
Approach to coma
43
APPROACH TO COMATOSE CHILD Dr Surya Ganapathi MD
-
Upload
surya-ganapathi -
Category
Education
-
view
62 -
download
1
Transcript of Approach to coma

APPROACH TO COMATOSE CHILD
Dr Surya Ganapathi MD

Objectives
Incidence
Definition
Causes
Evaluation & management
Outcome & prognosis

RAS

COMA
Medical emergency
Diagnostic & therapeutic challenge
Causes are numerous
Critical window period for diagnosis and intervention
Pediatricians have to frequently manage coma cases .

Incidence
Non-traumatic coma - 30/100,000 children per year
Traumatic brain injury - 670/100,000
Wong CP, Forsyth RJ, Kelly TP, et al. Incidence, etiology and outcome of non-traumatic coma: a population based study. Arch Dis Child.
2001;84:193–9

Incidence, etiology and outcome of non-traumatic coma: a population based studyC P Wong et al , Arch Dis Child 2001;84:193-199
Abstract AIM To determine the incidence, presentation, etiology, and outcome of non-
traumatic coma in children aged between 1 month and 16 years. METHODS In this prospective, population based, epidemiological study in the
former Northern NHS region of the UK, cases were notified following any hospital admission or community death associated with non-traumatic coma. Coma was defined as a Glasgow Coma Score below 12 for more than six hours.
RESULTS The incidence of non-traumatic coma was 30.8 per 100 000 children under 16 per year (6.0 per 100 000 general population per year). The age specific incidence was notably higher in the first year of life (160 per 100 000 children per year). CNS specific presentations became commoner with increasing age. In infants, nearly two thirds of presentations were with non-specific, systemic signs. Infection was the commonest overall aetiology. Aetiology remained unknown in 14% despite extensive investigation and/or autopsy. Mortality was highly dependent on aetiology, with aetiology specific mortality rates varying from 3% to 84%. With follow up to approximately 12 months, overall series mortality was 46%.

Non traumatic coma.Bansal A1, Singhi SC, Singhi PD, Khandelwal N, Ramesh S.
Indian J Pediatr. 2005 Jun;72(6):467-73.
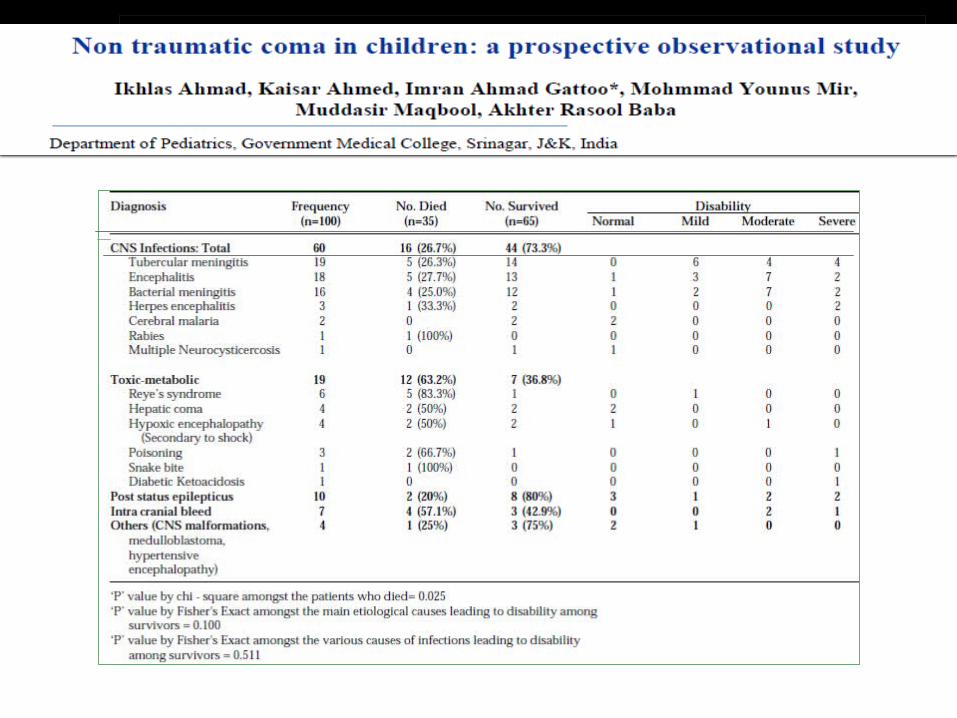
OBJECTIVE: To study the etiology and clinical profile of non-traumatic coma in children and to
determine the clinical signs predictive of outcome. METHODS: 100 consecutive cases of non-traumatic coma between 2 months to 12 years. Clinical signs
studied were temperature, pulse, heart rate, blood pressure, coma severity by Glasgow coma scale (GCS), respiratory pattern, pupillary and corneal reflex, extra ocular movements, motor patterns, seizure types and fundus picture. These were recoded at admission and after 48 hours of hospital stay. Etiology of coma was determined on basis of clinical history, examination and relevant laboratory investigations by the treating physician..
RESULTS: Etiology of coma in 60% cases was CNS infection (tubercular meningitis-19, encephalitis-18,
bacterial meningitis-16, others-7); other causes were toxic-metabolic conditions (19%), status epilepticus (10%), intracranial bleed (7%), and miscellaneous (4%). 65 children survived, 11 were normal, 14 had mild disability, 21 had moderate disability and 14 were severely disabled and dependent. Survival was significantly better in patients with CNS infection (63%) as compared to those with toxic-metabolic causes (27%) and intracranial bleed (43%, P < 0.05).
Definition
State of altered consciousness with
loss of wakefulness ( arousal , vigilance ) and loss of awareness of self & environment
Should lasts for at least one hour
Swaiman KF, Ashwal S, Ferriero DM, editors. Pediatric neurology: principles and practice. 4th ed.

Coma – continuum
Vegetative state
• Unawareness of self and environment
• Preserved brain stem reflexes• 3months after Nontraumatic
injury
Brain death • Irreversible comatose child• Brain stem reflexes are lost

Not equivalent to coma - usage obsolete now
Lethargy reduced wakefulness
Obtundation blunted alertness , diminished awareness to environment
Stupor Unresponsive but arousable with vigorous stimulus
Minimal Conscious State definite behavioral evidence of self- or environmental awareness is intact
Akinetic Mutism Slowing of movement and cognitionPreserved wakefulness & awareness
Locked In Syndrome Complete paralysis with preserved consciousness

Causes
Diffuse bilateral hemispheric processToxins and drugs• Alcohol, narcotics, benzodiazepines
Metabolic• Diabetic ketoacidosis/ hyperosmolar
coma• Hepatic encephalopathy• Hypercarbia• Hypoglycemia• Hypothyroidism• Hypo/hypernatremia• Hypo/hyperthermia• Hypo/hypercalcaemia• Hypoxia• Porphyria• Uremia
Other• Head trauma/ NAI• Hypertensive encephalopathy• Meningitis, encephalitis, Reye’s
syndrome• Seizures, post-ictal• Sepsis• Subarachnoid haemorrhage
Brainstem pathology• Brainstem infarction or haemorrhage• Herniationfrom any space-occupying
lesion• Posterior fossatumour• Severe trauma• Wernicke’sencephalopathy

1)Coma with focal signs2) Coma without focal signs and without meningeal irritation3) Coma without focal signs and with meningeal irritationHypoxia-Ischemia: Cardiac or pulmonary failure, Cardiac
arrest, Shock, Near drowning• Metabolic disorders: Hypoglycemia Acidosis (e.g. Organicacidemias, diabetic keto-acidosis) Hyperammonemia (e.g. hepaticencephalopathy, urea cycle disorders, valproic acid encephalopathy,disorders of fatty acid metabolism, Reye syndrome) Uremia,Fluid and Electrolyte disturbances (dehydration, hyponatremia,hypernatremia)• Systemic Infections: Bacterial: gram-negative sepsis, meningitis,toxic shock syndrome, cat-scratch disease, Shigella encephalopathy,Enteric encephalopathy• Post infectious disorders: Acute necrotizing encephalopathy,ADEM, Hemorrhagic shock and encephalopathy syndrome• Post immunization encephalopathy: Whole cell pertussis vaccine,Semple Rabies vaccine• Drugs and toxins• Cerebral malaria• Rickettsial: Lyme disease, Rocky mountain spotted fever• Hypertensive encephalopathy• Post seizure states• Non-convulsive status epilepticus• Post migraine
• Meningitis• Encephalitis• Subarachnoid hemorrhage
• Intracranial hemorrhage• Stroke: arterial ischemic or sinovenous thrombosis• Tumors• Focal infections-brain abscess• Post seizure state: Todd’s paralysis• Acute disseminated encephalomyelitis

C P Wong et al , Arch Dis Child 2001;84:193-199

Int J Contemp Pediatr. 2015 May;2(2):77-84

Acute management
• Rapid assessment of general state.
• Non Specific interventions for all ill children.
• Specific measures to rapidly categorize cause of coma.
• Institute specific interventions when cause verified.

Preliminaries
• Check Airway
• Breathing
• Circulation
• Check pupil size, symmetry, and reaction to light

Rapid assessment
APVU scale : •Alert•Responds to Voice•Responds to Pain•Unresponsive
Monitor : Heart rate, Respiration, Oxygen saturation, BP, temperature, ECG.

Rapid History
Infections : fever ,headache , vomiting , rash , seizures,irritable
Encephalopathy with preceding fever or minor illness
ADEM , IEM , Reye’s syndrome
Toxin exposure , trauma , animal bite ( dog / snake)
Seizures / past medical history & family history

General examination
Vital signs
Head to toe examination
bite marks for snake bite , regional lymphadenopathy , local signs if present

Neurological assessment
Level of consciousness
Pupils
Motor response
Brainstem function
Fundus
Signs of meningeal irritation
Herniation syndromes

Herniation Syndromes

Problem check list
• Shock• Sepsis• Trauma /NAI• Metabolic illness• Intracranial infection Snake bite Toxin exposure
Always check blood sugar
Raised intracranial pressure
• Hypertension• Status epilepticus• Post convulsive state• Cause unknown

Investigations
Basic investigations :
Blood glucose , complete blood count , blood biochemistry
Urine ketones / reducing substances
Blood & urine culture
CSF study
PS for malaria
WBCT – whole blood clotting time
CT – trauma / hemorrhage / stroke / abscess

Investigations

Second line of investigations Metabolic testing MRI EEG In unexplained cases – thyroid antibodies / CNS vasculitis
Serum ammonia , lactate
Serum & urine amino &organic acidsFree fatty acid ,
carnitine Viral encephalitis
ADEM
Diffuse Theta & Delta ActivityTriphasic WavesPledsEpileptiform Activity
Investigations

Second Line Investigations

Treatment – Initial Stabilization

Non Specific intervention – General measures

Raised ICP – management
Immediate management : tilt head up 20 to 30 degrees. Ensure adequate circulation –do not restrict fluids routinely.
Avoid hypotonic fluids
If there is good urine output consider osmotic diuresis with either 20% mannitol or 3% saline. Oral Glycerol useful in meningitis
Consider ventilating the child to maintain PaCO2 between 4.0 to 4.5kPa.

Raised ICP – management
Systemic review of all studies - use osmotic agents to treat raised intracranial pressure in traumatic and non traumatic encephalopathies
Hypertonic saline improved ICP and maintained Cerebral Perfusion Pressure better than Mannitol.
The role for osmotic agents in children with acute encephalopathies; a systemic review. Gweret al BMC pediatrics, 2010,10:23

Specific intervention

Treat as per identified cause

Accidental Vs Inflicted Head Injury (iHI)
Infants presenting with non specific symptoms or altered consciousness with seizures have may have inflicted head injury(iHI).
Estimated incidence in UK is 21-24 per 100,000 infants annually.
Clinicians need to be familiar with signs pointing to iHI
Which clinical features distinguish inflicted from non-inflicted brain injury? A systematic review.Arch DisChild 2009 94: 860-867

Apnea has a positive predictive value of 93% and an Odds Ratio of 17.
Retinal Hemorrhages have a PPV of 71% with an Odds Ratio of 3.5.
A child with intracranial injury with retinal hemorrhages is significantly more likely to have iHI.
Absence of history of trauma had PPV of 92% with a specificity of .97. Only 1 study
Which clinical features distinguish inflicted from non-inflicted brain injury? A systematic review.Arch DisChild 2009 94: 860-867
Accidental Vs Inflicted Head Injury (iHI)

Rib fractures : 73% PPV and OR of 3.02, but wide confidence interval, so not so useful.
Seizures : PPV of 66% and OR of 2.9 also with wide confidence interval.
Long bone fracture : PPV of 59%, OR of 1.72. Hence weak association.
Skull fracture and bruising in head and neck region more supportive of accidental HI.
Which clinical features distinguish inflicted from non-inflicted brain injury? A systematic review.Arch DisChild 2009 94: 860-867
Accidental Vs Inflicted Head Injury (iHI)

Apnea probably reflects hypoxic ischemic injury as a consequence of iHI.
Final diagnosis must take into consideration history and full examination and exclusion of other possible causes like Glutaric aciduria and thrombotic disorders.
However this review gives odds ratio and PPV for the first time.
Accidental Vs Inflicted Head Injury (iHI)

Outcome
Depends on the etiology, depth and duration of impaired consciousness
Prolonged coma after a hypoxic-ischemic insult carries a poor prognosis
Most children surviving infectious encephalopathies have a comparatively better outcomes, often surviving with mild or moderate difficulties only

C P Wong et al , Arch Dis Child 2001;84:193-199
Indian studies
Non traumatic coma.Bansal A1, Singhi SC, Singhi PD, Khandelwal N, Ramesh S.
Indian J Pediatr. 2005 Jun;72(6):467-73.

Prognosis
Poor Prognostic Factors :
Younger age group
Lower GCS score on presentation
Absent brainstem reflexes
Worse motor responses
Hypothermia
Hypotension

Follow - up
Developmental disabilities
Learning and behavior problems
Visual or hearing deficit
Seizure disorder

Take home message
Coma and other states of impaired consciousness represent a medical emergency.
Potential causes are numerous, and the critical window for diagnosis and effective intervention is often short.
The common causes of non-traumatic coma include central nervous system infections, metabolic encephalopathy , intracranial bleed, stroke and status epilepticus.
The basic principles of management include 1) Rapid assessment and stabilization, 2) Focussed clinical evaluation 3) Treatment including general and specific measures.
Commonly associated problems such as raised intracranial pressure and seizures must be recognized and managed to prevent secondary neurologic injury.



















