
Aspirin delays mesothelioma growth by inhibiting...
11
OPEN Aspirin delays mesothelioma growth by inhibiting HMGB1-mediated tumor progression H Yang* ,1 , L Pellegrini 1 , A Napolitano 1,2 , C Giorgi 3 , S Jube 1 , A Preti 4 , CJ Jennings 1 , F De Marchis 4 , EG Flores 1 , D Larson 1 , I Pagano 1 , M Tanji 1 , A Powers 1 , S Kanodia 5 , G Gaudino 1 , S Pastorino 1 , HI Pass 6 , P Pinton 3 , ME Bianchi 4 and M Carbone* ,1 High-mobility group box 1 (HMGB1) is an inflammatory molecule that has a critical role in the initiation and progression of malignant mesothelioma (MM). Aspirin (acetylsalicylic acid, ASA) is the most widely used nonsteroidal anti-inflammatory drug that reduces the incidence, metastatic potential and mortality of many inflammation-induced cancers. We hypothesized that ASA may exert anticancer properties in MM by abrogating the carcinogenic effects of HMGB1. Using HMGB1-secreting and -non-secreting human MM cell lines, we determined whether aspirin inhibited the hallmarks of HMGB1-induced MM cell growth in vitro and in vivo. Our data demonstrated that ASA and its metabolite, salicylic acid (SA), inhibit motility, migration, invasion and anchorage- independent colony formation of MM cells via a novel HMGB1-mediated mechanism. ASA/SA, at serum concentrations comparable to those achieved in humans taking therapeutic doses of aspirin, and BoxA, a specific inhibitor of HMGB1, markedly reduced MM growth in xenograft mice and significantly improved survival of treated animals. The effects of ASA and BoxA were cyclooxygenase-2 independent and were not additive, consistent with both acting via inhibition of HMGB1 activity. Our findings provide a rationale for the well documented, yet poorly understood antitumorigenic activity of aspirin, which we show proceeds via HMGB1 inhibition. Moreover, the use of BoxA appears to allow a more efficient HMGB1 targeting while eluding the known gastrointestinal side effects of ASA. Our findings are directly relevant to MM. Given the emerging importance of HMGB1 and its tumor-promoting functions in many cancer types, and of aspirin in cancer prevention and therapy, our investigation is poised to provide broadly applicable information. Cell Death and Disease (2015) 6, e1786; doi:10.1038/cddis.2015.153; published online 11 June 2015 Malignant mesothelioma (MM) is an aggressive cancer that arises from the neoplastic transformation of mesothelial cells lining the pleural, peritoneal, and pericardial cavities. 1 In the United States, ~ 3200 individuals are diagnosed annually with MM and a similar number dies of this almost invariably fatal disease. 1 Major risk factors for MM are exposure to asbestos and erionite mineral fibers and germline BAP1 mutations. 1,2 We have demonstrated that high-mobility group box 1 (HMGB1), the prototypical damage-associated molecular pattern molecule that is normally present in the nucleus of cells, is a critical mediator of asbestos-induced MM (reviewed in Carbone and Yang 3 ). Within the nucleus, HMGB1 is a non- histone chromatin-binding protein that regulates nucleosome assembly and chromatin structure. 4 HMGB1 is passively released by necrotic cells or actively secreted by immune and cancer cells. 4–7 When in the extracellular space, HMGB1 is responsible for the initiation and perpetuation of the inflam- matory response and also directly promotes MM growth. 4,5,7 Our published data show that asbestos causes necrosis of primary human mesothelial cells that results in the passive release of HMGB1 into the extracellular space where it induces the secretion of TNF-α and other cytokines, recruits macro- phages and thus initiates inflammation. 5 The prolonged biopersistence of asbestos fibers lodged in the pleura initiates a vicious cycle of chronic cell death and chronic inflammation that, over a period of many years, can lead to MM. 5 As MM arises in an HMGB1-rich environment, most of the MM cells are HMGB1 growth dependent and require HMGB1 to migrate and invade nearby tissues. 7 Accordingly, out of seven MM cell lines available in our lab, six actively secrete high amounts of HMGB1 and are dependent on it for growth. 7 Moreover, we have demonstrated that the tumor phenotype of HMGB1-secreting human MM cells requires HMGB1 for continued growth, and that abrogation of HMGB1 function may have therapeutic efficacy. 7 Although MM is the most well-characterized HMGB1- related tumor model, 7 the relevance of extracellular HMGB1 1 University of Hawaii Cancer Center, University of Hawaii, Honolulu, HI 96813, USA; 2 Department of Molecular Biosciences and Bioengineering, University of Hawaii, Honolulu, HI 96813, USA; 3 Department of Morphology, Surgery and Experimental Medicine, University of Ferrara, Ferrara 44121, Italy; 4 San Raffaele University and Scientific Institute, Milan 20132, Italy; 5 Samuel Oschin Comprehensive Cancer Institute and Department of Biomedical Sciences, Cedars-Sinai Medical Center, Los Angeles, CA 90048, USA and 6 Department of Cardiothoracic Surgery, NewYork Langone Medical Center, New York, NY 10016, USA *Corresponding author: H Yang, University of Hawaii Cancer Center, University of Hawaii, 701 Ilalo Street, Room 439, Honolulu, HI 96813, USA. Tel: +1 808 440 4588; Fax: +1 808 587 0790; E-mail: [email protected] or M Carbone, University of Hawaii Cancer Center, University of Hawaii, 701 Ilalo Street, Room 450, Honolulu, HI 96813, USA. Tel: +1 808 440 4596; Fax: +1 808 587 0790; E-mail: [email protected] Received 24.3.15; revised 04.5.15; accepted 07.5.15; Edited by G Melino Abbreviations: ASA, acetylsalicylic acid; COX, cyclooxygenase enzymes; EMT, epithelial–mesenchymal transition; fMLP, N-formyl-methionyl-leucyl-phenylalanine; GI, gastrointestinal; HMGB1, high-mobility group box 1; MEF, mouse embryonic fibroblast; MM, malignant mesothelioma; NSAID, nonsteroidal anti-inflammatory drug; SA, salicylic acid; SCID, severe-combined immunodeficient; TNF-α, tumor necrosis factor-α Citation: Cell Death and Disease (2015) 6, e1786; doi:10.1038/cddis.2015.153 & 2015 Macmillan Publishers Limited All rights reserved 2041-4889/15 www.nature.com/cddis
Transcript of Aspirin delays mesothelioma growth by inhibiting...

OPEN
Aspirin delays mesothelioma growth by inhibitingHMGB1-mediated tumor progression
H Yang*,1, L Pellegrini1, A Napolitano1,2, C Giorgi3, S Jube1, A Preti4, CJ Jennings1, F De Marchis4, EG Flores1, D Larson1, I Pagano1,M Tanji1, A Powers1, S Kanodia5, G Gaudino1, S Pastorino1, HI Pass6, P Pinton3, ME Bianchi4 and M Carbone*,1
High-mobility group box 1 (HMGB1) is an inflammatory molecule that has a critical role in the initiation and progression ofmalignant mesothelioma (MM). Aspirin (acetylsalicylic acid, ASA) is the most widely used nonsteroidal anti-inflammatory drug thatreduces the incidence, metastatic potential and mortality of many inflammation-induced cancers. We hypothesized that ASA mayexert anticancer properties in MM by abrogating the carcinogenic effects of HMGB1. Using HMGB1-secreting and -non-secretinghuman MM cell lines, we determined whether aspirin inhibited the hallmarks of HMGB1-induced MM cell growth in vitro and in vivo.Our data demonstrated that ASA and its metabolite, salicylic acid (SA), inhibit motility, migration, invasion and anchorage-independent colony formation of MM cells via a novel HMGB1-mediated mechanism. ASA/SA, at serum concentrations comparableto those achieved in humans taking therapeutic doses of aspirin, and BoxA, a specific inhibitor of HMGB1, markedly reduced MMgrowth in xenograft mice and significantly improved survival of treated animals. The effects of ASA and BoxA werecyclooxygenase-2 independent and were not additive, consistent with both acting via inhibition of HMGB1 activity. Our findingsprovide a rationale for the well documented, yet poorly understood antitumorigenic activity of aspirin, which we show proceeds viaHMGB1 inhibition. Moreover, the use of BoxA appears to allow a more efficient HMGB1 targeting while eluding the knowngastrointestinal side effects of ASA. Our findings are directly relevant to MM. Given the emerging importance of HMGB1 and itstumor-promoting functions in many cancer types, and of aspirin in cancer prevention and therapy, our investigation is poised toprovide broadly applicable information.Cell Death and Disease (2015) 6, e1786; doi:10.1038/cddis.2015.153; published online 11 June 2015
Malignant mesothelioma (MM) is an aggressive cancer thatarises from the neoplastic transformation of mesothelial cellslining the pleural, peritoneal, and pericardial cavities.1 In theUnited States, ~ 3200 individuals are diagnosed annually withMM and a similar number dies of this almost invariably fataldisease.1 Major risk factors for MM are exposure to asbestosand erionite mineral fibers and germline BAP1 mutations.1,2
We have demonstrated that high-mobility group box 1(HMGB1), the prototypical damage-associated molecularpattern molecule that is normally present in the nucleus ofcells, is a critical mediator of asbestos-induced MM (reviewedin Carbone and Yang3). Within the nucleus, HMGB1 is a non-histone chromatin-binding protein that regulates nucleosomeassembly and chromatin structure.4 HMGB1 is passivelyreleased by necrotic cells or actively secreted by immune andcancer cells.4–7 When in the extracellular space, HMGB1 isresponsible for the initiation and perpetuation of the inflam-matory response and also directly promotes MM growth.4,5,7
Our published data show that asbestos causes necrosis ofprimary human mesothelial cells that results in the passiverelease of HMGB1 into the extracellular space where it inducesthe secretion of TNF-α and other cytokines, recruits macro-phages and thus initiates inflammation.5 The prolongedbiopersistence of asbestos fibers lodged in the pleura initiatesa vicious cycle of chronic cell death and chronic inflammationthat, over a period of many years, can lead to MM.5 As MMarises in an HMGB1-rich environment, most of the MM cells areHMGB1 growth dependent and require HMGB1 to migrate andinvade nearby tissues.7 Accordingly, out of seven MM cell linesavailable in our lab, six actively secrete high amounts of HMGB1and are dependent on it for growth.7 Moreover, we havedemonstrated that the tumor phenotype of HMGB1-secretinghumanMMcells requiresHMGB1 for continued growth, and thatabrogation of HMGB1 function may have therapeutic efficacy.7
Although MM is the most well-characterized HMGB1-related tumor model,7 the relevance of extracellular HMGB1
1University of Hawaii Cancer Center, University of Hawaii, Honolulu, HI 96813, USA; 2Department of Molecular Biosciences and Bioengineering, University of Hawaii,Honolulu, HI 96813, USA; 3Department of Morphology, Surgery and Experimental Medicine, University of Ferrara, Ferrara 44121, Italy; 4San Raffaele University andScientific Institute, Milan 20132, Italy; 5Samuel Oschin Comprehensive Cancer Institute and Department of Biomedical Sciences, Cedars-Sinai Medical Center,Los Angeles, CA 90048, USA and 6Department of Cardiothoracic Surgery, New York Langone Medical Center, New York, NY 10016, USA*Corresponding author: H Yang, University of Hawaii Cancer Center, University of Hawaii, 701 Ilalo Street, Room 439, Honolulu, HI 96813, USA. Tel: +1 808 440 4588;Fax: +1 808 587 0790; E-mail: [email protected] M Carbone, University of Hawaii Cancer Center, University of Hawaii, 701 Ilalo Street, Room 450, Honolulu, HI 96813, USA. Tel: +1 808 440 4596; Fax: +1 808 587 0790;E-mail: [email protected]
Received 24.3.15; revised 04.5.15; accepted 07.5.15; Edited by G Melino
Abbreviations: ASA, acetylsalicylic acid; COX, cyclooxygenase enzymes; EMT, epithelial–mesenchymal transition; fMLP, N-formyl-methionyl-leucyl-phenylalanine;GI, gastrointestinal; HMGB1, high-mobility group box 1; MEF, mouse embryonic fibroblast; MM, malignant mesothelioma; NSAID, nonsteroidal anti-inflammatory drug;SA, salicylic acid; SCID, severe-combined immunodeficient; TNF-α, tumor necrosis factor-α
Citation: Cell Death and Disease (2015) 6, e1786; doi:10.1038/cddis.2015.153& 2015 Macmillan Publishers Limited All rights reserved 2041-4889/15
www.nature.com/cddis

to carcinogenesis has also been proposed in otherinflammation-related malignancies.8 Recent data indicate thatHMGB1 initiates a chain of events that promotes tumormetastasis in melanoma,9 a malignancy that shares somecommon molecular pathogenetic mechanisms with MM.2
HMGB1 levels in blood are elevated in MM,7,10 and in severalother inflammation-related cancers.11,12
Acetylsalicylic acid (ASA), commonly known as aspirin,is the most widely used nonsteroidal anti-inflammatorydrug (NSAID) worldwide.13 In addition to its well-knowneffects in reducing inflammation, and preventing plateletaggregation and related effects on cardiovascular diseases,ASA reduces the incidence, metastatic potential andmortality of colon cancer, and possibly of other solidmalignancies, most of which have inflammation-mediatedinitiation or progression.14,15
ASA is absorbed by the stomach and upper intestine and isdeacetylated to form salicylic acid (SA) in about 15–30min.SA has a half-life of several hours in human plasma; thus,much of ASA bioactivity is attributed to SA. In humans, peaklevels of SA in plasma vary between 20 and 150 μM at ASAdoses of ≤325mg per day and vary between 0.3 and 1.5 mMin patients taking up to 1.5 g per day of ASA.16,17 These dosesare hereafter collectively referred to as 'therapeutic levels' asthese are the dose ranges of aspirin that are administered fordifferent therapies to millions of people every day.To the best of our knowledge, the possible beneficial effects
of ASA in humanMM have not been investigated. However, byreviewing the information collected for the Physician's HealthStudy,18 we found data suggesting a possible associationbetween ASA use and reduced MM incidence. In this study,22 067 physicians were followed for 24 years with 17 reportedcases of MM. An intention-to-treat analysis comparing ASA(325mg on alternate days) and placebo treatment revealeda relative risk of 0.7 (0.3–1.9, 95% confidence interval),indicating a 30% reduction in MM risk. The small number ofMM cases resulted in insufficient power for a statisticallysignificant analysis; however, these findings suggested thatASA might have the potential as an effective drug for MM. Inthe present study, we demonstrate that ASA and itsmetabolite, SA, exert anticancer activity against MM byinhibiting the biological effects of HMGB1 at physiologicallyrelevant concentrations.
Results
Treatment with ASA significantly reduces MM tumorgrowth in vivo. To determine whether ASA influences MMgrowth in vivo, a xenograft model was established byinjecting severe-combined immunodeficient (SCID) mice withluciferase-expressing HMGB1-secreting human MM cell lineREN (REN/luc) intraperitoneally.7 ASA was given by oralgavage at the doses of 25mg/kg per day, which according toprevious studies should be equivalent to 80–110mg per day inhumans.19 ASA treatment was initiated 4 days after injectingREN/luc cells, which is when the tumors became detectable byIVIS imaging. ASA was administered daily thereafter, until theexperiment was halted because of gastrointestinal (GI)bleeding (Figure 1a). A slope comparison test revealed thatASA treatment caused a significant suppression of MM growthcompared with controls (t(67)=4.8, Po0.0001) (Figure 1b).Mice receiving ASA showed a significant reduction of HMGB1in serum (Figure 1c). We ruled out the possibility that SA-HMGB1 interaction might impair measurement of HMGB1 byELISA (Supplementary Figure S1). Therefore, the loweramount of HMGB1 in the serum of mice receiving ASA maybe related to smaller tumor sizes.The experiment was repeated with a modified protocol
designed to reduce ASA side effects, such as GI bleeding.When the tumors were established and visible by IVIS (day 4postinjection of REN/luc cells), ASA was administered by oralgavage daily for the first 2 weeks, and three times per weekthereafter. Two different doses of ASA (25 and 50mg/kg) wereused, which yielded slightly different peak levels of SA inplasma, with the 50mg/kg dose of ASA providing SA for alonger duration. Specifically, these doses achieved peaklevels of SA of 1 and 1.3 mM, respectively, at 30min post-ASA administration, which decreased to 0.4 and 0.7 mM,respectively, at 2 h post-ASA administration (Figure 1d).Forty-eight days from MM cell injection, the tumor growth
curves (Figures 1e and f) were comparable with thoseobserved in the previous experiment (Figures 1a and b), andshowed a marked reduction in tumor growth in animalsreceiving ASA (t(302)= 11.2, Po0.0001, based on a slopecomparison test). As therewas no evidence of GI bleeding, theexperiment could be continued past 48 days. Median survivalwas 76 days in the control group, 87.5 days in theASA 25mg/kg group and 91 days in the ASA 50mg/kg group.The increased survival of treated animals was statistically
Figure 1 Treatment with ASA significantly reduces MM tumor growth in vivo. Fourteen SCID mice were injected intraperitoneally with 5 × 105 REN/luc cells. After formation ofdetectable tumor nodules by IVIS imaging (4 days after cells injection), mice were weighed and randomly assigned to control (gavage of vehicle solution) and treatment (gavage of25 mg/kg per day ASA); groups of seven animals each. (a) Representative IVIS images. (b) Tumor growth curves of the two groups. Based on a slope comparison test, ASAtreatment resulted in significant suppression of MM growth compared with controls (t(67)= 4.8, Po0.0001). (c) Female SCID mice were randomly assigned to receive ASA-(25 mg/kg) or vehicle-supplemented gavage feeding. Blood was collected by cheek bleeding and serum levels of HMGB1 were measured by ELISA. *Po0.05. (d) SA plasmalevels in mice receiving ASA. Fifteen female SCID mice were randomly assigned to receive ASA (25 or 50 mg/kg) or vehicle by gavage feeding in groups of five mice. Blood wascollected by cheek bleeding at different time points ranging from 30 min to 24 h after feeding, and plasma levels of SA were measured with a specific ELISA. (e) RepresentativeIVIS images at different days postinjection of REN/luc cells shows reduced tumor growth in ASA-treated mice. Sixty SCID mice were injected intraperitoneally with 5 × 105 REN/luc cells. After formation of tumor nodules detectable by IVIS imaging (4 days after cells injection), mice were weighed and randomly assigned to control (gavage of vehicle) andtreatment (gavage of ASA at 25 or 50 mg/kg per day for the first 2 weeks and three times a week thereafter), groups of 20 animals each. (f) Tumor growth curves of the threeanimal groups up to 76 days. Measurement was halted thereafter as most mice in the control group had died. Based on a slope comparison test, treated animals showed amarked reduction in tumor growth (t(443)= 9.9, Po0.0001). (g) Kaplan–Meier survival plot of the three animal groups. Median survival was 76 days in the control group,87.5 days in the ASA 25 mg/kg group and 91 days in the ASA 50 mg/kg group. The increase in survival of treated animals is statistically significant for both ASA -treated groups(χ2(2)= 38.0, Po0.0001, log-rank test)
Aspirin inhibits HMGB1-mediated tumor growthH Yang et al
2
Cell Death and Disease

significant (χ2(2)= 38.0, Po0.0001, log-rank test) for bothASA- treated groups (Figure 1g). Overall, these data supportthe hypothesis that ASA/SA has therapeutic efficacy onestablished MM tumors.
Salicylates inhibit colony formation of MM cells. As MMgrowth relies on HMGB1 and HMGB1 is a critical factor for
MM pathogenesis,7 we hypothesized that the observedASA antitumor effects on MM may be, at least in part,mediated via an HMGB1-dependent mechanism. There-fore, using a panel of three different patient-derived MM celllines, REN, HMESO and PHI, we further analyzed whetherASA/SA could influence MM growth via targeting HMGB1in vitro. All three cell lines secrete high amounts of HMGB1
Aspirin inhibits HMGB1-mediated tumor growthH Yang et al
3
Cell Death and Disease

and are 'addicted' to HMGB1 for growth.7 The PPM-MILLcell line, which secretes low to undetectable amounts ofHMGB1 and that does not require HMGB1 to grow, wasused as a control.7
In vivo, ASA is rapidlymetabolized toSA; however, the kineticsof this conversion in cell culture have not been elucidated. Ourdata show that 1mM of ASA (the highest concentration used inour in vitro experiments) was completely hydrolyzed to SA in48 h, with 46% and 76% of ASA converted into SA after 8 and24 h, respectively (Supplementary Figure S2). REN cells treatedwith therapeutic levels of salicylates showed no significantdifference in viability compared with controls at 24 h(Supplementary Figure S3A) and 72 h (Supplementary FigureS3B), suggesting that ASA and SA are not directly cytotoxic.To determine whether anchorage-independent growth of
the HMGB1-secreting MM cell lines might be suppressed byASA/SA, MM cell lines were cultured in 6-well plates coatedwith soft agar for 4 weeks. Fresh medium supplemented with1% FBS and different doses of ASA/SA or vehicle was addedevery 2 days. Concentrations of ASA and SA as low as 100 μMsignificantly inhibited the formation of colonies in soft agar ofhigh HMGB1-secreting MM cells (Figures 2a–d), whereas noeffects were observed on the anchorage-independent growthof the low HMGB1-secreting MM cell line, PPM-Mill (Figures2e and f). These findings indicate that salicylates specificallysuppressed anchorage-independent growth of MM cells thatsecrete high amounts of HMGB1 and require HMGB1 for theirgrowth, supporting the hypothesis that ASA exerts antitumor/MM activity through interfering with HMGB1 functions.
Salicylates inhibit HMGB1-dependent cell motility, migra-tion, invasion and EMT signaling. To determine whetherASA inhibited HMGB1-dependent cell motility, migration andinvasion, REN cells were treated with 100 ng/ml of reducedHMGB1, the isoform of HMGB1 that has chemoattractantactivity,7,20 which induced cell motility, migration and Matrigelinvasion (Figures 3a–c). ASA and SA inhibited all HMGB1-induced effects at concentrations as low as 0.1 μM 48 hafter administration (Figures 3a–c). In contrast, HMGB1did not induce chemotactic migration of PPM-MILL cells(Supplementary Figure S4) and ASA/SA had no influence onPPM-MILL cells in any of the assays (Figures 2e and f). Torule out the effects may be due to changes in cells viability,we examined the effect of ASA and SA on HMGB1-inducedcell growth. We found that at 48 h, HMGB1-induced REN cellgrowth was only slightly increased and that ASA and SA didnot impact cell viability (Figure 3d). Therefore, the significantinhibitory effects of ASA and SA seen at 48 h on cellmigration, motility and invasion were not caused by changesin cell proliferation. However, at 72 h, HMGB1 inducedsignificant cell growth above background, an additionalmechanism by which HMGB1 promotes MM, and at thistime point, ASA/SA inhibited HMGB1-induced cell growth(Figure 3e). Similar results were obtained with other HMGB1-secreting MM cells (Supplementary Figure S5).To investigate whether ASA and SA influences epithelial–
mesenchymal transition (EMT) inMM cells induced by HMGB1,we analyzed the expression of N-cadherin and β-catenin inREN and PHI cells, upon treatment with ASA and SA in thepresence of HMGB1 (Figure 4 and Supplementary Figure S6).
As shown in Figure 4, we observed that HMGB1 increasedsignificantly the levels of both N-cadherin and β-catenin andthese effectswere inhibited byASA/SA, indicating that ASAandSA inhibited the expression of adhesion molecules and EMTsignaling induced by HMGB1. We also found that HMGB1induced p-AKTand that this activity was significantly reduced inthe presence of ASA (Supplementary Figure S7). Inhibition ofAKT activity may contribute to the overall inhibitory effect ofASA/SA on HMGB1-induced cell growth.Overall, these results, together with the data from the colony
formation assay (Figure 2), support the hypothesis that ASA/SA specifically act on high HMGB1-secreting MM cells. Thesedata demonstrate that at concentrations ranging from 0.1 μMto 1mM, which are the concentrations obtained in humanserum, following ingestion of therapeutic levels of aspirin,salicylates effectively suppress the chemoattractant activitiesof HMGB1 in HMGB1-secreting MM cells and suppress theMM malignant phenotype induced by HMGB1.
Effect of salicylates on HMGB1-induced cell migration isindependent of COX-2 and is not additive with theHMGB1 antagonist BoxA. Extracellular reduced HMGB1acts as a chemoattractant and mediates migration ofdifferent cell types, including mouse embryonic fibroblasts,mononuclear cells and ovarian cancer cells.21–23 Theprimary action of ASA in mammals has been attributedto its effects on cyclooxygenase enzymes (COX),13,14 andCOX-2 deficiency impairs cell adhesion and migration ofmacrophages.24 To test whether SA-mediated inhibition ofchemotaxis was mediated via COX-2 rather than HMGB1, weused mouse embryonic fibroblasts (MEFs) with ablation of thegene coding for COX-2 (Pgts2)25 and performed the cellmigration assay using both Ptgs2− /− MEFs and wild-type(WT) fibroblasts. Our data show that SA effectively inhibitedHMGB1-induced fibroblasts migration in a dose-dependentmanner, in both Ptgs2− /− MEFs and WT fibroblasts, with anIC50 of ~3–4 μM (Figures 5a and b). In contrast, SA did notaffect cell migration induced by the chemoattractant N-formyl-methionyl-leucyl-phenylalanine (fMLP) (Figures 5a and b).Thus, SA appears to inhibit specifically the chemoattractantactivity of HMGB1, rather than suppress cell migration per se.To further investigate whether the antichemoattractant effectsof salicylates on MM cells are through COX inhibition or not,we compared the effects of ASA to indomethacin, anonselective inhibitor of COX, and we found that ASA, butnot indomethacin, inhibited HMGB1-induced motility of MMcells (Supplementary Figure S8). In addition, we found thatASA and BoxA, a specific HMGB1 antagonist,26 did not havesynergic or additive effects, as it would have been expected ifthey acted through different pathways (Figure 5c). Takentogether, these data support the hypothesis that the anti-chemoattractant effect of ASA is largely mediated via HMGB1-dependent mechanisms and it is COX-2 independent.
Specific inhibition of HMGB1 significantly reduces tumorgrowth in vivo. Following the identification of a commonpathway of action of ASA/SA and BoxA, we tested theefficacy of BoxA in vivo. Twenty SCID mice were injectedintraperitoneally with 5 × 105 REN/luc cells. After formation oftumor nodules detectable by IVIS imaging (4 days after
Aspirin inhibits HMGB1-mediated tumor growthH Yang et al
4
Cell Death and Disease

injection of REN/luc cells), mice were weighed and randomlyassigned to control (PBS) and treatment (400 μg BoxAinjection) groups of 10 animals each. Mice were injectedintraperitoneally three times a week for a total of 10 weeks(12mg BoxA/mouse in the treatment group). Based on aslope comparison test, tumors in BoxA-treated mice grewsignificantly slower than controls (Figure 6a, t(146)= 4.8,Po0.0001), and these mice had a median survival of142 days, compared with 76.5 days median survival in the
control group in which the longest survival was 96 days(Figure 6b). Based on the log-rank test, this difference wasstatistically significant (χ2(1)=18.4, P o0.0001). One animalin the BoxA-treated group survived 413 days when eventuallyit became ill and had to be killed. Necropsy revealed that thismouse died of a CD3+ T-cell lymphoma (SupplementaryFigure S9), a tumor type that is frequent in SCID mice.Pathological and immunohistochemical studies revealed noevidence of residual human MM cells in this mouse.
Figure 2 Salicylates inhibit anchorage-independent colony formation of high HMGB1-secreting REN and HMESO cells but not of low HMGB1-secreting PPM-MILL cells. Fivethousand REN (a and b), HMESO (c and d) and PPM-MILL (e and f) cells were seeded on soft agar-coated plates. Fresh medium (DMEM plus 1% FBS) supplemented withdifferent concentrations of salicylates or vehicle control was added every 2 days for 4 weeks. Representative photographs of colonies (a, c and e) and quantification of number ofcolonies (b, d and f). Cells were treated with vehicle or salicylates. For each well, all colonies larger than 0.1 mm in diameter were counted using the ImageJ software (NIH). In allpanels, experiments were carried out in triplicate and repeated three times. *Po0.05
Aspirin inhibits HMGB1-mediated tumor growthH Yang et al
5
Cell Death and Disease

Discussion
We report that salicylates inhibit the activities of extracellularHMGB1 and that at least part of the anticancer effects ofaspirin are due to inhibition of HMGB1’s activities and areCOX-2 independent.The primarymechanism of action of aspirin in mammals has
been attributed to the disruption of eicosanoid biosynthesisthrough the irreversible inhibition via acetylation of COX,thereby altering the levels of prostaglandins.13,14 Aspirin’sprotective effect against cancer has therefore been associated
with the inhibition of COX. In supporting this, studies haveshown that: (i) other NSAIDs that, similar to aspirin, inhibitCOX activity, also reduce cancer risk, (ii) COX-2 is over-expressed in many tumors, and (iii) Ptgs2 (Cox-2)-null micehave much reduced number of precancerous colon polyps.27
In contrast, other studies challenge the hypothesis that COXinhibition is responsible for the anticancer effects of aspirinand other NSAIDs,28 because: (i) inhibition of cancer cellgrowth by NSAIDs cannot be reversed by addition ofprostaglandins, (ii) genetic suppression of Cox-1 and/or
Figure 3 Salicylates inhibit MM cell migration, cell motility and invasion induced by HMGB1. (a) Quantification of wound healing assay of REN cells in the presence of HMGB1(100 ng/ml) with or without different concentrations of ASA or SA after 48 h. The percentage of wound reduction was analyzed using the ImageJ software (NIH). Experiments werecarried out in triplicate. (b) Both ASA and SA inhibit HMGB1-induced MM cell migration. Quantification of REN cells migrating towards HMGB1 in the presence of differentconcentrations of ASA or SA. Bars represent mean values per field from three fields. (c) Both ASA and SA inhibit HMGB1-induced MM cell invasion. Quantification of Matrigelinvasion of REN cells in the presence of HMGB1 and different concentrations of ASA or SA. Bars represent mean values per field from three fields. (d and e) ASA and SA do notinhibit HMGB1-induced MM cell proliferation at 48 h (d), but significantly inhibit HMGB1-induced MM cell proliferation at 72 h (e). One thousand REN cells were treated withHMGB1 (100 ng/ml) in the presence or absence of different concentrations of ASA or SA. Cell metabolic activity was assessed by Alamar Blue assay after 48 and 72 h. Effects oftreatments were assessed by analysis of variance (ANOVA) with Bonferroni-corrected posttests. (Here we are comparing MM cells treated with HMGB1 in the presence orabsence of ASA/SA.) **Po0.01, ***Po0.001 and ****Po0.0001
Aspirin inhibits HMGB1-mediated tumor growthH Yang et al
6
Cell Death and Disease

Cox-2 expression often does not alter sensitivity to NSAIDs,and (iii) some derivatives, metabolites or enantiomers ofseveral NSAIDs retain anticancer activity despite having losttheir ability to inhibit COX-1/2. Taken together, these studiesargue that mechanism(s) independent of inhibition of the COXactivity of COX-1/2 are, at least partially, responsible for theanticancer activity of aspirin and other NSAIDs, a conclusionalso reached by others.29
In the present study, we examined whether aspirin and itsmetabolite, SA, exert anticancer activity against MM byinhibiting the biological effects of HMGB1 at physiologicallyrelevant concentrations. We found that ASA significantlyinhibited MM growth in a xenograft model, a result that wasreproduced using gavage feeding in two independent experi-ments. The mean survival of mice treated with 25 or 50mg/kgASA were significantly higher as compared with untreatedcontrol mice (Figure 1). Therapeutic levels of ASA and SAsuppressed the migration, invasion, wound healing, EMT
signaling and anchorage-independent colony formation ofHMGB1-secreting MM cells but not those of MM cells, whichsecrete low to undetectable amounts of HMGB1, suggestingthat the antitumor activity of ASA/SA was related to HMGB1(Figures 2-4). Moreover, SA inhibited HMGB1-induced cellmigration in MEFs in which the gene coding for COX-2 (Pgts2)had been genetically ablated indicating that this effect isCOX-2 independent (Figures 5a and b). These findingssupport the interpretation that the observed biological/antitumor effects were a direct consequence of SA-mediatedinhibition of HMGB1 activities.As aspirin, in addition to inhibiting HMGB1, has other
activities, we used BoxA, a specific HMGB1 antagonist26 todetermine whether specific inhibition of HMGB1 functionmimicked the effects of aspirin. We tested whetherHMGB1 inhibition alone was sufficient to account for theantichemoattractant activity and reduced tumor growth orwhether other aspirin activities were also required. In vitro, the
Figure 4 Salicylates inhibit N-cadherin and β-catenin expression induced by HMGB1. (a) Representative western blots show N-cadherin and β-catenin expression in RENMM cells treated with HMGB1 in the presence or absence of different concentrations of ASA or SA. (b and c) The expression of N-cadherin (b) and β-catenin (c) relative toglyceraldehyde 3-phosphate dehydrogenase (GAPDH) levels was evaluated as band density using the ImageJ software (NIH). #Significantly different compared with MM cells nottreated with HMGB1. *Significantly different compared with MM cells treated with HMGB1 in the absence of salicylates (Po0.05)
Aspirin inhibits HMGB1-mediated tumor growthH Yang et al
7
Cell Death and Disease
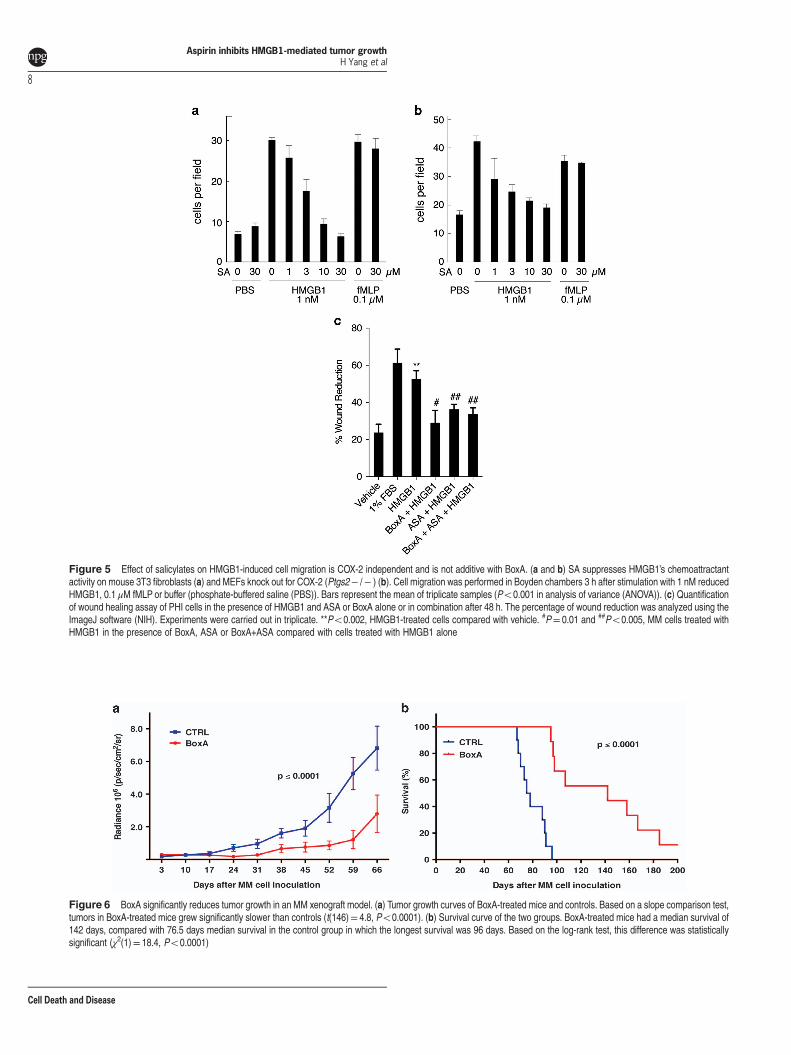
Figure 5 Effect of salicylates on HMGB1-induced cell migration is COX-2 independent and is not additive with BoxA. (a and b) SA suppresses HMGB1’s chemoattractantactivity on mouse 3T3 fibroblasts (a) and MEFs knock out for COX-2 (Ptgs2− /− ) (b). Cell migration was performed in Boyden chambers 3 h after stimulation with 1 nM reducedHMGB1, 0.1 μM fMLP or buffer (phosphate-buffered saline (PBS)). Bars represent the mean of triplicate samples (Po0.001 in analysis of variance (ANOVA)). (c) Quantificationof wound healing assay of PHI cells in the presence of HMGB1 and ASA or BoxA alone or in combination after 48 h. The percentage of wound reduction was analyzed using theImageJ software (NIH). Experiments were carried out in triplicate. **Po0.002, HMGB1-treated cells compared with vehicle. #P= 0.01 and ##Po0.005, MM cells treated withHMGB1 in the presence of BoxA, ASA or BoxA+ASA compared with cells treated with HMGB1 alone
Figure 6 BoxA significantly reduces tumor growth in an MM xenograft model. (a) Tumor growth curves of BoxA-treated mice and controls. Based on a slope comparison test,tumors in BoxA-treated mice grew significantly slower than controls (t(146)= 4.8, Po0.0001). (b) Survival curve of the two groups. BoxA-treated mice had a median survival of142 days, compared with 76.5 days median survival in the control group in which the longest survival was 96 days. Based on the log-rank test, this difference was statisticallysignificant (χ2(1)= 18.4, Po0.0001)
Aspirin inhibits HMGB1-mediated tumor growthH Yang et al
8
Cell Death and Disease

combination of ASA and BoxA did not increase their antic-hemoattractant activity (Figure 4c). The data are consistentwith the two agents being in the same pathway. In vivo, BoxAadministration produced similar antitumor effects as observedwith aspirin, without causing the well-known side effects ofaspirin, that is, GI bleeding. Median survival in control micewas 76.5 days and maximum survival was 96 days, whereasmedian survival of BoxA-treated mice was 142 days(Figures 6a and b). One of the BoxA-treated mice survived413 days. This mouse eventually died of a mouse T-celllymphoma and humanMMcells could no longer be detected init (Supplementary Figure S8). In summary, BoxA was moreeffective than ASA in suppressing MM growth and extendingsurvival, and mice treated with BoxA did not appear to sufferany side effects.Although BoxA is not yet available for clinical use, aspirin is.
The beneficial effects of aspirin and BoxA detected in ourstudy were observed treating animals during the early stagesof tumor growth. Our experiments were not designed toaddress the possible beneficial effects of aspirin and BoxA onsymptomatic MM with large tumor masses. Therefore, similarto what has been proposed for colon cancer,14 we proposethat in human MM the beneficial effects of aspirin and BoxAmay be better achieved during the early phases of tumorgrowth and/or in a preventive/early stage setting. Thus, aspirinadministration to individuals at high risk of developing MM,such as those with a history of asbestos and or erioniteexposure or germline BAP1 mutation carriers,1,2 may preventor delay the growth of MM, possibly increasing life expectancyand also increasing opportunities for early MM detection,which is associated with a prolonged life expectancy.1 In thisregard, promising newMM biomarkers are being developed toincrease opportunities for early MM detection in cohorts athigh risk for MM.3,30
Our data present a compelling argument that at least some ofthe so far elusive antitumor activity of aspirin is mediatedthrough inhibition of HMGB1 activity. Future studies shalladdress the precisemechanism bywhichASA inhibits HMGB1.In summary, we propose a novel mechanism by which aspirinmay exert its antitumorigenic properties (i.e., HMGB1 inhibition)while remaining consistent with its well-described anti-inflam-matory properties. Indeed, by identifying HMGB1 as a potentialtarget of salicylates in our experimental MM system, we providea proof-of-concept of a novel therapeutic mechanism that isresponsible for aspirin’s anticancer effects. Our results are ofrelevance to MM, and also to other inflammation-relatedmalignancies, such as melanoma, breast, GI, prostate, andpancreatic cancers, whose growth and development appearalso supported by high levels of HMGB1.7,8
Materials and MethodsStudy design. This study objective was to investigate the HMGB1-mediatedantitumorigenic effects of salicylates. To this aim, we designed in vitro and in vivoassays using high and low HMGB1-secreting MM cell lines, which exhibit differentHMGB1 dependence for cell growth. Sample selection for in vitro studies was based onavailability of high and low HMGB1-secreting MM cell lines. Sample numbers andexperimental replicates for each experiment are indicated in the figure legends. MMsample selection for our in vivo orthotopic xenograft mouse model was based on highHMGB1 secretion levels and on robust intraperitoneally grafting in SCID mice. Samplesize, randomization and in vivo study end points are described in the ‘Animal Studies’Section in the Materials and Methods.
Cell cultures and reagents. The MM cell lines PPM-MILL, PHI (originallydenominated as HP3; Pass et al.31), and HMESO were established from surgicallyresected human MM specimens and characterized for their mesothelial origin by Drs.Harvey Pass and John Minna at the National Cancer Institute (NCI, Bethesda, MD,USA).7 The MM cell line REN was provided by Dr. Steven Albelda (University ofPennsylvania, Philadelphia, PA, USA). This line was originally derived from an explantof an epithelial mesothelioma. MM cell line characterization is performed routinely inour lab by immunostaining using specific antibodies against mesothelial markers,including WT-1, calretinin and pancytokeratin. All MM cell lines routinely testednegative for mycoplasma contamination. All cell lines were cultured in Dulbecco'smodified Eagle's medium (DMEM; Gibco, Grand Island, NY, USA), supplemented with10% FBS at 37 °C in a 5% CO2 atmosphere. REN/luc cells expressing luciferasewere generated by our lab as described previously.7 MEFs were derived fromPtgs2− /− E16 mouse embryos: Ptgs2+/− mice were purchased from TaconicBiosciences (Germantown, NY, USA) and mated to obtain Ptgs2− /− embryos;embryos were genotyped.25 The 3T3 cells were purchased from ATCC (Manassas,VA, USA). Full-length, lipopolysaccharide-free purified reduced HMGB1 and BoxAwere obtained from HMGBiotech (Milan, Italy). ASA, SA and indomethacin werepurchased from Sigma-Aldrich (St. Louis, MO, USA) and were dissolved in ethanol.fMLP was obtained from Sigma-Aldrich. Salicylates ELISA Kit used for SAmeasurement was purchased from Neogen (Lansing, MI, USA). HMGB1 ELISA kitwas purchased from IBL International (Hamburg, Germany).
Cell viability assay. REN cells were plated in a 96-well plate (1 × 103 perwell), starved overnight and treated with HMGB1 (100 ng/ml) with or without variousconcentrations of ASA/SA. Cell viability was assessed using the Alamar Blue (AbDSerotec (Raleigh, NC, USA)) assay according to the manufacturer’s instructions 48and 72 h after treatment.
Motility assay. MM cells were grown in 6-well plates to 80–90% confluence inmedium supplemented with 10% FBS. The cell monolayer was then scratched witha P200 tip, serum-free medium supplemented with HMGB1 (100 ng/ml) anddifferent concentrations of ASA or SA (ranging from 0.1 μM to 1 mM) were added,and cells were allowed to close the wound for 48 h. Migration distance wasphotographed and measured at zero time and after 48 h using the ImageJ software(NIH, Bethesda, MD, USA).
Migration and invasion assays. The in vitro cell migration and invasionassays were carried out using Costar Transwell-permeable polycarbonate supports(8.0 μm pores) in 24-well plates (Corning Inc., New York, NY, USA). A total of1 × 105 MM cells were seeded in the insert in serum-free medium. For the invasionassays, the upper compartment of the support was coated with Matrigel (BD,San Jose, CA, USA). Experiments were performed in triplicate. MM cells wereseeded on the top compartment of a Boyden chamber. The lower chamber wasfilled with serum-free medium supplemented with HMGB1 (100 ng/ml) and with orwithout different concentrations of either ASA or SA (ranging from 0.1 μM to 1 mM),and cells were allowed to migrate or invade for either 3 (MEF and 3T3) or 48 h (MMcell lines). The invaded/migrated cells were quantified per field of view using theImageJ software (NIH) and statistically analyzed.
Western blotting. Total cell protein extracts were prepared using lysis buffer(Sigma-Aldrich). Fifty micrograms of protein were used for each sample. Theproteins were separated on a 10% polyacrylamide gel and transferred topolyvinylidene difluoride membranes (EMD Millipore, Darmstadt, Germany). Themembranes were blocked in Tris-buffered saline containing 0.05% Tween-20 (TBST)and 5% bovine serum albumin at 4 °C overnight before incubation with specificprimary and secondary antibodies. The antibodies used were N-cadherin, β-catenin(Santa Cruz Biotechnology, Dallas, TX, USA) and GAPDH (EMD Millipore). Therelative density of western blot bands was evaluated by ImageJ software (NIH).
Soft agar assay. MM cells were incubated with different concentrations of ASAor SA (ranging from 0.1 μM to 1 mM) and the anchorage-independent cellproliferation was assayed as described previously.7 Briefly, the cells (5 × 103) weremixed with an equal volume of 0.6% agar in DMEM 10% FBS and placed on top ofa 6-well plate precoated with 1.2% agar in DMEM plus 10% FBS. Cells wereincubated at 37 °C with 5% CO2 and fresh medium (DMEM plus 1% FBS)supplemented with different concentrations of ASA or SA (ranging from 0.1 μM to1 mM) was added every 2 days. After 4 weeks of culture, the number and size of the
Aspirin inhibits HMGB1-mediated tumor growthH Yang et al
9
Cell Death and Disease

colonies formed in each treatment were evaluated. For each well, all colonies largerthan 0.1 mm in diameter were counted using the ImageJ software.
Animal studies. SCID (NOD.CB17-SCID) female mice aged 6 to 8 weeks(Jackson Laboratories, Bar Harbor, ME) were housed and handled under asepticconditions, in accordance with the University of Hawaii’s Institutional Animal Care andUse Committee (IACUC) guidelines. An orthotopic mouse model of MM wasestablished by intraperitoneal injection of 5 × 105 REN/luc cells suspended in 500 μl ofPBS. Cells were visualized by luminescence after D-luciferin injection (150 mg/kg)using the In Vivo Imaging System (IVIS; Xenogen Corp., Alameda, CA, USA), withregions of interest quantified as total photon counts by Living Image software(Xenogen Corp.). Mice were then weighed and randomly assigned to control andtreatment groups. Treatments were ASA, BoxA or vehicle solutions. ASA was firstdissolved in dimethyl sulfoxide, and then diluted to 2.5 mg/ml with 0.5%carboxymethylcellulose sodium salt (Sigma-Aldrich).19 BoxA (400 μg) was diluted in200 μl of PBS. Control (vehicle) solutions were DMSO in 0.5% carboxymethylcelluloseor PBS for ASA and BoxA, respectively. ASA treatments were administrated via oralgavage, whereas BoxA was administered via intraperitoneal injection. Throughouttreatment, tumor dimension was measured every seventh day as average radiance(photons/s/cm2/sr) by IVIS. Primary end points were tumor size and survival. Theanimals were killed when declared 'ill' by the vivarium veterinary team (i.e., becauseof tumor masses 42 cm, dyspnea, ascites, lethargy, and so on). Animals werenecropsied and all abdominal organs were analyzed histologically. The cause ofdeath for all the mice used in the xenograft model was intestinal occlusion causedby tumor nodules, except for one mouse in the BoxA-treated group, which diedaccidently during a blood draw to measure HMGB1 serum levels. In the first ASAmouse experiment, 14 MM-xenotransplanted SCID mice were randomized into twogroups of seven animals each, receiving ASA 25 mg/kg or vehicle daily via oralgavage. Mice were treated for 48 days, and during the course of the experiment,ASA-treated animals experienced weight loss and died of GI bleeding. In thesecond ASA mouse experiment, 60 MM-xenografted SCID mice were randomizedinto three groups of 20 animals each. Treatment groups received ASA 25 or 50 mg/kg, daily for the first 2 weeks, and then three times a week thereafter. During thecourse of the experiment, there was no difference in body weight between thecontrol and treatment groups, and no evidence of GI bleeding. In the BoxA in vivoexperiment, 20 MM-xenografted SCID mice were randomized into two groups(control and treatment) of 10 animals each. Mice were treated intraperitoneal witheither 400 μg BoxA or vehicle (PBS) three times per week for 10 weeks (12 mg totalBoxA/mouse). There was no difference in body weight between the control andtreatment groups during the course of the experiment.
Immunohistochemistry. Immunohistochemistry was performed with anti-CD3 antibodies (Abcam, San Francisco, CA, USA; rabbit polyclonal). VectastainElite ABC Kit (rabbit IgG; Vector Labs, Burlingame, CA, USA) was used accordingto the manufacturer’s instructions. The staining was analyzed blindly by two board-certified pathologists (AP and MC).
Statistical analysis. Statistical analysis is described in the Result section andin the Figure legends. Unless otherwise specified, statistical differences wereevaluated by unpaired Student's t-test and considered significant at Po0.05.
Conflict of InterestThe University of Hawaii has filed for patents on HMGB1 and mesothelioma, on whichHY, MC, MEB, and HIP are inventors. MC provides consultation for mesotheliomaexpertise and diagnosis. MEB is founder and part owner of HMGBiotech.
Acknowledgements. We thank Dr. Shumin Zhang, Harvard School of PublicHealth, for information and discussion about the Physician's Health Study. We aregrateful to Drs. Marcus Tius, James Turkson, Joe Ramos and David C Ward forcritical reading of this manuscript and Simone Patergnani for technical advice. Thiswork was supported by the NCI-R01 CA160715, DOD CA120355 and The RivieraUnited 4-a Cure (to HY), and by NCI P01 CA114047 and NCI P30 CA071789 (to MC);by the V-Foundation (to MC and HY), by the University of Hawai’i Foundation, whichreceived donations to support mesothelioma research from Honeywell InternationalInc. (to MC); by Ricerca Finalizzata from the Italian Ministry of Health (to MEB) and bythe Associazione Italiana Ricerca sul Cancro (IG-10411 to MEB, IG-14442 to PP andMFAG-13521 to CG).
Author contributionsHYand MC designed and directed the study. LP, AN, CG, SJ, A Preti, CJJ, FDM, EGF,DL and MT performed experiments. IP performed statistical analysis. AP and MCperformed and reviewed pathology, histology and immunohistochemistry. HY, MC, SKand SP reviewed experimental results, performed data analysis and wrote themanuscript. MB, SK, GG, HIP, PP and SP critically reviewed the results. MEBdesigned and directed some of the experiments and contributed to the writing of themanuscript.
1. Carbone M, Ly BH, Dodson RF, Pagano I, Morris PT, Dogan UA, et al. Malignantmesothelioma: facts, myths, and hypotheses. J Cell Physiol 2012; 227: 44–58.
2. Carbone M, Yang H, Pass HI, Krausz T, Testa JR, Gaudino G. BAP1 and cancer. Nat RevCancer 2013; 13: 153–159.
3. Carbone M, Yang H. Molecular pathways: targeting mechanisms of asbestos and erionitecarcinogenesis in mesothelioma. Clin Cancer Res 2012; 18: 598–604.
4. Scaffidi P, Misteli T, Bianchi ME. Release of chromatin protein HMGB1 by necrotic cellstriggers inflammation. Nature 2002; 418: 191–195.
5. Yang H, Rivera Z, Jube S, Nasu M, Bertino P, Goparaju C, et al. Programmed necrosisinduced by asbestos in human mesothelial cells causes high-mobility group box 1 proteinrelease and resultant inflammation. Proc Natl Acad Sci USA 2010; 107: 12611–12616.
6. Gardella S, Andrei C, Ferrera D, Lotti LV, Torrisi MR, Bianchi ME et al. The nuclear proteinHMGB1 is secreted by monocytes via a non-classical, vesicle-mediated secretory pathway.EMBO Rep 2002; 3: 995–1001.
7. Jube S, Rivera ZS, Bianchi ME, Powers A, Wang E, Pagano I et al. Cancer cell secretion ofthe DAMP protein HMGB1 supports progression in malignant mesothelioma. Cancer Res2012; 72: 3290–3301.
8. Ellerman JE, Brown CK, de Vera M, Zeh HJ, Billiar T, Rubartelli A, et al. Masquerader: highmobility group box-1 and cancer. Clin Cancer Res 2007; 13: 2836–2848.
9. Bald T, Quast T, Landsberg J, Rogava M, Glodde N, Lopez-Ramos D et al.Ultraviolet-radiation-induced inflammation promotes angiotropism and metastasis inmelanoma. Nature 2014; 507: 109–113.
10. Tabata C, Kanemura S, Tabata R, Masachika E, Shibata E, Otsuki TI, et al. Serum HMGB1as a diagnostic marker for malignant peritoneal mesothelioma. J Clin Gastroenterol 2013; 47:684–688.
11. Chung HW, Lim JB, Jang S, Lee KJ, Park KH, Song SY. Serum high mobility group box-1 is apowerful diagnostic and prognostic biomarker for pancreatic ductal adenocarcinoma. CancerSci 2012; 103: 1714–1721.
12. Lee H, Song M, Shin N, Shin CH, Min BS, Kim HS et al. Diagnostic significance of serumHMGB1 in colorectal carcinomas. PLoS One 2012; 7: e34318.
13. Weissmann G. Aspirin. Scientific Am 1991; 264: 84–90.14. Ulrich CM, Bigler J, Potter JD. Non-steroidal anti-inflammatory drugs for cancer prevention:
promise, perils and pharmacogenetics. Nat Rev Cancer 2006; 6: 130–140.15. Rothwell PM, Wilson M, Price JF, Belch JF, Meade TW, Mehta Z. Effect of daily aspirin on
risk of cancer metastasis: a study of incident cancers during randomised controlled trials.Lancet 2012; 379: 1591–1601.
16. Benedek IH, Joshi AS, Pieniaszek HJ, King SY, Kornhauser DM. Variability in thepharmacokinetics and pharmacodynamics of low dose aspirin in healthy male volunteers.J Clin Pharmacol 1995; 35: 1181–1186.
17. Cerletti C, Bonati M, del Maschio A, Galletti F, Dejana E, Tognoni G et al. Plasma levels ofsalicylate and aspirin in healthy volunteers: relevance to drug interaction on platelet function.J Lab Clin Med 1984; 103: 869–877.
18. Steering Committee of the Physicians' Health Study Research Group. Final report on theaspirin component of the ongoing Physicians' Health Study. N Engl J Med 1989; 321:129–135.
19. Reuter BK, Zhang XJ, Miller MJ. Therapeutic utility of aspirin in the ApcMin/+ murine modelof colon carcinogenesis. BMC Cancer 2002; 2: 19.
20. Antoine DJ, Harris HE, Andersson U, Tracey KJ, Bianchi ME. A systematic nomenclature forthe redox states of high mobility group box (HMGB) proteins. Mol Med 2014; 20: 135–137.
21. Schiraldi M, Raucci A, Munoz LM, Livoti E, Celona B, Venereau E et al. HMGB1 promotesrecruitment of inflammatory cells to damaged tissues by forming a complex with CXCL12and signaling via CXCR4. J Exp Med 2012; 209: 551–563.
22. Venereau E, Casalgrandi M, Schiraldi M, Antoine DJ, Cattaneo A, De Marchis F et al.Mutually exclusive redox forms of HMGB1 promote cell recruitment or proinflammatorycytokine release. J Exp Med 2012; 209: 1519–1528.
23. Chen J, Liu X, Zhang J, Zhao Y. Targeting HMGB1 inhibits ovarian cancer growth andmetastasis by lentivirus-mediated RNA interference. J Cell Physiol 2012; 227: 3629–3638.
24. Diaz-Munoz MD, Osma-Garcia IC, Iniguez MA, Fresno M. Cyclooxygenase-2 deficiency inmacrophages leads to defective p110gamma PI3K signaling and impairs cell adhesion andmigration. J Immunol 2013; 191: 395–406.
25. Morham SG, Langenbach R, Loftin CD, Tiano HF, Vouloumanos N, Jennette JC et al.Prostaglandin synthase 2 gene disruption causes severe renal pathology in the mouse. Cell1995; 83: 473–482.
26. Yang H, Ochani M, Li J, Qiang X, Tanovic M, Harris HE et al. Reversing established sepsiswith antagonists of endogenous high-mobility group box 1. Proc Natl Acad Sci USA 2004;101: 296–301.
Aspirin inhibits HMGB1-mediated tumor growthH Yang et al
10
Cell Death and Disease

27. Brown JR, DuBois RN. COX-2: a molecular target for colorectal cancer prevention. J ClinOncol 2005; 23: 2840–2855.
28. Gurpinar E, Grizzle WE, Piazza GA. COX-independent mechanisms of cancerchemoprevention by anti-Inflammatory drugs. Front Oncol 2013; 3: 181.
29. Tinsley HN, Grizzle WE, Abadi A, Keeton A, Zhu B, Xi Y, et al. New NSAID targets and derivativesfor colorectal cancer chemoprevention. Recent Results Cancer Res 2013; 191: 105–120.
30. Carbone M, Ferris LK, Baumann F, Napolitano A, Lum CA, Flores EG, et al. BAP1 cancersyndrome: malignant mesothelioma, uveal and cutaneous melanoma, and MBAITs. J TranslMed 2012; 10: 179.
31. Pass HI, Stevens EJ, Oie H, Tsokos MG, Abati AD, Fetsch PA et al. Characteristics of ninenewly derived mesothelioma cell lines. Ann Thorac Surg 1995; 59: 835–844.
Cell Death and Disease is an open-access journalpublished by Nature Publishing Group. This work is
licensed under a Creative Commons Attribution 4.0 InternationalLicense. The images or other third party material in this article areincluded in the article’s Creative Commons license, unless indicatedotherwise in the credit line; if the material is not included under theCreative Commons license, users will need to obtain permission fromthe license holder to reproduce the material. To view a copy of thislicense, visit http://creativecommons.org/licenses/by/4.0/
Supplementary Information accompanies this paper on Cell Death and Disease website (http://www.nature.com/cddis)
Aspirin inhibits HMGB1-mediated tumor growthH Yang et al
11
Cell Death and Disease


















