ASSESSMENT OF THE ABDOMEN Prepared by Hamdia Mohammed.
48
ASSESSMENT OF THE ABDOMEN Prepared by Hamdia Mohammed
-
date post
20-Dec-2015 -
Category
Documents
-
view
215 -
download
0
Transcript of ASSESSMENT OF THE ABDOMEN Prepared by Hamdia Mohammed.
ASSESSMENT OF THE ABDOMEN
Prepared by
Hamdia Mohammed
Learning Objectives:-At the end of this lecture each student will be
able to: Identify landmarks for the abdominal
assessment Correctly perform techniques of inspection,
auscultation, percussion and palpation Differentiate between normal & abnormal
findings.
Overview of abdominal structure.
1- Large oval cavity.
2- Extends from diaphragm to symphysis.
3- Viscera: solid and hollow.
A- Solid viscera are those organs that maintain their shape consistently ( liver, pancreas, spleen, adrenal glands, kidneys, ovaries and uterus ).
The liver is the largest solid organ in the body.
B- The hollow viscera consist of structures that change shape, depending on their contents . These include ( stomach, gallbladder, small intestine, colon , bladder ).
4- Vascular structures:
The abdominal organs are supplied with arterial blood by abdominal aorta & its major branches.
Locating abdominal structures by quadrants
Divided to four quadrants:-
1- Right upper quadrant ( RUQ )
2- Right lower quadrant ( RLQ )
3- Left upper quadrant ( LUQ )
4- Left lower quadrant ( LLQ )
Right upper quadrant
( RUQ ).- Liver
- Gallbladder
- Duodenum
- Head of pancreas
-Right kidney and adrenal
- Hepatic flexure of colon
- Part of ascending and transverse colon.
- Right ureter.
Left Upper Quadrant
(LUQ ).
- stomach
- spleen
- left lobe of liver
- body of pancrea
- left kidney and adrenal
- spleen flexure of colon
- part of transverse & descending colon
Right Lower Quadrant:
-Cecum
-Appendix
-Right ovary and tube
-Right ureter
-Right spermatic cord
Midline:-Aorta
-Uterus.
-bladder.
Left Lower Quadrant:
-Part of descending colon
-Sigmoid colon
-Left ovary and tube
-Left ureter
-Left spermatic cord
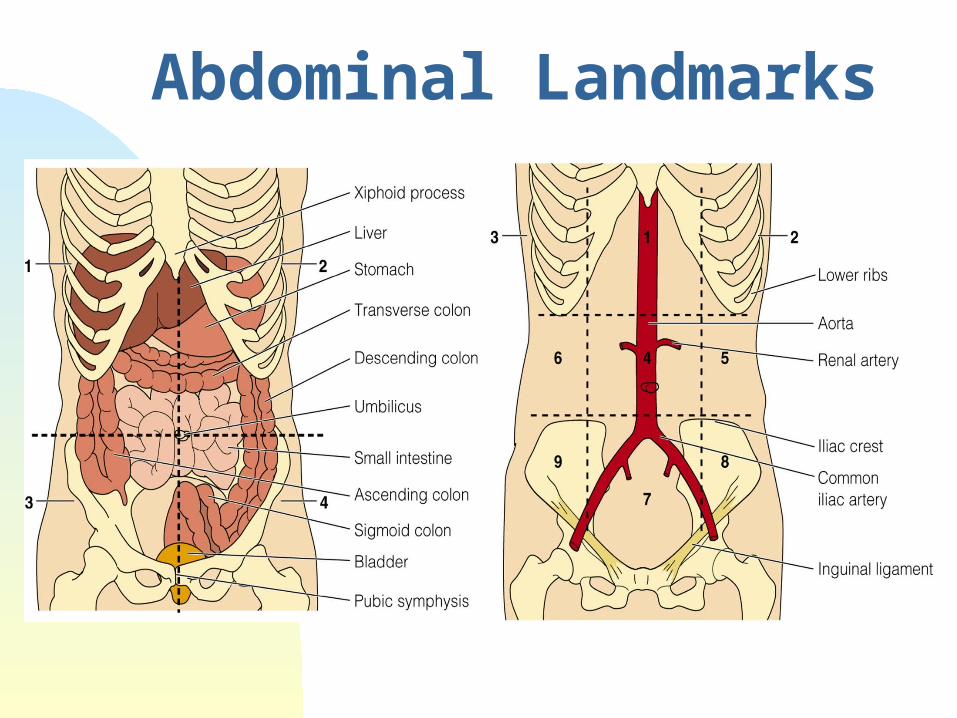
Abdominal Landmarks
Preparation for abdominal assessment
Preparing the exam room preparing the patient positioning the examiner
Health History:
Any chronic diseases that affect GIT or urinary systems? Describe.
Does he drink alcohol? How much? How often? When was last drink?
Smoke? How much and how long? Considered stopping or cutting down?
How often do you have a bowel movement? When was the last one? What are color and consistency of stool?
Nausea or vomiting for how long? Frequency? How much do vomit? What does it look like?
Contain blood? Have an odor?
Abdominal pain: How long have he had ? Where? When did he
first feel pain? What activity were he doing? Describe pain. Constant/intermittent? Had
episodes before? Did pain start suddenly?
Types of pain
1. Vesceral pain.
2. Parietal pain : as in appendicitis
3. Referred pain
Character of abdominal pain
Dull, aching( e.g cystitis ) Burning (e.g dyspepsia ) Colicky (e.g colon cancer) Sharp, knifelike (e.g renal colic ) Pressure ( urinary retention )
Assessment Techniques
1- Inspection.
2- Auscultation.
3- Percussion.
4- Palpation.

1- Inspection
skin: color, scars, veins, lesions. umbilical hernia, bleeding, inflammation. contour of the abdomen :flat ,rounded,
protuberant . symmetry enlarged organ. Masses. Peristalsis ,pulsation , distention.
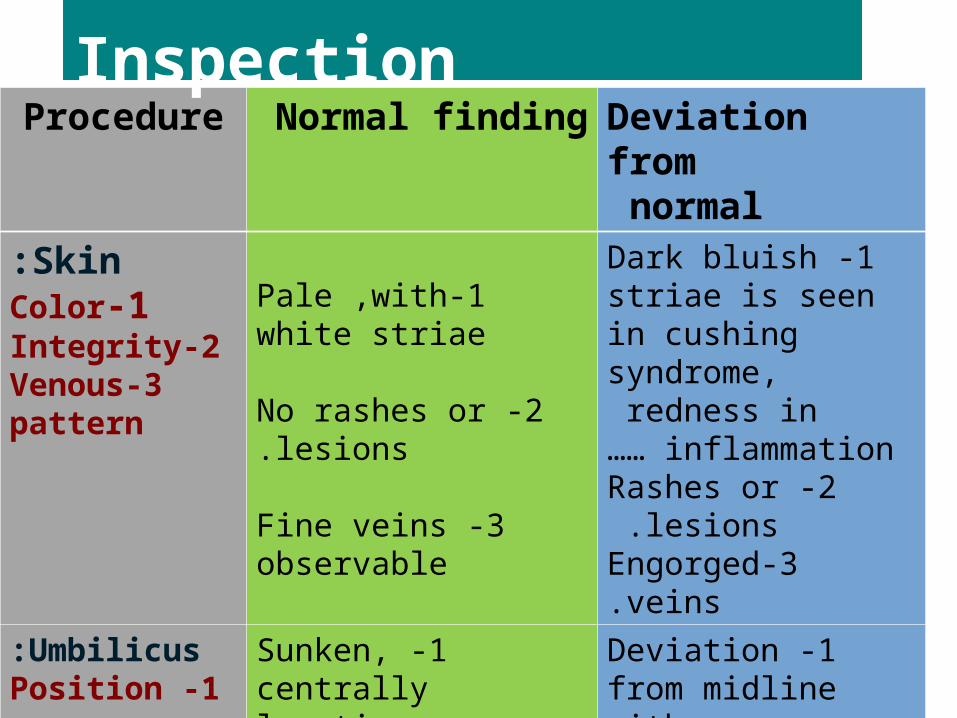
Procedure Normal finding Deviation from normal
Skin:1-Color
2-Integrity3-Venous
pattern
1-Pale ,with white striae
2 -No rashes or lesions.
3 -Fine veins observable
1 -Dark bluish striae is seen in cushing syndrome, redness in
inflammation ……2 -Rashes or lesions.
3-Engorged veins.
Umbilicus:1 -Position
2 -Color
1 -Sunken, centrally location
2 -Pinkish
1 -Deviation from midline with mass ,hernia,everted with distention..
2 -Bluish
Inspection
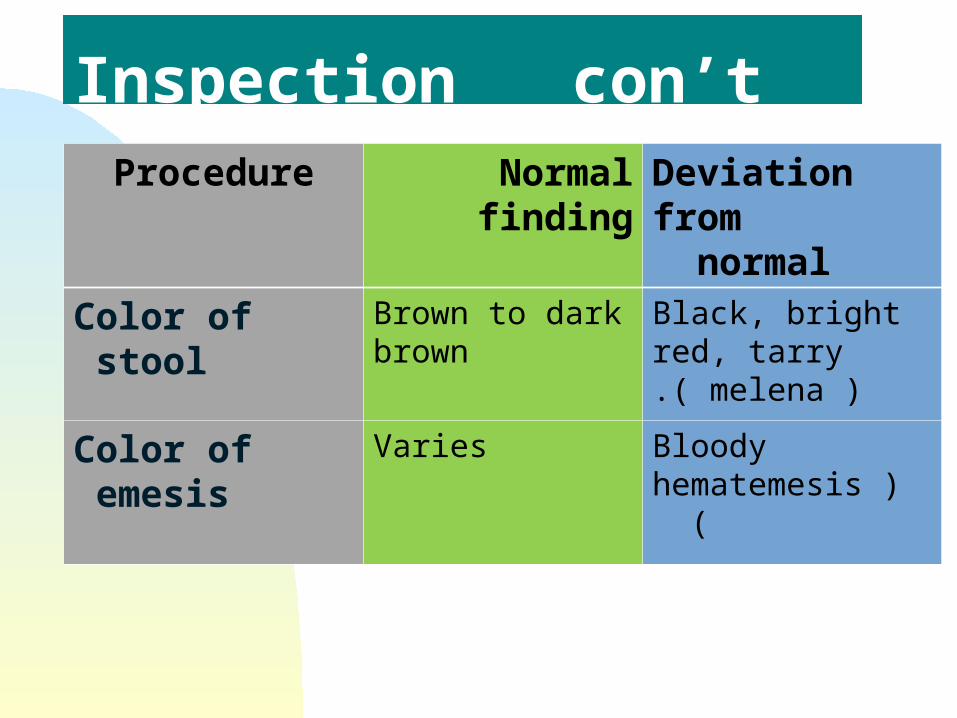
Procedure Normal finding Deviation from normal
Color of stool Brown to dark brown
Black, bright red, tarry ( melena ).
Color of emesis Varies Bloody )hematemesis (
Inspection con’t
Distention:-Definition: unusual stretching of abdominal wall
Abdominal distention can be caused by three factors:
1. Obesity – Abdomen is soft and rounded with a sunken umbilicus.
2. Ascites – Skin is shiny and glistening with an everted umbilicus. Veins are dilated and prominent (more visible in thin, malnourished skin).
3. Obstruction – There may be visible, marked peristalsis; restlessness; lying with knees flexed; grimacing facial expression; and uneven respirations.
Distention:- note position of umbilicus note portion of abdomen that is
distended reasons for distention: flat(obesity),
flatus(gas), feces, fluid, tumor , fetus(pregnancy )
2- Auscultation Auscultation performed before palpation and
percussion. Use diaphragm of stethoscope Listen to bowel sounds for up 5 minutes in each
quadrant. Normal sounds are clicks and gurgles, irregular, 5-
30 times per minute Influenced by digestion
Increased bowel sounds are due to hypermotility of peristalsis
Decreased are due to paralytic ileus or peritonitis Intestinal obstruction can present with increased
or decreased sounds
Auscultation con’t
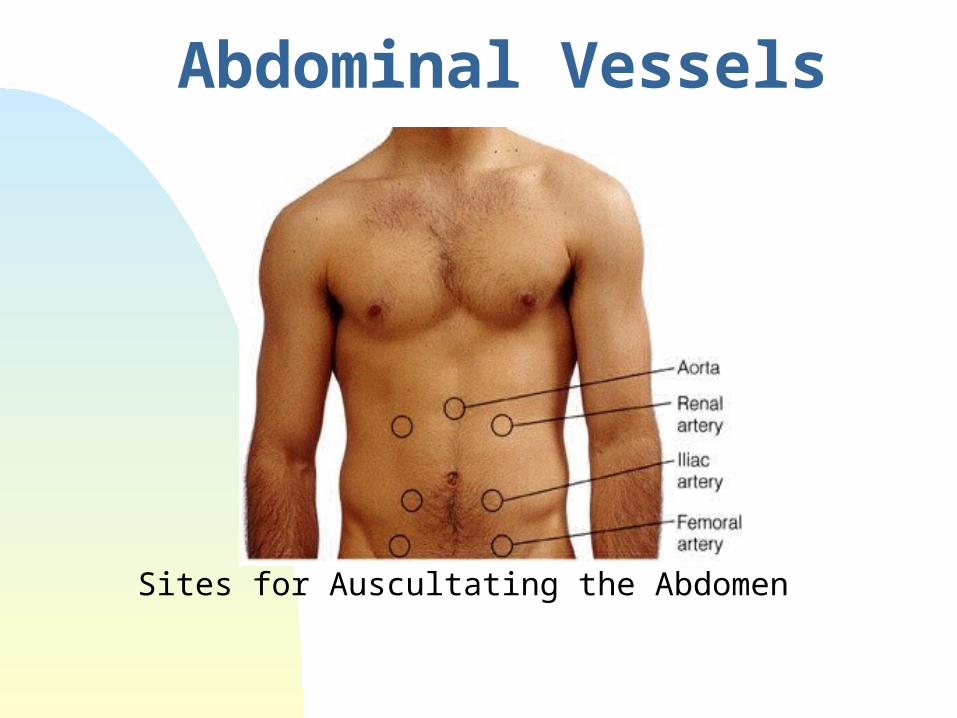
Abdominal Vessels
Sites for Auscultating the Abdomen
Additional Sounds
Bruits: Bruits are low pitched, vascular sounds,
resembling murmur Caused by partially obstructed artery– turbulence Listen in epigastrum and each upper quadrant Listen in costovertebral angle(with patient seated) Listen over aorta, iliac arteries, femoral arteries Arterial insufficiency in legs
3- Percussion Assessment technique used to assess size and
density of organs in the abdomen e.g used to measure size of liver or spleen.
In the right midclavicular line, percuss down from
lung resonance to liver dullness.
Used to identify air in stomach or in bowel.
Used to identify masses.
Used alone or in conjunction with palpation or to validate palpatory findings.
Orient to the abdomen by lightly percussing all 4 quadrants for tympany or dullness.
Percussion con’t
Tympany usually predominates due to gas in the bowel.
Dullness may be present due to feces or fluid or over organs or a solid mass.
Develop a specific percussion route and stick to it.
Percussion con’t
Percussing the spleen
Where is the spleen located?
In the curve of the diaphragm just posterior to the left midaxillary line.
When the spleen enlarges, it does so anteriorly, downward and medially. This will replace the tympany of the stomach and colon with dullness
Tricks to Assessing the Spleen Percuss in the lowest interspace in the left anterior
axillary line for tympany. Ask the patient to take a deep breath and percuss
on inspiration. The percussion note should remain tympanic. A change to dullness suggest spenomegally This is known as a positive splenic percussion sign
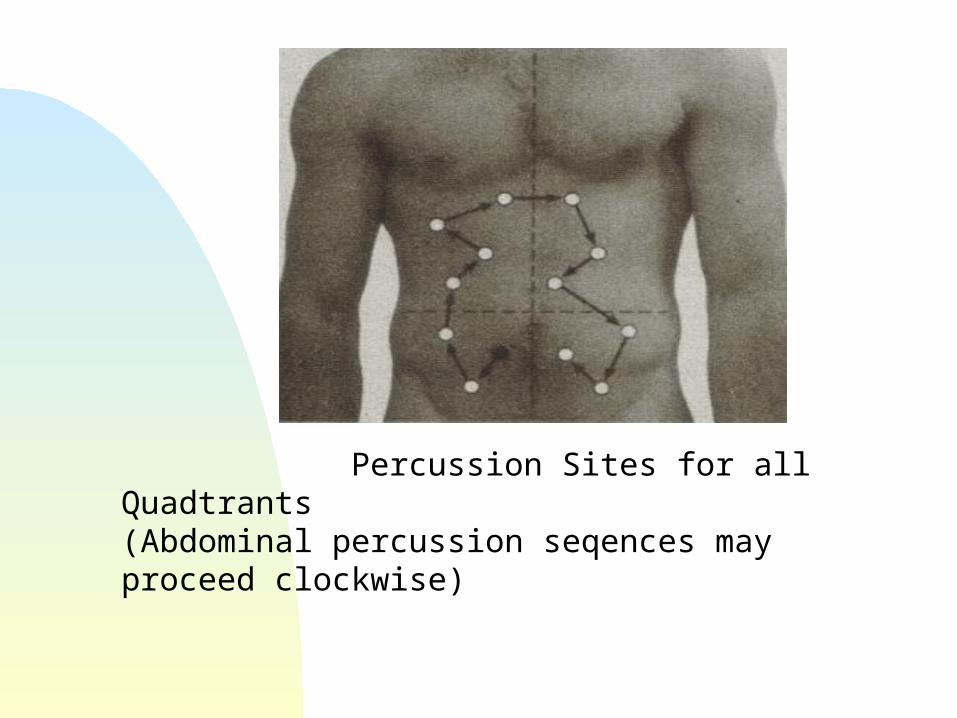
Percussion Sites for all Quadtrants(Abdominal percussion seqences may proceed clockwise)
4- Palpation
To differentiate voluntary from involuntary resistance: rectus muscle will relax with expiration.
Palpation is light or deep Deep palpation used to define and delineate
organs or abdominal masses. Use palmar surface of fingers and feel in all
four quadrants
Palpation con’t Used to assess muscle tone, tenderness, fluid,
organs. Use pads of fingertips in light dipping motions and
avoid short jabs.
Palpation of the liver
Stand on patients right side Place left hand behind patient parallel to and
supporting 11-12th ribs Patient should relax Press with left hand forward and place right hand
on abdomen with fingertips below lower edge liver dullness
Press in and up while patient takes deep breath; if palpable, liver should come down
Palpation of the spleen The spleen is usually not palpable
From patient’s right side, reach over and around under patient with left hand
Place right hand below left costal margin and press in toward spleen. Ask patient to take deep breath---will feel if palpable
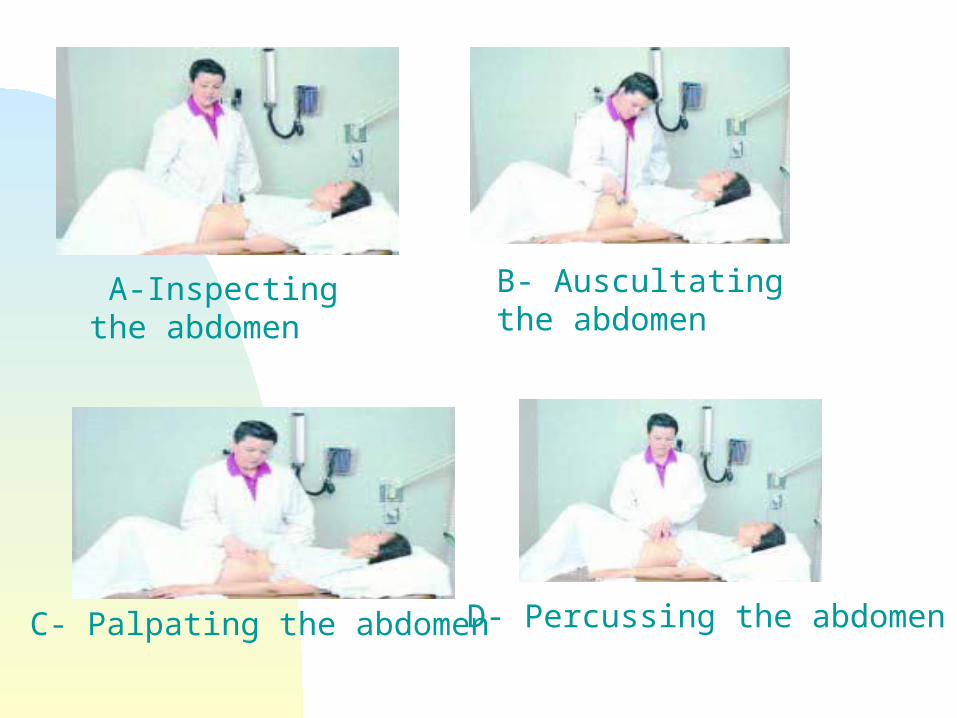
A-Inspecting the abdomen
B- Auscultating the abdomen
C- Palpating the abdomen D- Percussing the abdomen
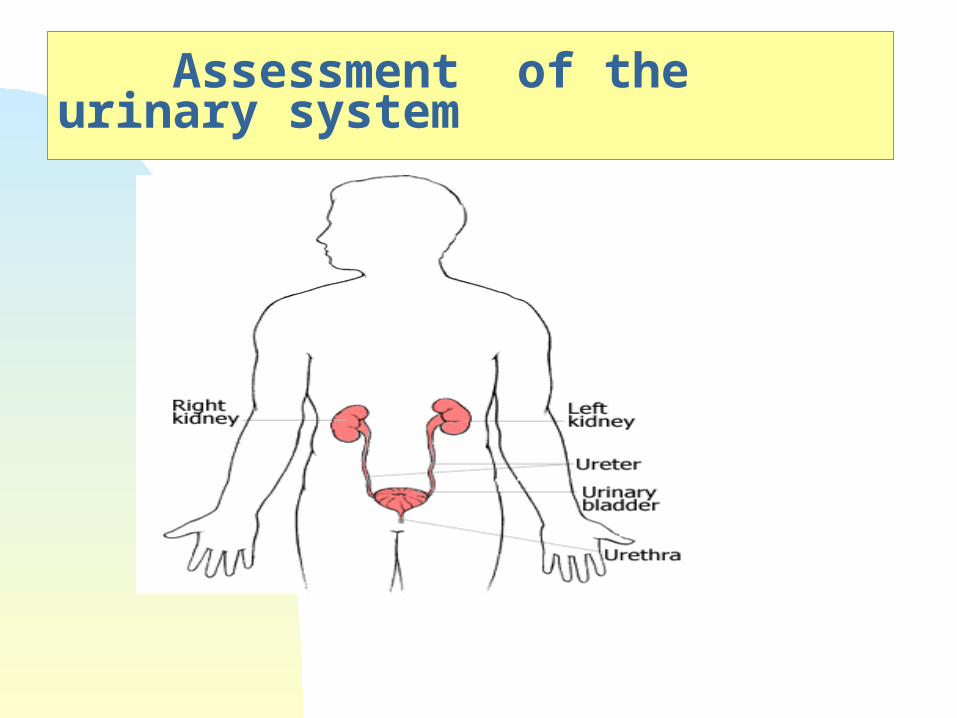
Assessment of the urinary system
Learning Objectives:-
1- Identify the important new terms related to urinary system.
2- List the factors which influencing urination.
3- Enumerate function of kidneys.
4- Differentiate between normal and abnormal finding.
Important new Terms
* Oliguria: voiding a scanty amount of urine.
* Anuria: inability to produce urine, less common, but caused by a decrease in renal perfusion.
* Polyuria: excessive output of urine.
* Hematuria: blood noted in urine.
* Nocturia: having to void at night.

* Dysuria: difficulty in voiding or pain in voiding.
* Enuresis: involuntary loss of urine at night.
* Pyuria : presence of pus in the urine.
* Glycosuria: presence of sugar in urine.
* Albumin urea: presence of albumin in the urine.
Factors influencing urination1. Socio cultural2. psychological3. muscle tone4. fluid balance5. surgical procedures6. medication
Functions of the kidneys Kidney:-
•Urine formation
• Excretion of waste products
• Regulation of electrolytes
• Regulation of acid–base balance
• Control of water balance
• Control of blood pressure
• Renal clearance
• Regulation of red blood cell production
• Synthesis of vitamin D to active form
• Secretion of prostaglandins.
Find the costovertebral angle which formed by the lower border of the 12th rib and the transverve processes of the upper lumbar vertebrae.
Place left hand flat in this area on one side, hit the hand sharply with the fist of the other patient will admit to tenderness if present.
Repeat on the other side
Palpation of kidney
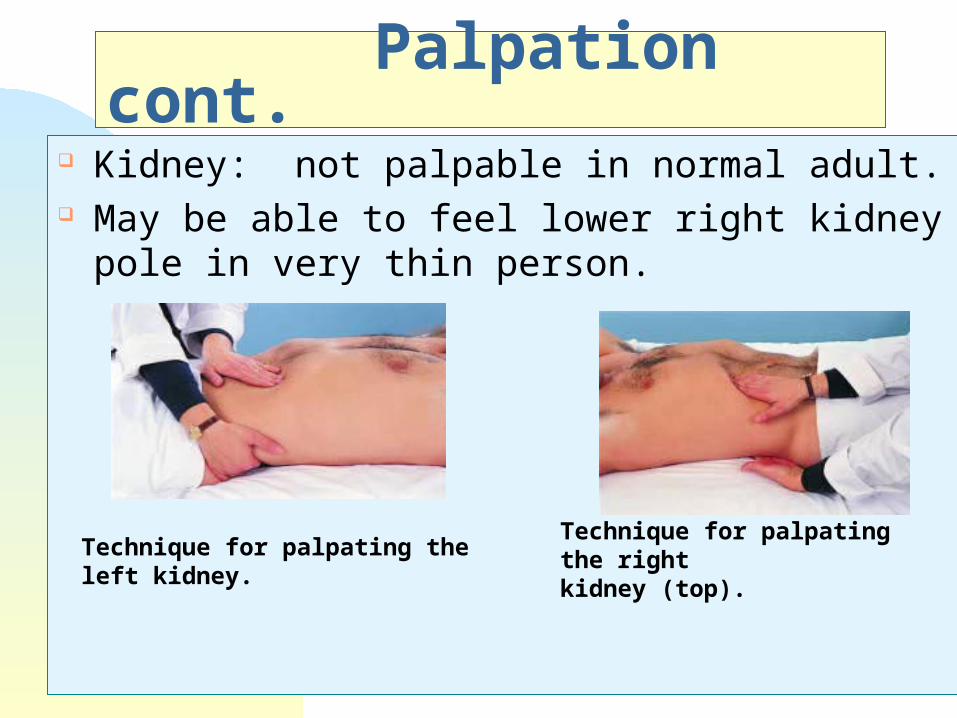
Palpation cont. Kidney: not palpable in normal adult. May be able to feel lower right kidney pole in very
thin person.
Technique for palpating the left kidney.
Technique for palpating the right kidney (top).
Deep palpation
If masses are felt, note: location, size, shalpe, consistency, tenderness, pulsations, mobility with respiration or with hand.
If patient is obese or rigid, use 2 hands to palpate Place one on top of other and feel with lower hand
Palpation of the bladder Bladder percussion is unnecessary unless
there is a suspicion of urinary retention.
Palpate above the symphysis.
An empty bladder is not palpable.
The bladder should be percussed after the patient voids to check for residual urine.
Percussion of the bladder begins at the midline just
above the umbilicus and proceeds downward.
The sound changes from tympanic to dull when
percussing over the bladder.
The bladder, which can be palpated only if it is moderately distended, feels like a smooth, firm, round mass rising out of the abdomen, usually at midline.
Dullness to percussion of the bladder following voiding indicates incomplete bladder emptying.
Assessing the Aorta Press firmly deep in upper abdomen slightly to
left of midline. Feel for aortic pulsations Determine width of aorta by pressing deeply on
either side of aorta What is the normal width of the aorta? If pulsatile mass is found, feel for femoral pulses
which may be dimished.
Special test for appendicitis:Rebound tenderness: mean deeply palpation&
withdrawal quickly, this caused pain in appendicitis.
Psoas sign : pt lie in supine position & raise right leg , if the pain found this is indicate to appendicitis.
Oburator sign: pt flex right leg at hip and knee. Then rotate leg internally and externally.