Ascension Phenomenon of Anterior Vitreous
2
1028 CORRESPONDENCE Experimentally the best results have come from injecting plasmin directly into the thrombus, which could be either dissolved or made sufficiently mobile to be "milked" into a position accessible to direct removal. Some four years ago Cliffton 1 reported on the use of plasmin in 40 patients. It was clear that the side-effects were substantial but that the method was not unpromising, though in each of two cases of thrombosis of the cen- tral retinal vein no substantial improvement resulted from this treatment. Subsequent re- ports on the use of plasmin in thrombosis of the central retinal veins have been few and inconclusive ; but Howden 2 reported a grati- fying response in a patient with thrombosis of two days' standing, and now Hecker and Zweng 3 have recorded improvement in a man with occlusion of the central retinal artery— recovery occurring after other methods had been tried unsuccessfully for three days. In contrast, they report in an addendum that in two further such cases, treated within 24 and 72 hours of the onset of symptoms, no bene- fit ensued ; but they record another success- ful outcome in a patient in whom both in- ferior branches of the central retinal artery were partly occluded. Occlusion of the central retinal artery has probably an even more complex pathology than thrombosis of the central vein. Arterial occlusion is sometimes due entirely to spasm, without any thrombotic changes. There are therefore considerable difficulties in any criti- cal assessment of a new remedy. Neverthe- less such an assessment should be attempted with plasmin. REFERENCES 1. Cliffton, E. E.: Ann. N. Y. Acad. Sei., 68: 209, 1957. 2. Howden, G. D.: Canad. M.A.J., 81:382, 1959. 3. Hecker, S. P., and Zweng, H. C: J.A.M.A., 176:1067, 1961. CORRESPONDENCE ASCENSION PHENOMENON OF ANTERIOR VITREOUS Editor, American Journal of Ophthalmology: In the January, 1962, issue of THE JOUR- NAL, Dr. Emanuel Rosen published an article concerning a study of the "Ascension Phe- nomenon," in the vitreous body, that I de- scribed in 1953 (Ophthalmologica: 126:355- 360). He begins by telling us that this phe- nomenon had been observed by Vogt, Mann and Kirby and he speaks of movements of the membrane plicata (Vogt) and other lu- minous bands, movements well observed in the normal vitreous bodies, that produced changing of position and pattern of the an- terior portion of Cloquet's canal. There is a misunderstanding by all about this phenom- enon. In my articles of biomicroscopy of the vitreous body, I said this humor is composed of luminous substances immersed in a dark substance (optically empty) ; I also said that the luminous substance has a specific weight, greater than the darker. For this reason it always goes down to the bottom of the eyeball (by force of gravity). The luminous sub- stance always takes, in the same eye, the same aspect or pattern under conditions of rest. It is true, as Dr. Rosen says, that these are facts already well known (more or less in their details) but by studying the normal, I had been able to describe a new pathologic phenomenon which I had called "ascension phenomenon" or better still "climbing of the luminous bands." Under pathologic conditions (sometimes during inflammatory conditions of the ocu- lar coats, or in the presence of hemorrhages into the vitreous body), after the eye makes sudden movements and turns quiet, these bands of luminous substances go upward and stay there instead of going down by ac- tion of gravity. Then we see the inversion of the anterior portion of Cloquet's canal. The funnel is now directed downward and
Transcript of Ascension Phenomenon of Anterior Vitreous

1028 CORRESPONDENCE
Experimentally the best results have come from injecting plasmin directly into the thrombus, which could be either dissolved or made sufficiently mobile to be "milked" into a position accessible to direct removal.
Some four years ago Cliffton1 reported on the use of plasmin in 40 patients. It was clear that the side-effects were substantial but that the method was not unpromising, though in each of two cases of thrombosis of the central retinal vein no substantial improvement resulted from this treatment. Subsequent reports on the use of plasmin in thrombosis of the central retinal veins have been few and inconclusive ; but Howden2 reported a gratifying response in a patient with thrombosis of two days' standing, and now Hecker and Zweng3 have recorded improvement in a man with occlusion of the central retinal artery— recovery occurring after other methods had been tried unsuccessfully for three days. In contrast, they report in an addendum that in two further such cases, treated within 24 and 72 hours of the onset of symptoms, no benefit ensued ; but they record another successful outcome in a patient in whom both inferior branches of the central retinal artery were partly occluded.
Occlusion of the central retinal artery has probably an even more complex pathology than thrombosis of the central vein. Arterial occlusion is sometimes due entirely to spasm, without any thrombotic changes. There are therefore considerable difficulties in any critical assessment of a new remedy. Nevertheless such an assessment should be attempted with plasmin.
REFERENCES
1. Cliffton, E. E.: Ann. N. Y. Acad. Sei., 68: 209, 1957.
2. Howden, G. D.: Canad. M.A.J., 81:382, 1959. 3. Hecker, S. P., and Zweng, H. C : J.A.M.A.,
176:1067, 1961.
CORRESPONDENCE
ASCENSION PHENOMENON OF ANTERIOR VITREOUS
Editor, American Journal of Ophthalmology:
In the January, 1962, issue of T H E JOURNAL, Dr. Emanuel Rosen published an article concerning a study of the "Ascension Phenomenon," in the vitreous body, that I described in 1953 (Ophthalmologica: 126:355-360). He begins by telling us that this phenomenon had been observed by Vogt, Mann and Kirby and he speaks of movements of the membrane plicata (Vogt) and other luminous bands, movements well observed in the normal vitreous bodies, that produced changing of position and pattern of the anterior portion of Cloquet's canal. There is a misunderstanding by all about this phenomenon. In my articles of biomicroscopy of the vitreous body, I said this humor is composed of luminous substances immersed in a dark substance (optically empty) ; I also said that the luminous substance has a specific weight, greater than the darker. For this reason it always goes down to the bottom of the eyeball (by force of gravity). The luminous substance always takes, in the same eye, the same aspect or pattern under conditions of rest. It is true, as Dr. Rosen says, that these are facts already well known (more or less in their details) but by studying the normal, I had been able to describe a new pathologic phenomenon which I had called "ascension phenomenon" or better still "climbing of the luminous bands."
Under pathologic conditions (sometimes during inflammatory conditions of the ocular coats, or in the presence of hemorrhages into the vitreous body), after the eye makes sudden movements and turns quiet, these bands of luminous substances go upward and stay there instead of going down by action of gravity. Then we see the inversion of the anterior portion of Cloquet's canal. The funnel is now directed downward and

BOOK REVIEWS 1029
backward. The walls are now directed upward and backward. This is a phenomenon, the pathogenesis of which is easy to explain.
The pathologic process induces a modification of the liquid component (dark substance), the specific weight of which increases. On the contrary, the specific weight of the luminous substance does not increase proportionally. By this means the density of luminous substance becomes less than that of the dark substance and it rises up in the eyeball.
I only stress here the main points of the phenomenon that I described in 1953, regretting that I cannot go into greater details, for the sake of brevity.
(Signed) Archimede Busacca, Säo Paulo, Brazil.
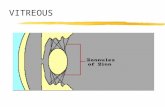
Figs. 1 and 2 (Busacca). (1) Normal position of anterior portion of Cloquet in eye at rest. (2) Position of anterior portion of Cloquet with eye at rest following rise of bands of luminous substance. (a) Portion adherent to free superior band and free plicata. (b) Superior portion of inferior band. (c) Portion adherent to free inferior plicata. (d) Portion of elbow of inferior band, (e) Free portion of inferior band.
BOOK REVIEWS OPHTHALMODYNAMOMETRIE. By A. Weige-
lin and A. Lobstein. Basel and New York, S. Karger, 1962. 141 pages, 18 illustrations, 17 tables. Price: $8.00. (American representative: Albert J. Phiebig, P.O. Box 352, White Plains, New York.) Forty-five years ago Bailliart published
his investigations concerning ophthalmody-namometry. For a while his work almost fell into oblivion. However, there has been a tremendous interest in this method during recent years, although for reasons different from Bailliart's original ideas. It must have given him great satisfaction to write the preface to the volume under discussion.
This monograph is noteworthy for it represents the combined efforts of E. Weigelin of the University Eye Clinic in Bonn, Germany, and of A. Lobstein of the Clinique Ophtalmologique, Strasbourg, France, and covers a period of 10 years. Weigelin is primarily interested in the physical aspects of the method, whereas Lobstein concerns himself mostly with its clinical application. In the first part of the book the general principles are discussed. The second part deals with the clinical application of these principles.
It is sheer delight to follow the sequence of deductions of these general principles which seem so complicated at first sight and which, in the end, are reduced to a few tables which should go a long way to simplify the mathematical aspects of the actual readings.
Standard curves relating the weight caused by the spring action of the instrument to the intraocular pressure are based on the investigations of Niesel and Leonardi, as well as of Bedavanija. (These considerations would be superfluous if the angiotonometer of Baurmann, which employs a manometer, were used; however, the authors seem to prefer the customary type of ophthalmody-namometer with spring action.) One table allows direct readings of the normal values













![Why worry about strabismus? [1,8] Vitreous Hemorrhage (dark reflex) Hypopyon (layering of WBCs in anterior chamber)](https://static.fdocuments.in/doc/165x107/5697bfc21a28abf838ca5133/why-worry-about-strabismus-18-vitreous-hemorrhage-dark-reflex-hypopyon.jpg)