Arthur Hill, M.D.; Professor, Department of Surgery...
102
Arthur Hill, M.D.; Professor, Department of Surgery Division of Cardiothoracic Surgery; University of California, San Francisco April 2, 2016
Transcript of Arthur Hill, M.D.; Professor, Department of Surgery...
Arthur Hill, M.D.; Professor, Department of SurgeryDivision of Cardiothoracic Surgery; University of California, San FranciscoApril 2, 2016

� Structural/Anatomic� Epidemiologic� Clinical presentation/Physiologic phenomena� Resuscitative thoracotomy





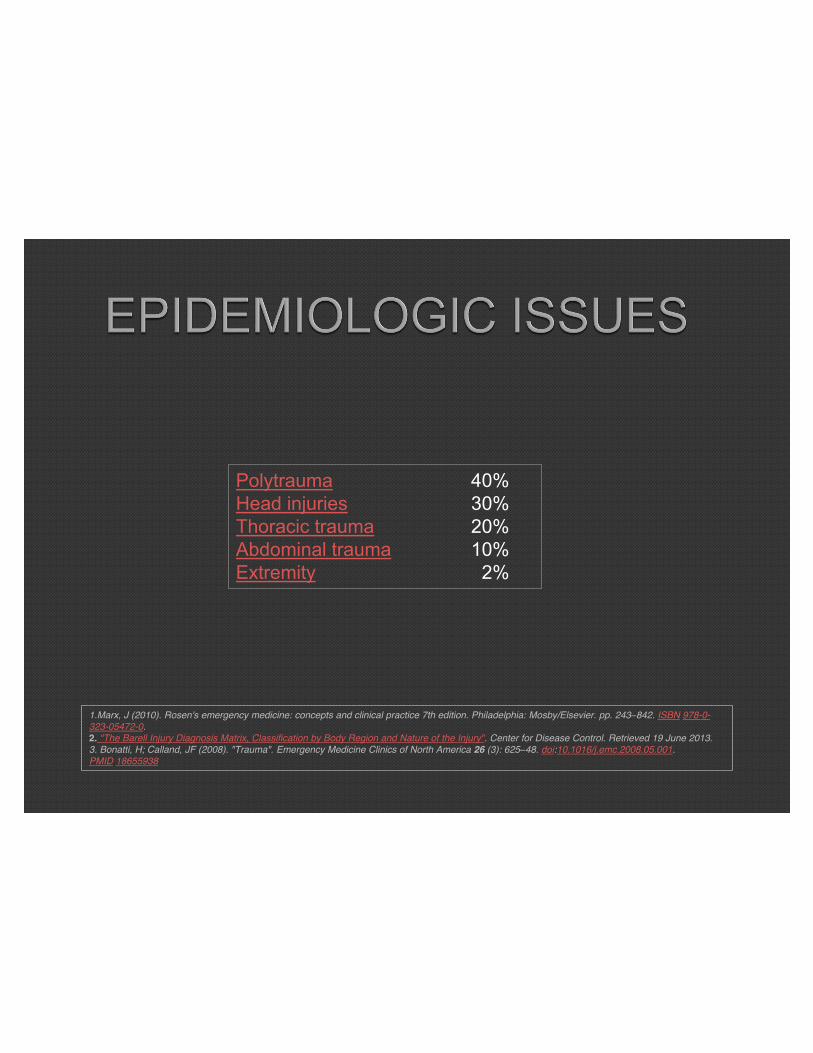
Polytrauma 40% Head injuries 30% Thoracic trauma 20% Abdominal trauma 10% Extremity 2%
1.Marx, J (2010). Rosen's emergency medicine: concepts and clinical practice 7th edition. Philadelphia: Mosby/Elsevier. pp. 243–842. ISBN 978-0-323-05472-0.2. "The Barell Injury Diagnosis Matrix, Classification by Body Region and Nature of the Injury". Center for Disease Control. Retrieved 19 June 2013.3. Bonatti, H; Calland, JF (2008). "Trauma". Emergency Medicine Clinics of North America 26 (3): 625–48. doi:10.1016/j.emc.2008.05.001. PMID 18655938

� BLUNT• MVC• Falls• Airplane Crashes
� PENETRATING• Stab wounds• Bullet wounds

� Thoracic injuries are present in 45 – 50% of unrestrained drivers involved in high speed MVC’s
� Thoracic injuries are the cause of death in 25% of MVC fatalities.

Distribution of Organ Injury:• Chest Wall 70%• Lung 21%• Heart 7%• Diaphragm 7%• Esophagus 7%• Aorta 4.8%• Tracheobronchial Injuries 0.8%
Jones KW. Thoracic Trauma. Surg Clin North Am 1980; 60: 957-81. Hill AB, Fleiszer DM, Brown RA. Chest trauma in a Canadian urban setting - implications for trauma research in Canada. J Trauma 1991; 31: 971-73. Devitt JH, McLean RF, Koch J-P. Anaesthetic management of blunt thoracic trauma. Can J Anaesth 1991; 38: 506-10. Shorr RM, Crittenden M, Indeck M, Hartunian SL, Rodriguez A. Blunt thoracic trauma; analysis of 515 patients. Ann Surg 1987; 206: 200-5.

�Low velocity missile
�High velocity missile

�40% Penetrating Injury Involves the Thorax
�15-28% of Penetrating Thoracic Injuries Require Thoracotomy

� Distribution of Organ Injury• Chest Wall 100%• Lung 65-90%• Heart 49%• Diaphragm 30%• Intra-Abdominal Injuryx Liver 20%x Stomach 8%x Small intestine 7%x Colon 6%x Kidney 5%
Clinical PresentationPhysiological Consequences
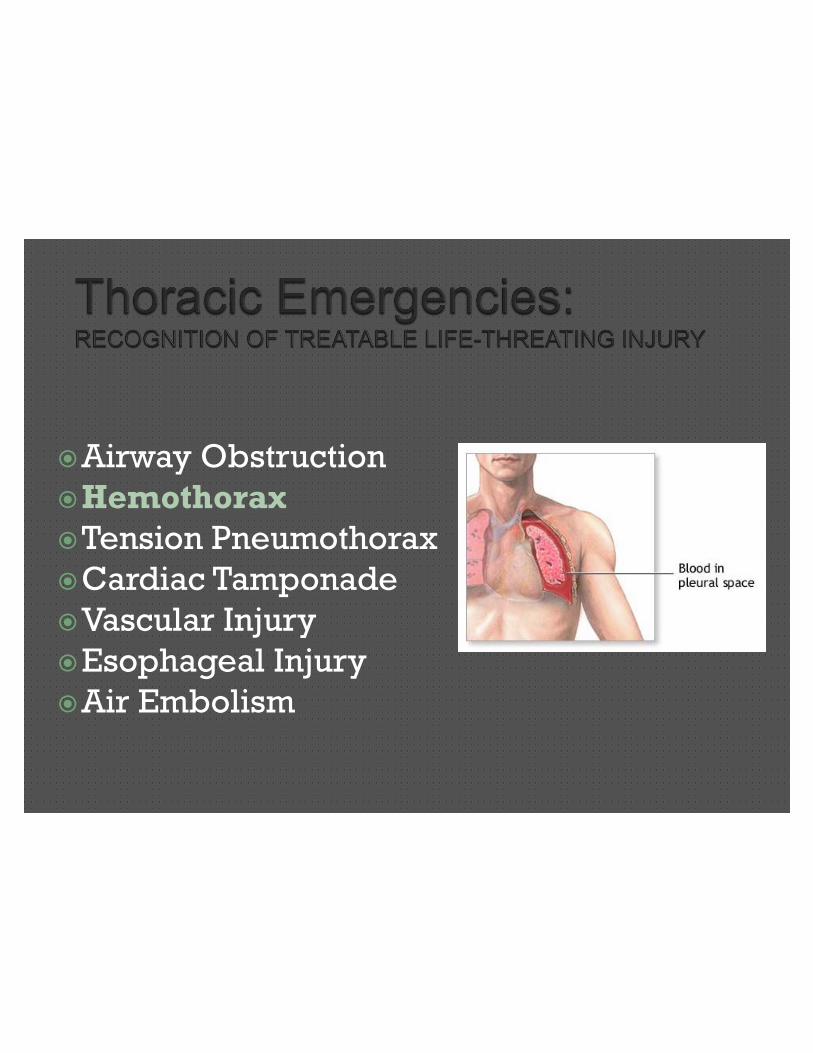
�Airway Obstruction�Hemothorax�Tension Pneumothorax�Cardiac Tamponade�Major Vascular Injury�Air Embolization
�A – Airway (with c-spine protection)
�B – Breathing (pleural drainage)
�C – Circulation (stop the bleeding)
�D – Disability (neuro status, fractures)
�E – Exposure (temperature, pain)

�Airway Obstruction/Injury�Hemothorax
�Tension Pneumothorax
�Cardiac Tamponade
�Vascular Injury
�Esophageal Injury
�Air Embolization
�Causes:• Blunt• Penetrating
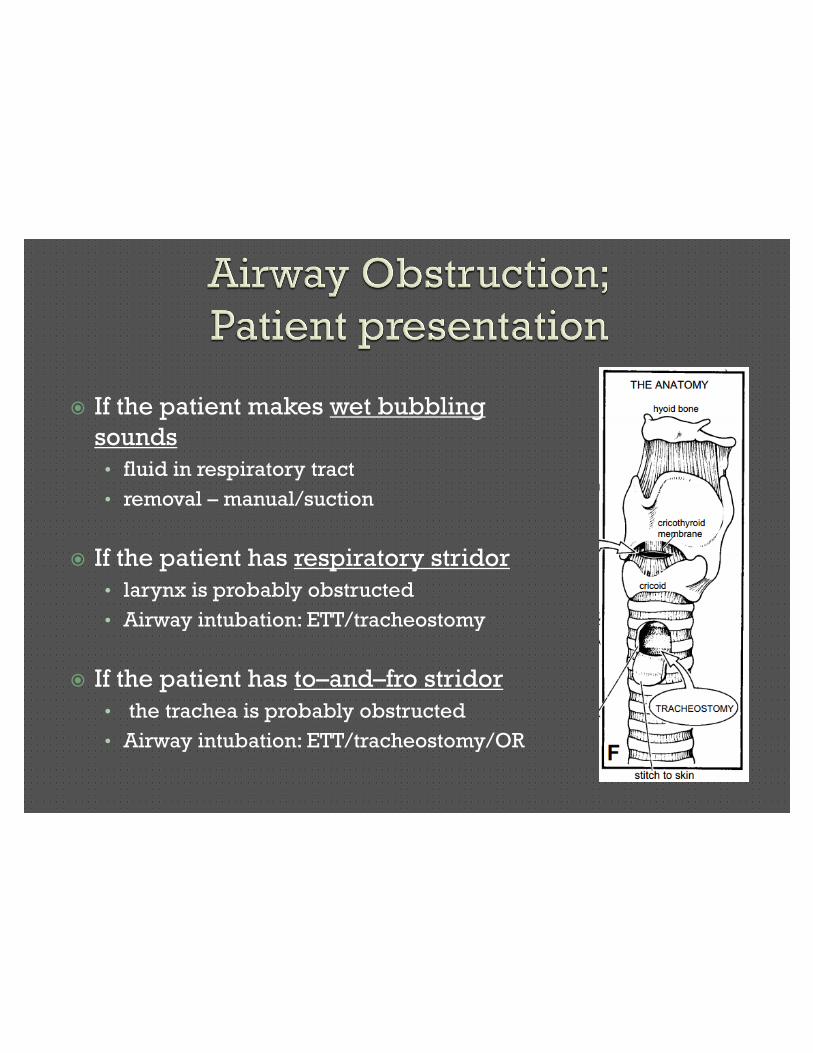
� If the patient makes wet bubbling
sounds
• fluid in respiratory tract
• removal – manual/suction
� If the patient has respiratory stridor
• larynx is probably obstructed
• Airway intubation: ETT/tracheostomy
� If the patient has to–and–fro stridor
• the trachea is probably obstructed
• Airway intubation: ETT/tracheostomy/OR

� Anatomic localization of site of obstruction (neck vs. thorax)
� Method of airway control• Standard ET intbation
• Tracheostomy
� Imaging• CXR
• CT
� Endoscopy• Simultaneous with airway control
� Teamwork• Anesthesiology
• ENT

� Simple maneuvers:• Upper airway• Manual removal of
obstructive objects• Suctioning
� Complex airway maneuvers• Operating Room• Oro-tracheal Intubation
vs. Tracheostomy• Bronchoscopy• Thoracotomy vs. Stenting

AIRWAY INJURY

INCISION CHOICE FOR TRACHEAL INJURY

�Stent placement

�Airway Obstruction
�Hemothorax�Tension Pneumothorax
�Cardiac Tamponade
�Vascular Injury
�Esophageal Injury
�Air Embolism
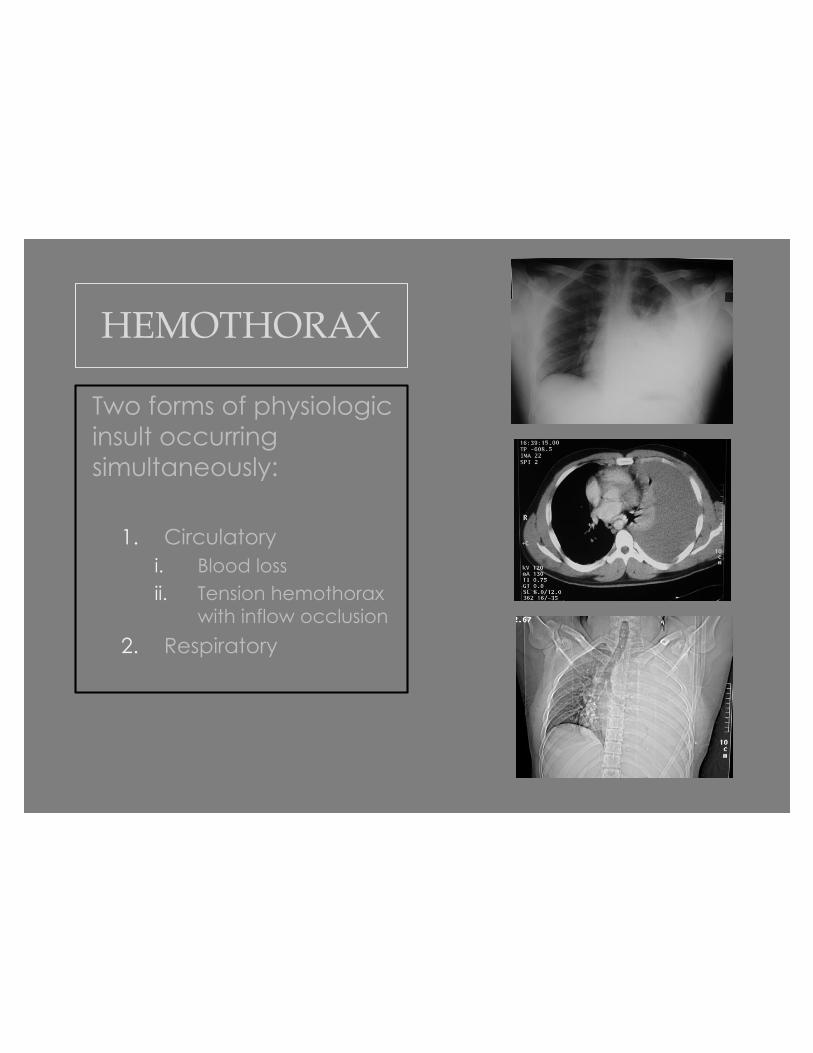
HEMOTHORAX
Two forms of physiologic insult occurring simultaneously:
1. Circulatoryi. Blood lossii. Tension hemothorax
with inflow occlusion
2. Respiratory

HEMOTHORAX
• Blunt or Penetrating Trauma• Requires chest tube
placement• Volume resuscitation• Thoracotomy required if:
• Hemodynamic Instability• Chest tube output > 1200cc• > 250 cc/hr• Ineffective chest tube drainage
with large hemothorax • (VATS may be an option in a stable
patient)

�Thoracotomy is done on the side with the hemothorax.
�Extension across midline if needed.�Median sternotomy is contraindicated.
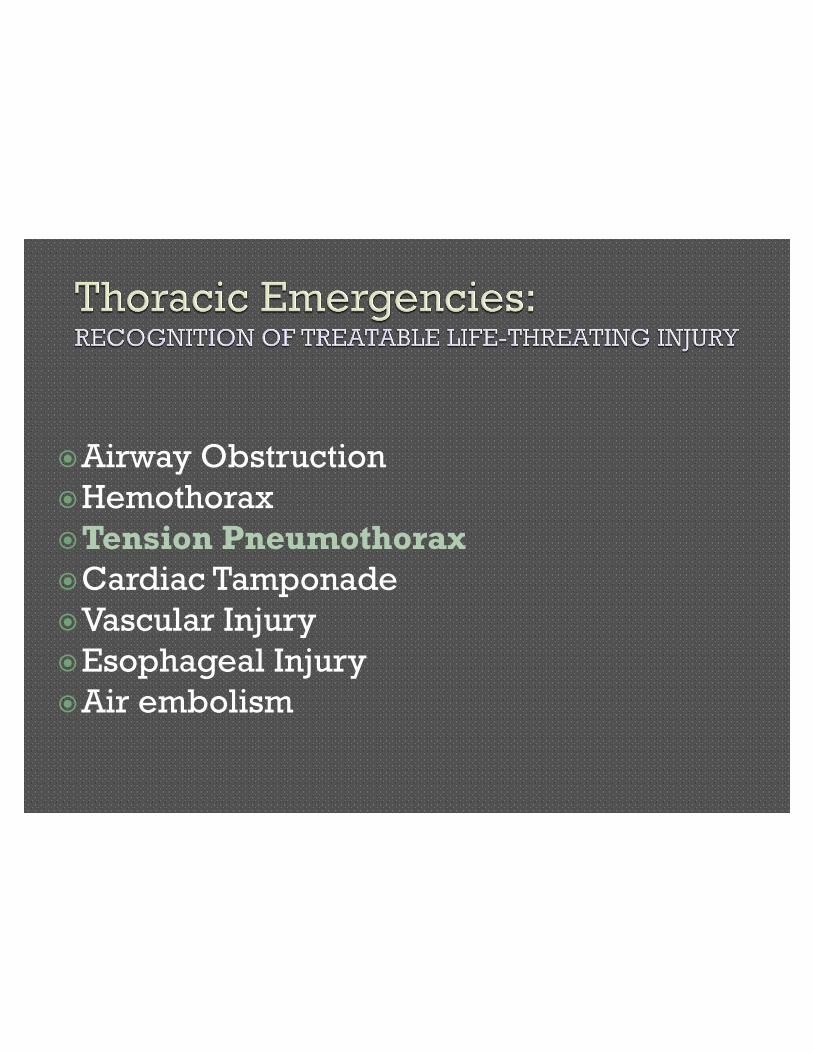
�Airway Obstruction
�Hemothorax
�Tension Pneumothorax�Cardiac Tamponade
�Vascular Injury
�Esophageal Injury
�Air embolism
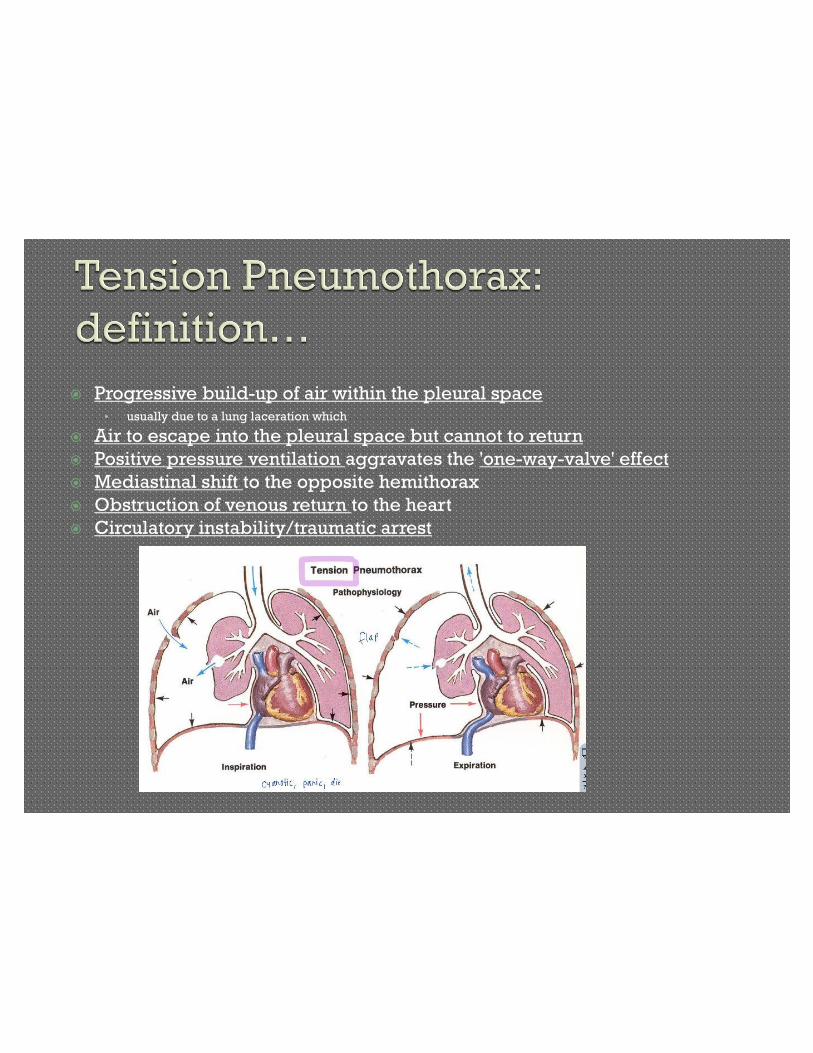
� Progressive build-up of air within the pleural space• usually due to a lung laceration which
� Air to escape into the pleural space but cannot to return
� Positive pressure ventilation aggravates the 'one-way-valve' effect
� Mediastinal shift to the opposite hemithorax
� Obstruction of venous return to the heart
� Circulatory instability/traumatic arrest
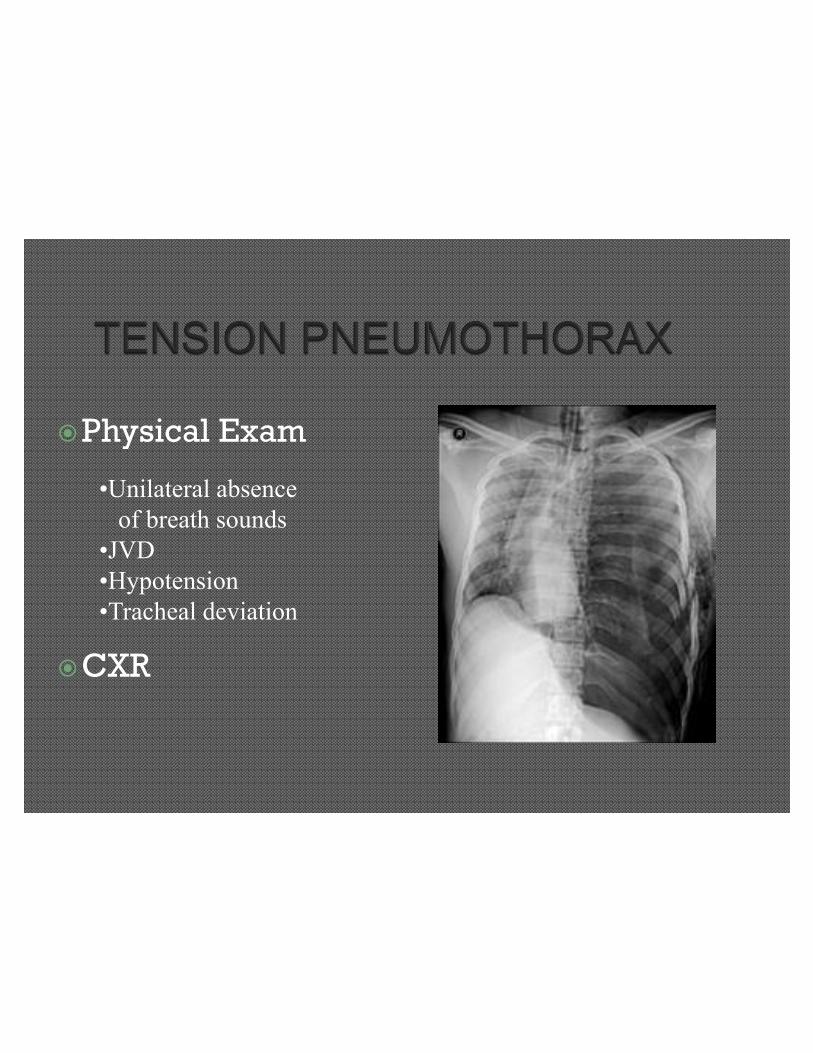
�Physical Exam
�CXR
•Unilateral absenceof breath sounds
•JVD•Hypotension•Tracheal deviation
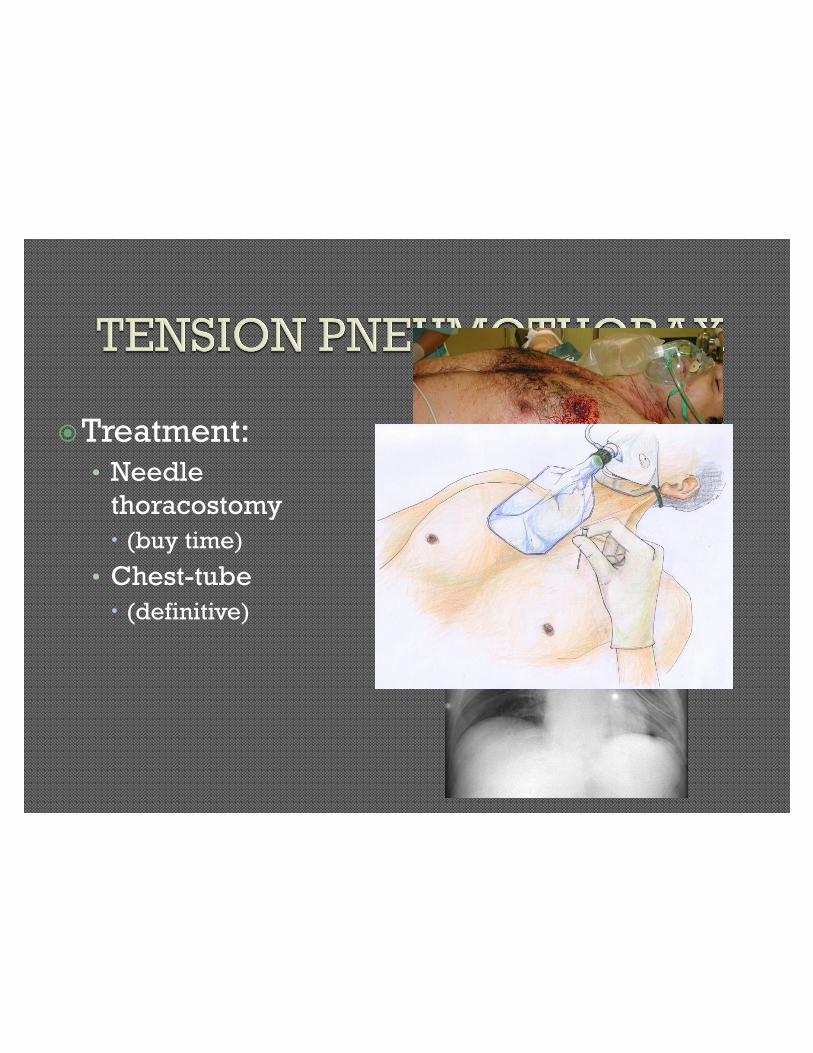
�Treatment:• Needle
thoracostomy
x (buy time)
• Chest-tube
x (definitive)
�Airway Obstruction�Hemothorax�Tension Pneumothorax�Cardiac Tamponade
• Cardiac Injury�Vascular Injury�Esophageal Injury�Air Embolism
Definition:
Fluid collection within the pericardium with: 9 compression of the heart9 hemodynamic compromise9 elevation and equalization of
atrial pressures9 physical exam findings
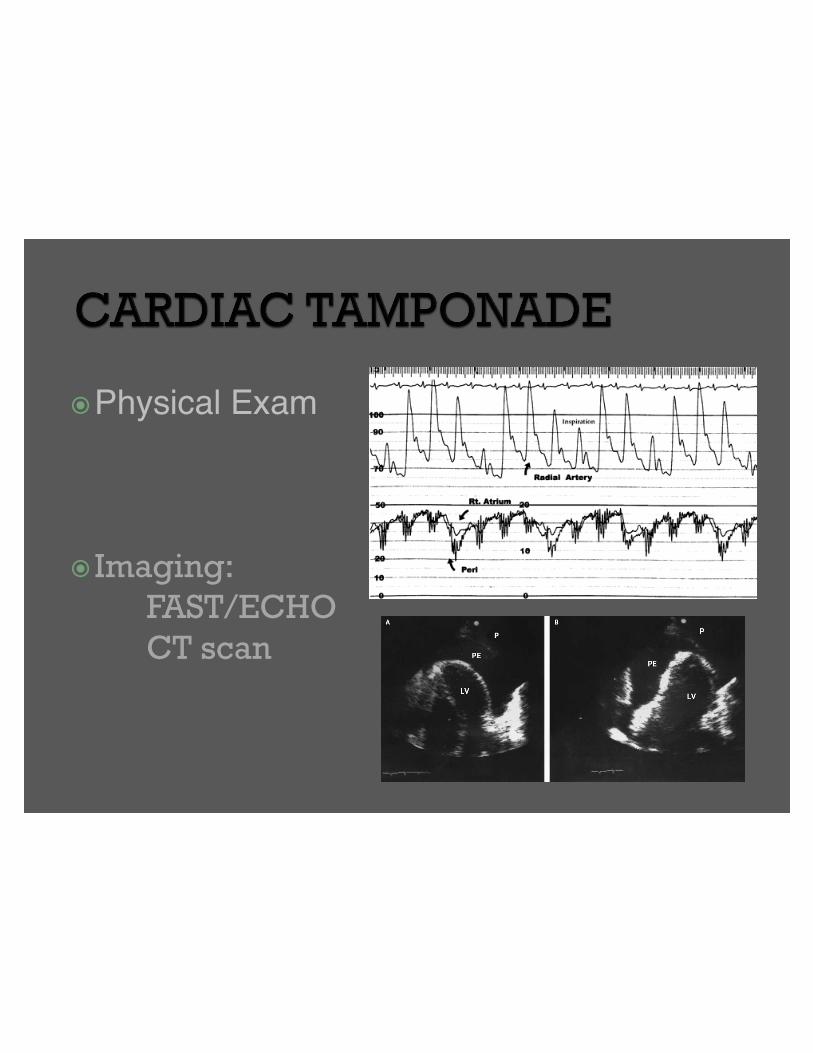
�Physical Exam
� Imaging:
FAST/ECHO
CT scan
•Hypotension•Muffled Heart Sounds
•JVD•Pulsus Paradoxus

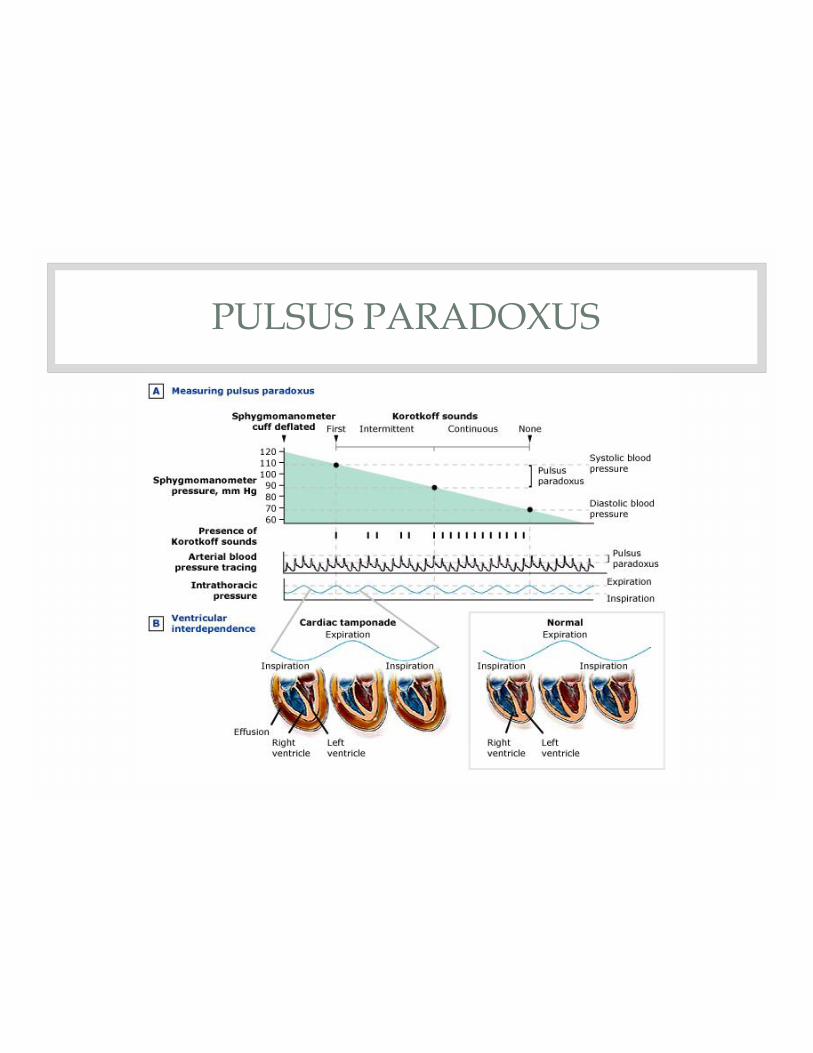
PULSUS PARADOXUS
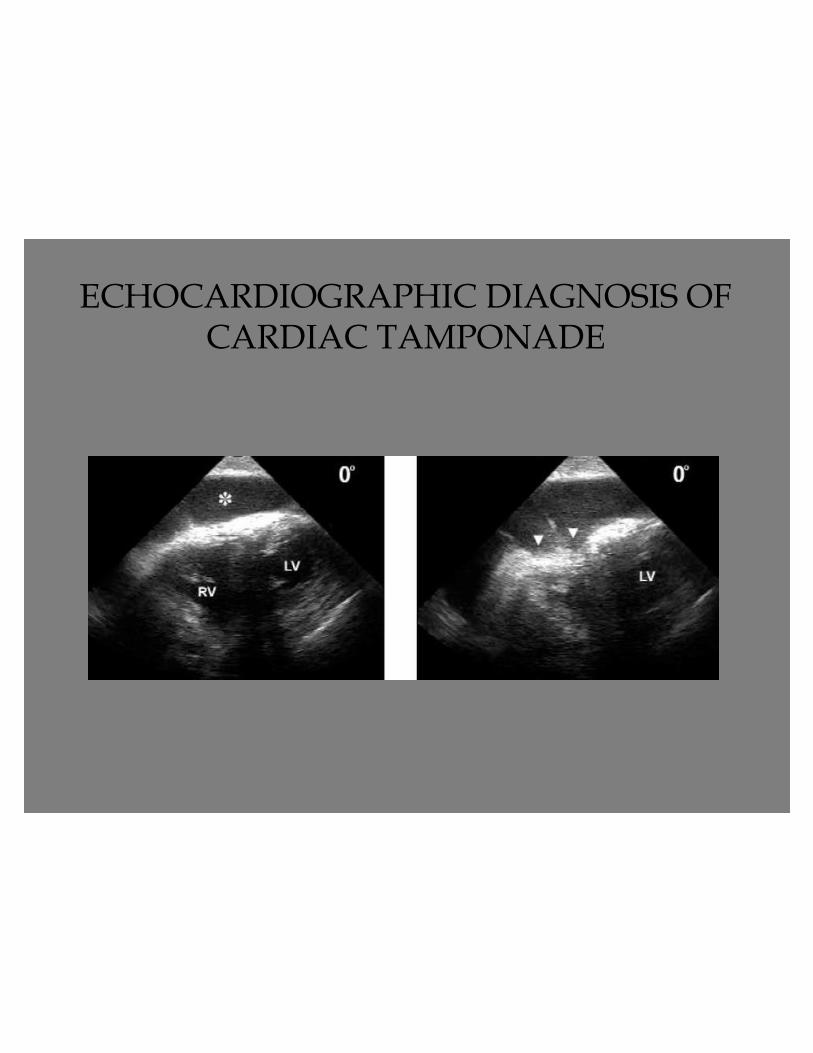
ECHOCARDIOGRAPHIC DIAGNOSIS OF CARDIAC TAMPONADE

CT SCAN DIAGNOSIS OF CARDIAC TAMPONADE
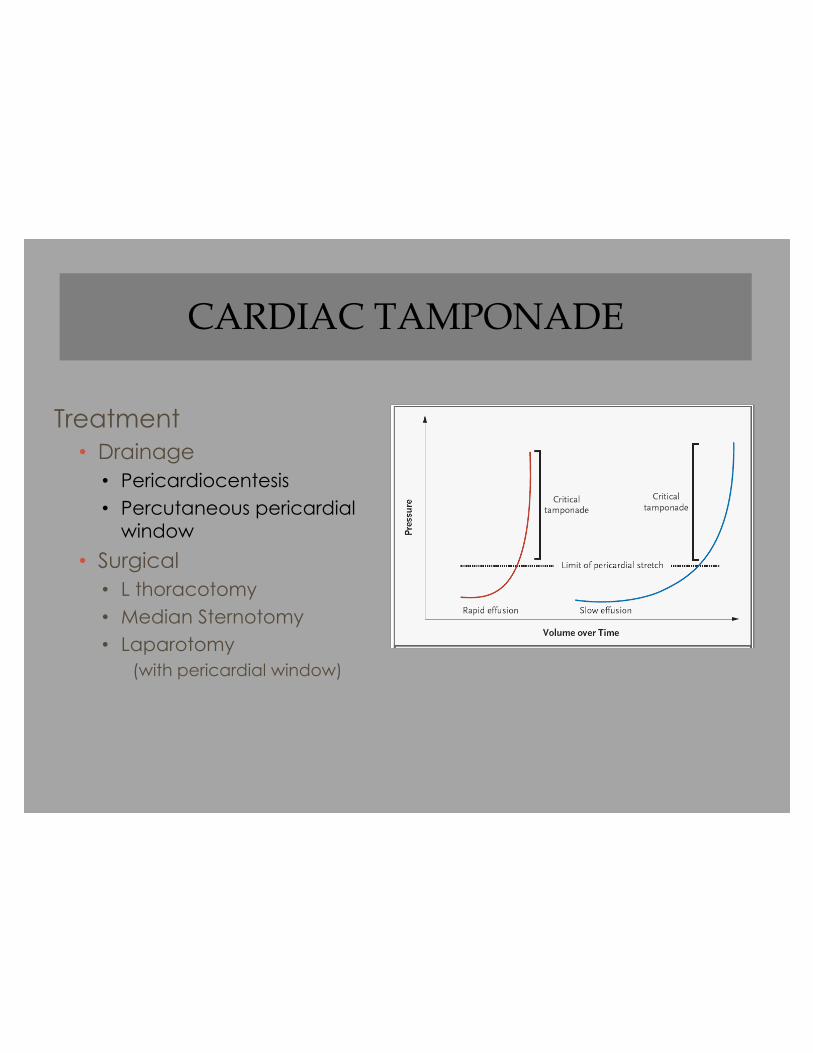
CARDIAC TAMPONADE
Treatment• Drainage
• Pericardiocentesis• Percutaneous pericardial
window
• Surgical• L thoracotomy• Median Sternotomy• Laparotomy
(with pericardial window)

�Cardiac injury with tamponade:Requires emergency surgery
x Left anterolateral thoracotomy
(Extension to clam-shell)
x Median Sternotomy
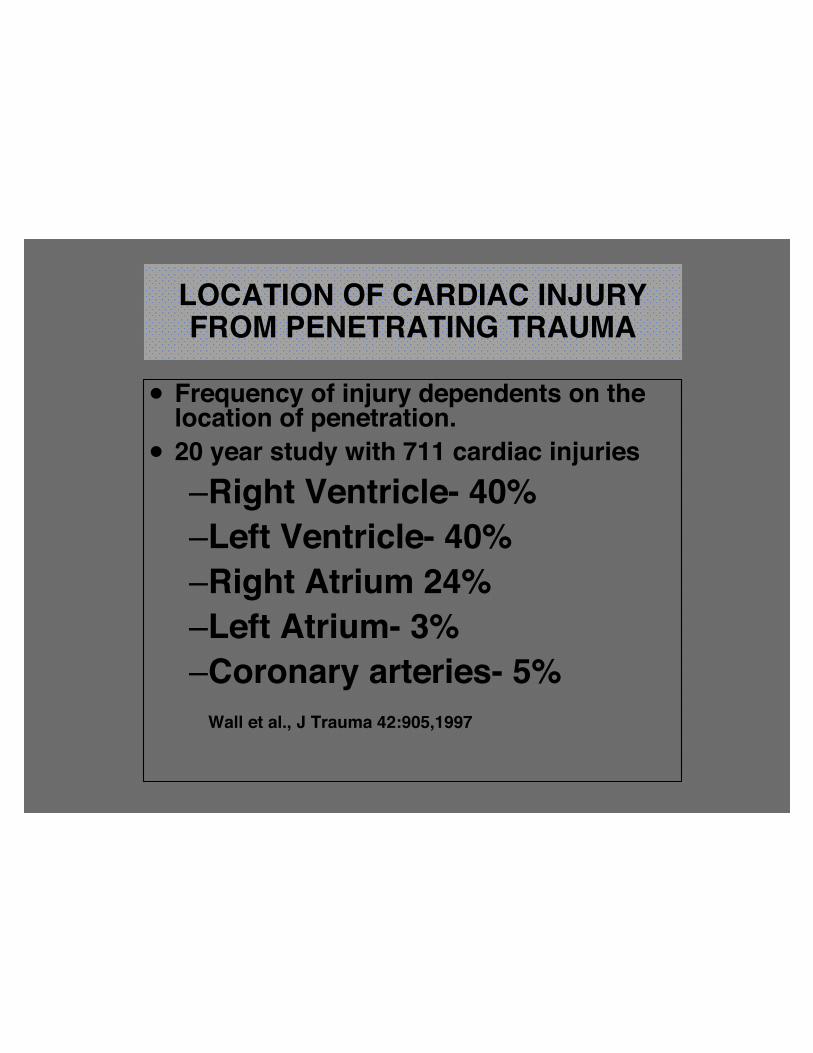
LOCATION OF CARDIAC INJURY FROM PENETRATING TRAUMA
x Frequency of injury dependents on the location of penetration.
x 20 year study with 711 cardiac injuries–Right Ventricle- 40%–Left Ventricle- 40%–Right Atrium 24%–Left Atrium- 3%–Coronary arteries- 5%
Wall et al., J Trauma 42:905,1997


�Airway Obstruction
�Hemothorax
�Tension Pneumothorax
�Cardiac Tamponade
�Thoracic Vascular Injury�Esophageal Injury
�Air Embolism

�Exsanguinating vascular injuries• Hemothorax
• Mediastinal hemorrhage
�Major vascular injury without
exsanguination• Aorta
• Major branches of thoracic aorta
Priorities:
• Identification of patients with possible vascular injury –mechanism of injury
• Identification of anatomic location of injury/site of exsanguination• Thoracic CT angiography• Formal angiography
• Rapid choice of therapy:• Surgical• Percutaneous/Interventional• Stent-graft placement
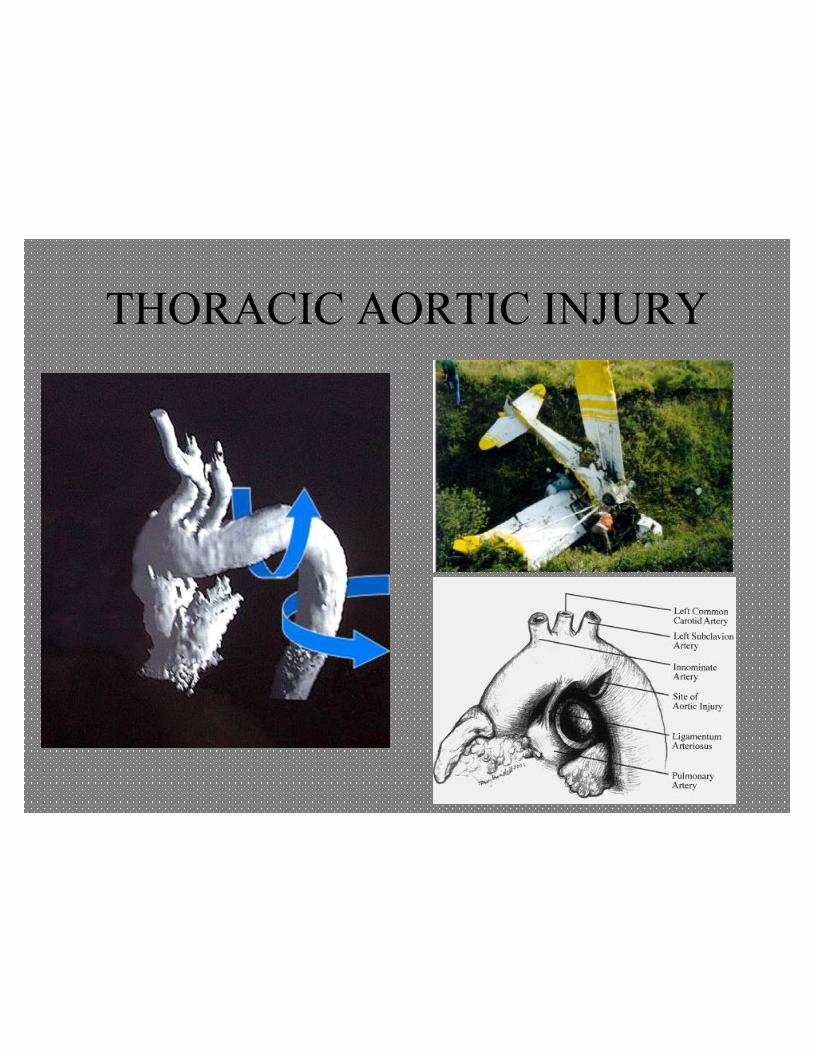
THORACIC AORTIC INJURY
Mechanism: rapid deceleration produces shearing injury between fixed and mobile portions of the aorta.

DISTRIBUTION OF AORTIC INJURIES
Traumatic Aortic Dissection/Rupture
• 15% of fatal MVC victims have aortic rupture• 85% die instantaneously• 10-15% survive to hospital• 21% die within six hours• 31% die within 24 hours• 84% die within 4 months• Must have high index of suspicion
Parmly et al (Circulation 1958)





TREATMENT OPTIONS IN BAI
• Pre-surgical pharmacologic treatment:– β Blocker (dP/dT reduction)– HR < 100; MAP < 100
• Surgical therapy– Clamp-and-sew– Bypass
• Endovascular Stent Therapy
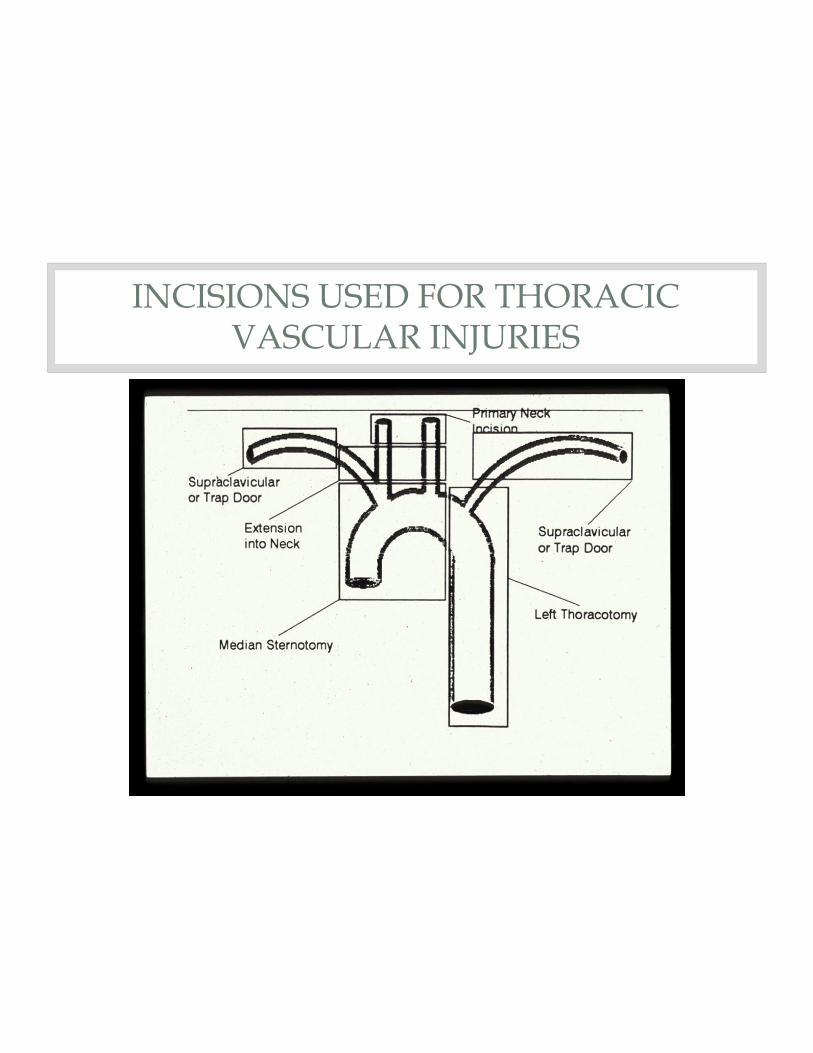
INCISIONS USED FOR THORACIC VASCULAR INJURIES
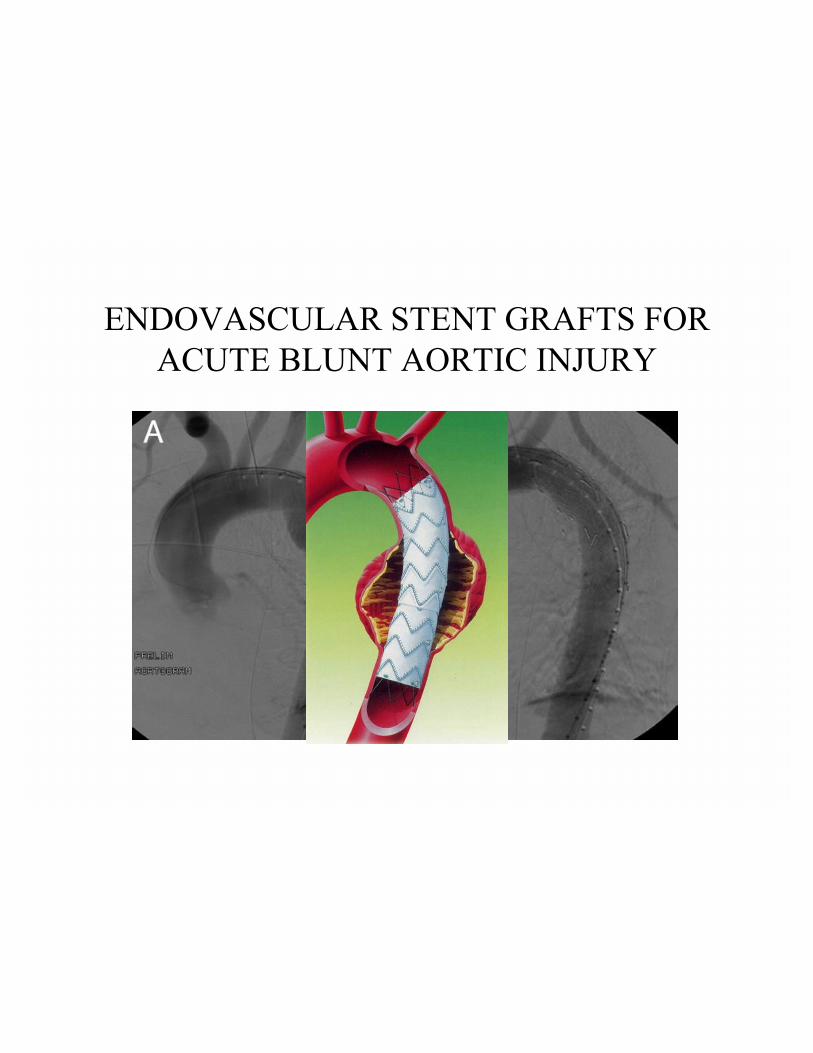
ENDOVASCULAR STENT GRAFTS FOR ACUTE BLUNT AORTIC INJURY
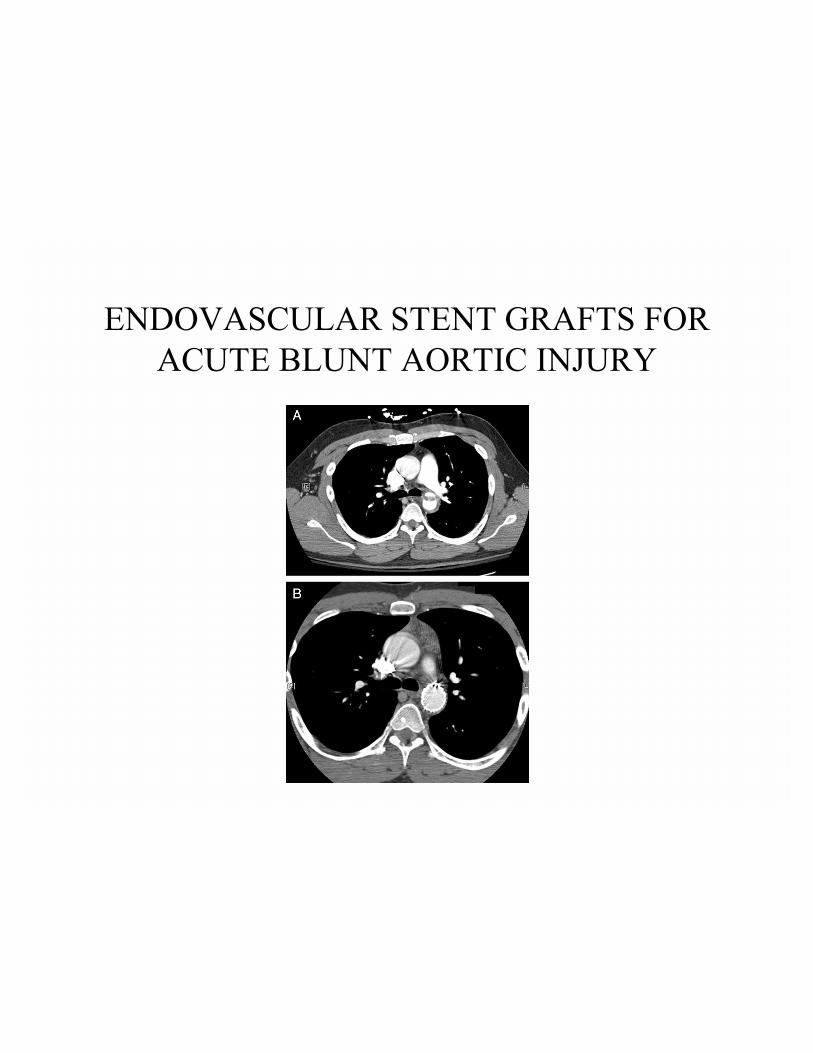
ENDOVASCULAR STENT GRAFTS FOR ACUTE BLUNT AORTIC INJURY

�Airway Obstruction
�Hemothorax
�Tension Pneumothorax
�Cardiac Tamponade
�Vascular Injury
�Air Embolism
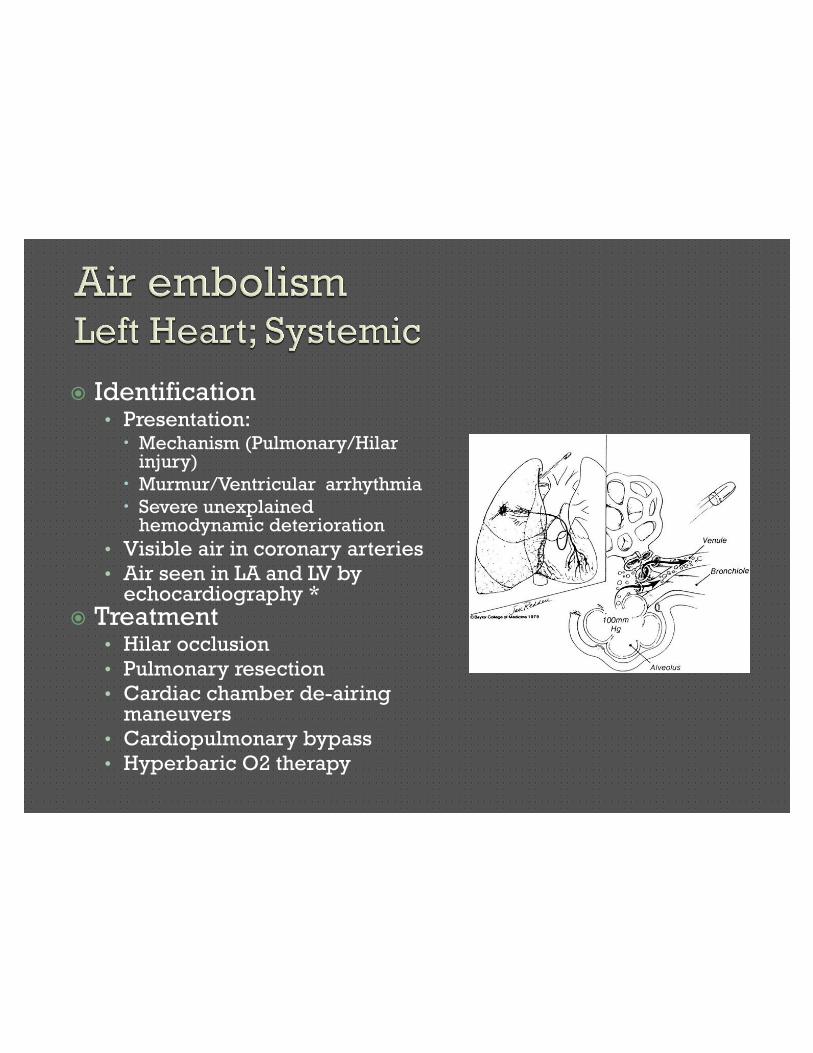
� Identification• Presentation:x Mechanism (Pulmonary/Hilar
injury)
x Murmur/Ventricular arrhythmia
x Severe unexplained hemodynamic deterioration
• Visible air in coronary arteries• Air seen in LA and LV by
echocardiography *� Treatment
• Hilar occlusion• Pulmonary resection• Cardiac chamber de-airing
maneuvers• Cardiopulmonary bypass• Hyperbaric O2 therapy

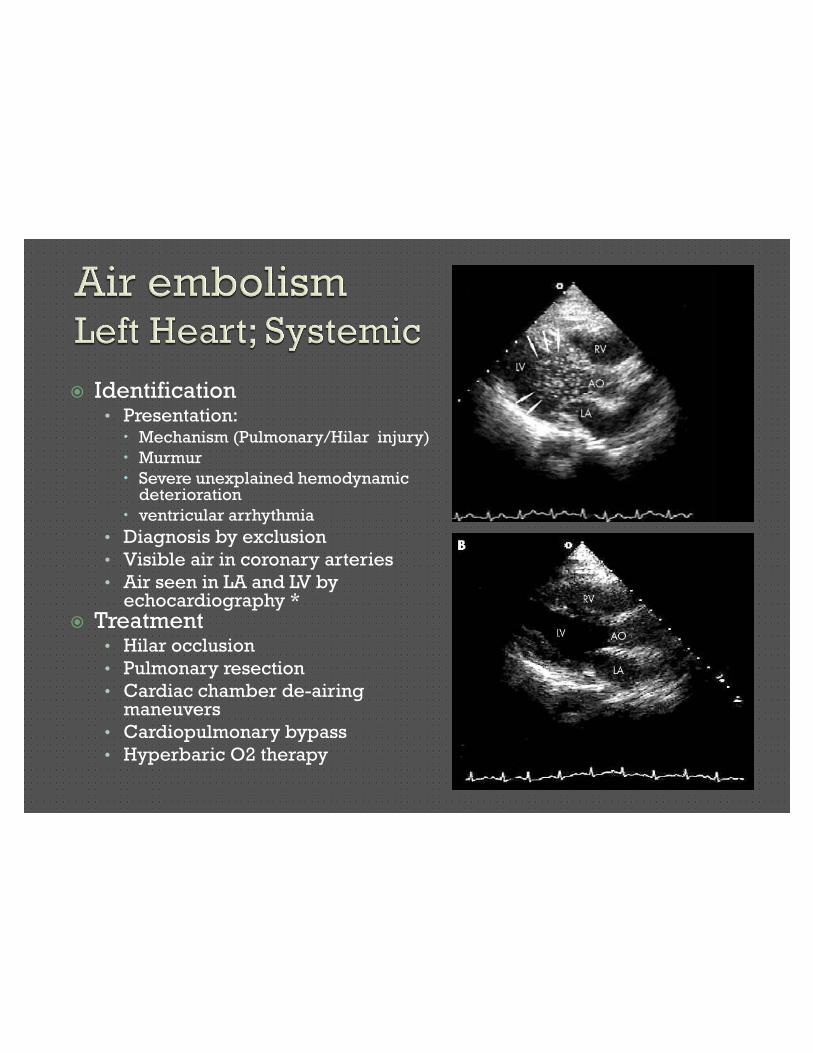
� Identification• Presentation:x Mechanism (Pulmonary/Hilar injury)
x Murmur
x Severe unexplained hemodynamic deterioration
x ventricular arrhythmia
• Diagnosis by exclusion
• Visible air in coronary arteries
• Air seen in LA and LV by echocardiography *
� Treatment• Hilar occlusion
• Pulmonary resection
• Cardiac chamber de-airing maneuvers
• Cardiopulmonary bypass
• Hyperbaric O2 therapy
�Airway Obstruction
�Hemothorax
�Tension Pneumothorax
�Cardiac Tamponade
�Vascular Injury
�Esophageal injury
�Air Embolism

• Esophageal Injuries• Cardiac Herniation• Flail Chest
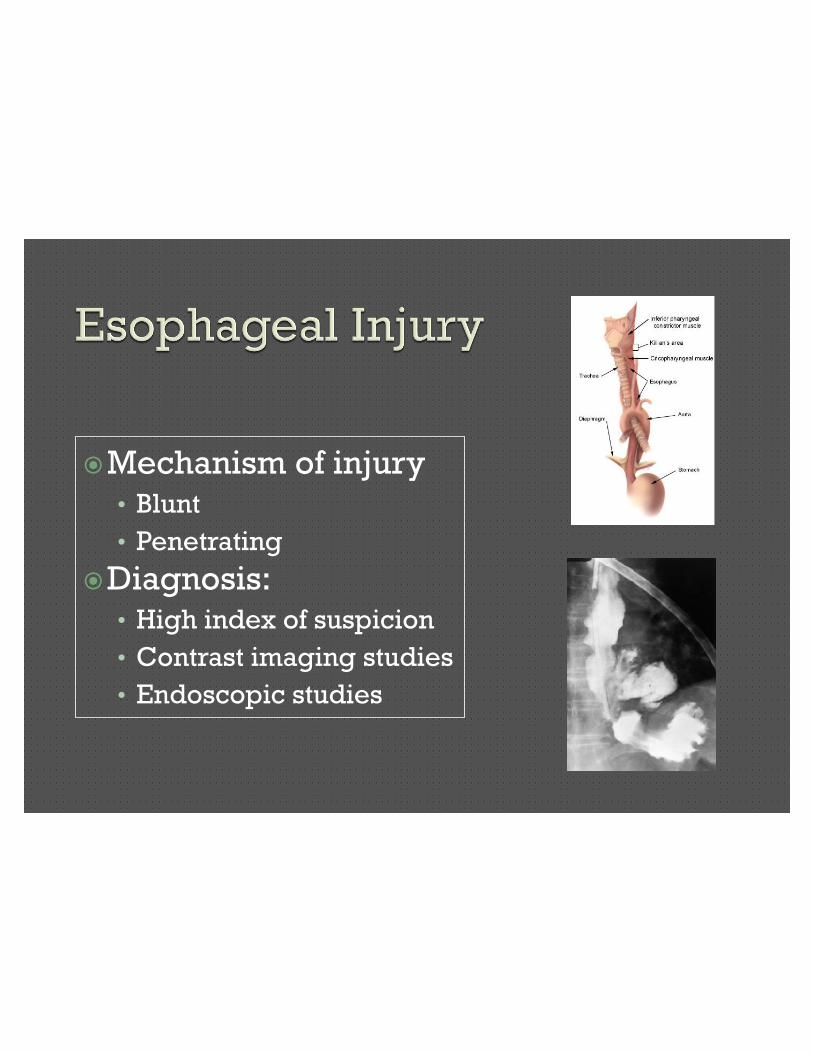
�Mechanism of injury• Blunt
• Penetrating
�Diagnosis:• High index of suspicion
• Contrast imaging studies
• Endoscopic studies
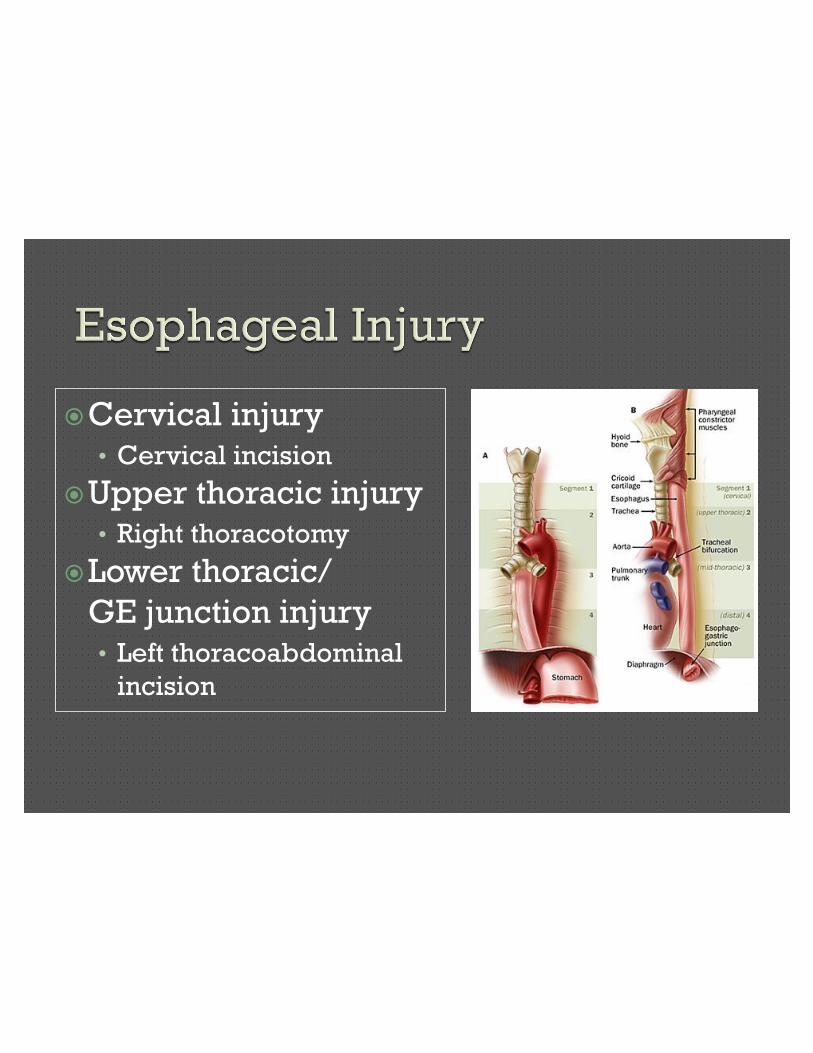
�Cervical injury• Cervical incision
�Upper thoracic injury• Right thoracotomy
�Lower thoracic/
GE junction injury• Left thoracoabdominal
incision
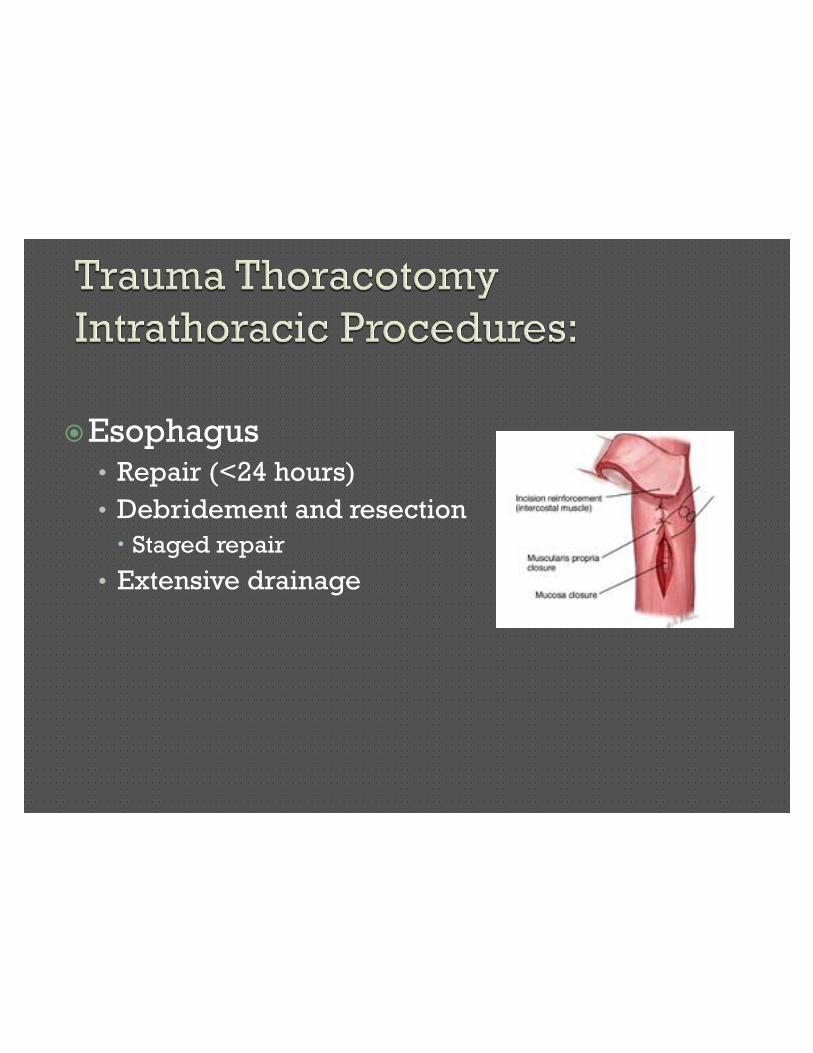
�Esophagus• Repair (<24 hours)
• Debridement and resection
x Staged repair
• Extensive drainage

Cardiac Herniation
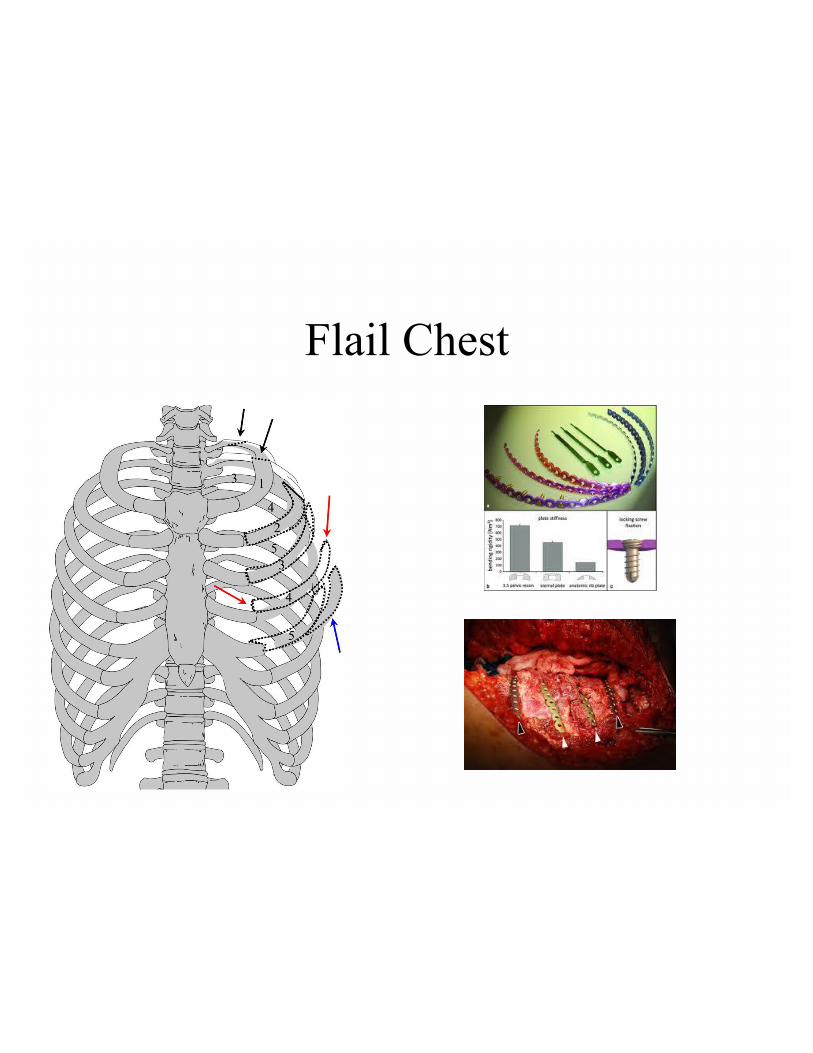
Flail Chest
INDICATIONS
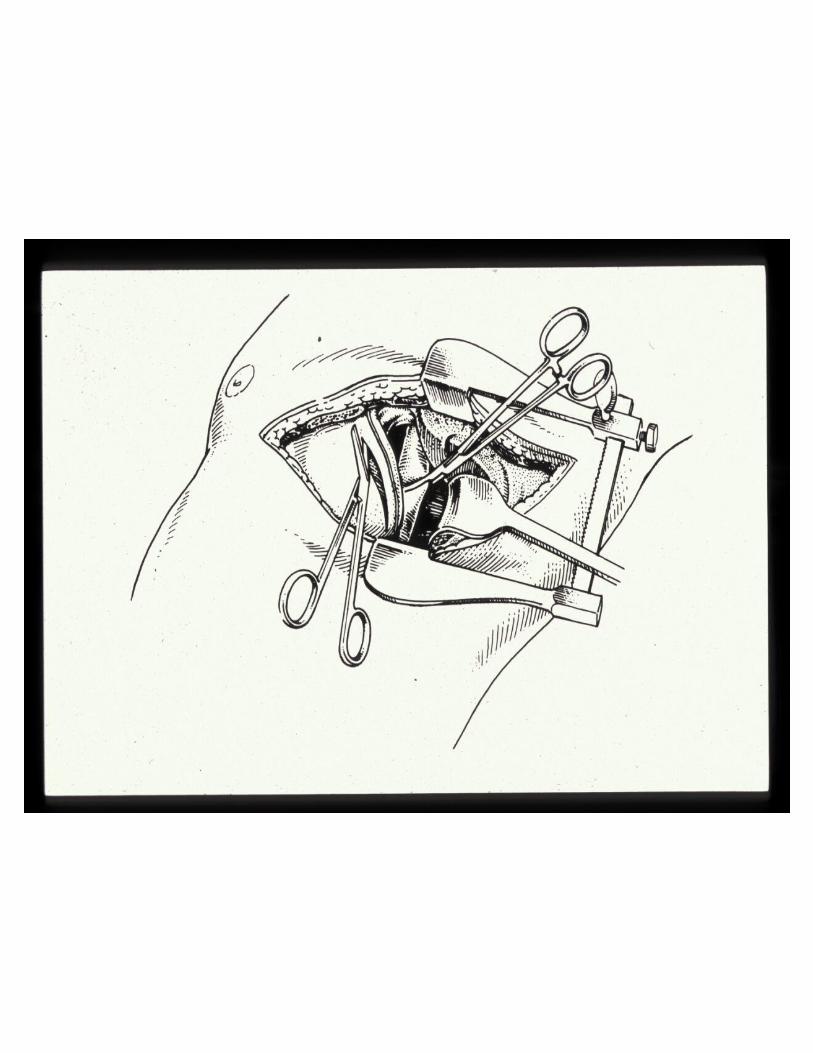
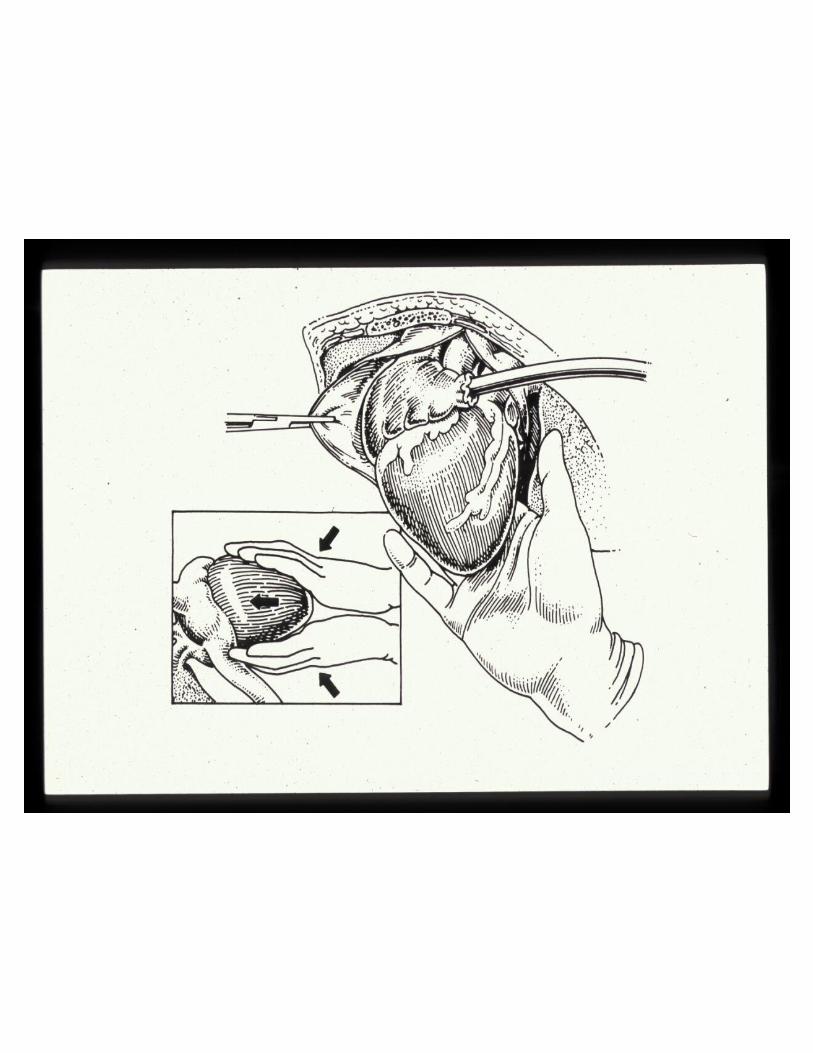
TECHNIQUE
10-15% of Thoracic Trauma patients
will require Resuscitative Thoracotomy
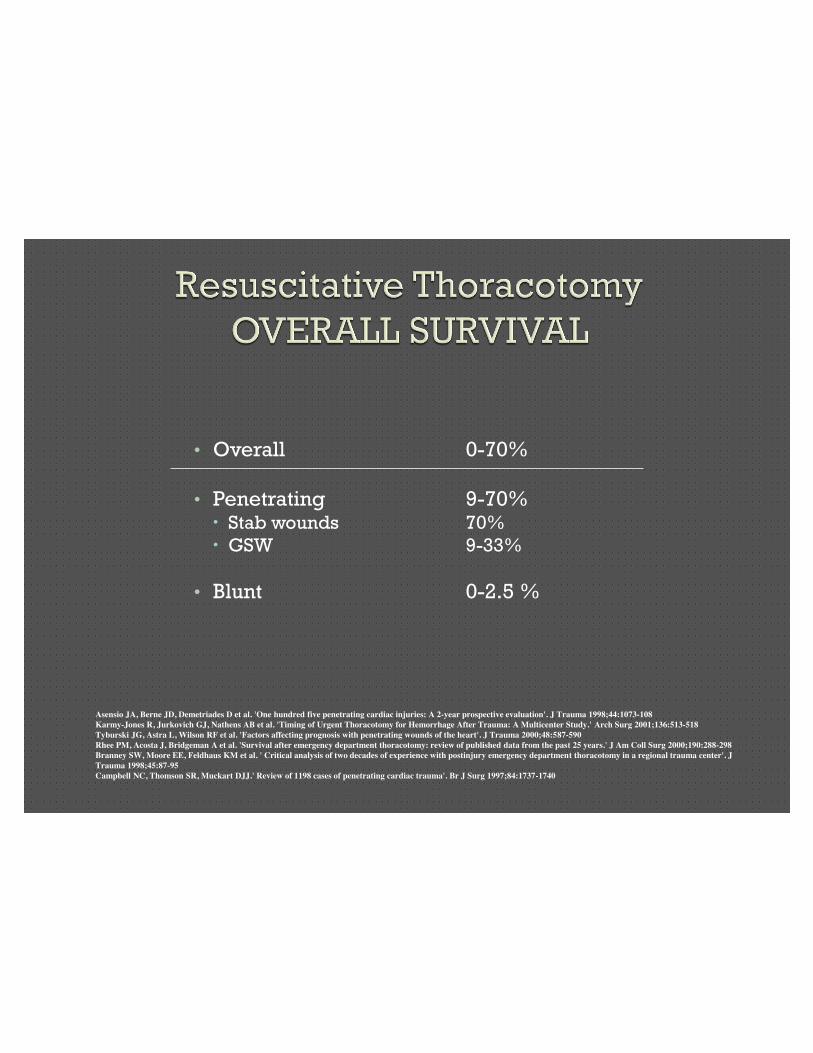
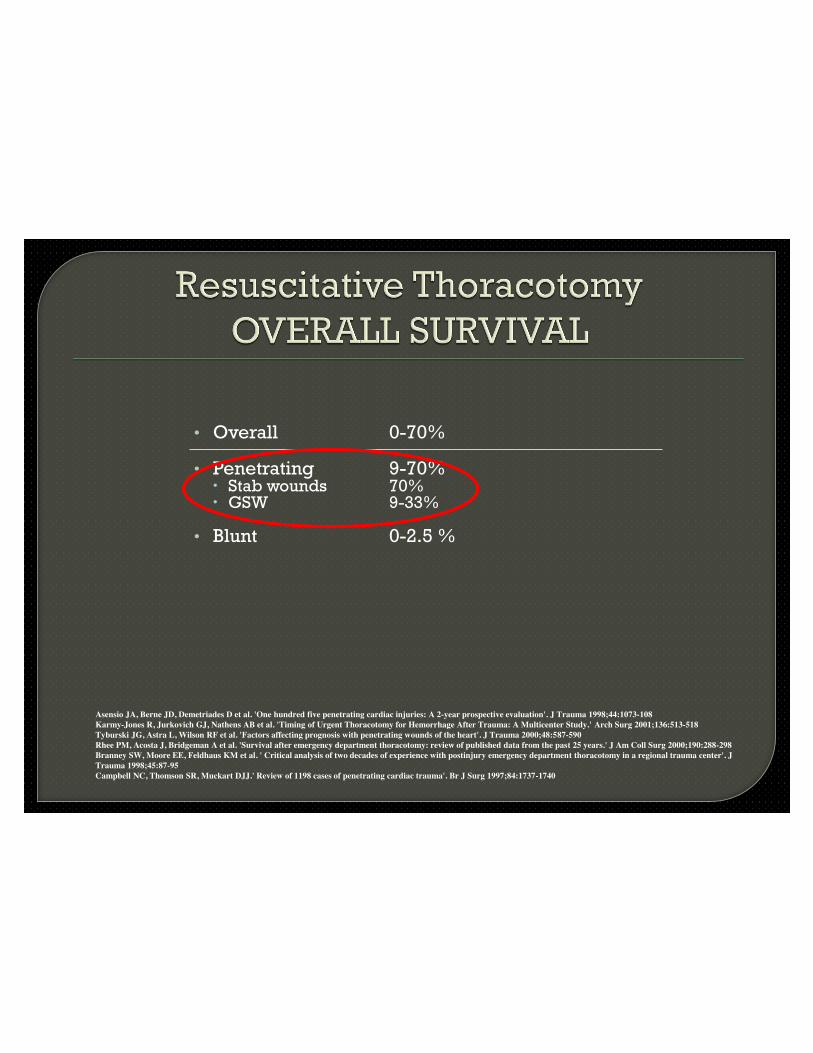
• Overall 0-70%
• Penetrating 9-70%x Stab wounds 70%
x GSW 9-33%
• Blunt 0-2.5 %
Asensio JA, Berne JD, Demetriades D et al. 'One hundred five penetrating cardiac injuries: A 2-year prospective evaluation'. J Trauma 1998;44:1073-108 Karmy-Jones R, Jurkovich GJ, Nathens AB et al. 'Timing of Urgent Thoracotomy for Hemorrhage After Trauma: A Multicenter Study.' Arch Surg 2001;136:513-518 Tyburski JG, Astra L, Wilson RF et al. 'Factors affecting prognosis with penetrating wounds of the heart'. J Trauma 2000;48:587-590 Rhee PM, Acosta J, Bridgeman A et al. 'Survival after emergency department thoracotomy: review of published data from the past 25 years.' J Am Coll Surg 2000;190:288-298 Branney SW, Moore EE, Feldhaus KM et al. ' Critical analysis of two decades of experience with postinjury emergency department thoracotomy in a regional trauma center'. J Trauma 1998;45:87-95 Campbell NC, Thomson SR, Muckart DJJ.' Review of 1198 cases of penetrating cardiac trauma'. Br J Surg 1997;84:1737-1740
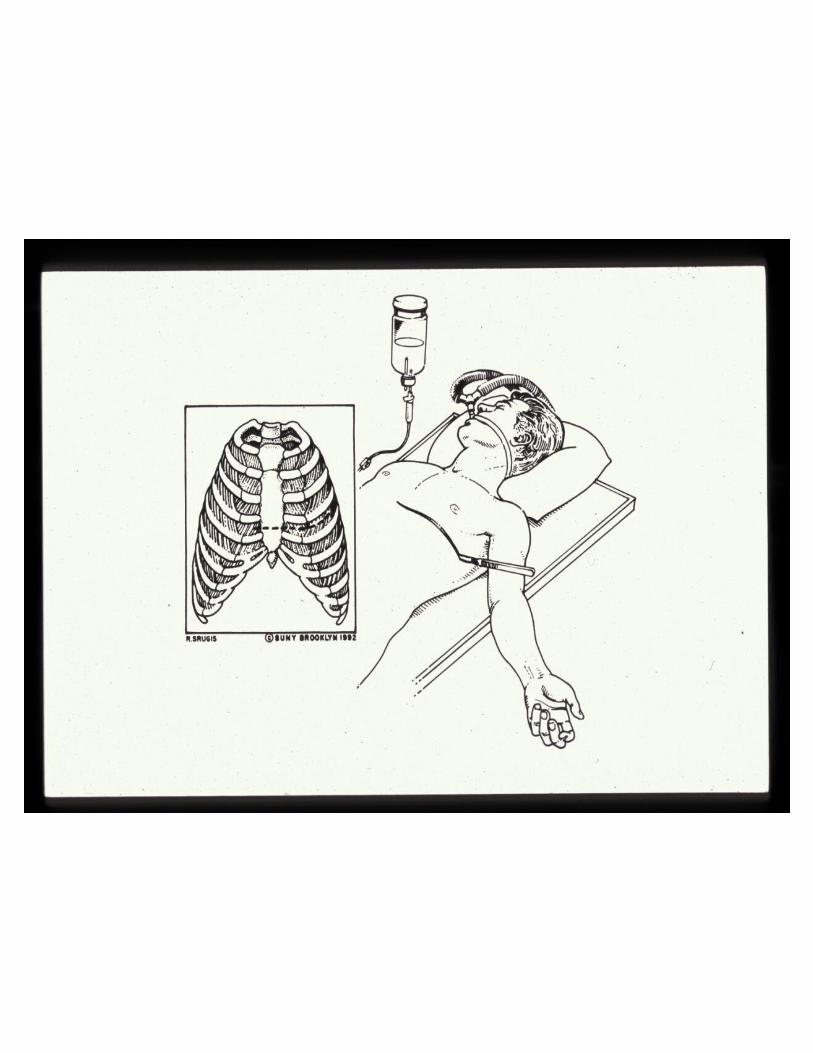
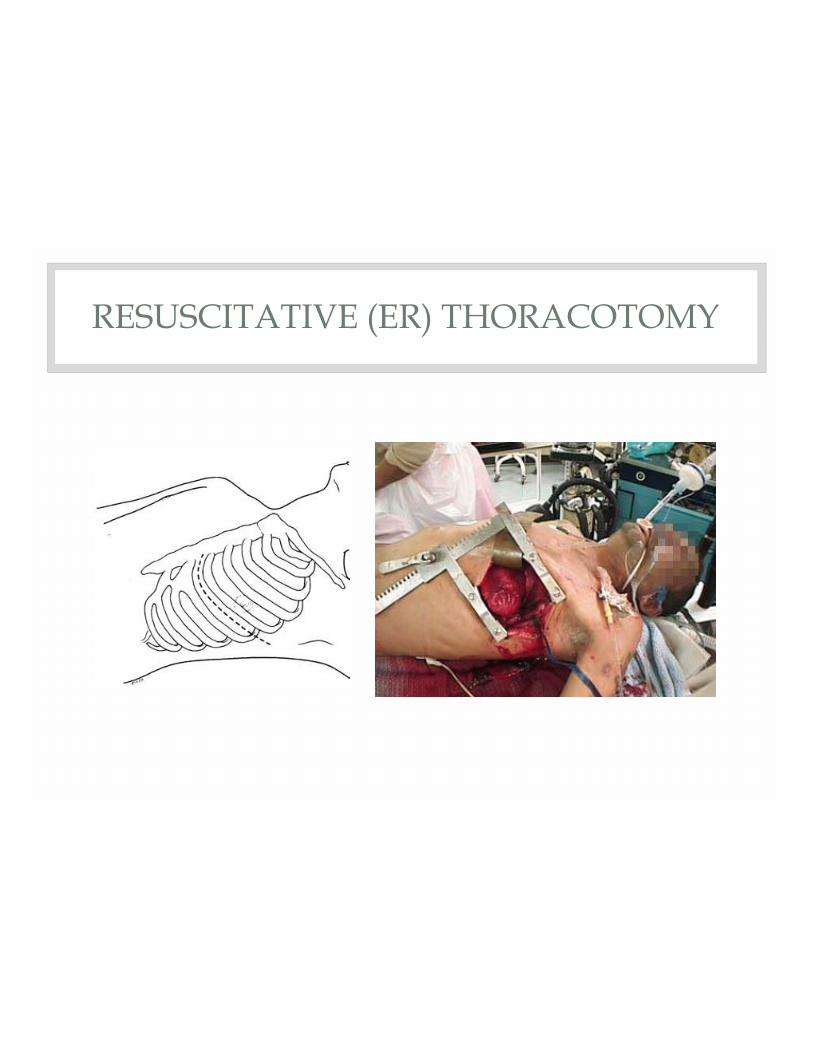
RESUSCITATIVE (ER) THORACOTOMY




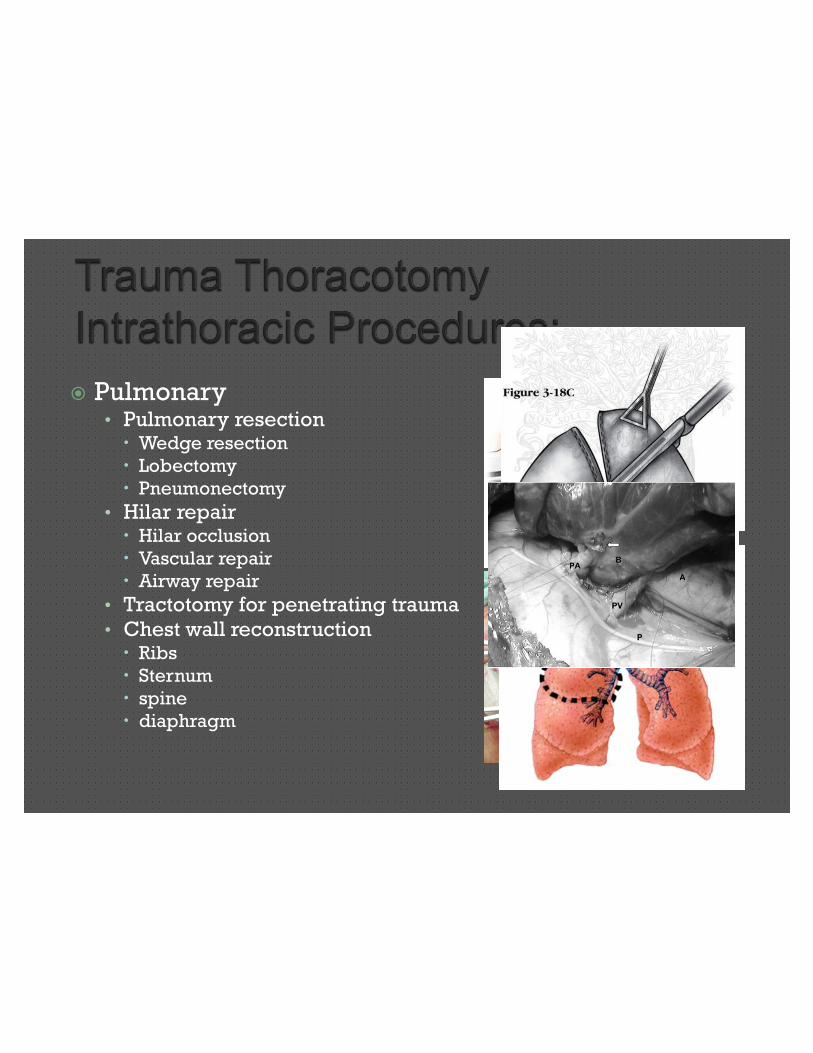
� Pulmonary• Pulmonary resectionx Wedge resection
x Lobectomy
x Pneumonectomy
• Hilar repairx Hilar occlusion
x Vascular repair
x Airway repair
• Tractotomy for penetrating trauma• Chest wall reconstructionx Ribs
x Sternum
x spine
x diaphragm
�Airway Obstruction
�Hemothorax
�Tension Pneumothorax
�Cardiac Tamponade
�Major Vascular Injury
�Air Embolization


�20 year old female driver of an
automobile which crashed head-on into
another vehicle at 80 mph
�Admitted to ER with HR 110; BP 121/60
�Head trauma: GCS 4
�What procedure should be done first?

• Thoracic Examination: • Crepitus at right chest wall• Absent right-sided breath sounds• Hypoxemia
�What procedure should be performed next?�A right-sided chest-tube is placed.�The patient became profoundly
hemodynamically unstable.

�What procedure should be performed next?
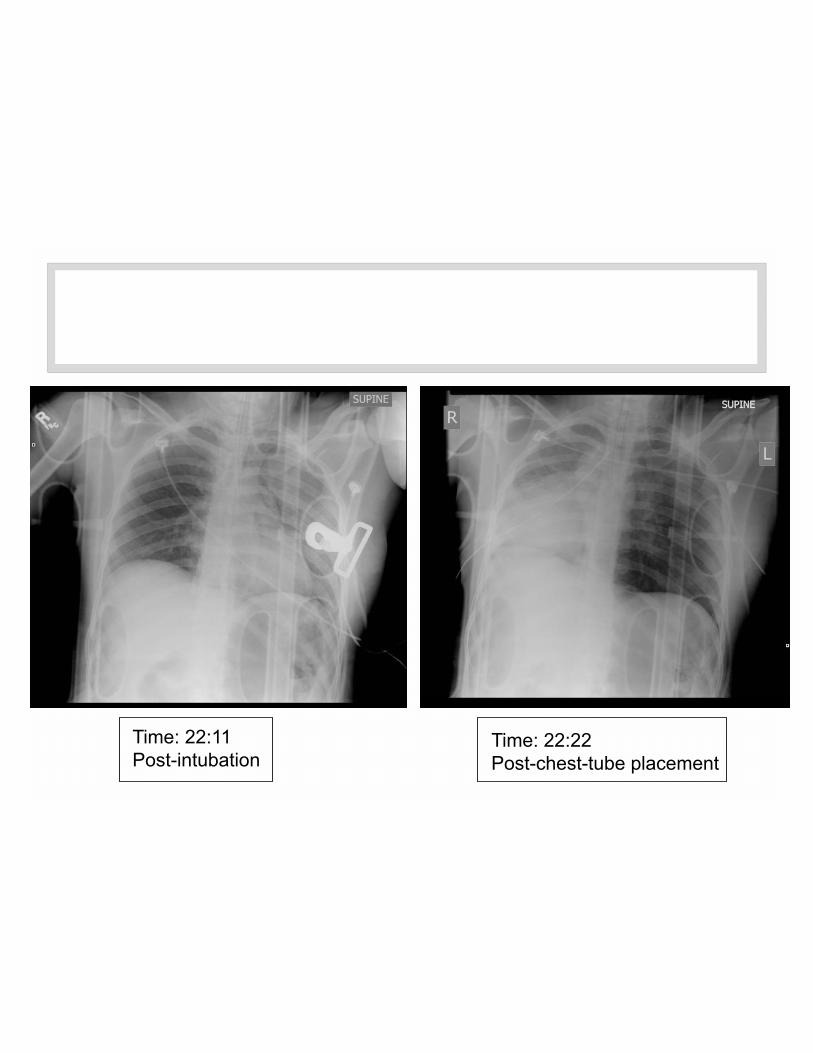
Time: 22:11Post-intubation
Time: 22:22Post-chest-tube placement

�What procedure should be performed next?
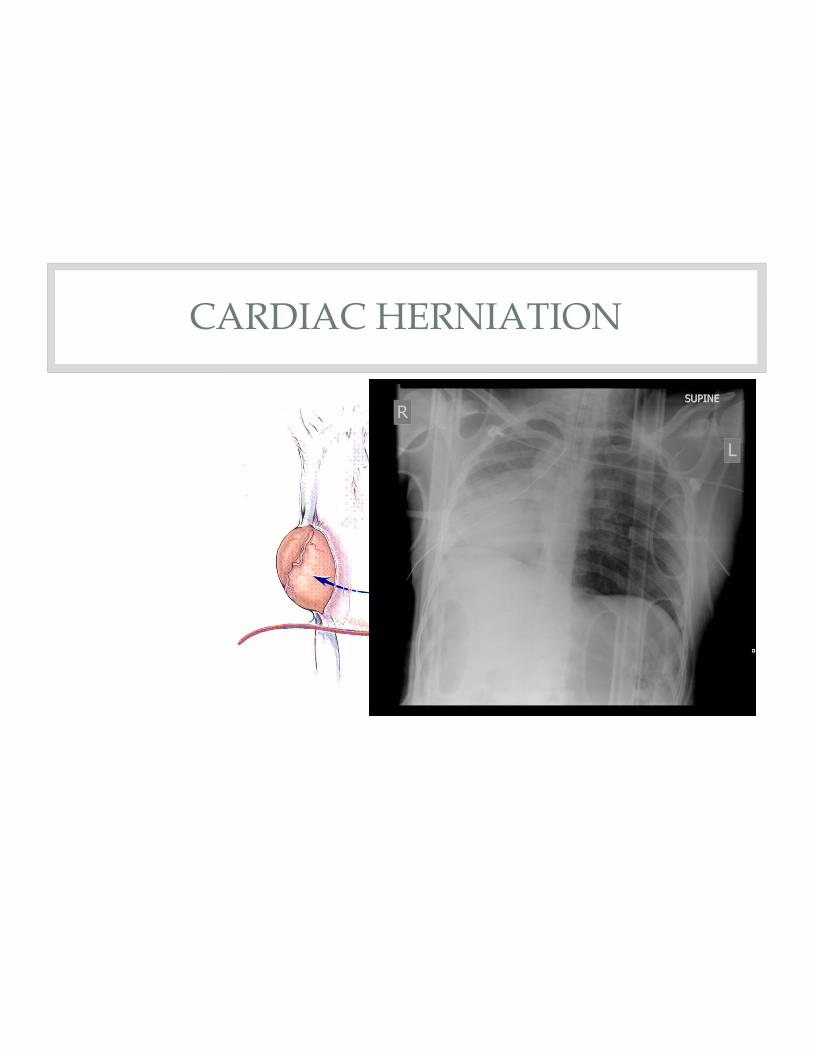
CARDIAC HERNIATION

Cardiac Herniation

• Overall 0-70%
• Penetrating 9-70%x Stab wounds 70%x GSW 9-33%
• Blunt 0-2.5 %
Asensio JA, Berne JD, Demetriades D et al. 'One hundred five penetrating cardiac injuries: A 2-year prospective evaluation'. J Trauma 1998;44:1073-108 Karmy-Jones R, Jurkovich GJ, Nathens AB et al. 'Timing of Urgent Thoracotomy for Hemorrhage After Trauma: A Multicenter Study.' Arch Surg 2001;136:513-518 Tyburski JG, Astra L, Wilson RF et al. 'Factors affecting prognosis with penetrating wounds of the heart'. J Trauma 2000;48:587-590 Rhee PM, Acosta J, Bridgeman A et al. 'Survival after emergency department thoracotomy: review of published data from the past 25 years.' J Am Coll Surg 2000;190:288-298 Branney SW, Moore EE, Feldhaus KM et al. ' Critical analysis of two decades of experience with postinjury emergency department thoracotomy in a regional trauma center'. J Trauma 1998;45:87-95 Campbell NC, Thomson SR, Muckart DJJ.' Review of 1198 cases of penetrating cardiac trauma'. Br J Surg 1997;84:1737-1740

�Blunt thoracic trauma – another example
of blunt trauma which requires
thoracotomy…
� Incisions:• Thoracotomy
• Median sternotomy
• (Laparotomy)
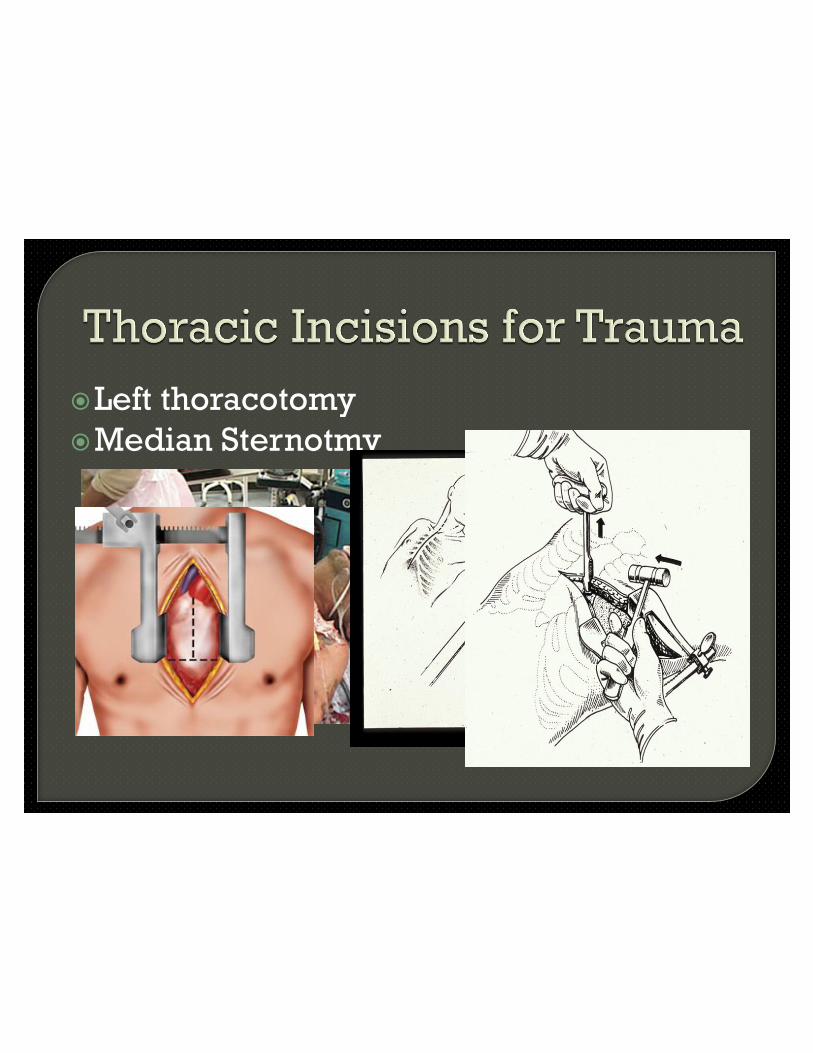
�Left thoracotomy
�Median Sternotmy

Flail Chest

Flail Chest
• Overall 0-70%
• Penetrating 9-70%x Stab wounds 70%x GSW 9-33%
• Blunt 0-2.5 %
Asensio JA, Berne JD, Demetriades D et al. 'One hundred five penetrating cardiac injuries: A 2-year prospective evaluation'. J Trauma 1998;44:1073-108 Karmy-Jones R, Jurkovich GJ, Nathens AB et al. 'Timing of Urgent Thoracotomy for Hemorrhage After Trauma: A Multicenter Study.' Arch Surg 2001;136:513-518 Tyburski JG, Astra L, Wilson RF et al. 'Factors affecting prognosis with penetrating wounds of the heart'. J Trauma 2000;48:587-590 Rhee PM, Acosta J, Bridgeman A et al. 'Survival after emergency department thoracotomy: review of published data from the past 25 years.' J Am Coll Surg 2000;190:288-298 Branney SW, Moore EE, Feldhaus KM et al. ' Critical analysis of two decades of experience with postinjury emergency department thoracotomy in a regional trauma center'. J Trauma 1998;45:87-95 Campbell NC, Thomson SR, Muckart DJJ.' Review of 1198 cases of penetrating cardiac trauma'. Br J Surg 1997;84:1737-1740