Armaan Khalid. HF is a syndrome that manifests as the inability of the heart to fill with or eject...
37
Armaan Khalid Heart Failure 101
-
Upload
victoria-montgomery -
Category
Documents
-
view
214 -
download
1
Transcript of Armaan Khalid. HF is a syndrome that manifests as the inability of the heart to fill with or eject...
Armaan Khalid
Heart Failure 101

HF is a syndrome that manifests as the inability of the heart to fill with or eject blood
HF can result from any structural/functional cardiac disorder that impairs the ability of the heart to function normally
Coronary Artery Disease (CAD) is the most commonest cause of HF
Anything that ↑ myocardial work may aggravate/initiate HF
What is Heart Failure?

Ischaemic Heart Disease (35-40%)Cardiomyopathy (dilated) (30-34%)Hypertension (15-20%)
Common Causes of HF

EXTREMELY COMPLEX!Compensatory physiological changes that
eventually get overwhelmed & become pathological
Factors involved are:Venous return (preload)Outflow resistance (afterload)Myocardial contractility (inotropic state)Salt & water retention
Pathophysiology

Stroke work is increased as ventricular end diastolic volume is raised (e.g. ↓ ejection fraction)↑ Preload will ↑ cardiac contractilityCompensatory mechanism
Frank-Starling’s Law of the Heart

SV is the volume of blood pumped from one ventricle of the heart with each heart beatUsually assumed to be the Left
SV = EDV – ESVEjection Fraction = SV / EDVDeterminants
PreloadSV is controlled by preload due to Frank-Starling’s Law
Afterload↑ Afterload will ↓ SV
Contractility↑ Ca2+
Stroke Volume

In HF, ejection fraction ↓Can be compensated by ↑ heart rate (sinus
tachycardia)In severe myocardial dysfunction, cardiac output can
only be maintained by ↑ venous pressure (Preload) &/ ↑ tachycardiaLow functional reservePerfusion only maintained to vital organs (huge
impact)Causes dyspnoea,
hepatomegaly, ascites, oedemaDue to ↑ venous pressure
Venous Return (Preload)

Afterload is defined as the myocardial wall tension developed during systolic ejection
It is formed by:Pulmonary & systemic resistancePhysical characteristics of the vessel wallsVolume of blood that is ejected
↑ in afterload ↓ cardiac output↑ end-diastolic volume↑ dilatation of the ventricle↑ AFTERLOAD
Vicious cycle
Outflow Resistance (Afterload)

Sympathetic nervous system is activated in early HF as a compensatory mechanism Inotropic support & maintains cardiac output
Chronic sympathetic activation leads to ↑ neurohormonal activation & myocyte apoptosis
Also causes ↑ cytosolic Ca2+ entryAugments myocardial contractility Impairs myocardial relaxation (lusitropy)
Myocardial Contractility

↓ CO leads to diminished renal perfusionActivation of RAAS↑ Aldosterone production to retain salt &
waterExacerbates increased venous pressure
Salt & Water Retention

Primary response to chronic ↑ wall stress is myocyte hypertrophy, apoptosis & regeneration
Myocardial remodelling is pathological (eccentric)Worsens the situation↑ stress on remaining myocytes
Myocardial Remodelling

Left Heart FailureClinical features
Fatigue, dyspnoeaCardiomegalyOn auscultation,
gallop rhythmCrackles in lung
basesPulmonary oedema
Clinical featuresFatigue, dyspnoea,
anorexia, nauseaJugular venous
distensionHepatomegalyPitting oedemaAscitesPleural transudates
Findings
Right Heart Failure
FBE/LFT/U&E/TFT/Cardiac troponinsCXR (to be discussed)ECG
Signs of ischaemia, MI, ventricular hypertrophy, LBBB
Echo (TTE/TOE)? Stress
BNPHighly indicative of CHF & poor prognosis factor
? Cardiac Biopsy? Cath Lab
Workup

Diagnosing Heart Failure

EducateObesity controlDietary modification
Low salt, minimise EToH +/- fluid restrictionSmokingSexual activityExercise
Light exercise is encouragedVaccination
General Lifestyle Advice

Heart Failure Treatment Guidelines

Overall Management Plan

Presents typically as 1 of 2 radiographic patterns:Pulmonary interstitial oedemaPulmonary alveolar oedema
Which radiographic pattern appears depends on the pulmonary (venous) capillary wedge pressure (PCWP)
Radiological Findings in CHF

4 key radiographic signs:Thickening of the interlobular septa
Kerley B linesNamed after Irish neurologist & radiologist, Peter
James KerleyPeribronchial cuffingFluid in the fissuresPleural effusions
Pulmonary Interstitial Oedema

Spot diagnosis!

Thickening of the interlobular septaNot visible on normal CXROnly visible when it accumulates excessive
fluid, PCWP about 15 mm HgVisible on frontal CXR, @ lung bases, @/ near
costophrenic anglesVery short (1-2cm), very thin (1mm) &
horizontal in orientationChronic Kerley B Lines
After repeated episodes of pulmonary interstitial oedema, fibrosis occurs
Kerley B Lines

A, B, C!

Yes, there are A & C lines unfortunatelyKerley A Lines
Appears when connective tissue around the bronchoarterial sheaths in the lungs distends with fluid
Extends from the hila (up to 6 cm) & don’t extend to the lung peripheries
Kerley C LinesIf you know what they are, you are wasting
time in this lecture? Overlap b/w A & B Lines? Myth
Kerley A Lines

Doughnuts!

Bronchi may only be visible when seen on-end in the region of the pulmonary hilaAnywhere else, it is pathological
Fluid collects in the interstitial tissue surrounding the wall of the bronchiBronchial wall becomes ‘thicker’ & appears as
doughnuts when seen on-endSame mechanics as air bronchograms
Peribronchial Cuffing

Normal & Pathological

The fissures may normally be visible however, are almost never thicker than a line drawn with a sharp pencil
Fluid may collect b/w the 2 layers of the visceral pleura or subpleural spaceAccumulated fluid distends the fissure(s)
Thicker, irregular & more visible
Fluids in the Fissures

Spot the Difference

Pleural effusions caused by CHF are usually bilateralWhen it is unilateral, almost always right-sided
Therefore when you see a left-sided pleural effusion, considerMets, TB, thromboembolic disease, etc
Laminar Pleural EffusionThin, band-like density along lat chest wall,
esp. near costophrenic angles (still sharp)Almost always due to left atrial pressure ↑↑↑
CHFLymphangitic spread of malignancy
Pleural Effusions

Which one is it?

Fluid spills out of the interstitium & into the airspaces when PCWP is sufficiently ↑↑↑ (25 mm Hg)
Almost known as Pulmonary OedemaRadiographic finding
Fluffy, indistinct patchy airspace densitiesOuter 1/3 usually sparedLower zones > Upper zonesButterfly/Bat-wing appearancePleural effusions usually present when the
oedema is cardiogenic in nature
Pulmonary Alveolar Oedema
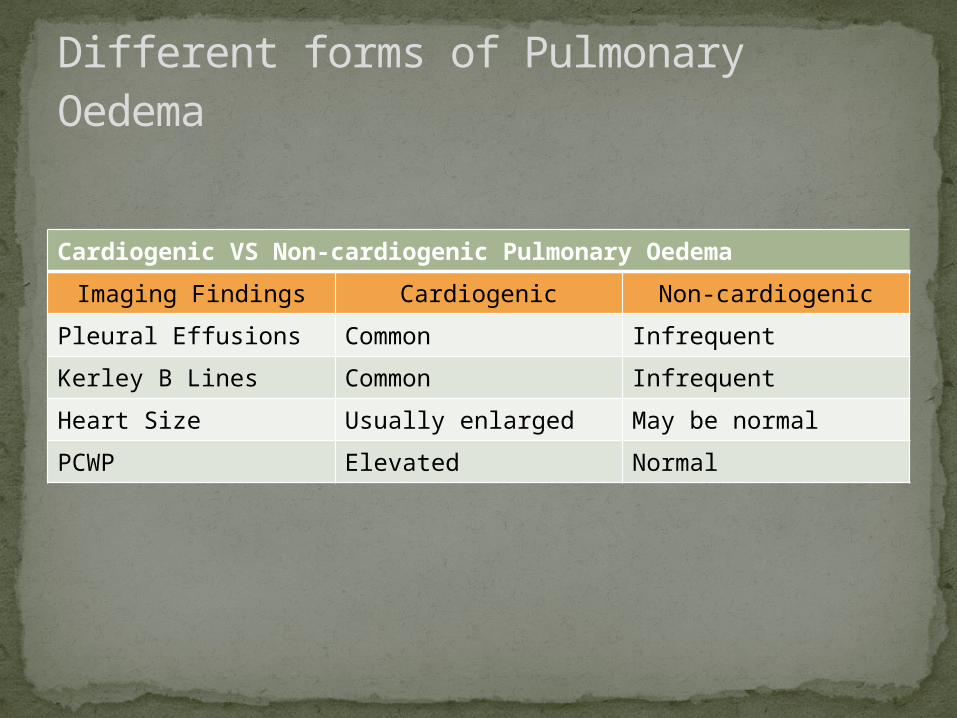
Cardiogenic VS Non-cardiogenic Pulmonary Oedema
Imaging Findings Cardiogenic Non-cardiogenic
Pleural Effusions Common Infrequent
Kerley B Lines Common Infrequent
Heart Size Usually enlarged May be normal
PCWP Elevated Normal
Different forms of Pulmonary Oedema

Mr XY, 80 y/o pensionerHOPC sudden & extreme SOBWheezing & diaphoreticCoughing with pink frothy sputumCold peripheriesGallop rhythm
DifferentialsInvestigationsManagement
Emergency!!!

a) Asthmab) COPDc) Pneumoniad) Pulmonary oedemae) All of the above
Differentials???

CXRECGU&E, Cardiac Troponins, ABGBNPEcho
Investigation!!!

Could this be Pneumonia?

Sit upright & OxygenIV access & ECG monitoringMorphine (5-10mg) +/- metoclopramide (10mg)
Beware of morphine systolic BP < 90 mm HgIV diuretics (furosemide 40-80 mg slowly)GTN (spray 2 puffs/ 2 x 0.3 mg SL)
Don’t give if systolic BP < 90 mm HgConsider nitrate infusion if systolic BP > 100 mm Hg
Isosorbide dinitrate 2-10mg/h IVEvaluate situation
If worsening, consider more diuretics & venesectionGet HELP!!!
Management