Approach to Rheumatologic Investigations September 10,2015.
63
Approach to Rheumatologic Investigations September 10,2015
-
Upload
marjorie-brown -
Category
Documents
-
view
223 -
download
0
Transcript of Approach to Rheumatologic Investigations September 10,2015.

Approach to Rheumatologic Investigations
September 10,2015

Objectives
• To review “Choosing Wisely” recommendations for Rheumatology and use within the clinical context
• To review the interpretation of common blood tests in the clinical context
• To review synovial fluid analysis

Visit Rate by Diagnosis
• All- 162.7/1000• OA- 40.7• RA- 7.4• CTD- 1.9• AS- 1.1• Gout- 5.2

Choosing Wisely
1) Don’t order an ANA without specific symptoms of SLE or another CTD
2) Don’t order HLA B27 testing unless spondyloarthropathy is suspected based on specific signs and symptoms
3) Don’t order whole body scans for screening for peripheral or axial arthrits

20 year old female developed swelling in her left elbow in March.
Swelling in her right knee in June and shortly there after saw her family physician.
She complained of pain in her hands, wrists, elbows, knees and feet
She was fatigued and stiff for 3 hours in the morning
The Case for ANA

• She has mild Raynauds• She denies a rash, fever, oral or nasal
ulceration, photosensitivity, or pleuritic chest pain
• She denies psoriasis, colitis, iritis • She is sexually active but has had one
boyfriend for the past 2 years• She has lost 10 lbs

• HPH- hypothyroidism• Family History- Her grandmother has
rheumatoid arthritis• F.I. - noncontributory

Examination
• Her general exam is normal• She has slight fusiform swelling of her PIPs,
MCPs .• Her wrists, L elbow are swollen• Her shoulders are tender• Her knees are swollen and her MTP joints are
all tender

What does RA look like?
Early RA in hands and fingers

Differential Diagnosis
• New onset of an inflammatory arthritis in a 20 y.o. female
- stiffness for three hours - fatigue - weight loss - swollen, tender joints - symmetrical pattern, involving the PIPs,
MCPs, wrists, knees, feet

Appropriate Lab Investigations
• CBC, ESR• CRP• Rheumatoid factor• Ant CCP• Antinuclear antibody• Urinalysis• LFTs, BUN and Creatinine

Rheumatoid Factor
• This is an immunoglobulin that binds to the Fc portion of IgG.
• The usual method for detecting an rheumatoid factor is the latex fixation. This only measures the IgM immunoglobulin.
• The RF is elevated in 1-2% of a healthy population.
• It may be elevated in chronic inflammatory conditions.

• Approximately 75% of patients with rheumatoid arthritis have a positive RF.
• In early disease, the rheumatoid factor can be negative
• High levels predict a poor outcome• Sjogren’s syndrome is associated with a high
positive rheumatoid factor• Hepatitis C causes a positive rheumatoid
factor

Anti CCP Antibodies (ACPA)
• are as sensitive as, and more specific than, IgM rheumatoid factors (RF) in early and fully established disease
• may predict the eventual development into RA when found in undifferentiated arthritis
• are a marker of erosive disease in RA/response to MTX
• may be detected in healthy individuals years before onset of clinical RA

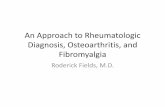
Table 1 Specificity and sensitivity of the CCP2 test for RA
van Venrooij, W. J. et al. (2011) Anti-CCP antibodies: the past, the present and the futureNat. Rev. Rheumatol. doi:10.1038/nrrheum.2011.76

Antinuclear Antibody
• These are autoantibodies that react to a variety of nuclear antigens.
• These antibodies are sensitive markers for SLE but are found in 5% of normals and with other diseases.
• It is highly unlikely a patient has SLE if the ANA is negative.
• The specifcity is low.


Diffuse Pattern

ENA
• Anti Ro and anti La- high frequency in Sjogrens and SLE
• Found in 50% of patients with SLE and are associated with a photosensitive rash, subacute cutaneous lupus, neonatal lupus and congenital heart block.
• Found in 75% of patients with Sjogren’s syndrome

• Anti Sm- Seen in SLE often in combination with RNP.
• Very specific for SLE
• Anti RNP on its own is seen in MCTD

Antiphospholipid Antibodies
• Lupus anticoagulant- prolonged PTT• Anti- cardiolipin antibody
• Associated with hypercoaguable state, thrombocytopenia and 2nd trimester abortions

Our Patient
• Hgb 107, MCV 76• Platelets 425,000, CRP 40• WBC 8.9• Rheumatoid factor- negative • Anti CCP- high positive• ANA neg• Urinalysis - normal

What does RA look like?

Rheumatoid Arthritis
A systemic inflammatory disease characterized by synovial proliferation that leads to bones destruction, cartilage loss, progressive deformities and serious functional disability
It affects approximately 1% of the population or 300,000 Canadians
It is more common in women 3:1 ratio and mean age of onset is between 52 years.

• 50% of patients are disabled within 10 years of the onset of disease.
• Severe disease is associated with premature mortality/ cardiovascular
• Joint erosions occur in 93% of patients within 2 years of disease onset.
• Erosions occur as early as four months after disease onset.
• Erosions predict a poor functional outcome

• Bony erosions and deformity are irreversible
• Initiation of a DMARD after 3 months of disease is crucial as a delay of even three months results in more radiographic damage at 5 years.
• “Window of Opportunity” – supported by COBRA trial and ERA trial with Entanercept and a meta-analysis of 1400 patients and 14 trials
• 50% of RA patients are not on DMARDs

Scenario 2 lab Work
Hgb 107 Platelets 98,000 WBC 2.1 R.F.- negative ANA 1/1600 speckled homogenous Urinalysis – 10 RBC/hpf, 10 WBC/hpf, 3 gms of
protein/L LFTs normal, Cr 134 and BUN 9.0

• Anti DNA- specific for SLE-95%• sensitivity-30-70%• Levels will fluctuate with disease activity• high levels are associated with active
glomerulonephritis


Interpretation
• Likely SLE with renal and hematological disease. Patient needs to be referred urgently.
• Order anti DNA, anti ENA, C3, C4, 24 hour urine for Cr clearance
• Likely requires renal biopsy

Scenario 3
• On exam: pitting of the nails• Mild erythema and scaling behind the ears• Blood work: ESR 40, CRP 22 RF neg, ANA neg

Interpretation
• Likely psoriatic arthritis• Subtype that is similar to RA• Serology negative in keeping with psoriatic
arthritis• Increased ESR and CRP in keeping with
inflammatory process• Pitting of nails and rash likely significant

Summary
• RHEUMATOID ARTHRITIS is the most common inflammatory arthritis you will see.
• Early recognition and referral alters outcome of the disease.
• SLE and other CTD are rare.

The Needle in a Haystack
• Axial SpA is found in approximately .5-1.9 % of the population
• It is found in about 5% of patients with chronic back pain
• The average length of time until diagnosis- 8 years• Diagnosis has required an abnormal sacroiliac X ray
and there may be a lag time from 8 -11 years after the onset of inflammatory back pain
• New therapies substantially reduce pain and disability and increase quality of life

Inflammatory Back Pain• Insidious onset• > 3months duration• Stiffness >30 minutes• Improvement with moderate physical activity• Diffuse non radiating pain in both buttocks

Plain radiograph showing bilateral sacroiliitis in a patient with ankylosing spondylitis.
McVeigh C M , Cairns A P BMJ 2006;333:581-585
©2006 by British Medical Journal Publishing Group

HLA B27• Class 1 gene• HLA B2705 strongest assoc• Also 2702,2703,2704,2707• Prevalence varies with the distance from the
equator, highest in Northern European countries• If HLA B27+ then 1-2% chance of developing the
disease• 15-20% develop AS if a first degree relative has
the disease


Likelihood Ratios• -a formulation of sensitivity and specificity of a test
into one value which is an indicator of the diagnostic value of the test
• +LR = (sensitivity)/(1-specificity) odds that a given diagnostic test would be positive in a patient with the disorder being tested
• -LR= (1-sensitivity)/specificity• In AS multiples of LR for clinical, radiographic and
genetic tests combined with pretest probabilities based on prevalence result in post test probabilities

• IBP – in 5% of back pain population• Hx of IBP LR=3.1 (probability 14%)• HLA B27+ LR=9.0 (probability 40%) • MRI evidence of sacroiliitis LR=9.0• The post test probability of AS is 93%

Final set of classification criteria for axial spondyloarthritis (SpA) selected by the Assessment of SpondyloArthritis international Society (ASAS).
Rudwaleit M et al. Ann Rheum Dis 2009;68:777-783
©2009 by BMJ Publishing Group Ltd and European League Against Rheumatism

Decision tree on diagnosing axial SpA.
Rudwaleit M et al. Ann Rheum Dis 2004;63:535-543
©2004 by BMJ Publishing Group Ltd and European League Against Rheumatism

ESR/CRP
• 72 y.o. woman complains of stiffness in the morning such that her husband has to pull her out of bed. The stiffness lasts 4 hours. She complains of pain in her shoulders and hips.
• Exam: pain on palpation of proximal muscles• no muscle weakness• Labs ESR 70, CRP 40• What is like diagnosis?

Polymyalgia Rheumatica
• Does not occur before age 50!• Muscle pain, not weakness• Symptoms should disappear within 48 hours
of starting 15-20 mgs of prednisone, reconsider diagnosis otherwise
• The onset of rheumatoid arthritis can be proximal muscle pain and stiffness in this age group.

Erythrocyte Sedimentation Rate
• During an acute phase response,plasma proteins form in abundance.
• These include paraproteins and immunoglobulins
• An ESR is measured by diluting the serum in sodium citrate , standing the tube upright and measuring the distance the red cells fall in 1 hour.

• If there is abundant paraprotein then the red cells will stick together called rouleaux
• The stacked cells are heavier and will fall quickly
• An ESR will increase with age• To calculate the upper limit for a man, divide
the age by 2.• For a woman, age +10 divided by 2

Intrepretation of an ESR
• An elevated ESR indicates an inflammatory response- infectious, immunologic or malignant.
• It is a crude guide to the severity of inflammation.
• It is increased in pregnancy, anemia and renal failure.

C-Reactive Protein
• This is a protein synthesized in the liver after tissue injury.
• It is a more timely indicator of inflammation than the ESR.

• 58 year old man presents with history of waking the night before with a painful swollen R ankle
• The pain is so severe he can’t bare weight on it
• He has been awake all night • History of similar episode 6 months ago and
the year before that, no kidney stones
Monoarthritis

• HPH _ hypertension, hyperlipidemia• Social_ drinks 2-3 beer per night, non smoker• Family_ father has gout• Meds_ hydrochlorthiazide 25 mgs po od,
lipitor 40 mgs po od, ASA 81 mgs po od• F.I. _ non contributory

• Exam- BP 140/86 temp 38.7 C• Wt- 230 kgs, height 5”10”• General exam otherwise normal• Dermatology- psoriasis scalp, elbows, knees• MSK- swollen R ankle

DifferentialDiagnosis
• Infection- Bacterial• Crystal-induced= Monosodium urate, Calcium
pyrophosphate dihydrate, Hydroxyapatite, Calcium oxalate, Lipid
• Hemarthrosis- Trauma, Anticoagulation, Clotting disorders, Fracture, Pigmented villonodular synovitis


Diagnostic Test?

Investigations
• Blood work- WBC 14,500, 85% neutrophils• ESR 45, CRP 56• Cr 110 mmol/l • uric acid level 456 mmol/l• Joint aspiration – WBC 36,000• - negatively birefrigent crystals• X ray- soft tissue swelling 1st MTP and ankle

Condition Cell count crystals Culture/gm stain
Gout 2000-50,000 -birefringent neg
CPPD 2000-50,000 +birefrigent neg
septic > 50,000 neg +
inflamed 2000-30,000 neg neg
normal <2000 neg neg





CPPD
• Pseudogout – wrists, knees, mid foot shoulder• Pseudoosteoarthritis- 2nd,3rd MCP, wrists,
shoulders• Pseudorheumatoid- MCPs, wrists, feet usually
spared• Pseudocharcot joint- mid foot• Associations- hemochromatosis,
hyperparathroidism. hypothroidism, hypomagnesemia, hypophosphatemia

Treatment
• NSAIDs• Colchicine• Injection of joint with corticosteroids