A.SOLEIMANI MD A history of ischemic-type discomfort and the initial 12-lead ECG are the primary...
48
IN THE NAME OF GOD
-
Upload
johnathan-oneal -
Category
Documents
-
view
219 -
download
1
Transcript of A.SOLEIMANI MD A history of ischemic-type discomfort and the initial 12-lead ECG are the primary...

IN THE NAME OF GOD

APPROACH TO ACUTE STEMI IN THE EMERGENCY
DEPARTMENT
A.SOLEIMANI MD




A history of ischemic-type discomfort and the initial 12-lead ECG are the primary tools for screening patients with possible STEMI
Because the 12-lead ECG is at the center of the decision pathway it should be obtained promptly (≤10 minutes after hospital arrival) in patients with ischemic discomfort.
Prehospital 12-lead ECGs: early triage of patients with STEMI.
Because lethal arrhythmias can occur suddenly in patients with STEMI, all patients should have bedside monitoring of the ECG and intravenous access.

If the initial ECG reveals ST-segment elevation of 0.1 mV or greater in at least two contiguous leads or a new or presumably new left bundle branch block, the patient should be evaluated immediately for a reperfusion strategy.

In patients with a clinical history suggestive of STEMI and an initial nondiagnostic ECG (i.e., no ST-segment deviation or T wave inversion), serial tracings should be obtained during evaluation in the emergency department. Emergency department staff can seek the sudden development of ST-segment elevation by periodic visual inspection of the bedside electrocardiographic monitor

Treatments
Aspirin Analgesics Nitrate Beta blocker Oxygen Reperfusion therapy:
Thrombolytic Primary PCI

Aspirin
Aspirin is effective across the entire ACS spectrum and is part of the initial management strategy for patients with suspected STEMI. Because low doses take several days to
achieve a full antiplatelet effect, 162 to 325 mg should be administered at the first opportunity after initial medical contact.
To achieve therapeutic blood levels rapidly, the patient should chew the tablet to promote buccal absorption rather than absorption through the gastric mucosa

Control of Cardiac Pain
Initial management of patients with STEMI should target relief of pain and its associated heightened sympathetic activity.
Control of cardiac pain is achieved with a combination of analgesics (e.g.,morphine) and interventions to favorably improve the balance of myocardial oxygen supply and demand, including oxygen, nitrates, and in appropriately selected patients, beta blockers.

ANALGESICSa wide variety of analgesic agents—including meperidine, pentazocine, and morphine—have been used to treat the pain associated with STEMI, morphine remains the drug of choice, except in patients with well-documented morphine hypersensitivity.
Doses of 4 to 8 mg administered intravenously and doses of 2 to 8 mg repeated at intervals of 5 to 15 minutes have been recommended until the pain is relieved or side effects emerge—hypotension, depression of respiration, or severe vomiting.
Appropriate dosing of morphine sulfate will vary, depending on the patient’s age, body size, blood pressure, and heart rate.
Reduction of anxiety with successful analgesia diminishes the patient’s restlessness and the activity of the autonomic nervous system, with a consequent reduction in the heart’s metabolic demands.

Morphine Morphine has beneficial effects in patients with
pulmonary edema caused by peripheral arterial and venous dilation (particularly in those with excessive sympathoadrenal activity); it reduces the work of breathing and slows the heart rate secondary to combined withdrawal of sympathetic tone and augmentation of vagal tone.
Maintaining the patient in a supine position and elevating the lower extremities if blood pressure falls can minimize hypotension following the administration of nitroglycerin and morphine. Such positioning is undesirable in patients with pulmonary edema, but morphine rarely produces hypotension in these circumstances. Administration of atropine intravenously may be helpful in treating the excessive vagomimetic effects of morphine

NITRATES
Enhance coronary blood flow by coronary vasodilation and decrease ventricular preload by increasing venous capacitance, sublingual nitrates are indicated for most patients with an ACS At present, the only groups of patients with STEMI in whom sublingual nitroglycerin should not be given are those with suspected right ventricular infarction or marked hypotension (e.g., systolic pressure <90 mm Hg), especially if accompanied by bradycardia.

Nitrate Once hypotension is excluded, a sublingual TNG
should be administered and the patient observed for improvement in symptoms or change in hemodynamics. If an initial dose is well tolerated, further nitrates should be administered while monitoring vital signs. Even small doses can produce sudden hypotension and bradycardia, a reaction that can usually be reversed with intravenous atropine.
Long-acting oral nitrate preparations should be avoided in the early course of STEMI because of the frequently changing hemodynamic status of the patient.
In patients with a prolonged period of waxing and waning chest pain, intravenous nitroglycerin may help control the symptoms and correct the ischemia, but frequent monitoring of blood pressure is required.
BETA-ADRENERGIC BLOCKING AGENTS
These drugs aid in the relief of ischemic pain, reduce the need for analgesics in many patients, and reduce infarct size and life-threatening arrhythmias. Avoiding early intravenous blockade in
patients with Killip class II or greater is important, because of the risk of precipitating cardiogenic shock

protocol for use of BB(1) Exclude patients with heart failure, hypotension (SBP <90 mm Hg), bradycardia (HR <60 beats/min),or significant AV block. (2) Administer metoprolol in three 5-mg intravenous boluses. (3) Observe the patient for 2 to 5 minutes after each bolus, and if the HR falls below 60 beats/min or SBP falls below 100 mm Hg, do not administer any further drug. (4) If hemodynamic stability continues 15 minutes after the last intravenous dose, begin oral metoprolol tartrate, 25 to 50 mg every 6 hours for 2 to 3 days as tolerated, and then switch to 100 mg twice daily. Lower doses may be used in patients who have a partial decline in blood pressure with the initial dosing or who appear to be at higher risk (e.g., larger infarction) for the development of heart failure because of poor left ventricular performance. Infusion of an extremely short-acting beta blocker, such as esmolol, 50 to 250 mg/kg/min, may be useful in patients with relative contraindications to the administration of a beta blocker and in whom slowing of the heart rate is considered highly desirable
oxygen
augmentation of the fraction of oxygen in the inspired air does not elevate oxygen delivery significantly in patients who are not hypoxemic. Furthermore, it may increase systemic vascular resistance and arterial pressure and thereby lower cardiac output slightly.
arterial oxygen saturation can be estimated by pulse oximetry, and oxygen therapy can be omitted if the oximetric findings are normal. On the other hand, patients with STEMI and arterial hypoxemia should receive oxygen. In patients with severe pulmonary edema, endotracheal intubation and mechanical ventilation may be necessary to correct the hypoxemia and reduce the work of breathing.
Efforts to limit infarct size have been divided among several different (sometimes overlapping) approaches: (1) early reperfusion (2) reduction of myocardial energy
demands (3) manipulation of energy production
sources in the myocardium (4) prevention of reperfusion injury

reperfusion strategy
Critical factors that weigh into selection of a reperfusion strategy include the time elapsed since the onset of
symptoms the risk associated with STEMI the risk related to administering a
fibrinolytic the time required to initiate an
invasive strategy

Major components of the delay from the onset of ischemic symptoms to reperfusion include the following: (1) the time for the patient to recognize the
seriousness of the problem and seek medical attention
(2) prehospital evaluation, treatment, and transportation
(3) the time for diagnostic measures and initiation of treatment in the hospital (e.g.,“door-to-needle” time for patients receiving a fibrinolytic agent and “door-to-balloon” time for patients undergoing a catheter-based reperfusion strategy)
(4) the time from initiation of treatment to restoration of flow.






Reperfusion Therapy for Patients with STEMI
*Patients with cardiogenic shock or severe heart failure initially seen at a non–PCI-capable hospital should be transferred for cardiac catheterization and revascularization as soon as possible, irrespective of time delay from MI onset (Class I, LOE: B). †Angiography and revascularization should not be performed within the first 2 to 3 hours after administration of fibrinolytic therapy.

Regional Systems of STEMI Care, Reperfusion Therapy, and Time-to-Treatment Goals
Reperfusion therapy should be administered to all eligible patients with STEMI with symptom onset within the prior 12 hours.
Primary PCI is the recommended method of reperfusion when it can be performed in a timely fashion by experienced operators.
I IIaIIbIIIEMS transport directly to a PCI-capable hospital for primary PCI is the recommended triage strategy for patients with STEMI with an ideal FMC-to-device time system goal of 90 minutes or less.*
I IIaIIbIII
I IIaIIbIII
*The proposed time windows are system goals. For any individual patient, every effort should be made to provide reperfusion therapy as rapidly as possible.

Regional Systems of STEMI Care, Reperfusion Therapy, and Time-to-Treatment Goals
Immediate transfer to a PCI-capable hospital for primary PCI is the recommended triage strategy for patients with STEMI who initially arrive at or are transported to a non–PCI-capable hospital, with an FMC-to-device time system goal of 120 minutes or less.*
In the absence of contraindications, fibrinolytic therapy should be administered to patients with STEMI at non–PCI-capable hospitals when the anticipated FMC-to-device time at a PCI-capable hospital exceeds 120 minutes because of unavoidable delays.
I IIaIIbIII
*The proposed time windows are system goals. For any individual patient, every effort should be made to provide reperfusion therapy as rapidly as possible.
I IIaIIbIII

Regional Systems of STEMI Care, Reperfusion Therapy, and Time-to-Treatment Goals
When fibrinolytic therapy is indicated or chosen as the primary reperfusion strategy, it should be administered within 30 minutes of hospital arrival.*
Reperfusion therapy is reasonable for patients with STEMI and symptom onset within the prior 12 to 24 hours who have clinical and/or ECG evidence of ongoing ischemia. Primary PCI is the preferred strategy in this population.
*The proposed time windows are system goals. For any individual patient, every effort should be made to provide reperfusion therapy as rapidly as possible.
I IIaIIbIII
I IIaIIbIII

Reperfusion at a Non–PCI-Capable Hospital
Guideline for STEMI

Fibrinolytic Therapy When There Is an
Anticipated Delay to Performing Primary PCI Within 120 Minutes of
FMC
Reperfusion at a Non–PCI-Capable Hospital

Fibrinolytic Therapy When There Is an Anticipated Delay to Performing Primary PCI
Within 120 Minutes of FMC
In the absence of contraindications, fibrinolytic therapy should be given to patients with STEMI and onset of ischemic symptoms within the previous 12 hours when it is anticipated that primary PCI cannot be performed within 120 minutes of FMC.
In the absence of contraindications and when PCI is not available, fibrinolytic therapy is reasonable for patients with STEMI if there is clinical and/or ECG evidence of ongoing ischemia within 12 to 24 hours of symptom onset and a large area of myocardium at risk or hemodynamic instability.
Fibrinolytic therapy should not be administered to patients with ST depression except when a true posterior (inferobasal) MI is suspected or when associated with ST elevation in lead aVR.
I IIaIIbIII
I IIaIIbIII
I IIaIIbIII
Harm

Indications for Fibrinolytic Therapy When There Is a >120-Minute Delay From FMC to
Primary PCI


Adjunctive Antithrombotic Therapy
With Fibrinolysis
Reperfusion at a Non–PCI-Capable Hospital

Adjunctive Antiplatelet Therapy With Fibrinolysis
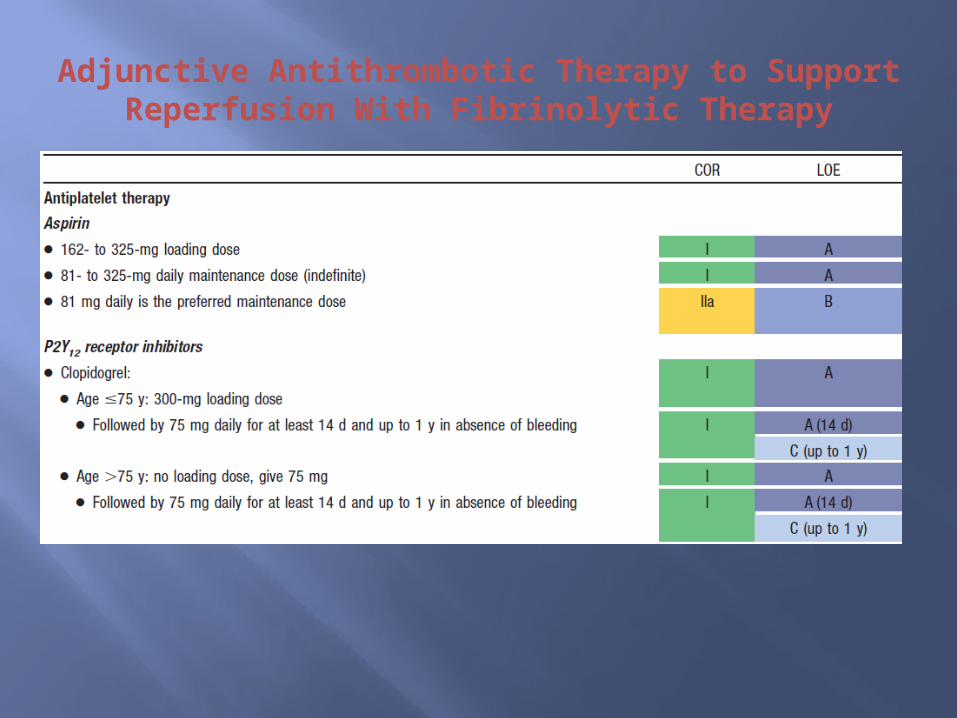
Aspirin (162- to 325-mg loading dose) and clopidogrel (300-mg loading dose for patients ≤75 years of age, 75-mg dose for patients >75 years of age) should be administered to patients with STEMI who receive fibrinolytic therapy.
I IIaIIbIII

Adjunctive Antiplatelet Therapy With Fibrinolysis
• aspirin should be continued indefinitely and
In patients with STEMI who receive fibrinolytic therapy: I IIaIIbIII
• clopidogrel (75 mg daily) for at least 14 days
o and up to 1 year I IIaIIbIII
I IIaIIbIII

Adjunctive Antiplatelet Therapy With Fibrinolysis
It is reasonable to use aspirin 81 mg per day in preference to higher maintenance doses after fibrinolytic therapy.
I IIaIIbIII
Adjunctive Antithrombotic Therapy to Support Reperfusion With Fibrinolytic Therapy

Adjunctive Antithrombotic Therapy to Support Reperfusion With Fibrinolytic Therapy (cont.)

Transfer to a PCI-Capable Hospital After Fibrinolytic Therapy
Reperfusion at a Non–PCI-Capable Hospital

Transfer of Patients With STEMI to a PCI-Capable Hospital for Coronary Angiography After Fibrinolytic
Therapy
Reperfusion at a Non–PCI-Capable Hospital

Transfer of Patients With STEMI to a PCI-Capable Hospital for Coronary Angiography
After Fibrinolytic Therapy
Immediate transfer to a PCI-capable hospital for coronary angiography is recommended for suitable patients with STEMI who develop cardiogenic shock or acute severe HF, irrespective of the time delay from MI onset.
Urgent transfer to a PCI-capable hospital for coronary angiography is reasonable for patients with STEMI who demonstrate evidence of failed reperfusion or reocclusion after fibrinolytic therapy.
I IIaIIbIII
I IIaIIbIII

Transfer of Patients With STEMI to a PCI-Capable Hospital for Coronary Angiography
After Fibrinolytic Therapy
Transfer to a PCI-capable hospital for coronary angiography is reasonable for patients with STEMI who have received fibrinolytic therapy even when hemodynamically stable* and with clinical evidence of successful reperfusion. Angiography can be performed as soon as logistically feasible at the receiving hospital, and ideally within 24 hours, but should not be performed within the first 2 to 3 hours after administration of fibrinolytic therapy.
I IIaIIbIII
*Although individual circumstances will vary, clinical stability is defined by the absence of low output, hypotension, persistent tachycardia, apparent shock, high-grade ventricular or symptomatic supraventricular tachyarrhythmias, and spontaneous recurrent ischemia.

Indications for Transfer for Angiography After Fibrinolytic Therapy
*Although individual circumstances will vary, clinical stability is defined by theabsence of low output, hypotension, persistent tachycardia, apparent shock, high-grade ventricular or symptomatic supraventricular tachyarrhythmias, and spontaneous recurrent ischemia.


THANKS FOR YOUR ATTENTION