
Askin (PNET) Tumor Unmasked by Trauma in a Young Male Patient
4
Journal of The Association of Physicians of India ■ Vol. 64 ■ March 2016 82 Askin (PNET) Tumor Unmasked by Trauma in a Young Male Patient Avas Chandra Ray 1 , Subhra Aditya 2 , Pulak Kumar Jana 3 , Apratim Chatterjee 4 , Anup Sarkar 4 , Jay Mehta 5 , Jotideb Mukhopadhyay 6 Abstract A young male labourer developed pain at the site of blunt trauma over back of chest followed by fever, cough with expectoration, breathlessness and hemorrhagic pleural effusion in the side of injury. What could have been passed as a sequel of trauma turned out to be the consequences of an underlying rare and aggressive malignant tumor of the chest wall known as Askin tumor or Primitive Neuroectodermal Tumor (PNET). CT thorax with guided FNAC, debulking operation, histopathological examination followed by immunohistochemistry of the tumor tissue led to the final diagnosis. Chemotherapy was administered following surgical resection. The patient died within nine months after diagnosis. 1 Associate Professor, 2 Assistant Professor, 4 PGT, 6 Professor and Head, Dept. of Medicine, 3 Associate Professor, Dept. of Chest Medicine, IPGME and R, Kolkata, West Bengal; 5 Consultant Pathologist, Centre of Excellence: Histopathology, Mumbai, Maharashtra Received: 08.10.2014; Accepted: 07.11.2014 Introduction A skin and his associates 1 described a rare and aggressive malignant tumor arising from the soft tissues of the chest wall, ribs, thoracic cavity and rarely from the periphery of the lungs. This tumor later on was recognized as Primitive Neuroectodermal Tumor (PNET). PNETs most frequently occur in children and young adults. Though no age is spared, PNETs in adults is exceedingly uncommon. Beside thoraco-pulmonary region, pelvis and lower extremities are the commonest site of involvement. PNET when localizeed to the thoracopulmonary region was defined as Askin tumor. Case Report A 20 years old, male construction worker sustained trauma over back of left side of chest with a blunt metal plate while working. He continued his usual daily activities till a dull aching pain over the site of injury compelled him to take bed rest three days after the incident. The pain was aggravating with deep inspiration, change of posture and while turning on bed. Seven days later he developed fever, cough and breathlessness. The cough evolved to produce yellowish expectoration but with no tinge of blood. Though he was experiencing exertional breathlessness with activities for last 2 to 3 months. This time he was having breathlessness even at rest. Chest X-ray (Figure 1A) followed by CT thorax were done outside on the same day and an intercostals tube was inserted in the left side of the chest. The patient was shifted next day to our hospital. He had in situ intercostals tube draining hemorrhagic fluid. The patient was not a known hypertensive, diabetic, alcoholic or smoker. He had no h/o tuberculosis nor any major illness in the past. His only brother was a physically handicapped; both parents were apparently of normal health. On general examination, pulse-104/ min, BP-130/80 mm of Hg, resp-30/min and temp. was 102 o F. Resp. System examinations revealed diminished movement of left side of chest with trachea shifted to right, dull percussion note, diminished vesicular breath sound and diminished vocal resonance over the whole left hemithorax except part of mammary, axillary and lower interscapular region. Other systemic examinations revealed no abnormalities. Routine laboratory work ups done before and after his admission were normal. X-ray chest done after admission (Figure 1B and C) apparently showed homogenous shadow obliterating the A B C Fig. 1: X-ray chest PA and lateral view
Transcript of Askin (PNET) Tumor Unmasked by Trauma in a Young Male Patient
Journal of The Association of Physicians of India ■ Vol. 64 ■ March 201682
Askin (PNET) Tumor Unmasked by Trauma in a Young Male PatientAvas Chandra Ray1, Subhra Aditya2, Pulak Kumar Jana3, Apratim Chatterjee4, Anup Sarkar4, Jay Mehta5, Jotideb Mukhopadhyay6
AbstractA young male labourer developed pain at the site of blunt trauma over back of chest followed by fever, cough with expectoration, breathlessness and hemorrhagic pleural effusion in the side of injury. What could have been passed as a sequel of trauma turned out to be the consequences of an underlying rare and aggressive malignant tumor of the chest wall known as Askin tumor or Primitive Neuroectodermal Tumor (PNET). CT thorax with guided FNAC, debulking operation, histopathological examination followed by immunohistochemistry of the tumor tissue led to the final diagnosis. Chemotherapy was administered following surgical resection. The patient died within nine months after diagnosis.
1Associate Professor, 2Assistant Professor, 4PGT, 6Professor and Head, Dept. of Medicine, 3Associate Professor, Dept. of Chest Medicine, IPGME and R, Kolkata, West Bengal; 5Consultant Pathologist, Centre of Excellence: Histopathology, Mumbai, MaharashtraReceived: 08.10.2014; Accepted: 07.11.2014
Introduction
Askin and his associates1 described a rare and aggressive malignant
tumor arising from the soft tissues of the chest wall, ribs, thoracic cavity and rarely from the periphery of the lungs. This tumor later on was recognized as Primitive Neuroectodermal Tumor (PNET). PNETs most frequently occur in children and young adults. Though no age is spared, PNETs in adults is exceedingly uncommon. Beside thoraco-pulmonary region, pelvis and lower extremities are the commonest s i te o f involvement . PNET when localizeed to the thoracopulmonary region was defined as Askin tumor.
Case Report
A 20 years old, male construction worker sustained trauma over back of left side of chest with a blunt metal plate while working. He continued his usual daily activities till a dull aching pain over the site of injury compelled him to take bed rest three days after the incident. The pain was aggravating with deep inspiration, change of posture and while turning on bed. Seven days later he developed fever, cough and breathlessness. The cough evolved to produce yellowish expectoration but with no tinge of blood. Though he was experiencing exertional breathlessness with activities for last 2 to 3 months. This time he was
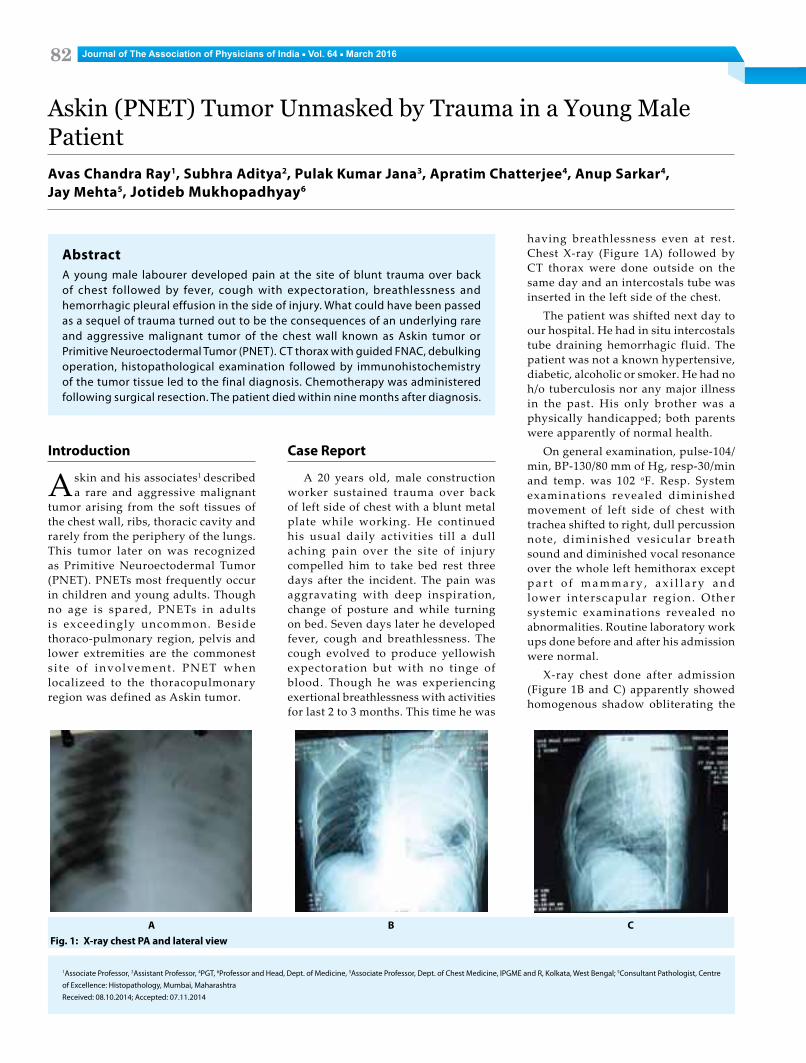
having breathlessness even at rest. Chest X-ray (Figure 1A) followed by CT thorax were done outside on the same day and an intercostals tube was inserted in the left side of the chest.
The patient was shifted next day to our hospital. He had in situ intercostals tube draining hemorrhagic fluid. The patient was not a known hypertensive, diabetic, alcoholic or smoker. He had no h/o tuberculosis nor any major illness in the past. His only brother was a physically handicapped; both parents were apparently of normal health.
On general examination, pulse-104/min, BP-130/80 mm of Hg, resp-30/min and temp. was 102 oF. Resp. System examinations revealed diminished movement of left side of chest with trachea shifted to right, dull percussion note, diminished vesicular breath sound and diminished vocal resonance over the whole left hemithorax except p a r t o f m a m m a r y , a x i l l a r y a n d lower interscapular region. Other systemic examinations revealed no abnormalities. Routine laboratory work ups done before and after his admission were normal.
X-ray chest done after admission (Figure 1B and C) apparently showed homogenous shadow obliterating the
A B CFig. 1: X-ray chest PA and lateral view
Journal of The Association of Physicians of India ■ Vol. 64 ■ March 2016 83
left costophrenic angle had decreased and the rounded shadow occupying upper and mid zone had increased in extent when compared with that done outside (Figure 1A).
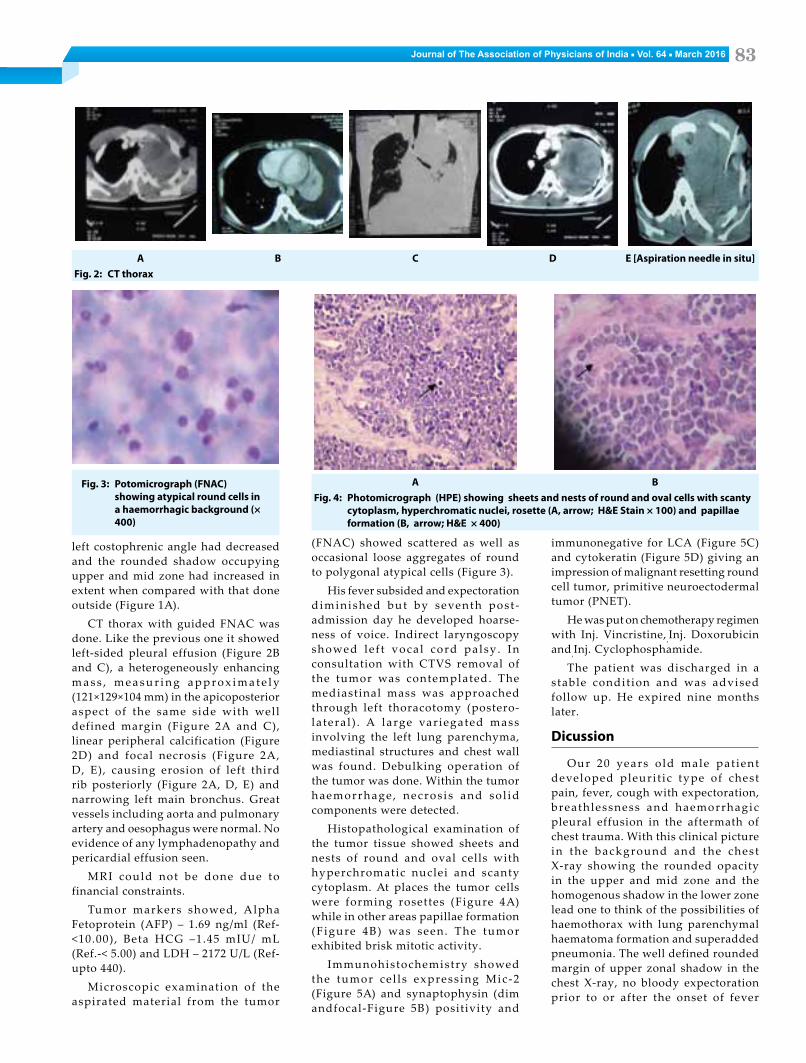
CT thorax with guided FNAC was done. Like the previous one it showed left-sided pleural effusion (Figure 2B and C), a heterogeneously enhancing m a s s , m e a s u r i n g a p p r o x i m a t e l y (121×129×104 mm) in the apicoposterior aspect of the same side with well defined margin (Figure 2A and C), linear peripheral calcification (Figure 2D) and focal necrosis (Figure 2A, D, E), causing erosion of left third rib posteriorly (Figure 2A, D, E) and narrowing left main bronchus. Great vessels including aorta and pulmonary artery and oesophagus were normal. No evidence of any lymphadenopathy and pericardial effusion seen.
MRI could not be done due to financial constraints.
Tumor markers showed, Alpha Fetoprotein (AFP) – 1.69 ng/ml (Ref-<10.00), Beta HCG –1.45 mIU/ mL (Ref.-< 5.00) and LDH – 2172 U/L (Ref- upto 440).
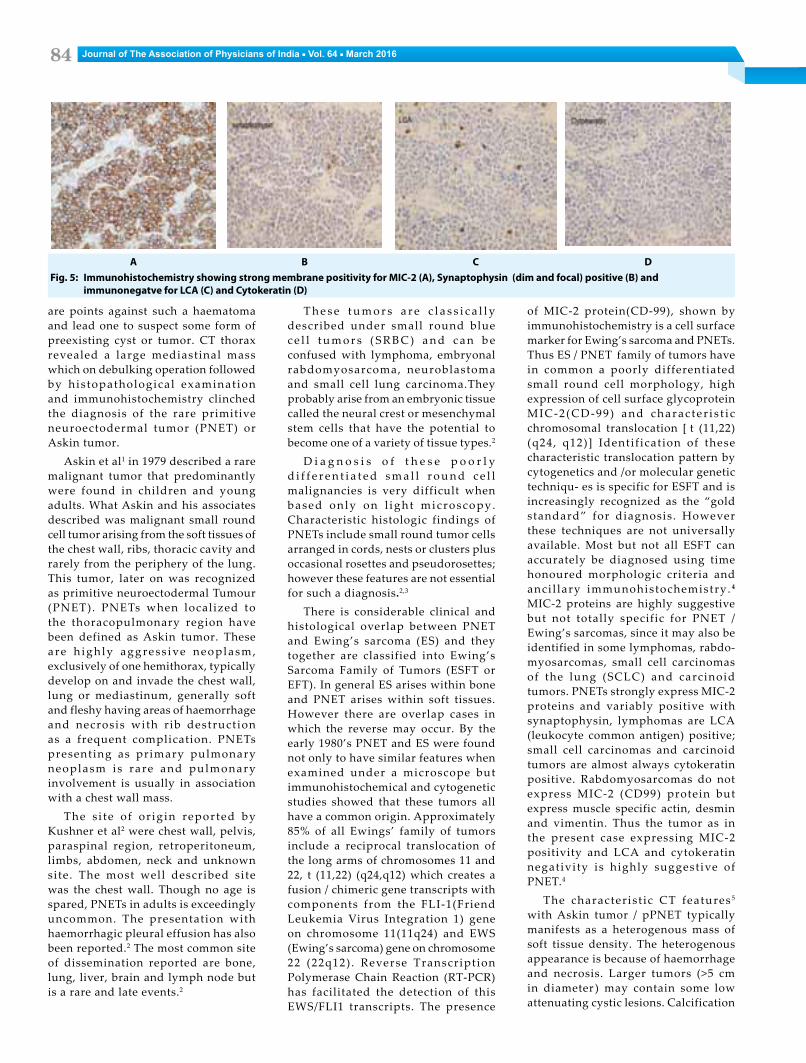
Microscopic examination of the aspirated material from the tumor
(FNAC) showed scattered as well as occasional loose aggregates of round to polygonal atypical cells (Figure 3).
His fever subsided and expectoration diminished but by seventh post -admission day he developed hoarse- ness of voice. Indirect laryngoscopy showed le f t vocal cord palsy . In consultation with CTVS removal of the tumor was contemplated. The mediastinal mass was approached through left thoracotomy (postero-lateral ) . A large var iegated mass involving the left lung parenchyma, mediastinal structures and chest wall was found. Debulking operation of the tumor was done. Within the tumor haemorrhage , necros is and so l id components were detected.
Histopathological examination of the tumor tissue showed sheets and nests of round and oval cells with hyperchromatic nuclei and scanty cytoplasm. At places the tumor cells were forming rosettes (Figure 4A) while in other areas papillae formation (Figure 4B) was seen. The tumor exhibited brisk mitotic activity.
Immunohistochemistry showed the tumor ce l ls express ing Mic-2 (Figure 5A) and synaptophysin (dim andfocal-Figure 5B) positivity and
immunonegative for LCA (Figure 5C) and cytokeratin (Figure 5D) giving an impression of malignant resetting round cell tumor, primitive neuroectodermal tumor (PNET).
He was put on chemotherapy regimen with Inj. Vincristine,,Inj. Doxorubicin and,Inj. Cyclophosphamide.
The patient was discharged in a stable condit ion and was advised follow up. He expired nine months later.
Dicussion
Our 20 years o ld male pat ient developed pleuri t ic type of chest pain, fever, cough with expectoration, breathlessness and haemorrhagic pleural effusion in the aftermath of chest trauma. With this clinical picture in the background and the chest X-ray showing the rounded opacity in the upper and mid zone and the homogenous shadow in the lower zone lead one to think of the possibilities of haemothorax with lung parenchymal haematoma formation and superadded pneumonia. The well defined rounded margin of upper zonal shadow in the chest X-ray, no bloody expectoration prior to or after the onset of fever
Fig. 3: Potomicrograph (FNAC) showing atypical round cells in a haemorrhagic background (× 400)
A B C D E [Aspiration needle in situ]Fig. 2: CT thorax
A BFig. 4: Photomicrograph (HPE) showing sheets and nests of round and oval cells with scanty
cytoplasm, hyperchromatic nuclei, rosette (A, arrow; H&E Stain × 100) and papillae formation (B, arrow; H&E × 400)
Journal of The Association of Physicians of India ■ Vol. 64 ■ March 201684
A B C DFig. 5: Immunohistochemistry showing strong membrane positivity for MIC-2 (A), Synaptophysin (dim and focal) positive (B) and
immunonegatve for LCA (C) and Cytokeratin (D)
are points against such a haematoma and lead one to suspect some form of preexisting cyst or tumor. CT thorax revealed a large mediastinal mass which on debulking operation followed by histopathological examinat ion and immunohistochemistry clinched the diagnosis of the rare primitive neuroectodermal tumor (PNET) or Askin tumor.
Askin et al1 in 1979 described a rare malignant tumor that predominantly were found in children and young adults. What Askin and his associates described was malignant small round cell tumor arising from the soft tissues of the chest wall, ribs, thoracic cavity and rarely from the periphery of the lung. This tumor, later on was recognized as primitive neuroectodermal Tumour (PNET). PNETs when localized to the thoracopulmonary region have been defined as Askin tumor. These are h igh ly aggress ive neoplasm, exclusively of one hemithorax, typically develop on and invade the chest wall, lung or mediastinum, generally soft and fleshy having areas of haemorrhage and necrosis with r ib destruction as a frequent complication. PNETs presenting as primary pulmonary neoplasm is rare and pulmonary involvement is usually in association with a chest wall mass.
The s i te of or ig in reported by Kushner et al2 were chest wall, pelvis, paraspinal region, retroperitoneum, limbs, abdomen, neck and unknown site. The most well described site was the chest wall. Though no age is spared, PNETs in adults is exceedingly uncommon. The presentation with haemorrhagic pleural effusion has also been reported.2 The most common site of dissemination reported are bone, lung, liver, brain and lymph node but is a rare and late events.2
T h e s e t u m o r s a r e c l a s s i c a l l y described under small round blue c e l l t u m o r s ( S R B C ) a n d c a n b e confused with lymphoma, embryonal rabdomyosarcoma, neuroblastoma and small cell lung carcinoma.They probably arise from an embryonic tissue called the neural crest or mesenchymal stem cells that have the potential to become one of a variety of tissue types.2
D i a g n o s i s o f t h e s e p o o r l y d i f f e r e n t i a t e d s m a l l r o u n d c e l l malignancies is very difficult when based only on l ight microscopy . Characteristic histologic findings of PNETs include small round tumor cells arranged in cords, nests or clusters plus occasional rosettes and pseudorosettes; however these features are not essential for such a diagnosis.2,3
There is considerable clinical and histological overlap between PNET and Ewing’s sarcoma (ES) and they together are classified into Ewing’s Sarcoma Family of Tumors (ESFT or EFT). In general ES arises within bone and PNET arises within soft tissues. However there are overlap cases in which the reverse may occur. By the early 1980’s PNET and ES were found not only to have similar features when examined under a microscope but immunohistochemical and cytogenetic studies showed that these tumors all have a common origin. Approximately 85% of all Ewings’ family of tumors include a reciprocal translocation of the long arms of chromosomes 11 and 22, t (11,22) (q24,q12) which creates a fusion / chimeric gene transcripts with components from the FLI-1(Friend Leukemia Virus Integration 1) gene on chromosome 11(11q24) and EWS (Ewing’s sarcoma) gene on chromosome 22 (22q12) . Reverse Transcription Polymerase Chain Reaction (RT-PCR) has facilitated the detection of this EWS/FLI1 transcripts. The presence
of MIC-2 protein(CD-99), shown by immunohistochemistry is a cell surface marker for Ewing’s sarcoma and PNETs. Thus ES / PNET family of tumors have in common a poorly differentiated small round cell morphology, high expression of cell surface glycoprotein MIC-2 (CD-99) and charac ter i s t i c chromosomal translocation [ t (11,22) (q24, q12)] Identif ication of these characteristic translocation pattern by cytogenetics and /or molecular genetic techniqu- es is specific for ESFT and is increasingly recognized as the “gold standard” for diagnosis. However these techniques are not universally available. Most but not all ESFT can accurately be diagnosed using time honoured morphologic criteria and anci l lary immunohistochemistry. 4 MIC-2 proteins are highly suggestive but not totally specific for PNET / Ewing’s sarcomas, since it may also be identified in some lymphomas, rabdo-myosarcomas, small cell carcinomas of the lung (SCLC) and carcinoid tumors. PNETs strongly express MIC-2 proteins and variably positive with synaptophysin, lymphomas are LCA (leukocyte common antigen) positive; small cell carcinomas and carcinoid tumors are almost always cytokeratin positive. Rabdomyosarcomas do not express MIC-2 (CD99) protein but express muscle specific actin, desmin and vimentin. Thus the tumor as in the present case expressing MIC-2 positivity and LCA and cytokeratin negativity is highly suggestive of PNET.4
The characterist ic CT features 5 with Askin tumor / pPNET typically manifests as a heterogenous mass of soft tissue density. The heterogenous appearance is because of haemorrhage and necrosis. Larger tumors (>5 cm in diameter ) may contain some low attenuating cystic lesions. Calcification

Journal of The Association of Physicians of India ■ Vol. 64 ■ March 2016 85
of the mass is rare. Rib destruction is common in chest wall tumors. On enhanced CT uniform or heterogeneous enhancement of the lesions are seen. Most tumors tend to displace rather than encase adjacent mediastinal structures such as vessels, the trachea and bronchi. A regional lymphadenopathy is rarely seen at diagnosis.
Neoadjuvent chemotherapy (therapy given before a tumor is removed) followed by surgical resection followed by post operative chemotherapy with or without radiotherapy (3500 to 5500 Rads) is the most accepted protocol. Surgery, based on the preoperative clinical and radiographic staging may be the treatment strategy of choice, both for confirming the diagnosis and for preventing invasion to other tissues that
might be fatal. Vincristine, doxorubicin, cyclophosphamide, ifosfamide and etoposide are the chemotherapeutic agents now most commonly used. If surgical removal is incomplete or is not possible and patient having local or distant spread radiotherapy is given with chemotherapy with or without surgery.6
PNETs have very high rate of local recurrence once resected. Topotecan or irinotecan in combination with an alkylating agent are often used in relapsed patients. Survival remains poor with a 2 year survival of 28% to 38% and a 6 year survival of 14% to 17%. Poor prognostic factors include metastases at diagnosis, incomplete resection of the mass and local or distant recurrences after surgery.3
References1. Askin FB, Rosai J, Sibley RK, Dehner LP, Mc Alister WH.
Malignant small cell tumor of the thoracopulmonary region in childhood. Cancer 1979; 43:2438-51.
2. Kushner BH, Hajdu SI, Gulati SC, et al. Extracranial Primitive Neuroectodermal Tumors; The Memorial Sloan Kettering Cancer Center Experience. Cancer 1991;67: 1825-1829.
3. Jurgens H, Bier V, Harms D, et al. Malignant peripheral neuroectodermal tumors – a retrospective analysis of 42 patients. Cancer 1988; 61:349-57.
4. Hashimoto H, Enjoji M, Nakajima T, Kiryn H, Daimaru Y. Malignant neuroepithelioma (peripheral neuroblastoma) : A clinocopathological study of 15 cases. Am J Surg Path 1983; 7:309-314.
5. Ibarburen C, Haberman JJ, Zerhouni EA. Peripheral primitive neuroectodermal tumors: CT and MRI evaluation. Eur J Radiol 1996; 21:225–232.
6. Christianansen S, Semik M, Dockhorn-Dworniczak B, et al. Diagnosis, treatment and outcome of patients with Askin tumors. Thorac Cardiov Surg 2000; 48:311-5.








![Vaticanism Unmasked [1878]](https://static.fdocuments.in/doc/165x107/577cd0ed1a28ab9e7893488a/vaticanism-unmasked-1878.jpg)









