
ART Update 2015
39
Joel E. Gallant, MD, MPH Medical Director of Specialty Services Southwest CARE Center Santa Fe, New Mexico Adjunct Professor of Medicine Division of Infectious Diseases Johns Hopkins University School of Medicine Baltimore, Maryland ART Update 2015 Supported by educational grants from AbbVie, Bristol- Myers Squibb, Gilead Sciences, Janssen Therapeutics, Merck and ViiV.
-
Upload
hivlife-info -
Category
Health & Medicine
-
view
757 -
download
0
Transcript of ART Update 2015
Joel E. Gallant, MD, MPHMedical Director of Specialty Services Southwest CARE CenterSanta Fe, New MexicoAdjunct Professor of MedicineDivision of Infectious DiseasesJohns Hopkins University School of MedicineBaltimore, Maryland
ART Update 2015
Supported by educational grants from AbbVie, Bristol-Myers Squibb, Gilead Sciences, Janssen Therapeutics, Merck and ViiV.
clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
About These Slides
Users are encouraged to use these slides in their own noncommercial presentations, but we ask that content and attribution not be changed. Users are asked to honor this intent
These slides may not be published or posted online without permission from Clinical Care Options (email [email protected])
DisclaimerThe materials published on the Clinical Care Options Web site reflect the views of the authors of the CCO material, not those of Clinical Care Options, LLC, the CME providers, or the companies providing educational grants. The materials may discuss uses and dosages for therapeutic products that have not been approved by the United States Food and Drug Administration. A qualified healthcare professional should be consulted before using any therapeutic product discussed. Readers should verify all information and data before treating patients or using any therapies described in these materials.

clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
Disclosures
Joel E. Gallant, MD, MPH, has disclosed that he has received consulting fees from Bristol-Myers Squibb, Gilead Sciences, Janssen, Merck, and ViiV and funds for research support from AbbVie, Bristol-Myers Squibb, Gilead Sciences, Janssen, Merck, Sangamo, and ViiV.
clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
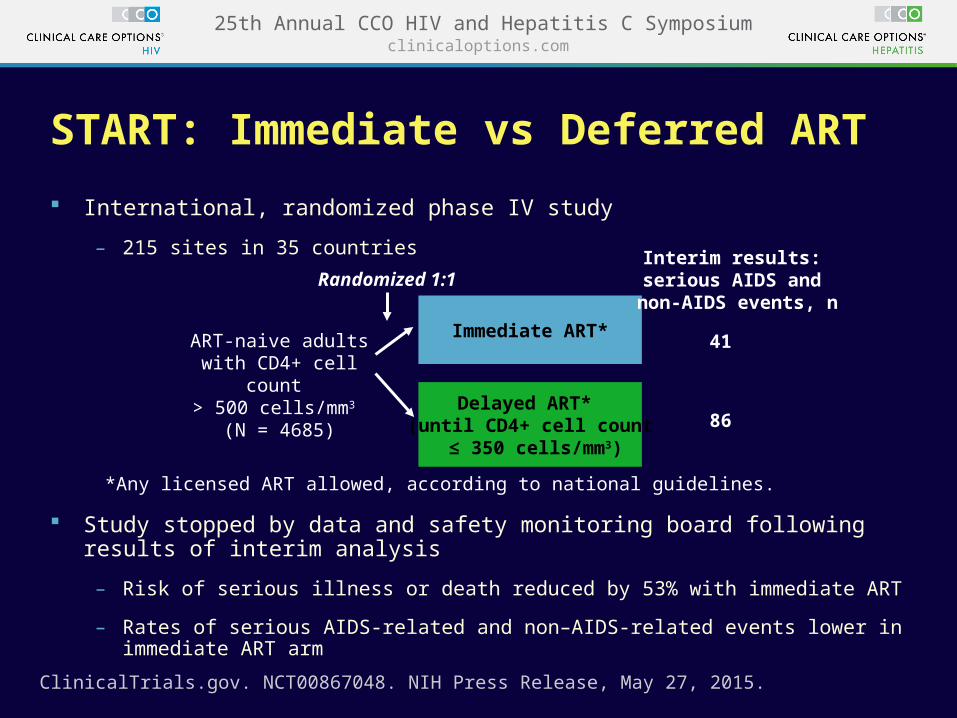
START: Immediate vs Deferred ART
International, randomized phase IV study
– 215 sites in 35 countries
Study stopped by data and safety monitoring board following results of interim analysis
– Risk of serious illness or death reduced by 53% with immediate ART
– Rates of serious AIDS-related and non–AIDS-related events lower in immediate ART arm
ART-naive adults with CD4+ cell count > 500 cells/mm3
(N = 4685)
Immediate ART*
Delayed ART* (until CD4+ cell count
≤ 350 cells/mm3)
Randomized 1:1Interim results:
serious AIDS and non-AIDS events, n
41
86
*Any licensed ART allowed, according to national guidelines.
ClinicalTrials.gov. NCT00867048. NIH Press Release, May 27, 2015.

clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
When to Start Therapy:Balance Now Favors Early ART
Drug toxicity Preservation of limited Rx
options Risk of resistance (and
transmission of resistant virus)
↑ potency, durability, simplicity, safety of current regimens
↓ emergence of resistance ↓ toxicity with earlier therapy ↑ subsequent treatment options Risk of uncontrolled viremia at all CD4
levels ↓ transmission
Delayed ART Early ART

clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
DHHS Guidelines, April 2015: What to Start
NNRTIs and ATV/r, previously classified as “recommended,” are now “alternative regimens”
DHHS Guidelines. April 2015.
*Only for pts who are HLA-B*5701 negative. †Only for pts with pre-ART CrCl ≥ 70 mL/min.
Recommended Regimens
INSTI based DTG/ABC/3TC*DTG + TDF/FTC
EVG/COBI/TDF/FTC†
RAL + TDF/FTC
PI based DRV/r + TDF/FTC

clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
DHHS Guidelines, April 2015: What to Start
DHHS Guidelines. April 2015.
*Only for pts with pre-ART HIV-1 RNA < 100,000 copies/mL and CD4+ > 200 cells mm3.†Only for pts with pre-ART CrCl ≥ 70 mL/min.‡Only for pts who are HLA-B*5701 negative.
Alternative Regimens
NNRTI based EFV/TDF/FTCRPV/TDF/FTC*
PI based ATV/COBI + TDF/FTC†
ATV/r + TDF/FTC DRV/COBI + ABC/3TC‡
DRV/r + ABC/3TC‡
DRV/COBI + TDF/FTC†
An alternative regimen may be the preferred regimen for some pts

clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
Integrase Inhibitors

clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
Difference in 96-wk cumulative incidence (97.5% CI)
-20 0-10 10 20
15% (10% to 20%)
7.5% (3.2% to 12%)
7.5% (2.3% to 13%)
ATV/r vs RAL
DRV/r vs RAL
ATV/r vs DRV/r
Favors RAL
Favors RAL
Favors DRV/r
Lennox JL, et al. Ann Intern Med. 2014;161:461-471.
*Plus TDF/FTC.
ATV/r*RAL*DRV/r*
ACTG 5257: Cumulative Incidence of Virologic or Tolerability Failure
1.00
0.75
0.50
0.25
0.00
Cu
mu
lati
ve In
cid
ence
Wks Since Study Entry
0 24 48 64 80 96 112 128 144

clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
Toxicities Associated With Discontinuation, n (%)
ATV/r†
(n = 605)RAL†
(n = 603)DRV/r†
(n = 601)
Any 95 (16%) 8 (1%) 32 (5%)
Gastrointestinal toxicity 25 2 14
Jaundice/hyperbilirubinemia 47 0 0
Other hepatic toxicity 4 1 5
Skin toxicity 7 2 5
Metabolic toxicity 6 0 2
Renal toxicity (all nephrolithiasis) 4 0 0
Abnormal chem/heme (excl. LFTs) 0 0 2
Other toxicity 2 3 4
*Participants allowed to switch therapy for intolerable toxicity.†Plus TDF/FTC.
Lennox JL, et al. Ann Intern Med. 2014;161:461-471.
ACTG 5257: Tolerability FailureToxicity-Associated Discontinuation of Randomized ART*

clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
GS 102: EVG/COBI/TDF/FTC Noninferior to EFV/TDF/FTC Through Wk 144
1. Sax PE, et al. Lancet. 2012;379:2439-2448. 2. Zolopa A, et al. J Acquir Immune Defic Syndr. 2013;63:96-100. 3. Wohl D, et al. J Acquir Immune Defic Syndr. 2014;65:e118-e120.
Wk 48
Wk 144
EVG/COBI/TDF/FTC (n = 348)
EFV/TDF/FTC (n = 352)
8075
8884 8482
Wk 96
7 7 6 8 7 105
9 9 11 12 15
Wk 48
Wk 144
Wk 96
Wk 48
Wk 144
Wk 96
Virologic Success Virologic Failure No Data
95% CI for Difference
Wk 48[1]
Wk 96[2]
Wk 144[3]
-12% 12%0
Favors EFV
Favors EVG/COBI
-1.3% 11.1%
4.9%
3.6%
8.8%
2.7%
-1.6%
-2.9%
0
20
40
60
80
100
8.3%

clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
GS 103: EVG/COBI/TDF/FTC Noninferior to ATV/r + TDF/FTC Through Wk 144
1. DeJesus E, et al. Lancet. 2012;379:2429-2438. 2. Rockstroh J, et al. J Acquir Immune Defic Syndr. 2013;62:483-486. 3. Clumeck N, et al. J Acquir Immune Defic Syndr. 2014;65:e121-e124.
EVG/COBI/TDF/FTC (n = 353)
ATV/RTV + TDF/FTC (n = 355)
7875
9087
Wk 48
Wk 144
0
20
40
60
80
100
Wk 96
Wk 48
Wk 144
Wk 96
Wk 48
Wk 144
Wk 96
Virologic Success Virologic Failure No Data
8382
5 5 57 7 78 8 101014
18
-12% 12%0
Favors ATV/RTV
Favors EVG/COBI
-3.2% 9.4%
3.1%
2.7%
7.5%1.1%
6.7%
-2.1%
-4.5%
Wk 48[1]
Wk 96[2]
Wk 144[3]
95% CI for Difference

clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
SINGLE: DTG + ABC/3TC Superior to EFV/TDF/FTC in ART-Naive Pts to Wk 144 Open-label extension, excluding pts with HBV Emergent resistance in those with VF: 0/39 (DTG) vs 7/33 (EFV)
Virologic Success*
Virologic Nonresponse
No Virologic Data
Pts
(%
)
FavorsEFV/TDF/FTC
95% CI for Difference
0
Wk 48
Wk 96
Wk 144
7.4%
8.0%
8.3%
2.5%
2.3%
2.0% 14.6%
13.8%
12.3%
FavorsDTG + ABC/3TC
15%
Pappa K, et al. ICAAC 2014. Abstract H-647a.
8881 80
72 7163
5 6 7 8 107 7
13 1220
30
18
100
80
60
40
20
0
DTG + ABC/3TC QD (n = 414)EFV/TDF/FTC QD (n = 419)
Wk 48 96 144 Wk 48 96 144 Wk 48 96 144
*HIV-1 RNA < 50 copies/mL as defined by FDA Snapshot algorithm.-10% noninferiority margin.
-15%

clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
FLAMINGO: DTG Superior to DRV/r in ART-Naive Pts to Wk 96
Virologic Success Virologic Nonresponse No Virologic Data
FavorsDRV/r
95% CI for Difference
0%-12%
Wk 48
Wk 96
7.1%
12.4%
0.9%
4.7% 20.2%
13.2%
Su
bje
cts
(%
)
FavorsDTG
25%
DTG 50 mg QD + 2 NRTIs (n = 242)
DRV/r 800 mg/100 mg QD + 2 NRTIs (n = 242)
Molina et al. HIV Drug Therapy Glasgow 2014; Glasgow, UK. Slides O153.
0
20
40
60
80
100
W48 W48 W48W96 W96 W96
9083
80
68
6 7 812
410 12
21

clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
Comparing the Integrase Inhibitors
Agent Advantages Disadvantages
Raltegravir Longest experience Fewer drug interactions than
EVG, DTG
Twice daily dosing (for now) No coformulation
Elvitegravir Single-tablet regimen (STR) Once-daily dosing
Requires COBI boosting COBI drug interactions similar to
RTV
Dolutegravir The only non-TDF–containing STR
Once-daily dosing Higher barrier to resistance Few drug interactions Active against some RAL- and
EVG-resistant virus
Coformulated with ABC/3TC only
Together, the results of STARTMRK, GS 102 and 103, SINGLE, FLAMINGO, and ACTG 5257 suggest that integrase inhibitor–based regimens are the preferred starting
regimens in the majority of pts

clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
PIs

clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
Difference in 96-wk cumulative incidence (97.5% CI)
-20 0-10 10 20
15% (10% to 20%)
7.5% (3.2% to 12%)
7.5% (2.3% to 13%)
ATV/r vs RAL
DRV/r vs RAL
ATV/r vs DRV/r
Favors RAL
Favors RAL
Favors DRV/r
Lennox JL, et al. Ann Intern Med. 2014;161:461-471.
*Plus TDF/FTC.
ATV/r*RAL*DRV/r*
ACTG 5257: Cumulative Incidence of Virologic or Tolerability Failure
1.00
0.75
0.50
0.25
0.00
Cu
mu
lati
ve In
cid
ence
Wks Since Study Entry
0 24 48 64 80 96 112 128 144
clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
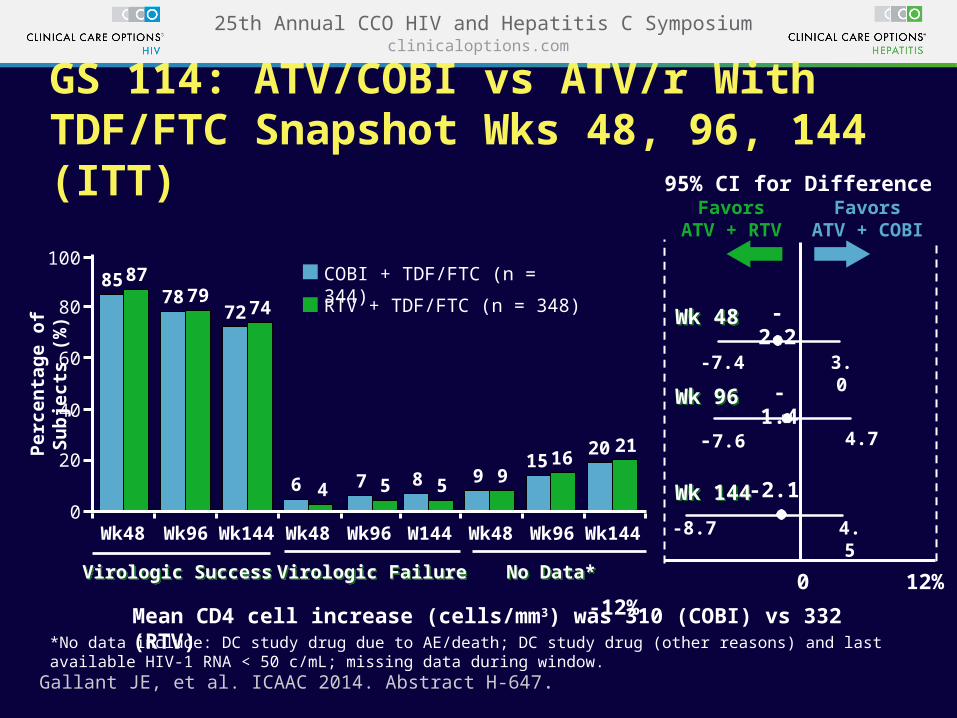
GS 114: ATV/COBI vs ATV/r With TDF/FTC Snapshot Wks 48, 96, 144 (ITT)
*No data include: DC study drug due to AE/death; DC study drug (other reasons) and last available HIV-1 RNA < 50 c/mL; missing data during window.
Per
cen
tag
e o
f S
ub
ject
s (%
)
Virologic SuccessVirologic Success Virologic FailureVirologic Failure No Data*No Data*
95% CI for Difference
-7.4 3.0
FavorsATV + RTV
-2.2
FavorsATV + COBI
Wk 48Wk 48
-7.6 4.7
-1.4Wk 96Wk 96
4.5-8.7
-2.1Wk 144Wk 144
Mean CD4 cell increase (cells/mm3) was 310 (COBI) vs 332 (RTV)
12% 0 -12%
Gallant JE, et al. ICAAC 2014. Abstract H-647.
100
80
60
40
20
0Wk48 Wk96 Wk144 Wk48 Wk96 W144 Wk48 Wk96 Wk144
85 8778 79
72 74
6 4 7 5 8 5 9 915 16 20 21
COBI + TDF/FTC (n = 344)
RTV + TDF/FTC (n = 348)

clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
Now Approved: New Boosted PI Fixed-Dose Combinations ATV/COBI 300/150 mg once daily[1]
DRV/COBI 800/150 mg once daily[2]
– Only for pts with no DRV resistance mutations
Both FDCs added as “alternative regimen” options in DHHS guidelines[3]
1. Atazanavir/cobicistat prescribing information 2015.2. Darunavir/cobicistat prescribing information 2015.3. DHHS Guidelines. April 2015.

clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
NRTIs
clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
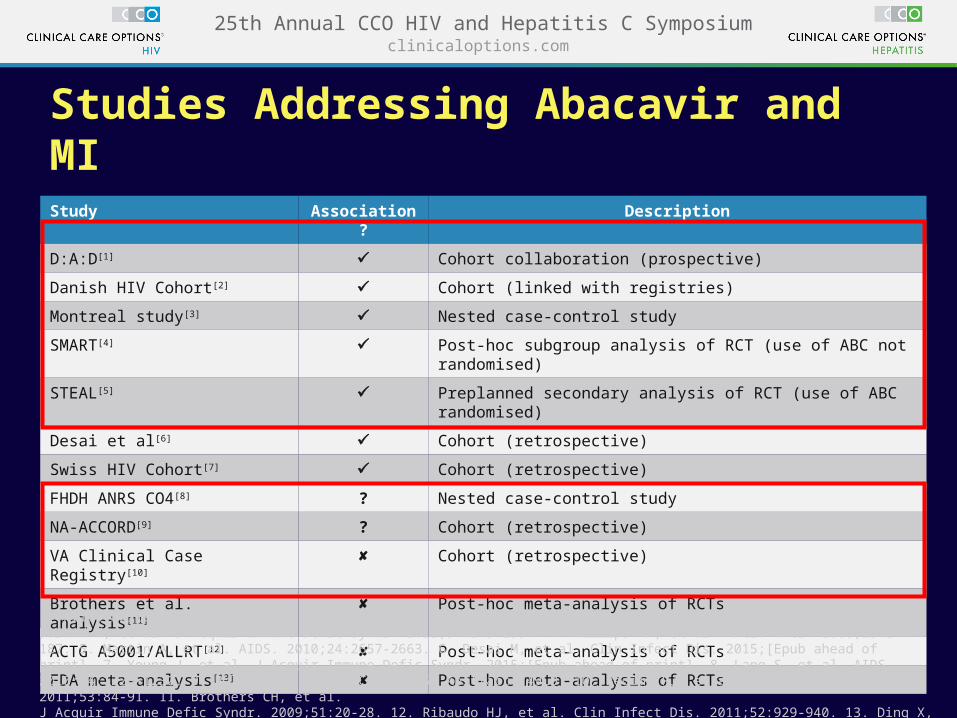
Study Association? Description
D:A:D[1] Cohort collaboration (prospective)
Danish HIV Cohort[2] Cohort (linked with registries)
Montreal study[3] Nested case-control study
SMART[4] Post-hoc subgroup analysis of RCT (use of ABC not randomised)
STEAL[5] Preplanned secondary analysis of RCT (use of ABC randomised)
Desai et al[6] Cohort (retrospective)
Swiss HIV Cohort[7] Cohort (retrospective)
FHDH ANRS CO4[8] ? Nested case-control study
NA-ACCORD[9] ? Cohort (retrospective)
VA Clinical Case Registry[10] Cohort (retrospective)
Brothers et al. analysis[11] Post-hoc meta-analysis of RCTs
ACTG A5001/ALLRT[12] Post-hoc meta-analysis of RCTs
FDA meta-analysis[13] Post-hoc meta-analysis of RCTs
1. Friis-Møller N, et al. N Engl J Med. 2003;349:1993-2003. 2. Obel N, et al. HIV Med. 2010;11:130-136. 3. Durand M, et al. J Acquir Immune Defic Syndr. 2011;57:245-253. 4. Phillips AN, et al. Antiv Ther. 2008;13:177-187. 5. Martin A, et al. AIDS. 2010;24:2657-2663. 6. Desai M, et al. Clin Infect Dis. 2015;[Epub ahead of print]. 7. Young J, et al. J Acquir Immune Defic Syndr. 2015;[Epub ahead of print]. 8. Lang S, et al. AIDS. 2010;24:1228-1230. 9. Palella F, et al. CROI 2015. Abstract 749LB. 10. Bedimo RJ, et al. Clin Infect Dis. 2011;53:84-91. 11. Brothers CH, et al. J Acquir Immune Defic Syndr. 2009;51:20-28. 12. Ribaudo HJ, et al. Clin Infect Dis. 2011;52:929-940. 13. Ding X, et al. J Acquir Immune Defic Syndr. 2012;61:441-447.
Studies Addressing Abacavir and MI

clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
Nuke-Sparing and “Nuke-Lite” Regimens
Regimen Results
DRV/r + RAL (ACTG 5262)[1] Poor performance at high VL
DRV/r + RAL (NEAT)[2] Less effective at high VL, low CD4
DRV/r + MVC (MODERN)[3] Less effective than standard ART
ATV/r + RAL (HARNESS – switch)[4] Less effective than standard ART
LPV/r + RAL (PROGRESS)[5] Small study; few pts with high VL
LPV/r + EFV (ACTG 5142)[6] Poorly tolerated but effective
LPV/r + 3TC (GARDEL)[7] As effective as standard ART
LPV/r + 3TC or FTC (OLE – switch)[8] As effective as standard ART
ATV/r + 3TC (SALT – switch)[9] As effective as standard ART
1. Taiwo B, et al. AIDS. 2011;25:2113-2122. 2. Raffi, et al. CROI 2014. Abstract 84LB. 3. Stellbrink HJ, et al. IAD 2014. Abstract MOAB0101. 4. Van Lunzen J, et al. IAC 2014. Abstract A-641-0126-11307. 5. Reynes J, et al. AIDS Res Hum Retroviruses. 2013;29:256-265. 6. Daar ES, et al. Ann Intern Med. 2011;154:445-456. 7. Cahn P, et al. Lancet Infect Dis. 2014;14:572-580. 8. Gatell J, et al. AIDS 2014. Abstract LBPE17. 9. Perez-Molina JA, et al. IAC 2014. Abstract LBPE18.

clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
How to Select a Nuke-Sparing Regimen When You Need One? All NRTI-sparing regimens should include a boosted PI . . .
for now
– LPV/r + EFV was effective but poorly tolerated, but other PI/NNRTI combinations could be considered
– Boosted PI + INSTI may not be enough
My choices:
– DRV/c + DTG + (3TC or FTC)
– DRV/c + ETR (+/- 3TC or FTC)
– DRV/c + (3TC or FTC)?

clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
LATTE: NRTI-Sparing Maintenance With Cabotegravir + Rilpivirine
6 pts in CAB arms with PDVF at Wk 96; 4 additional pts since Wk 48
Margolis D, et al. CROI 2015. Abstract 554LB.
VL
< 5
0 c/
mL
by
Sn
apsh
ot
Alg
ori
thm
(%
)
100
80
60
40
20
0BL 4 12 24 28 36 48 72 96
Induction Phase Maintenance Phase (NRTI Sparing)
CAB 10 mg + 2 NRTIs* CAB + RPV (n = 60) CAB 30 mg + 2 NRTIs* CAB + RPV (n = 60)†
CAB 60 mg + 2 NRTIs* CAB + RPV (n = 61)EFV 600 mg + 2 NRTIs* (n = 62)
68%63%
84%
75%
Wks
*TDF/FTC or ABC/3TC.†Cabotegravir 30 mg selected for future development.
Induction Regimen Maintenance Regimen

clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
Virologic Success*
Virologic Failure
No Data
Studies 104/111: TAF Noninferior to TDF at Wk 48
TAF also noninferior to TDF at Wk 48 in each study (104 and 111)
Results similar across all baseline virologic and demographic subgroups
7 pts in TAF arm and 5 pts in TDF arm with NRTI resistance at VF
– 1 in TAF arm and 2 in TDF arm with combined M184V/I + K65R
5 pts in TAF arm and 3 pts in TDF arm with INSTI resistance at VF
0.9% in TAF arm and 1.5% in TDF arm discontinued due to AE
CD4+ increases greater in TAF arm: 211 vs 181 (P = .024)
Pts
(%
)
9290
Δ +2.0%(95% CI: -0.7% to +4.7)
EVG/COBI/FTC/TAF (n = 866)EVG/COBI/FTC/TDF (n = 867)
0
20
40
60
80
100
4 4 4 6
n =
*HIV-1 RNA < 50 c/mL as defined by FDA Snapshot algorithm.Discontinued for AE, death, or missing data.
800 784
Wohl DA, et al. CROI 2015. Abstract 113LB.

clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
TAF vs TDF: Renal Safety
EVG/COBI/FTC/TAF(n = 866)
EVG/COBI/FTC/TDF(n = 867)
Events, n (%)Renal adverse events leading to discontinuation 0 4 (0.5)
Tubulopathy/Fanconi syndrome 0 0
-6.6P < .001
-11.2
Sax P, et al. CROI 2015. Abstract. 143LB.
20
10
0
-10
-20Mea
n (
SD
) C
han
ge
Fro
m B
asel
ine
eGF
R*
0Time (Wks)
12 24 36 48
EVG/COBI/FTC/TAF
EVG/COBI/FTC/TDF

clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
TAF vs TDF: Quantitative Proteinuria
Med
ian
% C
han
ge
Fro
m B
asel
ine
(Q1
, Q
3)
β2- microglobulin
P < .001for all
Baseline44
mg/g44
mg/g5
mg/g5
mg/g64
μg/g 67
μg/g 101
μg/g 103
μg/g
Protein (UPCR)
Albumin (UACR)
Retinol-binding protein
Sax P, et al. CROI 2015. Abstract. 143LB.
76* 133* 168*
-57*
*Upper or lower limit of error bar.
EVG/COBI/FTC/TAFEVG/COBI/FTC/TAF
EVG/COBI/FTC/TDFEVG/COBI/FTC/TDF
75
50
25
0
-25
-50
-3
20
-5
7 9
51
-32
24

clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
Switch to EVG/COBI/FTC/TAF in Renal Impairment
Change in eGFR (Cockcroft-Gault)
0 4 8 12 16 24 36 48-10
-5
0
5
10
15
0.6-1.4
Primary Endpoint
Me
dia
n (
Q1
, Q
3)
eG
FR
C
ha
ng
e F
rom
B
as
eli
ne
(m
L/m
in)
Baseline eGFR < 50 mL/min (n = 80) ≥ 50 mL/min (n = 162)
Retinol Binding Protein/Creatinine RatioWks
-40
-20
0
Me
dia
n %
Ch
an
ge
in
RB
P/C
rea
tin
ine
Ra
tio
(µ
g/g
)
P < .001 at all time points (for all pts combined)
-80
-60
-100
01 4 12 24 482
β2-Microglobulin/Creatinine Ratio
-40
-20
0
Me
dia
n %
Ch
an
ge
in
ß2-
M/C
rea
tin
ine
Ra
tio
(µ
g/g
)
-80
-60
-100 P < .001 at all time points (for all pts combined)
Wks01 4 12 24 482
Pozniak A, et al. CROI 2015. Abstract 795.
Baseline eGFRCG
< 50 mL/min ≥ 50 mL/min
65% receiving TDF at baseline

clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
EVG/COBI/TAF/FTC
TAF/FTC
RPV/TAF/FTC
clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
In the Pipeline
DRV/COBI/TAF/FTC: STR
Doravirine[1]: NNRTI
– Active against K103N, Y181C
Ibalizumab[2]: entry inhibitor
– Monoclonal antibody binds CD4
– Being studied for treatment and prevention
BMS-663068[3]: entry inhibitor
– Blocks attachment by binding to gp120
BMS 955176[4]: maturation inhibitor
– Disrupts processing of gag protein
– Trial in naive pts planned
1. Morales-Ramirez J, et al. CROI 2014. Abstract 92LB 2. Ernst J, et al. ICAAC 2014. Abstract H-995. 3. Lalezari J, et al. CROI 2014. Abstract 86. 4. Hwang C, et al. CROI 2015. Abstract 114LB.

clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
What to Start?(My personal recommendations) No comorbidities or interacting medications
– DTG/ABC/3TC
– EVG/COBI/FTC/TDF
High cardiac risk
– DTG + TDF/FTC
– EVG/COBI/FTC/TDF
Kidney disease (low cardiac risk)
– DTG/ABC/3TC (expect fall in eGFR)
– RAL + ABC/3TC
RTV or COBI interactions
– DTG/ABC/3TC
– DTG + TDF/FTC
– RAL + TDF/FTC

clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
How to Choose?(My personal recommendations) Adverse effects or desire for simplification
on a suppressive regimen
– DTG/ABC/3TC (no switch data yet, but why not?)
– EVG/COBI/TDF/FTC
– RPV/TDF/FTC
Known or predicted nonadherence
– DRV/COBI + TDF/FTC (compare with DHHS)
– DTG/ABC/3TC (?)
Likelihood of pregnancy
– ATV/r + TDF/FTC
HCV coinfection
– DTG/ABC/3TC (or TDF/FTC)
– RAL + TDF/FTC

Switching and Simplifying Therapy in Suppressed Patients
clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
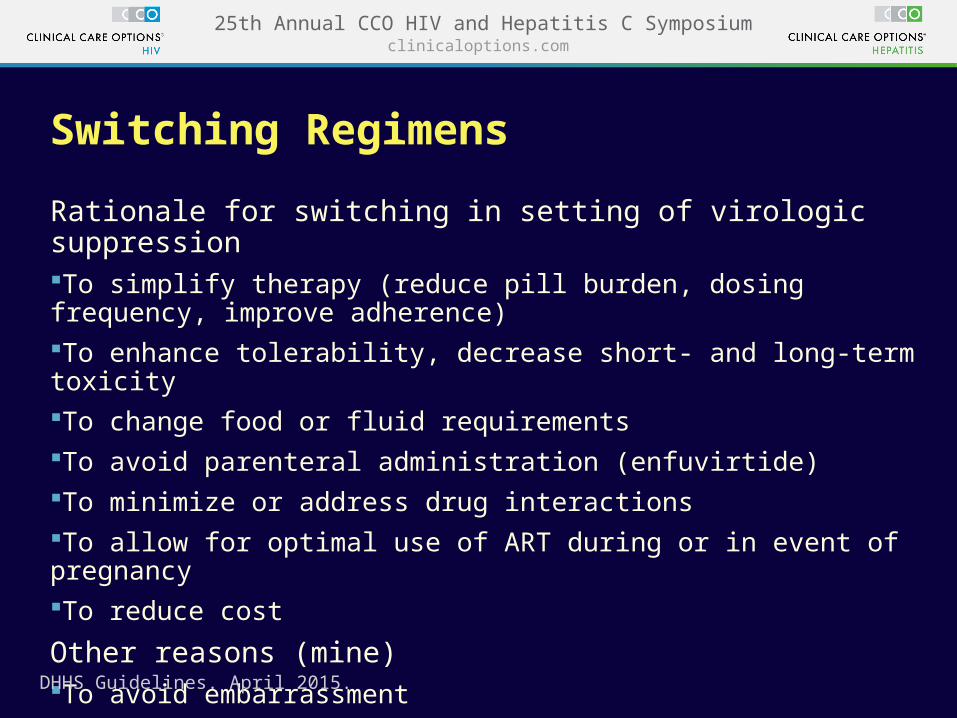
Switching Regimens
Rationale for switching in setting of virologic suppressionTo simplify therapy (reduce pill burden, dosing frequency, improve adherence)To enhance tolerability, decrease short- and long-term toxicityTo change food or fluid requirementsTo avoid parenteral administration (enfuvirtide)To minimize or address drug interactionsTo allow for optimal use of ART during or in event of pregnancyTo reduce cost
Other reasons (mine)To avoid embarrassmentTo prevent boredom
DHHS Guidelines. April 2015.
clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
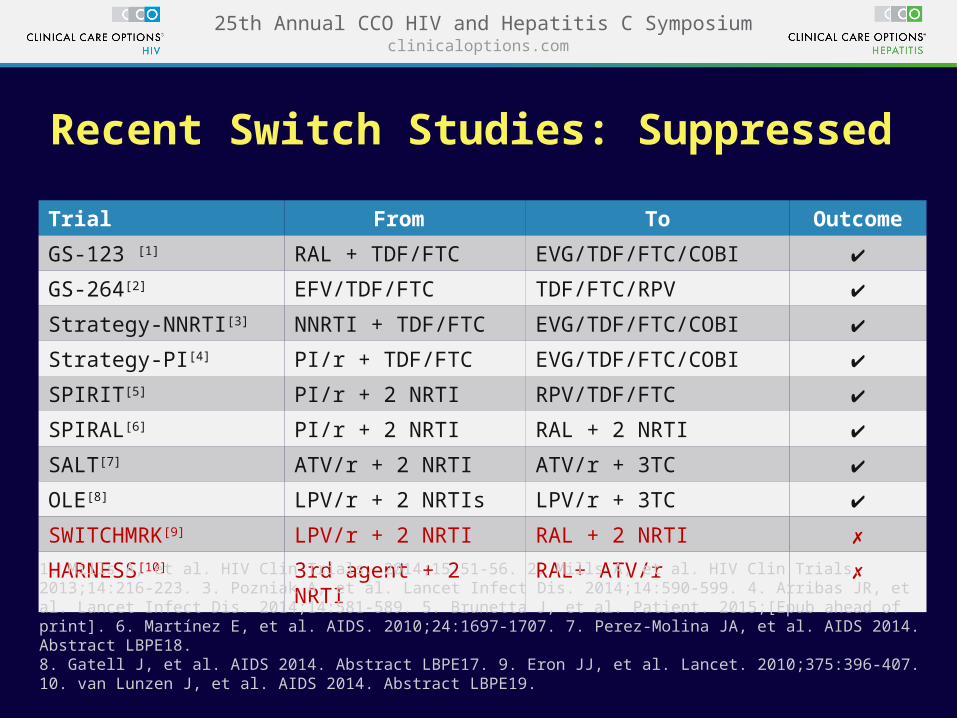
Recent Switch Studies: Suppressed
Trial From To Outcome
GS-123 [1] RAL + TDF/FTC EVG/TDF/FTC/COBI ✔
GS-264[2] EFV/TDF/FTC TDF/FTC/RPV ✔
Strategy-NNRTI[3] NNRTI + TDF/FTC EVG/TDF/FTC/COBI ✔
Strategy-PI[4] PI/r + TDF/FTC EVG/TDF/FTC/COBI ✔
SPIRIT[5] PI/r + 2 NRTI RPV/TDF/FTC ✔
SPIRAL[6] PI/r + 2 NRTI RAL + 2 NRTI ✔
SALT[7] ATV/r + 2 NRTI ATV/r + 3TC ✔
OLE[8] LPV/r + 2 NRTIs LPV/r + 3TC ✔
SWITCHMRK[9] LPV/r + 2 NRTI RAL + 2 NRTI ✗
HARNESS[10] 3rd agent + 2 NRTI RAL+ ATV/r ✗
1. Mills A, et al. HIV Clin Trials. 2014;15:51-56. 2. Mills A, et al. HIV Clin Trials. 2013;14:216-223. 3. Pozniak A, et al. Lancet Infect Dis. 2014;14:590-599. 4. Arribas JR, et al. Lancet Infect Dis. 2014;14:581-589. 5. Brunetta J, et al. Patient. 2015;[Epub ahead of print]. 6. Martínez E, et al. AIDS. 2010;24:1697-1707. 7. Perez-Molina JA, et al. AIDS 2014. Abstract LBPE18. 8. Gatell J, et al. AIDS 2014. Abstract LBPE17. 9. Eron JJ, et al. Lancet. 2010;375:396-407. 10. van Lunzen J, et al. AIDS 2014. Abstract LBPE19.

clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
Switching: Caveats
Know the treatment and resistance history
Avoid switching from high barrier to lower barrier agents when you don’t

clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
Switching and Simplifying Therapy: “Horizontal” vs “Vertical” SwitchesVertical Switches: switch to drug with lower resistance barrierMost drug discontinuations
Boosted PI → NNRTI
Boosted PI → INSTI
Boosted PI → any STR
DRV/r twice daily → once daily
Horizontal Switches: switch to drug with equal or higher resistance barrierRTV → COBI (boosters)
Switches within INSTI class in previously INSTI-naive pts
EFV or NVP → RPV or ETR
LPV/r or ATV/r → DRV/r
ABC or AZT → TDF
TDF → TAF
clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
Conclusions
Initial therapy
– Due to a combination of efficacy, safety, and tolerability, 4 of the 5 DHHS recommended regimens are now INSTI-based combinations
– DRV/r is the only recommended PI
– ATV/r, ETR, and RPV are now alternative agents
Some pts still need “nuke-sparing” or “nuke-lite” regimens
– DHHS guidelines list no NRTI-sparing regimen as “Recommended” or “Alternative”
– TAF may make this less necessary in the near future
Switching therapy in virologically suppressed pts is appropriate and safe, provided resistance profile and resistance barrier are considered

Go Online for More CCO Coverage of HIV!
Multimedia modules featuring video of expert faculty discussions of controversies and challenging cases
Downloadable slidesets for your own study or presentations
clinicaloptions.com/hiv


















