Arrhythmias - RCP London
51
Arrhythmias A simple guide to all things electrical Bradycardias
Transcript of Arrhythmias - RCP London

Arrhythmias A simple guide to all things electrical
Bradycardias

What’s Normal
• Heart rate
Normal at rest 60 – 100 / min
Bradycardia < 60 / min
Tachycardia >100 / min
expected ‘normal’ at peak exercise (220 – age)

Normal Electrics

Normal Pattern

Normal 12 lead ECG
P atrial
contraction
QRS
ventricular
contraction

Why are the leads different
Spine
LA
LV
RV
RA
V1 V2 V3
V4
V5
V6
R Arm L Arm
L Leg R Leg
AVf / II / III
AVr
AVL / I
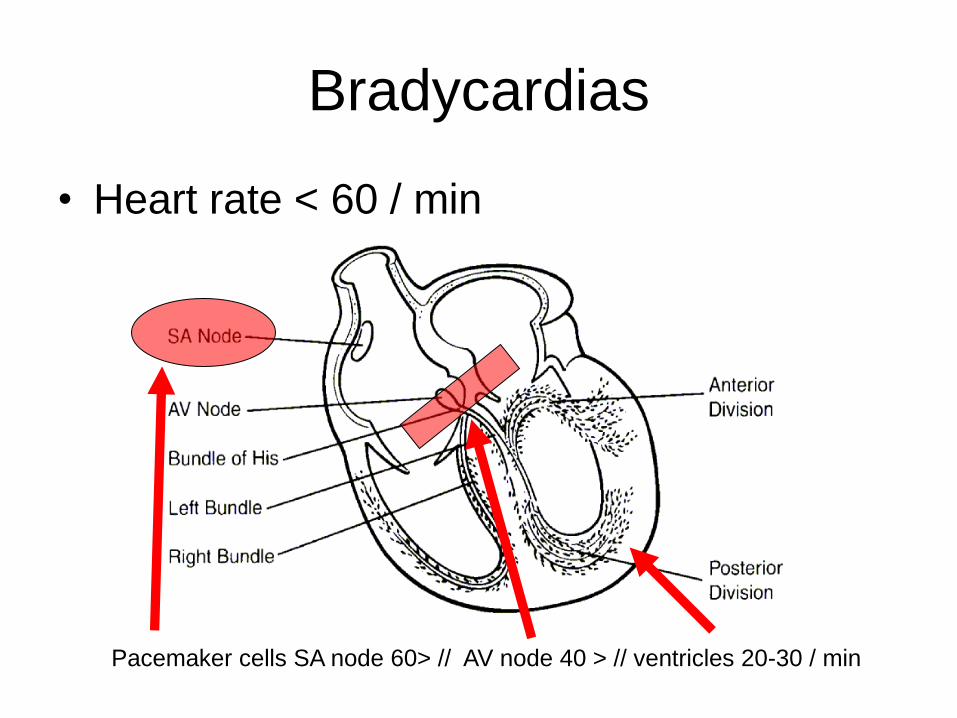
Bradycardias
• Heart rate < 60 / min
Pacemaker cells SA node 60> // AV node 40 > // ventricles 20-30 / min

First degree Block
P P P
R R R
PR interval – 200ms > (5 small squares >)

Second Degree Block
Mobitz Type 1
Wenkebach
PR P R P R P
//
PR

Second Degree Block
Mobitz Type 2
In this example transient 3:1 block
PR P R P P
//
PR
//

Third Degree Block
P P P P P
R R
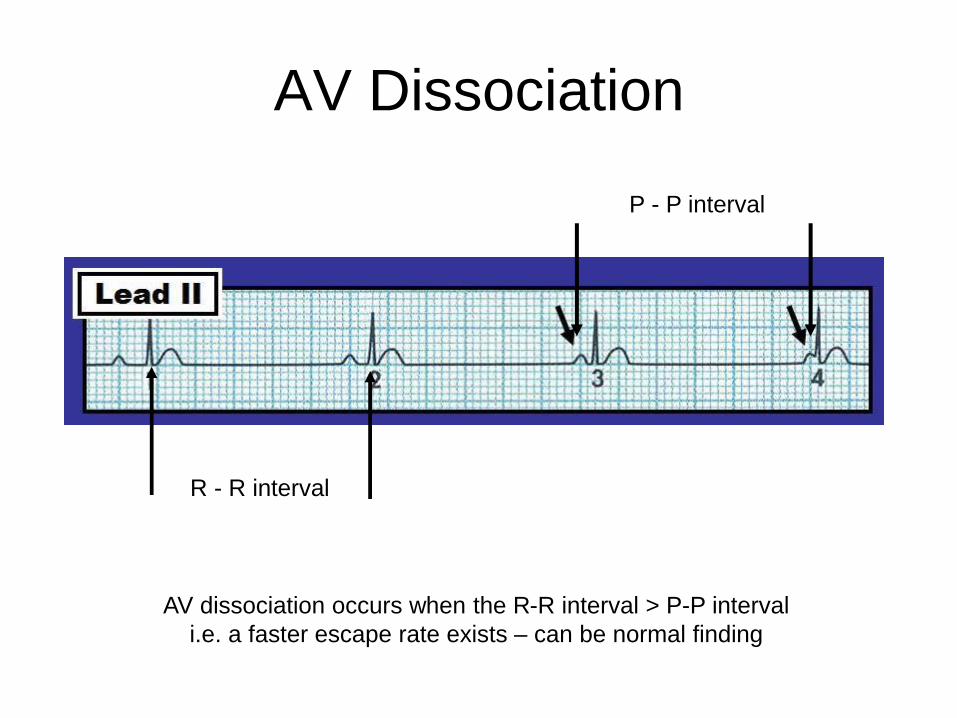
AV Dissociation
R - R interval
P - P interval
AV dissociation occurs when the R-R interval > P-P interval
i.e. a faster escape rate exists – can be normal finding

Pacemaker Indications

Types of pacemaker
Paced
Sensed
Action
Rate
AAIR A A I R
VVIR V V I R
DDDR D V I/T R

Cardiac Re-synchronisation
Therapy (CRT)
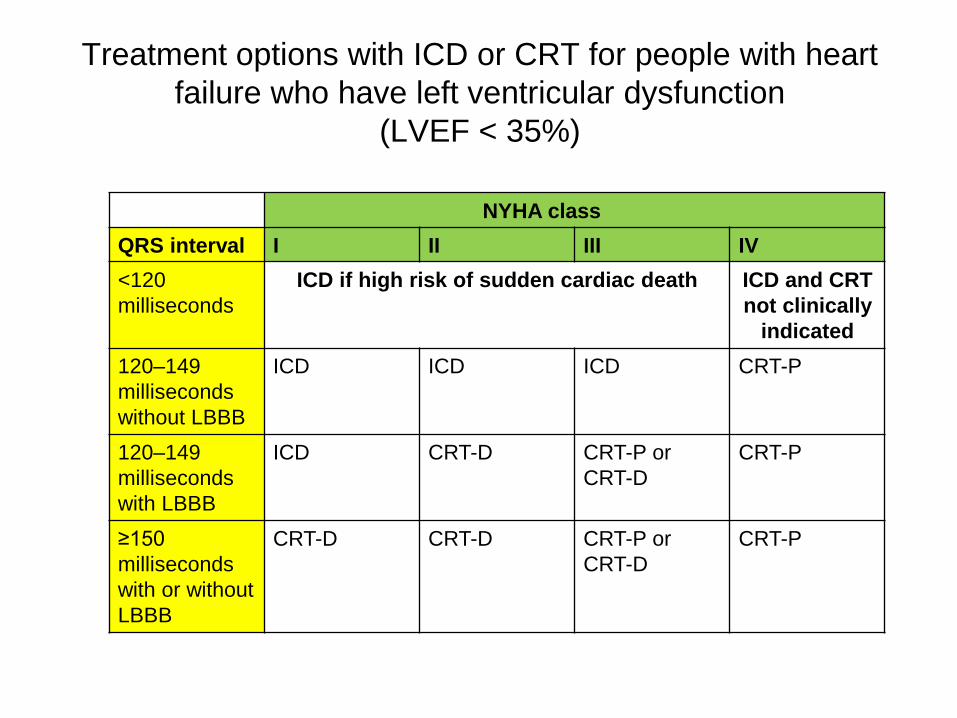
Treatment options with ICD or CRT for people with heart
failure who have left ventricular dysfunction
(LVEF < 35%)
NYHA class
QRS interval I II III IV
<120
milliseconds
ICD if high risk of sudden cardiac death ICD and CRT
not clinically
indicated
120–149
milliseconds
without LBBB
ICD ICD ICD CRT-P
120–149
milliseconds
with LBBB
ICD CRT-D CRT-P or
CRT-D
CRT-P
≥150
milliseconds
with or without
LBBB
CRT-D CRT-D CRT-P or
CRT-D
CRT-P

CXR appearances

Developing technologies
Leadless
pacemaker Sub-cutaneous
defibrillator
ILR Implant

Arrhythmias A simple guide to all things electrical
Tachycardia
Tachycardias
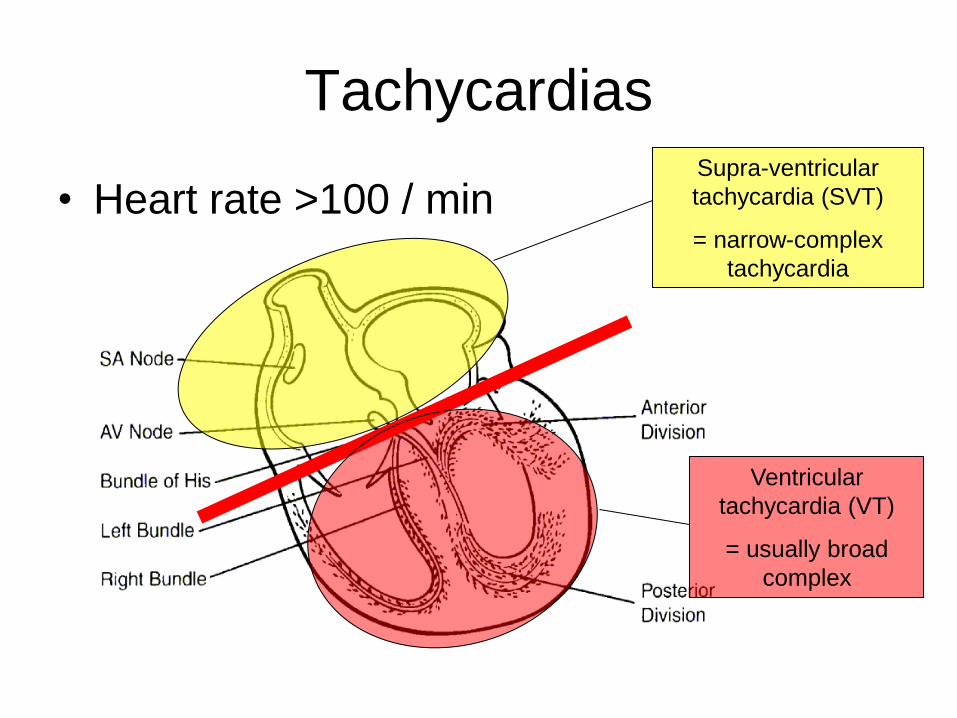
• Heart rate >100 / min Supra-ventricular
tachycardia (SVT)
= narrow-complex
tachycardia
Ventricular
tachycardia (VT)
= usually broad
complex

How to read a rhythm strip
1. Is there any electrical activity?
2. What is the ventricular (QRS) rate?
3. Is the QRS rhythm regular or irregular?
4. Is the QRS width normal or broad?
5. Is atrial activity present? (If so - P waves? Other atrial activity?)
6. How is atrial activity related to ventricular activity?
Mechanisms
• Automaticity
• Re-entrant circuits
• Accessory pathways (nodal and free wall)
• Ionic channelopathies

Pro-arrhythmia
SCAR
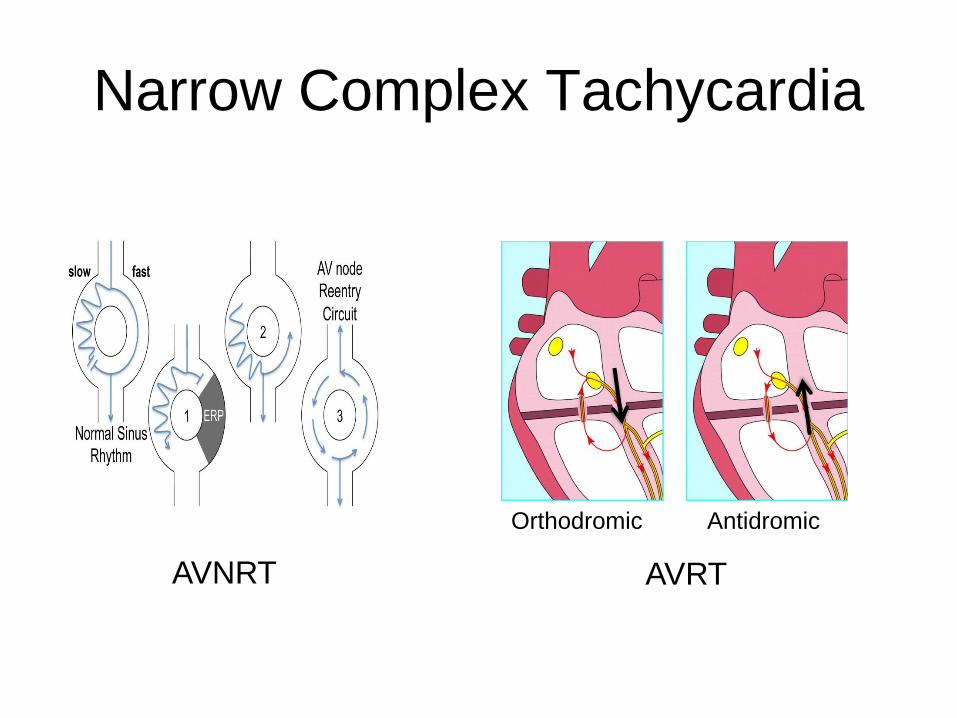
Narrow Complex Tachycardia
AVNRT AVRT
Orthodromic Antidromic

Patient Assessment
Adverse Signs
Reduced conscious level / syncope
Hypotension (SBP <90mmHg)
Chest Pain
Heart Failure
History
Description – rate / character
Frequency
Precipitants
Associated features
History of CHD / structural heart abnormality
Family history of SCD

Narrow Complex Tachycardia
AVNRT

Narrow complex tachycardia
• Terminate arrhythmia
– Adenosine
• Think about mechanism
• Future prophylaxis
• Definitive cure

Wolff-Parkinson-White Syndrome

WPW – orthodromic

WPW – antidromic AVRT

WPW – pre-excited AF

Atrial flutter
• Typical Flutter Ablation
• Increasing numbers
• Success rates >90%
– 5% recurrence, 25% AF
• First line or early second line prophylaxis
Drugs to cardiovert – Beta-blockers, amiodarone
Rate control – above + Digoxin, Verapamil
Electrical cardioversion / Ablation therapies

Atrial Fibrillation
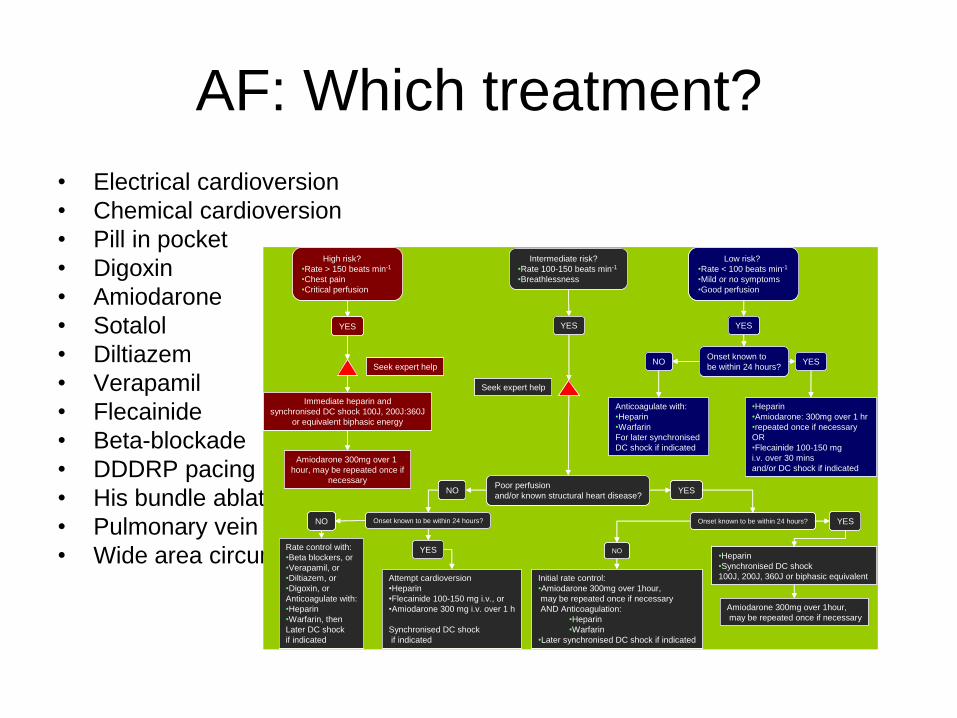
AF: Which treatment?
• Electrical cardioversion
• Chemical cardioversion
• Pill in pocket
• Digoxin
• Amiodarone
• Sotalol
• Diltiazem
• Verapamil
• Flecainide
• Beta-blockade
• DDDRP pacing
• His bundle ablation
• Pulmonary vein isolation
• Wide area circumferential ablation
Intermediate risk?
•Rate 100-150 beats min-1
•Breathlessness
Low risk?
•Rate < 100 beats min-1
•Mild or no symptoms
•Good perfusion
High risk?
•Rate > 150 beats min-1
•Chest pain
•Critical perfusion
YES
NO
Seek expert help
YES
Seek expert help
Immediate heparin and
synchronised DC shock 100J, 200J:360J
or equivalent biphasic energy
Amiodarone 300mg over 1
hour, may be repeated once if
necessary
Onset known to
be within 24 hours?NO YES
YES
YES
•Heparin
•Synchronised DC shock
100J, 200J, 360J or biphasic equivalentInitial rate control:
•Amiodarone 300mg over 1hour,
may be repeated once if necessary
AND Anticoagulation:
•Heparin
•Warfarin
•Later synchronised DC shock if indicated
Anticoagulate with:
•Heparin
•Warfarin
For later synchronised
DC shock if indicated
•Heparin
•Amiodarone: 300mg over 1 hr
•repeated once if necessary
OR
•Flecainide 100-150 mg
i.v. over 30 mins
and/or DC shock if indicated
Rate control with:
•Beta blockers, or
•Verapamil, or
•Diltiazem, or
•Digoxin, or
Anticoagulate with:
•Heparin
•Warfarin, then
Later DC shock
if indicated
Poor perfusion
and/or known structural heart disease?
Onset known to be within 24 hours?
Amiodarone 300mg over 1hour,
may be repeated once if necessary
NO
Onset known to be within 24 hours?
Attempt cardioversion
•Heparin
•Flecainide 100-150 mg i.v., or
•Amiodarone 300 mg i.v. over 1 h
Synchronised DC shock
if indicated
NO
YES
YES
Intermediate risk?
•Rate 100-150 beats min-1
•Breathlessness
Low risk?
•Rate < 100 beats min-1
•Mild or no symptoms
•Good perfusion
High risk?
•Rate > 150 beats min-1
•Chest pain
•Critical perfusion
YES
NO
Seek expert help
YES
Seek expert help
Immediate heparin and
synchronised DC shock 100J, 200J:360J
or equivalent biphasic energy
Amiodarone 300mg over 1
hour, may be repeated once if
necessary
Onset known to
be within 24 hours?NO YES
YES
YES
•Heparin
•Synchronised DC shock
100J, 200J, 360J or biphasic equivalentInitial rate control:
•Amiodarone 300mg over 1hour,
may be repeated once if necessary
AND Anticoagulation:
•Heparin
•Warfarin
•Later synchronised DC shock if indicated
Anticoagulate with:
•Heparin
•Warfarin
For later synchronised
DC shock if indicated
•Heparin
•Amiodarone: 300mg over 1 hr
•repeated once if necessary
OR
•Flecainide 100-150 mg
i.v. over 30 mins
and/or DC shock if indicated
Rate control with:
•Beta blockers, or
•Verapamil, or
•Diltiazem, or
•Digoxin, or
Anticoagulate with:
•Heparin
•Warfarin, then
Later DC shock
if indicated
Poor perfusion
and/or known structural heart disease?
Onset known to be within 24 hours?
Amiodarone 300mg over 1hour,
may be repeated once if necessary
NO
Onset known to be within 24 hours?
Attempt cardioversion
•Heparin
•Flecainide 100-150 mg i.v., or
•Amiodarone 300 mg i.v. over 1 h
Synchronised DC shock
if indicated
NO
YES
YES

Broad Complex Tachycardia
• ECG BCT

BCT - VT Discriminators
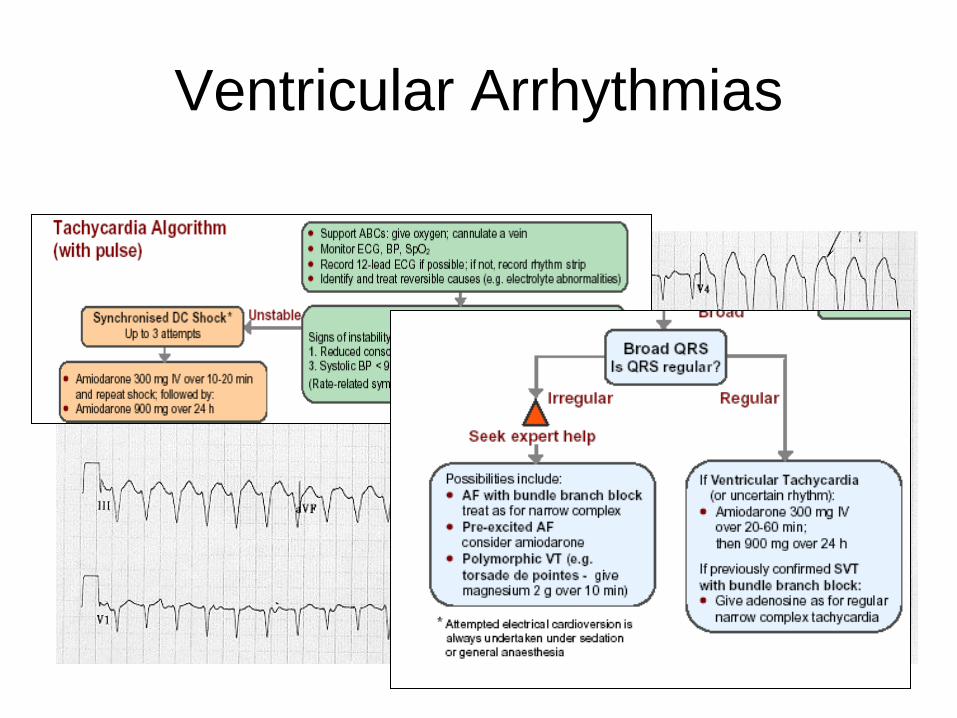
Ventricular Arrhythmias

Cardiac arrest is dangerous!
Total arrests
4888
Died before
admission
4173
Admitted
715
Discharged
303
WYMAS: 1987-1997
6%
Assessment Post Cardiac Arrest
• Cause of arrest apparent
(4H’s) Hypoxia / Hypovolaemia / Hyperkalaemia / Hypothermia
(4T’s) Toxins / Tension / Tamponade / Thrombo-embolic
• Has there been an acute ischaemic event ?
Troponins / ECG / Angiogram / MRI scarring pattern
• Any structural heart abnormaility ?
Echo / cardiac MRI / Signal averaged ECG / ETT
• Family history or genetic pattern to suggest inherited cardiac
condition (ICC) – Brugada (Ajmaline test) / Long & short QT’s / CPVT

SCD – Apical HCM
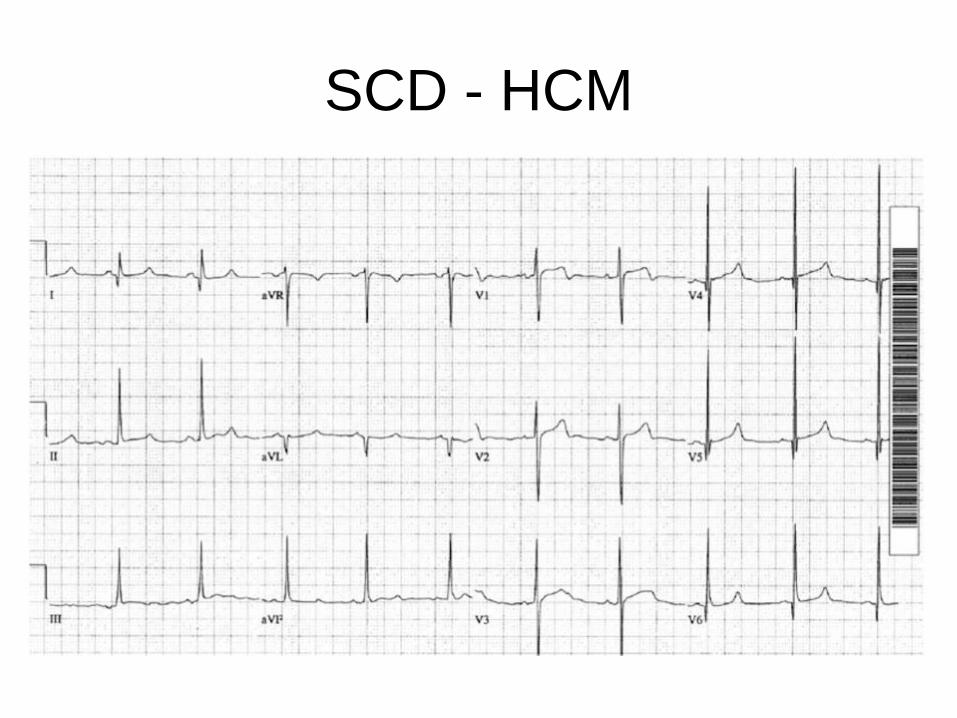
SCD - HCM

SCD - ARVD
Epsilon wave (most specific finding, seen in 30% of patients)
T wave inversions in V1-3 (85% of patients)
Prolonged S-wave upstroke of 55ms in V1-3 (95% of patients)
Localised QRS widening of 110ms in V1-3
Episodes of VT with LBBB morphology (i.e. right ventricular VT).

SCD – Long QT
• ECG polymorphic VT

SCD - Brugada

Antiarrhythmic Drugs
Arrhythmia Modifying Drugs
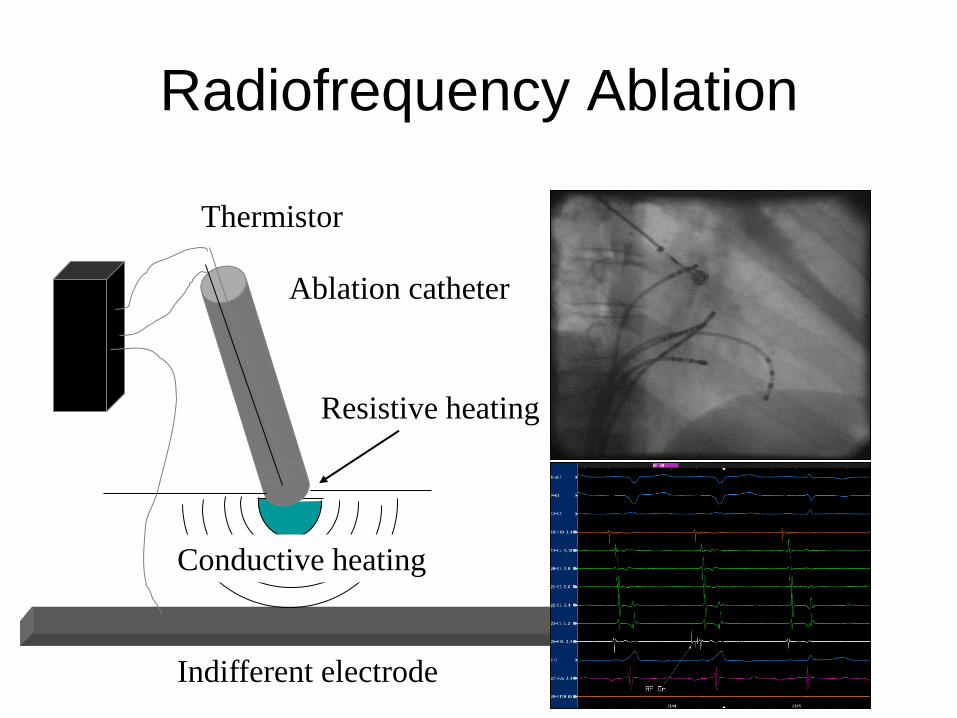
Radiofrequency Ablation
Resistive heating
Conductive heating
Ablation catheter
Indifferent electrode
Thermistor
Internal Cardiac Defibrillators
1) Survived a cardiac arrest caused by either VT or VF
2) Spontaneous sustained VT causing syncope or significant haemodynamic
compromise
3) Sustained VT without syncope or cardiac arrest, and also have LVEF <=35%
and symptoms are no worse than NHYA class III
4) Familial cardiac condition with a high risk of sudden death - long QT
syndrome, HCM, Brugada syndrome or ARVD or have undergone surgical repair
of congenital heart disease.

ICDs
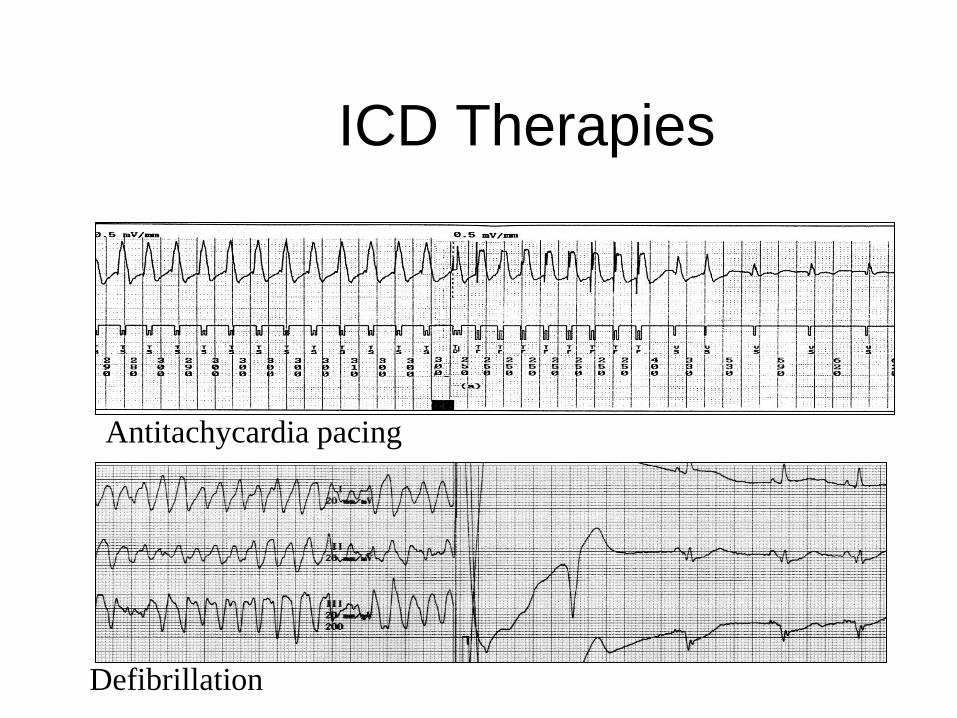
ICD Therapies
Antitachycardia pacing
Defibrillation

Conclusion
• Arrhythmia management has changed
• Devices and ablation are growing
• Drugs (esp class I) are declining
• Significant challenges await us
– Cost effectiveness of ICDs
– Epidemic of atrial fibrillation