Arrhythmias Mustafa Salehmohamed, D.O.. DEFINITIONS An arrhythmia is defined as any rhythm other...
87
Arrhythmias Arrhythmias Mustafa Salehmohamed, D.O.
-
Upload
dominic-phelps -
Category
Documents
-
view
220 -
download
0
Transcript of Arrhythmias Mustafa Salehmohamed, D.O.. DEFINITIONS An arrhythmia is defined as any rhythm other...

ArrhythmiasArrhythmias
Mustafa
Salehmohamed, D.O.

DEFINITIONSDEFINITIONS
An arrhythmia is defined as any rhythm other than normal sinus rhythm
Arrhythmias can be categorized as supraventricular or ventricular
Supraventricular arrhythmias can be further divided into tachyarrhythmias or bradyarrhythmias

SUPRAVENTRICULAR
ARRHYTHMIAS

SUPRAVENTRICULAR ARRHYTHMIAS
Any arrhythmia arising above the bifurcation of the His bundle is classified as supraventricular.
The QRS complex morphology either can be normal or may be wide owing to bundle-branch or fascicular block (aberrant conduction) or conduction over an accessory pathway (anomalous conduction or pre-excitation).
Supraventricular cardiac arrhythmias can be further sub-categorized into tachyarrhythmias or bradyarrhythmias.

TACHYARRHYTHMIAS
Sinus tachycardia is defined as a rapid sinus rhythm with a HR > 100bpm
Tachyarrhythmia is defined as an arrhythmia with a HR > 100bpm
Supraventricular tachyarrhythmias can occur either as isolated premature complexes or in the form of nonsustained or sustained tachycardias

PREMATURE ATRIAL CONTRACTIONSPREMATURE ATRIAL CONTRACTIONS
Premature atrial contractions (PACs) can arise from any part of the right or left atrium
The P wave morphology depends on the origin but differs from sinus rhythm
Frequent in normal persons and rarely cause symptoms
They are associated with respiratory disease, particularly in the presence of pulmonary hypertension

PREMATURE ATRIAL CONTRACTIONSPREMATURE ATRIAL CONTRACTIONS
Other precipitating factors include coffee, tea, alcohol, sympathomimetic cold remedies
If an etiology cannot be determined and treatment is necessary, a Beta -blocker can be given

AtrialAtrialTachycardiasTachycardias

Atrial FlutterAtrial Flutter
Atrial flutter is much less common than Atrial Fibrillation (AF)
Its hemodynamic consequences and management are similar to that of AF
It is due to a large reentrant circuit (several centimeters) that involves the low lateral right atrium

DiagnosisDiagnosis
ECG shows flutter waves, which (depending on rate) may look like discrete P waves or merge to form a classic sawtooth pattern
The atrial rate is 250 to 350 beats/min The ventricular rate depends on the AV conduction but typically is 150 to 220 beats/min
QRS complexes usually are normal Atrioventricular block may be consistent (2:1, 4:1, or
rarely 3:1 or 5:1) or may vary

Signs and SymptomsSigns and Symptoms
Symptoms depend principally on the resultant ventricular rate
If the rate is modest (< 120 beats/min) and regular (eg, stable 2:1 atrioventricular conduction), there may be no symptoms
Higher heart rates produce palpitations, and compromised cardiac output may produce dizziness and syncope

TreatmentTreatment
Medical therapy more likely to slow down ventricular response than to restore NSR
Medications used :• Digoxin
• Verapamil (works faster than digoxin but can cause hypotension
• Beta-blockers
• Class I drugs ( use with other drugs)
• IV Ibutilide (risk of developing Torsades)

TreatmentTreatment
If 1:1 conduction occurs with life-threatening rapid ventricular response rates (> 220 beats/min), immediate DC electroversion is indicated
Radiofrequency ablation (RFA) is emerging as an important approach for medically refractory atrial flutter.
The success rate is about 85% Some patients develop AF after the procedure

Atrial FibrillationAtrial Fibrillation

Atrial FibrillationAtrial Fibrillation
Atrial fibrillation (AF) is the most common sustained arrhythmia in adults
More than 2 million individuals in the United States have AF
With more than 160,000 new cases diagnosed every year
The incidence of AF increases with advancing age

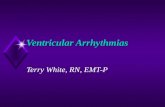
Atrial fibrillation Atrial fibrillation accounts for 1/3 of all accounts for 1/3 of all
patient discharges patient discharges with arrhythmia as with arrhythmia as principal diagnosis.principal diagnosis.
2% VF
Data source: Baily D. J Am Coll Cardiol. 1992;19(3):41A.
34% Atrial
Fibrillation
18% Unspecified
6% PSVT
6% PVCs
4% Atrial Flutter
9% SSS
8% Conduction
Disease3% SCD
10% VT

Prevalence of Atrial Fibrillation in the U.S.
Estimated prevalence of atrial fibrillation in the United States.8

EtiologyEtiology
Ischemic Heart Disease Hypertensive Heart Disease Rheumatic Valvular Disease Cardiomyopathy Non-rheumatic Valvular Disease Congenital Hear Disease CHF Pericarditis WPW

EtiologyEtiology
Thyrotoxicosis Pulmonary Embolism Chronic Lung Disease Pneumonia Neoplastic disease Post- operative states Normal heart affected by: alcohol, stress, drugs, excessive
caffeine, hypoxia, hypokalemia, hypoglycemia, infection

Atrial Fibrillation Atrial Fibrillation Morbidity and MortalityMorbidity and Mortality
Two fold increase in CV mortality
The most important consequence of AF are thrombo-embolic events
and stroke
AF is one of the most potent risk factors for stroke
4 – 6 fold increase risk of stroke/15 fold with h/o RHD
Persistent rapid ventricular rate associated with AF may lead to
tachycardia induced cardiomyopathy (reversible)
Limitation in functional capacity from symptoms of palpitations,
fatigue, dyspnea, angina, or CHF

DiagnosisDiagnosis
During AF, the atria have disorganized, rapid, irregular electrical activity exceeding 400 beats per minute
The ventricular response is also irregular and variable (irregularly irregular)
EKG: Absence of visible discreet P waves, or the presence of irregular fibrillation waves and an irregular ventricular response

DiagnosisDiagnosis
History – precipitating factors such as alcohol, caffeine,
sympathomimetic drugs
Laboratory studies: Electrolytes, TFTs, substance abuse-
toxicity screens
Echocardiogram
Holter (indicating arrhythmia: SVT, A. Flutter, Bradycardia
induced)
EST ( R/O ischemia)

Signs and SymptomsSigns and Symptoms
Palpitations Chest DiscomfortSigns of CHF - 2° to loss of atrial kick or
due to rapid rateWeakness, faintness, and breathlessnessSymptoms and signs of systemic emboli
(eg, stroke due to thrombus formation in the fibrillating atrium)

Atrial FibrillationAtrial Fibrillation
Paroxysmal
Chronic (chronic paroxysmal)
Acute (onset within 24 – 48 hrs)
Lone (younger than 60, no HTN no CVD
no Pulmonary disease)

TreatmentTreatment
Treatment goals are management of any underlying (causative) disorder, control of the ventricular response rate, restoration of sinus rhythm, and prevention of emboli
Rate control vs. Rhythm control

Medications for Rate ControlMedications for Rate Control
DigoxinBeta – blockersCalcium channel blockers (diltiazem,
verapimil)Short-term control of ventricular rate in
preparation for DC cardioversion is usually done with a beta -blocker or verapamil to avoid postconversion digoxin arrhythmias.

CardioversionCardioversion
Chemical Cardioversion• Class Ia and Ic Anti-arrhythmic Drugs (AEDs)• Amiodarone
in recent studies, prophylaxis with amiodarone before cardiac surgery has been found to decrease the occurrence of atrial fibrillation
Aasbo, J et al. Amiodarone prophylaxis reduces major cardiovascular morbidity and length of stay after cardiac surgery: a meta analysis. Ann Intern Med 143: 2005.

Pharmacologic CardioversionPharmacologic Cardioversion Class Ia agents
• procainamide (Procanbid)• quinidine (Quinidex, Quinaglute)• disopyramide (Norpace)
Class Ic agents• flecainide (Tambocor)• propafenone (Rhythmol)
Class III agents• amiodarone (Cordarone) - acute efficacy 16%-71%• sotalol (Betapace)• ibutilide - efficacy for flutter (63%), fib (31%)• dofetilide (Tikosyn)

CardioversionCardioversion
Electric cardioversion – method of choice for the hemodynamically Electric cardioversion – method of choice for the hemodynamically
compromisedcompromised
• Evaluate need for anticoagulationEvaluate need for anticoagulation
• R/O drug toxicityR/O drug toxicity
• AnesthesiaAnesthesia
• Synchronized 50 – 200 joules shockSynchronized 50 – 200 joules shock
Control of ventricular rateControl of ventricular rate
• AV nodal ablation with PPMAV nodal ablation with PPM
• Pulmonary vein ablation (maintenance)Pulmonary vein ablation (maintenance)

Atrial Fibrillation ManagementAtrial Fibrillation Management
Rate control versus rhythm control
• Advantage of maintaining NSR
• Adverse effects of antiarrhythmics
• After cardioversion even with antiarrhythmic therapy-50%
develop recurrent A.F after cardioversion
• Atrial Fibrillation Follow-up Investigation of Rhythm
Management (AFFIRM) : Anticoagulation advantageous

AFFIRMAFFIRM Atrial Fibrillation Follow-up Investigation of
Rhythm Management
Hypothesis: Effect on mortality of antiarrhythmic therapy to maintain sinus rhythm vs.
ventricular rate control alone, in the presence of anticoagulation
Primary endpoint: Total mortality
Secondary endpoint: Disabling CVACost of therapyQuality of life
NHLBI AFFIRM Investigators. Am J Cardiol. 1997;79:1198-1202.

Atrial FibrillationAtrial FibrillationManagement of the Risk of StrokeManagement of the Risk of Stroke
15 – 20% of ischemic strokes arise from emboli in the cardiac
chambers and valves
AF accounts for 45% of embolic strokes
Majority of emboli arise in the LAA
Other sources of emboli: LV thrombus Mitral valve disease (including
MVP and annular calcification), PFO Atrial septal aneurysm, and
complex aortic atheromatous plaques
Cerebrovascular disease may also be a cause of stroke

Transesophageal Echocardiogram Showing Thrombus
In this transesophageal echocardiogram, a thrombus (arrow) can be seen in the left atrial appendage (LAA).

Echocardiogram of Fibrillating Left Atrium
The smokelike echoes, or spontaneous echo contrast, in this transesophageal echocardiogram of a fibrillating left atrium are associated with prethrombotic conditions.

Protruding Atheroma in Descending Aorta
Protruding atheroma (arrows) in the descending aorta (DESC AO) is evident in this transesophageal echocardiogram.

Atrial FibrillationAtrial FibrillationManagement of the Risk of StrokeManagement of the Risk of Stroke
Anticoagulation with warfarin is twice as effective as
with Aspirin
SPAF III: compared warfarin vs. combination of low
dose warfarin and aspirin - in high risk AF patients
the combination was not as effective as warfarin.

Recommendations for Anticoagulation in AFRecommendations for Anticoagulation in AF Low risk patient (younger than 65) – do not need anticoagulation
Patients above 65 years who have AF should be anticoagulated. ACP
recommendation – INR 2.0 – 3.0 (reduces risk by 2/3)
Warfarin considered in younger patients with risk factors (previous TIA, HTN,
CHF, Diabetes, CAD. MS, Thyrotoxicosis)
Patients, who are high risk for bleeding – give ASA 325 mg/d
Patients 65 – 75 years with no risk – balance the the low risk of stroke with
side effects of therapy
Patients 75 years should receive oral anticoagulant

Atrial FibrillationAtrial FibrillationManagement of the Risk of StrokeManagement of the Risk of Stroke
Contraindications to AnticoagulationContraindications to Anticoagulation
Hemorrhage tendencies
Recent intra-cranial hemorrhage or neurosurgery
Recent hemorrhagic trauma
Recurrent or active bleeding
Diastolic BP>105
Other considerations
Risk of falling
Poor compliance with f/u
Uncontrolled siezure disorder

Atrial Fibrillation Management Atrial Fibrillation Management Cardioversion and the Risk ofCardioversion and the Risk of
ThromboembolismThromboembolism Risk of thromboembolism at cardioversion 0-5.6%
Dislodgement of a preexisting thrombus upon the return of the atrial
electrical and mechanical function (up to 4 weeks)
Formation and later dislodgment of newly formed thrombi, when
patient returns to NSR but atria in mechanical standstill
10-15% of patients with acute AF have thrombi on TEE
Most cardioversion related thrombi do not occur at cardioversion, but
are delayed for hours or weeks

Atrial Fibrillation Anticoagulation In Patients Atrial Fibrillation Anticoagulation In Patients Undergoing CardioversionUndergoing Cardioversion
Those with A.F. longer than 2 days or of unknown duration should receive anticoagulation
Warfarin should be given 3 weeks before cardioversion and 4 weeks after cardioversion
Anticoagulation beyond 4 weeks should be considered in patients with cardiomyopathy h/o previous ambolus or mitral valve disease
TEE role in cardioversion • Useful in r/o thrombus and facilitating early cardioversion by using
short term anticoagulation
• Acute trial: compared TEE directed approach with brief anticoagulation to conventional

Treatment Protocol in ACUTE Study
Treatment protocol used in Assessment of Cardioversion Using TEE (ACUTE) multicenter pilot study. The study involved 126 patients randomized into one of two treatment groups: the TEE guided group (62 patients) and the conventional-treatment group (64 patients).

Multifocal Atrial TachycardiaMultifocal Atrial Tachycardia
Presents similarly to AF but arise not by multiple interlacing wavelets of reentry (as in AF) but by focal pacemaker abnormalities
The term multifocal atrial tachycardia implies several different P wave morphologies (at least 3 different morphologies)
Atrial rates range between 100 and 250 beats per minute, and the ventricular response depends on the status of AV conduction
A 1:1 P wave-to-QRS complex ratio is common with rates less than 200 beats per minute, whereas at higher rates various degrees of block (e.g., 3:2, 2:1, 3:1) are common

Multifocal Atrial TachycardiaMultifocal Atrial Tachycardia
Causes• Chronic Obstructive Lung Disease• Any other underlying pulmonary disorders can
cause MAT• Can be exacerbated by theophylline

TreatmentTreatment
Treat underlying diseaseSimilar treatment as AFHowever beta-blockers contraindicated in
those whose MAT is caused by lung diseaseDigoxin is not as useful and may even
exacerbate the tachycardiaUse calcium channel blockers

Regular Atrial TachycardiasRegular Atrial Tachycardias 1) Sinus Tachycardia: physiologic or pathologic increase of sinus rate >
100 bpm. Treat the condition causing the tachycardia, not the tachycardia itself. However, in cases of acute MI sinus tachycardia must be controlled to
prevent myocardial ischemia (beta blockers or Ca-channel blockers)
2) Paroxysmal Atrial Tachycardia: sudden onset, a normal heart, HR 150-250 bpm.
P waves may be not visible because buried in the QRS complex or the T wave
Therapy: quiet setting and comfort the patient to reduce sympathetic discharge. Increase vagal tone by carotid sinus massage or valsalva maneuver. Medical therapy: Beta-blocker, Ca channel blocker, digoxin, adenosine. If angina, hypotension, or CHF then consider cardioversion.

Supraventricular TachycardiasSupraventricular Tachycardias
Atrial Tachycardia Atrial Fibrillation/flutter AV nodal reentry (micro) tachycardia AV reentry tachycardia (macro) - WPW Syndrome or concealed
accessory pathway
If the patient is very symptomatic or breaks through drugs, consider catheter ablation

Supraventricular Tachycardias

Supraventricular TachycardiaSupraventricular Tachycardia Atrioventricular Nodal Reentry TachycardiaAtrioventricular Nodal Reentry Tachycardia
(AVNRT)(AVNRT)
The most common type of paroxysmal SVT (PSVT)
AVNRT accounts for 50 – 60% of PSVT
AVNRT present later than SVT related to accessory
pathways (frequently after 20 years of age)

Tachycardia Induction-Reentry
During sinus rhythm, antegrade conduction occurs through both the fast pathway and the slow pathway. However, the fast-pathway conduction predominates and the atrioventricular conduction time is short. If a premature atrial beat blocks in the antegrade fast pathway, atrioventricular (AV) conduction proceeds via the slow pathway. Then, if the fast pathway recovers quickly enough to permit retrograde conduction, atrial echoes or typical slow-fast atrioventricular nodal reentrant tachycardia (AVNRT) occurs. This simplified diagram demonstrates only one method of tachycardia induction and implies the requisite tachycardia circuit is confined to the compact AV node.

AVNRT

Supraventricular TachycardiaSupraventricular Tachycardia AVNRT Diagnosis AVNRT Diagnosis
• The typical HR ranges 150 – 250 bpm
• Palpitation, light headedness and near-syncope may accompany the
paroxysm.
• True syncope unusual
• Neck pounding (connon waves) is pathognomonic of AVNRT

AVNRT Acute ManagementAVNRT Acute Management
Vagal maneuver (carotid Sinus Massage, valsalva
maneuver)
Adenosine (6 mg, 12mg, 12mg, 18mg)
Verapamil 5 – 10 mg I.V.P
If hypotension, angina or CHF is precipitated by AVNRT –
DC cardioversion (25 – 50 joules)

AVNRT AVNRT Chronic Pharmacologic ManagementChronic Pharmacologic Management
Long term pharmacological approach is still reasonable Digoxin – sometimes effective Beta-blockers - when arrhythmia induction is catecholamines
dependent Verapamil (240 mg qd) - may cause constipation, fatigue, flushing,
edema Diltiazem Class I agents (quinidine, flecainide) Amiodarone (Tissue toxicity) Catheter – RF ablation (success rate 94 – 100%, complete AV Block
2 – 4%)

Wolff – Parkinson – White Syndrome Wolff – Parkinson – White Syndrome and Concealed Accessory Pathwayand Concealed Accessory Pathway
Normal AV conduction is limited antegrade conduction to a single pathway through the AVN
Presence of an alternative pathway of AV conduction creates the potential for reentry
tachycardia
The most prominent manifestation of an accessory pathway is the wolff-parkinson – white
(WPW) syndrome
In WPW the accessary pathway can be located at various regions of the AV ring (most
common – left free wall of the mitral annulus)
In WPW a sinus beat will travel both through the accessory pathway (conducts like muscle,
no decremental conduction) and the AVN – HIS – Purkinji- system, creating a fusion beat.
The EKG presentation: short PR, Delta wave (may mimic a Q wave)

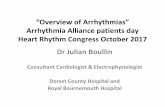
WPW- Left Free Wall Accessory Pathway
(a) Activation of the ventricles via an accessory pathway precedes earliest activation through the His-Purkinje system and results in a slurring of the QRS onset called a delta wave. (b) A more subtle delta wave is produced when there is minimal preexcitation, as shown in this example of a left free wall accessory pathway. Delta waves can be mistaken for infarction Q waves. For example, a posteroseptal accessory pathway produces a delta wave that mimics an inferior MI (a). (b) ECG changes related to early activation at the base of the LV free wall include the negative delta wave in lead aVl and the large R wave in V1, which can be mistaken for a posterolateral wall MI.

WPW Clinical PresentationWPW Clinical Presentation
Begin in teenage years – early adulthood
(pregnancy may precipitate).
Symptoms: Palpitations with or without dizziness,
syncope, SOB, weakness or chest pain. Sometimes
diuresis.

WPW Electrocardiographic FindingsWPW Electrocardiographic Findings
Tachyarrhythmia associated with the WPW can be of
several types
• Orthodromic reentry tachycardia
Most common (QRS narrow, no short PR, no delta)
• Antidromic reentry tachycardia
• Atrial fibrillation, may produce very rapid tachycardia with
QRS complexes that may cause syncope or S.D.

ECG During Reentrant Tachycardia
Electrocardiograms taken during episodes of reentrant tachycardia in a patient with the WPW syndrome reveal both antidromic and orthodromic tachyarrhythmias. (a) During an antidromic episode, the QRS complex is wide, resembling the morphology seen in VT. The
impulse then travels retrogradely up the AV node to the atria before reentering the ventricle via the accessory pathway. (b) In the orthodromic reentrant tachycardia, the QRS complex is narrow in all leads. The ventricle is activated strictly via the AV node, followed
by retrograde propagation of the impulse via the accessory pathway to the atria.


WPW ManagementWPW Management Asymptomatic patient
• need for invasive evaluation unclear. Competitive athletes and Pilots probably should be evaluated.
Acute Management: • Vagal maneuver • Procainamide• DC Cardoversion
Long-term Management• Flecainide (N. CAD, Normal LVF)• Amiodarone• Catheter Ablation

Concealed Accessory PathwayConcealed Accessory Pathway
An accessory pathway that conduct only in the
retrograde direction
Antegrade conduction only via normal pathway –
therefore preexcitation not present (no short PR, no
Dela waves) during NSR
Can participate in a reentry circuit. (AVRT)

Ventricular ArrhythmiasVentricular Arrhythmias
These are arrhythmias with broad QRS complexes (>120 ms in duration)• Ventricular tachycardia (VT)
Torsades de pointesPolymorphic VTAccelerated idioventricular rhythm
• Ventricular flutter/ fibrillation (VF)

Ventricular TachycardiaVentricular Tachycardia
Sustained ventricular tachycardia is defined as VT that persists for >30 s
VT generally accompanies some form of structural heart disease, most commonly chronic ischemic heart disease associated with a prior myocardial infarction.
Sustained VT may also be associated with nonischemic cardiomyopathies, metabolic disorders, drug toxicity, or prolonged QT syndrome, and it occurs occasionally in the absence of heart disease or other predisposing factors

Ventricular TachycardiaVentricular Tachycardia
Nonsustained VT (three beats to 30 s) is also associated with cardiac disease but occurs in its absence more often than the sustained arrhythmia.
While nonsustained VT usually does not produce symptoms, sustained VT is almost always symptomatic
It is often associated with marked hemodynamic compromise and/or the development of myocardial ischemia

Ventricular TachycardiaVentricular Tachycardia
The most important clinical predictor of VT is the presence of structural heart disease
The observation of intermittent cannon a waves and varying first heart sounds suggests AV dissociation and is diagnostic of VT
In a majority of cases, the diagnosis can and should be made by close examination of the 12-lead ECG

Ventricular TachycardiaVentricular Tachycardia
The ECG diagnosis of VT is suggested by a wide-complex QRS tachycardia at a rate exceeding 100 beats/min.
The QRS configuration during any episode of VT may be uniform (monomorphic) or it may vary from beat to beat (polymorphic).

Ventricular TachycardiaVentricular Tachycardia
Treatment• Immediate treatment of hypotensive VT requires synchronized DC
shock
• Drug treatment of VT is lidocaine 100 mg IV given over 2 min with a further 50 mg IV 5 min later if the arrhythmia has not reverted
• A second antiarrhythmic drug (flecainide, encainide, propafenone, procainamide, disopyramide, mexiletine, tocainide) may be used if DC cardioversion (or programmed stimulation) is unavailable or if the patient is not hemodynamically compromised and has shown no adverse response to lidocaine

Ventricular TachycardiaVentricular Tachycardia
All patients with sustained VT should be investigated by invasive electrophysiology and therapy selected accordingly
Long-term prophylaxis of VT may be achieved by any class Ia, Ib, Ic, II, or III drug
Calcium channel blockers – specifically diltiazem and verapimil are contraindicated because of reports of hemodynamic collapse and fatalities

Torsades de PointesTorsades de Pointes
Torsade de pointes or twisting of the points, causes symptoms and death in patients with the rare congenital long QT syndromes
Its importance in everyday practice is its provocation by drugs (especially antiarrhythmics, which are contraindicated in its further management) or electrolyte imbalance.
Management is to stop all cardioactive drugs (eg, antidepressants, antiarrhythmics, phenothiazines), normalize electrolytes (particularly K and Mg), and stabilize cardiac electrophysiology, if necessary by atrial overdrive pacing

Ventricular FibrillationVentricular Fibrillation
A rapid irregular ventricular rhythm due to multiple reentrant activity associated with essentially zero cardiac output
Causes :• Ischemic heart disease
• Severe hypoxia
• Electrical accidents
• Antiarrhythmic drugs
• WPW with rapid Afib
• After reperfusion therapy

Ventricular FibrillationVentricular Fibrillation
Clinical picture• Shock• Syncope• Sudden Death

Ventricular FibrillationVentricular Fibrillation
Treatment• Fatal unless patient defibrillated• Patients with recurrent VF benefit from
Automated Implantable Cardioverter Defibrillator( AICD)

Transvenous Cardioverter-Defibrillator
The transvenous implantable cardioverter-defibrillator is usually installed in the pectoral region. A transvenous defibrillating lead is inserted into the subclavian vein and advanced into the apex of the right ventricle. When a persistent ventricular tachyarrhythmia with a rate faster than the programmed rate cutoff is detected by the rate-sensing electrode in the lead's tip, the device charges and delivers a high-voltage shock between the right ventricular defibrillating elec-trode and the metal casing of the defibrillator, which serves as the return electrode (anode) for defibrillating shocks.

Congenital Long QT SyndromeCongenital Long QT Syndrome Usually present as syncope (cardiac arrest – rare)
Recurrent rapid episodes of polymorphic VT
Many youngsters are incorrectly diagnosed with grand mal seizures
The arrhythmia is triggered by an adrenergic surge (physical, emotional or auditory stimulus)
Family h/o S.D or syncope
QTC of longer than 0.46 sec in man and 0.48 sec in woman is abnormal
Jervell – large – Nielson – autosomal recessive with deafness
Romano – ward – autosomal dominant with no deafness
50% of affected experience SD or syncope by age 12.
Risk factors for SD: congenital deafness, h/o syncope, VT/NSVT on holler, female gender
Any patient or family member with one risk factor should be treated with beta - blockers

Schwartz PJ. Curr Probl Cardiol. 1997;22:297-351. Smith WM. Ann Intern Med. 1980;93:578-584. Garson A Jr. Circulation. 1993;87:1866-1872.
Long QT SyndromeLong QT Syndrome
Idiopathic LQTS is a congenital disorder that may lead to unexplained syncope, seizures, and SCA
Patients either remain asymptomatic or are prone to symptomatic and potentially lethal arrhythmias
A positive family history of LQTS or SCA is present in 60% of LQTS patients
Due to the hereditary linkage, it is necessary to identify other family members at risk

Bradyarrhythmias

Sick Sinus Syndrome(SSS)Sick Sinus Syndrome(SSS)
A wide variety of abnormalities of sinus node function
It is an intrinsic defect of the sinoatrial nodeConsists of:
• Sinus bradycardia• Sinoatrial blocks• Sinus arrest

SSSSSS
Bradycardia-tachycardia syndrome is an important variant of sick sinus syndrome, in which atrial flutter and fibrillation alternate with prolonged asystolic periods

Signs and symptomsSigns and symptoms
AsymptomaticLethargySyncope FatigueCHFTachycardia phases are often perceived as
palpitations

TreatmentTreatment
Permanent Pacemaker Placement – dual chamber preferred
Beta- blockers for paroxysmal tachycardic component

Atrioventricular BlocksAtrioventricular Blocks
First degree heart blockSecond degree heart block
• Wenkebach ( Mobitz type I) block• Mobitz type II block
Third Degree or Complete heart block (CHB)

First degree blockFirst degree block
PR interval is greater than normal (usually > 0.20 sec) It is asymptomatic and may be physiologic. It is often seen
in well-trained athletes, the young, and those with high vagal tone
It is a common manifestation of digitalis effect (not necessarily toxicity)
First-degree heart block is asymptomatic and may be physiologic.
It is often seen in well-trained athletes, the young, and those with high vagal tone
Treatment is not mandated but further testing maybe

Second degree heart blockSecond degree heart block
Mobitz type I or Wenkebach• progressive PR prolongation, a QRS complex is
dropped with restoration of atrioventricular nodal conduction and a repetition of the sequence
• It is seen most often as a transient abnormality with inferior wall infarction or with drug intoxication, particularly digitalis, beta blockers, and occasionally calcium channel antagonists
• Most of the time patients are asymptomatic and only need to be observed

Second degree heart blockSecond degree heart block
Mobitz type II• PR interval is constant but there is an unexpected dropped
QRS complex• Mobitz type II block may occur in the setting of
anteroseptal infarction or in the primary or secondary sclerodegenerative or calcific disorders of the fibrous skeleton of the heart
• It is important to recognize this type of block because it has a high incidence of progression to complete heart block with an unstable, slow, lower escape pacemaker
• Therefore, pacemaker implantation is necessary in this condition

Third degree heart blockThird degree heart block
There is no electrical communication between the atria and the ventricles.
Heart rate is maintained by an escape junctional (atrioventricular node or His) or ventricular pacemaker
Signs/symptoms - lethargy, postural hypotension, breathlessness, syncope, dizziness, acute heart failure and asystole

Third degree heart blockThird degree heart block
Treatment is based on cause of CHB Digoxin as a cause- stop drug and cautious restarting at a
lower dose; may need temporary pacemaker in the interim With an inferior wall MI, use of atropine is usually
sufficient, since CHB resolve with healing With an anterior wall MI, damage is extensive requiring
emergent transvenous pacemaker insertion for a CHB Usually resolution of CHB does not occur following an
AWMI, warranting the need to insert a permanent pacemaker (DDD dual chamber pacemaker)