
AREA BOARD REGULAR MEETING Thursday, June 01, 2017 · AREA BOARD REGULAR MEETING 4600 Emperor...
254
Thursday, June 01, 2017 AREA BOARD REGULAR MEETING 4600 Emperor Boulevard, Durham, NC, 27703 4:00-6:00 p.m. Page 1 of 6 MEMBERS PRESENT: ☒Cynthia Binanay, Vice-Chair, ☐Michael Boose, ☒Christopher Bostock, Chair, ☒Heidi Carter, ☒George Corvin, MD, ☒James Edgerton, ☒Greg Ford, ☒Lodies Gloston (arrived at 4:15 pm), ☒Phillip Golden (via phone), ☐John Griffin, Ed.D, ☒Curtis Massey (via phone), ☐George Quick, ☒William Stanford, Jr., ☒Amelia Thorpe, ☒Lascel Webley, Jr., and ☒McKinley Wooten, Jr. GUEST(S) PRESENT: Gary Bass, CEO of Pride of NC; Carrie Bradstock, CFAC Chair (via phone); Jess Brandes, Housing Developer with CASA; Denise Foreman, Wake County Manager’s office; Mary Hutchings, Wake County Finance Department; Debra King, CEO of CASA; Candace Mondragon, A Small Miracle, LLC; Brian Perkins, Government and Strategic Relations Advisor to Alliance; and Debbie White, CFO of CASA ALLIANCE STAFF PRESENT: Damali Alston, Director of Network Evaluation; Michael Bollini, Executive Vice-President/Chief Operating Officer; Margaret Brunson, Hospital Relations Director; Courtney Cantrell, Senior Vice-President/Clinical Operations; Joey Dorsett, Senior Vice-President/Chief Information Officer; Cheala Garland-Downey, Director of Human Relations; Kelly Goodfellow, Executive Vice-President/Chief Financial Officer; Amanda Graham, Senior Vice-President/Organizational Development; Veronica Ingram, Executive Assistant; Carlyle Johnson, Director of Provider Network Strategy & Initiatives; Wes Knepper, Director of Quality Management; Susan Knox, Senior Human Relations Business Partner; Beth Melcher, Executive Vice-President/Clinical Operations (interim); Joy Montemorano, Administrative Assistant; Ann Oshel, Senior Vice-President/Community Relations; Sara Pacholke, Senior Vice-President/Financial Operations; Monica Portugal, Chief Compliance Officer; Robert Robinson, Chief Executive Officer; Matthew Ruppel, Director of Program Integrity; and Sara Wilson, Director of Government Relations 1. CALL TO ORDER: Chairman Christopher Bostock called the meeting to order at 4:03 p.m. AGENDA ITEMS: DISCUSSION: 2. Oath of Office Chairman Bostock introduced new Board member and Wake County Commissioner, Greg Ford. Commissioner Ford received the oath of office at the June 1, 2017, Finance Committee meeting. 3. Announcements A. Special June Board Meeting: Chairman Bostock mentioned that a pending June Board meeting is still scheduled. It will be confirmed soon. Ms. Ingram will send an email reminder to Board members. B. Leadership Training: Ms. Graham mentioned one of the initiatives of her department is a year-long leadership program for staff. She provided a brief overview of the training and noted how it relates to the organization’s strategic plan. C. Resume/CVs: Mr. Robinson asked Board members to forward updated resume/CVs to Ms. Ingram. D. Board Surveys: Dr. Corvin mentioned that the majority of the Board surveys have been completed and requested the completion of remaining surveys. 4. Agenda Adjustments Chairman Bostock requested to move item 7F: Annual HR Classification and Compensation to item 13.B. BOARD ACTION A motion made by Dr. Corvin to move the item 7F: Annual HR Classification and Compensation to the updates section; motion seconded by Vice-Chair Binanay. Motion passed unanimously.
Transcript of AREA BOARD REGULAR MEETING Thursday, June 01, 2017 · AREA BOARD REGULAR MEETING 4600 Emperor...

Thursday, June 01, 2017 AREA BOARD REGULAR MEETING 4600 Emperor Boulevard, Durham, NC, 27703 4:00-6:00 p.m.
Page 1 of 6
MEMBERS PRESENT: ☒Cynthia Binanay, Vice-Chair, ☐Michael Boose, ☒Christopher Bostock, Chair, ☒Heidi Carter, ☒George Corvin, MD, ☒James Edgerton, ☒Greg Ford, ☒Lodies Gloston (arrived at 4:15 pm), ☒Phillip Golden (via phone), ☐John Griffin, Ed.D, ☒Curtis Massey (via phone), ☐George Quick, ☒William Stanford, Jr., ☒Amelia Thorpe, ☒Lascel Webley, Jr., and ☒McKinley Wooten, Jr.
GUEST(S) PRESENT: Gary Bass, CEO of Pride of NC; Carrie Bradstock, CFAC Chair (via phone); Jess Brandes, Housing Developer with CASA; Denise Foreman, Wake County Manager’s office; Mary Hutchings, Wake County Finance Department; Debra King, CEO of CASA; Candace Mondragon, A Small Miracle, LLC; Brian Perkins, Government and Strategic Relations Advisor to Alliance; and Debbie White, CFO of CASA ALLIANCE STAFF PRESENT: Damali Alston, Director of Network Evaluation; Michael Bollini, Executive Vice-President/Chief Operating Officer; Margaret Brunson, Hospital Relations Director; Courtney Cantrell, Senior Vice-President/Clinical Operations; Joey Dorsett, Senior Vice-President/Chief Information Officer; Cheala Garland-Downey, Director of Human Relations; Kelly Goodfellow, Executive Vice-President/Chief Financial Officer; Amanda Graham, Senior Vice-President/Organizational Development; Veronica Ingram, Executive Assistant; Carlyle Johnson, Director of Provider Network Strategy & Initiatives; Wes Knepper, Director of Quality Management; Susan Knox, Senior Human Relations Business Partner; Beth Melcher, Executive Vice-President/Clinical Operations (interim); Joy Montemorano, Administrative Assistant; Ann Oshel, Senior Vice-President/Community Relations; Sara Pacholke, Senior Vice-President/Financial Operations; Monica Portugal, Chief Compliance Officer; Robert Robinson, Chief Executive Officer; Matthew Ruppel, Director of Program Integrity; and Sara Wilson, Director of Government Relations 1. CALL TO ORDER: Chairman Christopher Bostock called the meeting to order at 4:03 p.m.
AGENDA ITEMS: DISCUSSION: 2. Oath of Office Chairman Bostock introduced new Board member and Wake County Commissioner, Greg Ford. Commissioner Ford received the
oath of office at the June 1, 2017, Finance Committee meeting. 3. Announcements A. Special June Board Meeting: Chairman Bostock mentioned that a pending June Board meeting is still scheduled. It will be
confirmed soon. Ms. Ingram will send an email reminder to Board members. B. Leadership Training: Ms. Graham mentioned one of the initiatives of her department is a year-long leadership program for
staff. She provided a brief overview of the training and noted how it relates to the organization’s strategic plan. C. Resume/CVs: Mr. Robinson asked Board members to forward updated resume/CVs to Ms. Ingram. D. Board Surveys: Dr. Corvin mentioned that the majority of the Board surveys have been completed and requested the
completion of remaining surveys. 4. Agenda
Adjustments Chairman Bostock requested to move item 7F: Annual HR Classification and Compensation to item 13.B. BOARD ACTION A motion made by Dr. Corvin to move the item 7F: Annual HR Classification and Compensation to the updates section; motion seconded by Vice-Chair Binanay. Motion passed unanimously.

Thursday, June 01, 2017 AREA BOARD REGULAR MEETING 4600 Emperor Boulevard, Durham, NC, 27703 4:00-6:00 p.m.
Page 2 of 6
AGENDA ITEMS: DISCUSSION: 5. Public Comment Gary Bass, CEO of Pride NC, provided public comments. He expressed appreciation for Alliance’s support and provided an update
on his agency. 6. Committee
Reports A. Consumer and Family Advisory Committee – page 7 The Alliance Consumer and Family Advisory Committee (CFAC) is composed of consumers and/or family members from Durham, Wake, or Cumberland Counties who receive mental health, intellectual/developmental disabilities or substance use/addiction services. This month’s report included draft minutes from the Cumberland, Durham, and Wake meetings. Caroline Bradstock, CFAC Chair, presented the report. Ms. Bradstock mentioned a nomination committee for the next CFAC officers, pending advocacy opportunities, and provided an update from recent CFAC meetings. The CFAC report is attached to and made part of these minutes. B. Finance Committee – page 37 The Finance Committee’s function is to review financial statements and recommend policies/practices on fiscal matters to the Area Board. This month’s report included draft minutes from the May meeting. James Edgerton, Committee Chair, presented the report. Mr. Edgerton mentioned that revenues exceeded expenditures and all State mandated ratios were met or exceeded. He mentioned a pending budget amendment. Ms. Goodfellow mentioned this is an annual process due to retroactive Medicaid payments and a legislative reduction of funds. BOARD ACTION A motion was made by Mr. James Edgerton to amend the FY16 budget by $4,300,000; seconded by Mr. McKinley Wooten. Motion passed unanimously. C. Policy Committee – page 43 Per Alliance Behavioral Healthcare Area Board Policy “Development of Policies and Procedures”, the Board reviews all policies annually. The Policy Committee reviews a number of policies each quarter in order to meet this requirement. This month’s report included minutes from the May meeting. Mr. Massey provided an update from the Policy Committee. He mentioned the following policies were reviewed and recommended for approval without revisions: Equal Employment Opportunity/Affirmative Action, Recruitment and Selection, Conditions of Employment, Classification and Compensation, Employee Benefits, Alcohol and Drug Free Workplace, Employee Time and Attendance, Sexual Harassment, Leave Policy, Family and Medical Leave Act, Clinical Staff Credentialing, Disciplinary Action, Performance Management, Separation, Employee Complaint, Employee Grievance, and Reduction-in-Force. Mr. Massey reviewed recommended changes for the following policies: Management and Investigation of Grievances and

Thursday, June 01, 2017 AREA BOARD REGULAR MEETING 4600 Emperor Boulevard, Durham, NC, 27703 4:00-6:00 p.m.
Page 3 of 6
AGENDA ITEMS: DISCUSSION: Fund Balance. Mr. Massey also reviewed a proposed new policy: Budget Transfers. The Board discussed approving the new policy or postponing approval for a later date. BOARD ACTION A motion was made by Dr. George Corvin to approve the recommended policies and adopt the new policies; motion seconded by Ms. Lodies Gloston. Motion passed unanimously.
7. Consent Agenda A. Draft Minutes from May Board Meeting – page 76 B. Audit and Compliance Committee Report – page 81 C. Executive Committee Report- page 101 D. Network Development and Services Committee Report – page 104 E. Quality Management Committee Report – page 133 The consent agenda was sent as part of the Board packet. There were no comments or discussion about the consent agenda. BOARD ACTION A motion was made by Mr. McKinley Wooten to approve the consent agenda; motion seconded by Ms. Lodies Gloston. Motion passed unanimously.
8. FY18 Budget – page 202
Chairman Bostock mentioned that as required by GS 159-12 (b), the Board shall hold a public hearing before adopting the budget ordinance for the fiscal year. The Board held a public hearing on the FY18 budget. There were no comments; the public hearing closed. Kelly Goodfellow, Executive Vice-President/Chief Financial Officer, provided a presentation on the FY18 budget. Board members discussed potential changes for those who are under served and the potential impact on persons with Medicaid. The FY18 budget presentation is attached to and made part of these minutes. BOARD ACTION A motion was made by Mr. McKinley Wooten to approve the FY18 budget; motion seconded by Mr. Lascel Webley. Motion passed unanimously. A motion was made by Mr. McKinley Wooten to approve the FY18 reinvestment plan; motion seconded by Mr. Lascel Webley. Motion passed unanimously.
9. Supportive Housing Proposal – page 244
Alliance has been given the opportunity to partner with CASA, a local developer, and invest $250,000 in thirteen one-bedroom units within the Durham City limits. This investment will allow exclusive access to nearly 20% of the units for persons Alliance serves (in accordance with the Olmstead settlement). The investment will go towards rehab of the existing property.

Thursday, June 01, 2017 AREA BOARD REGULAR MEETING 4600 Emperor Boulevard, Durham, NC, 27703 4:00-6:00 p.m.
Page 4 of 6
AGENDA ITEMS: DISCUSSION: Ann Oshel, Senior Vice-President/Community Relations, presented the proposal. She mentioned that this is part of a regional housing plan that is required annually by the State. She provided background related to supportive housing. Debra King, CEO of CASA, provided background on CASA.
Chairman Bostock mentioned that the Executive Committee reviewed the proposal and recommends its approval. Board members discussed the proposal. BOARD ACTION A motion was made by Mr. William Stanford to approve the $250,000.00 investment with CASA for thirteen TCLI supportive housing units restricted by deed restrictions or covenants for fifteen years for Maplewood and Underwood Avenues in Durham; motion seconded by Mr. Lascel Webley. Motion passed unanimously.
10. Proposal to Cancel July 6, 2017, Board Meeting – page 245
As stated in Article III Sections A and D of the Board By-Laws, regular meetings of the Area Board shall be held at least six times each year at a location and time designated by the Area Board. The matter is placed before the Board for a vote on whether the Board would like to cancel the July regularly scheduled meeting. If canceled, the proper notice shall be published per Open Meetings Law requirements. Chairman Bostock mentioned if a crucial topic occurs before the August Board meeting, the topic could be addressed at the June or July Executive Committee meeting. There were no additional discussion or questions about this agenda item. BOARD ACTION A motion was made by Mr. Lascel Webley to cancel the July 6, 2017, Board meeting; motion seconded by Dr. George Corvin. Motion passed unanimously.
11. Election of FY18 Board Officers – page 246
As stated in the by-laws officers of the Area Board shall be chosen for a one-year term at the final meeting of the fiscal year and shall be as follows: Chairperson and Vice-Chairperson. Officers shall serve for no more than two consecutive terms. Each Area Board member shall be eligible to serve as an officer. Nominations for Chairperson were opened. BOARD ACTION A motion was made by Mr. Curtis Massey to nominate Cynthia Binanay as FY18 Board Chairperson; motioned seconded by Mr. William Stanford. Motion passed unanimously. A motion was made by Mr. McKinley Wooten to close the nominations for Board Chairperson; motion seconded by Mr. William Stanford. Motion passed unanimously. By unanimous show of hands or verbal consent the Board elected Cynthia Binanay as FY18 Board Chairperson.

Thursday, June 01, 2017 AREA BOARD REGULAR MEETING 4600 Emperor Boulevard, Durham, NC, 27703 4:00-6:00 p.m.
Page 5 of 6
AGENDA ITEMS: DISCUSSION: Nominations for Vice-Chairperson were opened. BOARD ACTION A motion was made by Mr. James Edgerton to nominate George Corvin as FY18 Board Vice-Chairperson; motion seconded by Mr. McKinley Wooten. Motion passed unanimously. A motion was made by Ms. Lodies Gloston to close the nominations for Board Vice-Chairperson; motion seconded by Mr. McKinley Wooten. Motion passed unanimously. By unanimous show of hands or verbal consent the Board elected George Corvin as FY18 Board Vice-Chairperson. Chairman Bostock requested that the Policy Committee draft an officer selection policy.
12. Training: Service for Individuals with Complex Needs – page 247
The State has been working with Disability Rights of North Carolina for about two years to address unmet needs in children with both mental illness and developmental disabilities. Alliance has increased focus on these particular children as well. Beth Melcher, Executive Vice-President/Care Management, presented an overview of services for individuals with complex needs. She noted aspects of population health, advanced analytics, social determinants of health, engagement and self-management, expected outcomes, services for persons with complex needs, and next steps. There were no questions or discussion about the training presentation. BOARD ACTION The Board received the training; no additional action required.
13. Updates A. NC Legislation/Single Stream Funding Mr. Perkins provided an overview of recent activity in the NC General Assembly; his report included the House and Senate proposed budget and the proposed funding reduction of single stream funds. Ms. Wilson reviewed the potential impact on Alliance if either proposed budget is approved. Board members requested clarification regarding some of the handouts provided by Mr. Perkins and Ms. Wilson, specifically the details of a graphic for the reinvestment plan. Board members requested including elements of the reinvestment plan in this graphic.
B. Annual HR Classification and Compensation Schedule – page 248 Chairman Bostock reviewed this topic and the annual process to approve this classification and compensation schedule; he clarified that this is different from the CEO salary study. Board members discussed this topic and noted that any changes do not necessarily alter staff salaries.
Thursday, June 01, 2017 AREA BOARD REGULAR MEETING 4600 Emperor Boulevard, Durham, NC, 27703 4:00-6:00 p.m.
Page 6 of 6
AGENDA ITEMS: DISCUSSION:
BOARD ACTION A motion was made by Dr. George Corvin to approve the annual HR classification and compensation plan with the addition of the newly defined range for the Area Director/CEO; motion seconded by Mr. Lascel Webley. Motion carried unanimously.
14. Chairman’s Report
There was no report.
15. Closed Sessions BOARD ACTION A motion was made by Mr. William Stanford to enter closed session pursuant to NCGS 143-318.11 (a) (6) and NCGS 143-318.11 (1) to consider the qualifications, competence, and performance of an employee and to prevent the disclosure of information that is confidential and not a public record under NCGS 122C-126.1; motion seconded by Ms. Lodies Gloston. Motion passed unanimously. The Board returned to open session.
16. Adjournment With all business being completed the meeting adjourned at 7:33 p.m.
Next Board Meeting Thursday, August 03, 2017
4:00 – 6:00 8/3/17 Robert Robinson, Chief Executive Officer Date Approved

(Back to agenda)
ITEM: Consumer and Family Advisory Committee (CFAC) Report DATE OF BOARD MEETING: June 1, 2017 BACKGROUND: The Alliance Consumer and Family Advisory Committee, or CFAC, is made up of consumers and/or family members that live in Durham, Wake, or Cumberland Counties who receive mental health, intellectual/developmental disabilities and substance use/addiction services. CFAC is a self-governing committee that serves as an advisor to Alliance administration and Board of Directors. State statutes charge CFAC with the following responsibilities: Review, comment on and monitor the implementation of the local business plan Identify service gaps and underserved populations Make recommendations regarding the service array and monitor the development of additional
services Review and comment on the Alliance budget Participate in all quality improvement measures and performance indicators Submit findings and recommendations to the State Consumer and Family Advisory Committee
regarding ways to improve the delivery of mental health, intellectual/other developmental disabilities and substance use/addiction services.
The Alliance CFAC meets at 5:30pm on the first Monday in the months of February, April, June, August, October and December at the Alliance Corporate Office, 4600 Emperor Boulevard, Durham. Sub-committee meetings are held in individual counties, the schedules for those meetings are available on our website. The Alliance CFAC tries to meet its statutory requirements by providing you with the minutes to our meetings, letters to the board, participation on committees, outreach to our communities, providing input to policies effecting consumers, and by providing the Board of Directors and the State CFAC with an Annual Report as agreed upon in our Relational Agreement describing our activities, concerns, and accomplishments. REQUEST FOR AREA BOARD ACTION: Accept draft minutes and supporting documents from the April 27, 2017, Cumberland meeting, May 1, 2017, Durham meeting, and May 9, 2017 Wake meeting. CEO RECOMMENDATION: Accept the report. RESOURCE PERSON(S): Caroline Ambrose, CFAC Chair; Doug Wright, Director of Consumer Affairs
Alliance Behavioral Healthcare BOARD OF DIRECTORS
Agenda Action Form
6A

Thursday, April 27, 2017 CUMBERLAND CFAC SUBCOMMITTEE
Page 1 of 2
MEMBERS PRESENT: Michael McGuire, Lotta Fisher, Dorothy Johnson, Jackie Blue, and Shirley Francis. GUEST(S) PRESENT: Renee Loyd, T. Loyd, Na Headly (Alliance), Laressa Wit (Alliance), Doug Wright (Allaince), Starlett Davis (Alliance), and CJ Lewis (DMH/DD/SAS).
1. WELCOME AND INTRODUCTIONS Doug and Lotta made introductions of the committee to the visiting guest, Renee Loyd and her son T. Loyd. 2. REVIEW OF THE MINUTES - Minutes from March 23, 2017 were reviewed and accepted
AGENDA ITEMS: DISCUSSION: NEXT STEPS: TIME FRAME: Public Comment- Consumer/Family challenges and solutions
Starlett Davis went over handouts given to committee. Refer to deadlines of events and take note of the resources.
Ongoing
State Updates
C. J. Lewis The SWOT analysis was done as a group. Doug and CJ assisted with clarification and questions about the survey. CJ recorded the responses to take back to the State to be assessed.
CJ will follow up. Ongoing
Crisis Counseling Assistance and Training Program
Nathania Headly and Laressa Witt explained the Hope in the NC Program also known as the Crisis Counseling Assistance and Training Program through FEMA. This program is meant to assess the emotional well-being and mental stability of those affected by the hurricane/flood of October 2016.
Information was given out and Ms. Witt asked for anyone who was aware of anyone impacted by the flood to contact her.
Ongoing
MCO Updates
Doug Wright gave updates. Doug sent out an email on a Statewide CFAC meeting on June 1st from 9am-2pm in Statesville, NC. You have to register and let Doug or Star know about it so that we can see who is going and traveling arrangements. Hotels will be considered. Star will send out a reminder. The Consumer Affairs Department are considering changing their name to the Office of Individual and Family Affairs. The
Star will send out a reminder in the following week. Register and contact Doug or Star about the State CFAC conference.
By 5/12/17
As soon as possible

Thursday, April 27, 2017 CUMBERLAND CFAC SUBCOMMITTEE
Page 2 of 2
AGENDA ITEMS: DISCUSSION: NEXT STEPS: TIME FRAME: Consumer Affair Specialist will be called an Individual and Family Engagement Specialist. Rolls will be the same. Looking into a more recovery and individual orientated language.
Membership Discussion Community outreach
Star Davis and Doug Wright discussed the plans for the next meeting in the community. We will have the meeting in Godwin. The meeting place and time were confirmed while in the meeting. We will discuss gaps and needs with the community. They will get the opportunity to submit their questions on note cards for discussion. Doug will be on vacation and Star will provide a small presentation on Alliance. Lotta and Michael will present on CFAC. We will provide water and snacks for the meeting as well. Star will send flyers via email and have some printed out at with the front desk manager for pick up.
Flyers will be emailed the following week and copies left at desk for pick up. Next meeting will be in Godwin.
5/2/17
5/25/17
Prep for the next meeting
Discuss the next meeting agenda items. Go over expectations, reminders, etc for the next meeting. The meeting will be in Godwin. The committee is to pass out flyers and spread the word about the meeting.
Pass out flyers and inform community about meeting.
Until 5/25/17
Appreciation Everyone spoke about what they appreciated. N/A N/A
5. ADJOURNMENT The meeting was adjourned 7:35pm. Next Subcommittee meeting will be May 25, 2017 in Godwin, NC.

Monday, May 01, 2017 DURHAM CFAC SUBCOMMITTEE MEETING
Page 1 of 3
MEMBERS PRESENT: Steve Hill, Tammy Harrington, ☐ Joe Kilsheimer, James Henry, ☐ Latasha Jordan,
Dave Curro, ☐ Amelia Thorpe, ☐ Kyle Reece GUEST(S) PRESENT: C.J. Lewis, Div. MH/IDD/SAS ALLIANCE STAFF: Doug Wright, Director of Consumer Affairs; Yancee Pérez, Consumer Affairs Specialist
Dial-In Number: (605) 472-5464 Access Code: 289674
1. WELCOME AND INTRODUCTIONS 2. REVIEW OF THE MINUTES: No quorum, minutes reviewed with common consensus.
AGENDA ITEMS: DISCUSSION: NEXT STEPS: TIME FRAME: Public Comment No public comment. N/A N/A
Interest in Membership
There have been two guests that have attended CFAC lately from the Durham community that have expressed interest in becoming official members of CFAC. They were not present to discuss potential membership and being presented at the all-county CFAC meeting.
Yancee to reach out to Jessica and Tammy to reach out to Trula to gauge interest in becoming a CFAC member.
June 2017
Local CFAC Questionnaire & SWOT Analysis- CJ
C.J. Lewis from the Division of MH/IDD/SAS shared a questionnaire with the Durham subcommittee members to answer collectively regarding the performance of their statutory requirements. CFAC members discussed amongst the group, and answered each question collectively.
For hard copies of the questionnaire please contact C.J. Lewis at [email protected]
N/A
IDD Resource Fair/NAMI Walk logistics/volunteers
Yancee shared the details regarding the upcoming IDD resource fair to be held at the Alliance HQ. Both Wake and Durham agencies and supports will be in attendance. Yancee shared logistics about the upcoming
Dave Curro volunteered to help staff the CFAC table at the IDD resource fair. There will be Wake CFAC members present as well.

Monday, May 01, 2017 DURHAM CFAC SUBCOMMITTEE MEETING
Page 2 of 3
AGENDA ITEMS: DISCUSSION: NEXT STEPS: TIME FRAME: NAMI walk and confirmed CFAC volunteers to staff the table on May 6th.
Tammy and Dave both volunteered to staff the Alliance CFAC table at the NAMI walk this year.
Nomination Committee Upcoming elections ELT By-laws discussion (meet monthly-CFAC structure)
Yancee and Doug shared further details regarding the nomination committee and the upcoming CFAC elections for the June meeting. Jim Henry agreed to participate on the nominating committee. Steve, Doug, and Yancee shared information regarding the current draft of the new by-laws and how that would change the structure of CFAC to the Durham subcommittee meeting monthly, along with the monthly meeting that takes place at the Alliance HQ office (with the other counties). Durham subcommittee can change to monthly meetings now if they desire to. The consensus was that Durham subcommittee would wait till after the new by-laws were complete before moving to meeting monthly and potentially changing the day of the week/month that they meet on.
Yancee to email Carrie that Jim has volunteered to be on the nominating committee.
May 2017
Next year’s plans
Much discussion was had in regards to future presentations and opportunities for providers from the community to come and share about services and supports offered in the Durham community. Dave shared about a Trauma-Informed presentation he went to and stated that he would like for CFAC to have opportunities to learn content such as this. Yancee shared the potential for an ad-hoc committee to form to further plan the speakers that might be willing to come and share their knowledge with CFAC. CFAC members could
Continue the discussion and make some decisions to move forward. Potentially re-visit the document compiled at the CFAC retreat from Feb. 2017.
Ongoing

Monday, May 01, 2017 DURHAM CFAC SUBCOMMITTEE MEETING
Page 3 of 3
AGENDA ITEMS: DISCUSSION: NEXT STEPS: TIME FRAME: utilize their connections in the community to further plan what they would like to see at upcoming meetings.
May-Mental Health Month
Yancee shared a calendar of events for Durham for the month of May. CFAC members given presentation on mental health awareness to take home, as meeting agenda was full.
Participate if you like. Read over the presentation and offer further insight/edits/feedback.
N/A
Announcements/Opportunities No further announcements. N/A N/A
5. ADJOURNMENT: 7:30 PM

Tuesday, May 09, 2017 WAKE CFAC SUBCOMMITTEE MEETING
Page 1 of 2
MEMBERS PRESENT: GUEST(S) PRESENT:
Dial +1 (224) 501‐3412 Access Code: 437‐924‐685 1. WELCOME AND INTRODUCTIONS 2. REVIEW OF THE MINUTES ‐ Minutes from March were adopted
AGENDA ITEMS: DISCUSSION: NEXT STEPS: TIME FRAME:
Nominations for Upcoming elections Carolina Ambrose
Anyone interested becoming a member of the nominating committee? Caroline Ambrose‐Bradstock and Jim Henry are interested.
Upcoming Bylaws Israel Patterson
There is no additional information or comments except for what Doug put down. Doug explained the idea is to have larger groups for each county. The full CFAC will be more a steering committee and advise the ABH Board Members.
State CFAC CJ Lewis
5/10/2017 Monthly State CFAC at Dix Grill Dorthea Dix 9‐3:00 will be discussing crisis. 5/17 will be state local conference call. DMH hired a new Veterans liaison. NCI plan on releasing it to the public. Medicaid and Health Choice is doing a listening session. Next time we will do the SWOT analysis in July.
MCO Updates‐Doug Wright
Statewide CFAC June 1st 9‐3pm in Statesville. NC Med assist May 25, 11:30‐1 at Raleigh Marriott City Center. Rob requested a CFAC member to go. The office of Consumer Affairs will be changing the name and titles Individual and Family Engagement Specialist. The budget was presented to the Board Members last week. June 1st will have a public hearing and a vote will happen after the public hearing. There is an overall increase of $6 million. The benefit plan will change from county to county to ABH wide. ABH will incorporated a TBI pilot programs with around 40 slots for. The senate budget will come out soon and may cut state funding in our catchment area. IF the senate cuts,
Caroline Bradstock will attend the Med Assist and Doug will inform Rob.

Tuesday, May 09, 2017 WAKE CFAC SUBCOMMITTEE MEETING
Page 2 of 2
AGENDA ITEMS: DISCUSSION: NEXT STEPS: TIME FRAME: there will be a dramatic effect on individuals without Medicaid. There is a Stop Act, unfunded, about the Opioid Epidemic which is a good place to start at the state level.
Public Comments/Concerns Mercedes Vedock told her story and is looking for ways to advocate.
Mental Health Awareness Training Stacy Guse
5. ADJOURNMENT

Mental HealthAwareness
Serving Durham, Wake, Cumberland and Johnston Counties

Understanding Mental Health Challenges
• A medical condition that disrupts a person's thinking, feeling, mood, ability to relate to others and daily functioning
• Affect every aspect of life
• Can affect persons of any age, race, religion or income
• Not the result of personal weakness, lack of character or poor upbringing
Serving Durham, Wake, Cumberland and Johnston Counties

Understanding Mental Health Challenges
• One in four adults in American experiences a mental health disorder in a given year
o One in 17 lives with a serious mental health challenge such as schizophrenia, depression or bipolar disorder
• Half of the adults in America will develop a mental health challenge sometime in their lives
• One in 10 children lives with a serious mental or emotional disorder
Serving Durham, Wake, Cumberland and Johnston Counties
Understanding Mental Health Challenges
• Symptoms of mental health challenges can appear as physical problems, such as abdominal pain, back pain or headache
• A thorough medical workup is important to understanding the cause and diagnosis of mental health challenges
Serving Durham, Wake, Cumberland and Johnston Counties

Serious Mental Health Challenges
• Major depression
o Mood state that goes well beyond temporarily feeling sad or blue
• Schizophrenia/schizo-affective disorder
o Affects 2.4 million American adults
• Bipolar disorder
o Chronic illness with recurring episodes of mania and depression
Serving Durham, Wake, Cumberland and Johnston Counties

Serious Mental Health Challenges
• Obsessive compulsive disorder (OCD)
oObsessions are intrusive, irrational thoughts; unwanted ideas or impulses
• Anxiety/panic disorder
• Posttraumatic stress disorder (PTSD)
o Affects many different people, from survivors of rape and natural disasters to military service men and women
Serving Durham, Wake, Cumberland and Johnston Counties

Serious Mental Health Challenges
• Borderline personality disorder
o Pervasive instability in moods, interpersonal relationships, self-image and behavior
• Attention-deficit hyperactivity disorder (ADHD)
o Characterized by inattention, hyperactivity
and impulsivity
• Dissociative Identity Disorder
Serving Durham, Wake, Cumberland and Johnston Counties

Risk Factors
• Close blood relative with a mental health challenge.
• Mother’s exposure to viruses, toxins, drugs or alcohol during pregnancy
• Stressful life situations, such as financial problems, a loved one's death or a divorce
• Chronic medical condition, such as cancer
• Brain damage as a result of a serious injury
Serving Durham, Wake, Cumberland and Johnston Counties

Risk Factors
• Traumatic experiences, such as military combat or being assaulted
• Use of illegal drugs
• Being abused or neglected as a child
• Lack of friends or healthy relationships
• Having a previous mental health challenge
Serving Durham, Wake, Cumberland and Johnston Counties

Signs and Symptoms
• Feeling sad or down
• Confused thinking or reduced ability to concentrate
• Excessive fears or worries
• Extreme mood changes of highs and lows
• Withdrawal from friends and activities
• Significant tiredness, low energy or problems sleeping
Serving Durham, Wake, Cumberland and Johnston Counties

Signs and Symptoms
• Delusions, paranoia or hallucinations
• Inability to cope with daily problems or stress
• Extreme feelings of guilt
• Alcohol or drug abuse
• Major changes in eating habits
• Sex drive changes
• Excessive anger, hostility or violence
• Suicidal thinking
Serving Durham, Wake, Cumberland and Johnston Counties

Complications of Mental Health Challenges
• Unhappiness and decreased enjoyment of life
• Family conflicts
• Relationship difficulties
• Social isolation
• Problems with tobacco, alcohol and other drugs
• Problems at work or school
• Poverty and homelessness
Serving Durham, Wake, Cumberland and Johnston Counties

Complications of Mental health Challenges
• Self-harm and harm to others, including suicide or homicide
• Increased risk of motor vehicle accidents
• Weakened immune system
• Heart disease and other medical conditions
Serving Durham, Wake, Cumberland and Johnston Counties

Recovery from Mental Health Challenges
• As people become familiar with their illness they recognize their own patterns of behavior
• A holistic process that involves a variety of perspectives
• Recovery journey is unique for each individual
• A process, not an event
• Requires community support and continuity of care
Serving Durham, Wake, Cumberland and Johnston Counties

Recovery from Mental Health Challenges
• Seek effective and timely care
o Because mental health challenges have no cure, treatment may need to be continuous
• Treatment extends beyond medication
o Includes attaining and maintaining physical health
• Individuals with a mental health challenges benefit tremendously from taking responsibility for their own recovery
Serving Durham, Wake, Cumberland and Johnston Counties

Treatment of Mental Health Challenges
• Medications available to help with challenges including psychosis, depression and anxiety
o Usually effective but side effects should be
monitored and minimized
• Treatment program should also include other essential components such as:
o Psychotherapy
o Support groups
o Patient understanding of the challenge
Serving Durham, Wake, Cumberland and Johnston Counties

What Can You Do?
• If you have any signs or symptoms of a mental health challenge, see your doctor, mental health provider or other health professional
• If your loved one shows signs of a mental health challenge, have an open and honest discussion with him or her about your concerns
Serving Durham, Wake, Cumberland and Johnston Counties

The Treatment Team
• Family or primary care doctor
• Psychiatrist
• Psychotherapist, such as a psychologist or a licensed counselor
• Pharmacist
• Social worker
• Family members/Peers
Serving Durham, Wake, Cumberland and Johnston Counties

Questions for the Healthcare Team
• What mental health challenge might I have?
• Why can't I get over it on my own?
• How do you treat my mental health challenge?
• Will counseling or psychotherapy help?
• Are there medications that might help?
• How long will treatment take?
• What can I do to help myself?
Serving Durham, Wake, Cumberland and Johnston Counties

Questions for the Healthcare Team
• Do you have any brochures or other printed material that I can have?
• What websites do you recommend?
Serving Durham, Wake, Cumberland and Johnston Counties

Dealing with Suicidal Thoughts
• Call 911 or your local emergency number
• Call a suicide hotline number, such as 800-273-TALK, to reach a trained counselor
• Reach out to a close friend or loved one or a minister or someone in your faith community
• Contact your doctor, other health care provider or mental health specialist
Serving Durham, Wake, Cumberland and Johnston Counties

Living Well with Mental Health Challenges
• Stick to your treatment plan
• Avoid alcohol and drug use
• Stay active
• Don't make important decisions when your symptoms are severe
• Prioritize your life
• Learn to adopt a positive attitude
Serving Durham, Wake, Cumberland and Johnston Counties
(Back to agenda)
ITEM: Finance Committee Report DATE OF BOARD MEETING: June 1, 2017 BACKGROUND: The Finance Committee’s function is to review financial statements and recommend policies/practices on fiscal matters to the Area Board. The Finance Committee meets monthly at 3:00 p.m. prior to the regular Area Board Meeting. REQUEST FOR AREA BOARD ACTION: Accept the report. CEO RECOMMENDATION: Accept the report. RESOURCE PERSON(S): James Edgerton, Committee Chair; Robert Robinson, CEO; Kelly Goodfellow, Executive Vice-President/CFO
Alliance Behavioral Healthcare BOARD OF DIRECTORS
Agenda Action Form
6B
Thursday, May 04, 2017 BOARD FINANCE COMMITTEE
Draft minutes may be submitted with the monthly Board packet. Minutes will be approved by this Committee at a later date.
APPOINTED MEMBERS PRESENT: ☒ James Edgerton, Chair; ☒George Quick, MBA, ☐ John Griffin; BOARD MEMBERS PRESENT: Chris Bostock, Cynthia Binanay GUEST(S) PRESENT: Mary Hutchings, Wake County Internal Auditor, Vicki Evans, Cumberland County Finance Director
STAFF PRESENT: Rob Robinson, CEO; Kelly Goodfellow, EVP/CFO
1. WELCOME AND INTRODUCTIONS
2. REVIEW OF THE MINUTES – The minutes from the 2/2/17 and 3/2/2017 meeting were reviewed; Chris Bostock made a motion to approve
the minutes. George Quick seconded the motion.
AGENDA ITEMS: DISCUSSION: NEXT STEPS: TIME FRAME:
3. The monthly financial reports were discussed which includes the Statement of Revenue and Expenses – Actual to Budget, Senate Bill 208 Required Ratios, and DMA Contract Ratios
a) Statement of Revenue and Expenses – Actual to Budget as of March 31, 2017 – Alliance currently has revenues exceeding expenses of $15,796,073. The majority of this is related to Medicaid and Medicaid risk reserves. The amount of savings will likely come down as more is spent on claims and administrative functions. Earnings for this time of year are lower than previous years, however that is to be expected as we move forward in the managed care environment (savings are higher in the beginning).
b) Senate Bill 208 Ratios - Alliance is currently meeting and exceeding all required Senate Bill 208 ratios (current ratio and percent paid).
c) DMA Contract Ratios – Alliance is currently meeting all DMA contractual required ratios (defensive interval and MLR).
4. Kelly Goodfellow gave a high level overview of the FY18 recommended budget. The recommended budget will be presented at the board meeting following the Finance Committee meeting.
Finance Committee Meeting 6/1/17 Page 2 of 6

Thursday, May 04, 2017 BOARD FINANCE COMMITTEE
Draft minutes may be submitted with the monthly Board packet. Minutes will be approved by this Committee at a later date.
AGENDA ITEMS: DISCUSSION: NEXT STEPS: TIME FRAME:
5. Kelly Goodfellow gave a brief overview of care management software that Alliance is considering. An RFP was released and a select number of companies are in the final review process. A decision will be made soon. The funds for this investment are in both FY17 and the upcoming FY18 budget.
6. ADJOURNMENT
Finance Committee Meeting 6/1/17 Page 3 of 6

% Received/Original Budget Current Period Year to Date Balance Expended
REVENUESLocal Grants $36,874,048.00 $2,921,898.65 $26,580,611.64 $10,293,436.36 72.08%State & Federal Grants 55,113,711.00 3,374,049.04 31,800,295.93 23,313,415.07 57.70%Medicaid Waiver Services 348,220,800.00 30,210,359.16 302,912,533.17 45,308,266.83 86.99%In Kind - - 1,372,449.37 -
Total Revenue 440,208,559.00 36,506,306.85 362,665,890.11 78,915,118.26 82.39%
AdministrativeLocal Administration 369,835.81 30,874.65 308,746.50 61,089.31 83.48%LME Administrative Grant 4,359,385.00 363,282.00 3,632,820.00 726,565.00 83.33%Medicaid Waiver Administration 44,330,623.20 3,925,345.13 39,392,813.35 4,937,809.85 88.86%Miscellanous Revenue 100,000.00 46,998.32 243,182.67 (143,182.67) 243.18%
Total Administrative Revenue 49,159,844.01 4,366,500.10 43,577,562.52 5,582,281.49 88.64%
Total Revenues 489,368,403.01 40,872,806.95 406,243,452.63 84,497,399.75 83.01%
EXPENSESLocal Services 36,874,048.00 2,218,245.65 24,697,541.75 12,176,506.25 66.98%State & Federal Services 55,113,711.00 5,472,952.25 44,204,553.04 10,909,157.96 80.21%Medicaid Waiver Services 348,220,800.00 24,710,590.53 275,820,762.12 72,400,037.88 79.21%In Kind Expenses - - 1,372,449.37 -
Total Service Expenses 440,208,559.00 32,401,788.43 346,095,306.28 95,485,702.09 78.62%
AdministrativeOperational 6,749,177.51 528,061.29 4,434,456.87 2,314,720.64 65.70%Salaries, Benefits, and Fringe 34,017,214.69 3,096,446.83 29,657,884.12 4,359,330.57 87.18%Professional Services 8,293,451.81 459,655.15 5,872,877.11 2,420,574.70 70.81%Miscellanous Expense 100,000.00 - - 100,000.00 0.00%
Total Administrative Expenses 49,159,844.01 4,084,163.27 39,965,218.10 9,094,625.91 81.30%
Total Expenses 489,368,403.01 36,485,951.70 386,060,524.38 104,580,328.00 78.89%
CHANGE IN NET POSITION $4,386,855.25 $20,182,928.25
Statement of Revenue and Expenses (Budget and Actual) - As of April 30, 2017
Finance Committee Meeting 6/1/17 Page 4 of 6

Senate Bill 208 Ratios - As of April 30, 2017
99.84%
86%
88%
90%
92%
94%
96%
98%
100%
102%
N O V - 1 6 D E C - 1 6 J A N - 1 7 F E B - 1 7 M A R - 1 7 A P R - 1 7
PERCENT PAID
Bench Mark Alliance
Percent Paid = Percent of clean claims paid within 30 days of receiving. The benchmark is 90%.
Current Ratio = Compares current assets to current liabilities. Liquidity ratio that measures an organization's ability to pay short term oblications. The benchmark is 1.0.
3.38
0.00
0.50
1.00
1.50
2.00
2.50
3.00
3.50
4.00
N O V - 1 6 D E C - 1 6 J A N - 1 7 F E B - 1 7 M A R - 1 7 A P R - 1 7
CURRENT RATIO
Bench Mark Alliance
Finance Committee Meeting 6/1/17 Page 5 of 6

DMA Ratios - As of April 30, 2017
99.92
0
20
40
60
80
100
120
N O V - 1 6 D E C - 1 6 J A N - 1 7 F E B - 1 7 M A R - 1 7 A P R - 1 7
DEFENSIVE INTERVAL
Bench Mark Alliance
Defensive Interval = Current assets divided by average daily operating expenses. This rato shows how many days the organization can continue to pay expenses if no additional cash comes in. The benchmark is 30 days.
87%
70%
75%
80%
85%
90%
95%
N O V - 1 6 D E C - 1 6 J A N - 1 7 F E B - 1 7 M A R - 1 7 A P R - 1 7
MEDICAL LOSS RATIO
Bench Mark MLR
Medical Loss Ratio (MLR) = Total Services Expenses plus Administrative Expenses that go towards directly improving health outcomes divided by Total Medicaid Revenue less Risk Reserve Revenue. The benchmark is 85% however we are held harmless until July 2017. Beginning July 2017 Risk Reserve will be included in revenue.
Finance Committee Meeting 6/1/17 Page 6 of 6

5C
(Back to agenda)
ITEM: Policy Committee Report DATE OF BOARD MEETING: June 1, 2017 BACKGROUND: Per Alliance Behavioral Healthcare Area Board Policy “Development of Policies
and Procedures”, the Board is to review all policies annually. The Board Policy Committee reviews a number of Policies each quarter in order to meet this requirement. Policies reviewed at the May 11, 2017 Policy Committee meeting and ready for Board approval without revisions: Equal Employment Opportunity/Affirmative Action Recruitment and Selection Conditions of Employment Classification and Compensation Employee Benefits Alcohol and Drug Free Workplace Employee Time and Attendance Sexual Harassment Leave Policy Family and Medical Leave Act Clinical Staff Credentialing Disciplinary Action Performance Management Separation Employee Complaint Employee Grievance Reduction-in-Force Policies reviewed with suggested revisions: Management and Investigation of Grievances Fund Balance Proposed Policy reviewed and recommended for adoption: Budget Transfers REQUEST FOR AREA BOARD ACTION: Accept the report. Accept Board Policy Committee minutes from the May meeting as submitted. As part of the annual review process approve the above listed policies for continued use. Approve the recommended changes to the above listed policies. Accept proposed policy for adoption as submitted CEO RECOMMENDATION: Accept the report. Approve the reviewed policies for continued use and approve the proposed and revised policies. RESOURCE PERSON(S): Curtis Massey, Committee Chair; Monica Portugal, Chief Compliance Officer
Alliance Behavioral Healthcare BOARD OF DIRECTORS
Agenda Action Form

Thursday, May 11, 2017 BOARD POLICY COMMITTEE - REGULAR MEETING 4600 Emperor Boulevard, Durham, NC 27703 4:00-6:00 p.m.
Draft minutes may be submitted with the monthly Board packet. Minutes will be approved by this Committee at a later date. Page 1 of 4
APPOINTED MEMBERS PRESENT: ☒Lodies Gloston, M.A., ☐Phillip Golden, B.A., ☒Curtis Massey, J.D. (via teleconference) (Committee Chair)\
BOARD MEMBERS PRESENT: ☒ Christopher Bostock (via teleconference) STAFF PRESENT: Carol Hammett, General Counsel; Monica Portugal, Chief Compliance Officer; Asheena McMillan,
Administrative Assistant, Sarah Pacholke, SVP-Financial Operations 1. WELCOME AND INTRODUCTIONS 2. REVIEW OF THE MINUTES: The minutes from the February 9, 2017, and March 7, 2017 meetings were reviewed; a motion was made by Ms. Gloston and seconded by Mr. Massey to approve the minutes. Motion passed unanimously.
AGENDA ITEMS: DISCUSSION: NEXT STEPS: TIME FRAME:
Documents Provided February 9, 2017 and March 7, 2017 Minutes; Human Resources Policies (17); Quality Management Policy QM-2 – Management and Investigation of Grievances; Business Operations Policy BO-9 – Fund Balance; Proposed Business Operations Policy entitled Budget Transfers.
Annual Review of Policies:
The Committee reviewed all Human Resources policies: Human Resources Policies reviewed and considered for continued use without revisions: HR-1 - Equal Employment Opportunity/Affirmative Action. A Motion was made by Ms. Gloston to accept HR-1 as presented, and motion
was seconded by Mr. Massey. Motion carried.
HR-2 - Recruitment and Selection.

Thursday, May 11, 2017 BOARD POLICY COMMITTEE - REGULAR MEETING 4600 Emperor Boulevard, Durham, NC 27703 4:00-6:00 p.m.
Draft minutes may be submitted with the monthly Board packet. Minutes will be approved by this Committee at a later date. Page 2 of 4
AGENDA ITEMS: DISCUSSION: NEXT STEPS: TIME FRAME:
A Motion was made by Ms. Gloston to accept HR-2 as presented, and motion
was seconded by Mr. Massey. Motion carried.
HR-4 - Conditions of Employment A Motion was made by Ms. Gloston to accept HR-4 as presented, and motion
was seconded by Mr. Massey. Motion carried.
HR-5 – Classification and Compensation
A Motion was made by Ms. Gloston to accept HR-5 as presented, and motion
was seconded by Mr. Massey. Motion carried.
HR-6 – Employee Benefits
A Motion was made by Ms. Gloston to accept HR-6 as presented, and motion
was seconded by Mr. Massey. Motion carried.
HR-7 – Alcohol and Drug Free Workplace
A Motion was made by Ms. Gloston to accept HR-7 as presented, and motion
was seconded by Mr. Massey. Motion carried.
HR-8 – Employee Time and Attendance
A Motion was made by Ms. Gloston to accept HR-8 as presented, and motion
was seconded by Mr. Massey. Motion carried.
HR-9 – Sexual Harassment A Motion was made by Ms. Gloston to accept HR-9 as presented, and motion
was seconded by Mr. Massey. Motion carried.
HR-10 – Leave Policy
A Motion was made by Ms. Gloston to accept HR-10 as presented, and motion
was seconded by Mr. Massey. Motion carried.

Thursday, May 11, 2017 BOARD POLICY COMMITTEE - REGULAR MEETING 4600 Emperor Boulevard, Durham, NC 27703 4:00-6:00 p.m.
Draft minutes may be submitted with the monthly Board packet. Minutes will be approved by this Committee at a later date. Page 3 of 4
AGENDA ITEMS: DISCUSSION: NEXT STEPS: TIME FRAME:
HR-11 – Family and Medical Leave Act A Motion was made by Ms. Gloston to accept HR-11 as presented, and motion
was seconded by Mr. Massey. Motion carried.
HR-12 – Clinical Staff Credentialing
A Motion was made by Ms. Gloston to accept HR-12 as presented, and motion
was seconded by Mr. Massey. Motion carried.
HR-14 – Disciplinary Action
A Motion was made by Ms. Gloston to accept HR-14 as presented, and motion
was seconded by Mr. Massey. Motion carried. HR-15 – Performance Management A Motion was made by Ms. Gloston to accept HR-15 as presented, and motion
was seconded by Mr. Massey. Motion carried.
HR-16 – Separation A Motion was made by Ms. Gloston to accept HR-16 as presented, and motion
was seconded by Mr. Massey. Motion carried.
HR-17 – Employee Complaint A Motion was made by Ms. Gloston to accept HR-17 as presented, and motion
was seconded by Mr. Massey. Motion carried. HR-18 – Employee Grievance
A Motion was made by Ms. Gloston to accept HR-18 as presented, and motion
was seconded by Mr. Massey. Motion carried. HR-19 – Reduction-in-Force A Motion was made by Ms. Gloston to accept HR-19 as presented, and motion
was seconded by Mr. Massey. Motion carried.

Thursday, May 11, 2017 BOARD POLICY COMMITTEE - REGULAR MEETING 4600 Emperor Boulevard, Durham, NC 27703 4:00-6:00 p.m.
Draft minutes may be submitted with the monthly Board packet. Minutes will be approved by this Committee at a later date. Page 4 of 4
AGENDA ITEMS: DISCUSSION: NEXT STEPS: TIME FRAME:
Other Policies for Revision:
Network Administration, Clients Rights, Quality Management Policy QM-2 – Management and Investigation of Grievances. Revisions made to definition of Grievance to mirror language in Alliance’s Contract with DMA. A Motion was made by Ms. Gloston to accept QM-2 as amended,
pending approval of the definition by the External Quality Review
Organization (EQRO), and motion was seconded by Mr. Massey. Motion
carried. Business Operations Finance Policy
BO-9 – Fund Balance. Sara Pachokle presented proposed revisions to Policy. A Motion was made by Ms. Gloston to accept BO-9 as amended,
and motion was seconded by Mr. Massey. Motion carried.
New Proposed Policies:
Sara Pachokle presented a proposed Business Operations policy entitled Budget Transfers. The policy dictates that transfers under $100K shall be reported to the Finance Committee, while transfers over $100K shall be presented to the Area Board for approval. The policy would permit transfers of State funds up to $100K within an appropriation between counties. In addition, the policy would permit multiple transactions, to include those below the reporting threshold. A Motion was made by Ms. Gloston to accept the
proposed Budget Transfers Policy as presented, and motion was seconded by
Mr. Massey. Motion carried.
Upcoming Meetings: The Board Policy Committee will meet to conclude its review of the By-Laws on Tuesday, June 6, 2017 at 1:00 pm. A Motion was made by Ms. Gloston to
conduct a Special Meeting of the Board Policy Committee in June 2017, and
motion was seconded by Mr. Massey. Motion carried.
3. ADJOURNMENT: @ 5:05pm. Next regular meeting will be August 10, 2017, from 4:00 p.m. to 5:30 p.m.

AREA BOARD POLICIES & PROCEDURES
I. PURPOSE
The purpose of this policy is to ensure the fair treatment of applicants and employees in all aspects of personnel administration without regard to race, color, religion, sex, sexual orientation, national origin, political affiliations, age, or disability and with proper regard for their privacy and constitutional rights as citizens. This “fair treatment” principle includes compliance with the federal employment opportunity and nondiscrimination laws. II. POLICY STATEMENT 1. Equal Employment Opportunity:
Alliance Behavioral Healthcare is committed to equal employment opportunity for all who seek employment with the organization as well as those employed by the organization. Discrimination in all forms is prohibited. As a means of carrying out its commitment, the Area Board shall enforce the relevant provisions of the Civil Rights Act of 1964 as amended, the Equal Pay Act of 1963, the Age Discrimination in Employment Act of 1967 as amended, the Rehabilitation Act of 1973 as amended and all other statutes or regulations governing equal employment opportunity. In furtherance of this policy, the Area Board prohibits retaliatory action of any kind taken by any employee of Alliance Behavioral Healthcare against any other employee, client, or applicant for employment because that person filed a complaint or charge; or assisted, testified, or participated in any manner in a hearing, proceeding, or investigation of a complaint charge.
2. Affirmative Action:
Alliance Behavioral Healthcare is committed to ensuring utilization of women, minorities, and the disabled as part of its workforce. The Area Director shall develop and implement a program of affirmative action to assure that all personnel policies and practices facilitate employment opportunities for women, minorities and the disabled. Annually, the Area Director shall provide a report on the distribution of the gender, minorities and disabled employees to the Board.
TITLE: Equal Employment Opportunity/Affirmative Action BOARD POLICY #: HR-1 LINES OF BUSINESS: Human Resources RESPONSIBILITY: Area Board, Area Director REFERENCE(S): NC G.S. 126-11 URAC STANDARDS: CORE, v. 3.0, Standard 4 APPROVAL DATE: 5/3/2012 LATEST REVISION DATE: 6/2/2016
LATEST REVIEW DATE: 6/2/2016
TITLE: Equal Employment Opportunity/Affirmative Action
LATEST REVISION DATE: 6/2/2016
PAGE: 2 of 2
III. PROCEDURES The Area Director will develop procedures to implement this policy.
AREA BOARD POLICIES & PROCEDURES
I. PURPOSE
The purpose of this policy is to define certain terms and conditions that individuals must meet to be hired by Alliance Behavioral Healthcare. The contents of this policy are not intended to serve as an exhaustive list of requirements or conditions of employment, and some or all of the requirements and conditions described in this policy may not apply to every individual who is hired.
II. PERSONS AFFECTED
This policy primarily impacts newly hired, transferred, or promoted employees in all employee classifications. It also requires all current employees to report felony convictions that occur at any time during their employment.
III. POLICY STATEMENT
It is the policy of Alliance Behavioral Healthcare that all employees satisfy job-related eligibility conditions including but not limited to licensure, certification and/or credentialing and satisfactory criminal background checks and e-verify employment verification. Alliance shall not employ anyone who is excluded from participation in federal healthcare programs or federal procurement activities and has been identified on the list of excluded individuals/entities maintained by the Office of Inspector General of the US DHHS or the Excluded Parties List System maintained by the federal System for Award Management (SAM). IV. PROCEDURES The Area Director shall develop procedures to implement this Policy.
TITLE: Conditions of Employment BOARD POLICY #: HR-4 LINES OF BUSINESS: Human Resources RESPONSIBILITY: Area Board, Area Director REFERENCE(S): URAC STANDARDS: CORE, v. 3.0, Standard 27 APPROVAL DATE: 5/3/2012 LATEST REVISION DATE: 6/4/2015
LATEST REVIEW DATE: 6/2/2016

AREA BOARD POLICIES & PROCEDURES
I. PURPOSE The purpose of this policy is to set forth the basis for providing benefits for the employees of Alliance Behavioral Healthcare. II. POLICY STATEMENT Alliance Behavioral Healthcare shall offer a comprehensive benefits plan for employees and their eligible dependents as outlined below. A. Eligibility 1. All probationary, provisional, trainee and regular employees who work a minimum of 50% of a
regular work schedule per week are eligible. 2. Employees may also cover a legally recognized spouse and/or children, including legally adopted
children, step children, children placed for adoption, children for whom legal guardianship has been awarded to the employee, and children whose coverage is court-ordered.
B. Benefits The following Employee Benefits Plans shall be offered by Alliance:
1. Health Insurance 2. Dental Insurance 3. Vision Insurance 4. Life Insurance and Accidental Death and Dismemberment 5. Short Term Disability 6. Long Term Disability 7. Voluntary Life Insurance 8. Voluntary Long Term Care
TITLE: Employee Benefits BOARD POLICY #: HR-6 LINES OF BUSINESS: Human Resources RESPONSIBILITY: Area Board, Area Director REFERENCE(S): URAC STANDARDS: APPROVAL DATE: 5/15/2012 LATEST REVISION DATE: 6/2/2016
LATEST REVIEW DATE: 6/2/2016

TITLE: Employee Benefits
LATEST REVISION DATE: 6/2/2016
PAGE: 2 of 2
9. Voluntary Hospital Confinement 10. Voluntary Section 125-Flexible Spending Account 11. Voluntary NC 529 College Savings Plan 12. Local Government Employee Retirement System participation 13. NC 401K Plan 14. NC 457 Plan-Voluntary 15. Employee Assistance Program (EAP)
C. Availability of Funding
Benefit offerings are subject to change based on funding availability and Alliance Behavioral Healthcare directives. Deletion or addition to the Benefits listed in B above shall be subject to Board approval pursuant to the Alliance by-laws, however changes to employee benefit offerings (i.e. deductibles and co-pays) may be approved by the Area Director.
D. COBRA Rights
Employees who separate from Alliance Behavioral Healthcare for reasons other than gross misconduct may elect to continue their health, dental and vision benefits under COBRA (Consolidated Omnibus Budget Reconciliation Act). III. PROCEDURES
The Area Director shall develop procedures to implement this policy.

AREA BOARD POLICIES & PROCEDURES
I. PURPOSE
Alliance Behavioral Healthcare maintains work hours that ensure optimal productivity and customer service levels and which are compatible with state law, agency functions, and the maintenance of effective work schedules. II. POLICY STATEMENT It is the policy of Alliance Behavioral Healthcare to comply with the Fair Labor Standards Act. The normal work week for nonexempt full-time employees is 40 hours per week. The normal work schedule for exempt full-time employees may average more than 40 hours per week in order to complete work assignments. Employment with Alliance Behavioral Healthcare is based on the following principles:
i. Employees are expected to report for each and every scheduled working day or shift, to report on time and to complete all scheduled hours.
ii. Being absent from or reporting to work after the scheduled beginning time requires the employee to properly notify the supervisor in advance and to utilize appropriate leaves or to lose payment for time not worked.
iii. Employees scheduled to work are expected to remain on the job until completion of the last hour of the scheduled work day or shift.
iv. Arrival any time after the beginning of the scheduled work day or shift is considered late or tardy for performance purposes.
III. PROCEDURES The Area Director will develop procedures to implement this policy.
TITLE: Employee Time and Attendance BOARD POLICY #: HR-8 LINES OF BUSINESS: Human Resources RESPONSIBILITY: Area Board, Area Director REFERENCE(S): N/A URAC STANDARDS: N/A APPROVAL DATE: 5/3/2012 LATEST REVISION DATE: 6/4/2015
LATEST REVIEW DATE: 6/2/2016

AREA BOARD POLICIES & PROCEDURES
I. PURPOSE The purpose of this policy is to establish a consistent system of leave for Alliance Behavioral Healthcare staff.
II. POLICY STATEMENT Alliance Behavioral Healthcare recognizes the importance of balancing work and time away from the workplace and shall provide leave to employees as a privilege when approved by a supervisor according to applicable procedures. III. PROCEDURES The Area Director shall develop procedures to implement this policy.
TITLE: Leave Policy BOARD POLICY #: HR-10 LINES OF BUSINESS: Human Resources RESPONSIBILITY: Area Board, Area Director REFERENCE(S): N/A URAC STANDARDS: N/A APPROVAL DATE: 6/26/2012 LATEST REVISION DATE: 6/4/2015
LATEST REVIEW DATE: 6/2/2016

AREA BOARD POLICIES & PROCEDURES
I. PURPOSE The purpose of this policy is to ensure that clinical staff of Alliance Behavioral Healthcare is appropriately credentialed to perform clinical functions. II. DEFINITIONS Credential: Attestation of qualification, competence or authority issued to an individual by an organization or entity of competent jurisdiction Credentialing: The process of establishing the qualifications of licensed/certified professionals III. POLICY STATEMENT It is the policy of Alliance Behavioral Healthcare to ensure that only those persons with appropriate training, education, credentials and/or experience perform clinical functions. In order to accomplish this, Alliance Behavioral Healthcare shall verify the clinical license and/or certification of applicable personnel at the time of employment or contract and no less than every three years thereafter. Licensed and or certified employees and consultants shall notify Alliance Behavioral Healthcare management in writing of an adverse change in licensure or certification status immediately (within 24 hours) upon learning of the status change. Each employee or consultant shall attest to knowledge of this requirement by signing an attestation at the time of employment or beginning of a contract. IV. PROCEDURES The Area Director shall develop procedures to implement this policy.
TITLE: Clinical Staff Credentialing BOARD POLICY #: HR-12 LINES OF BUSINESS: Human Resources RESPONSIBILITY: Area Board, Area Director REFERENCE(S): DHHS Contracts URAC STANDARDS: CORE, v. 3.0, Standard 30 APPROVAL DATE: 8/2/2012 LATEST REVISION DATE: 6/4/2015
LATEST REVIEW DATE: 6/2/2016

AREA BOARD POLICIES & PROCEDURES
I. PURPOSE The purpose of this policy is to establish a formal assessment program in which each staff member’s performance is evaluated on an annual basis. II. POLICY STATEMENT
Alliance Behavioral Healthcare believes that employees need and deserve an opportunity to receive feedback from their supervisor relating to performance. In addition, a regular evaluation of employees’ performance supports the concept of ‘employee accountability’. The performance appraisal:
1. Provides employees direction in their jobs and an opportunity to discuss any job problems and interests with his or her supervisor;
2. Enhances the likelihood of achieving both the organization’s and the department’s objectives by providing periodic feedback and coaching;
3. Provides an objective, consistent, and uniform way to gauge and improve each employee’s on-the-job performance using objective criteria; and,
4. Correlates the job-performance evaluation directly to the recommended merit increases. A. Requirements The appraisal policy requires managers and supervisors to develop a work plan with individual performance objectives with employees for the year within 30 days of hire. It also requires managers and supervisors to hold periodic review and coaching sessions with employees prior to completion of the probationary period or annual performance evaluation session. Performance reviews are prepared annually. Probationary reviews are given to newly hired employees at the completion of the probationary period to determine performance level and determine regular status eligibility.
TITLE: Performance Management BOARD POLICY #: HR-15 LINES OF BUSINESS: Human Resources RESPONSIBILITY: Area Board, Area Director REFERENCE(S): URAC STANDARDS: CORE, v. 3.0, Standard 29 APPROVAL DATE: 8/2/2012 LATEST REVISION DATE: 6/4/2015
LATEST REVIEW DATE: 6/2/2016

TITLE: Performance Management LATEST REVISION DATE: 6/4/2015
PAGE: 2 of 2
III. PROCEDURES The Area Director shall develop procedures to implement this policy.

AREA BOARD POLICIES & PROCEDURES
I. PURPOSE The purpose of this policy is to provide a mechanism for employees to address unfair and/or poor employment practices that are not covered by the grievance policy. II. DEFINITION
Complaint: Any written employee concern or dissatisfaction for which redress is sought, that is not otherwise covered under the Grievance Policy (see Policy HR-18). Employee: Any permanent, temporary or contractual employee of Alliance Behavioral Healthcare.
III. POLICY STATEMENT
Alliance Behavioral Healthcare is committed to a consistent, equitable, and legally defensible process for the resolution of employee complaints. Employees shall have the right to file a complaint via the employee complaint procedure to address employment conditions other than disciplinary, reduction-in-force, or discriminatory actions. An employee that files a complaint shall not be subject to retaliation for filing a complaint. IV. PROCEDURES The Area Director shall develop procedures to implement the provisions of this policy.
TITLE: Employee Complaint BOARD POLICY #: HR-17 LINES OF BUSINESS: Human Resources RESPONSIBILITY: Area Board, Area Director REFERENCE(S): N/A URAC STANDARDS: CORE, v. 3.0, Standard 4 APPROVAL DATE: 8/2/2012 LATEST REVISION DATE: 6/4/2015
LATEST REVIEW DATE: 6/2/2016
AREA BOARD POLICIES & PROCEDURES
I. PURPOSE The purpose of this policy is to provide guidance for executing reductions in the workforce due to shortages of funds or work and/or changes in organizational objectives and policies which cause the consolidation, reorganization, or elimination of programs, functions, positions, or organizational work units. II. POLICY STATEMENT Alliance Behavioral Healthcare will make every effort to consider all feasible alternatives to involuntary separation of employees through reduction-in-force (RIF). Factors that will be considered in determining which employee(s) will be separated include: (1) applicable laws and regulations; (2) impact on overall program objectives; (3) departmental organization structure; (4) funding sources and budgetary guidelines; (5) possible re-distribution of staff and other resources; (6) appointment type (regular, provisional, probationary, temporary, emergency, seasonal); (7) seniority; and (8) employee job performance. The Area Director will present the circumstances of an impending RIF to the Area Board for approval. This notification should be in the form of a proposed reduction plan, which will document the reason(s) for the reduction in the workforce; the effective date of the reduction; the proposed course of action and associated factors considered; the specific classifications of positions scheduled for reallocation, reassignment and/or abolishment, along with before and after RIF organization charts. III. PROCEDURES The Area Director shall develop procedures to implement this policy.
TITLE: Reduction- in-Force BOARD POLICY #: HR-19 LINES OF BUSINESS: Human Resources RESPONSIBILITY: Area Board, Area Director REFERENCE(S): URAC STANDARDS: APPROVAL DATE: 8/2/2012 LATEST REVISION DATE: 6/4/2015
LATEST REVIEW DATE: 6/2/2016

AREA BOARD POLICIES & PROCEDURES
I. PURPOSE The purpose of this policy is to provide a standard for the staff recruitment and selection process. II. POLICY STATEMENT Alliance Behavioral Healthcare is committed to systematic recruitment and selection programs that are designed to identify, attract, and select from the most qualified applicants for employment. The Board strives for diverse representation at all levels of the workforce while engaging in recruitment and selection practices that are in compliance with all applicable employment laws. It is the policy of Alliance Behavioral Healthcare to provide equal employment opportunities for employment to all applicants and employees. III. PROCEDURES The Area Director will develop procedures to implement this policy.
TITLE: Recruitment and Selection BOARD POLICY #: HR-2 LINES OF BUSINESS: Human Resources RESPONSIBILITY: Area Board, Area Director REFERENCE(S): URAC STANDARDS: APPROVAL DATE: 5/3/2012 LATEST REVISION DATE: 6/4/2015
LATEST REVIEW DATE: 6/2/2016

AREA BOARD POLICIES & PROCEDURES
I. PURPOSE The purpose of this policy is to establish and maintain a classification and compensation plan in order to attract, motivate, and retain highly qualified employees. The plan shall provide a structure to administer salaries fairly and equitably. All employees shall be covered under the classification and compensation plan, except for the Area Director whose compensation is set by the Board of Directors. II. POLICY STATEMENT It is the policy of Alliance Behavioral Healthcare to ensure that its system of compensation is internally equitable, market competitive and administered without regard to age, sex, race, color, creed, religion, national origin, physical or mental condition, sexual orientation, non-job related disability, political affiliation, marital status, or other non-merit factors. A. The Classification and Compensation Plan The Classification and Compensation Plan shall consist of a system for identifying all types and levels of positions together with standards and procedures for maintaining the plan. Each position in Alliance Behavioral Healthcare is grouped with similar positions. This grouping is called a “Classification.” Job classifications shall be established to reflect the type of work performed, level of difficulty, and responsibilities associated with a position. Annually, the Board shall review and approve the Classification and Compensation plan. The Classification and Compensation Plan shall provide a salary rate structure that may be revised in response to labor market trends. Each classification shall be assigned to a grade level with a designated salary range. No beginning pay rate will be below the federal or state minimum wage. B. Minimum Qualification Standards It shall be the policy of Alliance Behavioral Healthcare to establish job related minimum qualification standards wherever practical for each class of work in the classification and compensation plan. The
TITLE: Classification and Compensation BOARD POLICY #: HR-5 LINES OF BUSINESS: Human Resources RESPONSIBILITY: Area Board, Area Director REFERENCE(S): URAC STANDARDS: APPROVAL DATE: 5/3/2012 LATEST REVISION DATE: 6/4/2015
LATEST REVIEW DATE: 6/2/2016

TITLE: Classification and Compensation
LATEST REVISION DATE: 6/4/2015
PAGE: 2 of 2
standards shall be based on the required skills, knowledge, and abilities common to each classification. The qualification standards and job related skills, knowledge and abilities shall serve as guides for the selection and placement of individuals. III. PROCEDURES The Area Director shall develop procedures to implement this policy.

AREA BOARD POLICIES & PROCEDURES
I. PURPOSE The purpose of this policy is to affirm the Area Board’s prohibition against the use, distribution, dispensation and possession of controlled substances and the use of alcohol and abuse of prescription drugs by employees and contractors at the workplace. This policy is also meant to comply with the requirements of the Drug Free Workplace Act of 1988 and Attachment H of the NC Department of Health and Human Services, Division of Medical Assistance 1915(b)(c) waiver. II. POLICY STATEMENT It shall be the policy of Alliance Behavioral Healthcare to maintain an alcohol and drug free workplace. The unlawful manufacture, distribution, dispensation, possession or use of nonprescription controlled substance or alcohol in the workplace by Alliance Behavioral Healthcare employees or contractors is prohibited. Employees and contractors may not report to work under the influence of a nonprescription controlled substance or alcohol and may not use any such substance during work hours. Also prohibited is the misuse of prescription or nonprescription medication which results in impaired behavior on the job. Violation of this policy shall constitute inappropriate personal conduct which will subject the employee or contractor to disciplinary action up to and including dismissal. III. PROCEDURES The Area Director shall develop procedures to implement this policy.
TITLE: Alcohol and Drug Free Workplace BOARD POLICY #: HR-7 LINES OF BUSINESS: Human Resources RESPONSIBILITY: Area Board, Area Director REFERENCE(S): Drug Free Workplace Act of 1988 URAC STANDARDS: CORE, v. 3.0, Standards 4 & 27 APPROVAL DATE: 5/3/2012 LATEST REVISION DATE: 6/4/2015
LATEST REVIEW DATE: 6/2/2016

AREA BOARD POLICIES & PROCEDURES
I. PURPOSE The Area Board believes that all employees are entitled to work in an environment that is free of sexual harassment. To this end, the Board shall establish a policy to govern the behavior of all its employees, consultants, contractors, vendors, and suppliers regarding the prohibition of sexual harassment.
II. POLICY STATEMENT It is the policy of Alliance Behavioral Healthcare to provide a work environment that is free of sexual harassment. For purposes of this policy, sexual harassment is defined as deliberate, unsolicited and unwelcomed verbal or physical conduct of a sexual nature or with sexual implications which:
i. has or may have a direct bearing on a selection decision; ii. creates an offensive, intimidating, or hostile work environment;
iii. interferes with a person’s job or job seeking performance.
Sexual harassment is herein deemed a form of sex discrimination prohibited by Title VII of the Civil Rights Act of 1964 and NC G.S. 126-16.
In furtherance of this policy, the Area Board prohibits retaliatory action of any kind taken by any employee of Alliance Behavioral Healthcare against any other employee, client, or applicant for employment because that person filed a complaint or charge; or assisted, testified, or participated in any manner in a hearing, proceeding, or investigation of a sexual harassment complaint charge. III. PROCEDURES All complaints of sexual harassment shall be promptly and thoroughly investigated. The Area Director shall develop procedures for handling sexual harassment complaints.
TITLE: Sexual Harassment BOARD POLICY #: HR-9 LINES OF BUSINESS: Human Resources RESPONSIBILITY: Area Board, Area Director REFERENCE(S): Title VII of the Civil Rights Act of 1964; NC G.S. 126-16 URAC STANDARDS: CORE, v. 3.0, Standard 4 APPROVAL DATE: 5/3/2012 LATEST REVISION DATE: 6/4/2015
LATEST REVIEW DATE: 6/2/2016

AREA BOARD POLICIES & PROCEDURES
I. PURPOSE The purpose of this policy is to set forth the conditions and process for implementing the provisions of the Family and Medical Leave Act of 1993, as amended. II. POLICY STATEMENT In compliance with the Family and Medical Leave Act (FMLA) of 1993, as amended, Alliance Behavioral Healthcare shall provide leave to eligible employees who have worked for Alliance for at least 12 months and at least 1,250 hours in the 12 calendar months immediately preceding the request for leave or otherwise deemed eligible under the FMLA Act. III. PROCEDURES The Area Director will develop procedures to implement this policy.
TITLE: Family and Medical Leave Act BOARD POLICY #: HR-11 LINES OF BUSINESS: Human Resources RESPONSIBILITY: Area Board, Area Director REFERENCE(S): FMLA of 1993, as amended in 2008 URAC STANDARDS: CORE, v. 3.0, Standard 4 APPROVAL DATE: 6/26/2012 LATEST REVISION DATE: 6/2/2016
LATEST REVIEW DATE: 6/2/2016

AREA BOARD POLICIES & PROCEDURES
I. PURPOSE The purpose of this policy is to ensure that Alliance Behavioral Healthcare develops a clear and consistent process for equitable disciplinary actions.
II. POLICY STATEMENT It is the Policy of Alliance to provide employees and supervisors a clear and consistent process for implementing and evaluating the fair and just delivery of appropriate disciplinary actions, promote efficient and equitable treatment for all employees. Alliance shall ensure that disciplinary actions, including dismissal, are administered in as near a uniform manner as possible, allow for the prompt, orderly and efficient resolution of problems and differences arising between the supervisor and employee, and ensure compliance with applicable federal and state laws, rules and regulations. It is the intent of Alliance to provide any employee, supervisors and management with a fair, clear and useful tool for correcting and improving performance issues, as well as to provide a process to assist management in addressing instances of unacceptable personal conduct. III. PROCEDURES The Area Director shall develop procedures to implement this Policy.
TITLE: Disciplinary Action BOARD POLICY #: HR-14 LINES OF BUSINESS: Human Resources RESPONSIBILITY: Area Board, Area Director REFERENCE(S): URAC STANDARDS: CORE, v. 3.0, Standards 27 & 29 APPROVAL DATE: 8/2/2012 LATEST REVISION DATE: 6/2/2016
LATEST REVIEW DATE: 6/2/2016

AREA BOARD POLICIES & PROCEDURES
I. PURPOSE The purpose of this policy is to provide guidelines for separation of employment with Alliance Behavioral Healthcare.
II. POLICY STATEMENT
Separation from employment may result from either voluntary or involuntary termination. For the purpose of this policy, voluntary termination means separation is initiated by the employee (examples: resignation or retirement). Involuntary termination means separation occurs when the separation is not initiated by the employee (examples: appointment ended, dismissal, probationary dismissal, reduction-in-force, and unavailability of leave). An employee is considered to have resigned in "good standing" if he/she provides written notice within at least fourteen calendar days of his/her separation date. Failure to give fourteen calendar days’ written notice may be cause for denial of consideration for reemployment, and the employee may be deemed to have resigned ‘not in good standing”. Unauthorized absences from work for a period of three or more days may be considered a voluntary resignation. The Area Director has the authority to set the time and conditions of employment separation. Regular employees who separate from Alliance and return within 30 calendar days will be reinstated with no break in service. III. PROCEDURES The Area Director shall develop procedures to implement this policy.
TITLE: Separation BOARD POLICY #: HR-16 LINES OF BUSINESS: Human Resources RESPONSIBILITY: Area Board, Area Director REFERENCE(S): URAC STANDARDS: APPROVAL DATE: 8/2/2012 LATEST REVISION DATE: 6/4/2015
LATEST REVIEW DATE: 6/2/2016

AREA BOARD POLICIES & PROCEDURES
I. PURPOSE The purpose of this policy is to provide a grievance process for certain employees of Alliance Behavioral Healthcare contesting a disciplinary action, Reduction in Force, alleged illegal discrimination or harassment based on race, religion, color, national origin, sex (including pregnancy, childbirth, and related medical conditions), age, disability (physical or mental including AIDS/HIV status), genetic information (i.e. Sickle cell or hemoglobin C trait), citizenship status, military status or service, or political affiliation, or other issue grievable under state law. This policy applies to Alliance career status and permanent employees. Career status employees are eligible for appeal rights through the internal Alliance grievance process and the State Human Resources Commission and Office of Administrative Hearings. Permanent employees who have not yet attained career status have appeal rights through the Alliance grievance process, but not outside Alliance unless they allege the employment action is being imposed on the basis of illegal discrimination. This policy does not apply to probationary, intern, temporary or trainee employees, except for grievances on the basis of alleged illegal discrimination or harassment or as otherwise provided under state law. It is the intent of this policy to encourage employees to resolve their grievance at the lowest level possible. II. DEFINITION
Career status employee – A permanent employee who has been continuously (without break) employed in a position subject to the State Personnel Act for the immediate preceding 12 months. Permanent employee – An employee who has been appointed to a permanently established position following the satisfactory completion of a probationary period in accordance with 25 NCAC 01I .2002(c). Probationary employee – An employee serving a probationary appointment of not less than 3 months but not more than 9 months in accordance with 25 NCAC 01I .2002(a). Reduction in Force (RIF) – Separation of employment with Alliance based on reductions in the workforce due to shortages of funds or work and/or changes in organizational objectives and policies
TITLE: Employee Grievance BOARD POLICY #: HR-18 LINES OF BUSINESS: Human Resources RESPONSIBILITY: Area Board, Area Director REFERENCE(S): NC G.S. 126 Article 8; 25 NCAC 01I .2002(a) URAC STANDARDS: CORE, v. 3.0, Standard 4 APPROVAL DATE: 8/2/2012 LATEST REVISION DATE: 6/2/2016
LATEST REVIEW DATE: 6/2/2016

TITLE: Employee Grievance
LATEST REVISION DATE: 6/2/2016
PAGE: 2 of 2
which cause the consolidation, reorganization, or elimination of programs, functions, positions, or organizational work units. III. POLICY STATEMENT Alliance Behavioral Healthcare is committed to a consistent, equitable, and legally defensible process for the resolution of employee grievances regarding hiring, separation, disciplinary, reduction-in-force, or alleged discriminatory actions that are grievable under state law. Permanent employees have the right to grieve when they disagree with certain disciplinary actions (suspension, demotion, or dismissal) taken against them. All employees also have the right to grieve if they believe they have been subject to illegal discrimination or harassment. Permanent employees subject to a reduction-in-force may also grieve as permitted under state law. Written warnings, placement on investigatory status with pay, and extensions of disciplinary actions are not grievable and are not appealable to the State Office of Administrative Hearings (OAH). Employees may file a complaint for all employment issues not covered by this policy. No action involving demotion, suspension, or dismissal is to be taken against an employee for disciplinary reasons until such action has been approved by the CEO/Area Director or designee except when, in the judgment of the manager the immediate suspension is necessary to protect the safety of persons or property. In no case, however, shall an employee be dismissed without the written approval of the Area Director/CEO or designee. Employees seeking redress under the grievance policy shall not suffer retaliation for filing a grievance. IV. PROCEDURES The Area Director/CEO shall develop procedures to implement the provisions of this policy. The procedures shall comply with all relevant Federal, State and local requirements. If any provision of this policy conflicts with duly promulgated Federal or State laws, rules or regulations, the provision of the law, rule or regulation shall govern.

AREA BOARD POLICIES & PROCEDURES
I. PURPOSE The purpose of this policy is to establish a process for receiving, investigating, resolving and managing grievances in a consistent manner. II. DEFINITIONS Complainant: Enrollee/consumer, legally responsible person, or Providers, authorized in writing and acting on behalf of the enrollee/consumer filing the grievance. Does not include providers, stakeholders or other individuals not acting on behalf of a consumer. Grievance: an expression of dissatisfaction, about any matter other than an adverse benefit determination, by an enrollee, their legal guardian, or Provider, authorized in writing and acting on behalf of the enrollee/consumer about matters involving Alliance or an Alliance Network Provider. Possible subjects for grievances include, but are not limited to, the quality of services provided through Alliance, and aspects of interpersonal relationships such as rudeness of a Network Provider or an employee of Alliance, or failure by Alliance or a Network Provider to respect the rights of an Enrollee.Grievance: an expression of dissatisfaction by an enrollee, their legal guardian, or Provider, authorized in writing and acting on behalf of the enrollee/consumer about any matter other than decisions regarding requests for Medicaid services. Provider: an individual, agency or organization that provides mental health, developmental disabilities and/or substance abuse services to consumers and families.
III. POLICY STATEMENT It is the policy of Alliance Behavioral Healthcare to respond to grievances received concerning the provision of publicly funded services in the Alliance Behavioral Healthcare catchment area. It is also the policy of Alliance Behavioral Healthcare to use the information gleaned from grievance proceedings as part of Alliance’s quality improvement process. IV. PROCEDURES
TITLE: Management and Investigation of Grievances BOARD POLICY #: QM-2 LINES OF BUSINESS: Network Administration, Clients Rights, Quality Management RESPONSIBILITY: Area Board, Area Director REFERENCE(S): 10A NCAC 27G. 7002, 7003 URAC STANDARDS: CORE, v. 3.0, Standard 35 APPROVAL DATE: 5/15/2012 LATEST REVISION DATE: 4/2/2015
LATEST REVIEW DATE: 3/3/2016

TITLE: Management and Investigation of Grievances
LATEST REVISION DATE: 1/13/2015
PAGE: 2 of 2
The Area Director shall develop procedures to implement this policy. The procedures shall comply with all relevant state and Federal statutes and requirements of all regulatory, funding or accrediting bodies.

AREA BOARD POLICIES & PROCEDURES
I. PURPOSE The purpose of this policy is to ensure Alliance Behavioral Healthcare has a fund balance that contributes to the Organization’s fiscal health and is adequate to meet Alliance Behavioral Healthcare’s operational and service needs. II. DEFINITIONS
Fund Balance: difference between the assets and liabilities in a governmental fund Unrestricted Fund Balance: amount of fund balance that a local government has placed constraints on its use (committed and assigned) and fund balance that does not have any specific purpose identified for the use of those net resources (unassigned)
II.III. POLICY STATEMENT It is the policy of Alliance Behavioral Healthcare to have the Finance Committee of the Area Board review the fund balance annually. Fund balance designations shall be appropriated at year end while adhering to G.S. 159-8 (a). The Local Government Commission recommends that the fund balance available (unrestricted fund balance) be an amount not less than eight percent (8%) of expenditures as presented in the most recent audited financial statements which should approximate expenditures for one month. Due to Alliance Behavioral Healthcare’s specific circumstances the target level of fund balance available (unrestricted fund balance) that the Organization strives to maintain is an amount not less than 1% of expenditures as presented in the most recent audited financial statements while working towards a target goal of 8%. The minimum level will be re-evaluated annually until 8% has been met. III.IV. PROCEDURES
TITLE: Fund Balance BOARD POLICY #: BO-9 LINES OF BUSINESS: Finance RESPONSIBILITY: Area Board, Area Director REFERENCE(S): G.S. 159-8 (a), DHHS DMA Contract URAC STANDARDS: CORE, v. 3.0, Standard 4 APPROVAL DATE: 9/6/2012 LATEST REVISION DATE: 9/3/2015
LATEST REVIEW DATE: 12/1/2016

TITLE: Fund Balance
LATEST REVISION DATE: 1/13/2015
PAGE: 2 of 2
The Area Director shall develop procedures to implement this policy.

AREA BOARD POLICIES & PROCEDURES
I. PURPOSE Alliance Behavioral Healthcare is a political subdivision of the State of North Carolina that is subject to Article 3 of N.C.G.S. Chapter 159, the Local Government Budget and Fiscal Control Act. N.C.G.S. §159-9 requires the governing board to appoint a budget officer to serve at the will of the governing board. The Alliance Board has appointed the Chief Financial Officer as the Budget Officer. N.C.G.S. §159-15 allows the governing board to authorize the Budget Officer to transfer moneys from one appropriation to another within the same fund subject to such limitations and procedures as it may prescribe. The purpose of this Board Policy is to define the authority level at which the Chief Financial Officer as the board appointed Budget Officer, can transfer moneys within and between appropriations. II. POLICY STATEMENT The Annual Operating Budget for Alliance Behavioral Healthcare is supported by Federal and State Medicaid Funds, State Funds, Federal and Other Grant Funds and County funds. Throughout the fiscal year it may be necessary from time to time to transfer moneys between and within the funding sources (or “appropriations”) to maximize the most appropriate use of funding for services. It is the policy of Alliance Behavioral Healthcare to authorize the Chief Financial Officer, as the board appointed Budget Officer to transfer moneys as outlined below: Transfers of $25,000 or less between appropriations may be made by the Budget Officer without
prior approval. Subject to the prior written approval from the Chief Executive OfficerArea Director, transfers
between appropriations of $ 25,001 - $100,000 per transaction, may be made if allowed by the funding source subject to a report to the Board Finance Committee at its next scheduled meeting. The report to the finance committee shall contain the reason and justification for the transfer. Consistent with N.C.G.S. §159-15, the Finance Committee will report these transfers to the Board at its next regular meeting for information and entry into the minutes.
Transfers within an appropriation up to $100,000 cumulatively for the fiscal year may be made subject to a year-end report to the Finance Committee. This year-end report will be provided to the Board at its next regular meeting for information and entry into the minutes.
TITLE: Budget Transfers BOARD POLICY #: LINES OF BUSINESS: Business Operations; Finance RESPONSIBILITY: Area Board; Area Director REFERENCE(S): URAC STANDARDS: APPROVAL DATE: LATEST REVISION DATE:
LATEST REVIEW DATE:

TITLE: Budget Transfers
LATEST REVISION DATE: 1/13/2015
PAGE: 2 of 2
Amounts exceeding the limits above shall require Board approval. A request to transfer money in excess of the Budget Officer’s authority shall be brought to the Finance Committee first for prior consideration/recommendation. The Finance Committee shall report its recommendation to the Board at the next regular meeting for final approval or denial. The Board action shall be recorded in the minutes. Funds allocated by the State for programs or services in a specific county may not be transferred between counties without the approval of the finance committee and the Board and/or direction from the State. Notwithstanding the foregoing, the Year-end adjustments made in the year end close process (August of the following fiscal year) may be made without prior approval and reported to the Finance Committee and the Board at the next meeting after the year-end financial statements have been completed. The transfer of county appropriations between counties is prohibited.
III. PROCEDURES The Chief Executive OfficerArea Director shall develop procedures to implement this policy.

(Back to agenda)
ITEM: Draft Minutes from the May 4, 2017, Board Meeting DATE OF BOARD MEETING: June 1, 2017 REQUEST FOR BOARD ACTION: Approve the draft minutes from the May 4, 2017, meeting.
CEO RECOMMENDATION: Approve the minutes. RESOURCE PERSON(S): Robert Robinson, CEO; Veronica Ingram, Executive Assistant
A.
Alliance Behavioral Healthcare BOARD OF DIRECTORS
Agenda Action Form
7A

Thursday, May 04, 2017 AREA BOARD REGULAR MEETING 4600 Emperor Boulevard, Durham, NC, 27703 4:00-6:00 p.m.
Page 1 of 4
MEMBERS PRESENT: ☒Cynthia Binanay, Vice-Chair, ☐Michael Boose, ☒Christopher Bostock, Chair, ☒Heidi Carter, ☒George Corvin, MD, ☒James Edgerton, ☒Lodies Gloston (via phone), ☐Phillip Golden, ☒John Griffin, Ed.D (via phone), ☒Curtis Massey, ☒George Quick, ☒William Stanford, Jr., ☐Amelia Thorpe, ☒Lascel Webley, Jr. (via phone), and ☒McKinley Wooten, Jr.
GUEST(S) PRESENT: Marilyn Avila, candidate for vacant Board seat; Caroline Bradstock, CFAC Chair (via phone); Denise Foreman, Wake County Manager’s Office; Yvonne French, NC DMH/DD/SAS; Mary Hutchings, Wake County Finance Department; and Brian Perkins, Government Relations and Strategic Advisor to Alliance ALLIANCE STAFF PRESENT: Damali Alston, Director of Network Evaluation; Hank Debnam, Cumberland Site Director/Veterans Point of Contact; Kelly Goodfellow, Executive Vice-President/Chief Financial Officer; Amanda Graham, Senior Vice-President/Organizational Development; Carol Hammett, General Counsel; Tina Howard, Quality Review Manager; Veronica Ingram, Executive Assistant; Wes Knepper, Quality Management Director (interim); Geyer Longenecker, Quality Management Director; Robert Robinson, Chief Executive Officer, and Sara Wilson, Government Relations Director 1. CALL TO ORDER: Chairman Christopher Bostock called the meeting to order at 4:01 p.m.
AGENDA ITEMS: DISCUSSION: 2. Oath of Office Chairman Bostock mentioned that the oath of office will not occur at this meeting. 3. Announcements A. LISTENING SESSIONS: Mr. Robinson mentioned that the department would like feedback on Medicaid Reform and the
1115c waiver. They are requesting input via listening sessions. Providers, LME-MCOs, consumers, and other stakeholders are invited to attend. The local listening session is May 11, 2017, from 5:00-7:00 pm at Creedmoor Baptist Church on Creedmoor Road in Raleigh.
B. RESUME/CVS: Mr. Robinson mentioned that Alliance is reviewing files and requesting updated resumes/CVs for all Board members. Board members may forward resume/CVs to Ms. Ingram.
C. ANNUAL BOARD SURVEY: Each year the Quality Management Committee sends a survey to Board members. This is an opportunity for Board members to provide input and assess the level of functioning of the Board and all Board Committees. Chairman Bostock reminded Board members that the survey was sent last week. Tina Howard, Quality Review Manager, provided hard copies. Dr. Corvin, Quality Management Committee Chair, advised the Board that the goal is 100% participation by Friday, May 26.
D. BOARD/STAFF UPDATES: Chairman Bostock informed the Board of Caroline Sullivan’s resignation due to a conflict of interest based on a new job at the governor’s office. He and Mr. Robinson shared Ms. Sullivan’s gratitude for Board members and staff, and the work Alliance does in our community.
Thursday, May 04, 2017 AREA BOARD REGULAR MEETING 4600 Emperor Boulevard, Durham, NC, 27703 4:00-6:00 p.m.
Page 2 of 4
AGENDA ITEMS: DISCUSSION: Mr. Robinson also mentioned that Geyer Longenecker is leaving Alliance and Wes Knepper is replacing him as Director of Quality Management.
4. Agenda Adjustments There were no adjustments to the agenda. 5. Public Comment There were no public comments. 6. Committee Reports A. CONSUMER AND FAMILY ADVISORY COMMITTEE – page 3
The Alliance Consumer and Family Advisory Committee (CFAC) is composed of consumers and/or family members from Durham, Wake, or Cumberland counties who receive mental health, intellectual/developmental disabilities or substance use/addiction services. This month’s report included draft minutes from the April CFAC meeting. Caroline Bradstock, CFAC Chair, presented the report. Ms. Bradstock provided highlights from the previous CFAC meeting. The CFAC report is attached to and made part of these minutes.
B. FINANCE COMMITTEE – page 212
The Finance Committee’s function is to review financial statements and recommend policies/practices on fiscal matters to the Area Board. This month’s report included draft minutes from the February and March Committee meetings. James Edgerton, Committee Chair, presented the report. Mr. Edgerton mentioned that revenue exceeded expenditures and all State mandated ratios were met. He mentioned today’s Committee meeting included the budget presentation which will be presented to the Board. The Finance Committee report is attached to and made part of these minutes.
BOARD ACTION The Board accepted the reports; no additional action required.
7. Consent Agenda A. Draft Minutes from April 6, 2017, Board Meeting – page 221 B. Executive Committee Report – page 226 C. Human Rights Committee Report – page 229
The consent agenda was sent as part of the Board packet. There were no comments or discussion about the consent agenda. BOARD ACTION A motion was made by Mr. William Stanford to approve the consent agenda; seconded by Dr. George Corvin. Motion passed unanimously.

Thursday, May 04, 2017 AREA BOARD REGULAR MEETING 4600 Emperor Boulevard, Durham, NC, 27703 4:00-6:00 p.m.
Page 3 of 4
AGENDA ITEMS: DISCUSSION: 8. Review of Board
Officer Selection Process – page 250
As stated in the by-laws officers of the Area Board shall be chosen for a one-year term at the final meeting of the fiscal year. All members are eligible to serve for up to two consecutive terms for each office. Chairman Bostock reviewed the process for determining Board officers: Board members interested in either the Chair or Vice-Chair position may contact him before June. Nominations will be made at the June meeting. Once all nominations are presented, the Board will vote to select FY18 officers. Terms of Board officers are concurrent with Alliance’s fiscal year. BOARD ACTION The Board accepted the report; no additional action required.
9. FY18 Recommended Budget – page 251
Kelly Goodfellow, Executive Vice-President/CFO, presented an overview of the FY 2017-2018 recommended budget. Board members discussed the advantages and challenges of determining a basic benefit package for State funded services. Chairman Bostock reminded Board members that the Board will hold a public hearing and vote on the budget at the June meeting. The budget presentation is attached to and made part of these minutes. BOARD ACTION The Board reviewed the recommended budget; no additional action required.
10. Updates – page 285 A. SINGLE STREAM FUNDING CUTS: NC Senate proposed substantial cuts for MH/SA/IDD services in their proposed budget. Ms. Goodfellow reviewed the potential impact on single stream funding if additional reductions are made. Board members discussed the pending impact of these potential cuts and possible next steps.
B. NC LEGISLATION: Brian Perkins, Government Relations and Strategic Advisor to Alliance, and Sara Wilson, Director of Government Relations, presented an overview of House Bill 403: LME/MCO Claims Reporting/Mental Health Amendments. The bill can be found at http://www.ncleg.net/Applications/BillLookUp/LoadBillDocument.aspx?SessionCode=2017&DocNum=2229&SeqNum=0.
BOARD ACTION The Board accepted the report; no additional action required.
11. Chairman’s Report There was no report.

Thursday, May 04, 2017 AREA BOARD REGULAR MEETING 4600 Emperor Boulevard, Durham, NC, 27703 4:00-6:00 p.m.
Page 4 of 4
AGENDA ITEMS: DISCUSSION: 12. Closed Sessions BOARD ACTION
A motion was made by Vice-Chair Cynthia Binanay to enter closed session pursuant to NC General Statute 143-318.11 (a) (6) and NCGS 143-318.11 (1) to consider the qualifications, competence, and performance of an employee and to prevent the disclosure of information that is confidential and not a public record under NCGS 122C-126.1; motion was seconded by Dr. George Corvin. Motion passed unanimously. The Board returned to open session.
13. Adjournment With all business being completed the meeting adjourned at 6:51 p.m.
Next Board Meeting Thursday, June 01, 2017
4:00 – 6:00 Robert Robinson, Chief Executive Officer Date Approved

(Back to agenda)
ITEM: Audit and Compliance Committee Report DATE OF BOARD MEETING: June 1, 2017 BACKGROUND: The purpose of the Audit and Compliance Committee is to put forth a meaningful effort to review the adequacy of existing compliance systems and functions and to assist the Area Board in fulfilling its oversight responsibilities. This report includes notes for the November 16, 2016 meeting and minutes from the February 22, 2017 meeting and proposed revisions to the Corporate Compliance Plan, which was reviewed by the Committee on May 24, 2017. The Alliance Corporate Compliance Plan includes the following elements: 1) the designation of a compliance officer and a compliance committee that are accountable to senior management; 2) written policies, procedures, and standards of conduct that articulate the organization's commitment to comply with all applicable Federal and State standards; 3) effective training and education for the compliance officer and the organization's employees; 4) effective lines of communication between the compliance officer and the organization's employees; 5) enforcement of standards through well-publicized disciplinary guidelines; 6) provision for internal monitoring and auditing; 7) provision for prompt response to detected offenses, and for development of corrective action initiatives. The Alliance Behavioral Healthcare Area Board adopted the Corporate Compliance Plan in 2012 and has reviewed and approved it every year since then, in accordance with the Area Board Corporate Compliance Plan Policy. The Audit and Compliance Committee has reviewed the revisions to the Plan this year and is recommending approval. REQUEST FOR AREA BOARD ACTION: Accept the report and approve the Plan. CEO RECOMMENDATION: Accept the report and approve the Plan. RESOURCE PERSON(S): Lascel Webley, Committee Chair; Monica Portugal, Chief Compliance Officer
Alliance Behavioral Healthcare BOARD OF DIRECTORS
Agenda Action Form
7B

Wednesday, November 16, 2016 BOARD AUDIT AND COMPLIANCE COMMITTEE - SPECIAL MEETING 4600 Emperor Boulevard, Durham, NC 27703 4:00-6:00 p.m.
Draft minutes may be submitted with the monthly Board packet. Minutes will be approved by this Committee at a later date. Page 1 of 1
APPOINTED MEMBERS PRESENT: ☐ George Quick, M.B.A, ☐ Vicki Shore, B.A., ☒ Lascel Webley, Jr., M.B.A., M.H.A. (Committee Chair)(via telephone), ☒McKinley Wooten, Jr., J.D. (via telephone),
BOARD MEMBERS PRESENT: Christopher Bostock, Board Chair (via telephone) GUEST(S) PRESENT: None STAFF PRESENT: Monica Portugal, Chief Compliance Officer, Tarsha Brown, Senior Compliance Analyst – Internal Auditor, Ken Marsh, Medicaid Program Director.
1. WELCOME AND INTRODUCTIONS
2. REVIEW OF THE MINUTES – The minutes from the October 10, 2016, meeting were not reviewed due to no quorum; Choose an item.
AGENDA ITEMS: DISCUSSION: NEXT STEPS: TIME FRAME:
3. Internal Audits (4): Baseline, Follow Up
Ms. Brown presented scope, methodology, findings and final results from baseline and follow up audits conducted in FY16. Ms. Brown reviewed regulatory requirements and impact to the organization if non-compliance findings are identified. Committee asked questions about the sample size, operational process and results. No motion was made due to quorum.
Committee will make a decision regarding acceptance of the 4 audit reports at the next meeting.
2/22/2017
4. Quarterly Reports Members reviewed and discussed the Corporate Compliance Dashboard (FY16 Q2-Q4, FY17 Q1): network compliance, overpayments, special investigations, compliance reports, internal investigations, internal audits and monitoring, HIPAA incidents and privacy complaints.
No follow up required N/A
5. ADJOURNMENT: next meeting will be February 22, 2017, from 4:00 p.m. to 6:00 p.m.

Wednesday, February 22, 2017 BOARD AUDIT AND COMPLIANCE COMMITTEE - SPECIAL MEETING 4600 Emperor Boulevard, Durham, NC 27703 4:00-6:00 p.m.
Draft minutes may be submitted with the monthly Board packet. Minutes will be approved by this Committee at a later date. Page 1 of 2
APPOINTED MEMBERS PRESENT: ☒ George Quick, M.B.A, (phone) ☒ Lascel Webley, Jr., M.B.A., M.H.A. (Committee Chair), (phone) ☒McKinley Wooten, Jr., J.D.,
BOARD MEMBERS PRESENT: Chris Bostock (Chair, Board of Directors) GUEST(S) PRESENT: None STAFF PRESENT: Monica Portugal, Chief Compliance Officer, Ken Marsh, Medicaid Program Director.
1. WELCOME AND INTRODUCTIONS
2. REVIEW OF THE MINUTES – The minutes from the October 10, 2016, meeting and notes from the November 16, 2016, meeting were
reviewed; a motion was made by Mr. Wooten and seconded by Mr. Quick to approve the minutes and notes. Motion passed unanimously.
AGENDA ITEMS: DISCUSSION: NEXT STEPS: TIME FRAME:
3. Annual Independent Auditor Evaluation and Contract Review
Committee reviewed the independent audit firm’s recent peer review conducted through American Institute of CPAs. The peer review report, which examines the system of quality control for the accounting and auditing practice, was accepted by the National Peer Review Committee on January 12, 2017 with a passing score. Firms can receive a rating of pass, pass with deficiencies, or fail. The FY18 Contract and Scope of Work between Alliance and the audit firm was reviewed. All relationships between Alliance and the firm were disclosed. Mr. Quick reported that Durham and Wake use the same firm. A motion was made by Mr. Quick to accept the peer review report and to recommend to the Board that the firm be retained. The motion was seconded by Mr. Wooten. Motion passed.
Mr. Webley Jr. will sign the audit firm contract at the upcoming Board Meeting.
3/2/2017
4. Annual Risk Assessment
Committee reviewed the proposed methodology for the annual risk assessment, which included a risk assessment of Alliance’s vulnerabilities to fraud. Mr. Quick suggested a change to the Financial risk scores from percentage of risk reserve to dollar amounts of total annual budget. He suggested a review of historical losses to inform the scoring. A motion was made by Mr. Quick to accept the proposed methodology for the FY18 risk assessment. Mr. Wooten seconded and the motion passed.
Ms. Portugal will implement the annual risk assessment and will work with Finance to update the financial scores.
6/30/2017

Wednesday, February 22, 2017 BOARD AUDIT AND COMPLIANCE COMMITTEE - SPECIAL MEETING 4600 Emperor Boulevard, Durham, NC 27703 4:00-6:00 p.m.
Draft minutes may be submitted with the monthly Board packet. Minutes will be approved by this Committee at a later date. Page 2 of 2
AGENDA ITEMS: DISCUSSION: NEXT STEPS: TIME FRAME:
5. Records Retention and Destruction
A summary of records that have been destroyed were reviewed. Administrative and medical records from the Cumberland LME have been reviewed for retention. Records that met retention were destroyed and records that did not meet retention were either logged, scanned and destroyed or stored. Destruction of records is completed in accordance with State Policy and the Department of Cultural Resources retention schedule. 24,482 medical records and 4,393 administrative documents were destroyed. 1,460 boxes of medical and administrative records were scanned and 341 boxes sent to storage, whereof some records are permanent. In accordance with applicable policies, Alliance obtained certificates of destruction and reports destruction to the Board of Directors.
N/A N/A
6. Quarterly Reports Committee reviewed the quarterly Compliance dashboard for the first two quarters of FY17.
No follow up required N/A
7. Updates
Internal Auditor: Ms. Portugal shared that the Internal Auditor position has been filled by an internal candidate with a background in Special Investigations, Program Integrity, and Medicaid services. The Auditor is a Certified Fraud Examiner and a licensed clinician. Recovery of Outstanding Overpayments: Alliance will issue judgments to providers leaving the Network with an outstanding debt. Finance, Legal and Compliance are developing criteria and other details to inform the process. EQR: Mr. Marsh provided an update regarding the upcoming External Quality Review.
N/A N/A
8. ADJOURNMENT: next meeting will be May 24, 2017, from 4:00 p.m. to 6:00 p.m.

Corporate Compliance Plan
FY178
Adopted by the Area Board: October 4th, 2012 Reviewed and Approved by the Area Board: June 11, 2013 Reviewed and Approved by the Area Board: June 5, 2014 Reviewed and Approved by the Area Board: June 4, 2015 Reviewed and Approved by the Area Board: June 2, 2016
Alliance Behavioral Healthcare Corporate Compliance Plan, Adopted October 2012, Rev. June 2016
2
Table of Contents
I. Introduction and Statement of Purpose………………………………………………………………..3
II. Compliance Infrastructure ……..…………………………………………………………………………….5 A. Chief Compliance Officer B. Board Audit and Compliance Committee C. Corporate Compliance Committee
III. Policy Guidelines and Standards of Conduct……………………......................................8
IV. Effective Education and Training…………………………………………………..………………………8
V. Effective Lines of Communication…………………….…………………………………..…………..….9 A. Reporting Compliance Issues B. Investigating Compliance Issues
VI. Enforcement of Standards and Disciplinary Guidelines…….…………………………………11
VII. Internal Auditing and Monitoring………………………….……………………………………………11
VIII. Response and Remediation……………………………………….……………………………………….12
IX. Effectiveness of the Compliance Program.……………………..…………………………………..13
A. Annual Compliance Report B. Annual Risk Assessment and Compliance Work Plan C. Revisions to the Compliance Plan
Appendix A – Federal Criminal and Civil Statutes Related to Fraud and Abuse in the Context of Health care…………………………..……………………………………………………………15
Criminal Statutes Civil and Administrative Statutes
References…………………………………………………….……………………………………………………16

Alliance Behavioral Healthcare Corporate Compliance Plan, Adopted October 2012, Rev. June 2016
3
CORPORATE COMPLIANCE PLAN ________________________________________________________________________ I. Introduction and Statement of Purpose It is the policy of Alliance Behavioral Healthcare to follow ethical standards of business practice established by Alliance Behavioral Healthcare’s Area Board and Management Team, by oversight agencies, and state and federal law. Alliance Behavioral Healthcare has an ongoing commitment to ensure that its affairs are conducted in accordance with applicable law and sound ethical business practice. Alliance Area Board, employees, and provider network are fully informed of applicable laws and regulations to which Alliance Behavioral Healthcare is obligated so that they do not inadvertently engage in conduct that may raise compliance issues. Alliance Behavioral Healthcare recognizes that its business relationships with contracted providers and vendors, Medicaid enrollees, and recipients of behavioral healthcare services are subject to legal requirements and accountability standards. To further its commitment to compliance and to protect its employees and contracted providers, Alliance Behavioral Healthcare places emphasis on its Compliance Plan to address regulatory issues likely to be of most consequences to Alliance operations. The Compliance Plan establishes the following framework for corporate compliance by Alliance Area Board, employees and providers:
A. Designation of a Chief Compliance Officer and Corporate Compliance Committee charged with directing the effort to enhance compliance and implement the Compliance Plan;
B. Incorporation of standards, policies, and administrative guidelines directing Alliance
Behavioral Healthcare personnel and others involved with operational practices;
C. Prevention and identification of criminal and unethical conduct and legal issues that may apply to business relationships and methods of conducting business;
D. Effective education and training for the Chief Compliance Officer, Area Board, and
employees addressing obligations for adherence to applicable compliance requirements;
E. Development and implementation of informational materials and training for employees, subcontractors, providers, and enrollees addressing obligations for adherence to applicable compliance requirements and information to prevent dishonest behavior which results in fraud, waste of public funding, and program abuse;
F. Implementation of mechanism for employees to raise questions and receive
appropriate guidance concerning regulatory and operational compliance issues;

Alliance Behavioral Healthcare Corporate Compliance Plan, Adopted October 2012, Rev. June 2016
4
G. Development and implementation of an ongoing monitoring and auditing process identifying potential risk areas and operational issues requiring remediation;
H. Development and implementation of a process for employees, subcontractors,
providers and recipients to report possible compliance issues, such as legal and ethical violations, or to report fraud, waste, and abuse, including a process for such reports to be fully and independently reviewed;
I. Enforcement of standards through documented disciplinary guidelines, policies and
training addressing expectations and consequences;
J. Formulation of plans for corrective action or remediation plans to address identified areas of noncompliance;
K. Evaluation of the effectiveness of the overall compliance efforts of Alliance Behavioral
Healthcare to ensure that operational practices reflect current compliance requirements and address strategic goals to improve Alliance Behavioral Healthcare operations.
This Compliance Plan is not intended to set forth all of the substantive programs and practices of Alliance Behavioral Healthcare that are designed to achieve compliance and integrity. In addition to this Plan, Alliance Behavioral Healthcare has developed and implemented a variety of monitoring processes for providers. The compliance practices included in those efforts will be coordinated with this Plan to direct Alliance’s overall compliance efforts. It is intended that the scope of all compliance activities promotes integrity, ensures objectivity, fosters trust and supports the stated values of Alliance Behavioral Healthcare.

Alliance Behavioral Healthcare Corporate Compliance Plan, Adopted October 2012, Rev. June 2016
5
II. Compliance Infrastructure Figure 1: Compliance Responsibility Organizational Chart
A. Chief Compliance Officer (CCO) The Chief Compliance Officer has been delegated day-to-day operational responsibility for the Alliance Behavioral Healthcare compliance program. The CCO will report compliance efforts and identified issues directly to the Chief Executive Officer (CEO) who has overall responsibility to ensure that Alliance has an effective compliance program. The CCO will report directly as necessary and required to the Area Board. The Alliance Area Board is accountable for governing Alliance Behavioral Healthcare as a knowledgeable body regarding the scope and operations of the compliance program, including expectations, practices, identified risk issues and compliance remediation. The Chief Compliance Officer is responsible for the following activities:
1. Formulate, review, and revise policies and procedures to guide all activities and functions of Alliance Behavioral Healthcare that involve issues of compliance, with assistance from the Compliance Committee;
2. Ensure processes for compliance integrate with and support Alliance Behavioral
Healthcare quality management and provider network monitoring processes; 3. Develop, in conjunction with the Compliance Committee and other relevant parties, the
Code of Ethics and Conduct for Alliance employees and providers; 4. Develop, in conjunction with the Compliance Committee and other relevant parties,
methods to ensure that employees and providers are aware of Alliance Behavioral Healthcare’s Code of Ethics and Conduct and understand the importance of compliance;

Alliance Behavioral Healthcare Corporate Compliance Plan, Adopted October 2012, Rev. June 2016
6
5. Develop and deliver, in conjunction with the Compliance Committee educational and
training programs; 6. Receive, review, and investigate instances of suspected internal and external
compliance issues, communicate findings and develop action plans with the program suspected of noncompliance and as appropriate with the assistance of the Compliance Committee;
7. Supervise Oversee a program integrity activities, such as claims audits, Special Investigations Unit to conduct fraud and abuse detection activities including data mining, pre-investigations, and full data analytics, and special investigations to detect and resolve instances of provider and enrollee fraud and abuse;
8. Refer to Division of Medical Assistance (DMA) Office of Compliance and Program Integrity Behavioral Health Section suspected cases of fraud for determination of credible allegation;
9. Prepare annual compliance summary for evaluation by the Corporate Compliance
Committee and Board Audit and Compliance Committee, as set forth in this Plan; 10. Conduct an annual risk assessment, as set forth in this Plan, with the Corporate
Compliance Committee and the Board Audit and Compliance Committee; 11. Prepare the annual compliance work plan, as set forth in this Plan, with the Corporate
Compliance Committee and the Board Audit and Compliance Committee; 12. Prepare revisions to Alliance Behavioral Healthcare Compliance Plan together with the
Corporate Compliance Committee and Board Audit and Compliance Committee, as set forth in this plan;
13. Report to and assist the Board of Directors through its Audit and Compliance Committee
to fulfill its oversight responsibilities; and
14. Provide other assistance with initiatives regarding compliance as directed by the CEO and/or Board of Directors.
B. Board Audit and Compliance Committee (ACC) The purpose of the Audit and Compliance Committee (ACC) is to put forth a meaningful effort to review the adequacy of existing compliance systems and functions. To assist the Board of Directors in fulfilling its oversight responsibilities for:
1. The integrity of the organization’s annual financial statements;

Alliance Behavioral Healthcare Corporate Compliance Plan, Adopted October 2012, Rev. June 2016
7
2. The system of risk assessment and internal controls;
3. The organization’s compliance with legal and regulatory requirements;
4. The independent auditor's qualifications and independence;
5. The performance of the organization’s internal audit function; and
6. To provide an avenue of communication between management, the independent auditors, and the Board of Directors.
C. Corporate Compliance Committee (CCC) To assist the Chief Compliance Officer (CCO) with the development and implementation of compliance efforts, a Corporate Compliance Committee has been formed representative of the clinical and administrative services of Alliance Behavioral Healthcare. The CCO will serve as the chair of the Committee and does not vote on any matters, unless the vote is required to break a tie. Committee members will serve one-year terms with no limitations on the number of terms to serve. The make-up of the committee will be re-evaluated at the end of each fiscal year. For the sake of maintaining the integrity of the Committee no more than 50% of committee members may resign from the Committee in the same year. New members will be nominated by their Department Head and will be selected by majority vote by the current Committee. The CCO must be consulted on the selection of membership. The role of the CCC is to advise the CCO, to assist in the implementation of the compliance program, and to evaluate the effectiveness of Compliance efforts. The Committee’s responsibilities include:
1. Analyzing the organization’s regulatory obligations; 2. Working with employees and providers to develop standards of conduct and policies
and procedures that promote compliance; 3. Developing and monitoring internal systems and controls to carry out Alliance
Behavioral Healthcare standards, policies and procedures as part of Alliance Behavioral Healthcare’s daily operations;
4. Determining the appropriate strategy and approach to promote compliance and
detection of potential risk areas through various reporting mechanisms;
5. Determining methodology to conduct the annual risk assessment, overseeing the process and determining the levels of risk as part of formulating the annual Compliance Work Plan;

Alliance Behavioral Healthcare Corporate Compliance Plan, Adopted October 2012, Rev. June 2016
8
6. Overseeing the implementation of the annual Compliance Work Plan in order to evaluate the effectiveness of compliance efforts;
7. Assisting, as appropriate, with the development of preventive and remediation plans;
8. Review Provider compliance violations and oversee enforcement of disciplinary guidelines, including making determinations regarding the approval of corrective actions and other sanctions as appropriate and per Alliance policies and procedures;
9. Developing a system to solicit, evaluate and respond to compliance issues, grievances,
and other problems; 10. Monitoring findings of internal and external reviews for the purpose of identifying risk
areas or deficiencies requiring further monitoring or preventive and corrective action; and
11. Reviewing and analyzing trends such as results from exclusions checks, internal and
external monitoring and auditing efforts, fraud, waste and abuse investigations, billing audits, enforcement actions, and final disposition.
III. Policy Guidelines and Standards of Conduct Alliance Behavioral Healthcare has adopted policies and procedures specific to Alliance Behavioral Healthcare’s operational practices. These policies and procedures are reviewed at least annually and revisions are made, as necessary. The policies and procedures specific to Alliance Behavioral Healthcare’s compliance efforts are intended to support and further define the operational practices and responsibilities and, when possible, are integrated within existing policies and procedures. Alliance Behavioral Healthcare has also adopted an Employee Code of Ethics and Conduct to guide all business activity. This code reflects a common sense approach to ensuring legal and ethical behavior. All new employees receive training and provide acknowledgement of receipt of the Alliance Code of Ethics and Conduct. As a condition of employment the Code of Ethics and Conduct is reviewed and acknowledged annually thereafter. It is the intent of Alliance Behavioral Healthcare to adopt and implement a Code of Ethics specific to the Alliance Provider Network. The Network Provider Code of Ethics will guide business activities of Providers who contract with Alliance. IV. Effective Education and Training It is essential to the Alliance Compliance Program to ensure that the Chief Compliance Officer receives effective training and education on an ongoing basis. The CCO shall seek out
Alliance Behavioral Healthcare Corporate Compliance Plan, Adopted October 2012, Rev. June 2016
9
opportunities to receive Continuous Education Credits in order to maintain Compliance Certification and to enhance job related skills. The CCO and CCC are responsible for ensuring Alliance Behavioral Healthcare policies regarding compliance are disseminated and understood by employees. To accomplish this objective, the CCO will assist with the development of a systematic and ongoing training program that enhances and maintains awareness of Alliance Behavioral Healthcare policies. Training materials directed to clinical, administrative or other regulatory compliance issues will be submitted to the CCO for review with the CCC.
Upon hire and annually thereafter, all Alliance employees will participate in compliance training whereby a system is in place to document that such training has occurred. Employees will be required to take a post-test in order to measure the effectiveness of training efforts. Training materials will identify Alliance Behavioral Healthcare’s CCO as available to respond to questions specific to compliance training or regulatory issues. Employees are made aware of their compliance obligations as a condition of employment. Adherence to policies will be addressed within the New Employee Orientation and ongoing training programs, and employee job descriptions. Employees will be expected to demonstrate a sufficient level of understanding as a result of compliance training. If a particular compliance or risk issue develops, the CCO and/or CCC may recommend that identified persons attend training addressing the risk issue. The CCO and CCC will develop compliance training opportunities for Providers in the Alliance Network. Such training may include an overview of Alliance policies and procedures, Provider Network Code of Ethics and Conduct, Compliance Program requirements, and healthcare fraud, waste, and abuse. To ensure compliance throughout the Alliance Network, the CCO and CCC will develop and offer training to Enrollees. Such training may include Client Rights and healthcare fraud, waste, and abuse. V. Effective Lines of Communication A. Reporting Compliance Issues In keeping with Alliance policies, all employees are required to report promptly all known or suspected violations of an applicable law or regulation, the Code of Ethics and Conduct, breach of privacy or security or any Alliance policies to their supervisor, the Chief Compliance Officer (CCO), or the confidential Compliance Line. As a general practice, employees are directed to address questions about operational issues to persons having supervisory responsibility of that function. Supervisors are responsible for ensuring that issues or violations of which they are aware are immediately reported to the CCO.

Alliance Behavioral Healthcare Corporate Compliance Plan, Adopted October 2012, Rev. June 2016
10
As another reporting option, training materials will inform employees that they may report directly to the Alliance CCO or to a confidential third party 24 hour Hotline, Compliance Line. The training materials will provide a contact method(s) to address compliance issues to the CCO and to the Compliance Line. The CCO will use various communication methods, including electronic, web based and telephonic communication methods, to ensure timely communication of the elements of this compliance program. The various communication methods will be available 24 hours a day. The intent of publicizing various methods of communication is to ensure both convenience and confidentiality for employees and enable immediate response to submitted issues. All reports will be investigated unless the information provided contains insufficient information to permit a meaningful investigation. Failing to report violations may result in disciplinary action. Employees reporting in good faith possible compliance issues will not be subjected to retaliation or harassment as a result of the report. Concerns about possible retaliation or harassment should be reported to the CCO or the CEO. The Compliance Program will also include a confidential third party 24 hour Fraud and Abuse Line, as a means to offer providers, enrollees, or other persons in the community an opportunity to report suspected fraud, waste of program funding, or abuse of services anonymously. The Fraud and Abuse Line will be advertised on the Alliance website, in Consumer Handbooks, Provider Manual, and other informational and training materials. The Alliance Access and Information line is another option for placing reports of this nature. Reported compliance concerns related to Providers will be logged in the Alliance Behavioral Healthcare grievance database. Concerns regarding fraud, waste, and abuse will be tracked in a separate compliance software by the CCO and/or Special Investigations Unit. Compliance concerns related to Alliance employees will be treated as a confidential document whereby access will be limited to the CCO and designated Compliance employee/s as requested by the reporter and as allowed by law. Internal compliance matters will be tracked using a confidential compliance software available to the CCO and designated Compliance employee/s. B. Investigating Compliance Issues When conduct is reported that is determined to be inconsistent with regulations, rules or laws or Alliance Behavioral Healthcare policy, the CCO will determine the level of potential risk and respond accordingly. If this preliminary review indicates that a problem may exist, the CCO will promptly report the risk issue to the CEO and inquiry into the matter will be undertaken. This inquiry may include appropriate assistance from Legal Counsel. Alliance employees and providers will be expected to cooperate fully with any inquires undertaken. The CCO shall report any compliance issues that may result in negative publicity and risk to Alliance Behavioral Healthcare to the Area Board. Responsibility for conducting the investigation will be decided on a case-by-case basis by the CCO. The CCO will delegate investigations of suspected provider or recipient abuse or fraud to the Director of Program Integrity and Special Investigations Unit. The findings will be reviewed

Alliance Behavioral Healthcare Corporate Compliance Plan, Adopted October 2012, Rev. June 2016
11
by the CCO to ensure consistency in the investigative process. All investigations will be documented in a confidential compliance software. Suspected cases of provider or enrollee fraud will be referred to DMA Program Integrity Behavioral Health Section for determination of credible allegation of fraud. Alliance will cooperate with DMA and/or the Department of Justice Medicaid Investigations Division on all fraud investigations. When the compliance issue concerns an Alliance employee, the investigative process will adhere to Alliance policies and procedures regarding internal investigations and applicable Human Resources policies. To the extent practical and appropriate, efforts will be made to maintain the confidentiality of such inquires and the information gathered. Consequences for conduct inconsistent with Alliance Behavioral Healthcare’s policy will be addressed according to the provisions identified in the applicable policies. VI. Enforcement of Standards and Disciplinary Guidelines Compliance standards will be consistently enforced through appropriate disciplinary actions, up to and including termination of employment. For providers in the Alliance Network compliance with standards will be enforced through sanctions up to and including termination of contract. The following guidelines will be used. Discipline must be:
1. documented and well-publicized; 2. consistent; 3. dependent on the severity of the violation; 4. enforced for those who commit a violation; and 5. enforced for those who fail to report a known violation
The CCO and CCC, in collaboration with Human Resources, will develop policies and procedures to guide disciplinary actions. CCC will ensure that such policies and procedures are made available to employees and providers through electronic means as well as incorporated into manuals and training materials. Disciplinary procedures will be approved by the CEO. The CCO will monitor to ensure consistent implementation of disciplinary guidelines.
VII. Internal Auditing and Monitoring Audits and monitoring are preventative and detective compliance measures which assist Alliance Behavioral Healthcare in identifying and acting on real or potential issues before they become larger compliance risks. Audits are objective and independent planned activities determined by the annual risk assessment and included in the annual compliance work plan. Monitoring is a subjective, detective control done as a self-review within a Department or by the Office of Compliance Department. Monitoring may be planned and part of the annual compliance work plan or may be conducted as a reaction to concerning trends identified as part of the Continuous Quality Improvement process, or based on concerns from within a Department, etc.

Alliance Behavioral Healthcare Corporate Compliance Plan, Adopted October 2012, Rev. June 2016
12
Internal audits and monitoring will be completed using tools as appropriate and will be documented in the Compliance Audit or Monitoring Report. At a minimum, the following components will be included in all audits and monitoring:
1. Sample selection 2. Data review and collection 3. Data analysis; and 4. Reporting
Techniques may vary depending on the nature of the area reviewed and may be a combination of two or more of the following:
1. On-site visits; 2. Unannounced mock audits; 3. Interviews; 4. Questionnaires; 5. Trend analysis; 6. Review and tracking of work flow and processes; 7. Reviews of written materials and documentation prepared by the different
departments; and 8. Other
The CEO delegates authority to the CCO to seek consultation with legal counsel when expert review is necessary to analyze the risk issue. If a review identifies risk issues for Alliance Behavioral Healthcare, the CCO will report the facts to the CEO. In consultation with legal counsel, as appropriate, the CCO will review the situation to determine whether there appears to have been activity inconsistent with federal and state rules and regulations, Alliance policies, procedures or the Code of Ethics and Conduct.
In addition to internal audits and monitoring, the Network Operations Department will conduct ongoing provider monitoring and billing audits according to Alliance Behavioral Healthcare’s policies and procedures on provider monitoring. Results of these reviews will be communicated to the CCC by the Provider Network Evaluators and/or Quality Management Department. All audit and monitoring activities will be reviewed by the CCC, CEO and ACC and summarized for Alliance Behavioral Healthcare Area Board, including sufficient information to evaluate the appropriateness of responses to identified violations of Alliance’s policies and Federal or State laws. VIII. Response and Remediation When an internal compliance issue has been identified through an audit or monitoring activity, the CCO will ensure the issue is reported to the CEO and will facilitate the process to develop corrective action initiatives or to enforce standards through disciplinary actions promptly as required by policies and law.

Alliance Behavioral Healthcare Corporate Compliance Plan, Adopted October 2012, Rev. June 2016
13
As appropriate, the CCO will develop a remediation plan. Plans may include: 1. additional or modified training and education; 2. corrective action; 3. development of new policies and procedures; 4. revision to existing policies and procedures; 5. revision to the Compliance Plan; 6. additional monitoring and auditing; or 7. reporting to outside agencies
The CCO must be involved in the development of all remediation plans that: 1. result from a significant compliance violation; 2. affect multiple departments; or 3. involve revisions or additions to the Compliance Plan or policies and procedures.
Reporting a compliance violation to an outside agency must be coordinated through the CCO prior to reporting. The Corporate Compliance DepartmentOffice of Compliance monitors settlement of issues reported to outside authorities.
Remediation plans, including any reporting to an external agency, should be attached to the investigative documentation in the confidential compliance software, or to the Compliance Audit/Monitoring Report. Remediation plans that require further monitoring are considered “open” and are not resolved and closed until the monitoring period is successfully completed. In accordance with Alliance’s policies and procedures, providers who have engaged in legal or ethical misconduct will be subject to consideration of penalties, sanctions, termination of contract for services and/or excluded from providing local, state, grant, and/or Medicaid funded services in the Alliance Provider Network, and/or other sanctions and penalties as required by law or state policy. All providers’ corrective action plans will be maintained electronically and will be used as historical reference tools whereby identified issues may be included in Alliance Behavioral Healthcare’s provider profiling and review processes. IX. Effectiveness of the Compliance Program A. Annual Compliance Report The Chief Compliance Officer (CCO) will ensure a review of Alliance Behavioral Healthcare’s status with current compliance and regulatory operations. The purpose of the review is to ascertain whether the compliance operations of Alliance Behavioral Healthcare are of sufficient scope and within substantial compliance with Alliance’s policy and regulatory requirements. The results of the self-assessment process along with a report of compliance efforts during the preceding year will be prepared by the CCO. With review and comments provided by the Corporate Compliance Committee (CCC) and Board Audit and Compliance Committee, the Annual Report will be presented to the Alliance Behavioral Healthcare Area Board.

Alliance Behavioral Healthcare Corporate Compliance Plan, Adopted October 2012, Rev. June 2016
14
B. Annual Risk Assessment and Compliance Work Plan Annually, the CCO and CCC will conduct a compliance risk assessment using an approved Risk Assessment tool. Risk will be identified through interviews with department heads, document reviews with input from management, results from previous audits and investigations, and review of the annual Office of Inspector General work plan, Fraud Alerts, Special Advisory Bulletins, and advice and guidance by Division of Medical Assistance. The level of risk will be assessed based on legal, reputational and financial risk to Alliance. Based on the assessment, CCC will prioritize the highest scored risk areas and will include at a minimum the top 5 to 10 areas that relate to Compliance in the annual compliance work plan. C. Revisions to the Compliance Plan This Compliance Plan is intended to be flexible and readily adaptable to changes in regulatory requirements and in the health care system as a whole. The plan will be regularly reviewed by the CCO and the CCC to assess the viability of the Plan and the inclusion of all appropriate Alliance policies and regulatory requirements. The Plan will be revised as experience demonstrates that a certain approach is not effective or suggests a better alternative. The Area Board will review and approve the Compliance Plan annually.

Alliance Behavioral Healthcare Corporate Compliance Plan, Adopted October 2012, Rev. June 2016
15
APENDIX A Federal Criminal and Civil Statutes Related to Fraud and Abuse in the Context of Health care Criminal Statutes This section contains references to criminal statutes related to fraud and abuse in the context of health care. It is not intended to be a compilation of all federal statutes related to health care fraud and abuse. It is merely a summary of some of the more frequently cited federal statutes.
Health Care Fraud (18 U.S.C. 1347) Theft of Embezzlement in Connection with Health Care (18 U.S.C. 669) False Statements Relating to Health Care Matters (18 U.S.C. 1035) Obstruction of Criminal Investigations of Health Care Offenses (18 U.S.C. 1518) Mail and Wire Fraud (18 U.S.C. 1341 and 1343) Anti-Kickback law/Criminal Penalties for Acts Involving Federal Health Care Programs
(Section 1128B of the Social Security Act/42 U.S.C. 1320a 7b) Civil and Administrative Statutes This section contains a description of civil and administrative statutes related to fraud and abuse in the context of health care. It is not intended to be a compilation of all federal statutes related to health care fraud and abuse. It is merely a summary of some of the more frequently cited federal statutes.
The False Claims Act (31 U.S.C. 3829-3733) Civil Monetary Penalties Law (Section 1128A of the Social Security Act/42 U.S.C. 1320a-
7aa) Stark/Self-Referral Law/Limitations on Certain Physician Referrals (Section 1877 of the
Social Security Act/42 U.S.C. 1395nn) Exclusion From Federal Health Care Programs (Section 1128(a), (b) and (c) of the Social
Security Act/42 U.S.C. 1320a-7a)

Alliance Behavioral Healthcare Corporate Compliance Plan, Adopted October 2012, Rev. June 2016
16
REFERENCES Bellucci, Margaret, Thornton, Mary, Corporate Compliance Manual for Behavioral Healthcare Providers, National Council for Community Behavioral Healthcare Troklus, Debbie, Warner, Greg, Compliance 101 Third Edition, Health Care Compliance Association 42 CFR § 438.608 Program Integrity Requirements. 2013 Federal Sentencing Guidelines Manual Chapter 8, Part B –Effective Compliance and Ethics Program

(Back to agenda)
ITEM: Executive Committee Report DATE OF BOARD MEETING: June 1, 2017 BACKGROUND: The Executive Committee sets the agenda for Area Board meetings and acts in lieu of the Area Board between meetings. Actions by the Executive Committee are reported to the full Area Board at the next scheduled meeting. This month’s report includes draft minutes from the May 16, 2017, meeting. REQUEST FOR AREA BOARD ACTION: Accept the report. CEO RECOMMENDATION: Accept the report. RESOURCE PERSON(S): Christopher Bostock, Board Chair; Robert Robinson, CEO
Alliance Behavioral Healthcare BOARD OF DIRECTORS
Agenda Action Form
7C

Tuesday, May 16, 2017 BOARD EXECUTIVE COMMITTEE MEETING - REGULAR MEETING 4600 Emperor Boulevard, Durham, NC 27703 4:00-6:00 p.m.
Draft minutes may be submitted with the monthly Board packet. Minutes will be approved by this Committee at a later date. Page 1 of 2
APPOINTED MEMBERS PRESENT: ☒Cynthia Binanay, Board Vice-Chair, B.S.N, M.A.; ☒Christopher Bostock, Board Chair, B.S.I.M.; ☒George Corvin, Quality Management Committee Chair, M.D.; ☒James Edgerton, Finance Committee Chair, B.S.; ☒Lodies Gloston, Human Rights Committee Chair, B.A., M.A.; ☒Curtis Massey, Policy Committee Chair, B.A., J.D. (via phone); ☒William Stanford, Previous Board Chair, B.A., J.D.; and ☐Lascel Webley, Audit and Compliance Committee Chair, B.S., M.B.A., M.H.A
BOARD MEMBERS PRESENT: None GUEST(S) PRESENT: Brian Perkins, Government Relations and Strategic Advisor to Alliance ALLIANCE STAFF PRESENT: Kelly Goodfellow, Executive Vice-President/CFO; Carol Hammett, General Counsel; Veronica Ingram, Executive Assistant; Robert Robinson, CEO; and Sara Wilson, Government Relations Director 1. WELCOME AND INTRODUCTIONS 2. REVIEW OF THE MINUTES – The minutes from the April 18, 2017, Executive Committee meeting was reviewed; a motion was made by Vice-Chair Binanay to approve the minutes; seconded by Mr. Stanford. Motion passed unanimously.
AGENDA ITEMS: DISCUSSION: NEXT STEPS: TIME FRAME:
3. Updates a) NEXT FUTURE DEVELOPMENT WORKGROUP MEETING: Chairman Bostock reminded Committee members that the next staff workgroup meeting is Tuesday, June 6 at 4:00 pm.
b) NC LEGISLATION/SINGLE STREAM FUNDING: Mr. Perkins reviewed potential State budget cuts if the General Assembly approves the Senate’s proposed budget. Additionally, he reviewed the impact on Alliance if this budget is approved.
Mr. Perkins mentioned that NAMI-Wake County (National Alliance on Mental Illness) is planning a day of advocacy and a press conference on May 17 at the NC General Assembly. The day of advocacy will use some documents provided by Alliance and reviewed during the Executive Committee meeting. Committee members discussed having Alliance staff and Executive Committee members attend the day of advocacy to answer questions related to Alliance.
c) APPLICATION FOR VACANT JOHNSTON SEAT: Chairman Bostock mentioned that this interview will occur at the June Committee meeting.
a) Committee members will contact Ms. Ingram if they need a call-in number.
b) i. Mr. Perkins and Ms. Wilson will attend the NAMI-Wake County day of advocacy.
ii. Mr. Robinson will forward information to the Directors groups and County Commissioners to inform them of the implications of the potential cuts.
c) Executive Committee will interview applicant at the June Committee meeting. Mr. Robinson will confirm if an applicant’s interim job poses a potential/perceived conflict of interest.
a) Before 6/2/17 b) 5/17/17; none
specified. c) None
specified.

Tuesday, May 16, 2017 BOARD EXECUTIVE COMMITTEE MEETING - REGULAR MEETING 4600 Emperor Boulevard, Durham, NC 27703 4:00-6:00 p.m.
Draft minutes may be submitted with the monthly Board packet. Minutes will be approved by this Committee at a later date. Page 2 of 2
AGENDA ITEMS: DISCUSSION: NEXT STEPS: TIME FRAME:
4. Vacant Board Seat
The Committee reviewed an application for the vacant seat representing Wake County. Committee agreed to continue accepting applications for this newly vacated seat.
Ms. Ingram will communicate with the applicant and inform them that they will be contacted when the Committee begins interviews.
5/17/17
5. Process for Electing FY18 Board Officers
Chairman Bostock reviewed the process for electing Board officers. He mentioned that he received inquiries about both officer positions. He also reviewed a nomination and ballot method if there are multiple people interested in each position.
Chairman Bostock will email Board members with the current nominations a week before the Board meeting.
By 5/25/17
6. Upcoming Board Training on Services for Individuals with Complex Needs
Mr. Robinson mentioned this potential training topic which he would like to present at the June Board meeting.
Ms. Ingram will add the training topic to the agenda.
5/16/17
7. June 1, 2017, Area Board Draft Agenda
Committee reviewed proposed agenda and provided input. COMMITTEE ACTION A motion was made by Vice-Chair Binanay to recommend that the Area Board cancels the July 6, 2017, regular meeting; motion seconded by Dr. Corvin. Motion passed unanimously. COMMITTEE ACTION A motion was made by Mr. Stanford to approve $250,000.00 investment with CASA for thirteen TCLI supportive housing units per approval by the Finance Committee and Area Board on June 1, 2017; motion seconded by Dr. Corvin. Motion passed unanimously.
Ms. Ingram will forward revised agenda to staff.
5/16/17
8. Closed Session COMMITTEE ACTION A motion was made by Dr. Corvin to enter closed session pursuant to NCGS 143-318.11 (a) (6) and NCGS 143-318.11 (1) to consider the qualifications, competence, and performance of an employee and to prevent the disclosure of information that is confidential and not a public record under NCGS 122C-126.1.; motion seconded by Ms. Gloston. Motion passed unanimously. Committee returned to open session.
None specified. N/A
9. ADJOURNMENT: the next Committee meeting will be June 20, 2017, at 4:00 p.m.

(Back to agenda)
ITEM: Network Development and Services Committee Report DATE OF BOARD MEETING: June 1, 2017 BACKGROUND: The committee reviews progress on the agency’s network development plan and progress on service development. The committee reports to the Area Board and provides guidance and feedback on development of the needs and gaps assessment to meet state and agency requirements. This month’s report includes draft minutes and materials from the May 10, 2017, meeting. REQUEST FOR AREA BOARD ACTION: Accept the report. CEO RECOMMENDATION: Accept the report. RESOURCE PERSON(S): William Stanford, Committee Chair; Beth Melcher, Senior Vice-President of Network Development and Evaluation
Alliance Behavioral Healthcare BOARD OF DIRECTORS
Agenda Action Form
7D
Wednesday, May 10, 2017 BOARD NETWORK DEVELOPMENT & SERVICES COMMITTEE - REGULAR MEETING 4600 Emperor Boulevard, Durham, NC 27703 4:00-5:00 p.m.
Draft minutes may be submitted with the monthly Board packet. Minutes will be approved by this Committee at a later date. Page 1 of 2
APPOINTED MEMBERS PRESENT: ☒Cynthia Binanay, M.A., ☒George Corvin, M.D., ☐ John Griffin, Ed.D., ☒William Stanford, Jr., J.D. (Committee Chair), ☒ McKinley Wooten, Jr., J.D.
BOARD MEMBERS PRESENT: Chris Bostick GUEST(S) PRESENT: None STAFF PRESENT: Beth Melcher, Senior VP Network Development and Evaluation; Director of Provider Evaluation; Carlyle Johnson, Director Strategic Initiatives
1. WELCOME AND INTRODUCTIONS
2. REVIEW OF THE MINUTES – The minutes from the March 8, 2017, meeting were reviewed; a motion was made by Ms. Binanay and
seconded by Dr. Corvin to approve the minutes. Motion passed unanimously.
AGENDA ITEMS: DISCUSSION: NEXT STEPS: TIME FRAME:
3. Suicide prevention activities
Reviewed presentation activities supported through the Alliance Community Relations department and with our community partners. These include:
o Partner with all our local school systems on suicide prevention awareness o Partner with Youth Thrive on efforts to eliminate youth suicide in Wake Co o Partner with the local chapters of the American Foundation for Suicide
Prevention o Still promoting Kids in Crisis campaign o MHFA training o CIT training o Social media training on bullying and suicide
Also discussed Alliances response and review of suicides and recommendations that may be developed from that process
4. Results of Needs and Gaps Analysis
Reviewed results of the Needs and Gaps Analysis including areas where requirements of access and choice are met as well as where not and reasons for that. Also reviewed areas identified by stakeholders as areas where improvements could be made. The Needs and Gaps Analysis is the foundation for the Network Development Plan which is submitted to the state at the end of June.
Submit Needs and Gaps Analysis to state Develop and submit Network Development Plan to state
June 1, 2017 June 30, 2017

Wednesday, May 10, 2017 BOARD NETWORK DEVELOPMENT & SERVICES COMMITTEE - REGULAR MEETING 4600 Emperor Boulevard, Durham, NC 27703 4:00-5:00 p.m.
Draft minutes may be submitted with the monthly Board packet. Minutes will be approved by this Committee at a later date. Page 2 of 2
AGENDA ITEMS: DISCUSSION: NEXT STEPS: TIME FRAME:
Results and recommendations of Substance Use Disorder continuum consultation
Alliance engaged Dr. Mee Lee, an editor of the substance use ASAM criteria, to survey and review Alliance’s current substance use continuum and assist in developing recommendations. This review included considerable input from providers and community stakeholders. Results will inform network service development as well as technical assistance and training with our providers.
Proposed topics for May meeting
Population Health Model; Network Development Plan
5. ADJOURNMENT: next meeting will be July 12, 2017, from 4:00 p.m. to 5:00 p.m.

Alliance SUD Continuum
Alliance Board Services CommitteeMay 10, 2017

Evaluation of Alliance SUD Continuum• FY17 Network Development Plan included
plan to review Alliance SUD service array
• Workgroup including multiple Alliance departments and DHHS convened in September, 2016
• Collaboration with external consultant, Dr. David Mee-Lee (Chief Editor, ASAM Criteria)
• Summary document prepared including recommendations for enhancing service array

Evaluation of Alliance SUD Continuum• Conduct an inventory of current Alliance
service continuum for substance use disorders
• Identify components and characteristics of an effective service array
• Develop recommendations for development of a comprehensive continuum of care for individuals with substance use disorders
Service Inventory ReviewService Inventory gaps identified:
• Withdrawal Management
• Opioid Treatment
• Residential Treatment
• Inpatient services, particularly for adolescents

SUD Provider Feedback
Service and resource gaps identified:
• Withdrawal Management continuum
• Residential Treatment
• Housing
• Transportation
• MAT
• Adolescent SUD services
• Providers with multiple levels of care

SUD Provider FeedbackSystem issues:
• Fragmentation of services
• Need for chronic care approach
• Lack of funding for uninsured
• Transportation/service accessibility concerns

Characteristics of an Effective Service Continuum
• Recognition of substance use disorders as chronic conditions
• Individually directed
• Integrated continuum focusing on community tenure and continuity of care
• Connected to community and stakeholders
Recommendations• Population Management approach
• Increase stakeholder involvement
• Philosophical change from program-driven to individually-focused care
• Reduce fragmentation and improve continuity of care
• Enhance breadth and accessibility of withdrawal management continuum
• Expand integrated treatment of co-occurring MI/SUD, particularly for adolescents

2017 Alliance Community Needs and Gaps Assessment
Alliance Board Services CommitteeMay 10, 2017

Updates on Needs AssessmentAreas covered in March presentation:
• Scope of Community Needs Assessment
• Survey and feedback methodology
• Breadth of community stakeholder input
• Preliminary survey and stakeholder feedback
Updates since March:
• Final summary of survey and stakeholder feedback
• Completed geographic access analysis
• Draft Community Needs Assessment complete
Objectives of Needs Assessment1. Fulfillment of State and Federal requirements
2. Improved understanding of community needs and identification of potential areas for improvement
3. Development of comprehensive “wishlist” that can contribute to strategic planning, network development initiatives and advocacy efforts
4. Identification of:
• Priorities for network development that can be supported with existing resources
• Needs and gaps that will require identification of resources through community partnership or advocacy

Access & Choice Access Choice:
Medicaid
Choice:
State
Outpatient 30 minutes / 30 miles 2 2
Location-Based 30 minutes / 30 miles 2 1
Community /
Mobile
ABH Catchment Area 2 1
Crisis ABH Catchment Area 1 1
Inpatient ABH Catchment Area 1 1
Specialized ABH Catchment Area 1 1
C-Waiver (two
sections)
ABH Catchment Area A: 2
B: 1
N/A

Access & Choice Review Service categories with adequate access and choice:
• Outpatient
• Community-Based and Mobile
• Crisis
• Inpatient
• C-Waiver

Access & Choice Review Services with limited access and choice:
• Location-Based:
• Opioid Tx (Mcaid: 69%, State: 65%)
• Child/Adol Day Treatment (State, 90%)
• SACOT (State, 77%)
• Day Supports (State: 96%)

Access & Choice Review Services with limited access and choice:
• Specialized:
• Partial Hospitalization (Medicaid)*
• SA Non-Medical CRT (Medicaid & State)*
• PRTF(State)
• Residential Level II: other than TFC (State)
• IDD Supported Living (State)

Addressing Access & Choice GapsResolved gaps:
• Partial Hospitalization (Medicaid)
• SA Non-Medical CRT (Medicaid & State)
Request DMA Waiver:
• Opioid Treatment: request waiver of choice and approval for continued use of MAT-Buprenorphine codes in place of Outpatient Opioid Treatment service codes

Addressing Access & Choice GapsRequest DMH Waiver:
• Child/Adol Day Treatment
• SACOT
• Opioid Tx
• Day Supports
• PRTF
• Residential Level II: other than TFC
• IDD Supported Living

Other Access & Choice Areas• Medicaid “In lieu of” services
• Family Centered Treatment• ACTT Step-Down• Outpatient Plus
• Rapid Response• Non-Medicaid Alternative Services
• Comp. Screening/Comm. Connections, Recovery Support, Hospital Transition, DBT, Assertive Engagement, Crisis Eval. & Observ.
• Non-Medicaid geographic disparities
Service Needs and GapsGeneral and cross-population:
• Housing
• Access and availability of appointments
• Continuum for justice-involved
• Inpatient capacity and access
• System navigation and information
• Cross-disability fluency and expertise
• Case Management

Service Needs and GapsChild and Adult IDD:
• Geographic disparities in Non-Medicaid benefit plan
• Limited services for non-Innovations
• Limited Innovations slots and long waiting lists for Innovations
• Shortage of qualified direct care workers
• Inpatient psychiatric treatment for dually diagnosed (IDD/MI)
• Residential options

Service Needs and GapsAdult MH/SUD:
• Comprehensive array of services for SUD
• Expanded continuum for withdrawal management
• Increased MAT availability and capacity
• Short-term residential treatment for SUD
• Services for uninsured
• Medication access for uninsured
• Respite
• Structured daily activity programs

Service Needs and GapsChild MH/SUD:
• Services for high needs youth, including residential treatment, school supports, and crisis services
• Services for transition age youth
• Specialized interventions for gang-involved youth
• Respite services
• Adolescent SUD services
• Residential treatment

Underserved Populations• Uninsured and underinsured
• Non-English service access
• Transition-Age Youth, youth aging out of foster care
• Dually Diagnosed (IDD/MI and SUD/MI)
• Individuals transitioning from criminal justice system
• Homeless
• Elderly
• Others: LGBTQ, Veterans, individuals in crisis, especially those with special needs (e.g., IDD, children)

Barriers• Funding: limited funds for uninsured, providers
reaching budget caps, underinsured access, benefit plan limitations, low provider reimbursement rates
• Knowledge of system: confusion by consumers and stakeholders about system navigation, Alliance roles General access barriers: timely access, evening and weekend hours, providers not accepting referrals, especially for complex needs, waiting lists
• Language: bilingual/bicultural providers, language lines, tracking of bilingual/bicultural services
• Transportation

Next Steps• Final review and preparation of draft for
submission
• Request for access and choice waivers
• Submission of report by June 1
• Identification of network development priorities that can be addressed in FY18 with existing resources
• Preparation and submission of Network Development Plan by June 30
Discussion and Questions

7E
(Back to agenda)
ITEM: Global Quality Management Committee Report DATE OF BOARD MEETING: June 1, 2017 BACKGROUND: The Global QMC is the standing committee that is granted authority for Quality Management by the MCO. The Global QMC reports to the MCO Board of Directors which derives from General Statute 122C-117. The Quality Management Committee serves as the Board’s monitoring and evaluation committee charged with the review of statistical data and provider monitoring reports. The goal of the committee is to ensure quality and effectiveness of services and to identify and address opportunities to improve LME/MCO operations and local service system with input from consumers, providers, family members, and other stakeholders. The Alliance Board of Directors’ Chairperson appoints the committee consisting of five voting members whereof three are Board members and two are members of the Consumer and Family Advisory Committee (CFAC). Other non-voting members include at least one MCO employee and one provider representative. The MCO employees typically assigned are the Director of the Quality Management (QM) Department who has the responsibility for overall operation of the Quality Management Program; the MCO Medical Director, who has ultimate responsibility of oversight of quality management; the Quality Review Manager, who staffs the committee; the Quality Management Data Manager; and other staff as designated. The Global QMC meets at least quarterly each fiscal year and provides ongoing reporting to the Alliance Board. The Global QMC approves the MCO’s annual Quality Improvement Projects, monitors progress in meeting Quality Improvement goals, and provides guidance to staff on QM priorities and projects. Further, the Committee evaluates the effectiveness of the QM Program and reviews and updates the QM Plan annually. The draft minutes and materials from the May meeting are attached. At the meeting, the Committee reviewed the data dashboard. QM noted red flags in Care Coordination assignment, resolution of complaints, and timeliness of initial appointments. All issues have been addressed and in process of being addressed. The committee was reminded that it is time to survey the Board members about their perception of Board functioning. Surveys have been emailed to members and will be handed out at Board meeting. Committee learned about an initiative in QM to improve internal performance of departments. Geyer informed committee about scores from the EQR visit at the end of February—Alliance scored 94%, an increase from last year’s performance. The Committee received a presentation on the progress of Quality Improvement Projects (QIPs): 9 projects are open and active, while 3 projects have been closed. QM is recommending that no new projects are started in FY 18. Committee will review recommendation and vote at their next meeting in June.
Alliance Behavioral Healthcare BOARD OF DIRECTORS
Agenda Action Form

7E
(Back to agenda)
REQUEST FOR AREA BOARD ACTION: Accept the report. CEO RECOMMENDATION: Accept the report. RESOURCE PERSON(S): George Corvin, Committee Chair; Wes Knepper, Quality Management Director

Thursday, May 04, 2017 GLOBAL QUALITY MANAGEMENT COMMITTEE
Page 1 of 3
VOTING MEMBERS PRESENT: ☒ George Corvin, MD, Chair (Area Board); ☐ Phillip Golden, BA, Co-Chair (Area Board); ☒ Chris Bostock (Area Board);
☐ Amelia Thorpe, BA (CFAC/Area Board); ☒ Lascel Webley, Jr., BS, MBA, MHA (Area Board) ☒ Joe Kilsheimer, MBA (CFAC)
NON-VOTING MEMBERS PRESENT: ☒ Tim Ferreira, BA (Provider Representative, I/DD); ☒ Jeremy Reed MH/SA (Provider Representative)
STAFF PRESENT: ☐ May Alexander, MS, LMFT (Quality Assurance Manager); ☒ Tina Howard, MA (Quality Review Manager); ☒ Geyer Longenecker, JD
(Quality Management Director); ☐ (Medical Director); ☒ Doug Wright (Director of Consumer Affairs); ☒ Linda Losiniecki, (Administrative Assistant) GUEST(S) PRESENT: Wes Knepper, Director of Quality Management starting May 8 (Alliance Behavioral Healthcare), Mary Hutchings, Auditor (Wake County Internal Audit) REVIEW OF THE MINUTES: GQMC Meeting minutes from March 2, 2017 were read. Chris Bostock motioned that the minutes be approved, Joe Kilsheimer seconded the motion. The motion was approved by the Committee.
AGENDA ITEMS: DISCUSSION: NEXT STEPS: TIME FRAME:
1. Welcome & Introductions:
Welcome: Chair Dr. Corvin opened the meeting and welcomed guests and new committee member Wes Knepper, Director of Quality Management of as May 8. Geyer Longenecker stepping down from the Quality Management Committee Board and leaving Alliance Behavioral Healthcare on 5-5-17. Wes Knepper will be the new Director of Quality Management. Best wishes to Geyer and his future endeavors.
2. New Business:
Area Board Surveys Tina reminded the committee that it is time again to hand out surveys to the Area Board members, and members who serve on Board committees but are not Board members. Survey tool will remain the same to determine if interventions of training and revising minutes make a difference. Surveys will be handed out at Board meeting this afternoon. Performance Dashboard Geyer presented dashboard data. Alliance did not meet benchmark for Care Coordination assignment in one quarter, but that has been addressed. There were two quarters in which Alliance did not meet benchmark for complaints resolution.
Goal: 100% response rate, Tina to update committee on progress
Next meeting

Thursday, May 04, 2017 GLOBAL QUALITY MANAGEMENT COMMITTEE
Page 2 of 3
AGENDA ITEMS: DISCUSSION: NEXT STEPS: TIME FRAME: Reasons include providers not responding in time with information and complaints resulting in investigations that take longer. QM expects performance in April to reach benchmark. Alliance continues to not meet benchmarks for Access to Care standards, thus, we continue the QIP to address concerns and continues to advocate for more realistic standards. Performance Metric Project Alliance QM has begun an initiative to develop a high-level view of current performance management activities within Utilization Management, Claims, Access and the IT Help Desk. Shortly, this initiative will be expanded to all units at Alliance. Interviews were conducted with leaders in each of the units. Analysis identified strengths in collecting quantitative measures and opportunities for improvement in efficient ways of collecting qualitative data. QM staff will lead teams to refine qualitative measures and streamline collection. EQR Update Geyer presented the results of the review:
This year’s was Alliance’s 3rd review. The EQR review was combined with the Mercer review. A 2-day panel conducted staff interviews, review documentation, analytics/surveys and reports.
Alliance scored 94% on review, higher than last year’s score of 85%.
QM scored 94%, an increase from last year’s score of 71%
EQRO required a corrective action plan to increase attendance at Alliance’s internal CQI Leadership Team.
QIP Updates Tina provided updates (Handout/Presentation):
9 projects are open and active, none are expected to close by June 30
Improve Crisis Services and First Responder QIPs may close by the end of the calendar year
The First Responder answered calls have increased to 79% and is the best seen in years.
Update committee on progress
In 2-3 months
Thursday, May 04, 2017 GLOBAL QUALITY MANAGEMENT COMMITTEE
Page 3 of 3
AGENDA ITEMS: DISCUSSION: NEXT STEPS: TIME FRAME: Challenges: Crisis Services – intervention does not seem to be impacting CAS
closures; Access to Care – continued poor show rate for all urgency levels. Recommendations for FY18:
No new QIPs are being recommended due to continuation of the active QIPs,
Request committee approval for QM to stop monitoring IDD IRR since improvement was sustained (FY15 QIP):
A motion by Dr. Corvin to close the follow-up period for the Interrater Reliability for the IDD Utilization Management Department, motion seconded by Joe, motion was approved.
Committee will review FY 18 QIP recommendations and vote next meeting
Upcoming Meetings: Dr. Corvin stressed the attendance to Global QMC meetings, quorums are not being met and committee is unable to complete business. A suggestion by Joe was to call members a few days before meeting as a reminder, in addition to the email reminders. Tina suggested to the committee a new time and/or day for the meetings. Decision was made to keep the same day and time. Next meeting: June 1, 2017 (Time: 2:00 – 3:30 pm Location: Corporate Site July 6th – No Meeting – Summer Break
Adjournment: Meeting adjourned at 3:15 p.m.

Please complete this survey as a member of the Alliance Board and Board Committees according tothe instructions on the following pages. A section has been provided at the end of the questionnairefor you to offer comments or suggestions if you choose. At the bottom of the survey is a boxlabeled "Done." When you are finished, click this box to submit the questionnaire.
Please complete this survey online or on hard copy. If you would like to request a copy of thesurvey, email Tina Howard at [email protected] and mail or email by Friday, May 26, 2017.Mailed copies may be sent to:
Alliance Behavioral HealthcareAttn: Tina Howard, Quality Review Manager4600 Emperor Blvd, Suite 200Durham, NC 27703
Alliance Board Survey 2017
Board Survey 2017
1
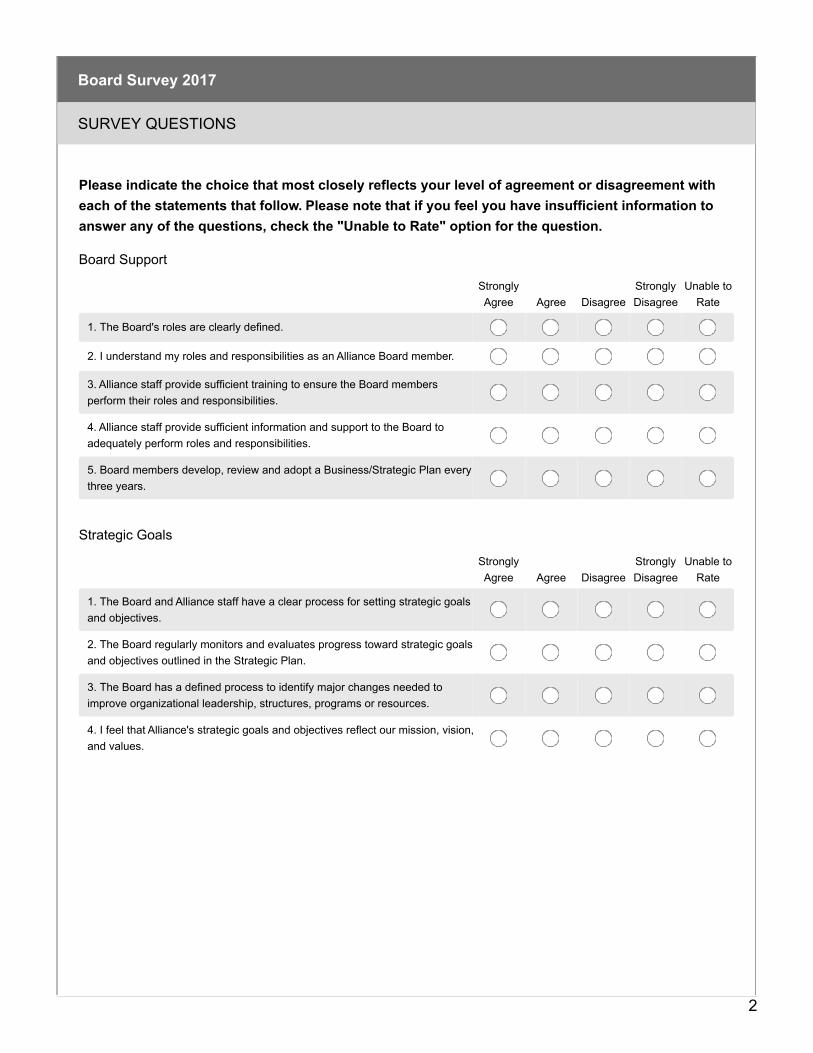
Please indicate the choice that most closely reflects your level of agreement or disagreement witheach of the statements that follow. Please note that if you feel you have insufficient information toanswer any of the questions, check the "Unable to Rate" option for the question.
SURVEY QUESTIONS
Board Survey 2017
StronglyAgree Agree Disagree
StronglyDisagree
Unable toRate
1. The Board's roles are clearly defined.
2. I understand my roles and responsibilities as an Alliance Board member.
3. Alliance staff provide sufficient training to ensure the Board membersperform their roles and responsibilities.
4. Alliance staff provide sufficient information and support to the Board toadequately perform roles and responsibilities.
5. Board members develop, review and adopt a Business/Strategic Plan everythree years.
Board Support
StronglyAgree Agree Disagree
StronglyDisagree
Unable toRate
1. The Board and Alliance staff have a clear process for setting strategic goalsand objectives.
2. The Board regularly monitors and evaluates progress toward strategic goalsand objectives outlined in the Strategic Plan.
3. The Board has a defined process to identify major changes needed toimprove organizational leadership, structures, programs or resources.
4. I feel that Alliance's strategic goals and objectives reflect our mission, vision,and values.
Strategic Goals
2

StronglyAgree Agree Disagree
StronglyDisagree
Unable toRate
1. Board members use the organization's vision, mission and values to monitorprovider services.
2. A wide range of community members participate in providing feedback andevaluating the performance of Alliance's Board, organization and providers.
3. Our Board regularly seeks feedback from our citizens on the quality andeffectiveness of the services they receive.
4. The Board reviews reports on unmet local service needs and providercapacity.
Provider Monitoring
StronglyAgree Agree Disagree
StronglyDisagree
Unable toRate
1. The Board uses standard benchmarks to assess financial performance andacts if performance standards are not met.
2. Board members review reports on Alliance's finances.
3. Our Board makes the hard choices and politically unpopular decisions whenrequired or necessary.
4. Our Board ensures finances are closely related to performanceexpectations and the organization's mission.
5. Our Board makes sure adequate financial tools and resources are in placefor the organization to accomplish strategic objectives.
6. Our Board has a long term financial plan.
7. I feel that I have the information and support from Alliance staff to providefiscal oversight of the organization.
Financial Accountability
StronglyAgree Agree Disagree
StronglyDisagree
Unable toRate
1. The Board oversees the quality and effectiveness Alliance's providernetwork.
2. Board members regularly review reports that provide performance data onour provider services, using comparable performance data where available.
3. The Board regularly monitors and evaluates progress toward strategic andprogram performance goals outlined in Alliance's Strategic Plan.
4. The Board reviews reports on local performance.
5. The Board reviews trends in service utilization.
6. The Board reviews reports on customer service.
Quality and Availability of Services
3

StronglyAgree Agree Disagree
StronglyDisagree
Unable toRate
1. Our Board members represent the community's interests.
2. Our Board stays informed about important trends in the larger environmentthat are likely to affect our communities and local governments.
3. The Board listens to people with diverse views, opinions and experiences.
4. Before reaching an important decision, this board seeks input from peoplelikely to be affected by the decision.
5. The Board seeks and acquires knowledge that can be used to satisfy theneeds of our citizens and communities.
6. If our Board thinks a key constituency or stakeholder group may disagreewith an issue we are considering, we will make an effort to hear from themdirectly before taking action.
7. Our Board seeks information and advice from leaders of similar and relatedorganizations.
8. Relationships among Board members and the public are characterized byopenness, trust and mutual respect.
9. Our Board communicates effectively with the county, other communityorganizations, and local businesses.
Partnerships with Community and Stakeholders
StronglyAgree Agree Disagree
StronglyDisagree
Unable toRate
1. Our Board takes responsibility for issues facing the organization.
2. Our Board is proactive and addresses issues before they become urgent orcritical.
3. Our Board has a clearly defined process to identify major changes neededto improve organizational leadership, structures, programs or resources.
4. The organization is able to respond and adapt to new opportunities andchallenges.
5. I feel that our process for evaluating the Area Director is clear, fair, andadequately measures expected performance.
Organizational Stability
4

Which standing committees are you a member of (select all that apply):
Finance Committee
Human Rights Committee
Quality Management Committee
Executive Committee
Policy/By-Laws Committee
County Commissioner Advisory Board
StronglyAgree Agree Disagree
StronglyDisagree
Unable toRate
1. The committee(s) I serve on have clear goals and objectives.
2. The committee(s) I serve on are organized well.
3. The committee(s) I serve on achieve goals promoted by the agency.
4. I feel the committee(s) I serve on adds value to the agency and community.
5. I am well informed of committee meetings ahead of time(dates/times/locations).
6. The information I receive regarding committee topics assists me withmaking appropriate decisions.
Board Committee Processes
Please offer any comments or suggestions in this box.
5

May 4, 2017 From: Geyer Longenecker To: Global QM Committee Re: Care Coordination assignment compliance update Issue: During January 2017, Alliance did not meet the state’s standard of 85% for assigning inpatient readmissions to care coordination. Analysis: On February 7, QM staff submitted its analysis to the Director of MH/SA Care Coordination. During January 2017, Alliance assigned 8 of 10 readmissions (80%). The analysis of the two cases where no assignment was made found that Alliance had no documentation of hospital liaison/care coordination involvement. Actions: The Director of MH/SA Care Coordination reviewed procedures with team leads and staff. Results: In February, care coordination assignment met the state’s standard in February (85.7%) with 6 of 7 cases properly assigned care coordination. The failure to assign in one case was attributed to an outage in the Alpha system. In March, 100% of cases (13 of 13) were properly assigned.
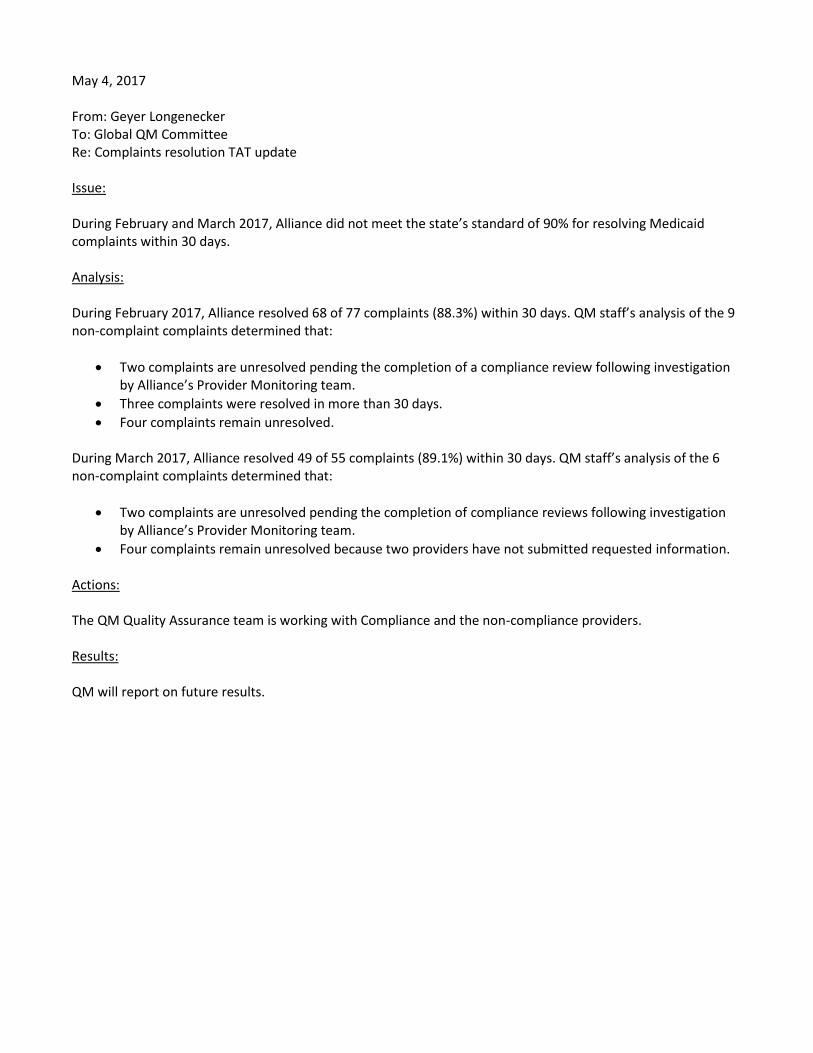
May 4, 2017 From: Geyer Longenecker To: Global QM Committee Re: Complaints resolution TAT update Issue: During February and March 2017, Alliance did not meet the state’s standard of 90% for resolving Medicaid complaints within 30 days. Analysis: During February 2017, Alliance resolved 68 of 77 complaints (88.3%) within 30 days. QM staff’s analysis of the 9 non-complaint complaints determined that:
Two complaints are unresolved pending the completion of a compliance review following investigation by Alliance’s Provider Monitoring team.
Three complaints were resolved in more than 30 days.
Four complaints remain unresolved. During March 2017, Alliance resolved 49 of 55 complaints (89.1%) within 30 days. QM staff’s analysis of the 6 non-complaint complaints determined that:
Two complaints are unresolved pending the completion of compliance reviews following investigation by Alliance’s Provider Monitoring team.
Four complaints remain unresolved because two providers have not submitted requested information. Actions: The QM Quality Assurance team is working with Compliance and the non-compliance providers. Results: QM will report on future results.
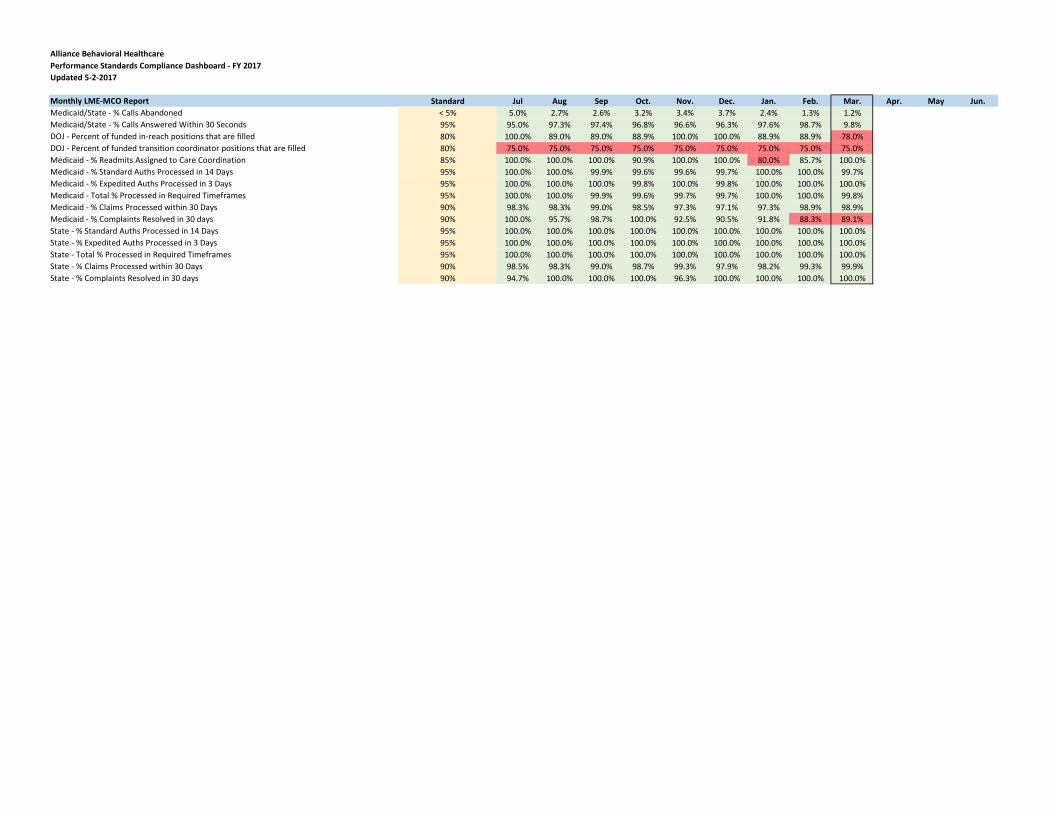
Alliance Behavioral Healthcare
Monthly LME-MCO Report Standard Jul Aug Sep Oct. Nov. Dec. Jan. Feb. Mar. Apr. May Jun.
Medicaid/State - % Calls Abandoned < 5% 5.0% 2.7% 2.6% 3.2% 3.4% 3.7% 2.4% 1.3% 1.2%
Medicaid/State - % Calls Answered Within 30 Seconds 95% 95.0% 97.3% 97.4% 96.8% 96.6% 96.3% 97.6% 98.7% 9.8%
DOJ - Percent of funded in-reach positions that are filled 80% 100.0% 89.0% 89.0% 88.9% 100.0% 100.0% 88.9% 88.9% 78.0%
DOJ - Percent of funded transition coordinator positions that are filled 80% 75.0% 75.0% 75.0% 75.0% 75.0% 75.0% 75.0% 75.0% 75.0%
Medicaid - % Readmits Assigned to Care Coordination 85% 100.0% 100.0% 100.0% 90.9% 100.0% 100.0% 80.0% 85.7% 100.0%
Medicaid - % Standard Auths Processed in 14 Days 95% 100.0% 100.0% 99.9% 99.6% 99.6% 99.7% 100.0% 100.0% 99.7%
Medicaid - % Expedited Auths Processed in 3 Days 95% 100.0% 100.0% 100.0% 99.8% 100.0% 99.8% 100.0% 100.0% 100.0%
Medicaid - Total % Processed in Required Timeframes 95% 100.0% 100.0% 99.9% 99.6% 99.7% 99.7% 100.0% 100.0% 99.8%
Medicaid - % Claims Processed within 30 Days 90% 98.3% 98.3% 99.0% 98.5% 97.3% 97.1% 97.3% 98.9% 98.9%
Medicaid - % Complaints Resolved in 30 days 90% 100.0% 95.7% 98.7% 100.0% 92.5% 90.5% 91.8% 88.3% 89.1%
State - % Standard Auths Processed in 14 Days 95% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0%
State - % Expedited Auths Processed in 3 Days 95% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0%
State - Total % Processed in Required Timeframes 95% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0%
State - % Claims Processed within 30 Days 90% 98.5% 98.3% 99.0% 98.7% 99.3% 97.9% 98.2% 99.3% 99.9%
State - % Complaints Resolved in 30 days 90% 94.7% 100.0% 100.0% 100.0% 96.3% 100.0% 100.0% 100.0% 100.0%
Performance Standards Compliance Dashboard - FY 2017
Updated 5-2-2017

DMH Data Submissions Reports Standard FY17 Q1 FY17 Q2 FY17 Q3 FY17 Q4
Monthly Financial Reports Timely/Complete Met Met
Substance Abuse/Juvenile Justice Initiative Quarterly Report Timely/Complete Met Met
Work First Initiative Quarterly Reports Timely/Complete Met Met
Traumatic Brain Injury (TBI) Services Quarterly Report Timely/Complete Met Met
Quarterly Complaints Report Timely/Complete Met Met
System of Care Report Timely/Complete Met Met
SAPTBG Compliance Report Timely/Complete Met Met
National Core Indicators (NCI) Consents, Pre-Surveys, and Mail Surveys Timely/Complete Met Met
Client Data Warehouse (CDW) - Screening Record Timely/Complete/90% Met Met
Client Data Warehouse (CDW) - ICD-9 Diagnosis Timely/Complete/90% Met Met
Client Data Warehouse (CDW) - Unknown Data (Admissions) Timely/Complete/90% Met Met
Client Data Warehouse (CDW) - Unknown Data (Discharges) Timely/Complete/90% Met Met
Client Data Warehouse (CDW) - Identifying and Demographic Records Timely/Complete/90% Met Met
Client Data Warehouse (CDW) - Drug of Choice Timely/Complete/90% Met Met
Client Data Warehouse (CDW) - Episode Completion Record (SA Clients) Timely/Complete/90% Met Met
NC Treatment Outcomes and Program Performance System (NC-TOPPS) 90% submitted Met Met
NC Support Needs Assessment Profile (NC-SNAP) 90% updated Met Met
Quarterly Access to Care Report Standard FY17 Q1 FY17 Q2 FY17 Q3 FY17 Q4
Emergent - Medicaid (2 hours) 97% 80.0% 55.0% 54.0%
Emergent - Non-Medicaid 97% 85.0% 60.0% 54.0%
Emergent - Combined 97% 84.0% 59.0% 54.0%
Urgent - Medicaid (48 hours) 82% 23.0% 23.0% 26.0%
Urgent - Non-Medicaid (48 hours) 82% 26.0% 11.0% 16.0%
Urgent - Combined (48 hours) 82% 25.0% 15.0% 19.0%
Routine - Medicaid (14 days) 75% 42.0% 37.0% 55.0%
Routine - Non-Medicaid (14 days) 75% 35.0% 38.0% 34.0%
Routine - Combined (14 days) 75% 39.0% 37.0% 45.0%

Quarterly NC-TOPPS Report Standard FY17 Q1 FY17 Q2 FY17 Q3 FY17 Q4
% Received 90% 99.2% 99.0%
% Received On-Time 90% 95.4% 96.3%
Quarterly Innovations Reports Standard FY17 Q1 FY17 Q2 FY17 Q3 FY17 Q4
D.6 - Proportion of new waiver beneficiaries receiving services within 45 days of ISP approval. 85% 100.0% 93.8%
G.1 - Percent of Actions Taken to Protect the Beneficiary 85% 91.4% 92.9%
G.2 - Percentage of level 2 and 3 incidents reported within required timeframes 85% 86.5% 91.1%
G.3 - Percentage of deaths where required LME/PIHP follow-up interventions were completed
as required. 85% 100.0% 100.0%
G.4 - Percentage of medication errors resulting in medical treatment. <15% 0.0% 0.0%
G.5 - Percentage of beneficiaries who received appropriate medication 85% 100.0% 99.9%
G.7 - Percentage of level 2 or 3 incidents where required LME/PIHP follow-up interventions
were completed 85% 100.0% 100.0%
G.8 - Percentage of incidents referred to the DSS or DHSR 85% 100.0% 100.0%
G.9 - Percentage of restrictive interventions resulting in medical treatment. <15% 0.0% 0.0%
Semi-Annual Innovations Reports Standard FY 2017-1 FY 2017-2
B.2 - Proportion of Level of Care evaluations completed at least annually for enrolled
beneficiaries 85% 99.9%
B.3 - Proportion of Level of Care evaluations completed using approved processes and
instrument 85% 100.0%
B.4 - Proportion of New Level of Care evaluations completed using approved processes and
instrument 85% 100.0%
D.2 - Proportion of Individual Support Plans that address identified health and safety risk
factors 85% 96.7%
D.4 - Proportion of PCPs that are completed in accordance with DMA requirements. 85% 99.0%
Annula Innovations Reports Standard FY 2017
B.1 - Percent of new waiver enrollees who have a LOC prior to receipt of services. 85%
C.1 - Proportion of new licensed providers that meet licensure, certification, and/or other
standards. 85%
C.2 - Proportion of providers reviewed according to PIHP monitoring schedule 85%
C.3 - Proportion of providers for whom problems have been discovered and appropriate
remediation has taken place 85%
C.4 - Proportion of providers that successfully implemented an approved corrective action plan 85%
C.5 - Proportion of monitored providers wherein all staff completed all mandated training 85%
D.1 - Proportion of ISPs in which the services and supports reflect participant assessed needs
and life goals 85%
D.3 - Percentage of beneficiaries reporting that their ISP has the services that they need 85%
D.5 - Proportion of individuals for whom an annual plan and/or needed update took place. 85%
D.7 - Proportion of beneficiaries who are receiving services as specified in the ISP 85%
D.8 - Proportion of records that contain a signed freedom of choice statement 85%
D.9 - Proportion of beneficiaries reporting their Care Coordinator helps them to know what
waiver services are available 85%
D.10 - Proportion of beneficiaries reporting they have a choice between providers 85%
G.10 - Percentage of beneficiaries age 21 and older who had a primary/preventative care visit
during year. 85%
I.1 - Proportion of claims paid by the PIHP for Innovations wavier services authorized in the
service plan. 85%

Performance MetricsMay 2, 2017

Phase I – Department Interviews
• Goal: Develop a high-level view of current performance management activities within Utilization Management, Claims, Access and the IT Help Desk.
• Process:
• SPMO and QM developed a standard set of interview questions;
• Interviews were conducted with staff from Claims, Utilization Management, IT and Access;
• Zelos participated in, reviewed interviews.

Phase I – General Trends
• Most of the easily countable quantitative measures are being tracked (“how many”, “how fast”, etc.);
• Many of the quantitative metrics rely on data entered into spreadsheets or logs;
• Analysis of the quantitative data often is manual;

Phase I – General Trends• Measuring the quality of staff decision making
currently requires manual analysis of free-text fields which takes a lot of supervisor time;
• Directors and supervisors currently do not rely on qualitative metrics because of a lack of such measures, or the insufficiency of existing measures;
• At this time, the quality of staff performance is not being measured based on metrics.
Phase I – General Opportunities
• Build forms into SharePoint or other database applications to improve data quality and facilitate analysis.
• Use new data analytics tools to do a “first pass” at analyzing free text fields;

Phase I – Department Goals
• UM: To ensure that the services consumers receive are medically necessary and align with best practices whenever possible.
• Access: To maintain the safety of callers during the process of screening, triage and referral for all new or inactive consumers seeking mental health, substance abuse, or IDD services.

Phase I – Department Goals
• Claims: To ensure that claims are paid according to prompt pay guidelines, and to help providers submit “clean” claims.
• IT: To provide a secure and reliable computing system for Alliance staff, and to respond quickly and professionally to issues and questions staff have about the Alliance computing system.
Phase I – Department GoalsQM and department staff will:
• Determine the department’s greater needs, improve current processes, and develop new reports focusing on quantitative measures;
• Develop new qualitative measures to better track staff and department performance;
• Most importantly, develop qualitative measures to advance Alliance’s strategic goals of improving consumer care and enhancing our staff’s work experience.

Phase II – Process
Project Advisory
Team
• Create Project Advisory Team of department, QM and other staff
• The PAT guides the direction of the project
Process building
• Conduct process mapping to define scope and boundaries
• Develop Quality Assurance for compliance with contract requirements
Benchmarking
• Gather and analyze data to determine current performance
• Set future performance standards
Identify Improveme
nt
• Identify and test interventions to improve performance
• Test new technologies for gathering, analyzing data
Evaluate Impact
• Determine if interventions, technologies are effective
• Revise measures, interventions and technologies as needed

Phase II – Next Steps• QM staff, department participants will review Phase I
interviews;
• Understand the department’s expectations for performance and assess current measures;
• Build consensus on the importance of developing qualitative measures;
• Agree on 2-3 possible qualitative performance measures;
• Examine current processes, data and reports, recommend improvements, and track changes.

Phase II – Next Steps
• Develop reports to track progress towards the qualitative goals;
• Assess new technologies to allow better qualitative reporting;
• Create quality assurance processes and reports for “hand off” to the department;
• Conduct follow-up reviews to assure sustained improvement and identify new opportunities.

Phase II – QM StaffLeadership:
• Wes Knepper, QM Director
• May Alexander, Quality Assurance Manager
• Tina Howard, Quality Review Manager
Project Advisory Teams:
• Access: Tina Howard
• Claims: Jamie Rizza
• IT: Shruti Mehta
• UM: Andrea Kinnaugh

Alliance BHC
(EQR) Summary Report Results
Alliance 2016 EQR Score results: 94.4%. // Alliance 2015 Score Results: 85.64% Met – 94.4% Met – 85.64% Partially Not Met – 3.0% Partially Not Met - 7.73% Not Met – 0.4% Not Met - 0.55% Not Evaluated – 2.2% Not Evaluated – 6.08%
Alliance 2014 EQR Summary Score: 70.17% LME-MCO function area scoring comparing 2016, 2015, with 2014 EQR score results:
Function Area Alliance BHC
Year>>>> 2016 (3rd YR) 2015 (2ndYR) 2014 (1st YR)
Total Summary Score: 94.4% 85.64% 70.17%
Administration 91% 100% 100%
Provider Services 94% 100% 62.07
Enrollee Services 95% 58.54% 58.54%
Quality Improvement 94% 71.43% 85.71%
Utilization Management
98% 89.13% 73.91%
Grievances & Appeals (new section)
95% n/a n/a
Delegation 100% 100% 100%
Program Integrity (new section)
93% n/a n/a
Financial (new section) 100% n/a n/a
State-Mandated Services
N/A 100% 50%
Corrective Action items (CAPs):
2016 – We have 13 CAPs to fix. (30 days to correct)
2015 – We had 15 CAPs to fix.
2014 – We had 33 CAPs to fix. Best Practice Recommendations (BPRs):
2016 – We have 44 BPRs items to fix. (9 months to implement BPRs)
2015 – We had 8 BPRs items to fix.
2014 – We had 18 BRP items to fix. Next steps related to the Report:
ELT – review the Alliance 201 EQR Report – discuss for disputes.
Alliance CAI Plan – to be submitted and approved by EQRO vendor CCME within 30 days.
Alliance BPR Tracking log for DHHS IMT.

EAQR CAP 11 - Continuous Quality Improvement Committee – DRAFT CHARTER Purpose The CQI Committee is the venue for the review and assessment of all performance data and quality activities for Alliance. The CQI Committee meets at least monthly to review clinical and provider network performance data and review operations. Responsibilities As a committee within the Alliance CQI structure, the CQI Committee is responsible for identifying and reporting:
Key areas of risk or concern for the committee;
Reports or data that support/identify these areas being considered a risk/concern;
An analysis of the risk/concern, including how long has been a concern, the impact on Alliance departments, or the organization as a whole;
Committee response to the area of risk/concern, including action steps, timeframes, and when CQI Leadership Team will receive an update;
How issues identified in your committee are communicated to other affected committees;
The results of any Quality Improvement activities implemented to address risk or concern. The CQI Committee is responsible for the implementation and evaluation of the Alliance Quality Management Plan, monitoring of quality improvement goals and activities and identifying opportunities for improvement within the provider network and Alliance operations. Data Reporting/Review The committee examines data and information for trends to identify areas of risk for the organization and areas where there has been or needs to be performance improvement. Relationships The committee reviews state reports, information and reports to be shared with the board of directors. Information reviewed with strategies for improvement are shared with the Global Quality Management Committee of the Board for additional review, feedback, recommendations and approval. Membership The committee is composed of:
Director of Quality Management - chair
Chief Executive Officer
Chief Compliance Officer
Medical Officer
Executive VP – Chief Financial Officer
Executive VP – Chief Operations Officer
Executive VP – Care Management
Senior VP - Community Relations
Senior VP – Clinical Operations
Senior VP – Chief Information Officer
Senior VP – Organizational Effectiveness
Director of Consumer Affairs
Medicaid Contract Manager Attendance 1. Committee members are required to attend at least 80% of meetings each fiscal year.

2. A committee member who is legitimately unable to attend a meeting will inform the committee chair prior to the meeting and may designate another staff member to attend as a representative. 3. The committee may replace a member who cannot consistently attend meetings with another department staff member. Quorum 1. A quorum requires the presence of at least 51% of committee members or designated representatives.

CAP 11 – CQI Committee Attendance – DRAFT Revised 4-28-2017 EQRO Findings: The Continuous Quality Improvement (CQI) Committee is the venue for the review and assessment of all performance data and quality activities for Alliance. The CQI Committee meets at least monthly to review clinical and provider network performance data and review operations. The CQI Committee is comprised of 11 internal MCO staff members. Four of nine voting members attended less than half of the meetings in the past year. Corrective Action: Ensure that all CQI Committee voting members attend meetings regularly. Current Process: 1. CQI Committee meetings are consistently held on the fourth Wednesday of each month. 2. A recurring Outlook invitation is sent to all committee members. 3. Members receive an email reminder prior to each meeting. 4. Attendance is tracked via a sign-in sheet, and recorded in the meeting minutes. Proposed Actions: 1. Modify the CQI Committee’s minutes to track member attendance during the current fiscal year
(July – June) (see accompanying draft version). 2. Create quarterly reports on committee attendance, and include a final report in the annual QM
Evaluation.
3. Establish a meeting attendance standard of 80% of meetings in a fiscal year. 4. Allow a member to inform the chair prior to the meeting that the member cannot attend and will be
sending a representative from their department. 5. Replace a member who cannot consistently attend CQI Committee meetings with another
department staff member.
6. Set a quorum of least 51% of committee members or designated representatives. Additional Submissions: 1. Draft committee charter
2. Draft meeting minutes form

Wednesday, March 22, 2017 CONTINUOUS QUALITY IMPROVEMENT (CQI)
FY 2017 MEMBER ATTENDANCE (P = Present; A = Absent; = Not a Member):
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun
Tedra Anderson-Brown, MD Chief Medical Officer P P P P P P P P
Michael Bollini, PhD Executive VP – Chief Operations Officer A P A P P P P P
Courtney Cantrell, PhD Senior VP – Clinical Operations P
Joey Dorsett, BS-Pharm Senior VP – Chief Information Officer A A P A P P P P
Kelly Goodfellow, MBA Executive VP – Chief Financial Officer P P A P A P P P
Amanda Graham, MS, LPC, NCC Senior VP – Organizational Effectiveness A P P A P A P A
Geyer Longenecker, JD Director, Quality Management P P P P P P P P
Ken Marsh Medicaid Contract Director P P P P P P P P
Beth Melcher, PhD Interim Executive VP – Care Management P P P P P P P P
Ann Oshel Senior VP – Community Relations P P A P P P P P
Monica Portugal, MA, CHC Chief Compliance Officer A A P P A A A P
Rob Robinson, MA, LCAS Chief Executive Officer A A P P A P A P
Sean Schrieber Executive VP – Care Management A A P A P
Doug Wright Director, Consumer Affairs P P A P A P P P
SCRIBE: Geyer Longenecker GUEST(S) PRESENT: 1. WELCOME AND INTRODUCTIONS: Courtney Cantrell
2. REVIEW OF THE MINUTES:
AGENDA ITEMS: DISCUSSION: NEXT STEPS: TIME FRAME:
3. Follow-up Items
4. Data Review (Geyer)
a. LME-MCO Monthly Report – Feb. b. LME-MCO Monitoring Summaries – Dec., Jan. c. Performance Contract Reports – Q1, Q2 FY17 d. Performance Standards Dashboard
5. Quality Improvement Activities
a. Care Coordination assignment - Geyer b. Medicaid appeals review - Geyer

Wednesday, March 22, 2017 CONTINUOUS QUALITY IMPROVEMENT (CQI)
AGENDA ITEMS: DISCUSSION: NEXT STEPS: TIME FRAME:
c. Complaints resolution TAT - Geyer d. EQRO update – Geyer, Ken
6. Committee Quality Improvement Reports a. Budget/Finance b. CCMT c. Community Relations d. Compliance e. IT f. Provider Networks g. UM
7. Organization Trends (Amanda)
8. New Business
Adjourn
NEXT MEETING Wednesday, April 26, 2017 – 1:00p-3:00p – Board Room 208

Quality Improvement Projects
Presentation to Global Quality Management Committee
(May 2017)

Quality Improvement Projects
Executive Summary for FY 17:
o Open/Active: 9 projects
o Closing by end of June: None
o May close by end of calendar year: 2 projects (Crisis and First Responder)
o Closed-conducting post-closure analysis: 4 projects (2 completed, 2 due later in Spring)
o QM no longer monitoring (post-closure improvement sustained): 2 projects
Quality Improvement ProjectsSuccesses:
o First Responder QIP – Continued improvement in satisfactory calls (1st Q: 65%, 2nd Q: 79%)
o Crisis Services QIP - WakeBrook CAS closures continue to decline since October 2016:
o Avg: Back Door – 14%, Front Door – 9%
o Goals: Back Door – 21%, Front Door – 13%
o Continued high level of consistency in Inter-Rater Reliability (IRR) studies with UM Care Managers (IDD and MH/SA)
o Sustained adherence to Alliance procedures for greeting staff who call from providers (MH/SA, IDD will be tested later in Spring)
Quality Improvement ProjectsRed Flags:
o Crisis QIP (Wake County): Reduction in CAS closures NOT due to intervention - fewer individuals showing to Open Access clinic after regular business hours even though facility is open later every weekday
o Access to Care QIP: Continued poor show rate of individuals identified as Urgent showing for care within 2 days, no overall improvement in individuals showing for care in 14 days (Routine) although those that receive reminder call are more likely to show than those that do not
Quality Improvement Projects
Recommendations for FY 18:
o No new QIPs are being recommended
o Even if the Crisis and First Responder projects close early in FY 18, we are still meeting all current contract, EQR, and URAC requirements (see matrix)
o QM is leading efforts to identify and improve on internal performance in FY 18—some of this work may lead to a QIP by FY 19
o Requesting GQMC approval for QM to stop monitoring IDD IRR since improvement was sustained (FY 15 QIP)

Detailed Results for QIPs

Access to Care - Improve Show Rate for Emergent Callers
Goal:
o 77% of callers identified as needing Emergent Care show for the care within 2:15 hours (state benchmark, which we feel is unreasonable, is 97%)
Interventions:
o Revised Mobile Crisis services (start: July 2017, delayed start)
o Improve internal coding and data entry (start: January 2017)
o Conducted another barrier analysis to identify any other interventions that may improve performance
FY 17 QIPs

Access to Care - Improve Show Rate for Emergent Callers
Results:
Next Steps:
o Project Advisory Team will meet in April to review barrier analysis and impact of internal review of data entry
FY 17 QIPs
Baseline(FY16Q4:Apr-Jun 2016)
FY 17, Q1:
Jul-Sep 2016
FY 17, Q2:
Oct-Dec 2016
FY 17, 3:
Jan-Mar 2017
FY 17, Q4:
Apr-Jun 2017Goal
67% 84% 59% 77%

Access to Care – Improve initiation in services for Routine & Urgent callers
Goals:
o Increase consumer initiation in services based on need—63% within 14 days for Routine and 62% in 2 days for Urgent callers
FY 17 QIPs
*All claims for Q2 most likely not submitted, yet.
Access to Care-Routine/Urgent
Methodology changes for FY 17
o Use only claims submitted to calculate measure due to inaccuracy of Alpha report
o Baseline-Routine: FY 16, Q1; Urgent: FY 16, Q4
Interventions-Routine:
o Reminder calls a few days before appointment (start: January 2016)
o Feedback letters to providers (start: February 2017)
FY 17 QIPs

Access to Care-Routine/Urgent
Interventions-Urgent:
o Expanded hours of Open Access on Friday late afternoons in Wake County (start: April 1, 2017)
o Interventions to improve engagement of CJ population (under development)
o Feedback letters to providers (start: February 2017)
FY 17 QIPs

Access to Care-Routine/Urgent
Results:
Routine callers:
FY 17 QIPs
Time Period Total # of Calls # show in 14 % show in 14
FY 16, Q1 (Jul-Sep 2015) 1,051 424 40%
FY 16, Q2 (Oct-Dec 2015) 959 430 45%
FY 16, Q3 (Jan-Mar 2016) 778 370 48%
FY 16, Q4 (Apr-Jun 2016) 806 361 45%
FY 17, Q1 (Jul-Sep 2016) 753 365 48%
FY 17, Q2 (Oct-Dec 2016)* 699 260 37%
*All claims for Q2 most likely not submitted, yet.

Impact of Reminder Calls: Attended vs. No Show*
Of those individuals who attended their appointments, 52% made direct contact with an Access staff person reminding them of their appointment. Another 28% received a message. A total of 80% received some kind of reminder about their appointment. Conversely, only 31% of those callers indicated as “No Show” to their appointment spoke to an Access staff person regarding the appointment and 28% received a message. In total, 59% of individuals not showing for appointment received a reminder call.
*The appointment status for the remaining calls were coded as Other: canceled, error in data, consumer did not meet criteria for Care Coordination, etc.
52%
28%
13%
0%
1%
6%
1-Contact
2-Left message
3-Unable to contact
4-Appt rescheduled
5-Consumer refused
No call made/Unk
Attended in 14 Days (n=344)
31%
28%
29%
0%2%10%
1-Contact
2-Left message
3-Unable to contact
4-Appt rescheduled
5-Consumer refused
No call made/Unk
Indicated as “No Show” to Appointment (n=90)
FY 17 QIPs

Urgent Callers - Percent Met
The table below compares overall performance based on claims and attendance status:
Time Period Total # of Calls # show in 2 % show in 2
FY 16, Q4 (Apr-Jun 2016)-claims 452 84 19%
FY 16, Q4 (Jul-Sep 2016)-attend status 452 122 27%
FY 17, Q1 (Jul-Sep 2016)-claims 479 89 19%
FY 17, Q1 (Jul-Sep 2016)-attend status 479 122 26%
FY 17, Q2 (Oct-Dec 2016)-claims 447 67 15%
FY 17, Q2 (Oct-Dec 2016)-attend status 447 123 28%
FY 17 QIPs

Access to Care-Routine/Urgent
Next Steps:
o Continue to conduct reminder calls to all Routine callers, making every effort to contact the consumer or guardian directly
o Make the reminder calls at different times of the day (even after regular business hours) if it increases the likelihood of making direct contact with consumer or guardian
o Conduct Multivariate statistical analysis of reminder calls with larger samples sizes to control for confounding variables1
o Analyze impact of expanded Open Access for Urgent callers and feedback letters for Routine & Urgent callers
FY 17 QIPs
1Pourhoseingholi, M. A., Baghestani, A. R., & Vahedi, M. (2012). How to control confounding effects by statistical analysis. Gastroenterology and Hepatology From Bed to Bench, 5(2), 79–83
Improve Care Coordination for Individuals Discharging from Inpatient
Goal:
o 80% of individuals assigned to Care Coordinator, and recently discharged from inpatient, receive contact within 2 business days of discharge
Interventions:
o Training/coaching Care Coordination staff, revised desk reference
Next Steps:
o Project Advisory Team met 2/20, decided to revise measures to include contact with consumer AND provider
FY 17 QIPs

Improve Crisis Services in Wake and Cumberland Counties
Goals:
o Reduce ED admissions of youth in best practice pilot programs (FCT and Enhanced TFC) in Cumberland County
o Increase the number of consumers utilizing Open Access (Tier II) after 3:00 PM by 20%
o Reduce percentage of time that WakeBrook CAS in Wake County is on diversion by 2%
FY 17 QIPs

Crisis Services QIP
Interventions (Cumberland):
o Family Centered Treatment (FCT) and Enhanced Therapeutic Foster Care (TFC) pilots
Interventions (Wake):
o Encourage a provider offering Open Access (Tier II) to open after regular business hours
Update:
o Measure #1-Promising results from Cumberland pilots (Baseline: 19%, lower ED/Crisis/Inpatient admissions post discharge)
o Wake: Provider expanded hours of Tier II on April 1, now open until 7 PM on Mondays – Thursday, until 5 on Friday (Baseline: 0.24%)
FY 17 QIPs

Crisis QIP Measures: 2. Increase # of consumers using Open Access after 3 PM (Wake County)Data Drill-Down:
Same Day Acess-Monarch
3-Month Breakdown
12:00-4:59 000-459
5:00-8:59 500-859
9:00-11:59900-1159
12:00-2:59 1200-1459
3:00-4:59 1500-1659
5:00-6:59 1700-1859
7:00-9:00 1900-2059
9:00-11:59 2100-2359
Consumers Presenting (but not
admitted) to WakeBrook CAS
Feb-Apr 2016 11 28 76 91 42 30 26 18
May-July 2016 16 43 79 88 44 35 28 25
Aug-Oct 2016 12 17 69 65 45 35 22 32
# of Individuals presenting to
Monarch
Feb-Apr 2016 (Baseline)
not open 254 392 183 >10 >10 not open not open
May-July 2016 (Intervention
began 1 day/week)not open 209 338 140 21 11 not open not open
Aug-Oct 2016 (Intervention
expanded x2 days)not open 191 415 137 11 >10 not open not open
Even though Open Access has continued to expand hours, the number of individuals presenting during those hours, after the initial three months, has decreased. Data from Nov-Jan is being analyzed to determine if trend continues.
FY 17 QIPs

Crisis QIP Measures: 3. Reduce % of operating hours that CAS’ back door (IVC) is closed (Wake County)
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
2013 18% 11% 1% 4%
2014 6% 12% 24% 27% 34% 32% 24% 35% 43% 22% 32% 25%
2015 32% 34% 56% 50% 54% 38% 30% 36% 51% 42% 44% 30%
2016 41% 43% 43% 50% 50% 32% 27% 33% 30% 7% 6% 20%
2017 24%
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
Back Door Diversions
2013 2014 2015 2016 2017
Goal: 21%Baseline (Jan-June 2014): 23%, Measure #1 (Jan – June 2016): 43%
FY 17 QIPs

Crisis QIP Measures: 4. Reduce % of operating hours that CAS’ front door (“full diversion”) is closed (Wake County)
Goal: 13%Baseline (Jan-June 2014): 15%, Measure #1 (Jan – June 2016): 20%
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
2013 7% 6% 0% 2%
2014 5% 5% 10% 19% 26% 22% 19% 26% 29% 17% 24% 16%
2015 16% 13% 35% 29% 30% 23% 8% 17% 22% 20% 24% 13%
2016 17% 24% 20% 25% 27% 10% 13% 16% 12% 4% 3% 12%
2017 13%
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
Front Door Diversions
2013 2014 2015 2016 2017
FY 17 QIPs

Crisis QIP Measures 3. & 4. Reduce % of operating hours that CAS’ front and back doors are closed (Wake County)
Front Door: Sharp decrease in closures starting in October (leadership change at CAS; Additional Beds added to Inpatient), Avg % closed:• After leadership change: Oct 2016 – Jan 2017: 14%• Prior to leadership change/additional beds:
• Jun-Sept 2016: 31%• Oct 2015 – Jan 2016: 39%• Oct 2014 – Jan 2015: 28%
Back Door (IVC): Similar trend in decreases of closures starting in October 2016, Avg % closed:• After leadership change/additional beds: Oct 2016 – Jan 2017: 8%• Prior to leadership change:
• Jun-Sept 2016: 13%• Oct 2015 – Jan 2016: 16%• Oct 2014 – Jan 2015: 18%
FY 17 QIPs

Crisis Services QIP
Next Steps:
o Network Development meets on a regular basis with provider to discuss low showing at Open Access after regular business hours, provider has made a leadership change at Open Access clinic
o Network Development will schedule meeting with provider and WakeBrook to improve communication between two agencies
FY 17 QIPs
First Responder – test crisis lines of providers after business hours
Goals: 85% of calls meet standard for satisfactory (call goes through successfully and it is answered live or returned within 1 hour)
Interventions:
o Providers assigned to “Tiers” based on last FY’s performance (some called more frequently, others less)
o Written feedback to all providers after calls
o Refer to Compliance the providers who continue to score “unsatisfactory”, issue Plan of Correction if poor performance continues
o Compare test results with actual data of consumers, open to enhanced services, using crisis services
FY 17 QIPs

First Responder QIP
Results:
o No Plans of Correction (POCs) issued after 1st Measurement
o One provider was referred to Compliance after 2nd Measurement
o Calls for 3rd measurement currently taking place
Call Cycle1st
Measurement2nd
Measurement3rd
Measurement4th
MeasurementSatisfactory 65% (N=17) 79% (N=33)Unsatisfactory 35% (N=9) 21% (N=9)Total calls made 26 42
FY 17 QIPs

Intensive In-Home – Improve quality of IIH services
Goals: Reduce use of crisis services, reduce behavioral health interference with daily activities, and decrease severity of mental health symptoms.
Project Start Date: 1/1/2013; Project End Date: still active
Interventions:
o IIH providers to implement specific, family-focused EBP with external fidelity monitoring
o Training and technical assistance to providers
FY 17 QIPs

Intensive In-Home QIP
Update:
o Evidence based practice models selected, Alliance offered subsidized trainings in June 2016
o Implementation plans included in FY17 contracts, implementation deadline March 2017
o Collect post-intervention data late 2017
FY 17 QIPs

Improve Person-Centered Plans
Goals:
o at least 55% of health and safety quality elements are met or partially met
Interventions:
o Focus on service lines with fewest health/safety elements met (substance abuse services)
o Reached out to SA providers for input on improving performance, will provide targeted training
o Revised review tool to expand on health/safety elements
FY 17 QIPs
Improve Timeliness of Services for IDD Consumers
Improve timeliness of services for individuals who recently received Innovations slots
Goal:
o 85% receive services within 45 days of plan approval
Update:
o Project Advisory Team, along with other subject matter experts, conducted comprehensive process map to identify bottlenecks in process
o Gathering more data on bottlenecks to identify interventions
FY 17 QIPs

TCLI – Increase private housing options for TCLI population
Goals:
o Increase the # of housing units available within the private sector
o Increase the # of units that get rented to TCLI pop
Interventions (under development by PAT):
o Training to property owners on Alliance, housing program, anti-stigma and recovery oriented system of care.
o Look at measuring level of change in renters’ outlook and if there was a difference in their willingness to rent to this population.
FY 17 QIPs
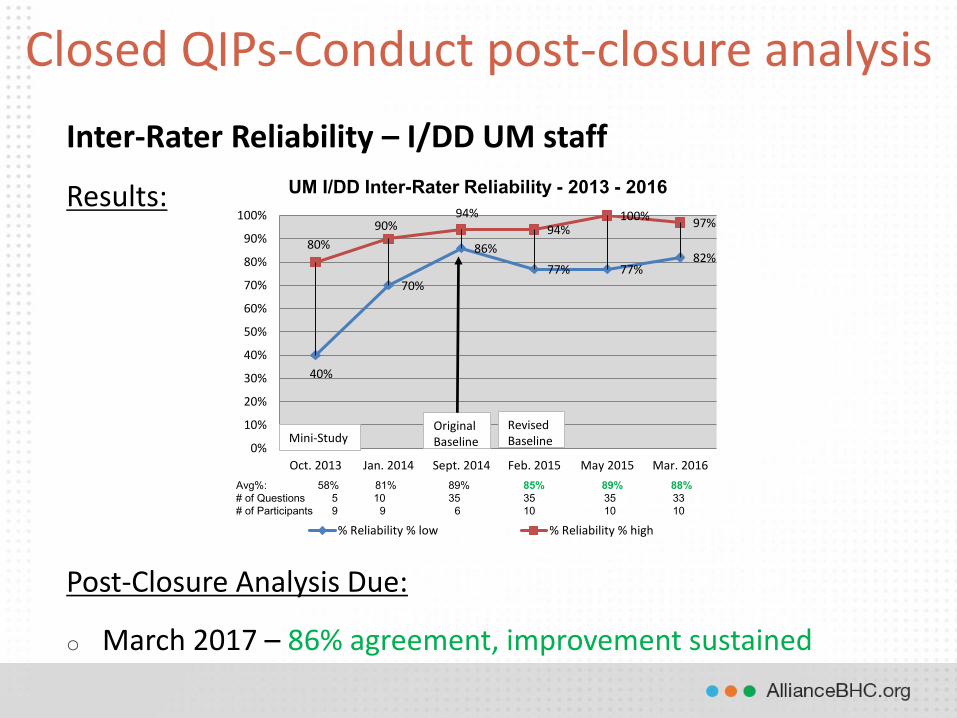
Inter-Rater Reliability – I/DD UM staff
Results:
Post-Closure Analysis Due:
o March 2017 – 86% agreement, improvement sustained
Closed QIPs-Conduct post-closure analysis
40%
70%
86%
77% 77%82%
80%
90%94%
94%100%
97%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Oct. 2013 Jan. 2014 Sept. 2014 Feb. 2015 May 2015 Mar. 2016
% Reliability % low % Reliability % high
UM I/DD Inter-Rater Reliability - 2013 - 2016
Avg%: 58% 81% 89% 85% 89% 88%# of Questions 5 10 35 35 35 33# of Participants 9 9 6 10 10 10
Mini-StudyRevised Baseline
Original Baseline
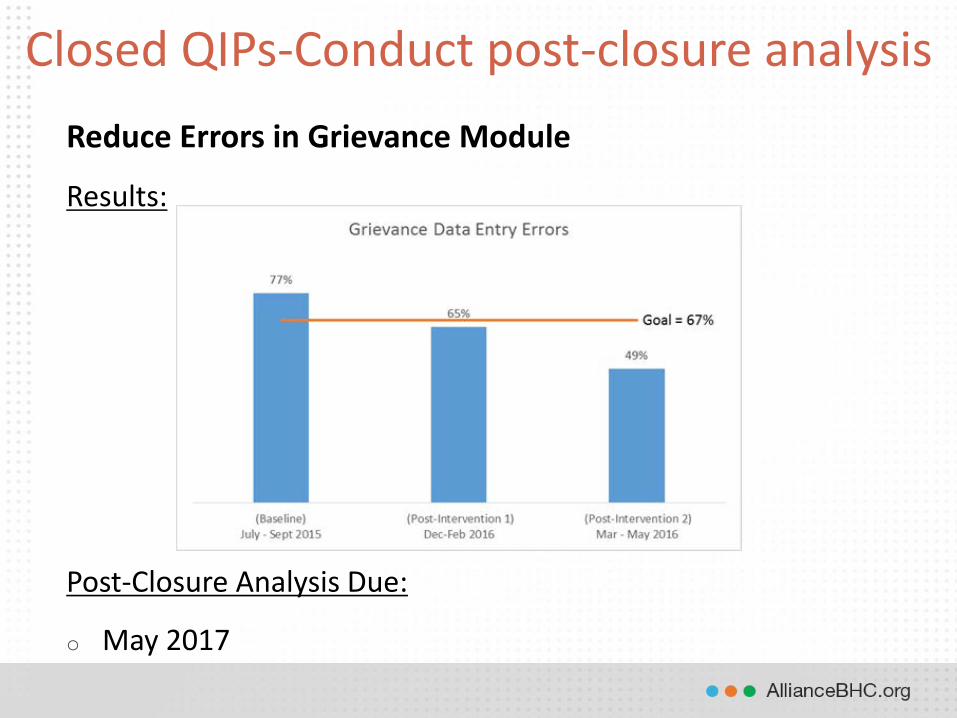
Reduce Errors in Grievance Module
Results:
Post-Closure Analysis Due:
o May 2017
Closed QIPs-Conduct post-closure analysis

UM Call Monitoring– MH/SA UM staff
Results: 91% met (October 2015), Goal: 85%
Post-Closure Analysis:
o Oct. 2016: 86% met, improvement sustained, QM stopped monitoring (approved by GQMC in February 2017)
Closed QIPs-Conduct post-closure analysis
14%
82%91%
0%
20%
40%
60%
80%
100%
Oct 2014 July 2015 Oct 2015
UM MHSA Calls
Met Not Met
Benchmark = 85%

UM Call Monitoring– I/DD UM staff
Results: 98.6% met (June 2016)
Post-Closure Analysis Due:
o June 2017
Closed QIPs-Conduct post-closure analysis
1 16
70
0
10
20
30
40
50
60
70
80
N NA Y
Count of Staff followed SOP ? (first name, title, agency)

Alliance FY 18 QIPs-proposed1 CMS Projects (for EQR)2 URAC Projects
QIP Requirements
Improve Crisis
Services-Cumb &
Wake1
Improve Access
to Care (Urgent,
Routine)1, 2 First Responder1, 2
Best Practices-
IIH2 Improve PCPs2
Initiation (IDD)
in 45 days2
Improve Access to
Care (Emergent)1, 2
Care Coordination
(MH/SA)1
(1st Contact from
Inpt Discharge) TCLI Project
Leads:
Primary: Damali
Secondary:
Michelle
Primary: Tina
Secondary: Wes
Primary: Jose
Secondary: Tina
Primary: Damali
Secondary: Jose
Primary: Shruti
Secondary: Tina
Primary: Shruti
Secondary:
Andrea
Primary: Tina
Secondary: Jose
Primary: Jose
Secondary: Brittany
Primary: Shruti
Secondary: Jose
Date Opened 8/1/2015 7/1/2014 9/1/2012 1/1/2013 2/1/2013 7/1/2016 7/1/2016 7/1/2016 1/1/2017
3 QIPs X X X X X X X X XReduce need for inpatient at community
hospitals for Medicaid recipients with
medical/MHDDSA X X X X XReduce use of crisis & ED services for hi-
risk Medicaid recipients X X X X X
At least 1 with Clinical focus X X X X X
At least 1 with Non-Clinical focus X X X X
2 QIPs per URAC program-UM X X
2 QIPs per URAC program-Call Center X X
2 QIPs per URAC program-Health Network X X X X X
At least 1 QIP addresses consumer safety X X X X
At least 2 QIP topics measured (1 clinical
and 1 non-clinical) use one or more
quality indicators--changes in health
status, functional status, or satisfaction X X X X X X X XAt least 2 QIP topics measured (1 clinical
and 1 non-clinical) use multiple data
sources X X X X X X XTopics identified through continuous data
collection & analysis X X X X X X X X X(Suggestion) At least 1 focuses on entire
MCO catchment area X X X X X X X(Suggestion) At least 1 focuses on local
communities X X
Continuation Projects

1 CMS Projects (for EQR)2 URAC Projects
QIP Requirements
Improve Crisis
Services-Cumb &
Wake1
Improve Access
to Care (Urgent,
Routine)1, 2 First Responder1, 2
Best Practices-
IIH2 Improve PCPs2
Initiation (IDD)
in 45 days2
Improve Access to
Care (Emergent)1, 2
Care Coordination
(MH/SA)1
(1st Contact from
Inpt Discharge) TCLI Project
Continuation Projects
Required in at least one of our contracts
or by an auditor X X X X X X X XProject Advisory Teams:
Link to Existing Committee (provide at
least quarterly updates to committees) UM
UM/Provider
Network Provider Network
Provider
Network
Provider
Network UM UM UM
TCLI Steering
Committee
Membership: (in addition to primary &
secondary leads) Beth Melcher Carlyle Johnson Danny Merwin Dr. Foster Amy Johndro Dr. Foster
MD (CMO)-Dr. M,
interim Nave TCLI Workgroup
Nave Sands Tiffany Harris Tonia Joyner Carlyle Johnson Robert Bell Kelly Goodfellow Margaret B. Courtney/Vera
Tina Howard Jenny Edwards Kathy Niblock Kathy Niblock April Parker Jarret Stone Jenny Edwards Beth Melcher
Suzanne Marens Tasha Griffin Amy Johndro Beth Melcher Sarah Simms Beth Melcher Nave (Karen G.) Miki
Margaret Brunson Suzanne Marens
Rose-
Ann/Migeya/
Shannon (PN) April Parker Matt Ruppel Lloyd M. Damali Alston Tina
Courtney Michael Bollini
Provider Rep:
Wendy Wenzel Tasha Griffin Tasha Griffin Jeffrey Payne Beth Melcher Wes
Kate Peterson
Provider Rep:
Lena klumper Nay Headley Danny Merwin
April Parker (or
designee)
Kristee Jordan
Provider Rep:
Renee White
Provider Rep:
Sara Leonard

(Back to agenda)
8
ITEM: FY18 Public Hearing and Budget Approval DATE OF BOARD MEETING: June 1, 2017 BACKGROUND: Per GS 159-12 (b) a public hearing shall be held to allow any persons who wish to be heard on the budget to appear. The FY 2017-2018 budget is also being presented to the Board for approval and adoption per GS 159-13. REQUEST FOR AREA BOARD ACTION: Approve the proposal. CEO RECOMMENDATION: Approve the proposal. RESOURCE PERSON(S): Robert Robinson, CEO; Kelly Goodfellow, CFO
Alliance Behavioral Healthcare BOARD OF DIRECTORS
Agenda Action Form

1 | F Y 1 8 R e c o m m e n d e d B u d g e t
FY18 APPROVED BUDGET JUNE 1, 2017

2 | F Y 1 8 R e c o m m e n d e d B u d g e t
Alliance Behavioral Healthcare Annual Budget
FY 2017-2018
Board of Directors
Christopher Bostock, Chair
Cynthia Binanay, Vice Chair
Durham County Wake County
Cynthia Binanay George Corvin, MD
Commissioner Heidi Carter James Edgerton
Phillip Golden Commissioner Greg Ford
Curtis Massey William Stanford, Jr.
George Quick Vacancy
Amelia Thorpe McKinley Wooten, Jr.
Lascel Webley, Jr. Vacancy
Cumberland County Johnston County
Christopher Bostock Vacancy
Lodies Gloston
John Griffin, Ed. D
Commissioner Michael Boose
Robert Robinson, CEO
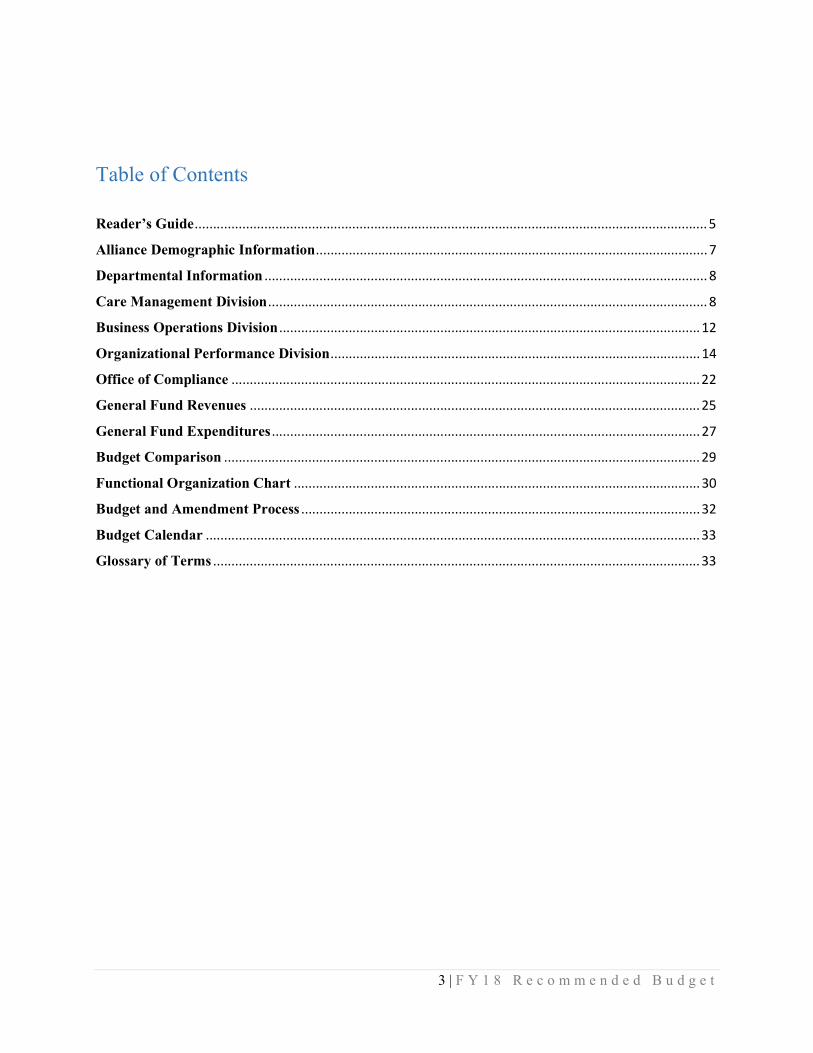
3 | F Y 1 8 R e c o m m e n d e d B u d g e t
Table of Contents
Reader’s Guide ............................................................................................................................................ 5
Alliance Demographic Information ........................................................................................................... 7
Departmental Information ......................................................................................................................... 8
Care Management Division ........................................................................................................................ 8
Business Operations Division ................................................................................................................... 12
Organizational Performance Division ..................................................................................................... 14
Office of Compliance ................................................................................................................................ 22
General Fund Revenues ........................................................................................................................... 25
General Fund Expenditures ..................................................................................................................... 27
Budget Comparison .................................................................................................................................. 29
Functional Organization Chart ............................................................................................................... 30
Budget and Amendment Process ............................................................................................................. 32
Budget Calendar ....................................................................................................................................... 33
Glossary of Terms ..................................................................................................................................... 33

4 | F Y 1 8 R e c o m m e n d e d B u d g e t
June 1, 2017 Alliance Board Members, We are pleased to share with you our FY18 budget for your approval. It reflects a few changes to our non-Medicaid budget from the recommended budget that was presented to you on May 4th but the total funding amount is unchanged. As I mentioned in my introduction to the recommended budget document, this version continues to reflect Alliance’s vision to more effectively and strategically manage our all of our funding sources to create a benefit plan that allows individuals across our region to benefit uniformly from the services and supports available through our provider network. It focuses on key initiatives to help children and youth receive the treatment they need in their communities, rather than in out-of-home placements, and to enhance our continuum of services available to adults and children who are experiencing a behavioral health crisis. We thank you for your continued participation and wise counsel during this budget process. Best Regards,
Rob Robinson Chief Executive Officer

5 | F Y 1 8 R e c o m m e n d e d B u d g e t
Reader’s Guide FY 2017 - 2018 is the sixth annual budget presented for Alliance Behavioral Healthcare (Alliance). This section is provided to help the reader understand the budget by explaining how the document is organized. This document details the budget for fiscal year 201-2018 for Alliance’s administrative and service operations covering Cumberland, Durham, Johnston and Wake counties. The budget year begins July 1, 2017 and ends June 30, 2018. The document will show how the funds are allocated and how they will be spent. Alliance Behavioral Healthcare LME/MCO will have one fund called the General Fund. The General Fund will account for all administrative and service operations and will be divided into functional areas for Administration, Medicaid Services, State Services, Local Services, and Grant Funds, when applicable. Revenues and Expenditures of the General Fund The categories of the revenue and expenditures are the same. They include the following: Administration Alliance Behavioral Healthcare is administratively funded through a combination of the Medicaid waiver, state LME allocation, and county administrative contribution. Alliance began the management of Medicaid services under a waiver according to Session Law 2011-264 House Bill 916 on February 1, 2013. These funds refer to the administration dollars allocated under a contract with the NC Division of Medical Assistance. The funds are allocated based on a per member per month basis. The members per month budgeted is based on historical experience and projections. The NC Division of Mental Health, Developmental disabilities, and Substance Abuse services (NC DMH) continue to allocate funds to administer state and federal block grant dollars for the purposes of serving the non-Medicaid population. Cumberland, Durham, and Wake counties allocate 1% of the county dollars in administrative support for the management of their dollars in serving consumers in their respective county. Miscellaneous This category is to account for any funds received during the fiscal year that do not fall into one of the above mentioned categories and are not significant enough to require their own category. The funds roll up into the Administrative budget. Medicaid Services Alliance Behavioral Healthcare began the management of Medicaid services under a waiver according to Session Law 2011-264 House Bill 916 on February 1, 2013. These funds refer to the dollars allocated under the contract with the NC Division of Medical Assistance to provide services to Medicaid enrollees of Cumberland, Durham, Johnston, and Wake counties.

6 | F Y 1 8 R e c o m m e n d e d B u d g e t
State Services These funds represent state allocated dollars for Cumberland, Durham, Johnston, and Wake communities to provide services for non-Medicaid citizens with mental health, intellectual/developmental disabilities and substance abuse needs. The funds include Federal Block Grant dollars as allocated from the NC DMH. Local Services These funds represent the Cumberland, Durham, and Wake county allocations to Alliance to provide services for citizens with mental health, intellectual/developmental disabilities, and substance abuse needs in their respective counties. Grants When applicable, grant funds are those that are specified for a particular project or program. Draft Budget Ordinance A draft budget ordinance is being included for informational purposes. Additional Information The basis of accounting and budgeting for Alliance Behavioral Healthcare is modified accrual per G.S. 159-26. This means that revenues are recorded in the time period in which they are measurable and available. Revenues are recognized when they are received in cash. Expenditures are recognized in the period when the services are received or liabilities are incurred. This document was prepared by Alliance Behavioral Healthcare Business Operations and is available online at www.alliancebhc.org. If further information is needed, please contact Kelly Goodfellow, Executive Vice President/CFO, at 4600 Emperor Blvd, Durham, North Carolina 27703 or by email at [email protected].
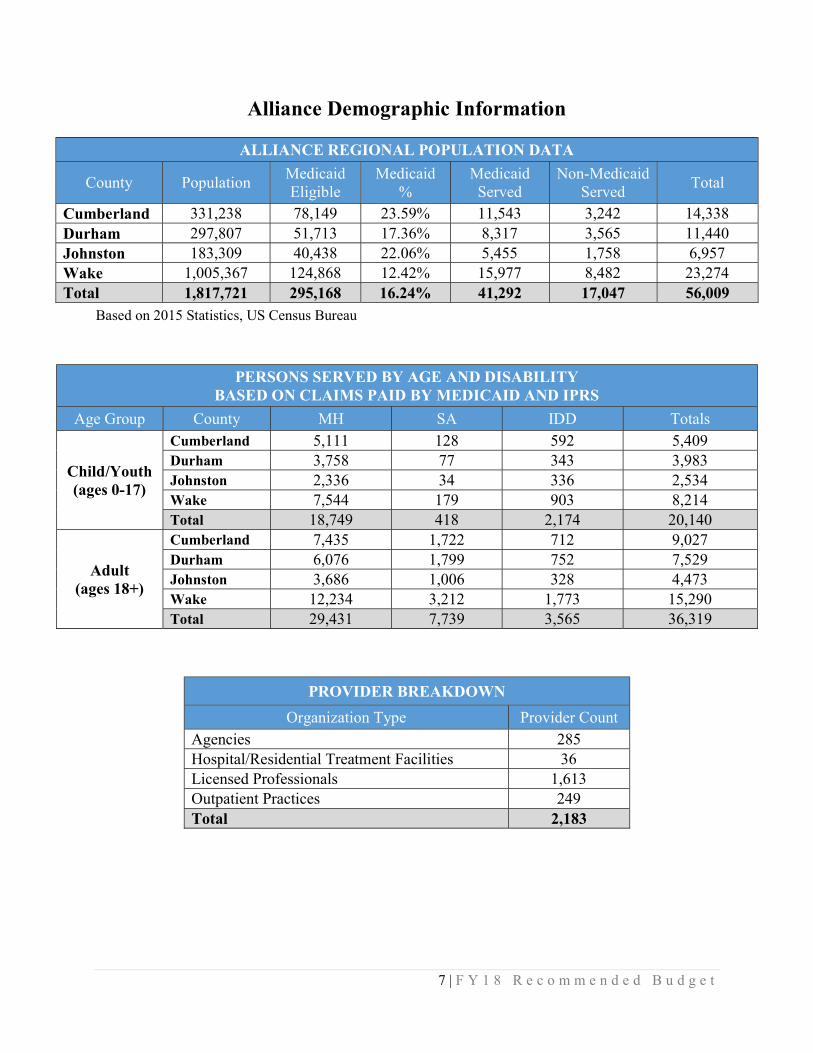
7 | F Y 1 8 R e c o m m e n d e d B u d g e t
Alliance Demographic Information
ALLIANCE REGIONAL POPULATION DATA
County Population Medicaid Eligible
Medicaid %
Medicaid Served
Non-Medicaid Served
Total
Cumberland 331,238 78,149 23.59% 11,543 3,242 14,338 Durham 297,807 51,713 17.36% 8,317 3,565 11,440 Johnston 183,309 40,438 22.06% 5,455 1,758 6,957 Wake 1,005,367 124,868 12.42% 15,977 8,482 23,274 Total 1,817,721 295,168 16.24% 41,292 17,047 56,009
Based on 2015 Statistics, US Census Bureau
PERSONS SERVED BY AGE AND DISABILITY BASED ON CLAIMS PAID BY MEDICAID AND IPRS
Age Group County MH SA IDD Totals
Child/Youth (ages 0-17)
Cumberland 5,111 128 592 5,409 Durham 3,758 77 343 3,983 Johnston 2,336 34 336 2,534 Wake 7,544 179 903 8,214 Total 18,749 418 2,174 20,140
Adult (ages 18+)
Cumberland 7,435 1,722 712 9,027 Durham 6,076 1,799 752 7,529 Johnston 3,686 1,006 328 4,473 Wake 12,234 3,212 1,773 15,290 Total 29,431 7,739 3,565 36,319
PROVIDER BREAKDOWN
Organization Type Provider Count Agencies 285 Hospital/Residential Treatment Facilities 36 Licensed Professionals 1,613 Outpatient Practices 249 Total 2,183

8 | F Y 1 8 R e c o m m e n d e d B u d g e t
Departmental Information Care Management Division Care Management at Alliance Behavioral Healthcare is a data-informed, collaborative effort that identifies and addresses the full range of medical, functional, social, emotional, and environmental needs across all populations in order to improve health outcomes by focusing on prevention and person-directed care. Clinical Operations
Brief Description of Department and Units The Clinical Operations Department is comprised of two units and receives clinical oversight from the Alliance Senior VP for Clinical Operations and the Chief Medical Director.
MH/SA and IDD Utilization Management (UM) are responsible for authorizing services and monitoring and managing consumers during an episode of care. Activities include monitoring utilization of services authorized, reviewing effectiveness of treatment interventions and making recommendations to improve the effectiveness of consumer treatment plans.
MH/SA and IDD Care Coordination are responsible for working with specific high-risk populations identified within the waiver contract and priority populations that have been identified by Alliance, including individuals with high ED utilization patterns. Care Coordination links consumers with both services and supports and helps eliminate barriers that allow consumers to live as successfully as possible within the community. MH/SA Care Coordination is extending their ability to better address the needs of individuals with serious and persistent mental illness with co-occurring physical health conditions
Accomplishments for FY17
Clinical Operations met all waiver performance standards for the year. Successful implementation of the new Innovations waiver with individual budgeting. Innovations spending was within budget targets. There has been a continued downward trend in Intensive In-Home utilization; met target
utilization goal for the end of the year and continues to trend downward, keeping individuals in less restrictive, more successful levels of treatment.
Improved care coordination functions that are managed within the Access Center primarily around assisting families waiting for C Waiver slots and needing Medicaid covered behavioral health services. Average days between a call to Access and an appointment was 4 days.
Maintained low Psychiatric Residential Treatment Facility (PRTF) utilization. No children in true out of state facilities.
ED liaisons had a reported significant impact on both reducing consumer time in the ED and deferring consumers from inpatient care, with inpatient readmission rates remaining low throughout the year.
Successfully implemented best practice integrated care models in all Alliance counties. Successfully filled all available Innovations slots, moved from ICFs to the community
using Money Follows the Person Funding and B3 services

9 | F Y 1 8 R e c o m m e n d e d B u d g e t
Added IDD/MHSA care coordinator to Wake CC Team, reduction in IDD wait times in EDs already occurring
Implemented NC START program for children, available to all Alliance counties Implemented a population health analytics tool
Summary of Goals and Objectives for FY18
Continue to meet and exceed all waiver contract requirements. Develop and implement innovative population health transformations in order to improve
overall healthcare for consumers, including enhanced long-term management of chronic conditions to maintain meaningful life in the community.
Improve the clinical quality of care coordination, resulting in longer community tenure/less need for crisis services
Improve consumer adherence with antipsychotic medications Decrease services that require prior authorization and manage based on data review,
including outcome measures. Decrease number of consumers with stays beyond expected ranges for highly utilized
services Develop and pilot an IDD Patient Centered Behavioral Health Home that is responsible for
managing total health of patient population. Maintain low consumer appeals rate. Increase number of consumers served through integrated healthcare teams. Increase intensive in-home and residential services alternatives. Expand use of general outpatient services. Increase use of Medication Assisted Treatment for individuals with substance use disorders. Decrease average length of stay (ALOS) of children in Therapeutic Foster Care. Implement law enforcement division program in Cumberland for individuals arrested for
low level drug offenses. Decrease inappropriate Opiate and Benzodiazepine prescribing practices of both in-network
and primary care prescribers. Improve options and use of community based treatment for youth with problematic sexual
behavior. Implement Resource Allocation Model under the Medicaid C Waiver.
Provider Network and Evaluation
Brief Description of Department and Units The Provider Network and Evaluation Department is responsible for the continuous review and evaluation of the provider network for quality of services, adherence to contract requirements, standards of care and performance, while ensuring a full array of providers is available to meet the needs of our service recipients. It also is responsible to ensure the quality of all Alliance services and processes through quality management activities and evaluating the quality of services provided by Alliance.

10 | F Y 1 8 R e c o m m e n d e d B u d g e t
The Department is comprised of two sections: Provider Network Operations has three components:
o Networks is responsible for managing the communication and dissemination of information to the community of providers, identifying and recruiting new providers, and for providing or arranging for technical assistance for currently enrolled providers.
o Credentialing assures that all providers in the Alliance network meet agency, State, Federal and accreditation requirements and that credentialing information is reviewed and tracked for continuous and timely review.
o Contracts is responsible for the timely development and distribution of all contracts, amendments, and extensions and ensures coordination of administrative activities including official correspondence with providers, provider education and liaison, and administration of provider contracts.
Strategic Initiatives and Special Projects manages the following functions and initiatives: o Community Needs Assessment o Network Development Plan o Special Provider Initiatives o Provider Collaboratives o Requests for Proposals o Hospital Relations
Provider Evaluation o Network Evaluation is responsible for monitoring and evaluating Alliance providers,
programs and services. Evaluation ensures: the use of data as the basis for making decisions, providers and programs are performing effectively, services are outcome-oriented, and Alliance and providers are accountable for the services consumers receive.
Accomplishments for FY17
Expansion of provider collaboratives to provide technical assistance and improve quality. Implementation of multiple evidence based practice service models. Development of multiple new evidence based service definitions to fill service gaps. Improved processes and relationships with our hospital partners. Implementation of contract tracking software to improve accuracy and efficiency. Creation of Provider Evaluation team Implement credentialing software Streamline process for new service development
Summary of Goals and Objectives for FY18
Improve relationships with and contract management of hospitals/health systems. Improve capacity for risk and trends analysis. Address provider network needs and gaps as specified in network development plan. Focus provider collaborative efforts on implementation of evidence based practices. Enhance provider performance and outcome measure reporting. Streamline reports generation. Increase number of provider contracts for evidence based practices.

11 | F Y 1 8 R e c o m m e n d e d B u d g e t
Identify and implement a process for monitoring evidence based practices. Improve communication processes with Providers.
Community Relations
Brief Description of Department and Units Community Relations is one of the most varied and diverse departments within Alliance. Recognizing that a local and visible presence is essential to building and sustaining partnerships critical to meeting organizational outcomes, the Community Relations teams take an innovative approach to improving the systems that support the effectiveness of services. Teams are continually assessing system and service gaps from multiple vantage points including co-location within other systems, outreach activities to stakeholders and advocates, and hosting community collaborative and workgroups. Utilizing a System of Care (SOC) framework, Community Relations focuses on the strengths and vulnerabilities of complex public systems, treatment of the “whole person,” and system transformation to improve policy, shared funding, collaboration and best practices. Recognizing that social determinants of health (i.e. homelessness, poverty/inequality and lack of education/employment) are key drivers of health care costs, Community Relations often plays a tangential role to the MCO functions - improving the environments in which people live increases engagement and retention in services, overall health and wellness, and more meaningful and productive lives that promote recovery. Accomplishments for FY17
Reorganized the Department to better align and support Alliance strategic and clinical goals Implemented short-term rental assistance program (ILI) in each community. Also created a
longer term rental assistance program for a higher risk population Completed a regional Housing Plan Developed a standardized Alliance overview presentation training to over 500 community
partners and stakeholders. Durham, Johnston and Wake have highly successful Crisis Intervention Training (CIT)
training programs with designated CIT Coordinators. A CIT Veterans training was developed in Wake County which has received national attention
Expanded MHFA trainers and now have a CR staff trained on almost every module Implemented Wake Network of Care (NOC) and completed significant enhancements to
Durham NOC Implemented Care Review in each community Successfully completed BECOMING, the 6 year SAMHSA funded grant focusing on
transitional age youth Funding renewed for two HUD-funded supportive housing programs in Durham. All Community Collaborative completed strategic plans outlining SOC priorities. Hired a Director of Housing and a Director of System Engagement

12 | F Y 1 8 R e c o m m e n d e d B u d g e t
Summary of Goals and Objectives for FY18
Study the need for additional personnel to target key areas across the 4 counties (i.e. System of Care Manager).
Promote cross-departmental collaboration to improve person and service outcomes. Assist in the development of models of care for special and high-risk populations. Assist in the development of comprehensive community supports to increase community
tenure and quality of life for high-risk adolescents and adults. Identify activities of Community Relations (i.e. housing, Care Review) and develop key
performance indicators to show the impact and return on investment. Develop pilot programs in partnership with other internal departments to study the quality
and effectiveness of programs targeting high risk populations (i.e. IIH, ED diversion, etc.).
Business Operations Division The Business Operations Division is responsible for the oversight and management of Alliance’s financial accountability relating to budgeting, claims, auditing and financial analysis.
Claims Processing
Brief Description of Department and Units Claims Processing is responsible for the monitoring and review of all claims processing for all funding sources, analysis of paid and denied claims, special ED claim review, etc. The team consists of Specialists, that assist providers daily on basic billing, and Claims Analysts that work on denials and analysis, encounter claim submission, and large projects. In addition, we have an EDI Specialist who specifically is focused on provider EDI files and EDI files that we send to the State. Accomplishments for FY17
Alliance claims staff continues to provide weekly claims training for providers to ensure updated knowledge of systems and claim information is shared will all providers.
Implemented a new Accounts Receivable (AR) system to allow for denials to be worked more efficiently. The system allows staff to research, identify claims to rebill and claims to write off.
Increased encounter approved claims from 15% approved in May 2015 to 95% approved in December 2016. Alliance is expected to maintain an average 95% approval rate as of July 1, 2017.
Claims Staff collaborated with IT/Report Development to create reports that provide analysts with paid claims in different categories. Some of the reports include: retro authorizations for claims, Out of Network provider claims, claims outside of our covered age range, claims where Medicaid has changed, and invalid living arrangements.
The HMS audit for March 2016 through August 2016 resulted in high scores of 100% in timeliness of provider payment, 99.38% in claims processing accuracy, and 99.16% in financial accuracy.

13 | F Y 1 8 R e c o m m e n d e d B u d g e t
Summary of Goals and Objectives for FY18
Maintain focus on meeting the encounter requirement to have 95% approved claims. Develop new reports to analyze paid and denied claims to ensure we are maximizing our
payments to providers Work with IT to continue to make improvements in the AR system so that we can maintain
accurate accounting of all outstanding NC TRACKs submitted claims Continue to enhance training and development so that staff are fully trained and have the
tools they need to do their job. We will focus on building a unified team with the help of updated procedures and process flows, mutual understanding of work, cross departmental training and most importantly adhering to our mission and values.
Finance and Accounting
Brief Description of Department and Units
Finance and Accounting - responsible for the agency's financial transactions, financial reporting, adherence to Generally Accepted Accounting Principles (GAAP), ensuring adequate and effective internal controls, etc.
Budget and Financial Analysis - responsible for the development and monitoring of the Alliance budget and analyzing budget to actual at both the administrative and service level. The staff in this unit are also responsible for the review and analysis of Medicaid dollars to include Per Member Per Month (PMPM) spending by category of service and aid, budget vs. actual, individual provider or service trends, etc. Responsibility also includes rate setting for programs, services, and providers.
Accomplishments for FY17
Hired a Grant Accountant to explicitly focus on federal funding requirements. This has been especially critical with the growing complexity and requirements of our federal dollars.
Upgraded our accounting software to a newer version which provided team members access to more efficient software.
Revised our Vendor Maintenance procedure and incorporated an IRS Tax Identification Number Verification program to improve accuracy of vendor information.
Continued the Medicaid Services Committee specifically designed to review our PMPM by
category of service on a monthly basis. Through this Committee, we have been able to dive into service detail, compare financial perspective with the clinical team, and discuss initiatives in cases of over or under spending.
Collaborated with the claims and IT teams to improve reporting to providers to enhance their internal reconciliations related to Alliance payments.
Finalized the Medical Loss Ratio (MLR) project to include all allowable expenses in the ratio and to ensure the MLR performance is monitored regularly.
Created Frequently Asked Questions for payroll and accounts payable to provide employees with additional help and quicker answers to their questions.
Completed another successful independent financial statement audit and compliance audit receiving no material weaknesses, significant deficiencies and no required adjustments.

14 | F Y 1 8 R e c o m m e n d e d B u d g e t
Implemented a chart of accounts conversion to incorporate the Organization’s recent reorganization into our reporting and budgeting.
Continued the departmental focused administrative budgets, as well as budget to actual reports, to allow for budget ownership and flexibility of spending.
Summary of Goals and Objectives for FY18
Implement a new process for tracking programs/services by provider and by funding source. Implement changes to our billing software which will improve the interface between the
billing software and accounting software. Implement identified budget software that works in conjunction with the accounting
software which will streamline budgeting efforts and assist with reporting. Continue to enhance our reporting and analysis of our services especially in the area of
Medicaid drilling down to the population level, Medicaid eligible lives, and category of service.
Continue engagement with consultants to assist with higher level reporting and forecasting Continue to enhance training and development so that staff are fully trained and have the
tools they need to do their job. We will focus on building a unified team with the help of updated procedures and process flows, mutual understanding of work, cross departmental training and most importantly adhering to our mission and values.
Organizational Performance Division The Organizational Performance division’s primary focus is on driving and supporting Alliance’s ability to meet its strategic planning goals, in particular, the Performance Strategic Goal of “optimizing our business performance to meet today’s needs and prepare for the future”. This is accomplished through the alignment of divisional departments including Organizational Effectiveness, Strategic Analytics, Human Resources, Quality Management, Information Technology and Customer Service/Access Center.
Organizational Effectiveness Department
Brief Description of Department and Units Organizational Effectiveness (OE) is at the highest level achieved by integrating our organization’s work processes, our people, our systems, and our leadership and aligning all of that with our organizational strategy. The OE Department is new, and was formed as a result of the July 2017 reorganization, building on the strengths of some existing units, such as Strategic Project Management (SPMO), Communications and Facilities, and consolidating and expanding some other units, such as Training and Organizational Development, all to meet our primary purposes: 1) facilitate positive change within the organization that is in alignment with our strategic plan; and 2) enhance and support a healthy organizational culture that is in alignment with our values
The Strategic Project Management team (SPMO) has matured into an internal consulting group while still managing the enterprise wide projects. They have engaged in a number of high priority projects supporting Alliance’s reorganization, department process improvements, and helping to develop the new clinical vision and strategic consultant work to better position Alliance for the future while strengthening the organization.

15 | F Y 1 8 R e c o m m e n d e d B u d g e t
All of the projects have centered on the enterprise vision and increasing efficient use of resources while meeting legal and contractual requirements.
The Alliance Communications Unit has oversight of all internal and external organizational communications to multiple stakeholders within our catchment area. This broad scope of work includes all organizational marketing development and production, organizational branding efforts, content maintenance of a complex website and highly regarded social media program.
Organizational Development (OD) and Learning is the newest team for the OED and brings our training program together with an expansion of the OD program to focus on staff and leadership development and organizational culture and growth, while at the same time, overseeing all training provided to staff, community members, and providers.
Facilities is currently a one-person unit responsible for the management of construction projects, renovations, and day to day operations of the Alliance sites. Health and Safety also falls within this unit, as do revisions to the Business Continuity Plan (BCP). The SVP is responsible for the BCP.
Accomplishments for FY17
Created the new department aligning the work and goals of four separate units under one mission and vision
Created and hired a Director of Organizational Development and Learning and redesigned staffing, created tracking mechanisms, and initial work on comprehensive ODL Plan to be launched July 2017
Provided training for 9,000 staff, providers and community members 380 individuals trained in Mental Health First Aid Facilitated and managed implementation of major revision of organizational Strategic
Plan with four new goals, and multiple new objectives and initiatives, to accelerate Alliance into the future
Provided portfolio tracking and analysis using Tableau and SharePoint to support executive decisions on project priorities
Managed 32 Enterprise Projects which includes both consulting and enterprise project management engagements, for example the Jennings Community Assessment, the Data Analytics launch and the DOJ/TCLI Supported Employment process improvement
Developed 6-month Process Improvement Training class on-line to engage staff at all sites and further develop culture of quality improvement and project management across the company
Initiated an Evolutionary Site Redesign of the Alliance website, employing surveys and user testing of key audience segments to create a more satisfying and productive user experience as well as an enhanced graphic layout.
Developed the Communication Connectors Initiative engaging designated staff from all divisions and company offices – with support from the Communications Unit – with ensuring regular flow of organizational information for dissemination, i.e. “telling our Alliance stories.”
Added a second Communications and Marketing Specialist to team, focusing on support of the Community Relations Department, and on the enhancement of internal video production capacity and the company social media program.
16 | F Y 1 8 R e c o m m e n d e d B u d g e t
Completed renovation of Cumberland site office at 711 Executive Place to mirror layout and open design consistent with other Alliance offices
Purchase of Wake Crisis Building at 3309 Durham Drive, in Raleigh, and moving forward with design
Continuation of design phase of renovation of Recovery Response Center (formerly DCA) in Durham
Completion of Strategic Facilities Plan to begin process of preparing options for future growth and potential new office locations to handle growth. Current leases expire December 31, 2018.
Summary of Goals and Objectives for FY18
Launch Enterprise level Project Portfolio System to allow executives to budget, approve and prioritize all major projects or initiatives, and provide training for Alliance Staff which will be needed to support new system
Launch comprehensive Organizational Development and Learning plan to include the following programs/curricula: Leadership Development Academy (4 Programs: Aspiring Leaders, Emerging Leaders, Strategic Leaders, Leader to Leader); Mentoring Programs (Peer & Executive/Senior Leader); Onboarding/Off boarding Program (in tandem with HR); Peer Coaching Program
Provide leadership and project management of major organizational initiatives, including Complete Care, Care Management System, TBI Waiver, and OE Organization Transformation projects (recommendations from the Jennings Community Assessment)
Complete a comprehensive Internal Communications Plan and support organizational efforts to increase employee engagement through improved internal communication.
Work with Jennings Communications to implement recommendations from Community Assessment, related to development of new brand messaging, and an external marketing plan
Continue to implement components of Evolutionary Site Redesign findings to further enhance website value to our users, including increased capacity to assist with consumer self-management of health.
Enhance existing social media program, expanding the positioning of Alliance leadership as “subject matter experts” and investigating the addition of other platforms and increased use of video for communicating messaging
Evaluate current function of SPMO and consider restructuring to Portfolio Management Office to better meet needs of Alliance’s future
Implement Strategic Facilities Plan for office space to accommodate growth and possible consolidation of existing offices and/or merger
For employee safety and security, implement Everbridge - a secure, scalable and reliable critical communications platform that enables rapid delivery of critical communications with near real-time verification over numerous devices and contact paths.

17 | F Y 1 8 R e c o m m e n d e d B u d g e t
Information Technology
Brief Description of Department and Units The IT department is comprised of three distinct teams:
Application Development and Quality Engineering - Responsible for all internal application development and support, including SharePoint and the corporate Intranet. Manages all quality assurance and user acceptance testing and documentation to support corporate audits. Manage database security, file downloads, and IT Project management. Manage User Acceptance Testing (UAT) for all Alpha releases for the organization.
Data Analytics/Business Intelligence - Responsible for extracting, organizing, cataloging and defining all key data elements that support Alliance. This team is also responsible for report and dashboard development to support the advanced analytics and information needs of the company.
IT Infrastructure and Support - Installs and supports all business data and voice networks within the Alliance sites. They are responsible for maintaining network and data security, HIPAA compliancy, email security, network and server performance and administration.
Accomplishments for FY17
Added a Director of Strategic Data Analytics to the Alliance Team. Added other staff in other key Data Analytics roles – Director of Data Architecture,
Manager of Enterprise Reporting, Data Architect, ETL Developer and additional BI Report Development Staff.
Continued development of Alliance Enterprise Data Warehouse. Expanded reporting and dashboards using MicroStrategy Reporting Software. Deployed Teradata Aster Advanced Analytics Platform. Developed multiple use cases
and proof of concepts including support for Therapeutic Foster Care, Call Center use of Text Analytics and Compliance Provider/Claims review.
Developed a new IT Request Workflow application. This SharePoint application allows ABH staff to request IT services while providing continual feedback to the requestor and extensive monitoring of the project through the Software Development Life Cycle (SDLC).
Implemented the Finance Accounts Receivable (AR) application. This application is used by the claims department to track and manage all claims activity and to monitor claims that have been denied by NCTRACKS.
Developed a Provider Portal for DOJ-Supported Employment tracking and reporting. This application allows ABH to comply with the requirements of the DOJ Settlement. Providers enter checklists that meet all of the DOJ requirements. ABH staff then reviews the checklists for accuracy and completeness. This information is then submitted to DOJ to meet our contractual reporting requirements.
Developed the Independent Living Initiative (ILI) application. This application allows Providers and Care Coordinators to request housing services online. This application is used by Care Coordinators, Housing Department, Finance, and External Providers.
Relocated our Disaster Recovery site from our Cumberland Office to a Co-Location Facility in Greensboro, NC. In doing so, we implemented two-hour replication for

18 | F Y 1 8 R e c o m m e n d e d B u d g e t
Critical Servers from Peak10 to the new Co-location DR site in Greensboro, providing a higher level of redundancy.
Migrated from Exchange 2010 to Exchange 2016 and implemented a Database Availability Group (DAG) for additional redundancy for email operations.
Completed the Access Center phone system Resiliency Project that included adding 10 phone lines from secondary provider for failover.
Implemented Duo Security Two Factor Authentication for VPN and Server access to improve network access security.
Implemented monthly Qualys vulnerability scanning of our internal networks and public facing IP addresses.
Summary of Goals and Objectives for FY18
Redesign Provider Search database and website – this will be a major update to this application based on the evolving needs of the business
Develop EDI Processing Web Application – Allows processing of all EDI files within the Alliance Data Structure. This application will allow us to make the information received in our EDI files easily accessible and utilized by all internal applications.
Develop automated support for Application Development testing efforts by designing and implementing data-driven automated testing framework.
Continue enhancing Alliance’s Enterprise Data Warehouse by incorporating new data domains to support the data analytics needs of the organization.
Evolve Advance Analytics program by continuing to identify business use cases to improve the information capabilities throughout the organization.
Develop Governed Self-Service reporting environment for MicroStrategy to be used by the Alliance Power Users.
Implement an improved Care Management solution to include enhanced capabilities, communication and workflows.
Integrate Alliance applications with the NC Health Information Exchange. Integrate Admission-Discharge-Transfer data from the NC Hospital Association with
Alliance systems and analytics. Continue to enhance the Alliance Disaster Recovery (DR) systems and testing plans. Implement a log management system (SIEM) to capture and correlate logs from
communications hardware, server hardware and corporate laptops.
Access Center
Brief Description of Department and Units The Access and Information Center (the Alliance 24/7 call center) links consumers to a range of services in the community and ensures that callers in need of crisis services are provided with timely access and follow-up. In addition to screening and referral activities, the call center provides information to general healthcare providers, CCNCs and to crisis providers to help coordinate the care of consumers needing routine services or during an after-hours crisis. It handles general information requests for Alliance as well.

19 | F Y 1 8 R e c o m m e n d e d B u d g e t
Accomplishments for FY17
Achieved URAC Health Call Center accreditation for a new site. Score 100% Met State contractual requirements for time of answer and abandonment rate Filled all the IDD Innovations slots. Improved coordination of care with NC Start for children. Held a successful Resource Fair for stakeholders, members and families seeking services
for IDD. Promoted Open Access model of care to decrease the time between appointments to 4
days. Collaborated with multiple providers on increasing choice for members. Integrated SharePoint into our daily work to increase staff’s access to information for
callers. Implemented the use of MicroStrategy to predict staffing coverage and training needs. Collaborated with Clinical Operations on “whole person care”. Provided customer service training for other departments. Worked to accomplish Alliance Strategic Goals by participating on the following
committees: Rewards and Recognition, Alliance Connectors, and various IT transition teams for the implementation of MicroStrategy and other software.
Worked collaboratively with Network development on rolling out new service definitions, and assessing the needs and gaps in our service continuum.
Part of a larger team of clinical staff who participate on the Provider Reconsideration Committee. Compliance Committee, UM Committee and various subcommittees.
IDD Access team increased staff’s knowledge of available dual diagnosis providers, and community resources which is utilized across the agency.
Continued to support families with limited state resources and few providers accepting referrals—requiring creative resource development.
Maintained detailed waitlists and submitted timely monthly reports. Revised IDD eligibility and slot management procedures to improve consistency across
departments. Summary of Goals and Objectives for FY18
Maintain URAC accreditation. Increase our knowledge of Population Health Management and explore ways to serve the
“whole person” in the Access and Information Center. Improve access to care for routine and urgent appointments. Work collaboratively with other departments to increase provider choice for Non-English
speaking Medicaid Members. Work collaboratively to implement TBI waiver. Work with NC START to serve our most disabled children. Continue to meet our call center contractual requirements Ensure we can provide a 24 hour Behavioral Health Call Center for our catchment area. Decrease turnover rate in our afterhours shifts. Increase the number of calls monitored with innovative technologies.
20 | F Y 1 8 R e c o m m e n d e d B u d g e t
Challenge the way in which we have approached member’s access to care. Use creative ways to increase the number of members seeking services to obtain the services in a timely manner.
Continue to support the Consumer’s rights of choice, privacy and dignity. Continue to offer Customer Service training to other departments. Fill all the Innovations slots for the year. Continue to find new and innovative ways to serve more individuals within our budgetary
constraints. Ensure that the experience of our callers is responsive, respectful, useful and pleasant. Establish Call Center protocols that ensure the safety of callers, members, stakeholders
and the community at large during a behavioral health crisis and/or a natural disaster. Continue to merge supports across diagnoses/funding silos (MH/SA/IDD) and
collaborate across departments to better serve our members and families. Planning spring resource/training fair for IDD staff and community/families. Implement additional technology to introduce more of our Medicaid members to
Alliance, increase access to free screening tools, and ensure services are easily accessible through our toll free number.
Quality Management
Brief Description of Department and Units Quality Management is responsible for creating a culture of continuous quality improvement across Alliance and assuring quality within the agency. Quality Management has two components:
Quality Assurance develops reports for Alliance management, committees and the state; investigates and resolves incidents and complaints; and analyzes data from NC-TOPPS, IRIS and other sources.
Quality Review oversees our Quality Improvement Projects (QIPs); performs quality reviews to identify opportunities for improvement; and develops quality management standards and training.
Accomplishments for FY17
As part of the Alliance reorganization, refocused the Quality Management Department on measuring and improving internal Alliance processes;
Developed a model for assessing department performance metrics needs, evaluated four departments, and initiated the development of metrics reporting;
Supported the creation of a new Provider Evaluation Department in the Care Management Division responsible for quality improvement activities related to Alliance’s provider network;
Improved Alliance’s performance on key measurements including CDW submissions, NC-TOPPS and Innovations;
Developed a new clinical practice guidelines evaluation program and assessed provider compliance with two key Alliance-approved guidelines;
Increased QM Department staffing and skills include training in statistics and Six Sigma; Successfully completing three long-term Quality Improvement Programs (QIPs);

21 | F Y 1 8 R e c o m m e n d e d B u d g e t
Identified and launched a QIP related to the Transition to Community Living Initiative as required by the state;
Supported a successful URAC re-credentialing review that focused in large part on Alliance’s quality management program.
Summary of Goals and Objectives for FY18
Increase the focus on evaluating and recommending quality improvement projects related to internal business operations
Expand the new performance metrics program across additional Alliance departments; Expand the clinical practice guidelines evaluation program to other key guidelines
including the urgent issue of opioid use; Roll out the MicroStrategy reporting platform to QM staff; Implement new Integrated Care performance measures as designated by the state in its
FY 2018 contract; Participate in the state’s development of its Critical Performance Measures and assure the
validity the state’s reporting on Alliance’s performance. Human Resources
Brief Description of Department and Units The Human Resources Department serves as an essential function of the workforce, and as such, all HR responsibilities are employee-centered. The main areas include Benefits Administration, Employee Relations, Compensation and Classification, and Recruitment and Selection. In addition, HR maintain a lead role with the Wellness Committee and Rewards & Recognition Committee. Both of these initiatives were established by the Strategic Plan, and demonstrate Alliance’s commitment to and appreciation for its staff. Accomplishments for FY17
Posted 97 vacancies; Hired 55 candidates Created 35 new positions Played an instrumental part in the 2016 re-organization Conducted organizational Open Enrollment for benefits Work with external vendor to complete 2016-17 Performance Appraisal cycle Completed a comprehensive salary study for 75 positions, reviewed FLSA designation
for 15 positions, and conducted formal desk audits for 15 Administrative Assistant positions
Conducted preliminary research for a Human Capital Management (HCM) tool that will capture all HR processes from applicant tracking to off boarding employees
HR Consultants provided recommendations regarding best practices for an on boarding off boarding process. Recommendations are in the process of being implemented.
The Rewards and Recognition committee launched the Give-a-Wow platform for peer-to-peer recognition, and issued the Recognize Me! boxes to supervisors for staff recognition
New employees receive an Alliance t-shirt during the New Employee Orientation as a part of the ‘welcome kit’ sponsored by the Rewards and Recognition committee

22 | F Y 1 8 R e c o m m e n d e d B u d g e t
Implemented several Wellness initiatives in an effort to improve the whole body health of Alliance employees:
o Conducted monthly Lunch-n-Learn, Functional Desk Exercise, Financial Health, and Mindfulness sessions at all sites
o Sponsored blood drives at Home and Wake sites o Pedometers given to all staff at no cost o Launched walking challenge from Home site to Wilmington beach o Wellness Committee presented “Eight Dimensions of Wellness” in Care
Coordination meeting o Published Wellness Intranet as a source of information for all staff
HR initiated a business improvement process mapping for Finance and HR to identify opportunities for greater efficiency and productivity.
Summary of Goals and Objectives for FY18
Establish a calendar of wellness events and activities to increase employee participation across organization
Expand the Give-a-Wow platform to include Welcome Me! activities for newly hired employees, and establish a calendar of recognition events/activities
Design and implement Service Award program to recognize and celebrate employees’ years of service milestones
In continuation of the FY17 project, complete a comprehensive salary study for ALL positions and assess the respective impact of changes to the organizational compensation processes and classification structure
There are several objectives which strive to improve departmental and organizational efficiencies by maximizing technology:
o Launch online benefits enrollment o Outsource leave administration for FMLA and ADA usage o Select and outline FY19 implementation for HCM solution
There are several objectives which strive to improve employee satisfaction: o Explore career progression and laddering within classification structure o Research and implement flexible work options o Conduct an employee survey (Fall 2017)
Office of Compliance Brief Description of Department and Units The Alliance Office of Compliance focuses on the prevention, detection and correction of identified violations of federal and state laws and regulations, and fraud control and unethical conduct, and encourages an environment where employees can report compliance concerns without fear of retaliation. It includes fifteen employees divided up in a Program Integrity Department, which includes a Special Investigations Unit and Claims Audit Unit, and Corporate Compliance Department, which includes a HIPAA Compliance Unit and Corporate Compliance Unit. The Office of

23 | F Y 1 8 R e c o m m e n d e d B u d g e t
Compliance is responsible for internal and external compliance to include policies and procedures, accreditation compliance, compliance training, internal audits and monitoring, claims audits, hotline reporting, investigation and correction of non-compliance, remediation, HIPAA privacy and security, medical records, public records, Network fraud and abuse investigations, provider actions and sanctions, and provider dispute resolution. Accomplishments for FY17
Opened 59 fraud and abuse investigations in the first 6 months of FY17 and referred 7 full investigations to DMA Program Integrity for determination of credible allegation of fraud.
Developed additional and more efficient fraud detection reports. Conducted internal audits and monitoring activities. Coordinated the re-accreditation process and assisted the Organization in achieving full 3-
year URAC accreditation in Health Call Center, Health Utilization Management, and Health Network.
Monitored all sites for HIPAA Privacy compliance. Contracted with external vendor to conduct Security Risk Assessment and worked with IT and other departments to mitigate identified risk.
Issued and tracked 82 actions and sanctions to providers in response to Network compliance issues in the first 6 months of FY17.
Issued over $173,000 in overpayments through the Corporate Compliance Committee process in the first 6 months of FY17.
Managed 9 requests for reconsideration of actions against providers in the first 6 months of FY17.
Audited 3% of adjudicated claims weekly. Audited inpatient and ED claims weekly. Conducted internal investigations and developed remediation plans where applicable,
monitored corrective action plans to ensure successful implementation. Conducted new hire orientation ongoing, annual compliance and HIPAA training to all
employees and the Board of Directors, and published informational materials related to compliance, fraud and abuse to a variety of stakeholder groups.
Conducted Compliance and Program Integrity training to Network Providers. Coordinated activities to celebrate Corporate Compliance and Ethics Week organization-
wide at each site with the purpose to increase compliance awareness. Transitioned three employees to supervisor positions, hired a Medical Records Analyst, a
second Internal Auditor, and will be hiring a Policy Analyst and Compliance Officer. Summary of Goals and Objectives for FY18
Our goal is to embed compliance, fraud control, and business ethics into Alliance day-to-day business through the use of infrastructures and tools designed to help achieve compliance with Federal, State, and local laws and regulations, State contracts and accreditation standards. The infrastructure and tools of focus for FY18: o Finalize the implementation of C360 to increase efficiencies and better manage risk
related to third parties such as administrative contractors, vendors, consultants and Business Associates.

24 | F Y 1 8 R e c o m m e n d e d B u d g e t
o Improve process to assess the impact of regulatory changes on Alliance operations, including review and revision to policies and procedures, manuals and training to ensure compliance with applicable changes. Examples include changes as a result of the CMS Medicaid Managed Care Final Rule
o Contract with vendor for fraud detection purposes to enhance our current investigative techniques and increase effectiveness of fraud detection efforts.
o Provide specialized training to department staff to promote professional growth and to achieve and maintain nationally recognized certifications in the areas of fraud examination and internal audits.
An annual work plan developed as a result of an annual risk assessment drives all major compliance operations. Items selected for the work plan pose significant risk (legal, financial, reputation) to Alliance. The plan is finalized at the beginning of each fiscal year and has therefore not yet been developed for FY18. Below are a few anticipated areas of focus: o Increased staff training with focus on HIPAA, confidentiality, policies and procedures,
and regulatory and accreditation requirements. o Expand the internal audit plan and increase compliance monitoring with timely
resolution and implementation of risk mitigation plans. o Monitor implementation of identified strategies to correct HIPAA security deficiencies
and audit for compliance. o Provide compliance and program integrity training and resources to providers
regularly. o Expand focused and ad hoc claims audits to identify overpayments, underpayments
and other irregularities or compliance issues. o Conduct fraud and abuse investigations to detect and deter fraud and abuse in the
Alliance Network. Prioritize areas of highest risk. o Provide assistance, input and compliance oversight of Alliance pilots, strategic
initiatives, RFPs and other Alliance efforts.

25 | F Y 1 8 R e c o m m e n d e d B u d g e t
General Fund Revenues FY2017-2018 Recommended Budget
Total General Fund Revenues: $495,747,257
Administrative $ 51,433,417 Medicaid Services 359,425,264 Alliance
State 25,913,107 Federal 3,444,951
Cumberland State 2,960,883 Federal 521,495 County 4,752,000
Durham State 3,657,121 Federal 867,561 County 6,070,519
Johnston State 1,965,317 Federal 139,869
Wake State 6,695,743 Federal 1,615,139 County 26,034,871
Grants Miscellaneous 250,000 Total $ 495,747,257

26 | F Y 1 8 R e c o m m e n d e d B u d g e t
General Fund Revenues FY2017-2018 Recommended Budget
Total General Fund Revenues: $495,747,257
$51,683,417 10%
$ 359,425,264 73%
$ 47,781,186 10%
$ 36,857,390 7%
Administrative/Misc Medicaid State County
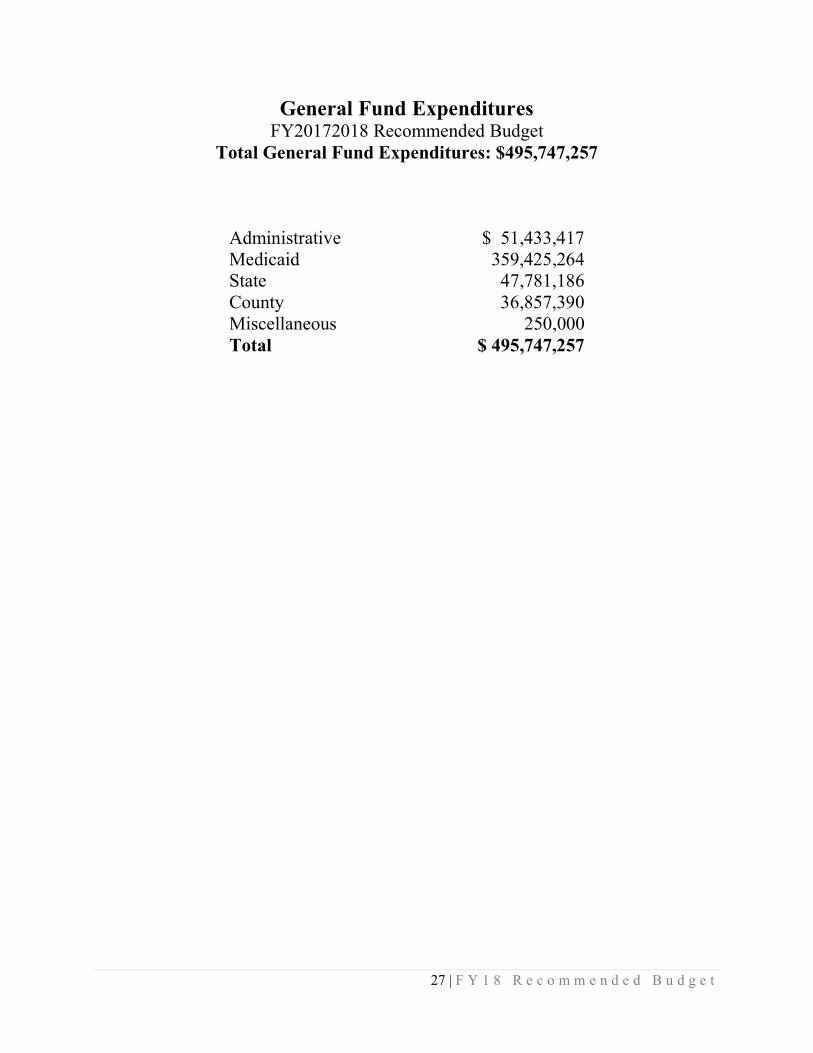
27 | F Y 1 8 R e c o m m e n d e d B u d g e t
General Fund Expenditures FY20172018 Recommended Budget
Total General Fund Expenditures: $495,747,257
Administrative $ 51,433,417 Medicaid 359,425,264 State 47,781,186 County 36,857,390 Miscellaneous 250,000 Total $ 495,747,257

28 | F Y 1 8 R e c o m m e n d e d B u d g e t
General Fund Expenditures FY2017-2018 Recommended Budget
Total General Fund Expenditures: $495,747,257
$51,683,417 10%
$444,063,840 90%
Administration Services

29 | F Y 1 8 R e c o m m e n d e d B u d g e t
Budget Comparison
Budgeted Revenue Budgeted Expenditures
FY17 Amended FY18
FY17
Amended FY18
Administrative $ 53,542,919 $ 51,433,417
Administrative $ 53,542,919 $ 51,433,417
Medicaid Services 375,648,164 359,425,264
Medicaid Services 375,648,164 359,425,264
Alliance
State & Federal Services
58,649,031 47,781,186
State 10,202,204 25,913,107
Federal 2,314,218 3,444,951
Local Services 37,717,388 36,857,390
Cumberland
Grants 403,224
State 3,636,905 2,960,883
Miscellaneous 325,000 250,000
Federal 1,250,272 521,495
County 2,537,000 4,752,000
Durham
State 7,288,954 3,657,121
Federal 1,116,380 867,561
County 6,155,207 6,070,519
Johnston
State 2,937,993 1,965,317
Federal 289,542 139,869
Wake
State 9,743,378 6,695,743
Federal 4,542,047 1,615,139
County 26,032,181 26,034,871
Grants 403,224
Miscellaneous 325,000 250,000
Fund Balance 18,320,138
TOTAL $ 526,285,726 $ 495,747,257
$ 526,285,726 $ 495,747,257
Administrative and Medicaid are lower than FY17 due to retroactive Medicaid received in FY17.
State dollars reflect a decrease due to one-time allocations received in the year. In addition, the FY17 Amended figures reflect the legislative reduction of $15M by each county.
Minimal changes in County dollars were to changes in programs or services.

30 | F Y 1 8 R e c o m m e n d e d B u d g e t
Functional Organization Chart
Area Board
1Chief Executive Officer
1
Office of Compliance
Business Operations
Care Management
1
Operational Performance
Medical Management
1
Office of Legal Affairs
Alliance Behavioral Healthcare
Accounting Financial
Management Budget &
Forecasting Claims
Processing
Medical Management
Peer Reviews Integrated
Healthcare
Clinical Mgmt. Medical Necessity Provider
Authorizations Care Coordination TCL Initiative Community
Relations Consumer Affairs Housing System
Engagement Network Devel. &
Eval. Credentialing Provider contracts
Human Resources Communications Org. Development Training Project
Management Facilities Mgmt. IT Consumer Access Quality
Management
Compliance HIPAA Privacy &
Security Program Integrity Internal Audits
Legal Affairs Governmental
Relations

31 | F Y 1 8 R e c o m m e n d e d B u d g e t
ANNUAL BUDGET ORDINANCE ALLIANCE BEHAVIORAL HEALTHCARE
FY 2017 - 2018
WHEREAS, the proposed budget and budget message for FY 2017 - 2018 was submitted to the Alliance Behavioral Healthcare Area Board on May 4, 2017 by the Budget Officer; was filed with the Executive Secretary to the Board;
WHERESAS, on June 1, 2017, the Alliance Behavioral Healthcare Area Board held a public hearing pursuant to NC G.S. 159-12 prior to adopting the proposed budget;
BE IT ORDAINED by the Alliance Behavioral Healthcare Area Board that for the purpose of financing the operations of Alliance Behavioral Healthcare, for the fiscal year beginning July 1, 2017 and ending June 30, 2018, there is hereby appropriated funds the following by function:
Section 1: General Fund Appropriations Administration $ 51,683,417 Medicaid Services $ 359,425,264 State Services $ 47,781,186 County Services $ 36,857,390 TOTAL $ 495,747,257
Section 2: General Fund Revenue
Administration $ 51,683,417 Medicaid Services $ 359,425,264 State Services $ 47,781,186 County Services $ 36,857,390 TOTAL $ 495,747,257 Section 3: Authorities A. The LME/MCO Board authorizes the Budget Officer to transfer up to $25,000 between appropriations without prior approval. B. The LME/MCO Board authorizes the Budget Officer, with written prior approval from the Chief Executive Officer, to transfer between appropriations of $25,001 - $100,000 per transaction if allowed by the funding source subject to a report to the Board Finance Committee at its next scheduled meeting. C. The LME/MCO Board authorizes the Budget Officer to transfer up to $100,000 cumulatively within an appropriation for the fiscal year subject to a year-end report to the Board Finance Committee. D. The CEO may enter into the following within budgeted funds:
1. Form and execute grant agreements within budgeted appropriations; 2. Execute leases for normal and routine business; 3. Enter into consultant, professional, maintenance, provider, or other service agreements; 4. Approve renewals for of contracts and leases; 5. Purchase of apparatus, supplies, materials or equipment and construction or repair work; 6. Reject any and all bids and re-advertise to receive bids.

32 | F Y 1 8 R e c o m m e n d e d B u d g e t
Budget and Amendment Process Overview The purpose of the budget and amendment process is to ensure that public dollars are spent in the manner as intended and in an effort to meet the needs of the citizens in relation to mental health, intellectual/developmental disabilities, and substance abuse needs. Through the budget, Alliance Behavioral Healthcare aims to fulfill its mission as granted by NC G.S. 122-C. Governing Statutes Alliance Behavioral Healthcare abides by the North Carolina Local Government Budget and Fiscal Control Act. It is the legal framework in which all government agencies must conduct their budgetary processes. NC G.S. 159 provides the legislation which includes several key dates such as:
159-10 - By April 30, Departments must submit requests to the Budget Officer 159-11(b) - By June 1, the Recommended Budget must be submitted the Board 159-12(b) - A public hearing must be held 159-13(a) - From 10 days after submitting to the Board, but by July 1, a balanced
budget must be adopted Budget Process FY 2017-2018 is the sixth recommended budget representing Alliance Behavioral Healthcare as a multi-county Area Authority. The budget represents services for Cumberland, Durham, Johnston and Wake counties. The administrative budget for this fiscal year was driven by our Per Member Per Month (PMPM) rate, FY18 projected costs, FTE positions, Department of Health and Human Services contract requirements, and costs related to the operating the Medicaid waiver. The Medicaid service budget was created based on historical experience and projections into the next fiscal year. Alliance will review the need for a budget amendment in the first quarter of FY18 if the projection of lives has changed based on payments received. The State and Local services budget was developed by gathering service information for each area based on the claims trends and information from staff. The FY18 allocations and benefit packages were reviewed and staff worked together to ensure all services were appropriately planned to be consistent with current services. Amendment Process The budget ordinance is approved at a function/appropriation level. The Budget Officer is authorized to transfer budget amounts within an appropriation up to $100,000 cumulatively without reporting to the Board. The Budget Officer is authorized to transfer budget amounts between functions up to $100,000 with an official report of such transfer being noted at the next regular Board meeting.

33 | F Y 1 8 R e c o m m e n d e d B u d g e t
Per G.S. 159-15, the governing board may amend the budget ordinance at any time after the ordinance's adoption in any manner, so long as the ordinance, as amended, continues to satisfy the requirements of G.S. 159-8 and 159-13. Budget Calendar Thursday, May 4, 2017 FY 2017-2018 recommended budget presented at LME/MCO Board
meeting
By Friday, May 12, 2017 Notice of June 1, 2017 Public Hearing published
Thursday, June 1, 2017 Public Hearing
By Friday, June 30, 2017 LME/MCO Board adoption of FY 2017-2018 Budget Ordinance
Monday, July 3, 2017 Budget is available in the General Ledger system
Glossary of Terms
LME
Per G.S. 122C-3(20b), Local Management Entity or LME means an area authority, county program, or consolidated human services agency. It is a collective term that refers to functional responsibilities rather than governance structure.
MCO
Managed Care Organization; LMEs that have adopted the financial risk and service review functions of the 1915(b) and 1915(c) waivers. LME-MCOs carry out the function of an LME and also act as health plans that provide health care in return for a predetermined monthly fee and coordinate care through a defined network of providers, physicians and hospitals.
Medicaid Waiver
States can submit applications to the federal Centers for Medicare and Medicaid Services, asking to be exempt from certain requirements. If granted a “1915(b)” waiver, a state can limit the number of providers allowed to serve consumers, easing the state’s administrative burden and saving money. If granted a “1915(c)” waiver, a state can offer more services focused on helping an intellectually or developmentally disabled consumer continue living in his or her home, rather than a group home.

FY18 Budget for ApprovalJune 1, 2017

• From Recommended to Approved:
• No change to Medicaid funding
• No change to State funding
• No change to County funding
• No change to total budget of $495,747,257
• Final Community Funds service listing
• FY18 reinvestment plan
Recommended vs. Approved

• Base Benefit Plan• Total $25,024,256• ACTT rate increase
State Funds
ACTT $ 2,546,258
Community Support Team $ 1,015,000
Developmental Therapy $ 1,075,000
Mobile Crisis $ 667,000
Outpatient/Physician Services $ 4,852,786
Personal Assistance $ 1,692,000
Residential Services $ 7,100,000
SAIOP $ 2,560,000
Supervised Living $ 2,400,000
DOJ/TCLI $ 1,116,212
Total $ 25,024,256

• Community Funds - Total $6,300,076• Changes in two services:
• Adult Day Vocational Program (-21%) • Intensive In Home Services (-45%)
• Recommendation based on spending in FY17
State Funds
Cumberland Durham Johnston Wake TotalHistorical Breakdown
Percentage breakdown 15.51% 29.80% 9.47% 45.21%Allocation of dollars $ 977,371 $ 1,877,689 $ 596,862 $ 2,848,154 $ 6,300,076
RecommendationPercentage breakdown 21.63% 28.78% 8.96% 40.63%
Dollars to allocate $ 1,362,968 $ 1,813,176 $ 564,370 $ 2,559,562 $ 6,300,076 Dollar change $ 385,597 $ (64,513) $ (32,492) $ (288,592)

• Services covered include:• Adult Day Vocational Program (ACVP)• Day Activity• Intensive In Home• Multi Systemic Therapy (MST)• Psychosocial Rehab (PSR)• Substance Abuse Comprehensive Outpatient Treatment
(SACOT)• Supported Employment• Other small community services
Community Funds Recommendation

State FundsTraditional New Model Services Expenses
Federal
Alliance $ 145,844 $ 3,444,951 $ 3,299,107 $ 145,844
Cumberland $ 864,164 $ 521,495 $ 179,689 $ 341,806
Durham $ 1,300,350 $ 867,561 $ 239,043 $ 628,518
Johnston $ 263,505 $ 139,869 $ 74,404 $ 65,465
Wake $ 4,015,152 $ 1,615,139 $ 337,443 $ 1,277,696
Total Federal $ 6,589,015 $ 6,589,015 $ 4,129,686 $ 2,459,329
State
Alliance $ 5,304,170 $ 25,913,107 $21,725,149 $ 4,187,958
Cumberland $ 6,510,340 $ 2,960,883 $ 2,950,883 $ 10,000
Durham $ 9,922,108 $ 3,657,121 $ 2,384,674 $ 1,272,447
Johnston $ 3,922,860 $ 1,965,317 $ 1,516,528 $ 448,789
Wake $15,532,693 $ 6,695,743 $ 3,907,352 $ 2,788,391
Total State $41,192,171 $ 41,192,171 $32,484,586 $ 8,707,585

FY18 Reinvestment Plan
Crisis Services
Behavioral Health Urgent Care 4,500,000 Child Facility Based Crisis 3,000,000 Durham Crisis Facility 1,000,000 Learning Enriched Autism Program (IDD facility) 300,000 Mobile Crisis 840,000 NC START 650,000 Paramedicine 250,000 Wake Crisis Facility 5,500,000 Subtotal $ 16,040,000
• Increased to include pilot programs• Categorized to tie directly to our population health
model
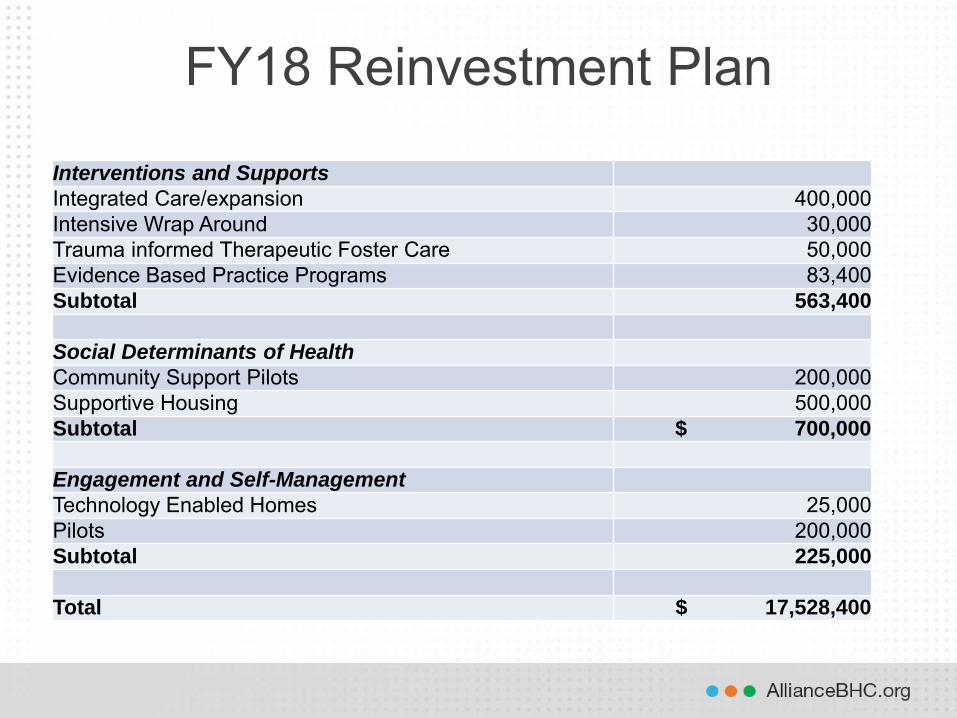
FY18 Reinvestment Plan
Interventions and Supports
Integrated Care/expansion 400,000 Intensive Wrap Around 30,000 Trauma informed Therapeutic Foster Care 50,000 Evidence Based Practice Programs 83,400 Subtotal 563,400
Social Determinants of Health
Community Support Pilots 200,000 Supportive Housing 500,000 Subtotal $ 700,000
Engagement and Self-Management
Technology Enabled Homes 25,000 Pilots 200,000 Subtotal 225,000
Total $ 17,528,400

(Back to agenda)
9
ITEM: Supportive Housing Proposal DATE OF BOARD MEETING: June 1, 2017 BACKGROUND: Alliance has been given the opportunity to partner with CASA, a local developer, and invest $250,000 in thirteen one-bedroom units within the Durham City limits. This investment will allow access to nearly 20% of the units exclusive for Alliance consumers in accordance with the Olmstead settlement. The investment will go towards rehab of the existing property. REQUEST FOR AREA BOARD ACTION: Approve the proposal. CEO RECOMMENDATION: Approve the proposal. RESOURCE PERSON(S): Ann Oshel, Sr VP Community Relations; Carol Hammett, General Counsel, Kelly Goodfellow, CFO
Alliance Behavioral Healthcare BOARD OF DIRECTORS
Agenda Action Form

(Back to agenda)
ITEM: Proposal to Cancel the July 6, 2017, Board Meeting DATE OF BOARD MEETING: June 1, 2017 BACKGROUND: As stated in Article III Sections A and D of the Board By-laws, regular meetings of the Area Board shall be held at least six times each year at a location and time designated by the Area Board. All meetings of the Area Board shall be conducted in accordance with provisions set forth in Open Meetings Law. The Board currently holds its regularly scheduled meetings on the first Thursday of each month. The matter is placed before the Board for a vote on whether the Board would like to cancel the July 6, 2017, regularly scheduled meeting. If canceled, the proper notice shall be published by the Executive Secretary of the Board. REQUEST FOR BOARD ACTION: Consider meeting schedule and determine if the Board will meet on July 6, 2017. CEO RECOMMENDATION: Consider meeting schedule and determine if the Board will meet on July 6, 2017. RESOURCE PERSON(S): Robert Robinson, CEO
Alliance Behavioral Healthcare BOARD OF DIRECTORS
Agenda Action Form
10

(Back to agenda)
ITEM: Election of FY18 Board Officers: Chairperson and Vice-Chairperson
DATE OF BOARD MEETING: June 1, 2017 BACKGROUND: As stated in Article II, Section D of the by-laws, officers of the Area Board shall be chosen for a one-year term at the final meeting of the fiscal year in which the Area Board is serving, and shall be as follows: Chairperson and Vice-Chairperson. With the exception of the Executive Secretary (which shall be filled by the CEO or the CEO’s designee), no officer shall serve in a particular office for more than two consecutive terms. Each Area Board member shall be eligible to serve as an officer. Duties of officers shall be as follows:
Chairperson – this officer shall preside at all meetings and generally perform the duties of a presiding officer. The Chairperson shall appoint all Area Board committees.
Vice Chairperson – this officer shall be familiar with the duties of the Chairperson and be prepared to serve or preside at any meeting on any occasion where the Chairperson is unable to perform his/her duties.
Nominations will be presented and Board members will elect officers at the June 1, 2017, Board meeting. REQUEST FOR AREA BOARD ACTION: Elect Chairperson and Vice-Chairperson. CEO RECOMMENDATION: Elect Chairperson and Vice-Chairperson. RESOURCE PERSON(S): Robert Robinson, CEO
Alliance Behavioral Healthcare BOARD OF DIRECTORS
Agenda Action Form
11

(Back to agenda)
12
ITEM: Training: Services for Individuals with Complex Needs DATE OF BOARD MEETING: June 1, 2017 BACKGROUND: The State has been working with Disability Rights of North Carolina for about two years to address unmet needs in children with both mental illness and developmental disabilities. Alliance has increased our focus on these particular children as well. There are numerous challenges involved in serving these children, including limited provider/community expertise, difficulty obtaining high quality comprehensive assessments, a lack of strong evidence for effective treatments for this population, separate DD and MH services that often don’t address or acknowledge comorbidity, and difficulty identifying the population. Alliance has developed a Crisis Response Team of care coordinators focused especially on helping children with complex needs and their families by coordinating their discharge from crisis facilities and by using data analytics to identify children with DD and MH issues who might be at risk of crisis. We are also working to use data analytics to further identify children who might have gaps in care related to their complex needs, identify a provider specializing in assessments for these individuals, and developing more resources in our provider network to support these children. REQUEST FOR AREA BOARD ACTION: Receive the training. CEO RECOMMENDATION: Receive the training. RESOURCE PERSON(S): Beth Melcher, Ph.D, Executive Vice-President of Care Management
Alliance Behavioral Healthcare BOARD OF DIRECTORS
Agenda Action Form
(Back to agenda)
13B
ITEM: FY18 Classification and Grade Plan DATE OF BOARD MEETING: June 1, 2017 BACKGROUND: Annually Alliance is required to report its classification and grade plan to the North Carolina Office of State Human Resources. This report requires that the Alliance Board review and approve this annual plan. Changes to the salary are highlighted on the attached document. Positions have been added or reclassified as a result of organizational needs. REQUEST FOR AREA BOARD ACTION: Approve the report. CEO RECOMMENDATION: Approve the report. RESOURCE PERSON(S): Cheala Garland-Downey, Director of Human Resources
Alliance Behavioral Healthcare BOARD OF DIRECTORS
Agenda Action Form

Rev Date: May 22, 2017 1 of 8
Working Title Classification Salary Grade Min Mid Max Accountant Accountant I 33 46,115$ 62,750$ 79,385$ Accounting Manager Accounting Manager 40 65,104$ 88,590$ 112,076$ Accountis Payable Manager Accounting Manager 40 65,104$ 88,590$ 112,076$ Finance Manager Accounting Manager 40 65,104$ 88,590$ 112,076$ Senior Accounts Payable Analyst Accounting Specialist II 33 46,115$ 62,750$ 79,385$ Accounts Payable Clerk Accounting Technician IV 24 $ 29,599 $ 40,276 $ 50,953 Administrative Assistant Administrative Assistant I 26 32,664$ 44,447$ 56,230$ Administrative Assistant II Administrative Assistant II 28 36,046$ 49,049$ 62,052$
Administrative Assistant III 30 39,779$ 54,128$ 68,478$ Appeals Coordinator Administrative Clinical Support Specialist I 26 32,664$ 44,447$ 56,230$ Provider Network Helpdesk Specialist Administrative Clinical Support Specialist I 26 32,664$ 44,447$ 56,230$ Contract Specialist Administrative Clinical Support Specialist II 27 34,313$ 46,691$ 59,069$ Credentialing Specialist Administrative Clinical Support Specialist II 27 34,313$ 46,691$ 59,069$ Provider Enrollment Specialist Administrative Clinical Support Specialist II 27 34,313$ 46,691$ 59,069$ Credentialing Specialist II Administrative Clinical Support Specialist III 29 37,866$ 51,526$ 65,186$ Credentialing Supervisor Administrative Officer I 32 43,898$ 59,733$ 75,569$ Credentialing Manager Administrative Officer II 35 50,890$ 69,248$ 87,605$ Healthcare Network Program Manager II Administrative Officer III 38 58,995$ 80,277$ 101,559$ Consumer Affairs Specialist Advocate 27 34,313$ 46,691$ 59,069$ Inreach Peer Support Specialist Advocate 27 $ 34,313 $ 46,691 $ 59,069 Assistant General Counsel Attorney I 42 71,846$ 97,763$ 123,681$ Deputy General Counsel Attorney II 45 83,290$ 113,335$ 143,381$ General Counsel Attorney III 48 96,556$ 131,387$ 166,218$ Budget Analyst Budget Analyst 35 50,890$ 69,248$ 87,605$ Power Analyst Business & Technology Analyst I 37 56,159$ 76,418$ 96,677$ EDI Specialist Business & Technology Analyst II 38 58,995$ 80,277$ 101,559$ Report Developer Business & Technology Analyst II 38 58,995$ 80,277$ 101,559$ ETL Developer Business & Technology Application Specialist I 40 65,104$ 88,590$ 112,076$ IT Quality Engineer Business & Technology Application Specialist I 40 65,104$ 88,590$ 112,076$ Sharepoint Developer Business & Technology Application Specialist I 40 65,104$ 88,590$ 112,076$ Application/Web Developer Business & Technology Application Specialist II 41 61,975$ 84,331$ 106,688$ Data Architect Business & Technology Application Specialist II 41 61,975$ 84,331$ 106,688$ Microstrategy Administrator Business & Technology Application Specialist II 41 68,392$ 93,064$ 117,735$ Senior Sharepoint Architect Business & Technology Application Specialist II 41 68,392$ 93,064$ 117,735$

Rev Date: May 22, 2017 2 of 8
Senior Database Administrator Business & Technology Application Specialist III 42 71,846$ 97,763$ 123,681$ Business & Technology Applications Technician 31 41,787$ 56,862$ 71,936$ Business Analyst 35 50,890$ 69,248$ 87,605$
Purchasing Manager Business Officer 38 58,995$ 80,277$ 101,559$ IT Quality Assurance Specialist Business Systems Analyst II 38 58,995$ 80,277$ 101,559$ IT Technical Trainer Business Systems Analyst II 38 58,995$ 80,277$ 101,559$ Area Director CEOExecutive Vice President-Care Management Chief Clinical Operations 53 123,526$ 168,087$ 212,647$ Executive Vice President-CFO Chief Financial Officer 53 123,526$ 168,087$ 212,647$ Executive Vice President-COO Chief Operations Officer 52 117,588$ 160,006$ 202,425$ Claims Analyst Claims Analyst 28 36,046$ 49,049$ 62,052$ Claims Auditor Claims Analyst 28 36,046$ 49,049$ 62,052$ Senior Claims Analyst Claims Analyst II 29 37,866$ 51,526$ 65,186$ Director of Claims Claims Director 40 65,104$ 88,590$ 112,076$ Claims Manager Claims Manager 35 50,890$ 69,248$ 87,605$ Claims Specialist Claims Specialist 24 $ 29,599 $ 40,276 $ 50,953 Claims Audit Supervisor Claims Supervisor 33 46,115$ 62,750$ 79,385$ Claims Supervisor Claims Supervisor 33 46,115$ 62,750$ 79,385$ Community Education Specialist Community Relations Specialist 30 39,779$ 54,128$ 68,478$ Community Liaison Community Relations Specialist 30 39,779$ 54,128$ 68,478$ Criminal Justice Specialist Community Relations Specialist 30 39,779$ 54,128$ 68,478$ Care Review Coordinator Community Services Consultant 28 36,046$ 49,049$ 62,052$ Cultural and Linguistic Competence Coord. Community Services Consultant 28 36,046$ 49,049$ 62,052$ Family Partner Coordinator Community Services Consultant 28 36,046$ 49,049$ 62,052$ Transition Coordinator Community Services Consultant 28 36,046$ 49,049$ 62,052$ Youth Coordinator Community Services Consultant 28 36,046$ 49,049$ 62,052$ Chief Compliance Officer Compliance Program Administrator 47 91,914$ 125,071$ 158,228$ Contract Administrator Contract Administrator 34 48,443$ 65,919$ 83,394$
Controller 45 83,290$ 113,335$ 143,381$ Data Consultant Data Analyst (Non-IT) 35 50,890$ 69,248$ 87,605$
Data Specialist 29 37,866$ 51,526$ 65,186$ Executive Assistant Executive Assistant 31 41,787$ 56,862$ 71,936$ Facilities Manager Facilities Manager 34 48,443$ 65,919$ 83,394$
Finance Director 45 83,290$ 113,335$ 143,381$ Financial Analyst Financial Analyst 34 48,443$ 65,919$ 83,394$

Rev Date: May 22, 2017 3 of 8
Health Information Data Manager 32 43,898$ 59,733$ 75,569$ HIPAA Privacy and Security Officer HIPAA Privacy and Security Officer 36 53,460$ 72,745$ 92,029$ Human Resources Business Partner HR Analyst 32 43,898$ 59,733$ 75,569$ Director of Human Resources HR Director 41 68,392$ 93,064$ 117,735$ Director of Organizational Development & Learning HR Director 41 68,392$ 93,064$ 117,735$ Senior Vice President-HR HR Executive 45 83,290$ 113,335$ 143,381$ Human Resources Specialist HR Specialist 29 37,866$ 51,526$ 65,186$ Housing Specialist Human Services Coordinator II 30 39,779$ 54,128$ 68,478$ ILI Coordinator Human Services Coordinator II 30 39,779$ 54,128$ 68,478$ System of Care Coordinator Human Services Coordinator II 30 39,779$ 54,128$ 68,478$ Tenancy Support Coordinator Human Services Coordinator II 30 39,779$ 54,128$ 68,478$ Youth Opportunity Coordinator Human Services Coordinator II 30 39,779$ 54,128$ 68,478$ UM I/DD Supervisor Human Services Coordinator III 36 53,460$ 72,745$ 92,029$ Access Coordinator Human Services Counselor I 29 37,866$ 51,526$ 65,186$ Administrative Care Coordinator Human Services Counselor I 29 37,866$ 51,526$ 65,186$ School Based Diversion Coordinator Human Services Counselor I 29 37,866$ 51,526$ 65,186$ Youth Resource Specialist Human Services Counselor I 29 37,866$ 51,526$ 65,186$ I/DD Care Coordinator I/DD Care Coordinator 31 41,787$ 56,862$ 71,936$ I/DD Olmstead Liaison I/DD Care Coordinator 31 41,787$ 56,862$ 71,936$ I/DD Clinical Director I/DD Clinical Director 40 65,104$ 88,590$ 112,076$ Director of I/DD Care Coordination I/DD Program Manager 38 58,995$ 80,277$ 101,559$ I/DD Care Coordination Supervisor I/DD Program Supervisor 36 53,460$ 72,745$ 92,029$ SIS Evaluation Team Lead I/DD Program Supervisor 36 53,460$ 72,745$ 92,029$ I/DD Access Coordinator I/DD Specialist 27 34,313$ 46,691$ 59,069$ SIS Evaluator I/DD Specialist II 30 39,779$ 54,128$ 68,478$ UM Care Manager-I/DD I/DD Specialist II 30 39,779$ 54,128$ 68,478$
Information and Communication Specialist I 26 32,664$ 44,447$ 56,230$ Communications & Marketing Specialist Information and Communication Specialist II 31 41,787$ 56,862$ 71,936$ Director of Communications Information and Communication Specialist III 41 68,392$ 93,064$ 117,735$ Director of Infrastructure and Security Information Technology Director 47 91,914$ 125,071$ 158,228$ Director of IT Applications Development Information Technology Director 47 91,914$ 125,071$ 158,228$ Director of IT Data Architecture Information Technology Director 47 91,914$ 125,071$ 158,228$ Director of Strategic Analytics Information Technology Director 47 91,914$ 125,071$ 158,228$ Senior Vice President-CIO Information Technology Executive 53 123,526$ 168,087$ 212,647$ IT Quality Engineering Manager Information Technology Manager 43 75,474$ 102,701$ 129,927$

Rev Date: May 22, 2017 4 of 8
Manager of Enterprise Reporting Information Technology Manager 43 75,474$ 102,701$ 129,927$ Internal Auditor 28 36,046$ 49,049$ 62,052$
Investigator I Investigator I 29 37,866$ 51,526$ 65,186$ Physician Peer Reviewer Medical Director I 55 136,317$ 185,492$ 234,667$ Associate Medical Director Medical Director II 57 150,433$ 204,700$ 258,967$ Chief Medical Officer Medical Director III 59 166,010$ 225,897$ 285,783$ ED Claims Reviewer Mental Health Nurse II 34 48,443$ 65,919$ 83,394$ Healthcare Integration Nurse Mental Health Nurse II 34 48,443$ 65,919$ 83,394$ UM Care Manager-MH/SA RN Mental Health Nurse II 34 48,443$ 65,919$ 83,394$ Government Relations Director MH Program Administrator I 43 75,474$ 102,701$ 129,927$ Healthcare Integration Director MH Program Administrator I 43 75,474$ 102,701$ 129,927$ Hospital Relations Director MH Program Administrator I 43 75,474$ 102,701$ 129,927$ Senior Vice President-Clinical Operations MH Program Administrator II 46 87,496$ 119,059$ 150,622$ Senior Vice President-Community Relations MH Program Administrator II 46 87,496$ 119,059$ 150,622$ Senior Vice President-Network Dev and Evaluation MH Program Administrator II 46 87,496$ 119,059$ 150,622$ Senior Vice President-Organizational Effectiveness MH Program Administrator II 46 87,496$ 119,059$ 150,622$ Senior Vice President-Strategy MH Program Administrator II 46 87,496$ 119,059$ 150,622$ Hospital Liaison MH/SA Clinician I 32 43,898$ 59,733$ 75,569$ I/DD Care Coordination Critical Response Clinician MH/SA Clinician I 32 43,898$ 59,733$ 75,569$ MH/SA Care Coordinator MH/SA Clinician I 32 43,898$ 59,733$ 75,569$ School Based Care Coordinator MH/SA Clinician I 32 43,898$ 59,733$ 75,569$ Access Clinician MH/SA Clinician II 33 46,115$ 62,750$ 79,385$ Investigator II MH/SA Clinician III 34 48,443$ 65,919$ 83,394$ UM Care Manager-MH/SA MH/SA Clinician III 34 48,443$ 65,919$ 83,394$ Senior UM Care Manager-MH/SA MH/SA Clinician IV 35 50,890$ 69,248$ 87,605$
MH/SA Unit Supervisor I 32 43,898$ 59,733$ 75,569$ Access Supervisor MH/SA Unit Supervisor II 37 56,159$ 76,418$ 96,677$ Director of Consumer Affairs MH/SA Unit Supervisor II 37 56,159$ 76,418$ 96,677$ MH/SA Care Coordination Supervisor MH/SA Unit Supervisor II 37 56,159$ 76,418$ 96,677$ MH/SA Crisis Services Supervisor MH/SA Unit Supervisor II 37 56,159$ 76,418$ 96,677$ Provider Network Development Supervisor MH/SA Unit Supervisor II 37 56,159$ 76,418$ 96,677$ Provider Network Evaluation Supervisor MH/SA Unit Supervisor II 37 56,159$ 76,418$ 96,677$ Transitions to Community Living Supervisor MH/SA Unit Supervisor II 37 56,159$ 76,418$ 96,677$ Utilization Review Manager MH/SA Unit Supervisor II 37 56,159$ 76,418$ 96,677$ Community Relations Manager MH/SA Unit/Program Director I 37 56,159$ 76,418$ 96,677$

Rev Date: May 22, 2017 5 of 8
Director of Community Education & Outreach MH/SA Unit/Program Director II 38 58,995$ 80,277$ 101,559$ UM MH/SA Supervisor MH/SA Unit/Program Director II 38 58,995$ 80,277$ 101,559$ Access Director MH/SA Unit/Program Director III 40 65,104$ 88,590$ 112,076$ Director of Housing MH/SA Unit/Program Director III 40 65,104$ 88,590$ 112,076$ Director of MH/SA Care Coordination MH/SA Unit/Program Director III 40 65,104$ 88,590$ 112,076$ Director of Network Evaluation MH/SA Unit/Program Director III 40 65,104$ 88,590$ 112,076$ Director of Program Integrity MH/SA Unit/Program Director III 40 65,104$ 88,590$ 112,076$ Director of Provider Network Operations MH/SA Unit/Program Director III 40 65,104$ 88,590$ 112,076$ Director of Provider Network Strategic Initiatives MH/SA Unit/Program Director III 40 65,104$ 88,590$ 112,076$ Director of System Engagement MH/SA Unit/Program Director III 40 65,104$ 88,590$ 112,076$ Director of UM MH/SA Unit/Program Director III 40 65,104$ 88,590$ 112,076$ Medicaid Program Director MH/SA Unit/Program Director III 40 65,104$ 88,590$ 112,076$ Desktop Infrastructure Supervisor Network Analyst (Senior) 38 58,995$ 80,277$ 101,559$
Network Analyst I 33 46,115$ 62,750$ 79,385$ Network Analyst II 34 48,443$ 65,919$ 83,394$
Senior Network Specialist Networking Specialist (Senior) 40 65,104$ 88,590$ 112,076$ Networking Specialist I 35 50,890$ 69,248$ 87,605$ Networking Specialist II 36 53,460$ 72,745$ 92,029$
Receptionist Office Assistant III 20 24,305$ 33,072$ 41,840$ Office Assistant Office Assistant IV 22 26,821$ 36,497$ 46,172$ Paralegal Paralegal 29 37,866$ 51,526$ 65,186$ Pharmacist Pharmacist 46 87,496$ 119,059$ 150,622$ Medical Records Specialist Processing Assistant V 23 28,176$ 38,340$ 48,504$ Eligibility & Enrollment Supervisor Processing Unit Supervisor 26 32,664$ 44,447$ 56,230$ Special Investigations Supervisor Program Integrity Unit Supervisor 36 53,460$ 72,745$ 92,029$ Provider Network Development Specialist I Program/Services Development Specialist I 32 43,898$ 59,733$ 75,569$ Provider Network Development Specialist II Program/Services Development Specialist II 34 48,443$ 65,919$ 83,394$ Healthcare Network Project Manager Project Manager 37 56,159$ 76,418$ 96,677$ Project Manager Project Manager 37 56,159$ 76,418$ 96,677$ Strategic Project Architect Project Manager 37 56,159$ 76,418$ 96,677$ Provider Network Evaluator I QA Specialist II 28 36,046$ 49,049$ 62,052$ Provider Network Evaluator II QA Specialist III 31 41,787$ 56,862$ 71,936$ Director of Quality Management Quality Management Director 39 61,975$ 84,331$ 106,688$ Quality Assurance Manager Quality Management Manager I 35 50,890$ 69,248$ 87,605$ Quality Review Manager Quality Management Manager I 35 50,890$ 69,248$ 87,605$
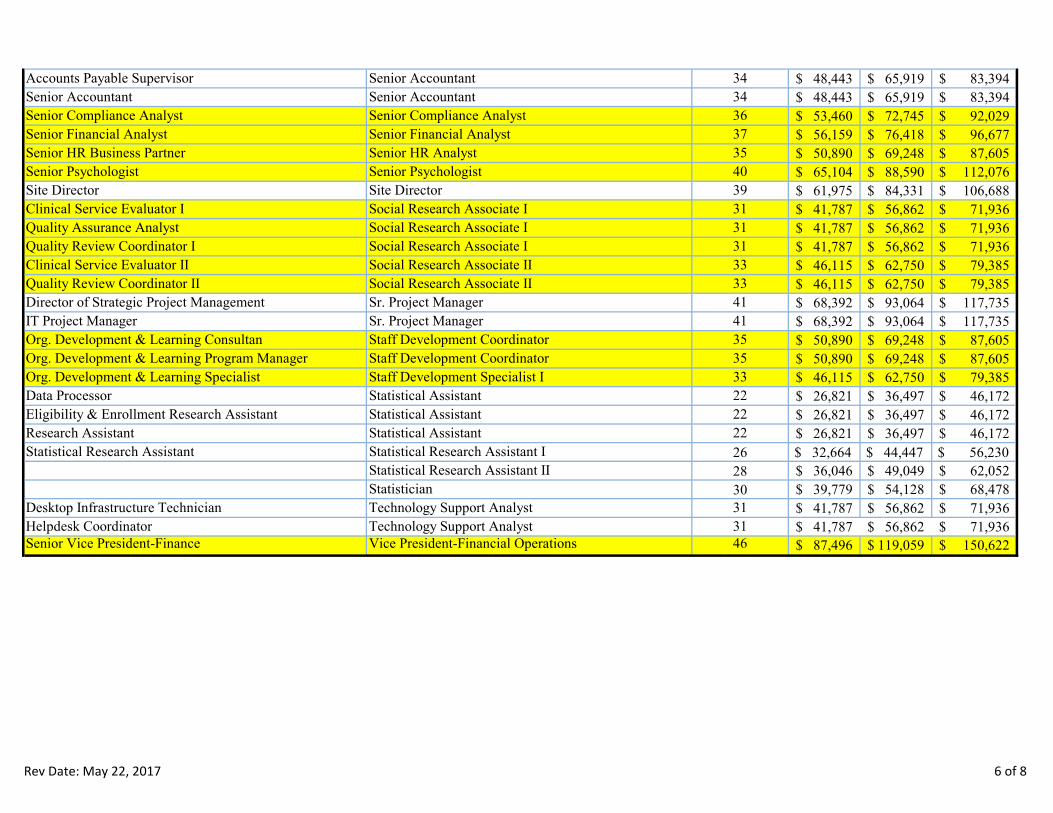
Rev Date: May 22, 2017 6 of 8
Accounts Payable Supervisor Senior Accountant 34 48,443$ 65,919$ 83,394$ Senior Accountant Senior Accountant 34 48,443$ 65,919$ 83,394$ Senior Compliance Analyst Senior Compliance Analyst 36 53,460$ 72,745$ 92,029$ Senior Financial Analyst Senior Financial Analyst 37 56,159$ 76,418$ 96,677$ Senior HR Business Partner Senior HR Analyst 35 50,890$ 69,248$ 87,605$ Senior Psychologist Senior Psychologist 40 65,104$ 88,590$ 112,076$ Site Director Site Director 39 61,975$ 84,331$ 106,688$ Clinical Service Evaluator I Social Research Associate I 31 41,787$ 56,862$ 71,936$ Quality Assurance Analyst Social Research Associate I 31 41,787$ 56,862$ 71,936$ Quality Review Coordinator I Social Research Associate I 31 41,787$ 56,862$ 71,936$ Clinical Service Evaluator II Social Research Associate II 33 46,115$ 62,750$ 79,385$ Quality Review Coordinator II Social Research Associate II 33 46,115$ 62,750$ 79,385$ Director of Strategic Project Management Sr. Project Manager 41 68,392$ 93,064$ 117,735$ IT Project Manager Sr. Project Manager 41 68,392$ 93,064$ 117,735$ Org. Development & Learning Consultan Staff Development Coordinator 35 50,890$ 69,248$ 87,605$ Org. Development & Learning Program Manager Staff Development Coordinator 35 50,890$ 69,248$ 87,605$ Org. Development & Learning Specialist Staff Development Specialist I 33 46,115$ 62,750$ 79,385$ Data Processor Statistical Assistant 22 26,821$ 36,497$ 46,172$ Eligibility & Enrollment Research Assistant Statistical Assistant 22 26,821$ 36,497$ 46,172$ Research Assistant Statistical Assistant 22 26,821$ 36,497$ 46,172$ Statistical Research Assistant Statistical Research Assistant I 26 $ 32,664 $ 44,447 $ 56,230
Statistical Research Assistant II 28 36,046$ 49,049$ 62,052$ Statistician 30 39,779$ 54,128$ 68,478$
Desktop Infrastructure Technician Technology Support Analyst 31 41,787$ 56,862$ 71,936$ Helpdesk Coordinator Technology Support Analyst 31 41,787$ 56,862$ 71,936$ Senior Vice President-Finance Vice President-Financial Operations 46 87,496$ 119,059$ 150,622$


















