Assessing Children’s Psychological Wellbeing in Namibia: Lessons for Research, Policy & Service...
36
Assessing Children’s Psychological Wellbeing in Namibia: Lessons for Research, Policy & Service Delivery Mónica Ruiz-Casares, Ph.D. McGill University Health Center 1 st ISCI Conference Chicago, IL, June 27, 2007
-
Upload
donna-lambert -
Category
Documents
-
view
214 -
download
0
Transcript of Assessing Children’s Psychological Wellbeing in Namibia: Lessons for Research, Policy & Service...
Assessing Children’s Psychological Wellbeing in Namibia:
Lessons for Research, Policy & Service Delivery
Mónica Ruiz-Casares, Ph.D.McGill University Health Center
1st ISCI ConferenceChicago, IL, June 27, 2007
Overview
I. Background informationa. Data sources & study overviewb. MH in Namibia: Situational analysis
II. Children & youth in Namibia: MH Associated Factors
a. Demographic factorsb. Social factors
III. Children & youth in Namibia: MH Indicatorsa. Depression in children & youthb. Juvenile suicide
IV. Moving forward: Lessons for research, policy & service delivery
I. Background Information
Sources of information
• Literature review & government statistics• Adults:
– Individual & group interviews
• Children & Youth: – Depression Inventory (CHH=33 + Schools=163)– Interviews (CHH)
• Open ended questions• Social networks• Life Changing Events• Suicide ideation
Namibia: Mental Health Situation Analysis
• South African legacy– Trauma-related illness
• Major challenges: – Unemployment
– Substance abuse
– Domestic violence
– Suicide and suicidal thinking
– HIV/AIDS
– Disabilities
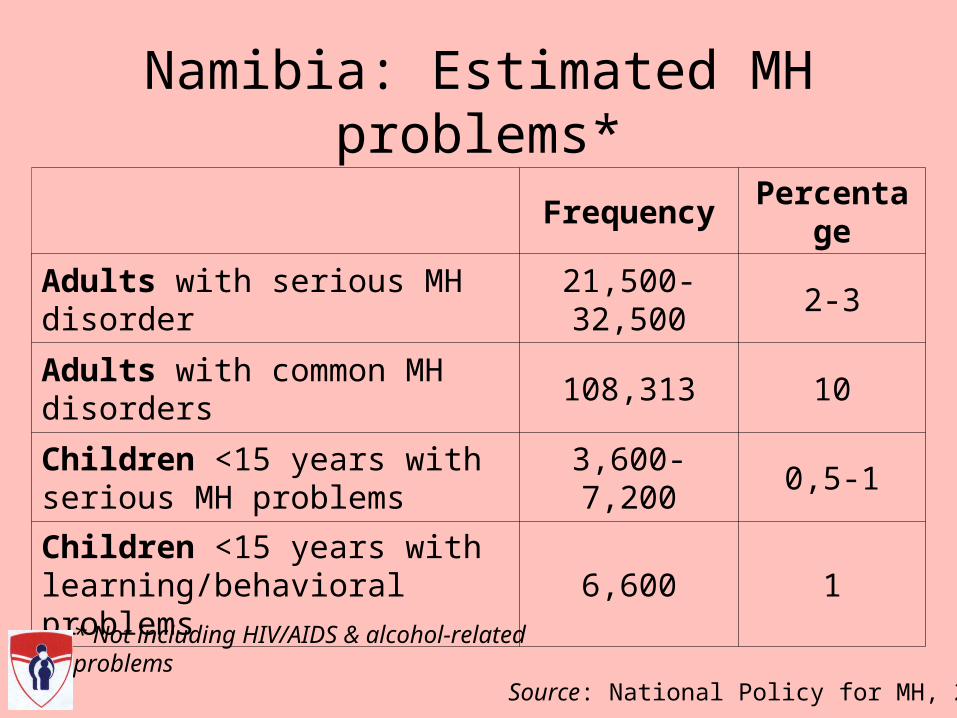
Namibia: Estimated MH problems*
Frequency Percentage
Adults with serious MH disorder 21,500-32,500 2-3
Adults with common MH disorders 108,313 10
Children <15 years with serious MH problems
3,600-7,200 0,5-1
Children <15 years with learning/behavioral problems
6,600 1
* Not including HIV/AIDS & alcohol-related problems
Source: National Policy for MH, 2005

Namibia: MH Services
• Public services– Windhoek MH Care Center
(National Referral Hospital)
– Oshakati Psychiatric Unit (intermediate hospital)
– District Hospitals
– Some Health Care Centers & Clinics
• Private services– Private specialists
– Traditional Healers
Beds/MH Practitioners(per 100 000 population)
Freq.
Total psychiatric beds 1.5
Psychiatrists 0.2
Neurologists 0
Psychiatric Nurses 0
Social Workers 6
Psychologists 6
Source: National Policy for MH, 2005

Namibia: Mental Health Resources• Legislation
– Mental Health & Substance Abuse Policies (2005)
– National Therapeutic Drug Policy/Essential List of Drugs (1995)
– Orphan & Vulnerable Children Policy (2004)
– Mental Health Legislation (1973)
• Administration– Primary Health Care Directorate
• Disability Prevention & Rehabilitation Division
– National MH Programme
– Social Services Directorate
– Alcohol & Substance Abuse Programme
– National Inter-sectoral MH Action Group

II. Children & youth in Namibia: Mental Health Associated Factors
150000 100000 50000 0 50000 100000 150000
00-04
05-09
10-14
15-19
20-24
25-29
30-34
35-39
40-44
45-49
50-54
55-59
60-64
65-69
70-74
75-79
80-84
85-89
90-94
95+
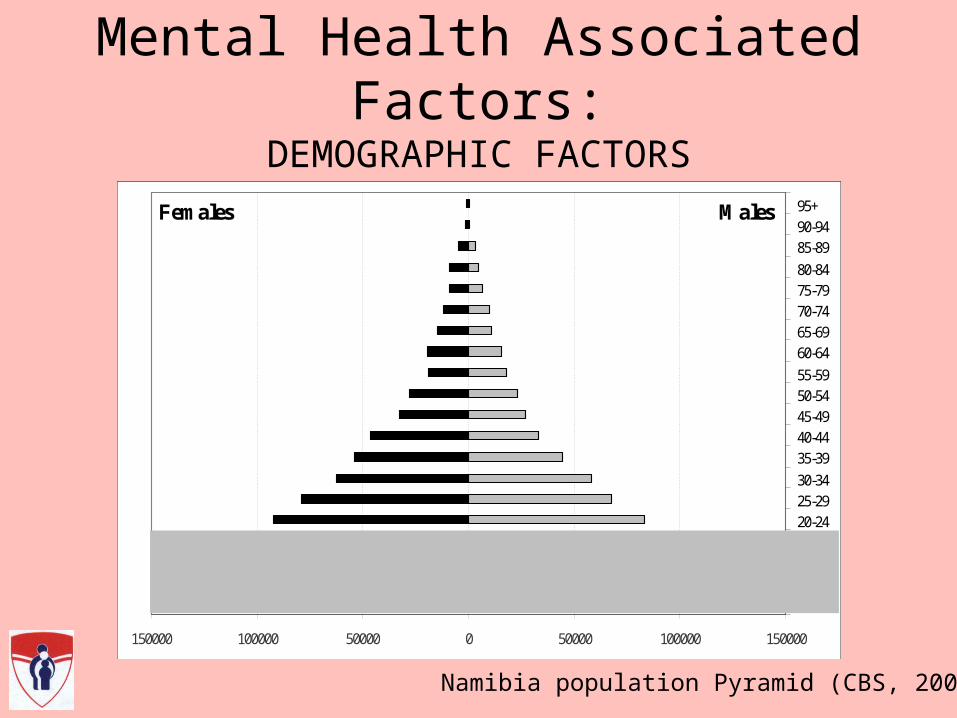
Figure 1. Namibia’s population pyramid (CBS, 2006).
MalesFemales
150000 100000 50000 0 50000 100000 150000
00-04
05-09
10-14
15-19
20-24
25-29
30-34
35-39
40-44
45-49
50-54
55-59
60-64
65-69
70-74
75-79
80-84
85-89
90-94
95+
Figure 1. Namibia’s population pyramid (CBS, 2006).
150000 100000 50000 0 50000 100000 150000
00-04
05-09
10-14
15-19
20-24
25-29
30-34
35-39
40-44
45-49
50-54
55-59
60-64
65-69
70-74
75-79
80-84
85-89
90-94
95+
150000 100000 50000 0 50000 100000 150000
00-04
05-09
10-14
15-19
20-24
25-29
30-34
35-39
40-44
45-49
50-54
55-59
60-64
65-69
70-74
75-79
80-84
85-89
90-94
95+
Figure 1. Namibia’s population pyramid (CBS, 2006).
MalesFemales
Namibia population Pyramid (CBS, 2006)
Mental Health Associated Factors:DEMOGRAPHIC FACTORS
“To play the role of a mother, looking after children. Some of my friends and other girls feel unhappy when that happens. At the beginning, I did not accept it. People wanted to bury [my youngest brother] with my mother, [but] I decided to keep the baby. I struggled to raise him, [and] wondered if I would know how to do it right…”
Kavango, girl head since 16
Things that make you upset

Mental Health Associated Factors
SOCIAL FACTORS• Family Environment
– Fostering & Orphanhood
– Domestic violence & child abuse
• Stigma & discrimination• Stressful events
• Poverty
• Social Networks and Social Support
• Schooling/Work
OTHER FACTORS• Physical health
• Habits
• Spirituality/religion
• Personal systems of meaning

“When someone tells you “I love you” (…), that feels good.”
Kavango, girl head since 17
Things that make you happy
“My friends can make me happy when they give me advice.”
Caprivi, girl head since 11
III. Children & youth in Namibia:
Mental Health Indicators

Contextualizing MH measurement : Exploring local meaning• Withdrawal (‘Hide from visitors’)
• Not play with other children
• Insult without a reason
• Sadness (‘Sad face’)
• Fearful
• Do not show emotions
• Poor hygiene
• Changes in sleep and appetite
• Envy
• Poor school performance

Measuring depression in children & youth: Children’s Depression Inventory
CDI (Kovacs, 1977)Self-reported severity rating scale
27 items1 suicidal ideation item
7-17 yearsPrevious 2 weeksMultidimensional (depressive symptoms): 5 factor scales
Negative moodPersonal problemsIneffectivenessAnhedoniaNegative self-esteem
CDI-AdaptedSelf-reported severity rating scale
27 + 3 items1 suicidal ideation item (CHH)
7-17 + 18-21 yearsPrevious 2 weeksMultidimensional (overall α = .708;5 factor scales α = .16-.52)
2 forms (non/schooling)CHHs (N=33) + Schools (N=163)

Measuring depression in children & youth: School sample
Frequency (%) Schools
Sex* Female 81 (50.6)
Male 79 (49.4)
Current age (years) 9-12 43 (26.4)
13-17 81 (49.7)
18-21 39 (23.9)
Currently schooling 163 (100.0)
Orphanhood Non-orphans 89 (54.6)
Orphans (S/D) 74 (45.4)
Paternal O. 55 (33.7)
Maternal O. 42 (25.8)
Double O. 23 (14.1)
TOTAL participants 163
* 3 MV
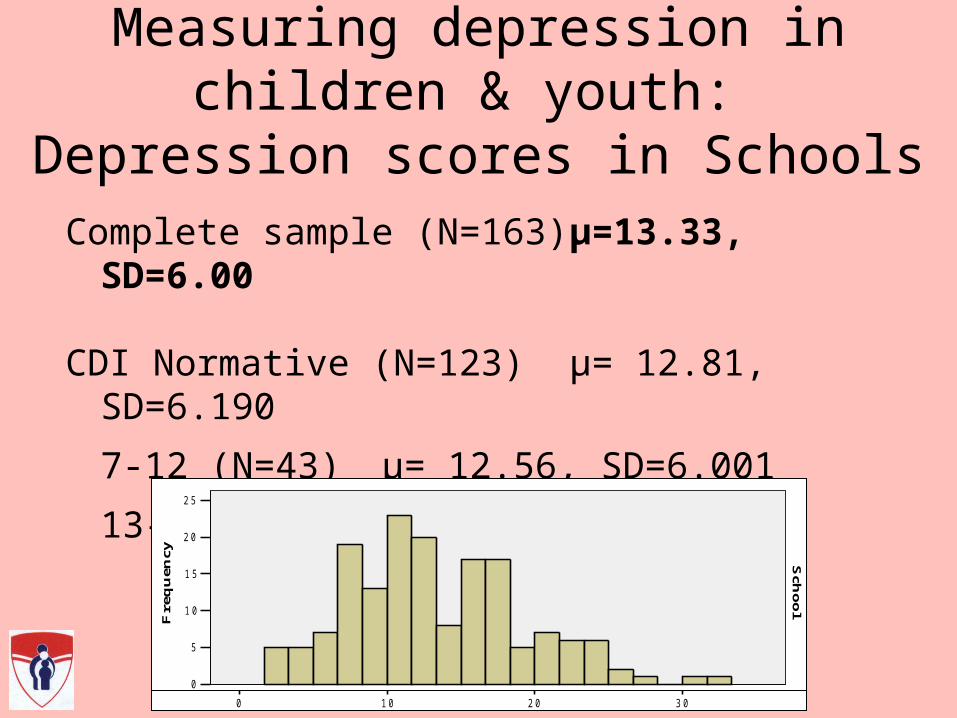
Measuring depression in children & youth: Depression scores in Schools
Complete sample (N=163) μ=13.33, SD=6.00
CDI Normative (N=123) μ= 12.81, SD=6.190
7-12 (N=43) μ= 12.56, SD=6.001
13-17 (N=81) μ= 12.95, SD=6.320
Sch
oo
lC
HH
3 02 01 00
F i g u r e 1 . T o t a l C D I - A d a p t e d s c o r e s f o r c o n t r o l g r o u p a n d p a r t i c i p a n t s
2 5
2 0
1 5
1 0
5
0
Fre
qu
ency
2 5
2 0
1 5
1 0
5
0
Fre
qu
ency
Sch
oo
lC
HH
3 02 01 00
F i g u r e 1 . T o t a l C D I - A d a p t e d s c o r e s f o r c o n t r o l g r o u p a n d p a r t i c i p a n t s
2 5
2 0
1 5
1 0
5
0
Fre
qu
ency
2 5
2 0
1 5
1 0
5
0
Fre
qu
ency
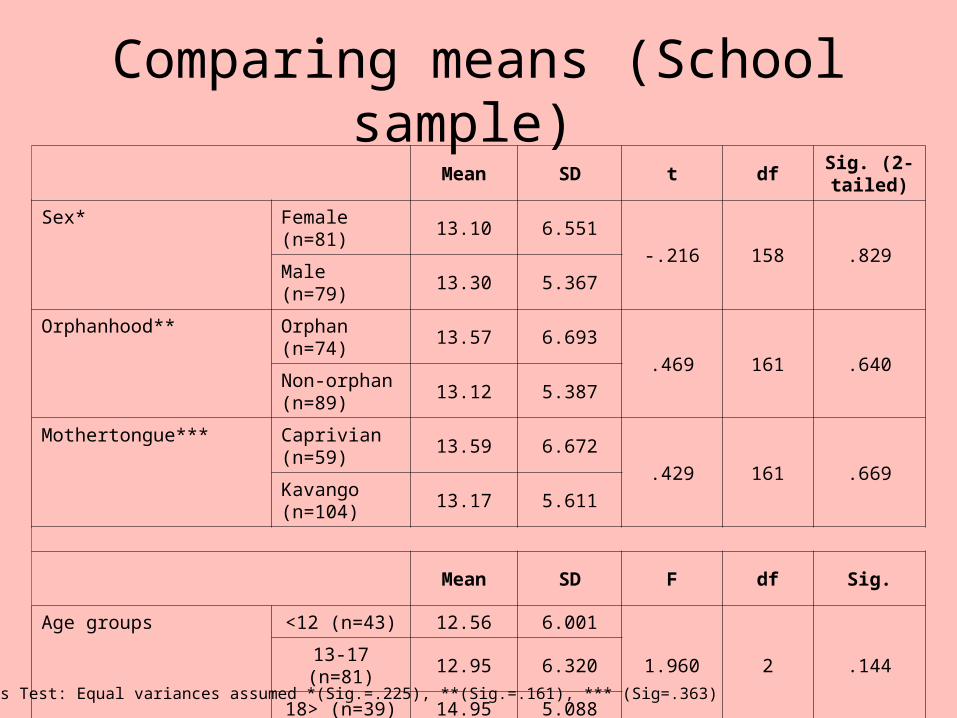
Mean SD t dfSig. (2-tailed)
Sex* Female (n=81)
13.10 6.551-.216 158 .829
Male (n=79) 13.30 5.367
Orphanhood** Orphan (n=74)
13.57 6.693
.469 161 .640Non-orphan (n=89)
13.12 5.387
Mothertongue*** Caprivian (n=59)
13.59 6.672
.429 161 .669Kavango (n=104)
13.17 5.611
Mean SD F df Sig.
Age groups <12 (n=43) 12.56 6.001
1.960 2 .14413-17 (n=81) 12.95 6.320
18> (n=39) 14.95 5.088
Levene’s Test: Equal variances assumed *(Sig.=.225), **(Sig.=.161), *** (Sig=.363)
Comparing means (School sample)
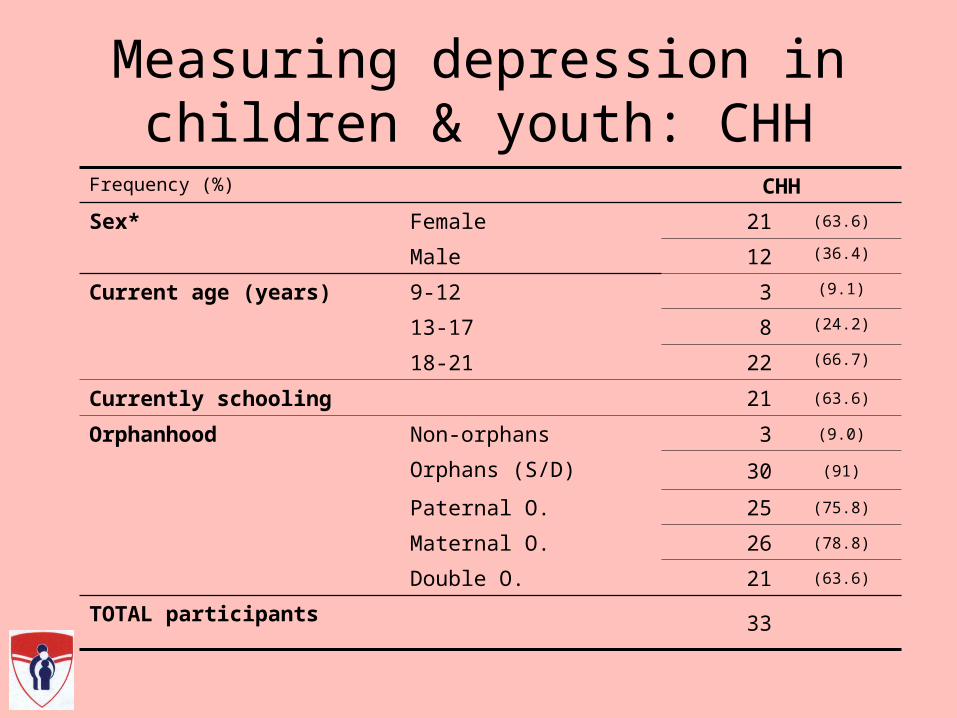
Frequency (%) CHH
Sex* Female 21 (63.6)
Male 12 (36.4)
Current age (years) 9-12 3 (9.1)
13-17 8 (24.2)
18-21 22 (66.7)
Currently schooling 21 (63.6)
Orphanhood Non-orphans 3 (9.0)
Orphans (S/D) 30 (91)
Paternal O. 25 (75.8)
Maternal O. 26 (78.8)
Double O. 21 (63.6)
TOTAL participants 33
Measuring depression in children & youth: CHH
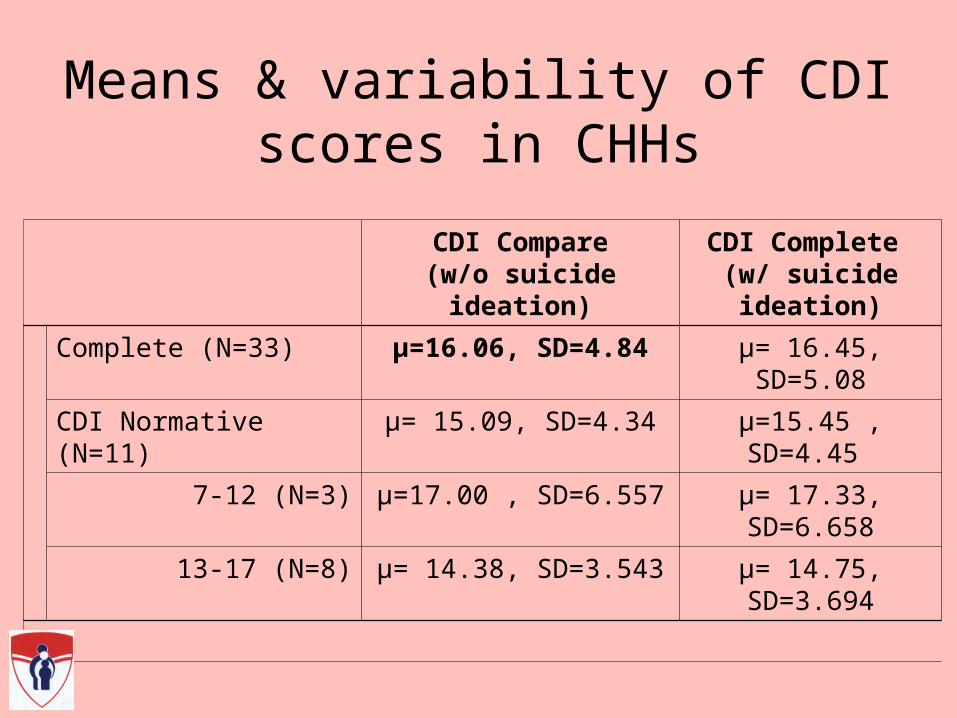
Means & variability of CDI scores in CHHs
CDI Compare(w/o suicide ideation)
CDI Complete (w/ suicide ideation)
Complete (N=33) μ=16.06, SD=4.84 μ= 16.45, SD=5.08
CDI Normative (N=11) μ= 15.09, SD=4.34 μ=15.45 , SD=4.45
7-12 (N=3) μ=17.00 , SD=6.557 μ= 17.33, SD=6.658
13-17 (N=8) μ= 14.38, SD=3.543 μ= 14.75, SD=3.694

Levene’s Test: Equal variances assumed *(Sig.=.668), **(Sig.=.220)L
Comparing means (CHHs)
Mean SD t dfSig.
(2-tailed)
Sex* Female (n=21) 16.43 5.192.572 31 .572
Male (n=12) 15.42 4.295
Orphanhood** Orphan (n=30) 16.23 4.987.642 31 .525
Non-orphan (n=3) 14.33 3.055
Mean SD F df Sig.
Mothertongue*** Caprivian/Kxoe (n=9) 17.22 4.738
6.261 2 .005Kavango (n=13) 18.31 4.498
Oshiwambo (n=11) 12.45 3.267
Age groups
<12 (n=3) 17.00 6.557
.637 2 .53613-17 (n=8) 14.38 3.543
18> (n=22) 16.55 5.096

Total CDI-Ad scores for control & CHHs
Sch
oolC
HH
3 02 01 00
F i g u r e 1 . T o t a l C D I - A d a p t e d s c o r e s f o r c o n t r o l g r o u p a n d p a r t i c i p a n t s
2 5
2 0
1 5
1 0
5
0
Fre
qu
ency
2 5
2 0
1 5
1 0
5
0
Fre
qu
ency
μ=13.33
SD=6.00
μ=16.06, SD=4.84
* Equal variances assumed (Sig.=.211)
Significant difference (t= 2.460, Sig= .015) lost for normative group
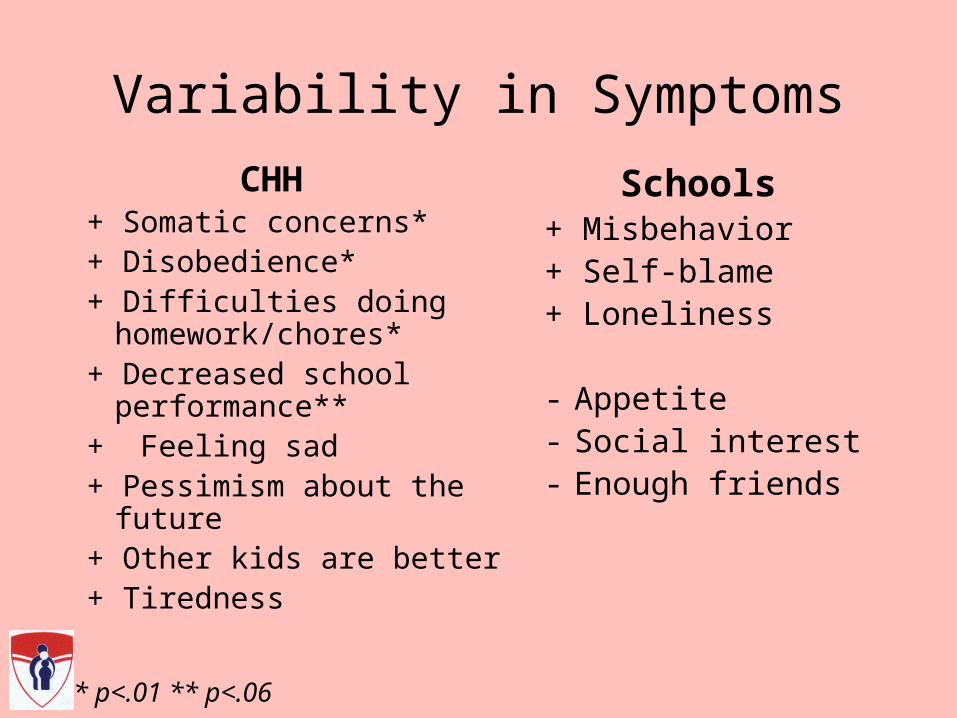
Variability in Symptoms
CHH+ Somatic concerns*+ Disobedience*+ Difficulties doing
homework/chores*+ Decreased school
performance**+ Feeling sad+ Pessimism about the
future+ Other kids are better+ Tiredness
Schools+ Misbehavior+ Self-blame+ Loneliness
- Appetite- Social interest- Enough friends
* p<.01 ** p<.06

Juvenile Suicide Statistics (Namibian Police, April 2006)
Method2003 2004 2005
TotalMales Females Males Females Males Females
Hanging 12 5 7 4 5 4 37
Shooting 1 1 2 7 11
Overdose 2 2
Drowning 1 1
Poisoning 2 2
Total13 6 10 6 14 4
5319 16 18

“I have not talked about it [suicide] with anyone. I know
some social workers, but I would not feel comfortable talking to
them about it…”
Caprivi, boy head since 16

Suicidal ideation among CHHs
“After the death of my mother, I wanted to cause suicide, but (…) I got an advice from my friend. She told me: ‘If you want to cause suicide, look! You are having your young sister! Who is going to take care of your young sister? It would be better if some of these relatives of yours liked you, but they hate you. If you are going to cause suicide, there is no one who is going to take care of your sister’”
Caprivi, girl head since age 18
“I just think it in my heart…”: Suicidal ideation among CHHs
REASONS for SUICIDE• Poverty
• Conflict—“[I think about it] when someone makes me angry”
• Helplessness—“Sometimes I feel I am suffering a lot”.
REASONS NOT TO COMMIT SUICIDE
• Have to care for siblings—“There is no way I can leave my siblings” and “nobody would stay with my brother and my sister”.
• Hope of a better future—“I think that in the future I may get a good life” and “maybe I’ll do something good in the future”
• It is “wrong”—“I doubt; it is a bad thought…” and “I think about the Ten Commandments of God…”.
Limitations
• Small population/sample
• Absence of clinical diagnosis for comparison
• Cultural appropriateness of measure
• Self-report & administration
• Limited MH resources (ethics & follow-up)
IV. Moving forward:
Lessons for Research, Policy, & Service Delivery

Children’s advice to children
• “Stay together & care for each other”
• “Give positive advice & encourage each other to focus on schoolwork”
• “Be satisfied with what you have and don't think too much about being alone”
• “Trust in God and don't loose hope”
• “Avoid peer pressure, and abstain from alcohol, tobacco & sex”
“Advise families who are staying on their own to take school seriously and stay in good health.”
Omusati, boy head since 16
Children’s request to leaders
Children & Adolescent Mental Health: Lessons for Policy & Service Delivery1. Formulate mental health legislation
– Develop a child and adolescent mental health policy, services and training.
2. Barriers to care:– Stigma & public knowledge Public education– Poverty/Resources Training programs– Transportation– Language
3. Integrate mental health, general health and community care:– Promotion– Prevention– Treatment & Rehabilitation: “Continuum” of services
4. Training
Children & Adolescent Mental Health: Lessons for Research
1. Epidemiological studies of mental health in children & adolescents and associated disabilities
2. Culturally appropriate expressions of grief & healing practices (outcomes)
3. Cultural development/adaptation & translation of measures
4. Involve children in research!

“I learnt something important [today]: to ask, because you asked me how we are living. This helps me because (…) since my mother passed away, nobody has asked me this type of questions.”
Caprivi, boy head of household since age 17