ART Progress 2016 R.M. Gulick, MD,...
42
ART Progress 2016 R.M. Gulick, MD, MPH Gladys and Roland Harriman Professor of Medicine Chief, Division of Infectious Diseases Weill Cornell Medical College New York City
Transcript of ART Progress 2016 R.M. Gulick, MD,...

ART Progress 2016
R.M. Gulick, MD, MPH Gladys and Roland Harriman Professor of Medicine
Chief, Division of Infectious Diseases Weill Cornell Medical College
New York City

Disclosures No financial interests or relationships to disclose. Co-Chair, U.S. DHHS Antiretroviral Guidelines Panel Member, Voluntary Board of Directors, International Antiviral Society (IAS)-USA
•

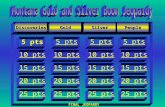
Life Expectancy: Kaiser Permanente • Kaiser Permanente California 1996-2011 • Individuals followed: 25,768 HIV+ and 257,600 HIV- • Deaths: 2229 (HIV+) and 4970 (HIV-) • Life expectancy (years) at age 20:
• 1996-2006: +36 (HIV+) vs. +62 (HIV-); ∆=26 • 2007-2011: +48 (HIV+); ∆=14
• lowest were among blacks (+45) and IDU (+43) • start ART CD4 >500 +54; ∆=9 • no history HBV, HCV, drug/ETOH/cigs ∆=6-7
Marcus CROI 2016 #54

ART: Questions
• When to start? • What to start? • When to change? • What to change to?

When to Start?

START (Strategic Timing of Antiretroviral Treatment Study): Design
HIV+, ART-naïve, CD4+ >500 cells/mm3
Immediate ART Group Initiate ART immediately
N=2,326
Deferred ART Group Defer ART until CD4+ <350 or AIDS
N=2,359
Primary composite endpoint, target = 213 Serious AIDS or death from AIDS Serious Non-AIDS Events and death not attributable to AIDS
– CVD, ESRD, decompensated liver disease, & non-AIDS defining cancers
Stopped early by DSMB; average f/u 3 years
INSIGHT, N Engl J Med 2015;373:795-807

START: Primary Endpoint
No. of Participants
Type of event Imm. ART Def. ART
Serious AIDS 14 50
Serious non-AIDS 29 47
Total* 42 (1.8%) 96 (4.1%)
* One participant in each group had both a Serious AIDS and a Serious Non-AIDS Event
HR 0.43 (0.30, 0.62; P<0.001)
Most common: AIDS events: TB, Lymphoma, Kaposi’s sarcoma, PCP, dissem VZV Non-AIDS events: Non-AIDS cancers, CV disease
INSIGHT, N Engl J Med 2015;373:795-807

START: Other Analyses
No difference (all groups benefit) by: age, sex, race, geography (low/middle vs. high income) cigarette smoking, Framingham risk baseline CD4, baseline VL
↑ risk of clinical events with ↑ age, ↓ CD4, ↑ Framingham score
Toxicity: no differences
Conclusion: ART benefits all
Implications (IAS 2015): Chile, Thailand, UK all changed to recommend ART for ALL WHO changed to recommend all in September 2015
INSIGHT, N Engl J Med 2015;373:795-807

When to Start?: Guidelines AIDS/
symptoms CD4 <200
CD4 200-350
CD4 350-500
CD4 >500
US DHHS 2016 www.aidsinfo.nih.gov
YES YES YES YES YES
IAS-USA 2014 JAMA 2014;312:390
YES YES YES YES YES
EACS 2015 www.europeanaidsclinicalsociety.org/
YES YES YES YES YES
UK 2015 www.bhiva.org
YES YES YES YES YES
WHO 2015 http://apps.who.int/iris/bitstream/10665/186275/1/9789241509565_eng.pdf
YES YES YES YES YES

What to Start?

Antiretroviral Drug Approval: 1987 - 2016
0
5
10
15
20
25
30
1987 1989 1991 1993 1995 1997 1999 2001 2003 2005 2007 2009 2011 2013 2015
AZT ddI ddC d4T
3TC SQV
RTV IDV NVP
NFV DLV
EFV ABC
APV LPV/r
TDF
ENF ATV FTC FPV TPV
DRV
ETR RAL MVC RPV
EVG DTG TAF

Recommended ART Regimens (2 NRTI + 3rd drug)
• Protease Inhibitor-based – TDF/FTC + DRV/r
• Integrase Inhibitor-based
– ABC/3TC/DTG – TDF/FTC + DTG – TAF/FTC/EVG/c – TDF/FTC/EVG/c – TDF/FTC + RAL
U.S. DHHS Guidelines 1/28/16 www.aidsinfo.nih.gov

ART Overview: U.S. Center for AIDS Research (CFAR) Network of Integrated Clinical Systems (CNICS) Cohort • 29,467 participants at 8
U.S. HIV clinics 19972014
• After 2010, predictors of VS were: older, white, male, ↑ adherence, integrase inhibitor use
Simoni CROI 2016 #1034

Newer ART Rx-Naïve Studies Study (reference) N Regimen VL <50 (96 wks)
ACTG 5257 Lennox Ann Intern Med 2014;161:461
605 2 NRTI + ATV/r 88%
601 2 NRTI + DRV/r 89% 603 2 NRTI + RAL 94%*
SINGLE Walmsley NEJM 2013;369:1807 + JAIDS 2015;70:515
414 ABC/3TC + DTG 80%*
419 TDF/FTC/EFV 72% FLAMINGO Molina Lancet 2014;383:2222 + Lancet HIV 2015;2:e127
242 2 NRTI + DTG 80%*
242 2 NRTI + DRV/r 68% * = significant difference

When to Change? US DHHS 2016 www.aidsinfo.nih.gov
confirmed HIV RNA >200
IAS-USA 2014 JAMA 2014;312:390
HIV RNA >200
EACS 2015 www.europeanaidsclinicalsociety.org/
confirmed HIV RNA >50 after 6 months of ART
UK 2015 www.bhiva.org
confirmed HIV RNA >200
WHO 2014 http://www.who.int/hiv/pub/guidelines/arv2013/arvs2013upplement_march2014/en/
persistently detectable HIV RNA >1000

Virologic Failure Threshold • 332 randomly selected clinical trials pts + 61
additional pt with VL >50 • VL assayed with: (1) Monitor (Roche); (2) Real
Time (Abbott); (3) Roche TaqMan 2.0 • Results (% VL <50): 19% (Monitor), 25% (Real
Time), 22% (Taqman) • Despite concordance, Real Time was most likely to
detect VL >50 and Taqman was more likely than Monitor; confirmed VF >50 differed
• With threshold VL >200, no differences Lalama J Clin Micro 2015;53:2659

What to change to? US DHHS 2016 www.aidsinfo.nih.gov
2, preferably 3, fully active agents
IAS-USA 2014 JAMA 2014;312:390
PI/r + 1 fully active drug
EACS 2015 www.europeanaidsclinicalsociety.org/
At least 2, and preferably 3, active drugs (including one PI/r and one from a new class)
UK 2015 www.bhiva.org
At least 2, and preferably 3, fully active agents (including one PI/r and one with
novel mechanism – FI, II, CCR5)
WHO 2014 http://www.who.int/hiv/pub/guidelines/arv2013/arvs2013upplement_march2014/en/
(TDF + FTC ↔ AZT + 3TC) + ATV/r or LPV/r

Newer ART Agents (partial list) NRTI NNRTI PI Entry
Inh II MI
Phase 3 doravirine BMS-663068 cabotegravir
Phase 2 apricitabine dexelvucitabinefestinavir
BILR 355 cenicriviroc ibalizumab PF-232798
GS-9883
BMS-955176
Phase 1/2 elvucitabine TMC 310911
HGS004
Phase 1 EFdA (MK-8591) CMX157
RDEA 806 CTP-298 CTP-518 PPL-100 SPI-256
SCH532706VIR-576
BI 224436 INH-1001
GSK-2838232

NRTI
Need: • Less long-term toxicity • Longer acting

Tenofovir alafenamide (TAF) • TAF vs. TDF: Similar virologic efficacy
– 1733 pts on [TAF or TDF]/FTC/EVG/c Sax Lancet 2015;385:2606
• Switch TDFTAF improved renal/bone markers – 1443 pts on TDF with GFR >50 cc/min Mills Lancet ID 2016;16:43 – 663 pts on TDF with GFR >50 cc/min Gallant Lancet HIV 2016;3:e158 – 242 pts on TDF (65%) or not (35%) with eGFR 30-69
Pozniak JAIDS 2016;71:530
• Co-formulations – TAF/FTC/EVG/c (FDA approved 11/5/15) – TAF/FTC/RPV (FDA approved 3/1/16) – TAF/FTC (FDA approved 4/4/16) – TAF/FTC/DRV/c (in clinical trials)

MK-8591 (EFdA)
Grobler CROI 2016 #98 Friedman CROI 2016 #437LB
• 4’-ethynyl-2-fluoro-2’-deoxyadenosine; EFdA
• Non-obligate chain terminator
• Inhibits RT by preventing translocation (NRTTI)
• Potent antiviral activity (PBMC EC50 = 0.2 nM) with broad coverage (HIV-1, HIV-2, MDR strains)

Grobler CROI 2016 #98 Friedman CROI 2016 #437LB
MK-8591 (EFdA)

NNRTI needs: • Less toxic and better tolerated • Fewer drug interactions • Active against resistant viral strains

Doravirine (DOR; MK-1439) • Investigational NNRTI • Pre-clinical
–Potent at low milligram dose –Metabolized by CYP3A4; not a CYP450 inhibitor or inducer –Active in vitro against viral strains with:
• K103N • Y181C • G190A • E101K • E138K • K103N/Y181C
Lai AAC 2014;58:1652-1663

Doravirine (DOR): Phase Ib Double-blind, randomized, placebo-controlled
Study population: HIV+, treatment-naïve (N=18)
Schurmann AIDS 2016;30:57-63

Doravirine – Phase 2
Gatell CROI 2016 #470
Randomized, double-blind, 2-part study Study population: Rx-naïve participants, VL >1000, CD4 >100 (N=216) Study regimen: TDF/FTC + DOR or EFV
TDF/FTC+

• Phase 3 studies in progress
Doravirine – Phase 2
Gatell CROI 2016 #470

Integrase Inhibitors Needs: • long-acting

Cabotegravir (CAB) • Integrase inhibitor similar to DTG; similar resistance • Potent in HIV+ individuals (10, 30, 60 mg oral)
Margolis EACS 2013 • Nanotechology formulation; SC + IM injections • T½ 21-50 days! • Supports monthly
or quarterly dosing • Safety: ISR and
nodules with SC dosing
• Phase 2 study with CAB and RPV IM (LATTE-2)
Spreen JAIDS 2014;67:481

New Mechanisms of Action

HIV Entry Inhibitors
Virus-Cell Fusion
Adapted from Moore JP, PNAS 2003;100:10598-10602.
gp41 gp120
V3 loop
CD4 Binding
CD4
Cell Membrane
Coreceptor Binding
CCR5/CXCR4 (R5/X4)
CCR5 Inhibitors maraviroc
enfuvirtide BMS 663068

BMS-663068: Oral HIV Attachment Inhibitor
• Prodrug of BMS-626529 • Inhibits CD4 binding by
binding to gp120 • PK suggest QD or BID
dosing without boosting • ↓ baseline susceptibility in
12% of pts due to envelope polymorphisms; screened by baseline IC50
Nettles JID 2012;206:1002
Study pop: CD4 >200, VL >5000 off ART X >8 wks or ART-naive (N=50)

BMS-663068: Phase 2b
Lalezari Lancet HIV 2015;2:e427-37 and DeJesus CROI 2016 #472
Phase 2b, randomized, controlled, partially blinded (to ‘068 dose) Study pop: Rx-experienced (>1 wk on >1 ART); IC50 <100 nM for ‘529 (N=254) Study rx: TDF + RAL + [BMS-663068 or ATV/r]
80% 69% 76% 72% 75% VL<50
61% 53% VL<50

BMS-663068: Phase 2b Safety
DeJesus CROI 2016 #472 Given FDA “Breakthrough Status” 7/15; currently in phase 3 in rx-experienced pts.

HIV Maturation Inhibitors (MI)

Lataillade CROI 2015, #114LB
• No serious adverse events, grade 3/4 events, no d/c due to adverse events • Phase 2b studies in progress in treatment-experienced pts.
Study population: HIV+, VL >5K, CD4 >200, PI and MI naive

–2.5
–2
–1.5
–1
–0.5
0
0.5
1
Med
ian
chan
ge in
HIV
-1
RN
A (l
og10
c/m
L)
from
bas
elin
e
TDF/FTC 300 mg/200 mg + ATV 300 mg + RTV 100 mg* BMS-955176 40 mg + ATV 300 mg + RTV 100 mg BMS-955176 40 mg + ATV 400 mg BMS-955176 80 mg + ATV 400 mg
Study day 10 15 20 25 30 35 40 45 50 5 0
Dosing period
BMS-955176 (Maturation Inhibitor)
Median change in HIV-1 RNA at Day 29: •-1.66 to -2.18 log10 c/mL (BMS-955176 arms) •-2.22 log10 c/mL (2 NRTI +ATV/r arm) Hwang IAS 2015 #TUAB0106LB
Study population: Rx-naïve, VL>5000, CD4>200 (N=28)

BMS-955176: PI-resistant viral strains
• 21 clinical isolates from 15 patients – median 6 years on PI therapy – all had major PI resistance-associated mutations in
protease – 17 of 21 had 2o changes in GAG associated with PI
resistance (at positions 128, 431, 436, 437, 449, 452, 453)
• 7 highly PI-resistant virus strains • BMS-955176 retained virologic activity
Ray CROI 2016 #464

ART Controversies: Conclusions • ART improves life expectancy. • When to start? At any CD4 and “when the patient
is ready.” • What to start? Many excellent options and new
comparative data; individualization is key. • When to change? Confirmed VL >200. • What to change to?: Drugs with new mechanisms
of action (CD4 attachment and maturation inhibitors) offer hope.
• Further research is necessary.

Acknowledgments • Cornell HIV Clinical Trials
Unit (CCTU) Division of Infectious Diseases
• Weill Medical College of Cornell University
• AIDS Clinical Trials Group (ACTG)
• Division of AIDS, NIAID, NIH
• The patient volunteers!

Cornell HIV Clinical Trials Unit
Kristie Marshall Trip
Tim
Joanne Valery Marisol
Glenn Luis
Todd
Yismilka
Mufida
Jaylyza Leah
Tiina Ashley
Eileen
Brian
Julia
Christina




![Presentation1 (gulick)[2]](https://static.fdocuments.in/doc/165x107/54ba3b9d4a7959d26f8b45b0/presentation1-gulick2.jpg)