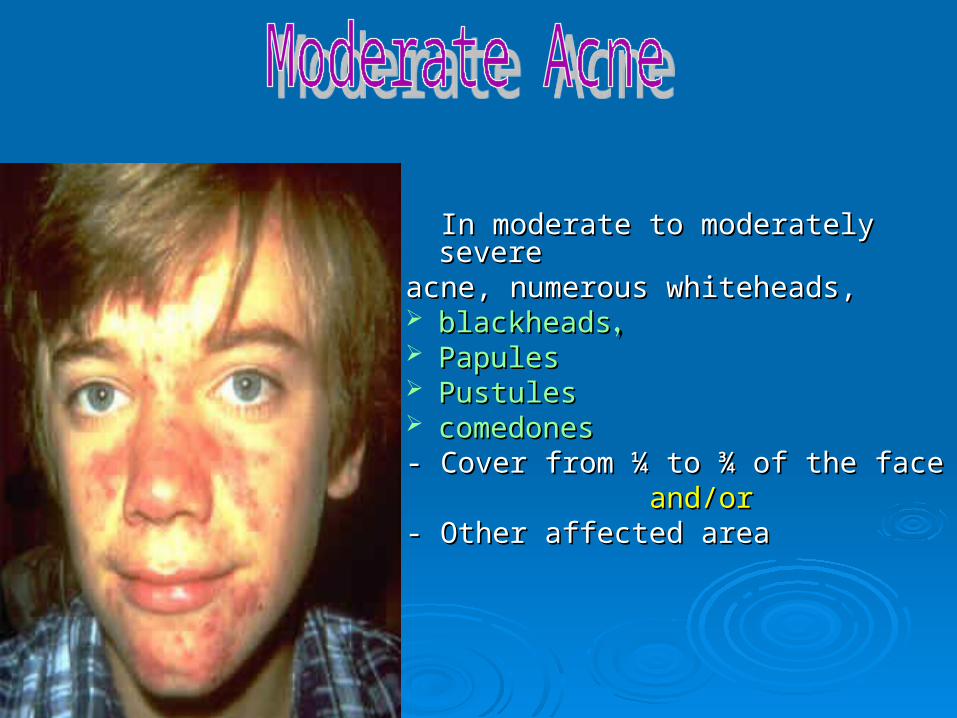
In moderate to moderately severe In moderate to moderately severe acne, numerous whiteheads, acne, numerous whiteheads, blackheadsblackheads,, PapulesPapules PustulesPustules comedonescomedones- Cover from ¼ to ¾ of the face- Cover from ¼ to ¾ of the face and/orand/or - Other affected area- Other affected area
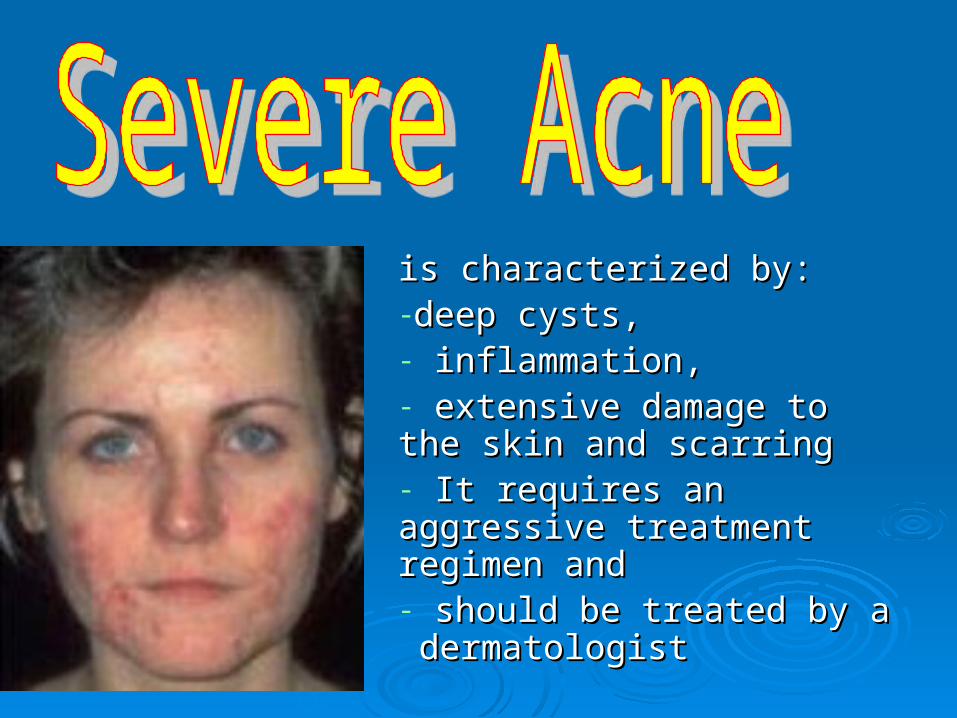
is characterized by:is characterized by:-deep cysts,deep cysts,- inflammation, inflammation, - extensive damage to the extensive damage to the skin and scarring skin and scarring - It requires an aggressive It requires an aggressive treatment regimen andtreatment regimen and- should be treated by a should be treated by a dermatologistdermatologist
The tendency to develop acne is an inherited. The tendency to develop acne is an inherited. Acne can’t be prevented,Acne can’t be prevented, Careful cleanliness and gentle skin care can Careful cleanliness and gentle skin care can
help to lessen the effectshelp to lessen the effects. .
Treatment protocol for mild to moderate acneTreatment protocol for mild to moderate acne
a.a. Begin with topical benzoyl peroxide 2.5 %. Increase to 5% and Begin with topical benzoyl peroxide 2.5 %. Increase to 5% and 10% rapidly. apply twice a day.10% rapidly. apply twice a day.
b.b. Add topical tretinoin, applied at bedtime. Add topical tretinoin, applied at bedtime. Remember to tell your patient:Remember to tell your patient: To expect redness and irritation of the face initially. To expect redness and irritation of the face initially. Urge them not to discontinue.Urge them not to discontinue.
c.c. Add topical erythromycin or topical clindamycin. Add topical erythromycin or topical clindamycin. a systemic antibiotic from the beginning.a systemic antibiotic from the beginning.
d.d. You may need to prescribe a systemic tetracycline to the You may need to prescribe a systemic tetracycline to the topical benzoyl peroxide and topical tretinoin. topical benzoyl peroxide and topical tretinoin. Continue the Continue the topical antibiotic.topical antibiotic.
About Acne TreatmentAbout Acne Treatment approachapproach
The key to getting rid of acne lesions and The key to getting rid of acne lesions and preventing new ones.preventing new ones.
Psychological Support.Psychological Support. Resolution takes time. Resolution takes time. What works for one person may not work What works for one person may not work
for another. for another. A dermatologist’s help may be required.A dermatologist’s help may be required.
Treating Mild AcneTreating Mild Acne Gently washing the affected area(s) with Gently washing the affected area(s) with
warm water and a mild soap twice a day to warm water and a mild soap twice a day to remove dead skin cells and excess oil.remove dead skin cells and excess oil.
A topical over-the-counter acne treatment A topical over-the-counter acne treatment containing benzoyl peroxide or salicylic acid.containing benzoyl peroxide or salicylic acid.
Acne medications can cause an initial Acne medications can cause an initial worsening of symptoms.worsening of symptoms.
Following the Following the Acne Skin Care Guidelines
Good skin-care programGood skin-care program
cleansing gently and non abrasively.cleansing gently and non abrasively. using oil-free products, using oil-free products, leaving the skin lesions alone.leaving the skin lesions alone. It is also important to match the vehicle It is also important to match the vehicle
(lotion, cream, gel, or solution) with the (lotion, cream, gel, or solution) with the skin type. skin type.
Gels and solutions tend to be more drying, Gels and solutions tend to be more drying, whereas lotions and creams are whereas lotions and creams are somewhat more emoliant .somewhat more emoliant .
Patients with acne should avoidPatients with acne should avoid
occlusive clothingocclusive clothing rubbing face or picking skinrubbing face or picking skin. . Oily cosmeticsOily cosmetics
Treatment measures:Treatment measures:))summary)summary)A.A. Non-pharmacologic:Non-pharmacologic: Gentle face washing, avoidance of manipulation of acne lesions, using Gentle face washing, avoidance of manipulation of acne lesions, using
water based cosmetics only, water based cosmetics only, and using oil-free moisturizers only.and using oil-free moisturizers only.
B. B. Pharmacologic:Pharmacologic: Step 1:Step 1: Begin with benzoyl peroxide gel. Begin with benzoyl peroxide gel.
Step 2:Step 2: Add topical tretinoin or adapalene (Consider using step 1 in the Add topical tretinoin or adapalene (Consider using step 1 in the morning and step 2 in the evening)morning and step 2 in the evening)
Step 3:Step 3: Add topical antibiotic (erythromycin, clindamycin). (Consider using Add topical antibiotic (erythromycin, clindamycin). (Consider using step3 along with a combination of steps1 and 2)step3 along with a combination of steps1 and 2)
Step 4:Step 4: Add systemic antibiotics, such as tetracycline, minocycline, Add systemic antibiotics, such as tetracycline, minocycline, doxycycline, erythromycin, clindamycin,or trimethoprim-doxycycline, erythromycin, clindamycin,or trimethoprim-sulfamethoxazole).Consider using a combination of steps 1, 2, 3, and 4(.sulfamethoxazole).Consider using a combination of steps 1, 2, 3, and 4(.
Step 5:Step 5: For severe nodular-cystic acne only, For severe nodular-cystic acne only, use oral isotretinoin (associated with serious, dose-related side effects)use oral isotretinoin (associated with serious, dose-related side effects)
Common myths believed by patientsCommon myths believed by patients
::
A. A. Acne is caused by failure to wash away dirt. Acne is caused by failure to wash away dirt. Not true Not true –– Acne can be made worse by washing too vigorously.Acne can be made worse by washing too vigorously.B. B. Too much junk food causes acne. Too much junk food causes acne. Not true Not true –– No connection between diet and acne.No connection between diet and acne.C.C. Stress can cause acne. Stress can cause acne. Not true Not true –– However,stress can increase a nervous tendency to pick, squeeze, However,stress can increase a nervous tendency to pick, squeeze,
and/or rub pimples and make them worse.and/or rub pimples and make them worse.D.D. Acne is a normal adolescent problem of no consequence that should Acne is a normal adolescent problem of no consequence that should
be allowed to run its course. be allowed to run its course. Not true Not true –– Prompt treatment can prevent severe outbreaks and avoid physical Prompt treatment can prevent severe outbreaks and avoid physical
and emotional scarring.and emotional scarring.E. E. Acne vulgaris always clears up after adolescence.Acne vulgaris always clears up after adolescence.Not trueNot true,, More than 10% of individuals continue to have this form of acne well More than 10% of individuals continue to have this form of acne well
into adulthood.into adulthood.
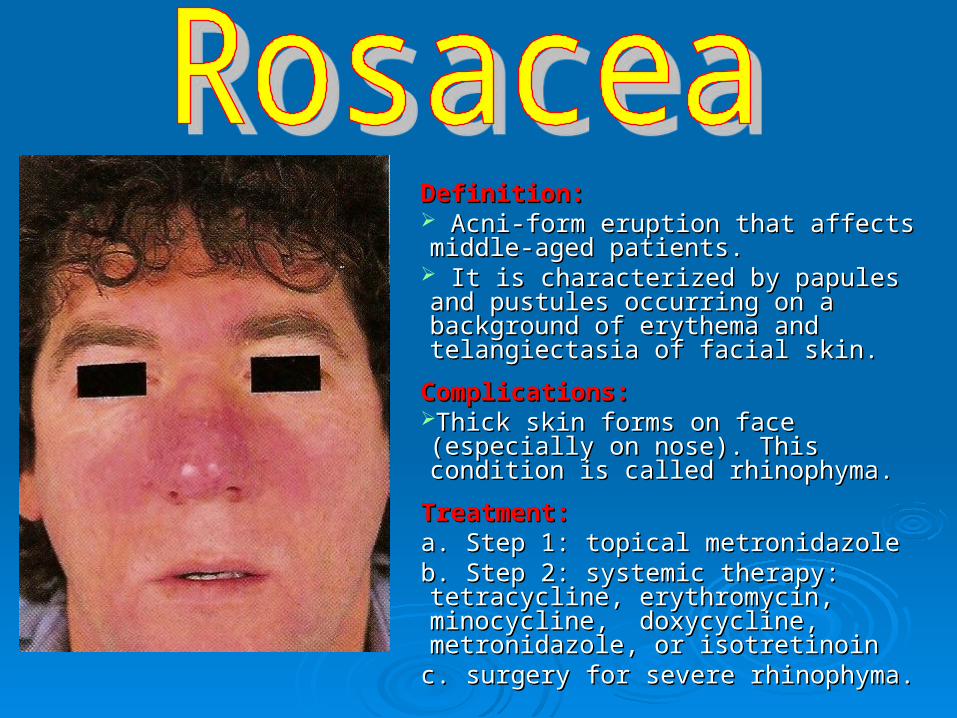
Definition:Definition: Acni-form eruption that affects middle-Acni-form eruption that affects middle-aged patients. aged patients.
It is characterized by papules and It is characterized by papules and pustules occurring on a background of pustules occurring on a background of erythema and telangiectasia of facial skin.erythema and telangiectasia of facial skin.
Complications:Complications:Thick skin forms on face (especially on Thick skin forms on face (especially on nose). This condition is called rhinophyma.nose). This condition is called rhinophyma.
Treatment:Treatment:a. Step 1: topical metronidazolea. Step 1: topical metronidazoleb. Step 2: systemic therapy: tetracycline, b. Step 2: systemic therapy: tetracycline, erythromycin, minocycline, doxycycline, erythromycin, minocycline, doxycycline, metronidazole, or isotretinoinmetronidazole, or isotretinoin
c. surgery for severe rhinophyma.c. surgery for severe rhinophyma.
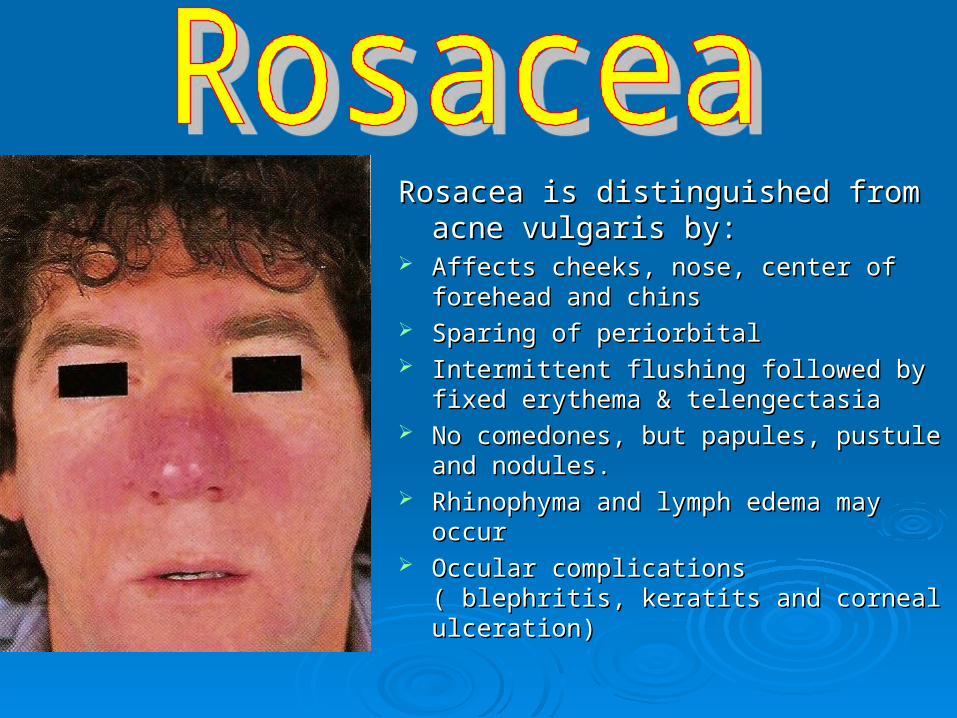
Rosacea is distinguished from acne Rosacea is distinguished from acne vulgaris by:vulgaris by:
Affects cheeks, nose, center of forehead Affects cheeks, nose, center of forehead and chinsand chins
Sparing of periorbitalSparing of periorbital Intermittent flushing followed by fixed Intermittent flushing followed by fixed
erythema & telengectasiaerythema & telengectasia No comedones, but papules, pustule and No comedones, but papules, pustule and
nodules. nodules. Rhinophyma and lymph edema may occurRhinophyma and lymph edema may occur Occular complications ( blephritis, keratits Occular complications ( blephritis, keratits
and corneal ulceration)and corneal ulceration)

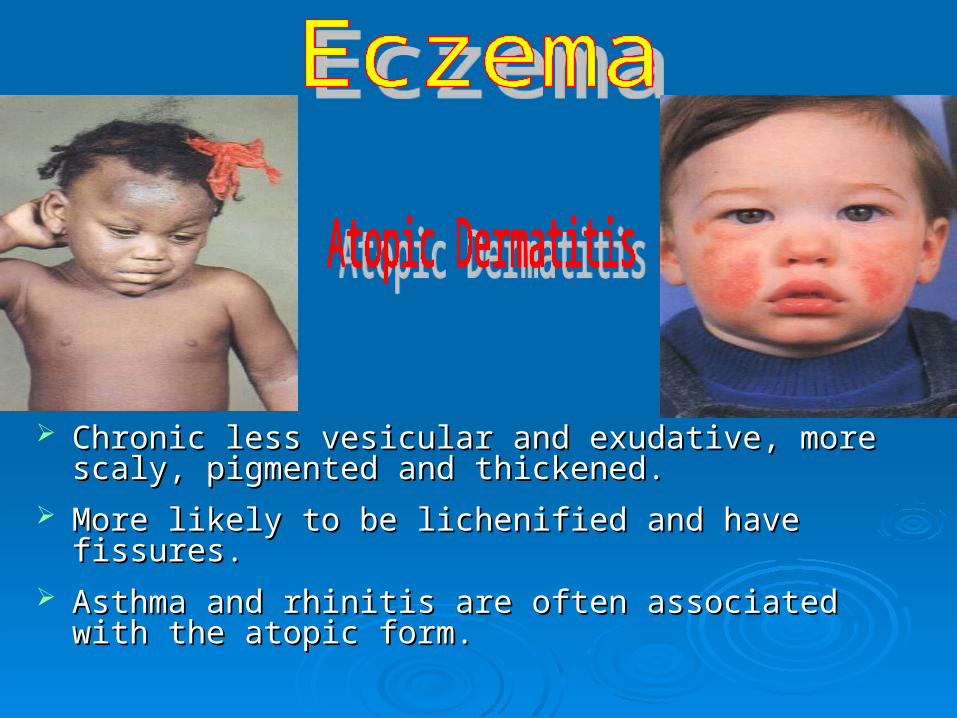
Chronic less vesicular and exudative, more scaly, Chronic less vesicular and exudative, more scaly, pigmented and thickened. pigmented and thickened.
More likely to be lichenified and have fissures.More likely to be lichenified and have fissures.
Asthma and rhinitis are often associated with the atopic Asthma and rhinitis are often associated with the atopic form.form.
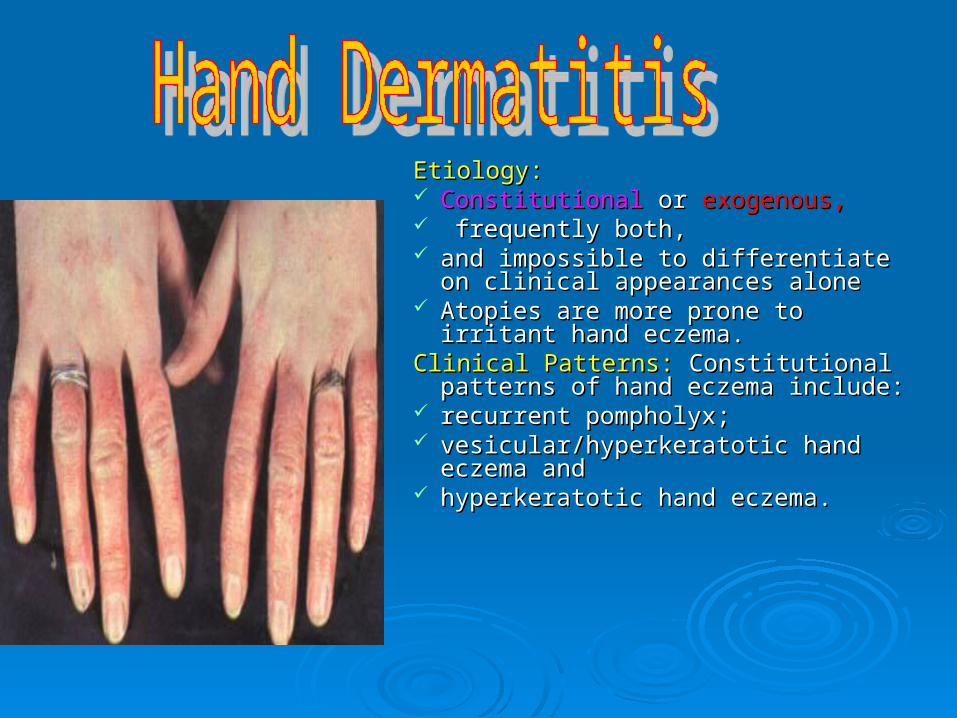
Etiology:Etiology: Constitutional Constitutional or or exogenous,exogenous, frequently both, frequently both, and impossible to differentiate on and impossible to differentiate on
clinical appearances aloneclinical appearances alone Atopies are more prone to irritant hand Atopies are more prone to irritant hand
eczema.eczema.Clinical Patterns: Clinical Patterns: Constitutional patterns of Constitutional patterns of
hand eczema include:hand eczema include: recurrent pompholyx; recurrent pompholyx; vesicular/hyperkeratotic hand eczema vesicular/hyperkeratotic hand eczema
and and hyperkeratotic hand eczema.hyperkeratotic hand eczema.
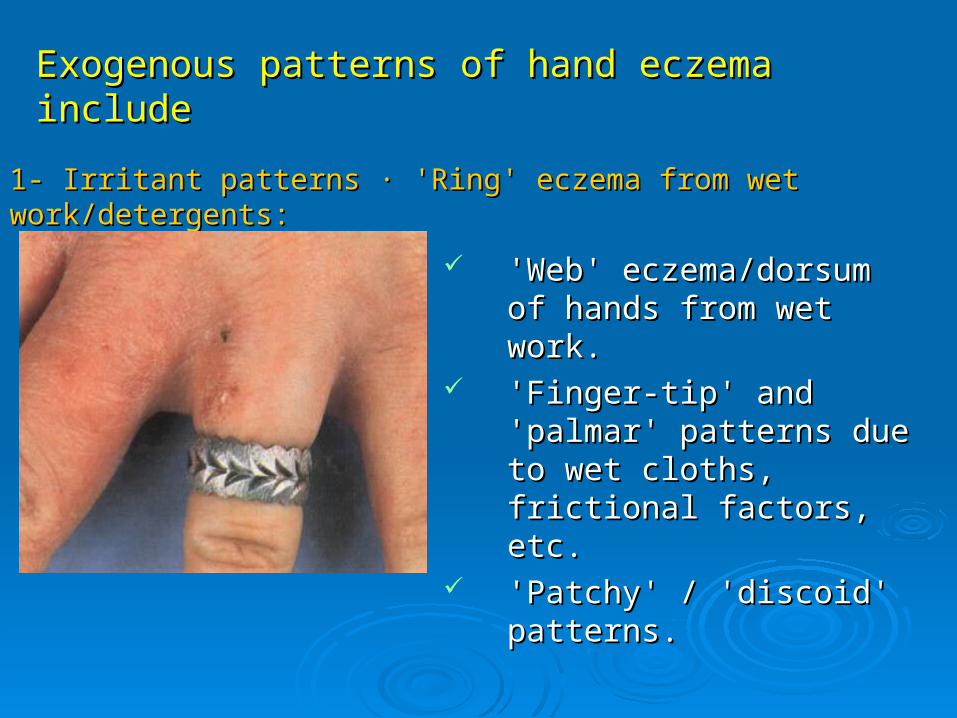
'Web' eczema/dorsum of 'Web' eczema/dorsum of hands from wet work.hands from wet work.
'Finger-tip' and 'palmar' 'Finger-tip' and 'palmar' patterns due to wet cloths, patterns due to wet cloths, frictional factors, etc.frictional factors, etc.
'Patchy' / 'discoid' patterns.'Patchy' / 'discoid' patterns.
Exogenous patterns of hand eczema includeExogenous patterns of hand eczema include
1- Irritant patterns 1- Irritant patterns ·· 'Ring' eczema from wet work/detergents: 'Ring' eczema from wet work/detergents:
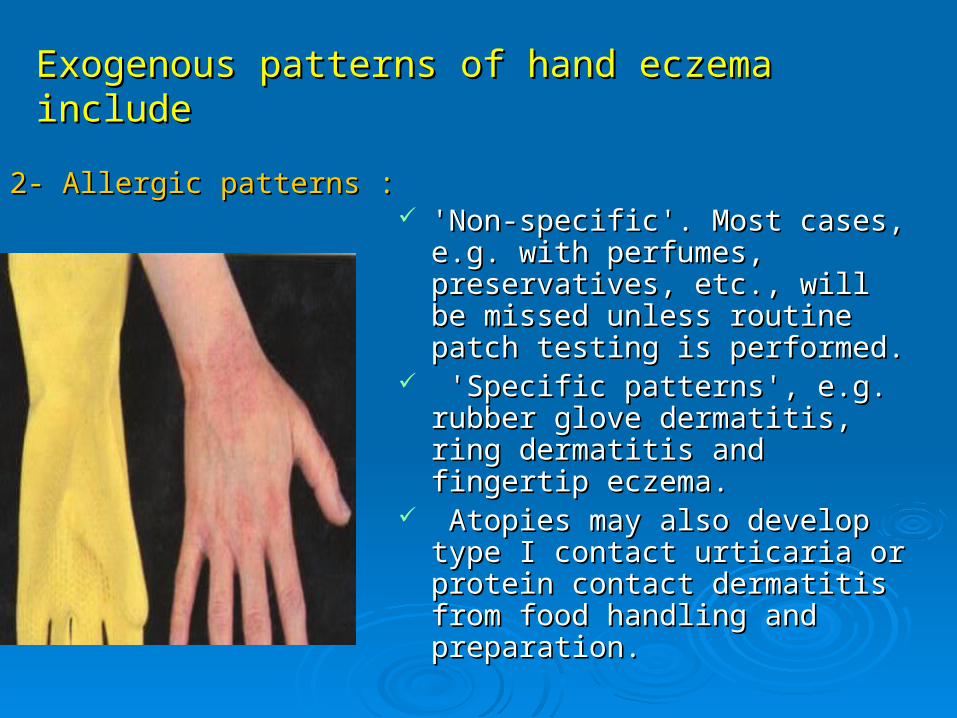
'Non-specific'. Most cases, e.g. 'Non-specific'. Most cases, e.g. with perfumes, preservatives, with perfumes, preservatives, etc., will be missed unless etc., will be missed unless routine patch testing is routine patch testing is performed.performed.
'Specific patterns', e.g. rubber 'Specific patterns', e.g. rubber glove dermatitis, ring dermatitis glove dermatitis, ring dermatitis and fingertip eczema.and fingertip eczema.
Atopies may also develop type I Atopies may also develop type I contact urticaria or protein contact urticaria or protein contact dermatitis from food contact dermatitis from food handling and preparation.handling and preparation.
2- Allergic patterns :2- Allergic patterns :
Exogenous patterns of hand eczema includeExogenous patterns of hand eczema include
Identify the cause. Identify the cause. Patch testing is helpful.Patch testing is helpful. Provide hand care advice, e.g. cotton-Provide hand care advice, e.g. cotton-
lined PVC gloves for wet work and lined PVC gloves for wet work and frequent applications of emollients.frequent applications of emollients.
Potent steroids with or without Potent steroids with or without antibiotics can be used for secondary antibiotics can be used for secondary infection. infection.
Atopies with a history of eczema should Atopies with a history of eczema should be given employment counselling.be given employment counselling.
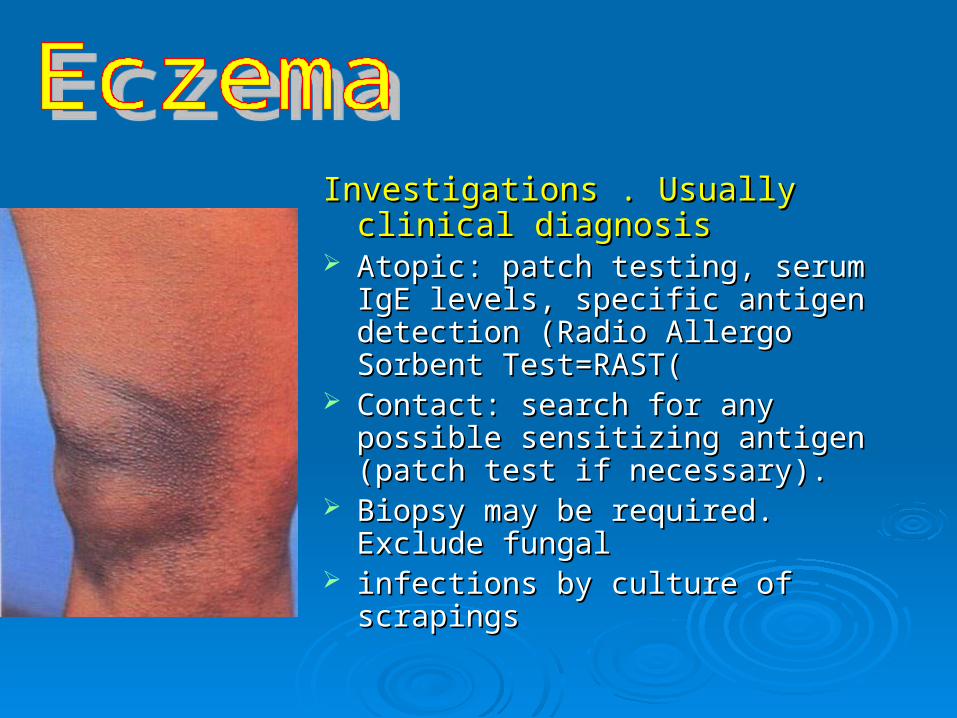
Investigations . Usually clinical Investigations . Usually clinical diagnosisdiagnosis
Atopic: patch testing, serum IgE Atopic: patch testing, serum IgE levels, specific antigen detection levels, specific antigen detection (Radio Allergo Sorbent Test=RAST((Radio Allergo Sorbent Test=RAST(
Contact: search for any possible Contact: search for any possible sensitizing antigen (patch test if sensitizing antigen (patch test if necessary). necessary).
Biopsy may be required. Exclude Biopsy may be required. Exclude fungalfungal
infections by culture of scrapings infections by culture of scrapings
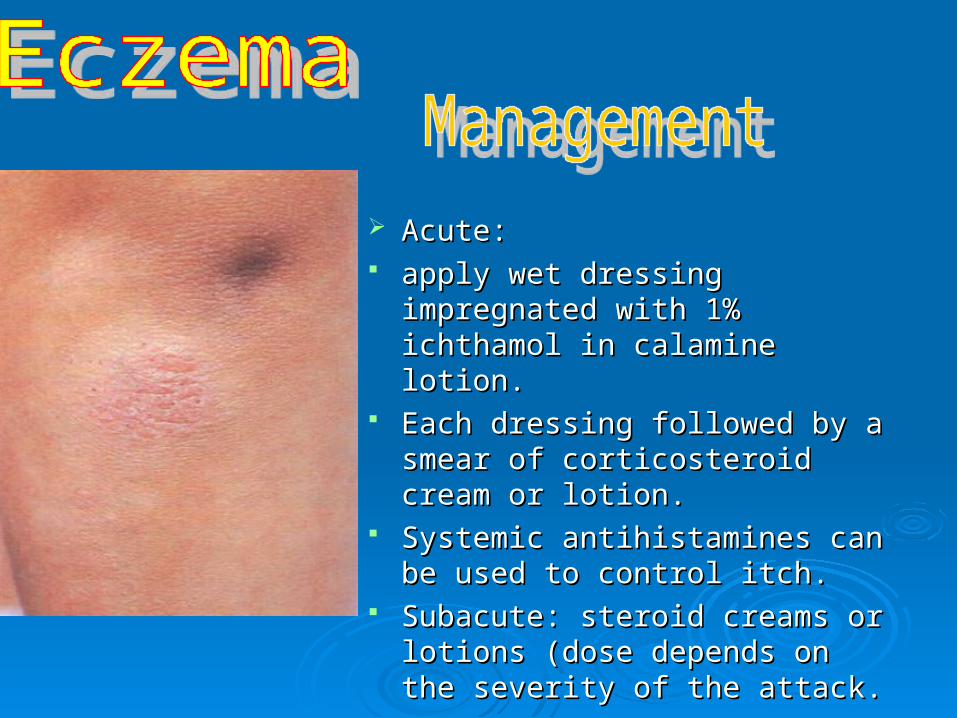
Acute: Acute: apply wet dressing impregnated apply wet dressing impregnated
with 1% ichthamol in calamine with 1% ichthamol in calamine lotion. lotion.
Each dressing followed by a Each dressing followed by a smear of corticosteroid cream or smear of corticosteroid cream or lotion.lotion.
Systemic antihistamines can be Systemic antihistamines can be used to control itch.used to control itch.
Subacute: steroid creams or Subacute: steroid creams or lotions (dose depends on the lotions (dose depends on the severity of the attack.severity of the attack.
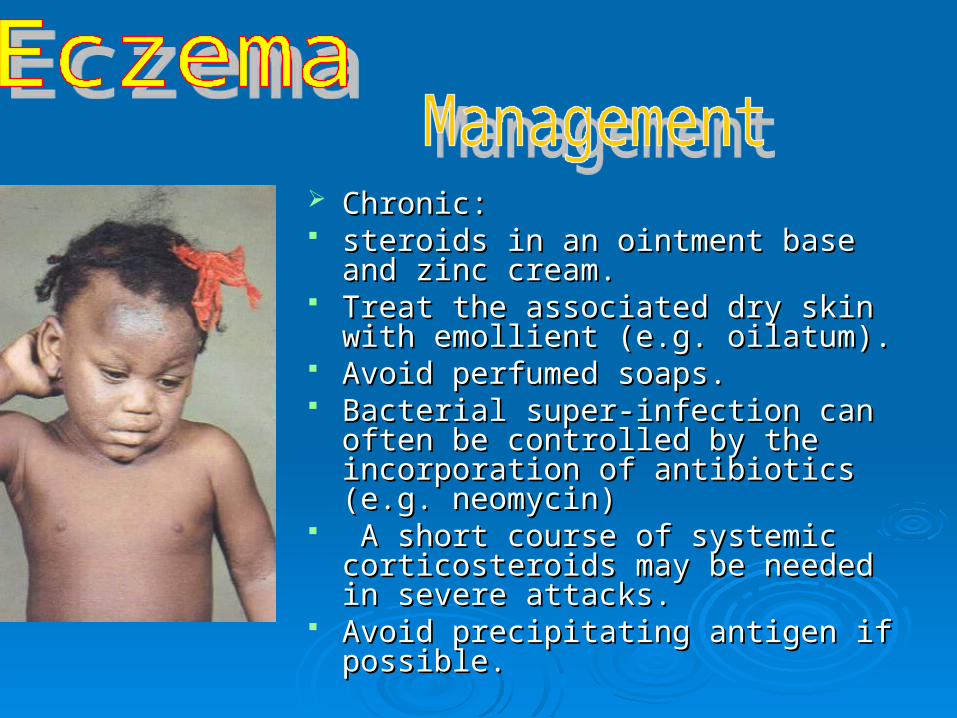
Chronic: Chronic: steroids in an ointment base and zinc steroids in an ointment base and zinc
cream.cream. Treat the associated dry skin with Treat the associated dry skin with
emollient (e.g. oilatum).emollient (e.g. oilatum). Avoid perfumed soaps.Avoid perfumed soaps. Bacterial super-infection can often be Bacterial super-infection can often be
controlled by the incorporation of controlled by the incorporation of antibiotics (e.g. neomycin)antibiotics (e.g. neomycin)
A short course of systemic A short course of systemic corticosteroids may be needed in severe corticosteroids may be needed in severe attacks.attacks.
Avoid precipitating antigen if possible.Avoid precipitating antigen if possible.
Complications:Complications: Higher incidence of warts and fungal Higher incidence of warts and fungal
infections in the atopic form.infections in the atopic form. Occasionally widespread viral infections Occasionally widespread viral infections
e.g. herpes simplex.e.g. herpes simplex. Time may be lost from work or alternative Time may be lost from work or alternative
employment may be necessary.employment may be necessary.
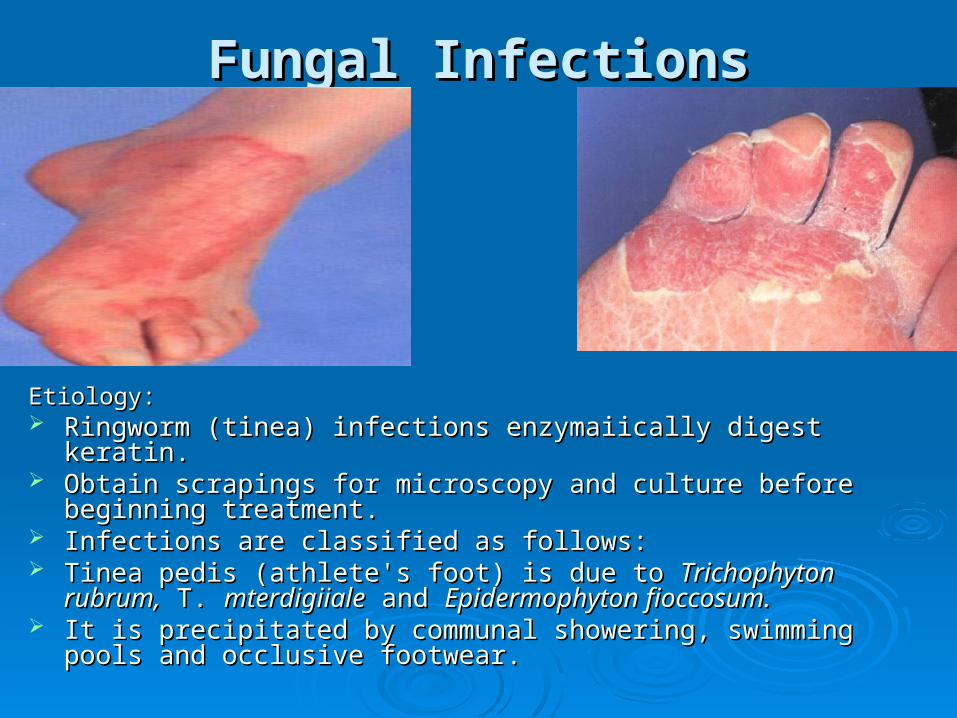
Fungal InfectionsFungal Infections
Etiology:Etiology: Ringworm (tinea) infections enzymaiically digest keratin. Ringworm (tinea) infections enzymaiically digest keratin. Obtain scrapings for microscopy and culture before beginning Obtain scrapings for microscopy and culture before beginning
treatment.treatment. Infections are classified as follows:Infections are classified as follows: Tinea pedis (athlete's foot) is due to Tinea pedis (athlete's foot) is due to Trichophyton rubrum,Trichophyton rubrum, T. T.
mterdigiialemterdigiiale and and Epidermophyton fioccosum.Epidermophyton fioccosum. It is precipitated by communal showering, swimming pools and It is precipitated by communal showering, swimming pools and
occlusive footwear.occlusive footwear.

Fungal InfectionsFungal Infections
Tinea manuum is predominantly due to Tinea manuum is predominantly due to T. rubrum.T. rubrum. Tinea cruris is caused by the same organisms as tinea Tinea cruris is caused by the same organisms as tinea
pedis.pedis. Tinea corporis is caused by all types of ringworm.Tinea corporis is caused by all types of ringworm.
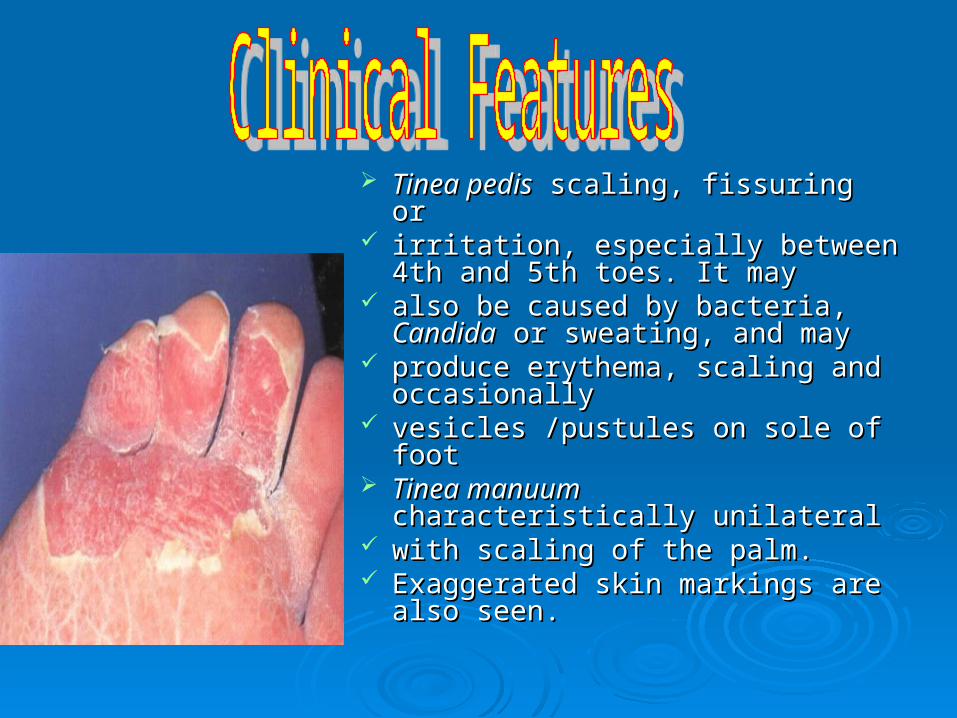
Tinea pedisTinea pedis scaling, fissuring or scaling, fissuring or irritation, especially between 4th irritation, especially between 4th
and 5th toes. It mayand 5th toes. It may also be caused by bacteria, also be caused by bacteria,
CandidaCandida or sweating, and may or sweating, and may produce erythema, scaling and produce erythema, scaling and
occasionallyoccasionally vesicles /pustules on sole of footvesicles /pustules on sole of foot Tinea manuumTinea manuum characteristically characteristically
unilateralunilateral with scaling of the palm. with scaling of the palm. Exaggerated skin markings are Exaggerated skin markings are
also seen.also seen.
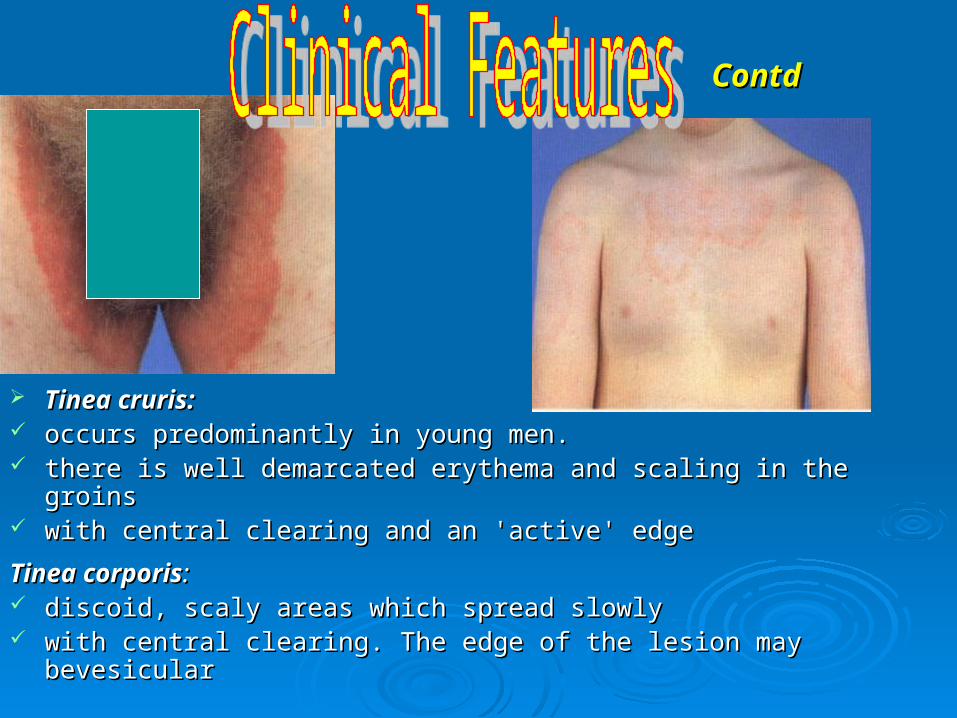
Tinea cruris:Tinea cruris: occurs predominantly in young men. occurs predominantly in young men. there is well demarcated erythema and scaling in the groinsthere is well demarcated erythema and scaling in the groins with central clearing and an 'active' edgewith central clearing and an 'active' edge
Tinea corporisTinea corporis:: discoid, scaly areas which spread slowlydiscoid, scaly areas which spread slowly with central clearing. The edge of the lesion may bevesicularwith central clearing. The edge of the lesion may bevesicular
ContdContd
TreatmentTreatment
Topical antifungal agents e.g. Whitfield's Topical antifungal agents e.g. Whitfield's ointment or imidazole creams/lotion, Castellani's ointment or imidazole creams/lotion, Castellani's paint for interdigitai macerationpaint for interdigitai maceration..
Giriseofulvin 500 mg daily (with food) for 4- 5 Giriseofulvin 500 mg daily (with food) for 4- 5 weeks or,weeks or,
one of the newer oral anti-fungals such as one of the newer oral anti-fungals such as terbinafine or miconozole may be necessary for terbinafine or miconozole may be necessary for T, rubrumT, rubrum or more extensive infections or more extensive infections..
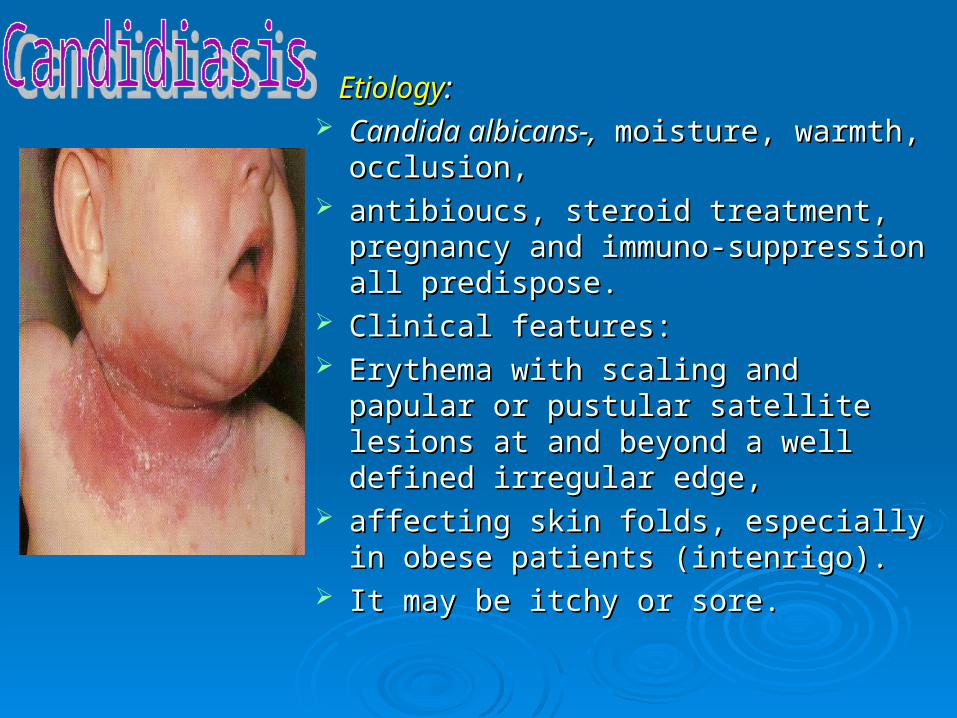
EtiologyEtiology:: Candida albicans-,Candida albicans-, moisture, warmth, moisture, warmth,
occlusion,occlusion, antibioucs, steroid treatment, pregnancy antibioucs, steroid treatment, pregnancy
and immuno-suppression all predispose.and immuno-suppression all predispose. Clinical features:Clinical features: Erythema with scaling and papular or Erythema with scaling and papular or
pustular satellite lesions at and beyond a pustular satellite lesions at and beyond a well defined irregular edge, well defined irregular edge,
affecting skin folds, especially in obese affecting skin folds, especially in obese patients (intenrigo). patients (intenrigo).
It may be itchy or sore. It may be itchy or sore.
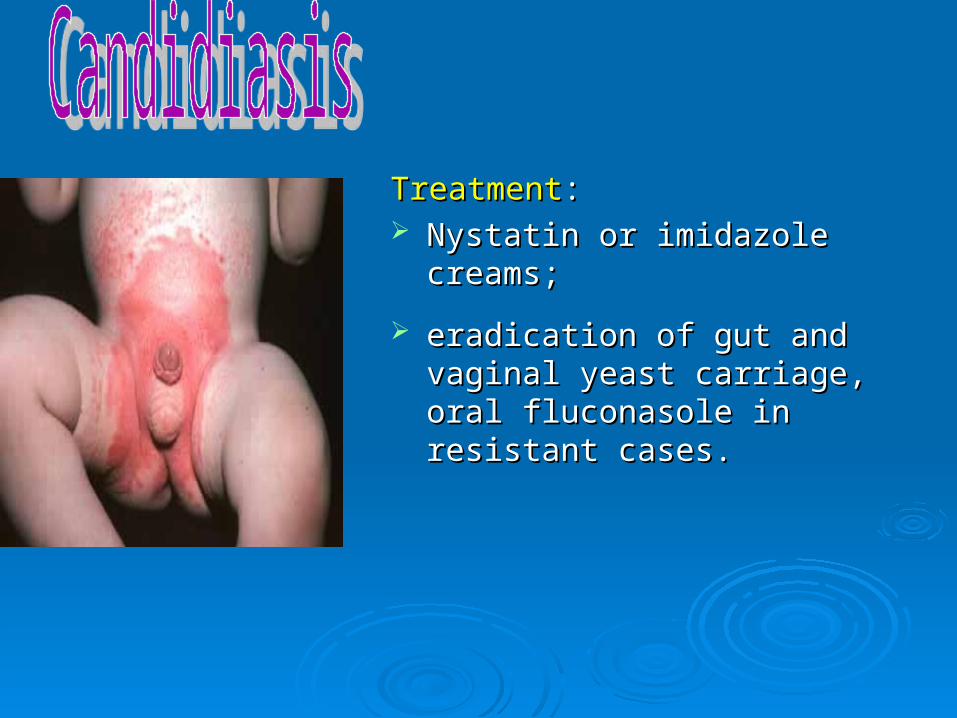
TreatmentTreatment:: Nystatin or imidazole creams; Nystatin or imidazole creams;
eradication of gut and vaginal yeast eradication of gut and vaginal yeast carriage, oral fluconasole in resistant carriage, oral fluconasole in resistant cases.cases.
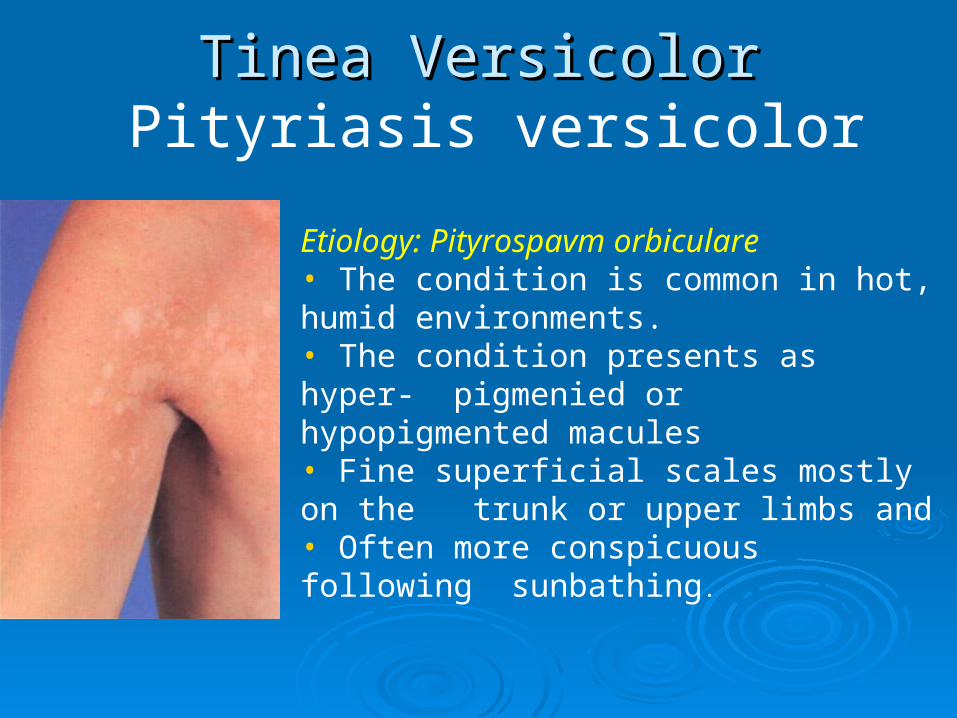
Tinea Versicolor Tinea Versicolor Pityriasis versicolor
Etiology: Pityrospavm orbiculare • The condition is common in hot, humid environments.• The condition presents as hyper- pigmenied or hypopigmented macules• Fine superficial scales mostly on the trunk or upper limbs and • Often more conspicuous following sunbathing.
Treatment
Selenium sulphide or ketoconazole shampoos and, topical imidazole creams. Oral miconazole (nizoral) may be used in resistant
cases. It may take several months for normal skin color to
return, and the condition tends to relapse.
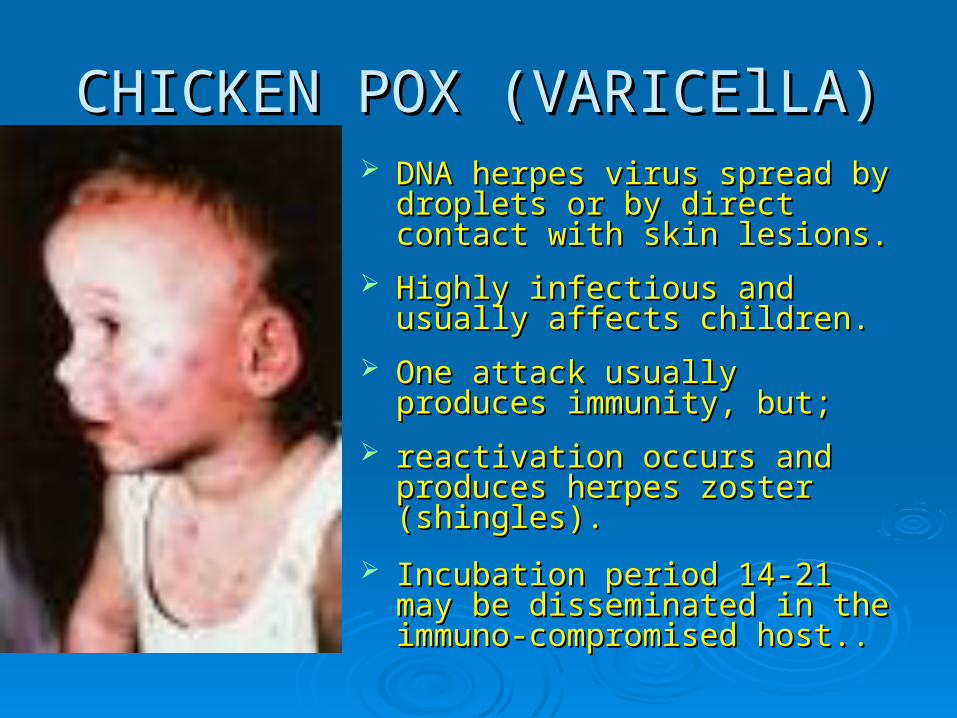
CHICKEN POX (VARICElLA)CHICKEN POX (VARICElLA) DNA herpes virus spread by DNA herpes virus spread by
droplets or by direct contact with droplets or by direct contact with skin lesions. skin lesions.
Highly infectious and usually affects Highly infectious and usually affects children.children.
One attack usually produces One attack usually produces immunity, but;immunity, but;
reactivation occurs and produces reactivation occurs and produces herpes zoster (shingles). herpes zoster (shingles).
Incubation period 14-21 may be Incubation period 14-21 may be disseminated in the immuno-disseminated in the immuno-compromised host..compromised host..
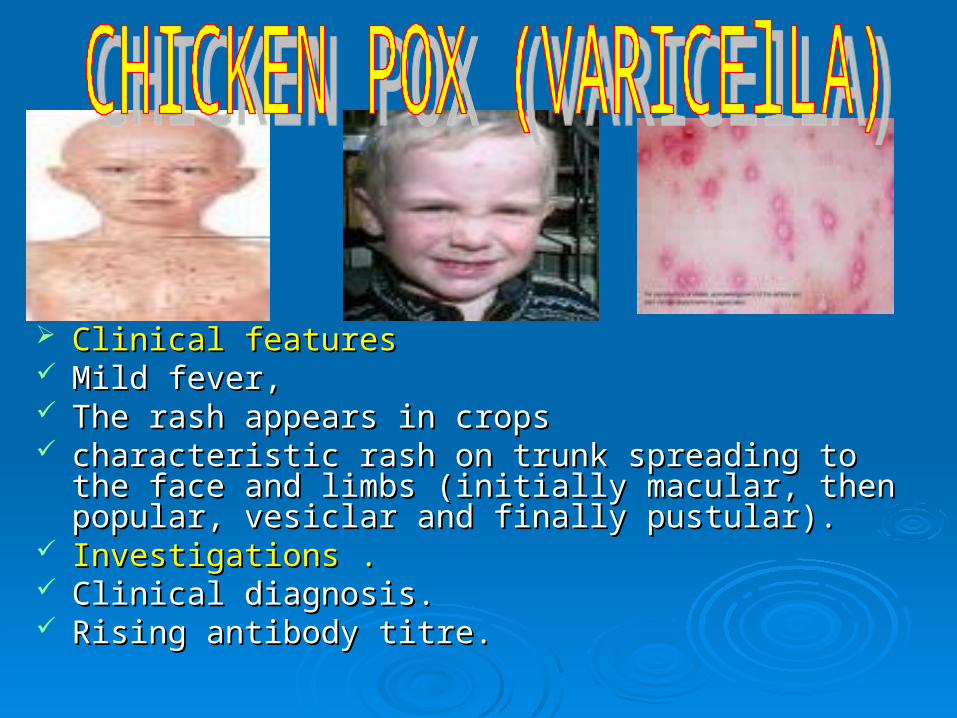
Clinical featuresClinical features Mild fever, Mild fever, The rash appears in cropsThe rash appears in crops characteristic rash on trunk spreading to the face and characteristic rash on trunk spreading to the face and
limbs (initially macular, then popular, vesiclar and finally limbs (initially macular, then popular, vesiclar and finally pustular). pustular).
Investigations .Investigations . Clinical diagnosis. Clinical diagnosis. Rising antibody titre.Rising antibody titre.
ComplicationsComplications 2ndary infection, pneumonia 2ndary infection, pneumonia
(leaves calcified scar on CXR), (leaves calcified scar on CXR), proliferative glomerulonephritis, proliferative glomerulonephritis, demyeilinating ecephalitis.demyeilinating ecephalitis. Manaagement Varicella: Manaagement Varicella: symptomatic. symptomatic. If secondary skin infection occurs If secondary skin infection occurs
use topical chlorhexidine. Oral use topical chlorhexidine. Oral augmentin. augmentin.
Human anti-varicella Human anti-varicella immunoglobulin can be given to immunoglobulin can be given to the immnocompromised the immnocompromised

Etiology Varicella-zoster virus Etiology Varicella-zoster virus (dormant in dorsal root ganglion after (dormant in dorsal root ganglion after childhood chickenpox).childhood chickenpox).
Clinical features: Clinical features: Pain in the affected dermatome. Pain in the affected dermatome. After 1- 3 days, there are clustered, After 1- 3 days, there are clustered,
red papules which become vesicular red papules which become vesicular then pustular. then pustular.
There may be fever, malaise and There may be fever, malaise and lymphadenopathy. Pain may persist lymphadenopathy. Pain may persist for months.for months.
Involvement of ophthalmic division of Involvement of ophthalmic division of trigeminal nerve may cause trigeminal nerve may cause keratitis/blindness. keratitis/blindness.
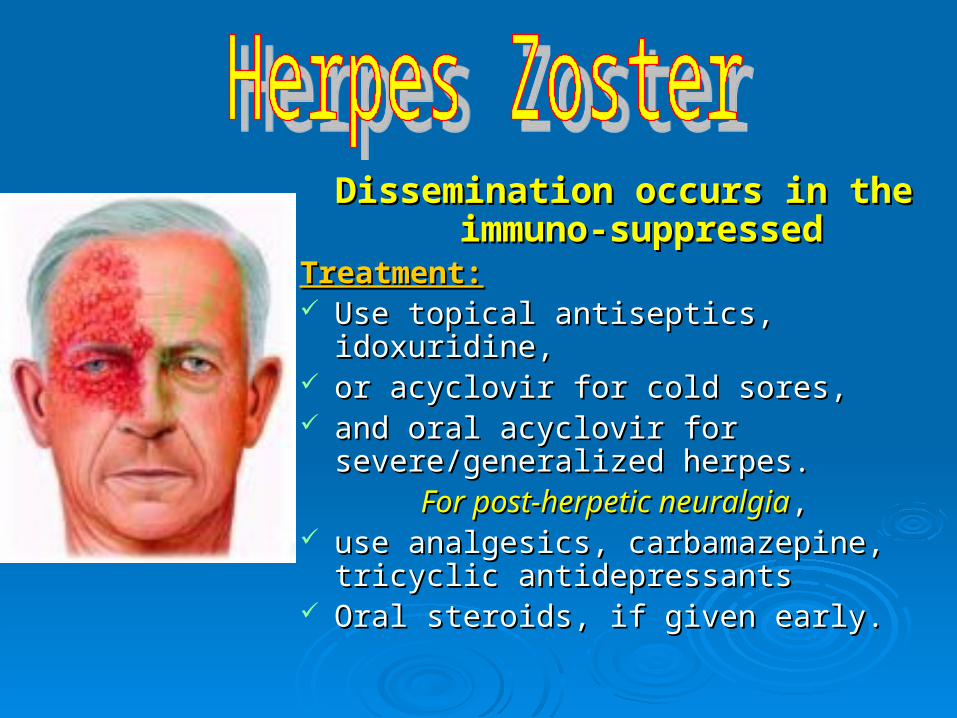
Dissemination occurs in the Dissemination occurs in the immuno-suppressedimmuno-suppressed
Treatment:Treatment: Use topical antiseptics, idoxuridine, Use topical antiseptics, idoxuridine, or acyclovir for cold sores, or acyclovir for cold sores, and oral acyclovir for severe/generalized and oral acyclovir for severe/generalized
herpes. herpes. For post-herpetic neuralgiaFor post-herpetic neuralgia, ,
use analgesics, carbamazepine, tricyclic use analgesics, carbamazepine, tricyclic antidepressants antidepressants
Oral steroids, if given early.Oral steroids, if given early.
Etiology:Etiology: Psoriasis affects approximately 2% of the Psoriasis affects approximately 2% of the
population. population. Genetic factors are important: 40% of Genetic factors are important: 40% of
patients have a positive family history. patients have a positive family history. There is a rapid epidermal transit time with There is a rapid epidermal transit time with
increased epidermal cell production increased epidermal cell production
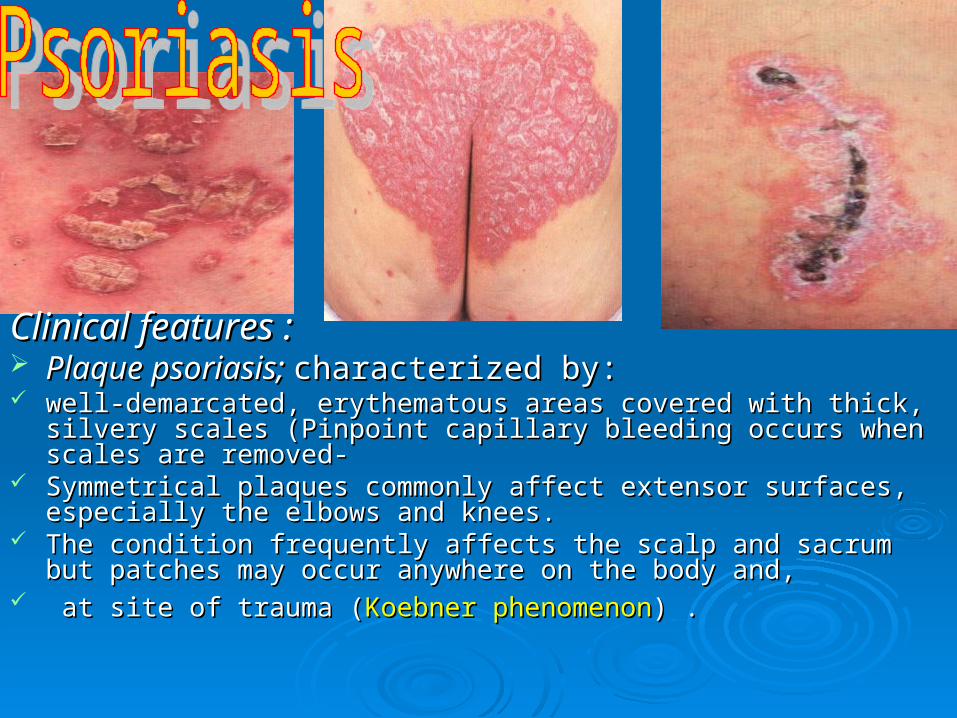
Clinical features :Clinical features : Plaque psoriasis; Plaque psoriasis; characterized by: characterized by: well-demarcated, erythematous areas covered with thick, silvery scales well-demarcated, erythematous areas covered with thick, silvery scales
(Pinpoint capillary bleeding occurs when scales are removed- (Pinpoint capillary bleeding occurs when scales are removed- Symmetrical plaques commonly affect extensor surfaces, especially the Symmetrical plaques commonly affect extensor surfaces, especially the
elbows and knees. elbows and knees. The condition frequently affects the scalp and sacrum but patches may The condition frequently affects the scalp and sacrum but patches may
occur anywhere on the body and,occur anywhere on the body and, at site of trauma (at site of trauma (Koebner phenomenonKoebner phenomenon) .) .
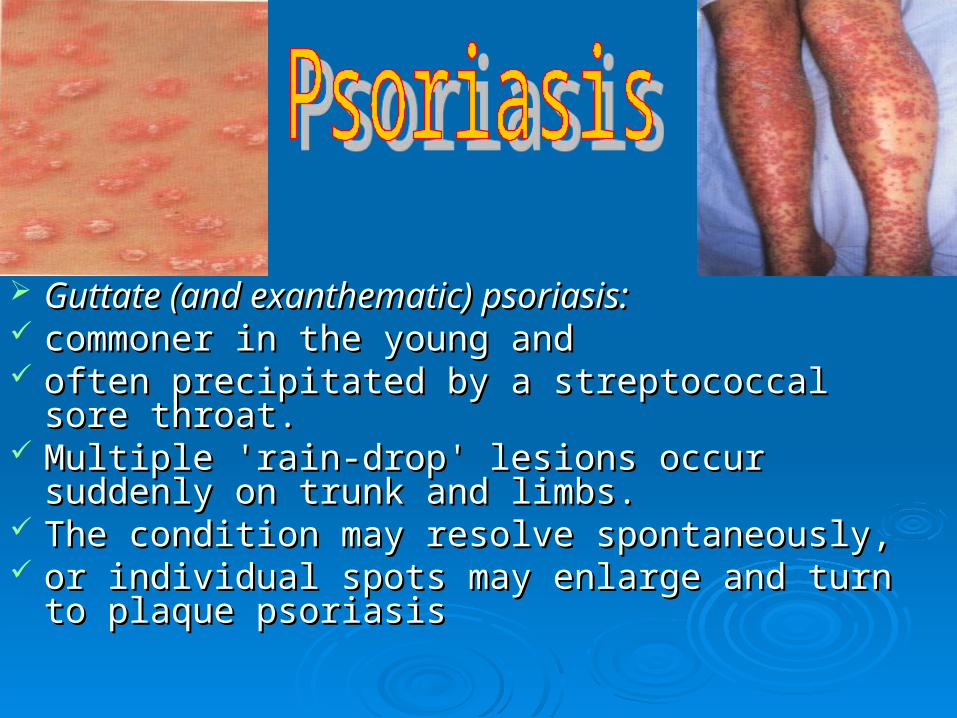
Guttate (and exanthematic) psoriasis:Guttate (and exanthematic) psoriasis: commoner in the young and commoner in the young and often precipitated by a streptococcal sore throat. often precipitated by a streptococcal sore throat. Multiple 'rain-drop' lesions occur suddenly on trunk Multiple 'rain-drop' lesions occur suddenly on trunk
and limbs. and limbs. The condition may resolve spontaneously, The condition may resolve spontaneously, or individual spots may enlarge and turn to plaque or individual spots may enlarge and turn to plaque
psoriasispsoriasis
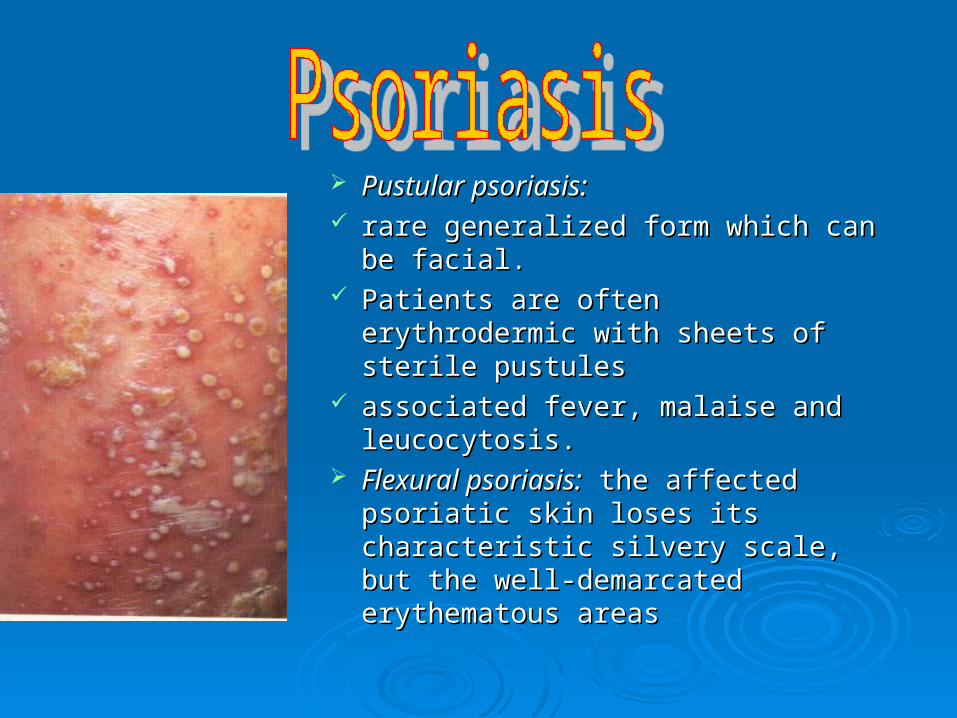
Pustular psoriasis:Pustular psoriasis: rare generalized form which can be rare generalized form which can be
facial. facial. Patients are often erythrodermic Patients are often erythrodermic
with sheets of sterile pustules with sheets of sterile pustules associated fever, malaise and associated fever, malaise and
leucocytosis.leucocytosis. Flexural psoriasis:Flexural psoriasis: the affected the affected
psoriatic skin loses its characteristic psoriatic skin loses its characteristic silvery scale, but the well-silvery scale, but the well-demarcated erythematous areasdemarcated erythematous areas
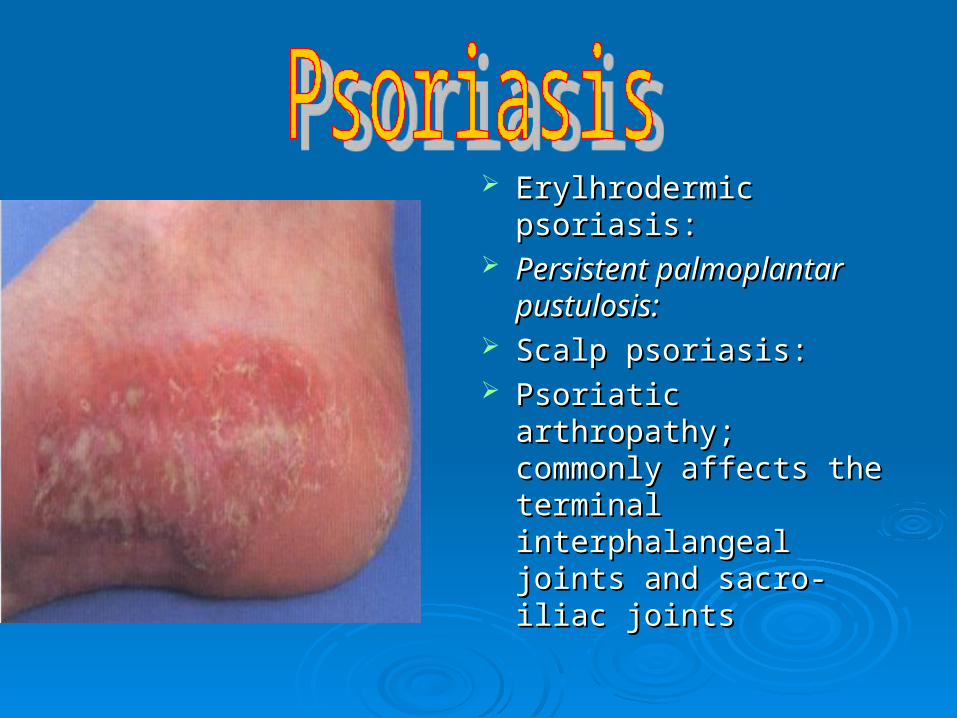
Erylhrodermic psoriasis:Erylhrodermic psoriasis: Persistent palmoplantar Persistent palmoplantar
pustulosis:pustulosis: Scalp psoriasis: Scalp psoriasis: Psoriatic arthropathy; Psoriatic arthropathy;
commonly affects the commonly affects the terminal interphalangeal terminal interphalangeal joints and sacro-iliac joints and sacro-iliac jointsjoints
Topical steroids:Topical steroids: Controversial effective, but Controversial effective, but continued use may lead to lessening of effect continued use may lead to lessening of effect
Another treatment modality, e.g. tar; effects of a Another treatment modality, e.g. tar; effects of a coal tar preparation (at night), remain very useful coal tar preparation (at night), remain very useful for intertriginous areas.for intertriginous areas.
Tar:Tar: can be used , but replaced by anthralin or can be used , but replaced by anthralin or dithranol (tar stains clothes)!!dithranol (tar stains clothes)!!
Dithranol: useful for plaque psoriasis inpatients Dithranol: useful for plaque psoriasis inpatients and replaced tarand replaced tar
Ultraviolet light (UVB): E0-E1 dose alone or combined Ultraviolet light (UVB): E0-E1 dose alone or combined with tar/tar baths. with tar/tar baths.
A newer treatment combining psoralen with UVA (PUVA) A newer treatment combining psoralen with UVA (PUVA) is even more clearing extensive refractory psoriasisis even more clearing extensive refractory psoriasis
Vitamin D, ointment (calcipitriol):Vitamin D, ointment (calcipitriol): a new topical treatment a new topical treatment for psoriasis, with an efficacy equivalent to topical for psoriasis, with an efficacy equivalent to topical steroids.steroids.
Systemic therapy:Systemic therapy: cytotoxic drugs, e.g. methotrexate, cytotoxic drugs, e.g. methotrexate, cyclosporin, etc. are treatments normally only initiated by cyclosporin, etc. are treatments normally only initiated by dermatologists.dermatologists.
Scalp psoriasis regimens: keratolytics, tar shampoos, Scalp psoriasis regimens: keratolytics, tar shampoos, topical steroids as lotions/gels.topical steroids as lotions/gels.