
Arizona Department of Health Services/Division of Behavioral Health Services Challenges and...
26
Arizona Department of Health Services/Division of Behavioral Health Services Challenges and Innovation in Integrating Care Robert J. Sorce Assistant Director Arizona Department of Health Services Division of Behavioral Services June 29, 2011
-
Upload
debra-stevenson -
Category
Documents
-
view
213 -
download
0
Transcript of Arizona Department of Health Services/Division of Behavioral Health Services Challenges and...
Arizona Department of Health Services/Division of Behavioral Health
Services
Challenges and Innovation in Integrating Care
Robert J. SorceAssistant Director
Arizona Department of Health ServicesDivision of Behavioral Services
June 29, 2011

Arizona’s Publically Funded Health Care System
• Arizona Health Care Cost Containment System (AHCCCS)
• Arizona Department of Health Services/Division of Behavioral Health (ADHS/DBHS)
• AHCCCS/Arizona Long Term Care System (ALTCS)• Community Health Centers(CHC),
– Federally Qualified Community Health Centers (FQHC)
– Rural Health Clinics (RHC)

AHCCCS
• State Medicaid Agency• Established in 1981 under Section 1115 demonstration
waiver• Oversees contracts with ten managed care health plans
for the delivery of acute care services to Medicaid eligible members
• Reimbursement through capitated payments on a per member/per month basis
• As of June 2011, served approximately 1,200,000 members

ALTCS• Administered by AHCCCS to provide long term
care services to elderly and disabled Medicaid eligible members
• Oversees managed care contracts with nine program contractors
• Contractors provides full array of acute care and behavioral health care services
• Home and community based services keep members out of institutions
CHC
• FQHCs and RHCs provide primary health care to the indigent regardless of ability to pay
• Offer acute, behavioral and dental primary care services
• 16 sites throughout the state• Reimbursed by AHCCCS, federal grants (HRSA)
and self-pay

ADHS/DBHS• “Carve Out” to provide behavioral health
services to Medicaid eligible members• No direct service delivery except for Arizona
State Hospital• Oversees contracts with managed care
organizations, Regional Behavioral Health Authorities and American Indian tribes to deliver services (RBHA)

ADHS/DBHS Contracts
• State is divided into six geographic service areas (GSAs)
• Four RBHAs serve the six GSAs• Contracts are bid on a 3-5 year
competitive cycle • Five Tribal Contractors

ADHS/DBHS FundingFiscal Year 2010
Fund Source Percent
Title XIX 87%
TXXI 1%
Other Federal Funds 3%
Non-Title XIX General Funds 6%
County Funds 3%
Total Funding $1,403,355,525
100%
*Funding information, 2008 Annual Report
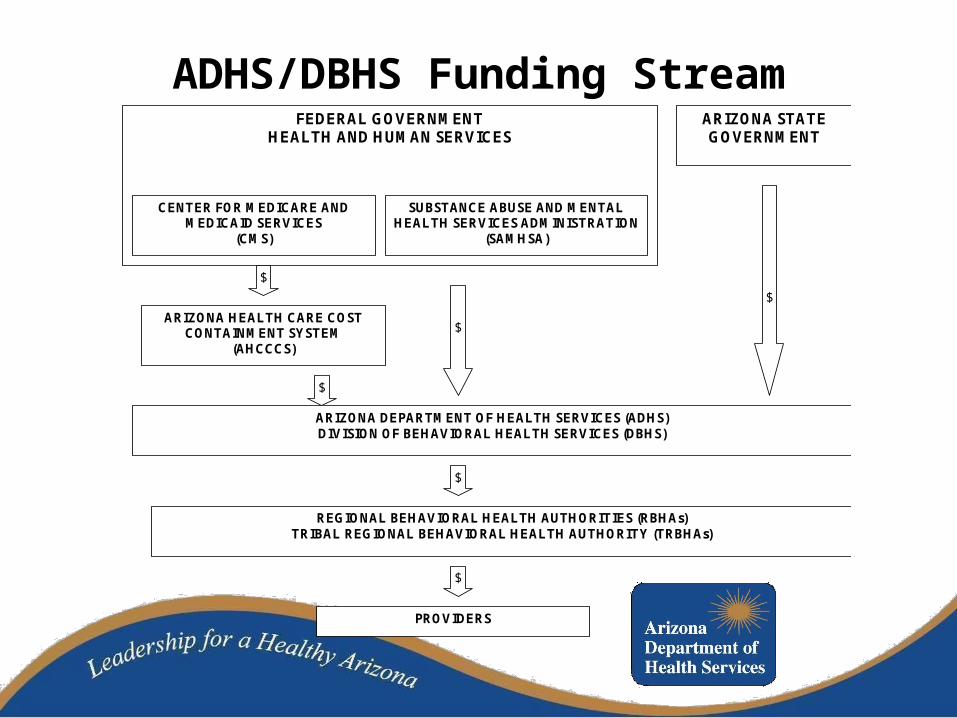
ADHS/DBHS Funding StreamSTATE OF ARIZONA BEHAVIORAL HEALTH FUNDING STREAM
FEDERAL GOVERNMENT
HEALTH AND HUMAN SERVICES ARIZONA STATE GOVERNMENT
ARIZONA DEPARTMENT OF HEALTH SERVICES (ADHS) DIVISION OF BEHAVIORAL HEALTH SERVICES (DBHS)
ARIZONA HEALTH CARE COST CONTAINMENT SYSTEM
(AHCCCS)
REGIONAL BEHAVIORAL HEALTH AUTHORITIES (RBHAs) TRIBAL REGIONAL BEHAVIORAL HEALTH AUTHORITY (TRBHAs)
PROVIDERS
SUBSTANCE ABUSE AND MENTAL HEALTH SERVICES ADMINISTRATION
(SAMHSA)
CENTER FOR MEDICARE AND MEDICAID SERVICES
(CMS)
$
$
$
$
$
$

ADHS/DBHS Populations
• Adults with Serious Mental Illness (SMI)
• Adults with General Mental Health/Substance Abuse Disorders (GMH/SA)
• Children

Populations…January 2011
Populations Title XIX/XXI
Non-Title XIX/XXI
Total
Children 40,737 3,757 44,494
GMH/SA Adult
54,996 11,265 66,261
SMI Adult 23,772 11,487 35,259
Total 119,505 26,509 146,014

ADHS/DBHS Services• Inpatient, medication, medication management,
residential
• Support: case management, counseling, transportation,
• Home and Community Based Services: living skills, housing support, personal care
• Recovery: vocational, housing, peer support
• Crisis: statewide coverage, includes crisis phones, warm lines, mobile teams, inpatient psychiatric and detoxification facilities; operate 24/7, serves general public

Why Health Care Integration?• Federal Health Care Reform• Better outcomes; persons with SMI in Arizona die 25 to
30 years earlier than general population• Control costs; 60 percent of Medicaid’s highest cost
beneficiaries with disabilities have co-occurring physical and behavioral health conditions
• Focus on screening, prevention, early intervention, care management, patient education, wellness
• Current system is unsustainable• Use of technology

First Steps in Planning for Integrated Care
• Met with stakeholders that practice integrated care
• Identified key system partners• Developed structure to drive change• Obtained funding for planning; Section 2703
Planning Grant• Obtained support and commitment from
Executive; key decisions made to move forward

Met With Stakeholders
• CHCs, FQHCs—have been doing integrated care for decades
• RBHA/Health Plan partnerships
• Other states

Identified System Partners
• AHCCCS
• ADHS/DBHS
• RBHAs
• Health Plans
• Providers
• Members and Family members

Structure for Change; Planning Grant
• Formed Health Home Development Steering Committee:– AHCCCS and ADHS/DBHS are co-leads– Obtained Section 2703 Planning Grant to
develop health home for the SMI in Maricopa County
– Hired consultant to conduct data analysis– Specialty Health Plan for Maricopa County
SMI to begin October 1, 2013
Elements for Specialty Plan/Health Home
• Fully integrated at administrative and service delivery level; no “carve out”
• Multidisciplinary team delivers acute and behavioral health services in a dedicated facility or as a virtual team
• Outcomes measured as a team; not individually• Evidenced based practice for screening, prevention,
wellness, care management, disease management and Recovery programs
• Coordinate care through technology and information sharing systems

Steering Committee-Next Steps• Consultant—Data analysis
– Acute care, behavioral health care, Medicare data; utilization; profiling; co-morbid conditions; poly-pharmacy
• Stakeholder input– Members and family members– Providers– Managed care organizations– System partners
• Defining services and outcomes

Steering Committee-Next Steps
• Deciding requirements for health homes
• Guidance from CMS
• Consultation with SAMHSA
• State Plan amendment for Health Homes
• Staffing, work plan, project management
• Request for Information
• Request for Proposal; drafting

Challenges• Communication; transparency; messaging; buy-
in and support• Budget cuts; significant cutbacks in Medicaid• EHR/EMR/HIE; technology; sharing of data• Preserving Recovery in the health home model• Workforce development; training• Costs; billing codes; reimbursement• Confidentiality; HIPAA; substance abuse
regulations

More Challenges…• Opt in/out; member choice
• Oversight and administering multiple systems; staffing shortages
• Licensing; credentialing; privileging
• Provider network development
• Lawsuits; past, present and future

Still More Challenges…
• Staying true to mission, vision and values…avoiding “scope creep”
• Meeting the timeline
• Peer and Family voice and participation in program design
• Anticipating and planning for the unexpected


Questions???
ADHS/DBHS Website: http://www.azdhs.gov/bhs
AHCCCS Website: http://www.azahcccs.gov

Contact information
Robert J. SorceAssistant Director
Arizona Department of Health ServicesDivision of Behavioral Services
150 North 18th Avenue, Suite 200Phoenix, AZ 85007
(602) 364-4628 - office(602) 364-4570 - fax


















