Fabrication of Percutaneous Transvenous Mitral Annuloplasty Testing Device
ARRHYTHMIAS
The challenges of transvenous leadextractionMelanie Maytin, Laurence M Epstein
Transvenous lead extraction (TLE) has undergonean explosive evolution since its inception as a rudi-mentary skill with limited technology and thera-peutic options. Early techniques involved simplemanual traction that frequently proved ineffectivefor chronically implanted leads and carried a signif-icant risk of myocardial avulsion, tamponade, anddeath.1 2 The significant morbidity and mortalityassociated with these early extraction techniqueslimited their application to life threatening situa-tions such as infection and sepsis. The past 30 yearshave witnessed significant advances in lead extrac-tion technology resulting in safer and more effica-cious techniques and tools, providing the skilledextractor with a well equipped armamentarium.With the development of the discipline, we havewitnessed a growth in the community of TLEexperts coincident with a pronounced decline in theincidence of procedure related morbidity andmortality, with more recent registries at highvolume centres reporting high success rates withexceedingly low complication rates (figure 1).3e6
Future developments in lead extraction are likely tofocus on new tools that will allow us to providecomprehensive device management, alternativesystems for extraction training, and the design ofnew leads conceived to facilitate future extraction.
PATHOLOGY OF THE HUMANeLEAD INTERACTIONThe challenges and risks of TLE are principallyrelated to the body ’s foreign body response toa cardiovascular implantable electronic device(CIED). This response begins at implantation withthrombus development along the lead. Fibrosis ofthe thrombus occurs next with near completeencapsulation of the leads with a fibrin sheathwithin 4e5 days of implant.7 8 Robust fibrosisdevelops in areas of direct contact between the leadand the vasculature and endocardium (figure 2).The most common adhesion sites include thevenous entry site, the superior vena cava (SVC),and the electrodeemyocardial interface, andmultiple areas of scar tissue are found in themajority of patients.9 Calcification of the fibroticlesions can occur with time, further cementing theadhesion site and increasing the difficulties andrisks of the extraction. Although predictors ofsevere scar formation have not been clearly identi-fied, it appears that younger patients develop morevigorous fibrotic responses and more frequentlydevelop progressive calcification.10 In addition tohumanelead interaction, leadelead binding can
result in a significant challenge to extraction. Thus,multiple leads and duration of implantation arefactors impacting the safety and efficacy ofextraction. This is one of the arguments againstabandoning superfluous leads.
TLE INDICATIONSTLE indications have expanded to include moreclinical situations as advances in extraction tech-niques have made the procedure safer and moresuccessful.11 The recently published 2009 HeartRhythm Society (HRS) Expert Consensus State-ment on TLE has extended class I indications toinclude patients with CIED pocket infection, occultgram-positive infection, and functional leads that,due to design or failure, may pose an immediatethreat if left in place (table 1). The class II indica-tions for TLE were further divided into IIa(reasonable to perform the procedure) and IIb (mayconsider performing the procedure) indications.CIED patients with occult gram-negative bacter-aemia, severe chronic pain, ipsilateral venousocclusion with contraindication to contralateralimplantation, non-functional leads, and need forMRI with no other imaging alternatives, and inwhom implantation would result in more than fourleads on one side or more than five leads throughthe SVC, represent class IIa indications for TLE.Class IIb indications for TLE include CIED patientswith superfluous functional or non-functional leadsand with functional leads that pose risk of deviceinterference or that, due to design or failure, posepotential future risk.In assessing an individual’s indication for TLE,
a comparison of the risks of extraction with therisks of lead abandonment is mandated (figure 3).The consideration of patient and lead characteris-tics and, importantly, operator experience must befactored into the risk assessment of extraction. Therisk assessment evaluation must include specificattention to the number of leads, implant duration,defibrillator versus pacing electrodes, and patientage.Decisions regarding lead extraction must be
made on an individual case-by-case basis inte-grating various patient and lead characteristics andoperator related variables. Lead extraction with thepotential for significant morbidity and mortalitymay not be warranted in patients with a poorprognosis or where the risks of intervention clearlyoutweigh the risks of lead abandonment. Addi-tionally, those inexperienced in the procedure
Brigham and Women’s Hospital,Boston, Massachusetts, USA
Correspondence toDr Laurence M Epstein, Brighamand Women’s Hospital, 75Francis Street, Boston, MA02215, USA;[email protected]
Heart 2011;97:425e434. doi:10.1136/hrt.2009.189910 425
Education in Heart
group.bmj.com on February 7, 2011 - Published by heart.bmj.comDownloaded from

should not perform lead extractions, and norshould those without the necessary tools availableto attain complete success or in a setting notprepared and committed to the complete and safeperformance of the procedure.11
TLE TECHNIQUES AND TOOLSPre-procedure and patient preparationTLE, like any surgical procedure, requires a teamapproach with anticipation of and planning for allpotential situations. The required personnel of theextraction team include, at a minimum, the physi-cian performing the extraction, a cardiothoracicsurgeon, anaesthesia support, an x ray technician orother person to operate the fluoroscopy, and bothscrubbed and non-scrubbed assistants. Whilecomplications will occur, the single most importantfactor in preventing a major complication fromresulting in a death is the time to intervention.Thus, the procedure locationdthat is, the operatingroom or catheterisation or electrophysiologylaboratorydis less important than the immediateavailability of cardiothoracic surgical intervention.This mandates that a surgeon proficient atmanaging the potential complications be on siteduring the extraction procedure and that theequipment necessary for cardiopulmonary bypass bereadily available. Additional emergency equipmentthat should be present in the room or immediatelyavailable includes transthoracic and/or trans-oesophageal echocardiography, a pericardiocentesis
Figure 1 Success, morbidity and mortality in large series. Graphic representation of complete success as a function of time, represented by blackcolumns. Secondary y axis represents percentage morbidity (orange) and mortality (red). Timeline of extraction techniques and tools commensuratewith reported trials is at the top of the figure. Values below the graph represent the number of leads (N) extracted in each study. Composite majorcomplication (MC) and mortality (M) rate was calculated. Only studies with$50 leads extracted and data regarding mortality and major complicationswere included.
Figure 2 (A, B) Fibrosis in areas of direct contact. Vigorous fibrosis develops in areasof direct contact between the lead and the vasculature and myocardium. (A) Extractedatrial lead with intense fibrosis at its distal portion. (B) Extracted defibrillator lead foundto have a large amount of organised fibrosis at the electrode tipemyocardial interface.
426 Heart 2011;97:425e434. doi:10.1136/hrt.2009.189910
Education in Heart
group.bmj.com on February 7, 2011 - Published by heart.bmj.comDownloaded from
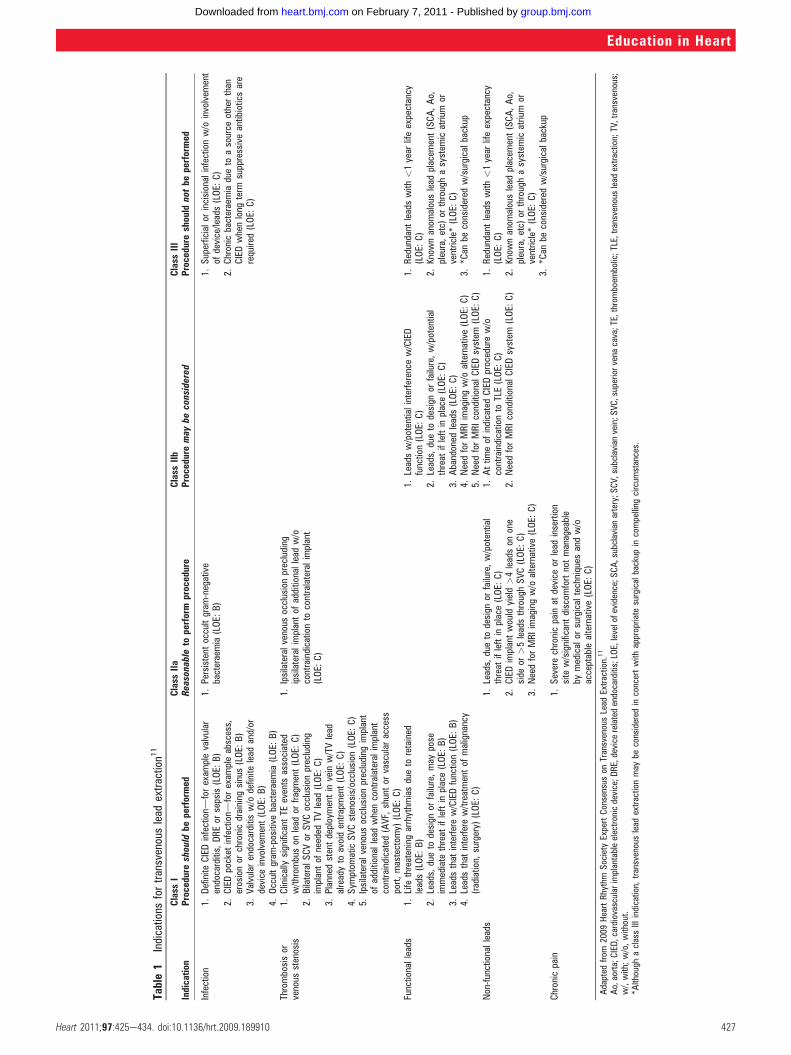
Table1
Indications
fortransvenouslead
extraction1
1
Indication
Class
IClass
IIa
Class
IIb
Class
III
Procedure
should
beperformed
Reasonableto
perform
procedure
Procedure
may
beconsidered
Procedure
should
notbe
performed
Infection
1.Definite
CIEDinfectiond
forexam
plevalvular
endocarditis,
DREor
sepsis(LOE:
B)
2.CIEDpocket
infectiond
forexam
pleabscess,
erosionor
chronicdraining
sinus(LOE:
B)
3.Valvularendocarditisw/o
definite
lead
and/or
device
involvem
ent(LOE:
B)
4.Occultgram
-positive
bacteraemia(LOE:
B)
1.Persistent
occultgram
-negative
bacteraemia(LOE:
B)
1.Superficialor
incisionalinfectionw/o
involvem
ent
ofdevice/leads(LOE:
C)
2.Chronicbacteraemiadueto
asource
otherthan
CIEDwhenlong
term
suppressiveantibioticsare
required(LOE:
C)
Thrombosisor
venous
stenosis
1.Clinicallysignificant
TEevents
associated
w/throm
buson
lead
orfragment(LOE:
C)
2.BilateralSCVor
SVCocclusionprecluding
implantof
needed
TVlead
(LOE:
C)
3.Plannedstentdeploymentin
vein
w/TVlead
alreadyto
avoidentrapment(LOE:
C)
4.Sym
ptom
aticSVCstenosis/occlusion
(LOE:
C)
5.Ipsilateralvenous
occlusionprecluding
implant
ofadditionallead
whencontralateralimplant
contraindicated(AVF,
shuntor
vascular
access
port,mastectom
y)(LOE:
C)
1.Ipsilateralvenous
occlusionprecluding
ipsilateralimplantof
additionallead
w/o
contraindicationto
contralateralimplant
(LOE:
C)
Functionalleads
1.Life
threateningarrhythm
iasdueto
retained
leads(LOE:
B)
2.Leads,
dueto
design
orfailure,may
pose
immediate
threat
ifleftin
place(LOE:
B)
3.Leadsthat
interferew/CIEDfunction(LOE:
B)
4.Leadsthat
interferew/treatmentof
malignancy
(radiation,
surgery)
(LOE:
C)
1.Leadsw/potentialinterference
w/CIED
function(LOE:
C)
2.Leads,
dueto
design
orfailure,w/potential
threat
ifleftin
place(LOE:
C)
3.Abandoned
leads(LOE:
C)
4.NeedforMRIimagingw/o
alternative(LOE:
C)
5.NeedforMRIconditionalCIEDsystem
(LOE:
C)
1.Redundant
leadswith
<1year
lifeexpectancy
(LOE:
C)
2.Know
nanom
alouslead
placem
ent(SCA,Ao,
pleura,etc)
orthroughasystem
icatrium
orventricle*(LOE:
C)
3.*C
anbe
considered
w/surgicalbackup
Non-functionalleads
1.Leads,
dueto
design
orfailure,w/potential
threat
ifleftin
place(LOE:
C)
2.CIEDimplantwould
yield>4leadson
one
side
or>5leadsthroughSVC(LOE:
C)
3.NeedforMRIimagingw/o
alternative(LOE:
C)
1.Attim
eof
indicatedCIEDprocedurew/o
contraindicationto
TLE(LOE:
C)
2.NeedforMRIconditionalCIEDsystem
(LOE:
C)
1.Redundant
leadswith
<1year
lifeexpectancy
(LOE:
C)
2.Know
nanom
alouslead
placem
ent(SCA,Ao,
pleura,etc)
orthroughasystem
icatrium
orventricle*(LOE:
C)
3.*C
anbe
considered
w/surgicalbackup
Chronicpain
1.Severechronicpain
atdevice
orlead
insertion
site
w/significantdiscom
fortnotmanageable
bymedicalor
surgicaltechniques
andw/o
acceptablealternative(LOE:
C)
Adapted
from
2009
HeartRhythm
Society
ExpertConsensus
onTransvenousLead
Extraction.11
Ao,aorta;CIED,cardiovascularimplantableelectronicdevice;D
RE,device
relatedendocarditis;LOE,levelofevidence;SCA,subclavianartery;S
CV,subclavianvein;S
VC,superiorvena
cava;TE,thromboem
bolic;TLE,transvenous
lead
extraction;TV,transvenous;
w/,with;w/o,without.
*Although
aclassIII
indication,
transvenouslead
extractionmay
beconsidered
inconcertwith
appropriate
surgicalbackup
incompelling
circum
stances.
Heart 2011;97:425e434. doi:10.1136/hrt.2009.189910 427
Education in Heart
group.bmj.com on February 7, 2011 - Published by heart.bmj.comDownloaded from

tray, vacuum containers for chest tube drainage,temporary pacing equipment, an anaesthesia cartfor general anaesthesia, and vasopressors and otheremergencymedications. We have fashioned amobile‘extraction cart’ that contains all the aforemen-tioned emergency equipment in addition to extrac-tion tools (locking stylets, non-powered andpowered sheaths, femoral workstations, extractionsnares, etc) and CIED implant tools (stylets,wrenches, fixation tools, introducer sheaths, intra-venous contrast, repair kits, etc).Recognising the potential need for emergent
surgical intervention (table 2), our patients areprepared for the procedure in such a way so as toeliminate any delays. We prep our patients witha chlorhexadine solution and drape so as to allowaccess for contralateral implant or emergent peri-cardiocentesis, thoracentesis, thoracotomy, ster-notomy or cardiopulmonary bypass. It is ourpractice that all patients have bilateral peripheralvenous access with large bore catheters, femoralvenous access, invasive haemodynamic monitoringwith a radial arterial line, general endotrachealanaesthesia, and four units of packed red blood cellsimmediately available.
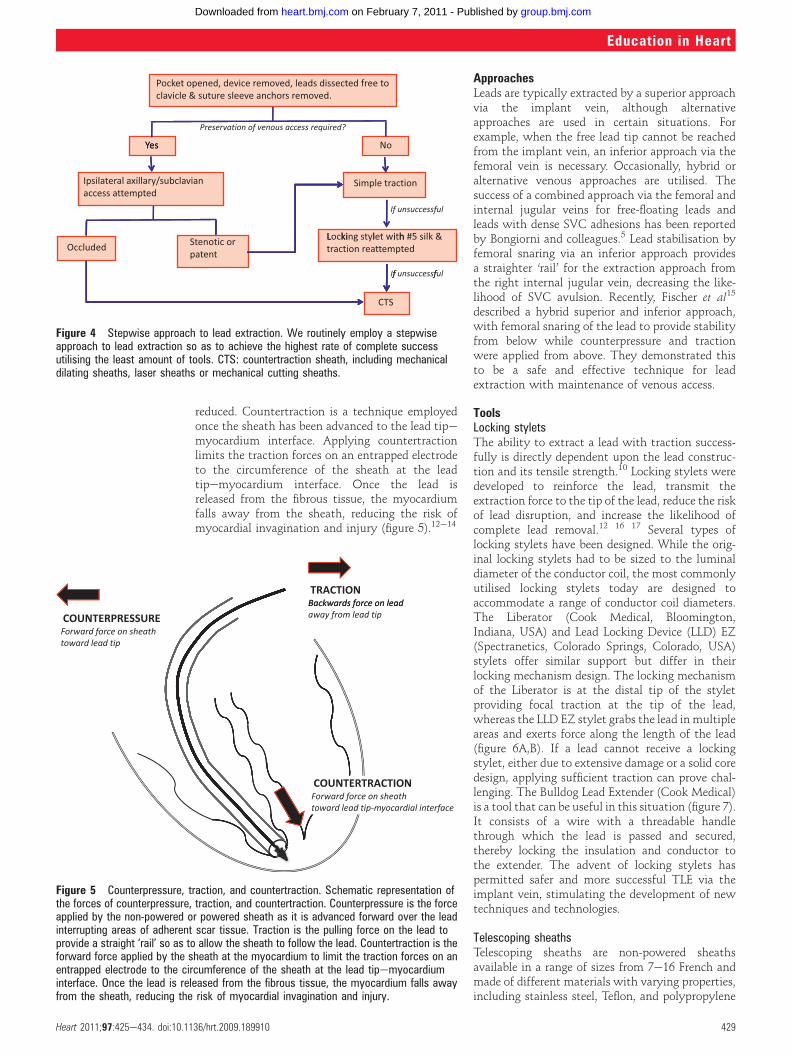
TechniquesWe employ a stepwise approach to lead extractionin every case with the goal of complete successutilising the least amount of tools (figure 4). As weroutinely perform TLE by the superior approach viathe implant vein, the initial step in the extractionprocedure is an appropriately positioned incisionthat permits easy access to the venous entry site ina plane parallel to the leads. It is our practice toattempt to use the existing incision wheneverpossible and perform an elliptical incision excisingthe existing incisional scar. Occasionally, two inci-sions are necessarydone over the venous entry siteof the leads and a second over the pocket or area ofskin erosion or adherence. Once the pocket isentered, microbial cultures of pocket tissue areobtained in all cases of CIED infection. Then, thedevice is removed and the leads are dissected freeback to their venous entry site. Dissection aroundthe venous entry site is important to allow easypassage of any devices that may be necessary forlead extraction, but aggressive dissection can resultin transient issues with haemostasis secondary toback bleeding. The anchor sleeves are then removedand all extraneous material, including suturematerial, is eliminated from the pocket. Completeremoval of infected tissue and foreign material ismandatory in cases of CIED infection. Additionally,it is our routine practice to perform a capsulectomywhenever ipsilateral reimplantation is planned.If ipsilateral reimplantation is planned, ipsilateral
venous access is attempted under fluoroscopicguidance with or without the aid of intravenouscontrast. In our experience, stenotic lesions canoften be crossed with use of a 5 French dilator andglidewire. If the vein is successfully cannulated anda wire could be passed into the inferior vena cava,or if ipsilateral reimplantation is not planned, leadremoval with simple traction is attempted. If thisproves unsuccessful, the lead is cut and a lockingstylet is introduced, a number 5 silk is tied aroundthe lead body, and traction reattempted. Thenumber 5 silk is used to reinforce the lead and toprevent the insulation from bunching up or ‘snowplowing’ under the force of counterpressure. If leadremoval still proves unsuccessful, a non-powered orpowered sheath is employed. Sheath selection isdetermined by the clinical situation and the oper-ator ’s preference and experience. If the lead is notretrievable from the implant vein or lead disruptionoccurs, transfemoral retrieval is performed.
Counterpressure, traction, and countertractionCounterpressure is the force applied by the non-powered or powered sheath as it is advanced overthe lead interrupting areas of adherent scar tissue.Sufficient traction must be applied to the lead andlocking stylet so the lead acts as a ‘rail’. This allowsthe sheath to follow the lead body and not damagethe vasculature as the lead curves within the vein.This is especially true when passing the sheathfrom the brachiocephalic vein through the SVC tothe right atrium. By exerting significantly more‘pull’ than ‘push’, lateral force on the SVC can be
Figure 3 Risk versus risk. The decision regarding leadextraction or abandonment requires comparison of thecurrent risks of lead extraction with the future risks ofboth lead abandonment and potential lead extraction. TLE,transvenous lead extraction.
Table 2 Potential complications of transvenous lead extraction
Major complications Minor complications
Death Pericardial effusion not requiring intervention
Cardiac avulsion requiring intervention(percutaneous or surgical)
Haemothorax not requiring intervention
Vascular injury requiring intervention(percutaneous or surgical)
Pocket haematoma requiring reoperation
Pulmonary embolism requiring surgicalintervention
Upper extremity thrombosis resulting inmedical treatment
Respiratory arrest/anaesthesia relatedcomplication prolonging hospitalisation
Vascular repair near implant site or venous entry site
Stroke Haemodynamically significant air embolism
CIED infection at previouslynon-infected site
Migrated lead fragment without sequelae
Blood transfusion as a result of intraoperative blood loss
Pneumothorax requiring a chest tube
Pulmonary embolism not requiring surgical intervention
CIED, cardiovascular implantable electronic device.
428 Heart 2011;97:425e434. doi:10.1136/hrt.2009.189910
Education in Heart
group.bmj.com on February 7, 2011 - Published by heart.bmj.comDownloaded from
reduced. Countertraction is a technique employedonce the sheath has been advanced to the lead tipemyocardium interface. Applying countertractionlimits the traction forces on an entrapped electrodeto the circumference of the sheath at the leadtipemyocardium interface. Once the lead isreleased from the fibrous tissue, the myocardiumfalls away from the sheath, reducing the risk ofmyocardial invagination and injury (figure 5).12e14
ApproachesLeads are typically extracted by a superior approachvia the implant vein, although alternativeapproaches are used in certain situations. Forexample, when the free lead tip cannot be reachedfrom the implant vein, an inferior approach via thefemoral vein is necessary. Occasionally, hybrid oralternative venous approaches are utilised. Thesuccess of a combined approach via the femoral andinternal jugular veins for free-floating leads andleads with dense SVC adhesions has been reportedby Bongiorni and colleagues.5 Lead stabilisation byfemoral snaring via an inferior approach providesa straighter ‘rail’ for the extraction approach fromthe right internal jugular vein, decreasing the like-lihood of SVC avulsion. Recently, Fischer et al15
described a hybrid superior and inferior approach,with femoral snaring of the lead to provide stabilityfrom below while counterpressure and tractionwere applied from above. They demonstrated thisto be a safe and effective technique for leadextraction with maintenance of venous access.
ToolsLocking styletsThe ability to extract a lead with traction success-fully is directly dependent upon the lead construc-tion and its tensile strength.10 Locking stylets weredeveloped to reinforce the lead, transmit theextraction force to the tip of the lead, reduce the riskof lead disruption, and increase the likelihood ofcomplete lead removal.12 16 17 Several types oflocking stylets have been designed. While the orig-inal locking stylets had to be sized to the luminaldiameter of the conductor coil, the most commonlyutilised locking stylets today are designed toaccommodate a range of conductor coil diameters.The Liberator (Cook Medical, Bloomington,Indiana, USA) and Lead Locking Device (LLD) EZ(Spectranetics, Colorado Springs, Colorado, USA)stylets offer similar support but differ in theirlocking mechanism design. The locking mechanismof the Liberator is at the distal tip of the styletproviding focal traction at the tip of the lead,whereas the LLD EZ stylet grabs the lead inmultipleareas and exerts force along the length of the lead(figure 6A,B). If a lead cannot receive a lockingstylet, either due to extensive damage or a solid coredesign, applying sufficient traction can prove chal-lenging. The Bulldog Lead Extender (Cook Medical)is a tool that can be useful in this situation (figure 7).It consists of a wire with a threadable handlethrough which the lead is passed and secured,thereby locking the insulation and conductor tothe extender. The advent of locking stylets haspermitted safer and more successful TLE via theimplant vein, stimulating the development of newtechniques and technologies.
Telescoping sheathsTelescoping sheaths are non-powered sheathsavailable in a range of sizes from 7e16 French andmade of different materials with varying properties,including stainless steel, Teflon, and polypropylene
Figure 4 Stepwise approach to lead extraction. We routinely employ a stepwiseapproach to lead extraction so as to achieve the highest rate of complete successutilising the least amount of tools. CTS: countertraction sheath, including mechanicaldilating sheaths, laser sheaths or mechanical cutting sheaths.
TRACTIONdaelnoecrofsdrawkcaB sdrawkcaB ecrof no dael
pit dael morf yawaCOUNTERPRESSUREhtaehs no ecrof drawroF
pit dael drawot
COUNTERTRACTIONhtaehs no ecrof drawroF
ecafretni laidracoym-pit dael drawot
Figure 5 Counterpressure, traction, and countertraction. Schematic representation ofthe forces of counterpressure, traction, and countertraction. Counterpressure is the forceapplied by the non-powered or powered sheath as it is advanced forward over the leadinterrupting areas of adherent scar tissue. Traction is the pulling force on the lead toprovide a straight ‘rail’ so as to allow the sheath to follow the lead. Countertraction is theforward force applied by the sheath at the myocardium to limit the traction forces on anentrapped electrode to the circumference of the sheath at the lead tipemyocardiuminterface. Once the lead is released from the fibrous tissue, the myocardium falls awayfrom the sheath, reducing the risk of myocardial invagination and injury.
Heart 2011;97:425e434. doi:10.1136/hrt.2009.189910 429
Education in Heart
group.bmj.com on February 7, 2011 - Published by heart.bmj.comDownloaded from

(figure 8). Teflon is soft and flexible but is unable tocut through dense scar tissue, while polypropyleneis stiffer and better at disrupting encapsulating scarbut must be used with caution so as to avoidvascular injury. Stainless steel sheaths are employedonly for disrupting dense and calcified fibrosis asthe central venous circulation is entered. The innerand outer sheath pair is advanced along the leadwith alternating counterclockwise and clockwisemotions with moderate pressure. The soft innersheath is used as a guide while the more rigid outersheath serves to disrupt and dilate the encapsu-lating fibrous tissue. Sufficient traction is essentialto ensure that the sheaths track the path of the leadand remain within the confines of the vasculatureunder fluoroscopic guidance. Utilising telescopingsheaths, TLE success rates via a superior (ie, implantvein) approach range from 71e97%.12 14 16 18
Powered sheathsPowered sheaths employ a source of energy to makethe dissection of encapsulating fibrous tissue easierand more efficient, thus enabling the advancement
of the sheath along the lead with reduced counter-traction and counterpressure forces.10 19 One suchpowered sheath is the Excimer Laser System (Spec-tranetics), a ‘cool’ pulsed ultraviolet laser at a wave-length of 308 nm available in 12, 14 and 16 Frenchsizes. The laser sheath applies circumferential pulsesof energy at its distal end, dissolving tissue incontact with the tip of the sheath by photochemicaldestruction of molecular bonds and photothermalablation that vaporises water and ruptures cells,with resultant photomechanical creation of kineticenergy (figure 9A,B).20 The sheath is advanced overthe lead body utilising the standard techniques ofcounterpressure and countertraction, and laserenergy is delivered when encapsulating fibrous tissuehalts sheath advancement. Tissue in direct contactwith the sheath tip is ablated to a depth of 50 mmuntil the distal electrode is reached; countertraction isstill necessary to dislocate the lead tip. Comparedwith mechanical telescoping sheaths, laser assistedextraction resulted in more frequent complete leadremoval and shortened extraction times without anincrease in procedural risk.21e23 The introduction oflaser extraction changed the landscape of transvenousextraction, providing a highly effective and lowmorbidity technique with broad applications.6 21 23
The Perfecta Electrosurgical Dissection Sheath(Cook Medical) represents another type of poweredsheath. The electrosurgical dissection sheathconsists of an inner polytetrafluoroethylene (PTFE)sheath with bipolar tungsten electrodes exposed atthe distal tip and an outer sheath for counterpres-sure and countertraction. Radiofrequency energy isdelivered between the bipoles to dissect throughfibrous binding sites, much like a surgical cauterytool, although the lead tip must be liberated withcountertraction. In contrast to the Excimer LaserSheath, the Electrosurgical Dissection Sheathpermits a localised application of radiofrequencyenergy with linear rather than circumferentialdissection of the encapsulating fibrous tissue. Thefocused and steerable dissection plane offers thepotential advantages of improved precision;however, the sheath may have to be repositionedrepeatedly as a result. The Electrosurgical Dissec-tion Sheath offers a cost effective alternative to theExcimer Laser System without compromisingsafety or efficacy.24
Despite the improved success rates of leadextraction with powered sheath technologies,disruption of calcified binding sites remains difficultwith either system. The most recent addition tothe armamentarium of lead extraction toolsprovides a solution. The Evolution and EvolutionShortie Mechanical Dilator Sheaths (Cook Medical)are ‘hand powered’ mechanical sheaths that consistof a flexible, braided stainless steel sheath witha stainless steel spiral cut dissection tip. The sheathis attached to a trigger activation handle thatrotates the sheath and allows the threaded metalend to bore through calcified and dense adhesions(figure 10).25 In our experience, we have found theEvolution sheath quite useful for disrupting sites ofcalcified fibrosis, but often at the expense of
Figure 6 (A, B) Locking stylets. (A) The Liberator Locking Stylet (Cook Medical,Bloomington, Indiana, USA) fits leads with lumen diameters of 0.016e0.032 inches. Anundeployed Liberator locking stylet is shown above a deployed Liberator locking stylet.When deployed, the wound spring at the end of the stylet opens up, locking into place.(B) The Lead Locking Device (LLD) EZ (Spectranetics, Colorado Springs, Colorado, USA)has a radiopaque tip and accommodates inner coil diameters of 0.015e0.026 inches(undeployed stylet, top image). In contrast to the Liberator locking stylet, the LLD lockingstylet has a braided mesh over the entire length of a solid lead that expands whendeployed (bottom image).
430 Heart 2011;97:425e434. doi:10.1136/hrt.2009.189910
Education in Heart
group.bmj.com on February 7, 2011 - Published by heart.bmj.comDownloaded from

functional leads that we were attempting topreserve. Regardless, this technology has providedan effective alternative for dealing with the chal-lenges posed by densely scarred venous entry sitesand heavily calcified adhesions.26
Femoral toolsTransfemoral lead retrieval with the Byrd Work-station (Cook Medical) is a necessary skill forsuccessful lead extraction, particularly in caseswhen the lead is not accessible from the implantvein as in a cut or fractured lead (figure 11). TheByrd Workstation consists of a 16 French outersheath with a one-way valve that is advanced overa wire into the femoral vein, and a 12 French innersheath through which a number of retrieval snarescan be advanced. The Workstation packagecontains a Needle’s Eye snare, but a number ofother snares can be utilised including Tulip andAmplatz gooseneck snares. If lead retrieval witha Needle’s Eye snare proves unsuccessful, we havefound the combination of a gooseneck snare and
bioptome forceps to be quite successful. We preloadthe gooseneck snare on the bioptome, advance thetwo together to the lead fragment, grasp the freelead tail with the bioptome, and then advance thegooseneck snare over the bioptome to ensnare thelead. The challenge of femoral retrieval remainsmanipulating the tools and snaring the lead in threedimensions using two dimensional fluoroscopicimaging. The recent description of a novel tech-nology to facilitate extraction and the maintenanceof vascular access proposed a hybrid superior andinferior approach, with femoral snaring of the leadto stabilise the lead while countertraction andcounterpressure are used to free the lead, reiteratingthe clinical importance of femoral retrieval.15
OutcomesEarly studies of TLE with a laser sheath such as thePLEXES trial demonstrated a pronouncedimprovement in extraction efficacy from 64% withtraditional extraction techniques to 94% with laserassisted extraction without a significant differencein complications, although significant crossoverbetween groups occurred.21 Coincident with thegrowth of the discipline of TLE, we have witnesseda notable decline in the incidence of procedurerelated morbidity and mortality, with a number ofhigh volume single centres reporting morbidity andmortality rates less than 1.0% and 0.3%, respec-tively (figure 1).3e5 A recent multicentre study oftransvenous laser lead extraction in 1449 patientsdemonstrated similarly low morbidity andmortality complication rates of 1.1% and 0.28%,respectively, with a higher clinical success rate of98.8%. The operators in this study were from 13centres and represented small (#60 cases), medium(61e130 cases), and large volume (>130 cases)extraction centres, although the majority of sitesconsisted of medium and high volume extrac-tionists with all extractors having significantexperience.Recently, Cook Medical initiated the LEADER
database to gather ‘real world’ result data. Thepreliminary data demonstrate low major compli-cation (1.2%) and mortality rates (0%) amongpredominantly low (#2 extractions/month) andmoderate (3e5 extractions/month) volume opera-tors. These risks, in fact, are significantly less than
Figure 7 Bulldog Lead Extender (Cook Medical, Bloomington, Indiana, USA). TheBulldog Lead Extender is a useful tool for leads that cannot receive a locking stylet, eitherdue to extensive damage or a solid core design. The exposed end of the lead is passedthrough the loop of the Bulldog (arrow) and the metal sleeve (asterisk) is advanced overthe loop grasping the lead.
Figure 8 Telescoping non-powered countertraction sheaths. Telescoping sheaths are available in a range of sizes from 7e16 French and made ofdifferent materials with varying properties, including stainless steel, Teflon, and polypropylene (from left to right).
Heart 2011;97:425e434. doi:10.1136/hrt.2009.189910 431
Education in Heart
group.bmj.com on February 7, 2011 - Published by heart.bmj.comDownloaded from

other routinely performed cardiovascular proce-dures. For example, published major adverse eventsfor atrial fibrillation ablation and percutaneouscoronary intervention (PCI) procedures are severalfold higher, with a reported 1e2% mortality ratewith PCI.Complication rates with TLE directly parallel
operator experience. Major and minor complica-tions are reduced by approximately 50% withincreased operator experience from 20e120 cases to>300 cases performed.27 Large scale multicentrerandomised trials have confirmed the effect ofexperience on outcomes.6 9 21 23 27 Likewise,observational registries of experienced, high volumeextractionists have consistently demonstratedeven higher success rates (>99%) with exceedinglylow major complication (<1.0%) and mortalityrates (<0.3%).3e5 Consequently, the 2009 HRSExpert Consensus Statement on Lead Extractionrecommends that physicians being trained in TLE
extract a minimum of 40 leads as the primaryoperator under the direct supervision of a qualifiedphysician and extract a minimum of 20 leadsannually to maintain their skills.11 This isa minimum recommendation; there are many whofeel that the best outcomes come with additionalexperience. The ability for trainees and those post-training to gain this experience is limited. Recently,Spectranetics and others have begun the develop-ment of a realistic simulator to allow for thoseinterested in performing extractions to practise,gain experience, and confront emergencies in a safeand controlled environment.
FUTURE DIRECTIONSTLE has evolved dramatically over the past 30 yearsand exponentially throughout the past decade.
Figure 9 (A, B) Excimer laser sheaths (Spectranetics, Colorado Springs, Colorado, USA). (A) The Excimer laser sheathutilises ultraviolet laser energy to vaporise tissue in contact with the tip of the sheath where the optical fibres terminate.The sheath is available in a range of sizes (12 French, 14 French, and 16 French) displayed from top to bottom. (B) End-on view of the laser sheath demonstrating the distal end where the optical fibres terminate.
Figure 10 The Evolution device. The Evolution and Evolution Shortie Mechanical DilatorSheath (Cook Medical, Bloomington, Indiana, USA) are ‘hand powered’ mechanicalsheaths that consist of a flexible, braided stainless steel sheath with a stainless steelspiral cut dissection tip (inset). The sheath is attached to a trigger handle that rotates thesheath and allows the threaded metal end to agar out the scar tissue.
Figure 11 Transfemoral snaring of lead. Transfemorallead retrieval with the Byrd Workstation (Cook Medical,Bloomington, Indiana, USA) is a necessary skill forsuccessful lead extraction, particularly in cases when thelead is not accessible from the implant vein as in a cut orfractured lead. The lead has been snared and wound up bythe Needle’s Eye snare (arrow) allowing successfulremoval of the lead.
432 Heart 2011;97:425e434. doi:10.1136/hrt.2009.189910
Education in Heart
group.bmj.com on February 7, 2011 - Published by heart.bmj.comDownloaded from

Despite these advances, the basic tenants of coun-terpressure, traction, and countertraction remaincritical to ensuring successful and safe outcomes.As indications for device therapy expand andyounger patients receive devices, it is likely that the
number of lead extractions performed will increase,as will the pressure on the field to continue toevolve not simply as a technique but as a disciplineand a science.The 2009 HRS Expert Consensus on TLE
provides several recommendations to help thespecialty of lead extraction evolve. The documentcreates standard definitions, recommends guidelinesfor safe lead extraction, identifies indications forextraction, and emphasises the importance ofreporting outcomes. As new extraction tools andnovel leads designed to facilitate future extractionare introduced, standardised reporting of outcomeswill become essential. Data collection will serve toadvance our collective knowledge and allow us todraw conclusions regarding the safety and compli-cations of these techniques. To date, questionsregarding the benefits of lead extraction in specificsituations remain and a nationwide database ofextraction outcomes and complications will allowus to critically evaluate and rigorously answer thesequestions. Moreover, collaboration among thoseperforming lead extraction will be critical tobuilding a community of lead extractors andcreating a field committed to quality. The future oflead extraction lies in the development of newtechniques, tools and training methods, the crea-tion of a collaborative community, and the growthof the science.
Competing interests In compliance with EBAC/EACCME guidelines,all authors participating in Education in Heart have disclosed potentialconflicts of interest that might cause a bias in the article.Honorarium/Consultant for Spectranetics Inc.
Provenance and peer review Commissioned; internally peerreviewed.
REFERENCES1. Madigan NP, Curtis JJ, Sanfelippo JF, et al. Difficulty of
extraction of chronically implanted tined ventricular endocardialleads. J Am Coll Cardiol 1984;3:724e31.
2. Rettig G, Doenecke P, Sen S, et al. Complications with retainedtransvenous pacemaker electrodes. Am Heart J 1979;98:587e94.
3. Kennergren C, Bjurman C, Wiklund R, et al. A single-centreexperience of over one thousand lead extractions. Europace2009;11:612e17.
4. Jones SO, Eckart RE, Albert CM, et al. Large, single-center,single-operator experience with transvenous lead extraction:outcomes and changing indications. Heart Rhythm 2008;5:520e5.
5. Bongiorni MG, Soldati E, Zucchelli G, et al. Transvenous removalof pacing and implantable cardiac defibrillating leads using singlesheath mechanical dilatation and multiple venous approaches: highsuccess rate and safety in more than 2000 leads. Eur Heart J2008;29:2886e93.
6. Wazni O, Epstein LM, Carrillo RG, et al. Lead extraction in thecontemporary setting: the LExICon Study an observationalretrospective study of consecutive laser lead extractions. J AmColl Cardiol 2010;55:579e86.
< Recent, large prospective observational study of laser leadextraction including 1449 patients.
7. Robboy SJ, Harthorne JW, Leinbach RC, et al. Autopsy findingswith permanent pervenous pacemakers. Circulation1969;39:495e501.
8. Huang TY, Baba N. Cardiac pathology of transvenouspacemakers. Am Heart J 1972;83:469e74.
9. Smith HJ, Fearnot NE, Byrd CL, et al. Five-years experience withintravascular lead extraction. U.S. Lead Extraction Database.Pacing Clin Electrophysiol 1994;17:2016e20.
10. Smith MC, Love CJ. Extraction of transvenous pacing and ICDleads. Pacing Clin Electrophysiol 2008;31:736e52.
11. Wilkoff BL, Love CJ, Byrd CL, et al. Transvenous lead extraction:Heart Rhythm Society expert consensus on facilities, training,
Challenges of transvenous lead extraction (TLE): key points
< TLE has evolved dramatically since its beginnings in the 1980s.< The challenge and risk of TLE are directly related to the humanelead
interaction.< Most common sites of scar formation include the venous entry site, superior
vena cava, and electrode tipemyocardial interface.< Younger patients develop more robust scar formation.< TLE indications are outlined in the 2009 HRS Expert Consensus Statement on
TLE.< Class I TLE indications have expanded to include pocket infections, occult
gram-positive infection, and functional leads that may pose an immediatethreat if left in place.
< In assessing an individual’s indication for TLE, the risks of extraction must becompared with the risks of lead abandonment.
< TLE requires a team approach with anticipation of and planning for allpotential situations.
< Principles of counterpressure, traction, and countertraction should be appliedto all TLE tools.
< Several extraction tools are available and the extractionist should be wellversed in all techniques as several different approaches can be necessary.
< Several groups have reported major complication and mortality rates of lessthan 1% and 0.3%, respectively.
< LExICon, a recent multicentre prospective observational study of laser leadextraction in 1449 patients, demonstrated a major complication and mortalityrate of 1.1% and 0.28%, respectively.
< Complication rates parallel operator experience.< Suggested minimum standards for training and maintenance of competency
are 40 and 20 leads, respectively.< Standardised outcomes reporting is essential.
You can get CPD/CME credits for Education in Heart
Education in Heart articles are accredited by both the UK Royal College ofPhysicians (London) and the European Board for Accreditation in Cardiologydyou need to answer the accompanying multiple choice questions (MCQs). Toaccess the questions, click on BMJ Learning: Take this module on BMJLearning from the content box at the top right and bottom left of the onlinearticle. For more information please go to: http://heart.bmj.com/misc/education.dtl< RCP credits: Log your activity in your CPD diary online (http://www.
rcplondon.ac.uk/members/CPDdiary/index.asp)dpass mark is 80%.< EBAC credits: Print out and retain the BMJ Learning certificate once you
have completed the MCQsdpass mark is 60%. EBAC/ EACCME Credits cannow be converted to AMA PRA Category 1 CME Credits and are recognisedby all National Accreditation Authorities in Europe (http://www.ebac-cme.org/newsite/?hit¼men02).
Please note: The MCQs are hosted on BMJ Learningdthe best availablelearning website for medical professionals from the BMJ Group. If prompted,subscribers must sign into Heart with their journal’s username and password. Allusers must also complete a one-time registration on BMJ Learning and subse-quently log in (with a BMJ Learning username and password) on every visit.
Heart 2011;97:425e434. doi:10.1136/hrt.2009.189910 433
Education in Heart
group.bmj.com on February 7, 2011 - Published by heart.bmj.comDownloaded from

indications, and patient management: this document wasendorsed by the American Heart Association (AHA). Heart Rhythm2009;6:1085e104.
< Transvenous lead extraction consensus statement creatingminimum educational standards, providing guidelines forthe practice of transvenous lead extraction, and definingstandardised outcome definitions.
12. Byrd CL, Schwartz SJ. Transatrial implantation of transvenouspacing leads as an alternative to implantation of epicardial leads.Pacing Clin Electrophysiol 1990;13:1856e9.
13. Byrd CL, Schwartz SJ, Hedin N. Lead extraction. Indications andtechniques. Cardiol Clin 1992;10:735e48.
14. Byrd CL, Schwartz SJ, Hedin N. Intravascular techniques forextraction of permanent pacemaker leads. J Thorac CardiovascSurg 1991;101:989e97.
15. Fischer A, Love B, Hansalia R, et al. Transfemoral snaring andstabilization of pacemaker and defibrillator leads to maintainvascular access during lead extraction. Pacing Clin Electrophysiol2009;32:336e9.
16. Fearnot NE, Smith HJ, Goode LB, et al. Intravascular leadextraction using locking stylets, sheaths, and other techniques.Pacing Clin Electrophysiol 1990;13:1864e70.
17. Goode LB, Byrd CL, Wilkoff BL, et al. Development of a newtechnique for explantation of chronic transvenous pacemakerleads: five initial case studies. Biomed Instrum Technol1991;25:50e3.
18. Brodell GK, Castle LW, Maloney JD, et al. Chronic transvenouspacemaker lead removal using a unique, sequential transvenoussystem. Am J Cardiol 1990;66:964e6.
19. Bongiorni MG, Giannola G, Arena G, et al. Pacing and implantablecardioverter-defibrillator transvenous lead extraction. Ital Heart J2005;6:261e6.
20. Gijsbers GH, van den Broecke DG, Sprangers RL, et al. Effect offorce on ablation depth for a XeCl excimer laser beam delivered by
an optical fiber in contact with arterial tissue under saline. LasersSurg Med 1992;12:576e84.
21. Wilkoff BL, Byrd CL, Love CJ, et al. Pacemaker lead extractionwith the laser sheath: results of the pacing lead extraction withthe excimer sheath (PLEXES) trial. J Am Coll Cardiol1999;33:1671e6.
< First randomised controlled trial of laser lead extractioncompared with mechanical dilating sheaths.
22. Byrd CL, Wilkoff BL, Love CJ, et al. Clinical study of the lasersheath for lead extraction: the total experience in the UnitedStates. Pacing Clin Electrophysiol 2002;25:804e8.
< Report of the US Lead Extraction Database, a largeprospective observational registry.
23. Epstein LM, Byrd CL, Wilkoff BL, et al. Initial experiencewith larger laser sheaths for the removal of transvenouspacemaker and implantable defibrillator leads. Circulation1999;100:516e25.
< First prospective registry of large laser sheath (14 French,16 French) experience.
24. Neuzil P, Taborsky M, Rezek Z, et al. Pacemaker and ICD leadextraction with electrosurgical dissection sheaths and standardtransvenous extraction systems: results of a randomized trial.Europace 2007;9:98e104.
25. Dello Russo A, Biddau R, Pelargonio G, et al. Lead extraction:a new effective tool to overcome fibrous binding sites. J IntervCard Electrophysiol 2009;24:147e50.
26. Hussein AA, Wilkoff BL, Martin DO, et al. Initial experience withthe Evolution mechanical dilator sheath for lead extraction: safetyand efficacy. Heart Rhythm 2010;7:870e3.
27. Byrd CL, Wilkoff BL, Love CJ, et al. Intravascular extraction ofproblematic or infected permanent pacemaker leads: 1994e1996.U.S. Extraction Database, MED Institute. Pacing Clin Electrophysiol1999;22:1348e57.
< A further report of the US Lead Extraction Database.
434 Heart 2011;97:425e434. doi:10.1136/hrt.2009.189910
Education in Heart
group.bmj.com on February 7, 2011 - Published by heart.bmj.comDownloaded from

doi: 10.1136/hrt.2009.189910 2011 97: 425-434Heart
Melanie Maytin and Laurence M Epstein extractionThe challenges of transvenous lead
http://heart.bmj.com/content/97/5/425.full.htmlUpdated information and services can be found at:
These include:
References http://heart.bmj.com/content/97/5/425.full.html#ref-list-1
This article cites 27 articles, 9 of which can be accessed free at:
serviceEmail alerting
the box at the top right corner of the online article.Receive free email alerts when new articles cite this article. Sign up in
CollectionsTopic
(377 articles)Education in Heart � (3 articles)Arrhythmias �
Articles on similar topics can be found in the following collections
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on February 7, 2011 - Published by heart.bmj.comDownloaded from




![Home Page [] · Transvenous Lead Extraction: Heart Rhythm Society Expert Consensus on Facilities, Training, Indications, and Patient Management - Bruce L. Wilkoff and al. Heart Rhythm](https://static.fdocuments.in/doc/165x107/5f768935a636bf51d33a812a/home-page-transvenous-lead-extraction-heart-rhythm-society-expert-consensus.jpg)