Approach to Pulmonary Manifestations of HIV/AIDS
20
Approach to Pulmonary Manifestations of HIV/AIDS Dr. Flip Otto Dept. of Radiology Universitas Academic Hospital
description
Approach to Pulmonary Manifestations of HIV/AIDS. Dr. Flip Otto Dept. of Radiology Universitas Academic Hospital. Pulmonary Manifestations of HIV/AIDS. Opportunistic infection Drug reactions Immune restoration syndrome Lymphoproliferative disorders AIDS related malignancy - PowerPoint PPT Presentation
Transcript of Approach to Pulmonary Manifestations of HIV/AIDS

Approach to Pulmonary Manifestations of HIV/AIDS
Dr. Flip OttoDept. of RadiologyUniversitas Academic Hospital

Pulmonary Manifestations of HIV/AIDS
Opportunistic infection Drug reactions Immune restoration syndrome Lymphoproliferative disorders AIDS related malignancy Non-specific interstitial pneumonitis HIV related pulmonary hypertension Bronchiolitis obliterans Emphysema and bronchiectasis

Infective pulmonary conditions in HIV/AIDS
Bacterial PJP TB MAI Fungal: Cryptococcus; Aspergillosis etc. Viral: CMV

Non-infective pulmonary conditions in HIV/AIDS
Kaposi’s sarcoma Lymphoma Lung carcinoma Lymphocytic interstitial pneumonitis Emphysema Cardiovascular complications

Prevalence of HIV/AIDS associated pulmonary conditions in relation to CD4 count
CD4>400: Increased risk for - Bacterial infection - Mycobacterium tuberculosis CD4 200-400: Increased risk for - Recurrent bacterial infections - Mycobacterium tuberculosis - Lymphoma and lymphoproliferative disorders CD4<200: Increased risk for - PJP - Disseminated Mycobacterium tuberculosis CD4<100: Increased risk for - PJP - Atypical Mycobacterium tuberculosis - CMV - Kaposi’s sarcoma - Lymphoma

Radiographic patterns
Nodules Cavities Adenopathy Focal consolidation Pleural effusion

Nodules
Common Size: - <1cm (random or centrilobular) more likely due to
infection - >1cm more likely neoplastic Miliary nodularity typically fungal or TB, rarely seen
in PJP KS peribronchovascular vs lymphoma and lung
cancer peripheral

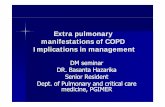
Miliary TB

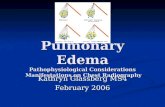
CMV pneumonia

Cavities
Mostly infective 85% polymicrobial, majority bacterial: mixed
infections often involving Staph and Pseudomonas
Remainder include: TB, PJP, fungi, CMV

Necrotizing cavitating pneumonia

Pneumocystis pneumonia

Adenopathy
Mostly due to infection TB most common cause of isolated adenopathy, can
be seen with Cryptococcus. Associated with low attenuation with ring enhancement.
Lung cancer included in differential diagnosis Calcified adenopathy: TB, fungus, described in PJP Hyperattenuating adenopathy in KS due to vascular
enhancement

TB lymphadenopathy

Focal consolidation
Mostly due to infection Bacterial pneumonia most common cause in
AIDS, but Pneumocystis most common individual pathogen (rarely segmental pattern)
TB, MAI, fungi (Cryptococcus), mixed infections and occsionally neoplasms (lymphoma and KS)

Primary TB

Pleural effusion
Majority small, equal incidence in infection and malignancy
Infective causes (bacterial and TB) tend to be unilateral
KS associated tend to be bilateral Non-AIDS causes eg PE and organ failure
should also be considered

Kaposi sarcoma

Approach
Combine: - Risk factors - Level of immunocompromise - prophylactic Rx - clinical presentation - radiographic pattern CD4 count most important determinant for assessing
relative likelyhood Chest radiography 1st line imaging CT and HRCT 2nd line when CXR findings equivocal
or non-specific

References
Aviram G, Fishman JE, Boiselle PM. Thoracic manifestations of AIDS. Applied Radiology 2003;Vol 32:8
Allen CM, Al-Jahdali HH, Irion KL, Ghamen SA, Gouda A, Khan AN. Imaging lung manifestations of HIV/AIDS. Ann Thorac Med 2010;5:201-16












![Severe pulmonary radiological manifestations are ... · radiographic manifestations of pulmonary TB [15]. Other studies, however, have failed to demonstrate that DM impacts radiographic](https://static.fdocuments.in/doc/165x107/5fd15363a2500027f4297b60/severe-pulmonary-radiological-manifestations-are-radiographic-manifestations.jpg)