Approach to Bipolar Spectrum Disorders M NAJIB M ALWI MD(USM), Dip IC(UK), MSc(UK), MRCPsych(UK)...
42
Approach to Bipolar Approach to Bipolar Spectrum Disorders Spectrum Disorders M NAJIB M ALWI M NAJIB M ALWI MD(USM), Dip IC(UK), MSc(UK), MD(USM), Dip IC(UK), MSc(UK), MRCPsych(UK) MRCPsych(UK) Dept of Psychiatry School of Medical Sciences Universiti Sains Malaysia
-
Upload
marcus-hampton -
Category
Documents
-
view
215 -
download
1
Transcript of Approach to Bipolar Spectrum Disorders M NAJIB M ALWI MD(USM), Dip IC(UK), MSc(UK), MRCPsych(UK)...
Approach to Bipolar Approach to Bipolar Spectrum DisordersSpectrum Disorders
M NAJIB M ALWIM NAJIB M ALWIMD(USM), Dip IC(UK), MSc(UK), MRCPsych(UK)MD(USM), Dip IC(UK), MSc(UK), MRCPsych(UK)
Dept of PsychiatrySchool of Medical SciencesUniversiti Sains Malaysia
Mania/Hypomania Episode:DSM-IV Symptoms
• Persistently elevated, expansive, or irritable mood (at least 1 + >3 of below, 4)
• Inflated self-esteem or grandiosity
• Decreased need for sleep
• Talkativeness or pressured speech
• Flight of ideas or “racing” thoughts
• Distractibility
• Increase in goal-directed activity or psychomotor agitation
• Excessive involvement in pleasurable activities with high potential for negative consequences
• DURATION: 1 week / need for hospitalisation (MANIA); 4 days (HYPOMANIA)
1. American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision Washington, DC. American Psychiatric Association, 2000.
2. Ghaemi SN. Bipolar Disorder and Antidepressants: An Ongoing Controversy. Primary Psychiatry. 2001;(8):28-34.

Major Depressive Episode:DSM-IV Symptoms
• Depressed mood* interest/pleasure*• Weight loss/gain or need for sleep• Psychomotor agitation/retardation• Fatigue/loss of energy• Feelings of worthlessness ability to think or concentrate• Suicidal thoughts or thoughts of death
*Either must be present for the diagnosis of a major depressive episode.
American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision. Washington, DC. American Psychiatric Association, 2000.

Bipolar Disorder:Mixed Mania and Rapid Cycling
• Mixed mania–Simultaneous symptoms of depression and
mania–Evident in up to 30-40% of all bipolar I patients–Women >men
• Rapid cycling–4 mood episodes yearly–3 times women >men–Ultrarapid cycling: 4 episodes monthly
1. Evans DL. J Clin Psych 2000;61 (Suppl 13):26-31. 2. American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision. Washington, DC. American Psychiatric Association, 2000.

5
BIPOLAR DISORDERS (DSM-IV)
• Bipolar I Disorder– (manic depressive illness with or without psychosis)
• Bipolar II disorder– (episodes of major depression alternating with episodes
of hypomania which are not severe enough to result in impairment of function)
• Cyclothymic disorder– (brief and attenuated episodes of depression and
hypomania sometimes known as minor cyclic mood disorder)
• Lifetime prevalence: 3% to 4% of general population
6
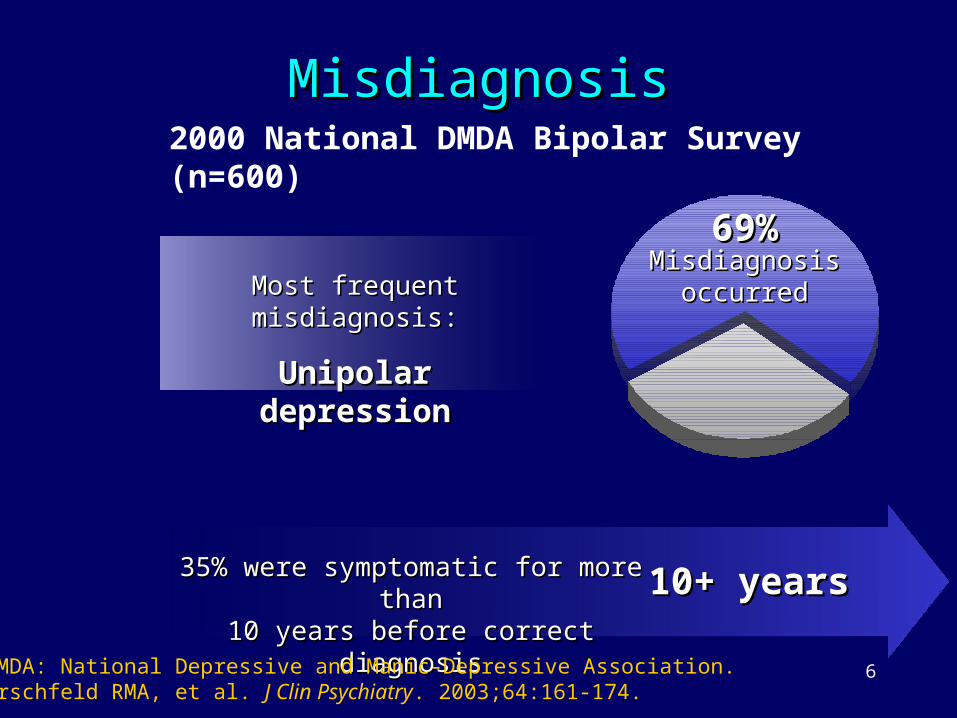
MisdiagnosisMisdiagnosis2000 National DMDA Bipolar Survey(n=600)
35% were symptomatic for more than35% were symptomatic for more than10 years before correct diagnosis10 years before correct diagnosis 10+ years10+ years
Most frequent misdiagnosis:Most frequent misdiagnosis:
Unipolar depressionUnipolar depression
69%69%Misdiagnosis Misdiagnosis
occurredoccurred
NDMDA: National Depressive and Manic-Depressive Association. Hirschfeld RMA, et al. J Clin Psychiatry. 2003;64:161-174.

7

8
Further Diagnostic Difficulty• A much larger group of patients
demonstrate milder and/or atypical forms of episodic mood disturbances– Frequently resistant to standard
antidepressants– Some worsened by antidepressants
• Efforts at clinical subtyping the so-called soft bipolar spectrumsoft bipolar spectrum are ongoing– Currently: DSM-IV Bipolar II Disorder, NOS
(not otherwise specified).
• If included: lifetime prevalence of Bipolar DO - 5% to 8 % of the general population

11
History of Mood Disorders• Kraepelin (1890s):
– “manic-depressive insanity”– Included DSM-IV subtypes, mixed and rapid cycling states,
many of the soft bipolar variations and also episodic depressions
• DSM-I (1960s):– proposed a differentiation between major depression and
manic-depressive illness
• Later DSMs:– unipolar - bipolar dichotomy
• Fieve and Dunner (1970s):– discriminated bipolar I from bipolar II disorder
– a seminal event in the evolution of the soft bipolar spectrum
12
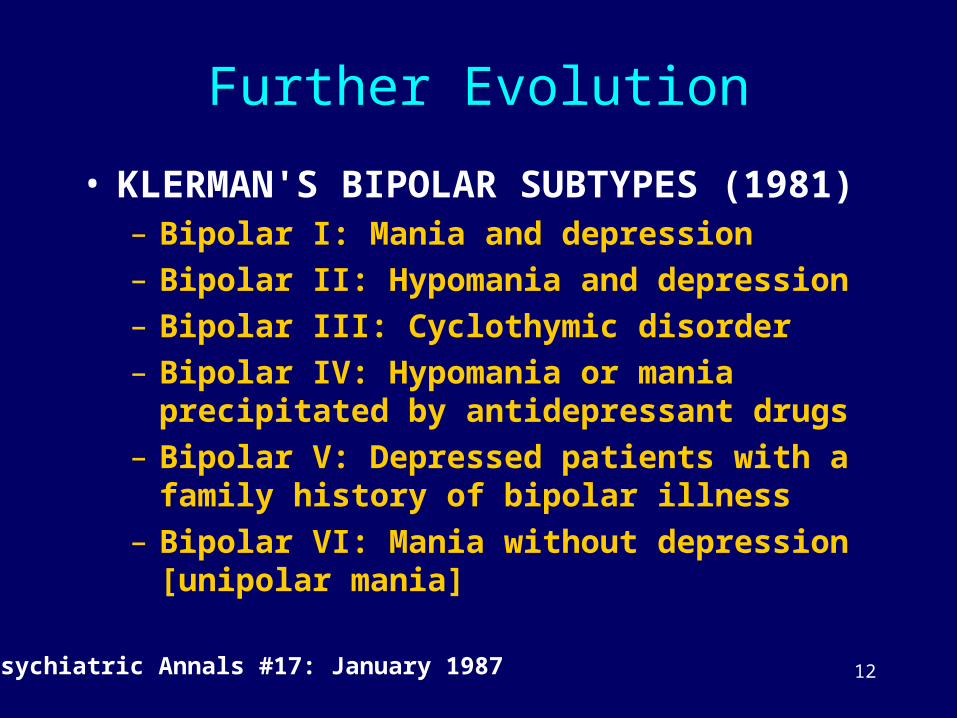
Further Evolution
• KLERMAN'S BIPOLAR SUBTYPES (1981)– Bipolar I: Mania and depression– Bipolar II: Hypomania and depression– Bipolar III: Cyclothymic disorder– Bipolar IV: Hypomania or mania precipitated
by antidepressant drugs– Bipolar V: Depressed patients with a family
history of bipolar illness– Bipolar VI: Mania without depression [unipolar
mania]
Psychiatric Annals #17: January 1987

13
Current Thinking
• Hagop Akiskal: nosologic pendulum is swinging back towards Kraepelinian original unitary concept unitary concept of the bipolar spectrum of mood of the bipolar spectrum of mood disordersdisorders
• He added four more subtypes: according to some unique clinical features.

14
AKISKAL'S SCHEMA OF BIPOLAR SUBTYPES
• Bipolar I: full-blown mania• Bipolar I ½: depression with protracted hypomania• Bipolar II: depression with hypomanic episodes• Bipolar II ½: cyclothymic disorder • Bipolar III: hypomania due to antidepressant drugs• Bipolar III ½: hypomania and/or depression
associated with substance use• Bipolar IV: depression associated with hyperthymic
temperament
Akiskal & Pinto (1999) Psychiatric Clinics of North America 22:3, 517-534

15
AKISKAL'S SCHEMA OF BIPOLAR SUBTYPES
• Bipolar I: full-blown mania• Bipolar I ½: depression with protracted hypomania• Bipolar II: depression with hypomanic episodes• Bipolar II ½: cyclothymic disorder • Bipolar III: hypomania due to antidepressant drugs• Bipolar III ½: hypomania and/or depression associated
with substance use• Bipolar IV: depression associated with hyperthymic
temperament• Proposed subtypes V and VI have not yet been
characterized:– presumably will involve:
• episodic anxiety disorders• seasonal mood states• mood disorders co morbid with various anxiety disorders of an
episodic nature.
Akiskal & Pinto (1999) Psychiatric Clinics of North America 22:3, 517-534
16
Complicated….?That’s not all……..

17
Lieber’s “soft” Bipolar Lieber’s “soft” Bipolar Spectrum DisordersSpectrum Disorders
• Episodic Mood Instability
• Episodic Atypical Depression
• Episodic Dysphoric Hypomania
18
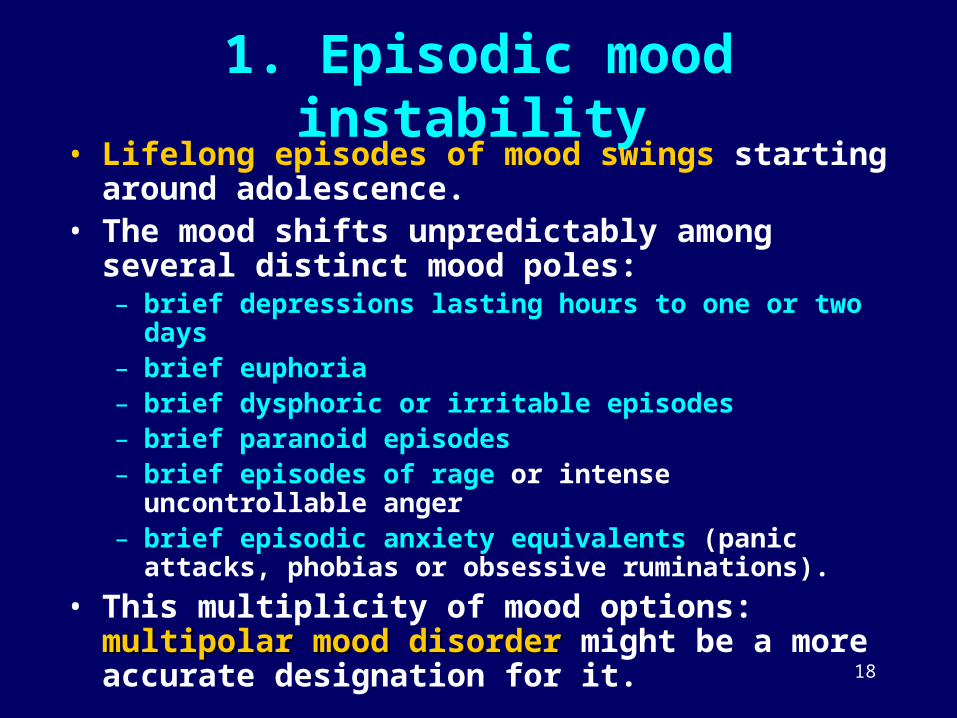
1. Episodic mood instability
• Lifelong episodes of mood swings starting around adolescence.
• The mood shifts unpredictably among several distinct mood poles:– brief depressions lasting hours to one or two days– brief euphoria– brief dysphoric or irritable episodes– brief paranoid episodes– brief episodes of rage or intense uncontrollable anger– brief episodic anxiety equivalents (panic attacks, phobias or
obsessive ruminations).
• This multiplicity of mood options: multipolar mood multipolar mood disorderdisorder might be a more accurate designation for it.
19
2. Episodic atypical depression (EAD)
• shows atypical depressive features:– eating too much, sleeping too much, feeling
worse towards evening and intense tiredness or lethargy.
• mood responsive:– Temporary response to favourable circumstances
(hours to a day or two) before returning to the depressed state.
• co-existing anxiety and its subtypes (phobias, panic attacks, OCD )
20
Subtypes of Episodic Atypical Depression
• (distinguished by special features):– seasonal affective disorder
• winter-onset atypical depressions
– premenstrual dysphoric disorder • a/w irritability, mood swings and dysphoria (irritability)• a week to ten days on either side of the menstrual period
– hysteroid dysphoria• mainly in women with histrionic personality features• episodes precipitated by romantic rejection
– abulic depression• a/w a deficit syndrome (apathy, amotivation, lack of will
power, lack of energy, lack of pleasure in life, emotional blunting )

21
3. Episodic Dysphoric HypomaniaNB: Hypomania:
• Two types: euphoric and dysphoric (irritable)• Two durations: episodic and protracted
• Episodic dysphoric hypomania: – Irritability, emotional discomfiture, impulsiveness, temper
dyscontrol and impaired judgment– Interfere with interpersonal relationships and to limit
productivity at work– Sense of inner speeding combined with restless over activity
and racing thoughts, which can lead to a state of desperation.– Episodes of depression and mood instability almost always depression and mood instability almost always
presentpresent + sometimes brief euphoric episodes.– Triad: irritable episodes alternating with rage episodes and
paranoid episodes is characteristic of dysphoric hypomania.

23
A Proposed Definition of Bipolar Spectrum Disorder
A. At least 1 major depressive episodeB. No spontaneous hypomanic or manic
episodesC. Either:
• 1 of the following plus at least 2 of D;• or 2 of the following, plus 1 item from D:
• Family history of bipolar disorder in 1st degree relatives
• Antidepressant induced mania or hypomania
Ghaemi SN et al (2002) Can J Psychiatry. 47(2):125-134

24
A Proposed Definition of Bipolar Spectrum Disorder
D. If no items from C are present, 6 / 9 of below are needed:
1. Hyperthymic personality (at baseline, non-depressive state)
2. Recurrent major depressive episodes (>3)3. Brief major depressive episodes (ave <3 months)4. Atypical depressive symptoms5. Psychotic major depressive episodes6. Early age of onset of major depressive episodes (<age
25)7. Postpartum depression8. Antidepressant “wear-off” (acute, but not prophylactic
response)9. Lack of response to ≥ 3 antidepressants trial
Ghaemi SN et al (2002) Can J Psychiatry. 47(2):125-134
25
COMORBIDITY
• A high percentage of bipolar mood disorders, perhaps more than 50%, are comorbid with other medical and/or psychiatric conditions.
26
Thyroid disorders
• Hyperthyroidism: resembles hypomania/ mania and it can worsen pre-existing mania/ hypomania
• Hypothyroidism: resembles clinical depression and it can cause pre-existing depression to be unresponsive to antidepressant medications
• Treatment with lithium can produce hypothyroidism
• Subtle or subclinical hypothyroidism is often associated with the development of mixed and rapid cycling bipolar disorders.

27
Substance misuse
• Psychoactive effects on the brain and can worsen the bipolar condition
• Interfere with effective treatment• Can mimic both depression and hypomanic
states• Unmask a pre- existing depression or bipolar
disorder
• Can be secondary to self-medication of bipolar
disorder

28
ADHD• ADHD is now known to often persist into adulthood
and symptoms may overlap with bipolar spectrum disorder
• Overlapping symptoms:– Restlessness– Motor hyperactivity– Easy distractibility– Impulsiveness– Inability to concentrate or focus attention– Temper dyscontrol
• Differentiation: ADHD continuous vs bipolar conditions episodic
• Incidence of their co morbidity is unknown.• Stimulants (eg Ritalin), tend to worsen the symptoms of
bipolar spectrum disorder

29
Borderline Personality Disorder (BPD)
• Stormy and unstable lifestyle, overly dramatic, intense but unstable relationships, and exhibit self-defeating and often self-destructive behaviours
• Recent years: a high percentage of these patients have co morbid bipolar spectrum disorders.
• 75 % of these patients will respond to combination pharmacotherapy using SSRI, a mood stabilizer and an atypical antipsychotic (e.g. olanzapine).
• Once the mood has become stable, they can then benefit from competent psychotherapy to deal with their emotional backwash.
• Better prognosis with this treatment approach?
30
*
*Mood Disorder Questionnaire (MDQ)
Bipolar Spectrum Disorder Scale (BSDS)

31 31
Hirschfield RM (2002) J Clin Psych. 4: 9-11

32
Bipolar Spectrum Disorder Scale (Ghaemi & Pies 2003)
• Read the following paragraph all the way through first, then follow the instructions which appear below it.
• Some individuals noticed that their mood and/or energy levels shift drastically from time to time ______ . These individuals notice that, at times, their moody and/or energy level is very low , and at other times, and very high______. During their " low" phases, these individuals often feel a lack of energy, a need to stay in bed or get extra sleep, and little or no motivation to do things they need to do______ . They often put on weight during these periods______ . During their low phases, these individuals often feel "blue," sad all the time, or depressed______ . Sometimes, during the low phases, they feel helpless or even suicidal _____ . Their ability to function at work or socially is impaired ______ . Typically, the low phases last for a few weeks, but sometimes they last only a few days ______ . Individuals with this type of pattern may experience a period of "normal" mood in between mood swings, during which their mood and energy level feels "right" and their ability to function is not disturbed ______ . They may then noticed they marked shift or "switch" in the way they feel ______ . Their energy increases above what is normal for them, and they often get many things done they would not ordinarily be able to do ______ . Sometimes during those "high" periods, these individuals feel as if they had too much energy or feel "hyper" ______ . Some individuals, during these high periods, may feel irritable, "on edge," or aggressive ______. Some individuals, during the high periods, take on too many activities at once ______. During the high periods, some individuals may spend money in ways that cause them trouble______ . They may be more talkative, outgoing or sexual during these periods ______ . Sometimes, their behavior during the high periods seems strange or annoying to others ______ . Sometimes, these individuals get into difficulty with co-workers or police during these high periods ______ . Sometimes, they increase their alcohol or nonprescription drug use during the high periods ______ .

33
Scoring the BSDS
• Add total of check marks from the first 19 sentences. To that total, add the number in parentheses below for the line you selected: – this story fits me very well, or almost perfectly (6)– this story fits me fairly well (4)– this story fits me to some degree, but not in most respects (2)– this story doesn't really describe me at all (0)
• The maximum is 19 plus 6, for 25 points.
• Interpretation: 19 or higher = bipolar spectrum disorder highly likely 11-18 = moderate probability of bipolar spectrum disorder. 6-10 = low probability of bipolar spectrum disorder <6 = bipolar spectrum disorder very unlikely

34
Bipolar Disorder Treatment Strategies Revisited
36
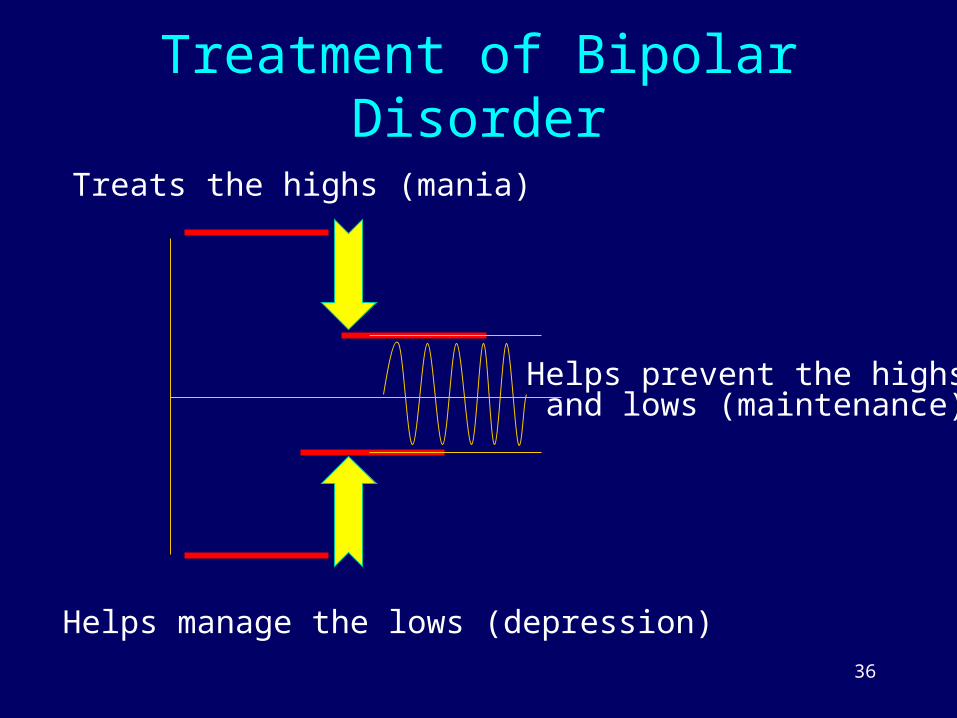
Treatment of Bipolar Disorder
Treats the highs (mania)
Helps manage the lows (depression)
Helps prevent the highs and lows (maintenance)
37
Long-term Treatment Goals
• Facilitating compliance– Tolerability of adverse effects of medications
– Denial of illness
• Recognizing ‘signal events’ that indicate1. Patient has returned to baseline functioning
2. Patient is at a risk for relapse
• Family Involvement– To pick up early warning signs of patient relapsing
– To assess the family’s expectations
38
World Federation of Societies of Biological Psychiatry (WFSBP) 2003 Guidelines
• Acute bipolar mania, mild to moderate
• Acute bipolar mania, severe
• Bipolar depression

43
Time to Recurrence Into Mania or Depression(Days)
0 100 200 300 400 5000
20
40
60
80
100OLZ plus Li or VPA, (n=30)Li or VPA, (n=38)
p=.023
Time to recurrence into either pole following symptomatic remission of mania (YMRS 12) and depression (HAMD-21 8), was significantly longer for the olanzapine cotherapy group compared to the monotherapy group (estimated 25th percentile 124 vs 15 days, respectively).Tohen M, et al. Presented at: 155th APA Annual Meeting; May 18-23, 2002; Philadelphia, Pa.
Efficacy of Olanzapine in Combination Efficacy of Olanzapine in Combination with Lithium or Valproatewith Lithium or Valproate
% P
roba
bilit
y of
Rem
aini
ngin
Rem
issi
on

44
Treatment Strategies for Bipolar Spectrum Disorder Lieber (2003)?
• Present with predominantly anxiety or depression symptoms:– Start initially on an SSRI (e.g. Fluoxetine)– If symptoms of hypomania occur during the
course of treatment, add a mood stabilizer (e.g. Sodium Valproate)
– If the patient fails to respond to the SSRI within four weeks or is unable to tolerate it due to side effects, I will switch to a dual neurotransmitter antidepressant (Effexor, Welbutrin, Remeron, Serzone).
– Once the patient is mood stable and without symptoms, monitor at one to three-month intervals. Advise to continue the same dose to prevent recurrence

45
Treatment Strategies for Bipolar Spectrum Disorder Lieber (2003)?
• Present with either euphoric or dysphoric hypomania/ uncontrollable rage/violent outbursts:– Start on a mood stabilizer.– If necessary, an antidepressant drug can be
added later after the mood has been stabilized.
• Patients with mixed or rapid cycling states:– Usually respond to combination therapy with
mood stabilizers and antidepressants.

46
Unanswered Questions
• Does bipolar spectrum disorder routinely require mood stabilisers?
• How safe are antidepressants in bipolar spectrum?
• What is the optimal duration of treatment?

47
Conclusion
• Bipolar Spectrum Disorders are only recently recognized
• May explain difficulties in treating mood disorder patients
• Treatment strategies need to be optimized depending on presenting problems and may need to be revised from time to time

48
Thank You