Assessment of the Trauma Patient.pdf

of 25
-
Upload
cotovairinax -
Category
Documents
-
view
219 -
download
0
Transcript of Assessment of the Trauma Patient.pdf
-
8/10/2019 Assessment of the Trauma Patient.pdf
1/25
91
OBJECTIVESUpon completion of this chapter, the reader should be able to:
Identify the components involved in the scene size up.
Differentiate between the golden hour and the platinum ten minutes and discuss the importance of
each in providing care to the multisystem trauma patient.
Apply the trauma triage protocols, based on mechanism of injury and physical assessment findings.
Identify the components of the initial assessment using the acronym ABCDE.
Acquired systematic approach to performing a physical assessment of the trauma patient.
Differentiate singular system trauma from multisystem trauma.
Identify load-and-go patients based on assessment findings.
Identify conditions requiring immediate definitive field treatment from those requiring treatment once en
route to the most appropriate facility.
Identify and discuss the essential equipment required to handle multisystem trauma patients.
Identify the components of the focused assessment.
KEY TERMSCUPS classification system Multisystem trauma
Decerebrate Platinum ten minutes
Decorticate Singular system trauma
Golden hour Stick-em-up positionLoad and go
Assessment of
the Trauma
Patient
6
C h a p t e r
In the late 1960s, ambulance personnel began to actu-ally treat seriously injured patients in the prehospitalsetting, and the era of scoop and swoop began to dis-appear. However, many critically injured, multisystemtrauma patients received care for injuries that wereobvious, but minor, while they died from severe hypox-emia or shock prior to arrival at a medical facility. Withthe indoctrination of the Advanced Trauma Life
Support (ATLS) course for emergency physicians, thescoop-and-swoop form of prehospital care reemerged,but with a new focus: the rapid identification andresuscitation of life-threatening conditions prior totransport that result in compromised airway, breathing,circulation, and neurological status. No longer arethese patients grounded for long periods of time withfield personnel trying to stabilize these injuries prior to
-
8/10/2019 Assessment of the Trauma Patient.pdf
2/25
transport. The old credo, stabilize the patient beforeleaving the scene, which had replaced scoop andswoop, has been replaced by the battle cry loadand go.1 It is no longer acceptable for the paramedicto delay transportation while attempting to start IVs,auscultate a blood pressure, bandage simple soft tissue
wounds, or splint minor fractures when the patientsairway, breathing, circulatory, or neurological status areseverely compromised. Our load-and-go patients arethose who present with decreased level of conscious-ness (LOC), compromised airway or difficulty breath-ing, sucking chest wounds, large flail segments, tensionpneumothorax, signs or symptoms of shock, head injurywith altered LOC or unequal pupils, indications ofabdominal trauma, unstable pelvis, bilateral femurfractures, or a combination of these criteria. In manag-ing load-and-go patients appropriately, we have real-ized that these patients must be transported to themost appropriate medical facility, which may not be
the closest medical facility, in order to decrease mortal-ity and morbidity. A fact of considerable significance toemergency medical service providers is that 70% oftrauma deaths occur in remote or rural areas wherepatients are treated at medical facilities unable toappropriately manage their multiplicity of traumainjuries.1 The paramedic must be able to rapidly, sys-tematically, and correctly identify load-and-go patientsand initiate transport to the most appropriate medicalfacility if survival rates are to increase.
SCENE SIZE UP
The initial observation during the approach to thescene will provide early clues regarding the potentialfor multisystem trauma. Prearrival information pro-vided by the emergency medical dispatcher (EMD)will often provide patient information that will enablethe paramedic to predict what injuries may exist uponarrival. Unfortunately, initial dispatch information isoften sketchy due to inadequate information from theperson reporting the incident. In any event, try toobtain as much information regarding the scene fromthe dispatcher as possible so that some prearrival deci-sions can be made regarding equipment and other
backup assistance.Upon arrival make a quick assessment of thescene. Ascertain if it is safe to proceed into the scene.Determine if there are hazards that will require spe-cialized equipment (e.g., fire apparatus, HAZ-MATspecialists, rescue tools). Call for law enforcement tocontain the area prior to entry if needed. Ask the fol-lowing questions:
Is there a fire or imminent danger of fire orexplosion?
Are any vehicles carrying hazardous materials?
Is there danger from oncoming vehicles?
Are all disabled vehicles out of the way ?
What is the mood of the bystanders? Do theyappear to be hostile or calm and approachable?
Is the vehicle or structure unstable, requiring spe-cial stabilizing equipment prior to approaching theinjured patient(s)?1
Once the scene has been deemed safe to enter,determine the mechanisms of injury and the kinemat-ics involved in producing the injury (see Chapter 5).Based on the mechanism, determine the injuries thatmay exist from the appearance of the scene, thepatients position or location, and bystander informa-tion obtained. Ask the following questions:
Are there obvious signs of injury that suggest life-threatening injuries may exist?
How many patients appear to be involved and are
additional personnel, resources, and EMS unitsneeded?
Do you need to employ triage?
Upon arrival, the paramedic must gather theequipment necessary to provide initial field care to life-threatening injuries. With critically injured patients,precious time is wasted returning to the ambulanceseveral times for equipment. Essential equipment thatshould be carried to each scene includes:
1. Personal protective equipment (PPE)
2. Long spine board, straps, head-immobilizingdevice, and cervical-immobilizing device
3. Oxygen (O2) and airway management equipment[O2 delivery devices, bag valve mask (BVM), suc-tion device, decompression supplies, intubationequipment]
4. Trauma kit that contains dressing-bandage mate-rial, blood pressure cuff, stethoscope, IV equip-ment and other supplies for trauma care
5. Pneumatic antishock garment (PASG) per localprotocol
ASSESSMENT AND MANAGEMENT
PRIORITIESThe majority of trauma patients have singular systemtrauma, that is, trauma that does not systemicallycompromise the patient. Less than 10% of all traumapatients are considered multisystem trauma, andtherefore, the paramedic must be able to quickly iden-tify these load-and-go patients from those with minortrauma.2 According to Donald D. Trunkey, the time ofdeath from trauma has a trimodal distribution:3
1. Within seconds to minutes
92 Chapter 6
-
8/10/2019 Assessment of the Trauma Patient.pdf
3/25
2. Within minutes to hours (golden hour)
3. Within several days or weeks after the initialinjury
Therefore, in dealing with multisystem traumapatients, the paramedic identifies and manages life-threatening conditions under specific time constraints.
This requires that assessment, diagnosis, stabilization,management, and reassessment be performed rapidlyand systematically.
Time is the vital link to patient survival whendealing with a multisystem trauma patient. Thegolden hour, as publicized by the Maryland Institutefor Emergency Medical Services, is the accepted stan-dard for these patients. R. Adams Cowley discoveredthat when the critically injured, multisystem traumapatient is received into surgery within an hour of injury,approximately 85% survive.4 On-scene time, includingassessment, critical interventions, and packaging,should not exceed theplatinum ten minutes,unless special circumstances dictate otherwise. Thesespecial situations include extended disentanglementtime and unexpected dangers or hazard occurrence.The average response time from the onset of the inci-dent to the arrival of EMS is 89 minutes.2 Therefore,EMS systems strive for an on-scene time of 5 minutesor less. Response times in rural areas often exceed the89 minute average, which eats deeply into the goldenhour. Therefore, the shorter the on-scene time, thesooner the patient receives critical definitive care.
As trauma care has evolved, it has become evi-dent that each patient must be transported to the most
appropriate medical facility capable of providing thetreatment required, rather than the closest facility.Table 6-1 identifies the mechanisms of injury and phys-ical findings that should prompt the paramedic to applytriage protocols that will meet the objectives of thegolden hour and platinum ten minutes.
Therefore, the initial approach is directed towardrapid identification and correction of the following fourmajor areas: airway, breathing, perfusion, and presenceor absence of significant external and internal hemor-rhage.6 Trauma patients are not assessed as thoroughlyas are medical patients; therefore, the key words arestabilization of the most immediate airway, breathing
and circulatory problems, and rapid transportation.6
ASSESSMENT
The initial assessment addresses life-threatening condi-tions and employs the following sequential five-stepapproach:2
AAirway management and cervical spine control
BBreathing (ventilation)
CCirculation and hemorrhage
DDisability
EExpose, examine, and evaluateThis assessment approach provides a systematic
and organized evaluation of the patients initial statusand allows for detection and stabilization of solely life-threatening problems on-scene. The components of theinitial assessment must be internalized, not just memo-rized. Once internalized, the initial assessment shouldimmediately surface into an automatic response, with-out hesitating to recall what step of the assessmentshould be performed next. The focus must be on whatthe assessment data reveal in relation to the patients
Assessment of the Trauma Patient 93
Mechanism of injury
Falls greater than 20 feet for adults, greater than 10 feet for
infants or children, or three times the patient s bodyheight
Death of any car occupant
Struck by a vehicle traveling greater than 20 mph
Ejection from a vehicle
Severe vehicle deformity
Rollover with signs of severe impact
Penetrating injuries to the head, chest, or abdomen
Physical findings
Pulse greater than 120 beats per minute (bpm) or less
than 50 bpmSystolic blood pressure (BP) less than 90 millimeters of
mercury (mm Hg)
Respiratory rate less than 10 or greater than 30 breaths
per minute
Glasgow Coma Score less than 13
Penetrating trauma, excluding extremities
Flail chest
More than two proximal long-bone fractures
Burns greater than 15% total body surface area (TBSA)
Facial and airway burns
Table 6-1
Indicators of Multisystem Trauma
Visit the Electronic Medicine Web site at
http://www.medicine.com. Click on the
Emergency Medicine folder. Then click on the
Trauma and Orthopedics on-line book. Review the
chapter on Hemorrhagic Shock.
INTERNET ACTIVITIES
-
8/10/2019 Assessment of the Trauma Patient.pdf
4/25
overall physiological status, and how the patterns ofinjuries and conditions are affecting overall aerobicmetabolism and homeostatic well-being. The paramedicmust be able to analyze assessment data and, based onthat data, anticipate, predict, and appropriately managethe patient in order to prevent further detrimental
effects. The paramedic should follow, as closely as possi-ble, the order of the initial assessment, keeping in mindthere are circumstances that require deviation from thesurvey format (e.g., severe external hemorrhage requir-ing immediate treatment when the patient is obviouslybreathing upon initial approach). When the paramedicmust deviate from the order of the survey, vital organsystem assessment may be omitted; therefore, it isimportant to go back to the previous steps if they wereomitted initially.
Multisystem trauma patients quickly deteriorateinto anaerobic metabolism as a result of inadequate tis-sue perfusion. This is described as a four-component
deterioration:1. Inadequate oxygenation of the red blood cells
(RBCs) in the lungs
2. Inadequate delivery of the RBCs to the tissuecells
3. Inadequate distribution of the oxygen to thetissues
4. Inadequate availability of RBCs necessary todeliver oxygen to tissue cells
The paramedic is able to appropriately and adequatelymanage the first two phases of deterioration during thefirst steps of the initial assessment by rapidly evaluatingand resuscitating those conditions that are physiologi-cally linked to this deterioration. A clinically competentparamedic, who has developed a consistent approach tothe assessment of every patient, will be able to deter-mine whether or not the problem is immediately lifethreatening and if it involves singular or multisystemtrauma in less than 2 minutes.4
The initial assessment begins upon arrival andincludes scene size up and a global evaluation of thepatients respiratory, circulatory, and neurological sta-tus.2 Upon approaching the scene, the paramedicanswers the following: Does the patient appear to be
conscious? What is the patients position? Is the patientmoving or does he or she appear to be unresponsive?2
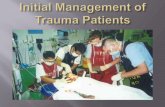
A sweeping glance over the patient may detect grossexternal hemorrhage or deformity or extreme use ofaccessory or neck muscles, possibly indicating severeairway compromise. The paramedic may see that thepatient is extremely pale, exhibiting restlessness andagitation, indicative of early signs of shock. A patientwith an injury around cervical spine vertebrae number6 (C-6) often lies with forearms flexed across his or herchest and hands half closed. Another position often
assumed with spinal injury is the arms flexed andextended above the head, termed the stick-em-upposition1 (see Figure 6-1). Movement of the patientout of this position should not be attempted, unless theairway is compromised, until adequate personnel areavailable to move the patient as a unit.1
While comparing the initial global assessmentfindings with scene size up, mechanism of injury(MOI), and kinematic findings, begin formulating aninitial impression of whether the patient is a singular ora multisystem trauma patient. This global assessmenttakes about 15 seconds and provides a rapid gross eval-uation of the patients respiratory, circulatory, and neu-rological functions.7
It is a fundamental instinct to reach the injuredpatient(s) as quickly as possible. However, if possible, it isbest to approach the patient from the front. If responsiveto verbal stimuli, the patient may turn his or her head orbody toward the sounds of approaching personnel. This
excessive or sudden body movement could produce fur-ther injury to the C-spine or other internal organ struc-tures if injury is already present. If unable to assume afrontal approach, the paramedic should avoid startling orstimulating the patient during the approach. Often a sim-ple statement, such as please dont move, we are here tohelp, will prevent unnecessary patient movement.
94 Chapter 6
FIGURE 6-1 Stick-em-up position often assumed by the
patient with a spinal injury.
FIGURE TO COME
-
8/10/2019 Assessment of the Trauma Patient.pdf
5/25
It is important to repeat the phrase please remainstill as you approach and once you arrive at the patientsside. The lead paramedic should direct his or her part-ner or first responder to obtain manual stabilization ofthe patients head and neck, using a trauma jaw thrustprocedure to open the airway. It is assumed that all
trauma patients have the potential for spinal injury and,therefore, all suspected trauma patients should be man-ually stabilized in this manner (see Figure 6-2). Caremust be taken not to intentionally stimulate the patientwho appears to be unconscious until manual stabilizationhas been obtained, because the patient may turn his orher head laterally or rotate his or her body in an attemptto locate voice or touch. If manual stabilization isobtained before the LOC is assessed, the paramedicmay avoid a disastrous outcome for the patient.
Airway
Airway management and control are two of the mostimportant priorities of care when confronted with amultisystem trauma patient. The airway can be openedusing a trauma jaw thrust maneuver. If the patientshead is not in a neutral position, the paramedic mustgently move it into a neutral position unless resistance ismet with movement or the patient develops intolerablepain. If the patient is in a seated position or lying on theground, someone may need to take frontal or lateral sta-bilization of the head and neck until another respondercan assume a posterior, kneeling, or on-ground position(see Figures 6-3 and 6-4). When manual stabilization isobtained, the paramedic places his or her fingers on the
mandibular curve, gently pushing forward to create anopen airway without hyperextension of the head.
Assessment begins with evaluation of the patientsLOC. If the patient is not verbally responding, theparamedic must gently tap while verbally stimulating aresponse from the patient. It is importantnot to shakethe patient because doing so could aggravate existinginjuries. A verbally responsive or moaning patient indi-
cates an open airway. Any patient with a decreasedLOC is considered a load-and-go patient and shouldreceive immediate oxygenation with 100% oxygendelivered by a nonrebreathing mask or, if respirationsare inadequate, by BVM assist. Paramedics should be
Assessment of the Trauma Patient 95
FIGURE 6-2 Manual stabilization of the head and neck
using a trauma jaw thrust to manage the patients airway.
FIGURE 6-3 Manual stabilization of the head from behind
the seated patient.
FIGURE 6-4 Manual stabilization of a supine patients head
and neck.
-
8/10/2019 Assessment of the Trauma Patient.pdf
6/25
very attentive to the airway of a patient with an alteredmental status. These patients may have difficulty man-aging oral secretions. Once opened, the airway shouldbe immediately suctioned to clear blood, debris, andsecretions, if present.
The paramedic must gather further information
regarding the patients perfusion status if there is a ver-bal response elicited with the initial LOC assessment.This assessment can occur simultaneously as the para-medic continues to assess the patency of the patientsairway by asking how the incident occurred, the generaltime of day, general location, and the patients name. Ifthe patient is alert but confused, this is indicative ofearly inadequate tissue perfusion. Again, immediateresuscitation with 100% oxygen with a nonrebreathingmask should be initiated.
During this initial assessment, the paramedicmust listen for signs indicative of airway compromise.Are there silent, snoring, gurgling, or stridorous soundspresent that may require immediate action such asrepositioning the airway, removing a foreign body air-way obstruction, suctioning, or immediate intubation?Any delay in recognizing and resuscitating these condi-tions will lead to increased hypoxemia, anaerobicmetabolism, acidosis, and possibly death. Figure 6-5provides an algorithm for assessment of the airway.
Breathing
Trauma patients revert to anaerobic metabolism prima-rily due to hypoxemia. Simultaneous assessment of thepatients breathing status is conducted while thepatients airway is being opened and during the initialLOC evaluation. This initial evaluation focuses on the
patients relative respiratory rate (normal, fast, or slow)and quality of ventilations, and employs the look, listen,and feel method of evaluation.
First, the paramedic must determine if thepatient has spontaneous respirations. This is accom-plished by looking, listening, and feeling for breathingand chest excursion. Noisy or windy environments mayinterfere with hearing or feeling the patients exhaledair. Under such conditions it may be necessary toauscultate breathing by placing the head of the stetho-scope over the trachea at the suprasternal notch. Thiswill provide clear, audible air movement sounds upon
inspiration and expiration in breathing patients.
7
Immediate resuscitation is required if there are nospontaneous respirations or if the patient has agonalrespirations. Initially, this should be accomplished byinsertion of an oropharyngeal or nasopharyngeal airwayand use of a BVM with 100% oxygen. If this method ofairway control and ventilation is effectively oxygenatingthe patient, it is not necessary to immediately intubate.
96 Chapter 6
Algorithm Assessment Actions
Control C-spine Open airwayEstablish LOC
compromise?
Airway
Resuscitate
Cervical spine MOI
Alert/responsive
Airway obstruction
Silent
Snoring
Stridor
Gurgling
Manual stabilization
Approach patient from front
Trauma jaw thrust PRN
Load and go?
Clear
Obstruction/suction
Bag-valve-mask
Load and go?
FIGURE 6-5 Airway assessment algorithm.
-
8/10/2019 Assessment of the Trauma Patient.pdf
7/25
Intubation can be delayed until there are adequatepersonnel on-scene to quickly accomplish this proce-dure or until the patient is loaded into the ambulance.
Patients with spontaneous respirations should beevaluated for breathing difficulty. First, the paramedicdetermines if the patient is experiencing an irregular
breathing pattern, apnea, bradypnea, hypopnea,tachypnea, or dyspnea. Look for signs of respiratorydistress or compromise, which include pallor, cyanosis,nasal flaring, tracheal tugging, use of accessory mus-cles, intercostal muscle retractions, and diaphragmaticbreathing. With a C-6 injury, intercostal muscles will beparalyzed, severely compromising respiratory efforts.An injury at C-4 will paralyze the diaphragm, makingbreathing virtually impossible, and the patient will beusing accessory muscles in the neck to breathe.1 If anyof these signs are present, immediate resuscitativeefforts must be initiated. The patient will quickly dete-riorate if allowed to continue this inadequate ventila-
tory process. An apneic, bradypneic, or hypopneicpatient must receive assisted ventilation with 100%oxygen using a BVM. The tachypneic or dyspneicpatient may need assisted ventilation, or may only needto be placed on 100% oxygen by a nonrebreathingmask. The paramedic determines which oxygen deliv-ery device is going to be the most beneficial to thepatients current ventilatory pattern and which devicethe patient will tolerate. This determination is based onthe general rules of airway and breathing managementfound in Table 6-2.
The initial goal of breathing assessment is to detectlife-threatening conditions. Therefore, the next step in
the assessment process should be to seek out the etiologyof the respiratory compromise, especially if tachypnea ispresent. Remember, tachypnea is indicative of hypoxia,acidosis, and anaerobic metabolism. The paramedicshould quickly expose and assess the patients chest forsymmetry, paradoxical movement, sucking chest wounds,impalements, ecchymosis, hueing, deformity, or obvioussigns of blunt trauma to the chest wall. If the patient hasan injury to the lower cervical or upper thoracic spinalcord, there may be paralysis of the intercostal muscles.These types of injuries may present with abdominalbreathing, which may be detected during the assessmentfor symmetrical movement of the chest wall.
Bilateral breath sounds should be auscultated todetermine if the breath sounds are clear, equal, dimin-ished, or absent. This auscultation should be quick,using a two-point midaxillary assessment (see Figure6-6). Percussion can detect hyporesonance or hyperres-onance but is often difficult to perform in the prehospi-tal setting due to ambient noise. Pneumothorax, tensionpneumothorax, hemothorax, hemo-pneumothorax, andflail chest are conditions often responsible for inade-quate ventilation.
The final step of the breathing assessment involvespalpating the anterior neck for jugular venous distention(JVD) or flatness and assessing the trachea for deviation(see Figure 6-7). Jugular venous distention is associatedwith a building tension pneumothorax, or pericardialtamponade, whereas flat neck veins can indicate hemor-rhage and hypovolemia. However, it must be remem-bered that approximately 34 cm of venous engorgementis normal in patients lying supine. Venous engorgementin excess of this amount signifies JVD while flat neckveins in a supine patient may indicate hypovolemia.
If JVD or tracheal deviation is present, the patientis severely compromised and must be transported assoon as possible. Positive JVD associated with a tensionpneumothorax must be definitively resuscitated with
Assessment of the Trauma Patient 97
Adult respiratory rates
Less than 12 is considered slow and may be associatedwith central nervous system (CNS) trauma.
Less than 10 is inadequate.
Twelve to 20 is considered a normal range but may have
inadequate tidal volume.
Greater than 20 and up to 24 is considered possible early
warning sign of developing respiratory/circulatory
compromise.
Greater than 24 and up to 30 indicates developing
respiratory and systemic compromise associated with
hypovolemia.
Greater than 30 indicates hypoxemia, acidosis, orhypoperfusion.
Resuscitation rules of management
Respiratory rates less than 12 require assisted or total
ventilatory control with a fraction of inspired oxygen
(FiO2) of 0.85 or greater.
Respiratory rates of 1220 may need supplemental 100%
O2
by nonrebreather or assisted ventilations if the tidal
volume is very shallow or the LOC is depressed.
Respiratory rates of greater than 20 and up to 30 require
supplemental O2or assisted ventilation.
Respiratory rates of greater than 30 should receiveassisted ventilation with 100% O
2and early intubation
may be required to maintain full ventilatory control.
Source:Adapted from PHTLS Basic and Advanced Prehospital
Trauma and Life Support. (4th ed.), by N.E. McSwain, J.L.
Paturas, E.M. Wertz, 1999, Mosby: St. Louis.
Table 6-2
General Rules of Airway and Breathing
Management
-
8/10/2019 Assessment of the Trauma Patient.pdf
8/25
needle decompression and assisted ventilation with100% oxygen. The paramedic must also decidewhether intubation can be delayed until the patient isen route to the medical facility. Any patient who isunable to maintain an airway, has a high risk of aspira-tion, displays a large flail segment, presents with airwayinjuries or midface trauma, or has a Glasgow ComaScore of less than 9 requires a definitively secured air-way as soon as possible.2
If the patient must be assist ventilated or hyper-ventilated, the paramedic stabilizing the head and neckcan provide this treatment by placing his or her kneeson either side of the patients head. It will be important
that someone obtain manual stabilization frontallywhile the paramedic assumes this position. This allowsall other treatment personnel to focus on completion ofthe assessment process and preparation of the patientfor packaging and transport. Figure 6-8 presents analgorithm for assessment of breathing.
Circulation and Hemorrhage
Circulatory assessment is divided into three compo-nents: assessment of cardiac output, exsanguinatinghemorrhage, and, if internal hemorrhage is suspected,PASG survey .9 Failure of the circulatory system resultsin inadequate delivery of oxygen to the target tissue
cells, which leads to the signs and symptoms associatedwith inadequate tissue perfusion. Initial assessment ofcardiac output, cardiovascular status, and perfusion sta-tus can be rapidly obtained during the initial assess-ment of central and peripheral pulses, skin color, skintemperature, and capillary refill time. Quantitative vitalsigns may be included during this phase of the initialassessment only if adequate personnel are available toperform this assessment without interruption of thefocused assessment process.
Assessment of Pulses The patients carotid and
radial pulse should be evaluated simultaneously forpresence, quality, equality, and regularity. At this timeonly a relative rate and quality will be obtained. If aradial pulse is palpable, this establishes an initial base-line estimate that the patients systolic blood pressure isat least 8090 mm Hg depending on the strength ofthe pulse (see Table 6-3 for a comparative analysis ofperipheral pulses and systolic blood pressure). A radialpulse that is tachycardic and weak or weakening maybe the first indicator that the patient is experiencingcirculatory system failure or shock. Unexplained tachy-cardia may be indicative of internal hemorrhage, espe-cially intra-abdominal hemorrhage. An absent radial
pulse indicates the patients blood pressure is below 80mm Hg and that the patient is profoundly hypovolemic.A radial pulse that is full, bounding, and bradycardicmay be suggestive of increasing intracranial pressure(ICP). Refer to Chapter 11 for an in-depth discussion ofincreased intracranial pressure and Cushings reflex.The presence of a bounding radial pulse suggests thesystolic blood pressure (BP) is significantly above 100mm Hg. A normocardic or bradycardic pulse rate could
98 Chapter 6
Pulse Palpable at Systolic Blood Pressure of
at Least:
Radial 8090 mm Hg
Brachial 7080 mm Hg
Femoral 7080 mm Hg
Carotid 6070 mm Hg
Table 6-3
Estimating Systolic Blood Pressure Based on
Pulses
FIGURE 6-6 Auscultation of bilateral breath sounds utilizing
a two-point midaxillary assessment.
FIGURE 6-7 Jugular venous distention.
-
8/10/2019 Assessment of the Trauma Patient.pdf
9/25
be suggestive of neurogenic shock associated withspinal cord injury. The paramedic must begin to associ-ate the mechanism of injury (MOI) with assessmentfindings and analyze how these findings are directly
related to the physiological response the patient isexhibiting. Definitive field treatment relates directly tothe ability to recognize and differentiate normal fromabnormal physiological responses and how theseresponses relate to load-and-go patients.
Assessment of Skin Color and Sk inTemperature Skin color and temperature will pro-vide a rapid initial assessment of peripheral perfusion sta-tus. This assessment can be simultaneously performedduring the carotid and radial pulse check. A hypovolemicpatient will normally present with pale, cool or cold,clammy, and diaphoretic skin, whereas patients with neu-rogenic shock may present with normal to pink, warm,and dry skin below the level of spinal cord injury andpale, cool, clammy, and diaphoretic skin above the levelof cord injury. A patient with head injury may presentwith warm, sometimes hot skin temperature, and skincolor can be normal to flushed in appearance due to theincreased systolic BP.
Assessment of Capillary Refill The para-medic can quickly assess capillary refill time (CRT),
once the radial pulse check is completed, by exertingpressure to the nail beds or hypothenar eminence caus-ing the underlying tissue to blanche (see Figure 6-9). Ifthe patient is normovolemic, color will return within
2 seconds. However, if the sympathetic nervous systemhas caused a sympathomimetic response due to hypo-volemia, return of color will be greater than 2 seconds.The paramedic must keep in mind that capillary refilldelay, without the presence of other associated signs andsymptoms, may be unreliable. Changes can be caused byage, hypothermia, or simple fractures. Normal CRT mayoccur in the presence of neurogenic shock, isolated headtrauma with increasing ICP, and pharmacologicalvasodilatory medications.
Assessment of Hemorrhage External exsan-guinating hemorrhage must be rapidly detected and con-trolled to prevent deterioration of the patients cardiacoutput and perfusion status. Severe external hemorrhagemay be detected and corrected by application of directpressure, prior to any other assessment, if the patient isbreathing or if there are adequate personnel present tobegin hemorrhage control. There are circumstances thatprevent the paramedic from detecting life-threateninghemorrhage until a quick body sweep is performed (e.g.,patients size or position or inadequate lighting). Thisbody sweep generally occurs once initial airway,
Assessment of the Trauma Patient 99
Algorithm Assessment Actions
Resuscitate
O NRB mask/OPA/NPA2
Needle decompression
Load and go?
BMV with 100% O2
Assisted w/ BMV and 100%O2
Assisted w/ BMV and 100%O2
NRB mask/BVM with 100% O2
NRB mask/BVM with 100% O2
Relative rate/rhythm/quality
Expose chest
Chest symmetry/BBS
Neck veins
Tracheal deviation
Apnea
Bradypnea
Hypopnea
Tachypnea
Dyspnea
Assess breathingExpose chest
Assess BBSAssess anterior neck
Breathingdifficulty?
BVM/ETI/cricothyrotomy
FIGURE 6-8 Breathing algorithm.
-
8/10/2019 Assessment of the Trauma Patient.pdf
10/25
breathing, and circulatory status have been assessed. Itconsists of running the hands, beginning at the head,down the patient, paying particular attention to areaswhere blood can pool (e.g., posterior scapular area, lat-eral axillary area, lumbar-sacral area, medial/inner thigharea) (see Figure 6-10). As the quick sweep is performed,the paramedic is looking at his or her gloved hands forevidence of significant venous or arterial bleeding andfeeling for sudden warmth. If significant bleeding isfound, the area must be quickly exposed and the patientpositioned for visual examination of the area. Controlmethods must be initiated if significant hemorrhage isdetected. Use of pressure bandages, PASG, or even airsplints may provide adequate control, freeing the para-medic to perform other critical interventions or to con-tinue assessing the patient. Significant internalhemorrhage can occur in four body areas: the chest, theabdomen, the retroperitoneal/pelvic cavity, and the thigh.If internal hemorrhage is suspected, based on the pre-senting MOI, unexplained restlessness, tachypnea, andtachycardia, the paramedic must deviate from the strictABCDE assessment format and perform the PASG sur-vey by exposing the abdomen, pelvis, and legs. He or shemust look for hueing or ecchymosis, edema, or signs ofblunt trauma andpalpate for rigidity, swelling, or defor-
mity. A quick palpation of the pelvic region should beperformed since pelvic fractures have a high percentageof associated intra-abdominal hemorrhage. If internalhemorrhage is detected, rapid immobilization onto a longspine board with PASG in place, rapid transportation,and resuscitation with warmed IV fluids should be initi-ated. The paramedic quickly completes the initial assess-ment while the patient is being readied for transport,searching for any other life-threatening injuries that maybe present. Movement of the patient prior to completionof the assessment could aggravate undetected injuries.
Assessment of Vital Signs Quantitative vitalsigns (heart rate, respiratory rate, and blood pressure)provide necessary baseline data, especially when thepatient is rapidly deteriorating. Therefore, quantitativevital signs should be obtained as soon as possible butshould not take precedence over essential steps ofassessment, resuscitation, stabilization, and transport.Continual reevaluation of relative rate and quality ofrespirations and core versus peripheral pulses can pro-
vide adequate baseline data until the patient is en routeor adequate personnel are available to obtain quantita-tive vital signs. Figure 6-11 presents an algorithm forassessment of circulation.
Disability
Rapid neurological evaluation is a very important partof the initial assessment. It measures cerebral functionand indirectly measures cerebral oxygenation based onthe patients response to external stimuli and other
100 Chapter 6
FIGURE 6-9 Assessment of CRT by exerting pressure to the
nail beds or hypothenar eminence.
FIGURE 6-10 A quick sweep of the lumbar-sacral area forgross exsanguinating hemorrhage.
-
8/10/2019 Assessment of the Trauma Patient.pdf
11/25
assessment data. This evaluation establishes thepatients level of consciousness, pupillary size and reac-tion, and motor and sensory response in upper andlower extremities.
Assessment of Level of Consciousness The
patients initial LOC is assessed by gently tapping orverbally stimulating,not shaking, the patient to elicit aresponse at the beginning of the initial assessment. Atthat time a general idea of responsiveness is ascer-tained. Now the paramedic must perform a more defin-itive assessment using the AVPU scale (see Table 6-4).If the patient is able to verbally respond, determine ifhe or she is appropriately oriented by asking questions
related to time, place, person, and event. As cerebralfunction declines, the patient will begin to lose orienta-tion to place and events prior to the injury. As thepatient worsens, orientation to person will decline, notjust to family members, but to self as well. At this pointthe patient is moving toward unconsciousness. The
patient will respond to verbal stimuli by opening hiseyes and moving body parts when spoken to but isunable to coherently communicate. Verbal responsesare not intelligible and sound garbled or moaned.
When the patient is no longer responsive to ver-bal stimuli, the paramedic must determine the depth ofunresponsiveness by eliciting a purposeful response topain. Several methods are discussed in the literaturethat may be more appropriately used on medicalpatients (e.g., sternal rub or ear lobe pinch).7 However,these methods may produce unwanted movement inthe trauma patient. A sternal rub may cause the patientto move the torso in an attempt to avoid/escape the
painful stimuli. This movement may aggravate chest,spine, abdominal, and pelvic injuries. Pinching the earlobe could produce a severe lateral or twisting rotationof the head in an attempt to move away from the pain.Obviously, if there is cervical spine injury, this type ofmovement could be disastrous, especially if the personmanually stabilizing the head and neck is not ready for
Assessment of the Trauma Patient 101
Algorithm Assessment Actions
Resuscitate
Assesscirculation
Hypoperfusion?
Carotid/radial pulse
Relative rate/quality
Skin temp/color/capillary refill
Exsanguinating hemorrhage
PASG survey if internalhemorrhage suspected
Quantitative vital signs
Cardiopulmonaryresuscitation asneeded (PRN)
PASG
2 large-bore IVs enroute
Fluid trial PRN
Rapid infusion PRN
Load and go?
FIGURE 6-11 Circulation algorithm.
AVPU SCALEAAlert (to person, place, time, event)
VVerbal stimuli (appropriate or inappropriate response)
PPainful stimuli (appropriate or inappropriate response)
UUnresponsive
Table 6-4
Scale Used to Determine a Patients LOC
-
8/10/2019 Assessment of the Trauma Patient.pdf
12/25
this type of movement. For these reasons, the sternalrub and ear lobe pinch are not recommended.
There are two methods that can be employed toelicit a painful response with minimal risk for furtherinjury:
1. Pinch the patients upper arm, on the medial
aspect, mid-way between the antecubital spaceand axilla in the softest portion of the skin (seeFigure 6-12).
2. Take the fleshy region between the patientsthumb and forefinger, preferably in an uninjuredextremity, and pinch or squeeze it forcefully (seeFigure 6-13).
Purposeful response to this painful stimuli is indicatedby patient movement away from the pain. A twitch, orslight movement of the hand or forearm, indicatessevere cerebral dysfunction. Look for abnormal move-ments such as decorticate (rigid flexion of the arms
and extension of the legs) and decerebrate (rigidextension of the arms and legs; the back and neck maybe arched) posturing with and without this stimuli (seeFigures 6-14 and 6-15).
A patient who does not exhibit any response topainful stimuli is considered unresponsive. This is anominous sign and indicates profound hypoxemia, acido-sis, total patient decompensation, and severe inade-
quate tissue perfusion, especially cerebral hypo-perfusion. Obtaining initial baseline data regarding thepatients LOC with frequent reevaluation establishes afairly clear picture of how rapidly the patient is deterio-rating. As the patient slips down the AVPU scale, he orshe may become combative, display irrational
responses, exhibit uncooperative and belligerent behav-ior, and refuse medical help. The paramedic must trynot to antagonize the patient, knowing that the patientsbehavior may be the result of head injury, hypoxemia,and hypoperfusion. This type of behavior requiresimmediate or continued treatment with 100% oxygen.2
During this evaluation it is very important todetermine the history of the event. Specific questionswould include: Did the patient lose and regain con-sciousness prior to EMS arrival or since the injuryoccurred? Does the patient have any preexisting med-ical conditions that might be responsible for alteredLOC (e.g., diabetes, epilepsy, heart problems)? Could
there be toxic substances involved (e.g., drugs, alcohol,or other chemical substances)? The paramedic mustgather this history from the patient, family members, orbystanders, without interrupting the initial assessment.
Assessment of Pupils The pupils, controlled byhigher cranial nerves, are a direct link to the brain andprovide invaluable information concerning cerebral
102 Chapter 6
FIGURE 6-12 Painful stimuli applied by pinching the medial
aspect of the upper arm midway between the antecubital
space and axilla.
FIGURE 6-13 Painful stimuli applied by pinching or squeezing
the fleshy region between the patients thumb and forefinger.
FIGURE TO COMEFIGURE TO COME
-
8/10/2019 Assessment of the Trauma Patient.pdf
13/25
perfusion. Under normal conditions pupils reactquickly and consensually to changes in light intensity. Aquick pupil evaluation to determine if the pupils areequal, round, and reactive to light (PERRL) will pro-vide important baseline information regarding intracra-nial pathology and cerebral perfusion. A sluggish pupilreaction may reflect CNS depression from hypoxia,hypercarbia, injury, or the effects of drugs. Unequalpupils (anisocoria) may indicate eye trauma, headtrauma, or cerebrovascular accident (CVA). Dilated orfixed pupils are indicative of hypoxia, severe ICP, orCNS injury.2 Pupils are usually equal to within 1 mm,remain equal, and constrict equally when exposed to
light. Abnormal or sluggish reactions to light, signifi-cantly unequal pupils, or lack of consensual reactionusually results from insult to the brain or one of theoculomotor nerves in the absence of direct eye injury.7
Assessment of Pulse, Motor, and SensationThe paramedic should quickly perform a pulse, motor,and sensation (PMS) assessment of the upper andlower body extremities (PMS 4) during the disabilityassessment. (Note: The lower extremity PMS evalua-tion can be integrated into the expose, examine, andevaluate component of the lower extremities to savetime.) This is not an in-depth evaluation, but rather a
quick determination of neurological intactness prior tomoving the patient to a long spine board (LSB). Thiswill establish baseline assessment data for motor orsensory deficits in the extremities of a responsivepatient, which may indicate brain injury, spinal cordinjury, or injury to a limb. A deficit in distal circulationmay reflect a reduction in systemic circulation or com-promised circulation in that limb.7 Evaluation in a ver-bally responsive patient consists of:
1. Having the patient unilaterally, then bilaterally,squeeze one of your fingers, to compare the pres-
ence and equality of strength in the other extremi-ties (see Figure 6-16). This detects paralysis or pare-sis (weakness) in one or both upper extremities.
2. Having the patient unilaterally, then bilaterally,push and pull back on your hands with the feet asyou compare the strength and quality of the
movement (see Figure 6-17). Impairment mayindicate a spinal cord injury.
3. Having the patient wiggle the fingers and toes,which indicates the motor nerves are intact.
4. Asking the patient if he or she feels you touchinghis or her fingers and toes to rule out numbness,tingling, or decreased sensation.
Evaluation of the unresponsive patient consists of:
1. Pinching the fingers and toes or running a bluntobject along the palms and soles of the feet todetermine if the patient withdraws or localizesthe pain. Intact motor and sensation usually indi-cates normal or minimally impaired cortical func-tion, whereas a positive Babinski responseindicates spine injury. A positive Babinski is pres-ent if the big toe turns upward when a bluntobject is introduced to the sole of the foot (seeFigure 6-18). Normally the big toe will turndownward.
2. Exerting pressure with your thumb into thepatients palm, which should produce curling,withdrawal, or flexion.
During this evaluation the paramedic should noteany posturing displayed when painful stimuli are initi-ated. If there is no movement produced with painfulstimuli, the paramedic should assess for flaccid paraly-sis by lifting the patients forearm slightly, if there is nosign of extremity injury, and then let it fall. Absence ofany muscle tone usually denotes spinal cord injury.
Distal pulses should be assessed in each extremityand should be compared. Simultaneous assessment ofthe radial pulses and then pedal pulses can provideinvaluable assessment data regarding circulatory func-tion. The paramedic is able to determine the presence,absence, equality, and relative pulse rate, which mayindicate hypovolemia, undetected fractures, cardiac
tamponade, or aortic aneurysm. Remember, lowerextremity PMS assessment can be carried out with thelower extremity quick initial assessment.
Assessment of Cervical Spine The paramedicwill want to apply a cervical collar (C-collar) at this point.Prior to application, assessment of the posterior neckmust be performed to determine if there is tenderness,deformity, edema, muscle spasms, palpable vertebralstep-offs or gaps, impaled objects, or soft tissue injury.One should assume a cervical spine fracture in any
Assessment of the Trauma Patient 103
FIGURE 6-14 Decorticate posturing.
FIGURE 6-15 Decerebrate posturing.
-
8/10/2019 Assessment of the Trauma Patient.pdf
14/25
patient with an injury above the clavicle as 10% of allpatients with head injuries will have cervical spine frac-ture.9 If the paramedic suspects chest trauma, a quick
reevaluation of the anterior neck for JVD and trachealdeviation should be performed before applying theC-collar. Application of the C-collar can be delayed ifcontinued reevaluation of the anterior neck is warranted.
For more complete stabilization of the head and neck theC-collar should always be applied prior to movement ofthe patient onto the LSB. Once the cervical collar has
been applied, the paramedic manually stabilizing thehead and neck must continue this stabilization until thepatient is fully strapped to an LSB with head-immobiliz-ing devices in place.
104 Chapter 6
FIGURE 6-16 Assessment for paralysis or paresis by having the patient squeeze two to three of your fingers.
FIGURE 6-17 Assessment for lower extremity paralysis or
paresis by having the patient push, then pull back on your
hands.
FIGURE 6-18 A positive Babinski; the big toe turns upward
when a blunt stimulus is applied to the sole of the foot.
-
8/10/2019 Assessment of the Trauma Patient.pdf
15/25
Glasgow Coma Score The paramedic shouldobtain a Glasgow Coma Score (GCS) on all traumapatients. This scale provides a numerical measurebased on an assessment of the patients eye openingand verbal and motor responses. If the score is lessthan 9, this implies severe neurological insult, which
requires airway support with hyperventilation andrapid transport. Do not stop the evaluation process toscore the patient; instead, obtain baseline assessmentdata and record these data as soon as possible, usuallyafter the patient is in transit. The GCS is usually usedin conjunction with the revised trauma score, whichmeasures on the severity of trauma. For a detailed dis-cussion of these trauma-scoring systems, refer toChapter 7. Figure 6-19 presents an algorithm forchecking disability.
Expose, Examine, and Evaluate
The last step in the expanded initial assessmentinvolves a quick assessment of all systems not previ-ously exposed. It is important to expose the patientwhen assessing each system for severe soft tissue injury,open and closed fractures, and undetected hemor-rhage, especially when the patient is wearing bulkyclothing. It is very important to keep in mind that apatient experiencing anaerobic metabolism becomeshypothermic quickly. Preserve body heat by coveringthe patient once body parts are exposed and examinedor expose only what is necessary, especially if the out-side temperature is cold. If the patient is not fullyexposed prior to movement, complete exposure andexamination must take place once in the EMS unit.
Usually this assessment involves the chest, if notpreviously evaluated, abdomen, flanks, pelvis, lowerextremities, and back. All injuries should be locatedprior to PASG application and, hopefully, prior topatient movement since movement can aggravate exist-ing injuries (e.g., pelvic, femur, and lower leg frac-
tures). Based on assessment findings, conventionalmovement strategies may have to be modified toaccommodate the type of injury detected (e.g., utilizinga scoop stretcher instead of the log roll to place apatient with an unstable pelvic fracture onto an LSB).
Chest and Thorax Evaluation If the para-medic has not exposed and examined the chest duringthe breathing assessment or if there is reason to quicklyreevaluate the chest, this quick evaluation should beperformed at this time. As the chest is exposed, lookfor signs of injury such as hueing, ecchymosis, defor-mity, impalements, asymmetrical movement, soft tissue
injuries, and intercostal retractions. Quickly feel forsymmetrical expansion and movement of the chest wall(see Figure 6-20), paradoxical movement, crepitus, andinstability. Finally, listen for bilateral breath sounds andreevaluate endotracheal tube placement if the patienthas already been intubated. If this assessment has beenperformed as part of the breathing assessment, theevaluator can proceed on to the abdominal evaluation.
Abdominal Evaluation Rapidly expose theabdominal area and look for evidence of internal hem-orrhage in the form of abrasions, hueing, ecchymosis,edema, swelling, lacerations, penetrating wounds, andeviscerations. The abdominal area superior and inferior
Assessment of the Trauma Patient 105
Algorithm Assessment Actions
Assessdisability
AVPU
Pupils
All extremities
Pulse/motor/sensation
Examine posterior neck
Apply cervical collar
Unequalhyperventilate?
Spinal injurySolu Medrol?
Load and go?
FIGURE 6-19 Disability algorithm.
-
8/10/2019 Assessment of the Trauma Patient.pdf
16/25
to the umbilicus should be carefully evaluated for signsof contusion, often initially showing as a hued areaabout 4 cm wide lying transversely across the abdomen.This is indicative of an incorrectly worn seat belt andmay result in hollow viscus injury in the abdomen or alumbar spine fracture.2
Assessment includes palpation of all four quad-rants of the abdomen. Observe any painful response orguarding reaction. Feel for rigidity, spasms, edema,
local warmth, coolness, or masses. If a painful responseis elicited, such as voluntary or involuntary guarding,do not continue to palpate that area because furtherinjury can occur to the patient. The paramedic shouldnot be concerned with auscultating the abdomen forbowel sounds since this is not a reliable or easily per-formed prehospital evaluation. During the abdominalexamination remember to quickly feel laterally aroundthe patientss flank area to check for deformity, edema,impalements, or undetected hemorrhage that may bepooling in the curvature of the lumbar-sacral area.
Remember that unexplained tachycardia may be thefirst indicator of intra-abdominal hemorrhage.
Management priorities include consideration ofPASG application, especially if intra-abdominal hemor-rhage is suspected. This treatment may help tampon-ade significant hemorrhage long enough for the patient
to be received into surgery. Initiation of 100% oxygenshould occur immediately if not already initiated. Twolarge-bore IVs should be established once the patient isen route, unless an extended extrication time is antici-pated, which may warrant initiation of IV therapy priorto loading the patient. It is important to keep in mindthat this patient needs definitive surgical treatment assoon as possible, and time spent trying to initiate IVsprior to loading the patient for transport may unneces-sarily delay this definitive treatment.
Pelvic Evaluation Pelvic fracture is most com-monly caused by motor vehicle trauma, crush injury, or
a fall. Internal hemorrhage is the major cause of deathin patients with pelvic fractures. Thirty percent of thetotal blood volume may be lost into the surroundingsoft tissue of the pelvic cavity and retroperitoneally.1
Initial scene evaluation, MOI, and patient position canoften provide early clues that there might be an under-lying pelvic fracture or dislocation present, such aswhen the patients knees have impacted the vehiclesdashboard.1
The paramedic may notice, with a patient lyingon the ground, lateral or medial rotation of one leg sug-gestive of hip dislocation. Once the patient is exposed,the paramedic may observe ecchymosis, swelling, ordeformity. The patient may complain of pain in thatarea. Palpation of the pelvic region begins with com-pression of the iliac wings laterally and inwardly. Ifthere is no crepitus heard or felt and the pelvis feelsstable, exert gentle downward pressure on the iliaccrests, again noting any crepitus, instability, or painfulresponse from the patient. If this assessment isnegative, then place gentle downward pressure on thepubis, feeling for instability on crepitus (see Figure 6-21). If evidence suggestive of pelvic fracture is present,do not palpate any further. Movement of the patientonto an LSB can often produce further injury, and
therefore, the patient may need to be moved onto theLSB by use of a scoop stretcher. Patients with anunstable pelvis should not be log rolled except when analternative method would result in a life-threateningdelay. The paramedic must assume that any patientwith an unstable pelvis has a high potential for intra-abdominal or retroperitoneal hemorrhage. Therefore,the LSB should already have PASG in place for imme-diate stabilization of the fracture as well as control ofinternal hemorrhage (see Figure 6-22). Spinal immobi-lization must be provided because an unstable pelvis
106 Chapter 6
FIGURE 6-20 Assessment for expansion and movement of
the chest wall.
-
8/10/2019 Assessment of the Trauma Patient.pdf
17/25
often presents with associated spinal injuries, especiallyto the lumbar and lower thoracic spine.
Lower Extremity Evaluation Evaluation of thelower extremities begins with the initial assessment ofthe MOI. Any patient who has been involved in a motor
vehicle crash (MVC) or fall may have sustained hip,femur, knee, or lower leg injury, which must bedetected prior to movement and prior to application ofthe PASG. Hands-on assessment begins with palpationof the hip area to determine if there is an anterior orposterior hip dislocation. Dislocations frequently occurin MVCs, especially when the knees hit the dashboard,resulting in the femur being forced back into the hipjoint. This may result in disruption of the blood supplyto the femoral head and/or sciatic nerve damage. Basicassessment includes looking for hip flexion, adductionand internal rotation, shortening of the leg, and palpat-ing for a bony prominence posteriorly. Noticeable
prominence in the inguinal area is indicative of an ante-rior hip dislocation. The patient is often positioned withthe leg and foot laterally rotated (see Figure 6-23). If
the head of the femur has dislocated posteriorly, theparamedic may palpate a bony prominence in the but-tocks area and the patients leg may be rotated medially.This injury is an orthopedic emergency because theblood supply to the femur may be obstructed, leading toavascular necrosis of the femoral head.1 The patientmay have his or her leg flexed in order to relieve the
pressure and pain. The paramedic must assess distalpulse, motor, and sensation with this injury by checkingthe dorsalis pedus pulse and having the patient dorsiflexand plantar flex the foot if conscious. In an unrespon-sive patient, provide a painful stimuli with a bluntobject to the sole of the foot to elicit a reflex response.This type of injury does not take precedence over air-way, breathing, or circulatory problems. It may be nec-essary to stabilize the hip in the position found, but witha multisystem trauma patient requiring rapid trans-portation this is not always possible.
Assessment of the Trauma Patient 107
FIGURE 6-21 Assessment for pelvic injury by compression
of the iliac wings.
FIGURE 6-22 Utilization of a scoop stretcher with an unsta-ble pelvic fracture to place the patient onto an LSB. The
PASG should be placed and secured on the LSB prior to
placement of the patient on the board.
-
8/10/2019 Assessment of the Trauma Patient.pdf
18/25
Femur fractures can be life threatening and there-fore must be detected during the initial assessment.Assessment begins with exposure of the area. Once thearea is exposed, the paramedic looks for hueing orecchymosis, shortening of the leg, deformity, andswelling. Palpation should be gently applied, and ifcrepitus or shifting of the bone is felt, measures to stabi-lize the extremity should be initiated. In the multisystemtrauma patient, this can be accomplished by applicationof PASG for femoral stabilization. Prior to application ofthe PASG, assessment of distal PMS for neurovascular
impairment must be performed. If the paramedic electsto utilize a traction splint for stabilization along withapplication of PASG, the traction splint must be placedover the PASG after inflation. During inflation of thePASG, traction should be applied to the fractured femurto prevent spiraling or twisting of the femur.
The knee must be quickly palpated for dislocationor fracture. A dislocation can be an orthopedic emer-gency, especially if the popliteal artery or peronealnerve is damaged. Assessment findings include thepresence of ecchymosis, swelling, deformity, crepituswith palpation, and decreased or absent distal PMS inthat extremity. Again, this injury must not take prece-
dence over ABCD problems, but the paramedic mustdetect and report this injury to the receiving facility.Direct and indirect forces produce fractures to
the tibial and fibular area and the paramedic mustagain relate this injury with the MOI. Any direct blowis likely to result in open fractures requiring hemor-rhage control. Closed fractures can develop into com-partment syndrome, and the paramedic must quicklyassess for the 5 Ps of ischemia: pain, pallor, paresthe-sia, paresis, and puffiness.1 See Chapter 16 for furtherdiscussion.
Often, especially in multisystem trauma patients,the paramedic will take short cuts and fail to exposeand evaluate the lower extremities. Because theseinjuries often produce orthopedic emergencies, theymust be detected. During this quick examination it isvery important to assess for and detect deformity,
shortening, swelling, ecchymosis, tenderness, grating,crepitus, and exposed bone ends prior to placing thepatient on an LSB. It is also important to note skintemperature, presence or absence of distal pulses,CRT, and motor and sensory function and to comparethe extremity findings. Remember, it may not be possi-ble to perform a complete focused assessment en routeto the medical facility. These injuries may not betreated for several hours, or even days, once the patienthas arrived at the receiving facility, but the paramedicmust report his or her findings to the receiving nurseor physician. If the PASG is applied, the paramedic willnot be able to assess the lower extremities after appli-
cation; therefore, it is essential that assessment bequickly performed during the PASG survey segmentand prior to movement of the patient. Failure to assessthe lower extremities could result in further injury dur-ing movement of the patient onto the LSB. Alternativepackaging techniques may be necessary to prevent fur-ther patient compromise. Figure 6-24 provides an algo-rithm for exposure assessment.
Remember: If you have not assessed distal PMS inthe lower extremities, quickly perform this evaluationprior to movement of the patient. Movement of thepatient could produce further injury and result indecreased or absent PMS once the movement is com-
pleted. The paramedic should be able to report tomedical control any changes noted in neurological andcirculatory function after patient movement.
RAPID PATIENT PACKAGING ANDTRANSPORT
The paramedic is now ready to package the patient fortransport. This involves placement of the patient ontoan LSB with complete cervical immobilization. If yoursystem uses PASG, this device should already be placed
on the LSB. Movement of a supine patient will requirelog rolling the patient onto the side and lowering thepatient onto the board, unless there exists an unstablepelvic fracture, which will require a scoop stretcher forplacement onto the board. Refer to Chapter 19, for acomplete description of immobilizing devices and tech-niques. As the patient is log rolled, assessment of theentire back must be performed to detect any injuries.The paramedic should palpate from the occipital areadown to the lower leg area. At this time removal ofclothing should be completed if it has not already been
108 Chapter 6
FIGURE 6-23 Foot and leg rotation indicative of a hip dislo-
cation. Courtesy of Deborah Funk, MD. Albany Medical
Center, Albany, NY.
-
8/10/2019 Assessment of the Trauma Patient.pdf
19/25
removed. If the patient is extricated from a sitting posi-tion, the back should be quickly assessed prior to low-
ering the patient onto the LSB. Paramedics oftenforget this important assessment step and miss injuriesthat may be life threatening. Steps involved in rapidextrication techniques are found in Chapter 19.
With multisystem trauma patients time shouldnot be spent splinting/stabilizing fractures or dressingand bandaging soft tissue injuries. The initial goal is tostabilize only what is necessary to prevent furtherinjury. Once the patient has been placed on the LSB,treatment team members must secure the patient tothe board and secure the PASG around the patient.The patients body is secured to the board first and thehead is secured last. During this time the lead para-medic should reassess the patients LOC, airway,breathing, circulatory, and neurological status. As soonas the patient is fully secured onto the backboard, he orshe is quickly transferred into the ambulance or heli-copter for immediate transportation.
Paramedics must remember they are workingagainst the clock with a patient who has sustained criti-cal injuries. Therefore, transport to the most appropri-ate definitive care facility is imperative. This mayinvolve an actual increase in overall initial transporttime, but the patient will be received by a facility with atrauma and surgical team.
ON-SCENE RESUSCITATION VERSUS EN
ROUTE RESUSCITATION
Critical trauma patients rapidly decompensate and diedue to hypoxemia and shock. Therefore, prioritizepatients using the CUPS classification system(Table 6-5). Patients who fall into the urgent categoryhave injuries or conditions that, regardless of interven-tions provided in the field, continue to be life threaten-
ing and require definitive care such as blood replace-ment or surgical intervention.7 The elapsed time
between onset and definitive care is a paramount factoraffecting these patients morbidity and survival.7
Nonurgent patients have no life-threatening injuries orconditions, and therefore, further examination can bedone prior to packaging and transport.7
The paramedics initial goal is to provide early air-way management, oxygenation, and ventilatory supportas soon as the problem is identified. A suction unitshould always be part of the initial equipment taken tothe patients side in case there are immediate and ongo-ing problems with secretions, debris, vomit, or blood inthe airway. Early resuscitation consists of applying 100%oxygen by a nonrebreathing mask, BVM, or early intu-bation if the patients condition warrants field intuba-tion. If the paramedic detects a tension pneumothorax,immediate pleural decompression should be performedand intubation should follow as soon as possible. Theparamedic must reevaluate the patients airway andbreathing status frequently during the initial assessmentand patient packaging, constantly assessing for compli-ance problems if the patient is being assist ventilatedwith a BVM. Compliance problems may indicate theneed to decompress the pleura, reposition the patientsairway, or perform immediate oral or nasal intubation.If the patients airway and breathing can be managed
effectively with assisted ventilation until he or she isloaded into the ambulance or helicopter, intubation canbe delayed. It is often easier to intubate once thepatient is in a more controlled environment and in abetter position for visualization of anatomical land-marks. If the patient does not require immediate intu-bation to secure the airway but requires assistedventilation or hyperventilation, do not forget to use anoropharyngeal or nasopharyngeal airway. Use of theseadjunctive devices is often forgotten, resulting in aninadequately opened and maintained airway.
Assessment of the Trauma Patient 109
Algorithm Assessment Actions
Expose
Abdominal quadrants
Flanks
Pelvis
Back
Bruising, tenderness,rigidityIV
IV fluids
Spinal injurySolu-Medrol?
LSB
Load and go?
PASG survey/PASG
FIGURE 6-24 Expose, examine, and evaluate algorithm.
-
8/10/2019 Assessment of the Trauma Patient.pdf
20/25
Severe exsanguinating hemorrhage should be
immediately controlled using basic techniques of directpressure, pressure dressings, or pressure points. Volumeresuscitation may be delayed until the patient is en routeto the hospital unless a prolonged disentanglement is inprogress. When there are adequate personnel on scene,someone can prepare two large-bore, 1416-gauge IVsof normal saline or lactated Ringers in the ambulance orhelicopter. As soon as the patient is loaded, resuscitationcan be initiated. The IV fluid should be warmed, if pos-sible, to prevent hypothermia. It is no longer acceptableto delay transport to initiate fluid resuscitation in thefield, for the critical trauma patient generally requiresblood transfusion to restore the cardiovascular system
and maintain adequate perfusion status.The use of PASG should be considered when the
patients systolic blood pressure is 6080 mm Hg, espe-cially if there are abdominal or pelvic injuries.2 Specificcriteria for inflation will be based on local medical pro-tocols. The PASG is an excellent immobilizing devicefor stabilization of femur and pelvic fractures. Refer toChapters 15 and 21 for further discussion regardinguse and application of this device with these injuries.
As soon as the patient is loaded for transport,reevaluation of the ABCs begins, intubation is per-formed if the airway is unstable, two large-bore IVs areinitiated preferably with trauma tubing, quantitativevital signs are obtained, and the patient is completelystripped of all clothing and covered to preventhypothermia. All multisystem trauma patients areplaced on a cardiac monitor as soon as possible to mon-itor for dysrhythmias that often accompany head andthoracic trauma. Some EMS systems require a nasogas-tric (NG) tube to be placed to reduce the incidence ofaspiration. Nasogastric tube placement is contraindi-cated in patients with cribriform fractures and cere-brospinal fluid (CSF) drainage.9
FOCUSED ASSESSMENT
Once definitive treatment has been provided for all ini-
tial problems, the paramedic can begin to perform adetailed physical examination. The purpose of thefocused assessment is to detect other potentially life-threatening injuries missed in the initial assessment, toobtain a more detailed analysis of existing injuries, andto detect other non-life-threatening minor injuries.Often this survey is performed en route to the emer-gency department or sometimes it is not completed atall while all energies and time are spent managing life-threatening injuries.
When the focused assessment is performed, theparamedic obtains quantitative assessment information
and a patient history and performs a complete physicalexamination. The focused assessment consists of thecriteria found in Table 6-6. Begin this survey by obtain-ing, if possible, information regarding the patients his-tory, using the acronym AMPLE (Table 6-7). Duringthe head-to-toe survey, look for medic alert necklacesor bracelets that could provide some of the AMPLEinformation. Quantitative vital signs, if not obtainedsoon after the patient was loaded for transport, shouldbe performed and recorded now, and every 35 min-utes throughout transport.
110 Chapter 6
Category Action Examples of Patient Condition
CCritical Airway and spinal control, treat only Cardiac or respiratory arrest
immediate threats to life, then rapidtransport
UUnstable Same as above Respiratory distress and/or shock
PPotentially unstable Rapid assessment, treatment of potential Marginal vital signs
threats to life, airway and spinal control,
then expedient transport
SStable Continue with focused assessment Normal vital signs, no apparent distress,
no major mechanism of injury
Table 6-5
Classification System for Determining Patient Priority for Transport Decisions
Visit the British Trauma Society Web site and
review the material on the organization of the
trauma team at http://w ww.trauma .org/resus/
traumateam.html. How is this system of trauma
resuscitation similar to that of the field resuscita-
tion team? How does it differ?
INTERNETACTIVITIES
-
8/10/2019 Assessment of the Trauma Patient.pdf
21/25
Using the look, listen, and feel methods of assess-ment, perform the focused assessment, region by
region, as found in Table 6-8. If PASG has beenapplied, the survey will examine down to the diaphragmlevel. If PASG has not been applied, the survey willinclude the entire anterior and lateral body. Look forsigns of ecchymosis, deformity, hemorrhage, masses,swelling, abnormal indentations, or abnormal skin colorthat would indicate injury or underlying medical prob-lems. Listen for abnormal breath sounds or abnormalheart sounds (e.g., muffled heart tones). Feel all areasof the body for the presence of pulses in all extremities;for skin temperature; and for abnormal findings such asthe presence of abnormal pulsations, crepitus, abnormal
movement of long bones or joints, deformity, subcuta-neous emphysema, depressions in the skull, abdominalrigidity, or impaled fragments of glass or metal.Reassessment of the patients previous ABCD vitals willbe performed during this assessment phase. Reassessthe patients respiratory status, ECG, vital signs, neuro-logical status, skin color, and temperature at least every35 minutes while en route. It is equally important toclosely monitor fluid replacement by frequentlyreassessing the patients pulse strength, LOC, and lungsounds.
RADIO AND REPORTCOMMUNICATION
As soon as the paramedic can establish radio communi-cation with the emergency department, vital patientinformation should be communicated. It will be veryimportant to communicate specific information regard-ing the patients MOI and the kinematics involved, ven-tilatory, circulatory, and neurological status, treatmentand response to treatment, and estimated time ofarrival (ETA). Be as short and concise as possible. Tryto paint a realistic picture of the patients overall status.This will allow emergency department personnel timeto prepare for the patients arrival and alert the surgicalteam. Upon arrival at the medical facility, verbally
Assessment of the Trauma Patient 111
See Inspect-look-observe for contusions,
abrasions, lacerations, ecchymosis, edema,
hemorrhage, deformity (angulation shortening,abnormal position)
Listen Auscultate for breath sounds, heart sounds
Feel Palpate for tenderness, deformities, crepitus,
masses, edema, subcutaneous air, instability,
rigidity
Source:Adapted from The Paramedic Manual, by J.
Greenwald, 1988, Englewood, CO: Morton Publishing Co.
Table 6-6
Criteria for Performing a Focused Assessment
AAllergies
MMedications
PPast and present pertinent history
LLast meal
EEvents leading up to the incident
Table 6-7
Use of the Acronym AMPLE in Gathering
Pertinent Patient Information
Region Assessment
Head Soft tissue injuries,* raccoons eyes, Battles
sign, cerebrospinal fluid or blood from noseand/or ears, skull deformity, eye orbits,
stability of nasal and facial bones, foreign
bodies or blood in the oral cavity, stability
of mandible, pupillary response,
extraocular movements
Neck Soft tissue injuries,* jugular venous
distention, tracheal deviation, carotid pulse,
subcutaneous emphysema, cervical spine
deformity or tenderness
Chest Soft tissue injuries,* stability of ribs, sternum,
and clavicles, chest symmetry and
expansion, bilateral breath sounds, openpneumothorax, subcutaneous
emphysema, flail segments, heart sounds,
electrocardiogram
Abdomen Soft tissue injuries,* distention, tenderness,
and pelvis guarding, pulsatile masses, rigidity, bowel
sounds, rebound tenderness, pelvic stability,
priapism
Extremities Soft tissue injuries,* bony instability, pulses,
motor, sensation, range of motion,
tenderness, crepitus, deformity, malrotation,
shortening, lengthening, open fractures
Back Soft tissue injuries,* vertebral deformity ortenderness, stability of ribs, stability of
sacrum, buttocks
*Soft tissue injuries include lacerations, contusions, abrasions,
incisions, penetrating injuries, burns, edema, hematoma,
hueing, and amputations.
Table 6-8
Algorithm for Performing Focused Assessment
-
8/10/2019 Assessment of the Trauma Patient.pdf
22/25
transfer the patient to the receiving physician or nurse,providing a detailed account of the patients injuriesand treatment.
Finally, provide a written ambulance call reportto the receiving hospital. This report is importantbecause it gives the hospital staff a thorough under-
standing of the events surrounding the incident and aprogressive account of the patients condition andresponse (or lack of response) to treatment initiated onscene and en route to the hospital.
CONCLUSION
The multisystem trauma patient must be rapidly, sys-tematically, and thoroughly evaluated. Paramedicsmust develop an organized and consistent approach tothe trauma patient that outlines priorities of care (referto Figure 6-25 for a complete patient assessment algo-rithm). These priorities are found during the initial sur-vey, which evaluates the MOI and kinematics of theinjuries, airway and C-spine control, breathing, and cir-culatory and neurological status and includes com-pletely exposing the patient. Definitive field treatmentrevolves around rapid recognition and treatment ofhypoxemia and shock resulting from inadequate air-ways, compromised ventilatory and circulatory status,and inadequate cerebral perfusion.
The paramedic must be able to systematicallyevaluate and constantly reevaluate the patient every35 minutes, providing immediate definitive treatmentfor airway, breathing, and circulatory problems as they
are encountered. Needlessly delaying transportation ofthe trauma patient may increase the patients morbidityand severely decrease his or her chances for survival.Finally, initiate transportation to the most appropriatemedical facility with treatment teams trained to man-age the critically injured trauma patient.
REVIEW QUESTIONS
1. Which of the following represents a load and gopatient?
a. A patient with an isolated radius/ulna fractureb. A patient with a large flail segmentc. A patient with venous bleeding that is con-
trolled by direct pressured. A patient with a dislocated shoulder
2. It is acceptable to bypass the local hospital in
favor of transporting a critically injured patientdirectly to a trauma center.a. Trueb. False
3. List several questions that should be incorporatedinto the scene size up.
4. List several questions that should be incorporatedinto the global assessment upon approach of thescene.
5. Overall, what percentage of patients are trulyload and go?a. 5
b. 10c. 15d. 20
6. Compare and contrast the golden hour and plat-inum ten minutes.
7. List five mechanisms of injury that suggest majortrauma.
8. List five physical findings that suggest majortrauma.
9. Which oxygen delivery device is most appropriatefor a patient with a C-4 spinal injury?a. Nasal cannula
b. Nonrebreather maskc. BVMd. Simple mask
10. Bulging neck veins may indicate which of the fol-lowing pathologies?i. Simple pneumothoraxii. Tension pneumothoraxiii.Cardiac tamponadeiv. Myocardial contusion
a. i and iib. ii and iiic. iii and iv
d. ii and iv11. If a radial pulse is palpable, a crude estimate of
systolic blood pressure is:a. At least 50 mm Hgb. At least 60 mm Hgc. At least 70 mm Hgd. At least 80 mm Hg
12. The most likely source of unexplained internalhemorrhage is the:a. Abdomenb. Chest
112 Chapter 6
Review the prehospital trauma resuscitation
protocols of the North Central Texas Trauma
Regional Advisory Council at http://www.dfwhc.
org/ncttrac/protocols.htm. To review the protocols,you will need Acrobat Reader, which can be down-
loaded free of charge from http://www.
adobe.com/.
INTERNET ACTIVITIES
-
8/10/2019 Assessment of the Trauma Patient.pdf
23/25
Assessment of the Trauma Patient 113
Scene
Airway
Breathing
Circulation
Disability
Expose
Status
INITIA
L
ASSES
SMENT
Algorithm Assessment Actions
Scenesurvey
Establish LOCControl C-spine
Open airway
Airwaycompromise?
Resuscitate
Resuscitate
Resuscitate
Load and go
difficulty?
Assess breathingExpose chest
Assess anterior neckAssess bilateral breath sounds(BBS)
Breathing
Assesscirculation
Hypoperfusion?
Assessdisability
Expose
Determinepatientstatus
Critical?
Secondarysurvey
Hazards/body fluids/PPENumber of patientsMechanism of injuryExtrication
Remove hazards or patient/PPEMutual aidPredict injuriesNotify rescue
Alert/responsiveC-spine MOIAirway obstruction
Approach from frontManual stabilizationModified jaw thrust PRNLoad and go?
ApneaBradypneaHypopneaTachypneaDyspnea
BVM with 100% OAssisted with BVM and 100% OAssisted with BVM and 100% ONRB mask with 100% ONRB mask/BVM with 100% O
Carotid/radial pulseRelative rate/qualitySkin temperature/color/capillary refillExsanguinating hemorrhagePASG survey if internalhemorrhage is suspected
Quantitative vital signs
Cardiopulmonary resuscitationPRN PASG2 large-bore IVs en routeFluid trial PRN
Rapid infusion PRN
Load and go?
BVM/ETI/clear obstruction/cricothyroidotomyModified jaw thrustIntubateSuction/endotracheal intubationLoad and go?
Silent
SnoringStridorGurgling
AVPUPupilsPulse/motor/sensationExamine posterior neck
Apply C-collarUnequalhyperventilateSpinal injurySolu MedrolLoad and go?
Abdominal quadrantsFlanksPelvisBack
Bruising/tenderness/rigidityIVPASA/survey/PASA as neededIV fluidsSpinal injurySoluMedrolLSBLoad and go?
CUPS
CriticalUnstablePotentially unstableStable
Transport immediatelyTransport immediatelyTransport immediatelyContinue with secondary surveyGo to secondary survey
Relative rate/qualityExpose chestChest symmetry/BBSNeck veinsTracheal deviation
O nonrebreathing mask/BVM
Needle decompressionLoad and go?
2
2
2
2
2
2
FIGURE 6-25 Patient assessment algorithm.
-
8/10/2019 Assessment of the Trauma Patient.pdf
24/25
c. Retroperitoneal spaced. Epidural space
13. Normal capillary refill time is less than or equalto:a. 1 secb. 2 sec
c. 3 secd. 4 sec
14. Unequal pupils may indicate:a. Head traumab. Cerebrovascular accidentc. Eye traumad. All of the above
15. Upon applying lateral and inward pressure on theiliac wings, crepitus and instability are noted. Theparamedic should next:a. Palpate the iliac wings in a downward and pos-
terior direction
b. Palpate the symphysis pubisc. Rock the pelvis to confirm instabilityd. Recognize the pelvic fracture and discontinue
further palpation of the pelvis
16. The most immediate life threat from bilateralfemur fractures is:a. Fat embolib. Deep vein thrombusc. Hemorrhaged. Femoral nerve injury
17. Following the initial examination at the scene, thecritical patient should be packaged and transportinitiated with continued assessment conductedwhile en route to the trauma center.a. Trueb. False
18. The letter M of the pneumonic AMPLErepresents:a. past Medical historyb. last Mealc. Medicine allergiesd. Medications the patient is currently taking
19. Subcutaneous emphysema may indicate which ofthe following?a. Pneumothorax
b. Tracheal disruptionc. Bronchiole disruptiond. Any of the above
20. Quantitative vital signs must be obtained duringthe initial assessment even if it is necessary todelay airway and hemorrhage control.a. Trueb. False
CRITICAL THINKING
Correlate the etiologies of death in the trimodaldistribution of time of death (Chapter 3) with therapid trauma assessment. Why do you think theassessment sequence is ABCDE as opposed tosome other priority? How do the treatment priori-ties of the rapid trauma assessment impact eachmode of the distribution?
Think back to your last EMS response to a multi-system trauma patient. Was an organized assess-ment plan implemented? Were the on-scenetreatments properly prioritized? Based upon yourunderstanding of rapid trauma assessment, whatwould you now do differently if faced with a similarscenario? Why?
For the following scenario, describe your assess-ment plan and treatment priorities: You are called
to the scene of an MVC. A single car left the road-way at a high rate of speed and struck a tree. Thereare no skid marks on the road, and there is approxi-mately 36 inches of crush to the front of the vehi-cle. The driver is slumped over the steering wheeland appears unconscious. There is obvious defor-mity to the steering wheel and windshield. Norestraints were worn and the car was not equippedwith airbags.
REFERENCES1. Caroline NL. Emergency Care in the Streets. 5th
ed. Philadelphia, Pa: Lippincott Williams andWilkins, 1995.
2. Paturas JL, Wertz EM, McSwain NE Jr. PHTLSBasic and Advanced Prehospital Trauma and LifeSupport. 4th ed. St. Louis: Mosby-Year Book, 1999.
3. Trunkey, DD. Trauma.Sci Am. 1983; 249:28.4. Campbell , JE. Basic Trauma Life Support.
Englewood Cliffs, NJ: Prentice-Hall, 1998.5. Bledsoe BE, Porter RS, Shade BR. Paramedic
Emergency Care, 3rd ed. Englewood Cliffs, NJ:Prentice-Hall, 1997.
6. Miller RH, Wilson JK. Manual of PrehospitalEmergency Medicine. St. Louis: Mosby-Year Book,1992.
7. Butman AM, et al. Comprehensive Guide to Pre-Hospital Skills: A Skills Manual. Akron, Ohio:Emergency Training, 1995.
8. Pons P, Cason D, eds.ACEP Paramedic Field Care.St. Louis: Mosby, 1997.
114 Chapter 6
-
8/10/2019 Assessment of the Trauma Patient.pdf
25/25
9. Trauma: Review of Initial Management, InitialAssessment and Management Priorities. Internet:http://www.mc.vanderbilt.edu/surgery/backup/trauma.html, 1997.
10. Cleveland Clinic Foundation: Spine and SpinalCord Trauma, Department of General Anesthe-
siology. Internet: http://www.anes.ccf.org.8080/PILOT/NEURO/SCI.html, 1997.
11. Campbell JE. Basic Trauma Life Support, 3rd ed.Englewood Cliffs, NJ: Prentice-Hall, 1995.
12. Greenwald J. The Paramedic Manual. Englewood,Col.: Morton Publishing, 1988.
Assessment of the Trauma Patient 115