Arm edema is influenced by the extent of axillary surgery in patients treated with primary XRT
1
78 Radiation Oncology ?? Biology ?? Physics October 1984, Volume 10, Sup.2 3 m EDaN 1s EWLU’ iNCED BY THE EXTENT OF AXILLARY SURGERY IN PATIENTS'TREATED WITH PRIMARY XRT David Larson f Mark Weinstein! Itzhak Goldberg? Jay Harris1 1Joint Center for Radiation Therapy, 2 Beth Israel Hospital, Department of Surgery Arm edema is one of the most trying complications of primary treatment for carcinoma of the breast. It is bothersome to patients both functionally and cosmetically, and is poorly treated by currently available techniques. In order to determine treatment factors associated with the development of arm edema, we reviewed the records of 105 patients treated by axillary surgery and primary radiation therapy between July 1968 and December 1979 for whom adequate surgical records were available. Median follow-up was 63 months (39-161 mos.) . Of these 105 patients, 47 had a lower axillary sampling (removal of a portion of the lower axillary contents without formal bourdaries, varying from a simple node biopsy to excision of the axillary fat pad), 37 had a iower axillary dissection (removal of the lower axillary contents with formal boundaries: latissimus dorsi, tail of the breast, axillary vein, pectoralis major) and 11 had full axillary dissection (removal of entire axillary contents with stripping of the axillary vein). In 10 patients, the type of axillary dissection could not be easily classified into one of these 3 groups. The extent of surgery was left to the discretion of the individual surgeon. We also reviewed the records of 201 patients who received primary radiation therapy without axillary surgery. During this time period, patients typically were irradiated by a 3-field plan which included 4600 rad in 5 weeks to the axilla and supraclavicular regions. Only 6 patients received tangential fields to the breast alone. The incidence of arm edema was as follows: Type of Axillary Surgery No Axillary Surgery Axillary Surgery (All) # Patients 201 105 6 Year Actuarial Risk of Arm Edema 4% 16% p=o. 007 Lower Sampling Lower Dissection Full Dissection 47 8% 37 8% 11 78% p=o. 001 The median number of nodes obtained for pathologic review was 4 for lower axillary sampling (range l-14)) 9 for lower axillary dissection (l-35), and 12 for full axillary dissection (3-18). The likelihood of detecting path- ologically positive nodes in patients with clinically negative nodes was 7/29 (24%) for lower axillary sampling, 6/29 (21%) for lower axillary dissection and 2/9 (22%) for a full axillary dissection. These results stress the need to coordinate the extent of the surgery and radiation therapy in the treatment of the axilla. Patients who undergo a full axillary dissection and have axillary irradiation have a high risk of symptomatic arm edema. At the present time, we are unable to determine the risk of arm edema in patients with full axillary dissection who do not receive axillary irradiation. The use of a lower axillary sampling or dissection however, appears to be an effective means of detecting occult axillary metastases and is not associated with a significant risk of arm edema. 4 TEE RESULTS OF RADIATION THERAPY FOR LOCALLY RECURRENT. BREAST CARCINOMA AFTER MASTECTOMY ilillism J. Aherlzk *, Srirbsr? Silver, Samuel Hellman, Jay R, HiarrIs Joint Center for Rsdlsticn Therapy, iisrvsrd Hedlcsl School. * Current sddress- Hartford. Yospitsl, :!iertford, Connecticut. The role of redistlon therapy In the treatment of local-resionsl recurrence of breast carcinoma Is controversial. In order to determine factors Influencing local control and the effect of local control on distant metastasis we analyzed the records of 90 petlents with biopsy-proven local recurrence without evidence of dIs- tent nstastqsis trested between 1968 and 1978. Patients were typically treated to the chest well end adjoining lymph node areas to a dose of 4600 red In 5 weeks. In mary cases a boost to a-pas of residual gross disease was used. median follow- up was 39 months. GIghty seven of the ninety treated patlents (97%) obtained InItlal complete cllnlcal rsqessIon(CCR). Forty eight of the 87 patIents(555) who obtained CCR had no subsequent evidence of local failure. The actuarial probability of local con- trol, censored for prior distant relapse, W%S 39% at 5 years and 32% st 10 years. Pstierts undergoing excisions1 biopsy prior to redlatlon therspy had sn Improved 5 year probability of local tumor control compsred to patients with less than sx- c1sIor~l biopsy (53% vs. 307) but this difference was not statistically significant (P=O.lO). XIthIn the range of doses used here, we could not demonstrate a dose- response effect for local control but the number of patients who received high doses was small. The actuarial risk of distant metastssIs(DM) WRS 70% at five years and 93% at 10 years. The risk of DH did no% sppesr to be Influenced by whether or not persistent local control was obtained. The overall survival rate was 48% st 5 years and 26% at 10 years. Five year NED survival was 15% and 10 year NED survival was 8%.
-
Upload
david-larson -
Category
Documents
-
view
213 -
download
1
Transcript of Arm edema is influenced by the extent of axillary surgery in patients treated with primary XRT

78 Radiation Oncology ??Biology ??Physics October 1984, Volume 10, Sup. 2
3 m EDaN 1s EWLU’iNCED BY THE EXTENT OF AXILLARY SURGERY IN PATIENTS 'TREATED WITH PRIMARY XRT
David Larson f Mark Weinstein! Itzhak Goldberg? Jay Harris1
1Joint Center for Radiation Therapy, 2 Beth Israel Hospital, Department of Surgery
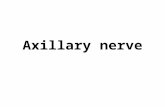
Arm edema is one of the most trying complications of primary treatment for carcinoma of the breast. It is bothersome to patients both functionally and cosmetically, and is poorly treated by currently available techniques. In order to determine treatment factors associated with the development of arm edema, we reviewed the records of 105 patients treated by axillary surgery and primary radiation therapy between July 1968 and December 1979 for whom adequate surgical records were available. Median follow-up was 63 months (39-161 mos.) . Of these 105 patients, 47 had a lower axillary sampling (removal of a portion of the lower axillary contents without formal bourdaries, varying from a simple node biopsy to excision of the axillary fat pad), 37 had a iower axillary dissection (removal of the lower axillary contents with formal boundaries: latissimus dorsi, tail of the breast, axillary vein, pectoralis major) and 11 had full axillary dissection (removal of entire axillary contents with stripping of the axillary vein). In 10 patients, the type of axillary dissection could not be easily classified into one of these 3 groups. The extent of surgery was left to the discretion of the individual surgeon. We also reviewed the records of 201 patients who received primary radiation therapy without axillary surgery. During this time period, patients typically were irradiated by a 3-field plan which included 4600 rad in 5 weeks to the axilla and supraclavicular regions. Only 6 patients received tangential fields to the breast alone. The incidence of arm edema was as follows:
Type of Axillary Surgery
No Axillary Surgery Axillary Surgery (All)
# Patients
201 105
6 Year Actuarial Risk of Arm Edema
4% 16% p=o. 007
Lower Sampling Lower Dissection Full Dissection
47 8% 37 8% 11 78% p=o. 001
The median number of nodes obtained for pathologic review was 4 for lower axillary sampling (range l-14)) 9 for lower axillary dissection (l-35), and 12 for full axillary dissection (3-18). The likelihood of detecting path- ologically positive nodes in patients with clinically negative nodes was 7/29 (24%) for lower axillary sampling, 6/29 (21%) for lower axillary dissection and 2/9 (22%) for a full axillary dissection.
These results stress the need to coordinate the extent of the surgery and radiation therapy in the treatment of the axilla. Patients who undergo a full axillary dissection and have axillary irradiation have a high risk of symptomatic arm edema. At the present time, we are unable to determine the risk of arm edema in patients with full axillary dissection who do not receive axillary irradiation. The use of a lower axillary sampling or dissection however, appears to be an effective means of detecting occult axillary metastases and is not associated with a significant risk of arm edema.
4 TEE RESULTS OF RADIATION THERAPY FOR LOCALLY RECURRENT. BREAST CARCINOMA AFTER MASTECTOMY
ilillism J. Aherlzk *, Srirbsr? Silver, Samuel Hellman, Jay R, HiarrIs
Joint Center for Rsdlsticn Therapy, iisrvsrd Hedlcsl School. * Current sddress- Hartford. Yospitsl, :!iertford, Connecticut.
The role of redistlon therapy In the treatment of local-resionsl recurrence of breast carcinoma Is controversial. In order to determine factors Influencing local control and the effect of local control on distant metastasis we analyzed the records of 90 petlents with biopsy-proven local recurrence without evidence of dIs- tent nstastqsis trested between 1968 and 1978. Patients were typically treated to the chest well end adjoining lymph node areas to a dose of 4600 red In 5 weeks. In mary cases a boost to a-pas of residual gross disease was used. median follow- up was 39 months.
GIghty seven of the ninety treated patlents (97%) obtained InItlal complete cllnlcal rsqessIon(CCR). Forty eight of the 87 patIents(555) who obtained CCR had no subsequent evidence of local failure. The actuarial probability of local con- trol, censored for prior distant relapse, W%S 39% at 5 years and 32% st 10 years. Pstierts undergoing excisions1 biopsy prior to redlatlon therspy had sn Improved 5 year probability of local tumor control compsred to patients with less than sx- c1sIor~l biopsy (53% vs. 307) but this difference was not statistically significant (P=O.lO). XIthIn the range of doses used here, we could not demonstrate a dose- response effect for local control but the number of patients who received high doses was small.
The actuarial risk of distant metastssIs(DM) WRS 70% at five years and 93% at 10 years. The risk of DH did no% sppesr to be Influenced by whether or not persistent local control was obtained. The overall survival rate was 48% st 5 years and 26% at 10 years. Five year NED survival was 15% and 10 year NED survival was 8%.