resident, non-resident and part-year resident income tax instructions ...
Upload
hester-leonardCategory
view
226download
0
Approach to the breast mass
By : Dr. Faramarz Shahri
Resident of surgery
DIAGNOSING BREAST CANCER
• In 33% of breast cancer cases, the woman discovers a lump in her breast.
• Other less frequent presenting signs and symptoms of breast cancer include (I) breast enlargement or asymmetry; (2) nipple changes, retraction, or discharge; (3) ulceration or erythema of the skin of the breast; (4) an axillary mass; and (5) musculoskeletal discomfort.
• up to 50% of women presenting with breast complaints have no physical signs of breast pathology.
• Breast pain usually is associated with benign disease.
• If a young woman (age 45 years or less) presents with a palpable breast mass and equivocal mammography finding, ultrasound examination and biopsy are used to avoid a delay in diagnosis.
Sab History
• The examiner should determine the patient’s age and obtain a reproductiv history.
• The age of menarche ,menstrual irregulaities ,and the age at menopause should be sougth .
Sab
• Previous surgical procedures should be recorded ,including previous breast biopsies and their pathologies and wether the ovaries were removed if a hysterectomy was performed.
Sab
• Because hysterectomy is a common procedure, accurate determination of menopause may be difficalt .
• It is usefull to inquire abaut menopausal symptoms in these patients .
Sab
• In younger women, a recent history of pregnancy and lactation shoud be recorded .
• A drug history shoud pay attention to hormone replacment therapy or the use of hormones for contraception .
Sab
• The family history should be directed to cancer of the breast and ovaries (parents, siblings, offspring) .
• In questioning the patient about the specific breast problem, it is worthwhile to inquire about breast pain, nipple discharge, and new masses in the breast.
Sab
• If the mass is present, it helps to know how it was found, how long it has been present, what has happened scince it’s discovery, and if it changes with the menstrual cycle .
Sab
• If cancer is likely, inquiry about constitutional symptoms, bone pain, weight loss, respiratory changes, and similar clinical indications of metastatic disease may occasionally reveal unsuspected distant spread .
Examination
Inspection
• The surgeon inspects the woman's breast with her arms by her side, with her arms straight up in the air, and with her hands on her hips (with and without pectoral muscle contraction).
• Symmetry, size, and shape of the breast are recorded, as well as any evidence of edema (peau d'orange), nipple or skin retraction, and erythema.
• With the arms extended forward and in a sitting position, the woman leans forward to accentuate any skin retraction.
Palpation
• Examination of the patient in the supine position is best performed with a pillow supporting the ipsilateral hemithorax.
• The surgeon gently palpates the breast from the ipsilateral side, making certain to examine all quadrants of the breast from the sternum laterally to the latissimus dorsi muscle, and from the clavicle inferiorly to the upper rectus sheath.
• A systematic search for lymphadenopathy then is performed.
Sab Breast examination
• Breast examination shoud be done with respect for privacy and patient comfort in a well-lighted room , preferably whith an available indirect light source.
Sab
• The examination begins with the patient in the upright sitting position with careful visual inspection for abvious masses, asymetries,and skin changes.
Sab
• The nipples are inspected and compared for the superficial epidermis in Paget’s disease.
• The use of indirect lighting can unmask subtle dimpling of the skin or nipple caused by the scirrhous reaction of a carcinoma placing Cooper’s ligament under tention .
Sab
• Simple maneuvers such as gently lifting the patient’s breast may accentuate asymmetries and dimplling .
Sab
• Peau d’orang when combined with tenderness and warmth ,these signs and symptoms are the hallmark of Inflammatory carcinoma and may be mistaken for acute mastitis.
Sab
• Flattening or actual inversion of the nipple can be caused by fibrosis in certain benign conditions, especially subareolar duct ectasia.
Sab
• In these cases , the finding is frequently bilateral and the history confirms that the condition has been present for many years.
• Unilateral retraction or retraction that develops over weeks or months is more suggestive of carcinoma.
FNA
• Because needle biopsy of breast masses may produce artifacts that make mammography assessment more difficult, many radiologists prefer to image breast masses before needle biopsy.
• However, in practice, the first investigation of palpable breast masses is frequently needle biopsy, which allows for the early diagnosis of cysts.
• If the fluid that is aspirated is not bloodstained, then the cyst is aspirated to dryness, the needle is removed, and the fluid is discarded as cytologic examination of such fluid is not cost-effective.
• After aspiration, the breast is carefully palpated to exclude a residual mass.
• If one exists, ultrasound examination is performed to exclude a persistent cyst, which is reaspirated if present.
• If the mass is solid, a tissue specimen is obtained.
• When cystic fluid is bloodstained, 2 mL of fluid are taken for cytology.
• The mass is then imaged with ultrasound and any solid area on the cyst wall is biopsied by needle.
• The presence of blood is usually obvious, but in cysts with dark fluid, an occult blood test or microscopy examination will eliminate any doubt.
• The two cardinal rules of safe cyst aspiration are (I) the mass must disappear completely after aspiration, and (2) the fluid must not be bloodstained.
• If either of these conditions is not met, then ultrasound, needle biopsy, and perhaps excisional biopsy are recommended,
Sab FNA
• Cystic fluid is usually turbid dark green or amber and can be discarded if the mass totally disappears and the fluid is not bloody.
Sab
• By using fine-needle aspiration in the routin examination of the breast ,unnecessary open biopsy of cystic change is avoided.
Sab
• As a result of adding fine-needele aspiration to the routin examination of breast masses , a restating of criteria for open biopsy is done when :
Sab
• 1) needle aspiration prodiuces no cyst fluid and a solid mass is diagnosed.
• 2) the cyst fluid produced is thick and blood tinged.
• 3) fluid is prodiuced but the mass fails to resolve completely.
Sab
• Other surgeons have added the frequent reappearance of the cyst in the same location and the rapid accumulation of fluid after initial aspiration (less than 2 weeks).
Sab
• If the mass is solid and the clinical situation is consistent with carcinoma, a cytologic examination of the aspirated material is performed.
Sab
• Most authors do not recommend definitive treatment based on a cytologic examination.
• In addition,the presence of carcinoma cells on fine-needle aspiration dose not differentiate between in situ and invasive breast cancer.
Sab
• However, a positive result allows for informed discussions with the patient, definitive plans for treatment, and appropriate consultations or second opinions.

Imaging Techniques
Ductography
• The primary indication for ductography is nipple discharge, particularly when the fluid contains blood.
• With the patient in a supine position, 0.1 to 0.2 mL of dilute contrast media is injected and CC and MLO mammography views are obtained without compression.
• Intraductal papillomas are seen as small filling defects surrounded by contrast media.
• Cancers may appear as irregular masses or as multiple intraluminal filling defects.
Mammography
• Conventional mammography delivers a radiation dose of 0.1 centigray (cGy) per study.
• By comparison, a chest x-ray delivers 25% of this dose, there is no increased breast cancer risk associated with the radiation dose delivered with screening mammography.
• With screening mammography, two views of the breast are obtained, the craniocaudal (CC) view and the mediolateral oblique (MLO) view.
• The MLO view images the greatest volume of breast tissue, including the upper outer quadrant and the axillary tail of Spence.
• Compared with the MLO view, the CC view provides better visualization of the medial aspect of the breast and permits greater breast compression.
• In addition to the MLO and CC views, a diagnostic examination may use views that better define the nature of any abnormalities, such as the 90-degree lateral and spot compression views.
• The compression device minimizes motion artifact, improves definition, separates overlying tissues, and decreases the radiation dose needed to penetrate the breast.
• Mammography also is used to guide interventional procedures, including needle localization and needle biopsy
• Specific mammography features that suggest a diagnosis of a breast cancer include a solid mass with or without stellate features, asymmetric thickening of breast tissues, and clustered microcalcifications.
• The presence of fine, stippled calcium in and around a suspicious lesion is suggestive of breast cancer and occurs in as many as 50% of nonpalpable cancers.
• These microcalcifications are an especially important sign of cancer in younger women, in whom it may be the only mammography abnormality.
• That normal-risk women age 20 years or older should have a breast exam at least every 3 years.
• At age 40 years, breast exams should be performed yearly along with a yearly mammogram.
• Xeromammography techniques are identical to those of mammography with the exception that the image is recorded on a xerography plate, which provides a positive rather than a negative image
• Details of the entire breast and the soft tissues of the chest wall may be recorded with one exposure.
Sab Breast imaging
• Breast radiographic imaging is used to detect small ,nonpalpable breast abnormalities ,to evaluate clinical findings, and to guide diagnostic procedures.
Sab
• Mamography is the most sensitive and specific imaging test currently available,though 10% to 15% of clinically evident breast cancers have no mammographic correlate.
Sab
• Digital mammography is a tecnology that acquires digital image and stores them electronically .
• This allows users to manipulate images of the breast to enhance certain strictures or densities while reducing the background of others.
Sab
• Film screen and digital mammography are equivalent in their ability to detect breast cancers.
Sab Screening mammography
• It is performed in efforts to detect breast cancer that is not clinically evident
• It identifies women whose mammograms contain an abnormality and separates these women from those whose mammograms are clearly normal .
Sab
• At present , screening mammography schoud be offered annually to women age 50and older , and at least biennialy in women age 40 to 49 with the screening interval made on an individual basis and considering the risk factors for breast cancer .
Sab
• Younger women with a significant family history , histologic risk factor , or a history of prior breast cancer shoud be offerrd annual screening .
Sab Diagnostic mammography
• It is performed when there is a abnormality on clinical exmination or screening mammography .
Sab
• It includes magnification and compression imaging in the MLO and CC views obtained with screening mammography , and is frequently supplemented by ultrasound .
Sab
• The mammographic features of malignancy can be broadly divided into density abnormalities (masses , architectural distortion, and assymetries ) and microcalcifications .
Sab
• Each mammogram is also assessed for the presence of abnormalities in the axillary nodes and for the presence of skin or nipple changes , such as thickening or retraction.
Ultrasonography
• Second only to mammography in frequency of use for breast imaging ultrasonography is an important method of resolving equivocal mammography findings, defining cystic masses, and demonstrating the echogenic qualities of specific solid abnormalities.
• On ultrasound examination, breast cysts are well circumscribed, with smooth margins and an echo-free cent.
• Benign breast masses usually show smooth contours, round or oval shapes, weak internal echoes, and well-defined anterior and posterior margins.
• Breast cancer characteristically has irregular walls, but may have smooth margins with acoustic enhancement.
• It is highly reproducible and has a high patient acceptance rate, but does not reliably detect lesions that are 1cm or less in diameter.
MRI
• In the process of evaluating MRI as a means of characterizing mammography abnormalities, additional breast lesions have been detected.
• However, in the circumstance of both a negative mammogram and a negative physical examination, the probability of a breast cancer being diagnosed by MRI is extremely low.
• There is current interest in using MRI to screen the breasts of high-risk women and of women with a newly diagnosed breast cancer
Sab CT.Scan
CT appears to be the best way to image internal mammary nodes and to evaluate the chest and axilla after mastectomy.
Sab MRI
• MRI is the imaging method of choice to evaluate implant rupture.
• It may be used in efforts to identify the primary site of cancer in the breast of a woman who presents with malignant axillary adenopathy in the context of an un revealing breast physical examination and mammogram(accult breast cancre ).
Sab
• Particularly for an invasive lobular breast cancer diagnosed by core needle biopsy , where physician examination and mammography may underestimate the extent of disease , MRI may facilitate the decision as to whether the patient is an appropriate candidate for breast conservation .
Sab
• Its efficacy as a screening tool remain unproven , though studies in population at increesed risk for breast cancer appear promising .
• MRI sensitivity for invasive cancer approches 100%, but is only 60% at best for DCIS .
Sab
• Specificity remain low , with significant overlap in the appearance of benign and malignant lesions .
Breast Biopsy
Nonpalpable Lesions
• Image-guided breast biopsies are frequently required to diagnose nonpalpable lesions.
• Ultrasound localization techniques are employed when a mass is present, while stereotactic techniques are used when no mass is present (microca1cifications only).
• The combination of diagnostic mammography, ultrasound or stereotactic
localization, and fine-needle aspiration (FNA) biopsy is almost 100% accurate in the diagnosis of breast cancer.

• However, while FNA biopsy permits cytologic evaluation, core-needle or open biopsy also permits the analysis of breast tissue architecture and allows the pathologist to determine whether invasive cancer is present.
• Core-needle biopsy is accepted as an alternative to open biopsy for nonpalpable breast lesions.
• The advantages of core-needle biopsy include a low complication rate, avoidance of scarring, and a lower cost.
Sab Non palpable mammographic abnormalities
• Mammographic abnormalities that cannot be detected by physical examination are classified in three broad categoty : (1) lesions consisting of microcalcification only , (2)density lesions (masses ,architectural distortion , and asymmetries),and (3)those with both calcifications and density abnormalities .
Sab
• The incidence of malignancy after biopsy depends on the characteristics of the radiographic finding .
Sab
• Lesion with microcalcification with an assosiated mass and linear branching calcifications carry the highest probability of being malignant .
Sab
• However , even well-defined , smooth densities can be malignant .
• Not every abnormalities should undergo biopsy , and recommendation should be made by surgeons in consultation with an experienced radiologist .
Sab
• For some patients not undergoing biopsy , a mammogram repeated in a shorter interval (6months) may be recommended to establish stability of the abnormality .
Sab
• The two methods available to evaluate a nonpalpable mammographic abnormality include wire localization with surgical excisional biopsy and image-guided stereotactic or ultrasound-guided large-core needle biopsy .
Sab Large core needle biopsy(LCNB)
• Since the early 1990s,LCNB increasingly is the diagnostic method of choice to histologically evaluate nonpalpable mammographic abnormalities .
• In experienced centers , it is considered the standard of care .
Sab
• LCNB can be performed using either mammographic (stereotactic) or ultrasound guidance .
• Mammographic calcifications are typically sampled using stereotactic capabilities .
Sab
• In the experienced centers , 65%of women who undergo the procedure are found to have a benign diagnosis and can resume annual mammographic screening .
Sab
• 25% of patients are found to have a malignancy.
• The diagnosis of malignancy by core biopsy affords the apportunity to proceed with one definitive surgery , with efforts toward breast preservation when appropriate and chosen by the patient.
Sab
• The remaining 10% of patients are found to have inconclusive histology , including: (1)atypical cells on pathology (atypical ductal hyperplesia ),(2)biopsy result that are discordant from the mammography findings ,(3) increased cellularity within a fibroadenoma,or(4)inadiquate sampling of the site.
Sab
• In these cases where the core obtained does not contain cancer , and the histology does not entierly explain the mammographic finding, surgical biopsy is recommended.
Sab
• The false-negative rate of stereotactic biopsy shoud be extremely low if these guidelines are followed.
Sab Atypia on core needle biopsy
• For patient with atypia on core needle biopsy ,a wire localization and excisional biopsy are performed to clarify the histology.
Sab DCIS on core needle biopsy
• For patients with a core needle biopsy diagnosis of DCIS , 7% have had the lesion fully excised with the core needle .
Sab
• At the time of surgical excision ,an upgrade of the DCIS is seen in 12% of patient who had undergone core needle biopsy using an 11-gauge,vacum-assisted needle device .
Palpable Lesions
• FNA biopsy of a palpable breast mass is performed in an outpatient setting.
• The cellular material is then expressed onto microscope slides.
• Both air-dried and 95% ethanol-fixed microscopy sections are prepared for analysis.
• When a breast mass is clinically and mammographically suspicious, the sensitivity and the specificity of FNA biopsy approaches 100%.
• Core-needle biopsy of palpable breast masses is performed using a 14-gauge needle, such as the Tru Cut needle.
• Automated devices also are available.
• While the false-negative rate for core-needle biopsy is very low, a tissue specimen that does not show breast cancer cannot conclusively rule out that diagnosis because a sampling error may have occurred.
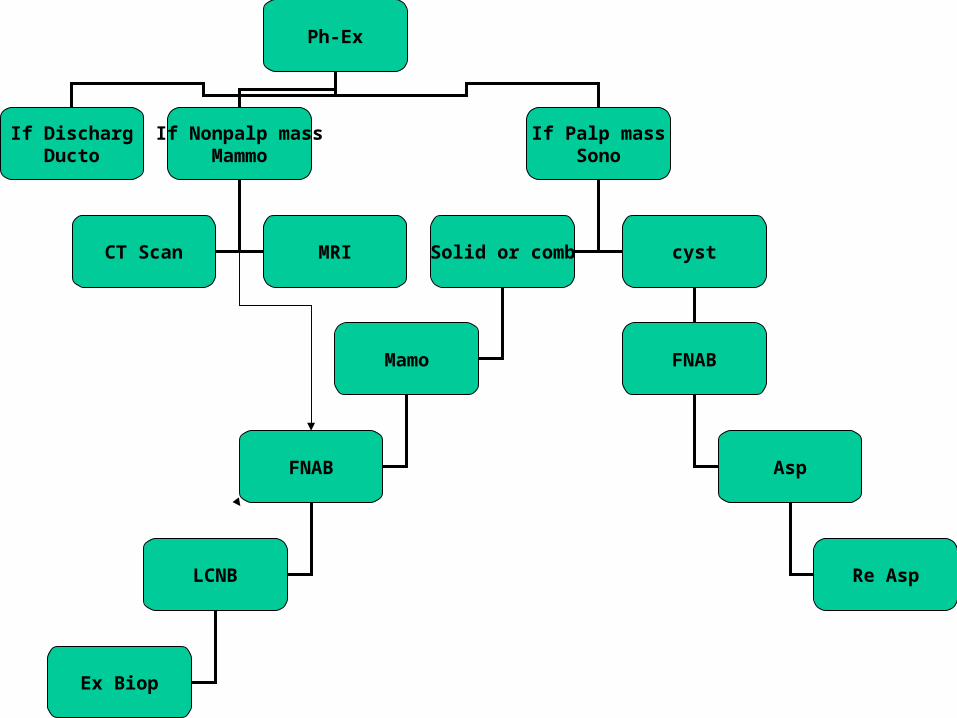
Ph-Ex
If DischargDucto
If Nonpalp massMammo
If Palp massSono
Solid or comb cyst
FNAB
Asp
Mamo
FNAB
LCNB Re Asp
Ex Biop
CT Scan MRI
را تيشه هاي طاقتضربه كه سنگي ندارد
زيبا تنديسيشد نخواهد
“ زرتشت حضرت“


Fibroadenomas
• Removal of all fibroadenomas has been advocated irrespective of patient age or other considerations, and solitary fibroadenomas in young women are frequently removed to alleviate patient concern.
• Yet most fibroadenomas are self-limiting and many go undiagnosed, so a more conservative approach is reasonable.
• Careful ultrasound examination with core-needle biopsy will provide for an accurate diagnosis, Subsequently, the patient is counseled concerning the biopsy results, and excision of the fibroadenoma may be avoided.
Sclerosing Disorders
• The clinical significance of sclerosing adenosis lies in its mimicry of cancer,
• It may be confused with cancer on physical examination, by mammography, and at gross pathologic examination,
• Excisional biopsy and histologic examination are frequently necessary to exclude the diagnosis of cancer
• The diagnostic workup for radial scars and complex sclerosing lesions frequently involves stereoscopic biopsy,
• It is usually not possible to differentiate these lesions with certainty from cancer by mammography features, so biopsy is recommended.
Periductal Mastitis
• Painful and tender masses behind the nipple-areola complex are aspirated with a 12-gauge needle attached to a 10-mL syringe.
• Any fluid obtained is submitted for cytology and for culture using a transport medium appropriate for the detection of anaerobic organisms.
• In the absence of pus, women are started on a combination of metronidazole and dicloxacillin while awaiting the results of culture.
• when there is considerable pus present, surgical treatment is recommended.
• Unlike puerperal abscesses, a subareolar abscess is usually unilocular and often is associated with a single duct system.
• Preoperative ultrasound will accurately delineate its extent.
• In a woman of childbearing age,
simple drainage is preferred, but if there is an anaerobic infection, recurrent infection frequently develops.
• Recurrent abscess with fistula is a difficult problem and may be treated by fistulectomy or by major duct excision, depending on the circumstances.
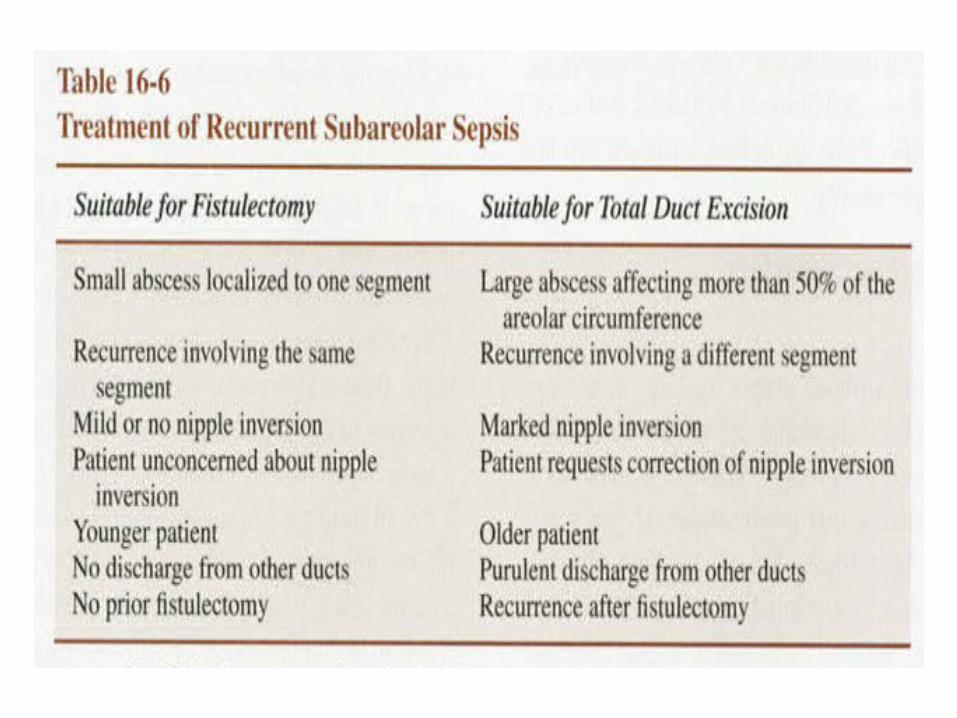
• When a localized periareolar abscess recurs at the previous site and a fistula is present, the preferred operation is fistulectomy, which has minimal complications and a high degree of success.
• when subareolar sepsis is diffuse rather than localized to one segment or when more than one fistula is present, total duct excision is the preferred procedure,
• fistula excision is the preferred initial procedure for localized sepsis irrespective of age.
• Antibiotic therapy is useful for recurrent infection after fistula excision, and a 2- to 4-week course is recommended prior to total duct excision
Nipple Inversion
• Congenital nipple inversion.
• Secondary to duct ectasia.
• Surgical complications : altered nipple sensation, nipple necrosis, and postoperative fibrosis with nipple retraction.
• Because nipple inversion is a result of shortening of the subareolar ducts, a complete division of these ducts is necessary for permanent correction of the disorder.