Applying knowledge to generate action: A community-based knowledge translation framework
7
Original Research Applying Knowledge to Generate Action: A Community-Based Knowledge Translation Framework BARBARA CAMPBELL, RN, PHD Introduction: Practical strategies are needed to translate research knowledge between researchers and users into action. For effective translation to occur, researchers and users should partner during the research process, recognizing the impact that knowledge, when translated into practice, will have on those most affected by that research. Method: Participatory action research (PAR) was used to generate a rural community’s knowledge of their chil- dren’s health. The Ottawa Model of Research Use (OMRU), a knowledge translation framework, was used to guide the translation of that generative knowledge into action, and the more current knowledge-to-action (KTA) concep- tual framework provided the rationale for the graphical depiction of engagement of a rural community in knowledge translation. Results: The definitions, perspectives, best practices, and existing frameworks of knowledge translation are out- lined. The foundational underpinnings and elements of PAR, the OMRU, and KTA are linked to form a conceptual framework for knowledge translation in a rural community context. Select strategies noted in OMRU to translate existing knowledge informed aspects of PAR to generate an action. Discussion: Diverse yet complementary approaches could be used by health professionals to advance the theory, method, and research of knowledge translation and exchange, regardless of context. Knowledge needs to be relevant, appropriate, applicable, timely, and reasonable to influence change. Key Words: knowledge translation, Ottawa model of research use, participatory action research Introduction For effective translation to occur, researchers must produce knowledge for translation by decision makers who can see the impact on users. 1 There is minimal identification of cur- rent knowledge-exchange processes, including the synthesis and evaluation of such information. 2 Current literature ac- knowledges that without firm efforts to disseminate and adopt innovative methods to translate research, information will not be actively used by intended users. 3 Graham et al 4 states the main reason why evidence is not put into action is the lack of clarity in the knowledge-to-action field, beginning with inconsistent definitions of knowledge translation and the related terminology. When designing a framework for knowledge translation ~ KT!, Jacobson et al 5 found that prac- tical strategies for disseminating knowledge to the users is lacking, whereas Graham et al 4 suggest research findings are not easily used by health professionals in the treatment of patients. This research story emerged from a concern about chil- dren’s health in a rural community on the east coast of Can- ada, juxtaposed with an interest in how knowledge about health is translated into action. Participatory action research ~ PAR! was chosen as the methodology to facilitate the co- creation of local knowledge concerning children’s health and then the sharing of existing research knowledge on chil- dren’s health, enabling the community of Souris to imagine a healthier future. The present study engaged a diverse group of users of research, rural community members in eastern Canada, with researchers in a participatory research project, to understand issues surrounding the communities’ chil- dren’s health. Participatory action research ~ PAR! is an ap- proach to engage individuals to apply their emergent knowledge in generating an action toward social change. Disclosures: The author reports none. Dr. Campbell: Director of the Webster Centre, Associate Professor, School of Nursing, University of Prince Edward Island. Correspondence: Barbara Campbell, Webster Centre for Teaching and Learn- ing, University of Prince Edward Island, 550 University Avenue, Charlotte- town, Prince Edward Island, C1A 4P3, Canada; e-mail: [email protected]. © 2010 The Alliance for Continuing Medical Education, the Society for Academic Continuing Medical Education, and the Council on CME, Association for Hospital Medical Education. • Published online in Wiley InterScience ~www.interscience.wiley.com!. DOI: 10.10020chp.20058 JOURNAL OF CONTINUING EDUCATION IN THE HEALTH PROFESSIONS, 30(1):65–71, 2010
-
Upload
barbara-campbell -
Category
Documents
-
view
214 -
download
0
Transcript of Applying knowledge to generate action: A community-based knowledge translation framework

Original Research
Applying Knowledge to Generate Action:A Community-Based KnowledgeTranslation Framework
BARBARA CAMPBELL, RN, PHD
Introduction: Practical strategies are needed to translate research knowledge between researchers and usersinto action. For effective translation to occur, researchers and users should partner during the research process,recognizing the impact that knowledge, when translated into practice, will have on those most affected by thatresearch.
Method: Participatory action research (PAR) was used to generate a rural community’s knowledge of their chil-dren’s health. The Ottawa Model of Research Use (OMRU), a knowledge translation framework, was used to guidethe translation of that generative knowledge into action, and the more current knowledge-to-action (KTA) concep-tual framework provided the rationale for the graphical depiction of engagement of a rural community in knowledgetranslation.
Results: The definitions, perspectives, best practices, and existing frameworks of knowledge translation are out-lined. The foundational underpinnings and elements of PAR, the OMRU, and KTA are linked to form a conceptualframework for knowledge translation in a rural community context. Select strategies noted in OMRU to translateexisting knowledge informed aspects of PAR to generate an action.
Discussion: Diverse yet complementary approaches could be used by health professionals to advance the theory,method, and research of knowledge translation and exchange, regardless of context. Knowledge needs to berelevant, appropriate, applicable, timely, and reasonable to influence change.
Key Words: knowledge translation, Ottawa model of research use, participatory action research
Introduction
For effective translation to occur, researchers must produceknowledge for translation by decision makers who can seethe impact on users.1 There is minimal identification of cur-rent knowledge-exchange processes, including the synthesisand evaluation of such information.2 Current literature ac-knowledges that without firm efforts to disseminate and adoptinnovative methods to translate research, information willnot be actively used by intended users.3 Graham et al4 statesthe main reason why evidence is not put into action is the
lack of clarity in the knowledge-to-action field, beginningwith inconsistent definitions of knowledge translation andthe related terminology. When designing a framework forknowledge translation ~KT!, Jacobson et al5 found that prac-tical strategies for disseminating knowledge to the users islacking, whereas Graham et al4 suggest research findingsare not easily used by health professionals in the treatmentof patients.
This research story emerged from a concern about chil-dren’s health in a rural community on the east coast of Can-ada, juxtaposed with an interest in how knowledge abouthealth is translated into action. Participatory action research~PAR! was chosen as the methodology to facilitate the co-creation of local knowledge concerning children’s health andthen the sharing of existing research knowledge on chil-dren’s health, enabling the community of Souris to imaginea healthier future. The present study engaged a diverse groupof users of research, rural community members in easternCanada, with researchers in a participatory research project,to understand issues surrounding the communities’ chil-dren’s health. Participatory action research ~PAR! is an ap-proach to engage individuals to apply their emergentknowledge in generating an action toward social change.
Disclosures: The author reports none.
Dr. Campbell: Director of the Webster Centre, Associate Professor, Schoolof Nursing, University of Prince Edward Island.
Correspondence: Barbara Campbell, Webster Centre for Teaching and Learn-ing, University of Prince Edward Island, 550 University Avenue, Charlotte-town, Prince Edward Island, C1A 4P3, Canada; e-mail: [email protected].
© 2010 The Alliance for Continuing Medical Education, the Society forAcademic Continuing Medical Education, and the Council on CME,Association for Hospital Medical Education. • Published online in WileyInterScience ~www.interscience.wiley.com!. DOI: 10.10020chp.20058
JOURNAL OF CONTINUING EDUCATION IN THE HEALTH PROFESSIONS, 30(1):65–71, 2010

The Ottawa model of research use ~OMRU! was originallyselected as an appropriate knowledge translation method toguide the utilization, implementation, and translation of thecommunities’ research into an action specific to the needs ofthe community members. Further development of the OMRUby the original authors resulted in a knowledge-to-action~KTA! conceptual framework that integrates both the cre-ation and application of knowledge to influence change inhealth practice settings.4 The more explicit framework, KTA,added value to the “applying knowledge to generate action”framework that emerged during this original community re-search. The value added is in the transparency and fluidityof the translation process between knowledge creation andaction that reflects the intent of the framework that emergedfrom the original study, where PAR helped create the com-munity knowledge and OMRU guided the facilitation ofcommunity action from their created knowledge. BecausePAR is grounded in a generative and participatory philoso-phy toward social change in a community and OMRU out-lines a prescriptive and systematic implementation of themedical model in a practice setting, and KTA has a broaderfocus with all stakeholders, some elements from each didsynergistically inform the other approach. As knowledge cre-ation and actions emerge through the various stages in theKTA, the authors suggest more useful knowledge for mul-tiple stakeholders will result, using local and external knowl-edge, similar to the work that emerged from this originalstudy.4 The authors of the KTA framework support a similarknowledge translation process known in PAR as generative,by stating “the action phases may occur sequentially or si-multaneously and the knowledge phases may influence theaction phases” ~p. 18!.4
Background
Although the initial intent of the study was to understandcommunity health issues through the emergent process ofPAR and to determine whether PAR could inform or beinformed by OMRU during the knowledge translation pro-cess, it became obvious that PAR and OMRU might bephilosophically incompatible. The OMRU is a comprehen-sive interdisciplinary model used to guide the utilizationand implementation of research findings in the context ofhealth care practice,6 but it has not been applied in a com-munity setting, where the users of the information are lo-cal people. Therefore, the focus of the study shifted to anexploration of points of intersection between PAR andOMRU to determine if both approaches collectively couldsymbiotically result in the creation and subsequent action,on the emergent knowledge, to improve rural communityhealth. In order to explore potential points of intersectionwithin PAR and OMRU, it is important to have an under-standing of the knowledge-translation literature retrievedfrom current scholarly sources. An in-depth document re-trieval search from 1999–2009 revealed numerous elec-tronic sources from CINAHL, Medline, ERIC, and PubMed
databases. Using the key word knowledge translation un-covered 1398 citations.
When the investigator began this study in 2003, the wordsknowledge translation produced about 5000 hits in the searchengine known as Google; the same phrase in 2009 results inover 18 400 000 hits. Although not a statistically sound ref-erence point, it may suggest new technologies for Google ora growing interest in knowledge translation. The extant lit-erature refers to knowledge translation between researchersand decision makers, not researchers and users, such as thepublic, patients, or community, a fundamental gap notedthroughout the literature review that framed the study.
The present article outlines the theoretical background,characteristics, and elements of knowledge translation, PAR,the OMRU, and the KTA framework, followed by a gen-eral description of the original community-based research.The final section evaluates the commonalities and differ-ences between these philosophically disparate paradigmsthat framed this community-based research on children’shealth, concluding with a graphical depiction linking keyelements of PAR and OMRU in a conceptual frameworkof knowledge translation.
Defining Knowledge Translation
Knowledge translation also is referred to as knowledge uti-lization, research utilization, research or knowledge trans-fer, research use, or knowledge exchange.7–16 Regardless ofthe terminology used, most authors agree that an effectiveexchange of knowledge involves interaction between deci-sion makers and researchers, and results in mutual learningfor all participants through the processes of planning, pro-ducing, disseminating, and applying existing or new re-search.4,17 This definition is also the shared ethos of fundinginstitutions such as Canadian Institutes for Health Research~CIHR!18 and Canadian Health Services Research Founda-tion ~CHSRF!.19
The term knowledge exchange ~formerly knowledge trans-fer! is recognized as an interactive approach to knowledgetranslation and is defined by CHSRF20 as collaborative prob-lem solving between researchers and decision makers thathappens through linkage and exchange. It brings togetherthe instrumental knowledge of the knowledge user and hisor her experiential, tacit knowledge of the context in whichthat instrumental knowledge will be used. For the purposesof this article, the term knowledge translation and its sub-sequent definition by CIHR20 will be used:
Knowledge translation is a dynamic and iterative processthat includes synthesis, dissemination, exchange and ethi-cally sound application of knowledge to improve the healthof Canadians, provide more effective health services andproducts and strengthen the health care system. ~p. 1!
Knowledge translation is a multifaceted, active processinvolving numerous strategies to improve outcomes for mul-
Campbell
66 JOURNAL OF CONTINUING EDUCATION IN THE HEALTH PROFESSIONS—30(1), 2010DOI: 10.1002/chp

tiple users from the time of creation of the knowledge to itsapplication and use.10,19,21 Graham et al4 use the funnel di-agram to represent knowledge to action as an extensive andongoing process in which a problem is identified, researchis disseminated to the audience, and then the researcher de-termines how the knowledge will be made applicable. Localcontext barriers are identified and assistance is undertakento overcome such barriers. Once an action is adopted, thetranslation is monitored and outcomes are evaluated; thenthe researcher and the audience work together to ensure sus-tainability of the new behavioral change. When this cyclehas been completed the process begins again, bringing the 2worlds of research and practice together.
Knowledge Translation’s Theoretical andConceptual Frameworks
The review begins with a brief account of the germinalwork by Everett Rogers, Michael Huberman, Bradley Cous-ins, and Ken Leithwood. Rogers’s 22 Diffusion of Innova-tions theory addresses how new ideas, products, and socialpractices spread within a society. Secondly, in the 1980s,Michael Huberman, in developing the Social IntegrationDissemination model,23–25 outlined several factors that in-fluence the dissemination of information. Thirdly, the Cous-ins and Leithwood26 knowledge utilization conceptualframework recognizes similar elements of credibility, va-lidity, quality, timeliness, and content relevant to the need,all necessary characteristics for knowledge to be adoptedor disseminated. Diffusion theory provides the basis forthe development of many KT frameworks, in particu-lar, the OMRU.
Theoretical Foundation: Diffusion ofInnovation Theory
Diffusion theory, originating in agriculture, has been ap-plied to translate information in a wide variety of disci-plines, such as education, public health, communication,marketing, geography, general sociology, and economics.27
In Rogers’s theory, an innovation is adopted over time byvarious adopters through numerous stages of a social sys-tem. The adoption and subsequent use of new knowledge orinnovation is dependent on the perceived characteristics ofthe innovation and the unique categories that adopters oc-cupy when beginning to use the innovation.25 According toRogers,22 diffusion is “the process by which an innovationis communicated through certain channels over time amongthe members of a social system” ~p. 5!. Diffusion is a spe-cial type of communication concerned with the spread ofmessages that are perceived by the users as new ideas. Theprocess of diffusion is considered to revolve around 4 keyelements: an idea or an innovation, channels of communi-cation to spread the knowledge of this innovation, the timeduring which the diffusion takes place, and a social systemof potential adopters in which this occurs.25 Rogers defines
an innovation as “an idea, practice, or object that is per-ceived as new by an individual or other unit of adoption” 25
~p. 11!. According to Rogers,25 the characteristics of an in-novation that determine the rate of adoption are relative ad-vantage, compatibility, complexity, amenability to trial, andobservability. Another core reason why certain innovationsspread more quickly than others is the perception of themembers of a social system, which is influenced by the char-acteristics and categories of the adopters as they determinethe importance or use of the innovation.
Characteristics of Adopters
The speed of adoption is also dependent on the 5 categoriesidentified by Rogers,22 which classify individuals in a socialsystem. Innovators, according to Rogers, represent 2.5% ofindividuals, followed by early adopters, who account for13.5% of a population. The middle majority represent 34%and are more deliberate in the undertaking, and 34% areknown as the late majority or the skeptics. The final groupto adopt an innovation are referred to as the laggards, com-prising 16% of a population and exhibiting a traditional mind-set.22 The power of influence may lead some adopters of aninnovation in the early stages of the diffusion process tocreate pressure on others to adopt this innovation in the laterstages. This explains why some innovations are widely ac-cepted before their efficacy is known, whereas other moreeffective innovations are underutilized.
Knowledge Translation: Conceptual Framework
Dobbins and colleagues,9 in developing a framework to il-lustrate the adoption process, base their work on Rogers’sdiffusion of innovations theory utilizing knowledge, persua-sion, decision, implementation, and confirmation stages aspart of a systematic approach to research utilization for pol-icy and practice. They surmise that diffusion theory mayhave numerous uses for health research, providing usefulinsights and understandings of the research utilization pro-cess. Jacobson et al5 highlight the key areas for researchersto note in their framework for knowledge translation as anawareness of the user group, the issue being translated, theresearch findings, the partnership between user and re-searcher, and the strategy to inform the user group of thefindings. They suggest that researchers should move out oftheir familiar context and into the context of the user groupto gain insights for effective knowledge translation. Con-curring with them, Best et al,28 in their integrative model,propose that a participatory collaborative approach to healthpromotion research is more effective in closing the theory0practice gap than the traditional expert-driven epidemiolog-ical study. The above authors investigated strategies thatencourage dissemination and adoption, methods by whichresearch is communicated to users, and the receptivity ofusers to research in their professional lives. More currenttheoretical and conceptual models and frameworks reflect
Applying Knowledge to Generate Action
JOURNAL OF CONTINUING EDUCATION IN THE HEALTH PROFESSIONS—30(1), 2010 67DOI: 10.1002/chp

alternate determining factors, multiple elements, and strat-egies to translate research into effective use.4,17 One shouldremain cautious when attempting to translate findings withusers, taking into account that, as these authors have noted,there remains no 1 panacea of method or strategy to effecttranslation. It remains certain that, theoretically and ideo-logically, the principles of collaboration, reflectivity, par-ticipation, and transformation with an ongoing user focusthat acts on created knowledge do support a participatory-based approach to research.
Participatory Action Research: Methods and Results
The purpose of PAR is more than the interpretation of socialreality; it is to facilitate the creation of knowledge during aprocess that may result in strategies to transform or changethat reality. PAR, therefore, has the potential to promote healthnot only by identifying factors that interfere with health andcause illness, but also by empowering people in the com-munity to interpret their emergent knowledge into actions toimprove their health. Because PAR seeks to create emergentknowledge, to address the practical concerns of people, itwas an appropriate methodology to conduct research withcommunity members in this rural setting.
The present study involves child health in a rural com-munity on the east coast of Canada, juxtaposed with aninterest in how knowledge about health is translated intoaction. Participatory action research was chosen as the meth-odology to facilitate the cocreation of local knowledge con-cerning children’s health coupled with existing researchknowledge on child health, enabling the community toimagine a healthier future. Data collected during a 5-phasemethod of community engagement were collated and an-alyzed from these multiple sources: ~a! historical docu-mentation of newspaper headlines retrieved during thatperiod in time; ~b! photographs of the community infra-structure, signage, and landscape; ~c! field notes; ~d! min-utes from meetings with town administration and theadvocacy group; and ~e! focus-group interviews.
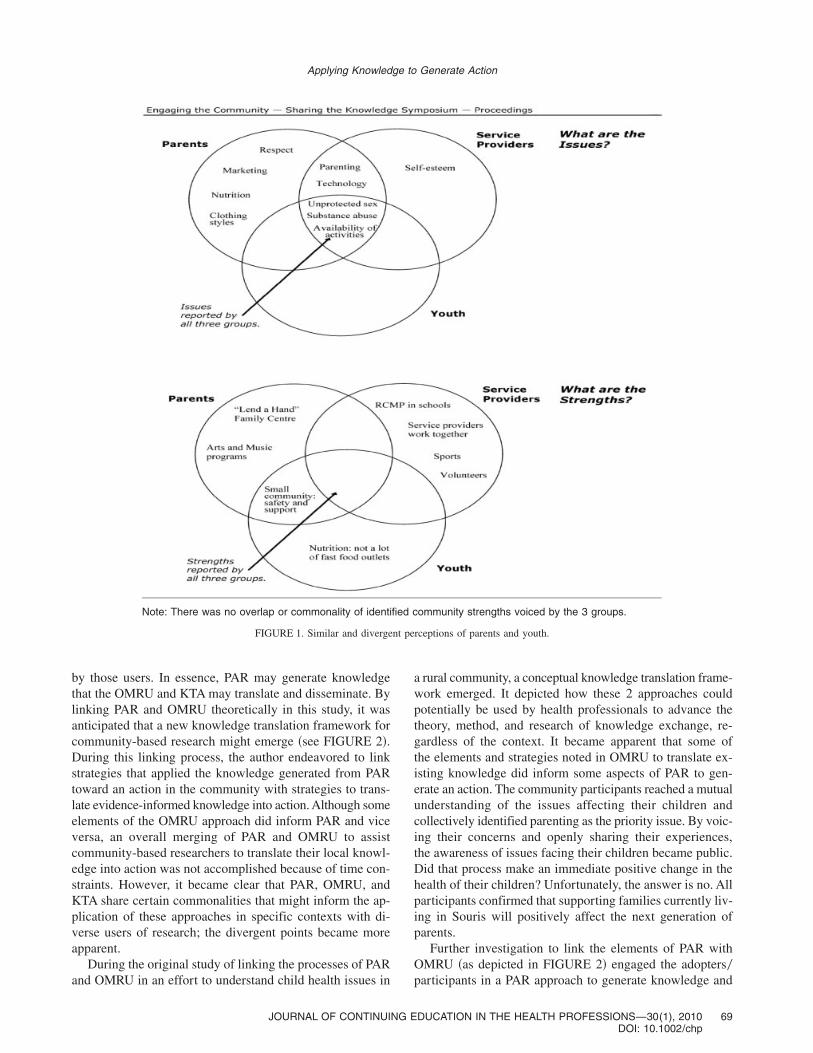
Results: Health Issues Concerning Youth
The issues identified by all participants as affecting the healthof the youth in their community included substance abuse,the lack of available activities, unhealthy sexual behavior,lack of resources to help parents, negative influence of tech-nology, and low self-esteem. To assist in the exchange ofwhat the research partners in the community identified asissues, strengths, and challenges for youth in the commu-nity, a Venn diagram was used to depict similar and diver-gent perceptions voiced by the 3 focus groups graphically.~See FIGURE 1.! The Venn diagram, consisting of 2 or moreoverlapping circles, is a useful tool to examine similaritiesand differences between concepts in a visual representationthat shows the shared characteristics in the overlappingcircles.
By reviewing data from the 3 stakeholder groups ~youth,parents, and service providers!, distinctive commonalitiesarose. All groups identified a lack of activities, substanceabuse, and unprotected sexual practice as common issues af-fecting the health of youth in their community. In addition,parents and service providers suggested that parenting issuesand the misuse of technology also had an influence on youth.
Ottawa Model of Research Use and theKnowledge-to-Action Framework
The OMRU and the KTA aim to share and implement re-search knowledge with appropriate users within a particularcontext. They both view research as a dynamic process ofdecisions and actions directed toward the transfer of specificknowledge into practice.4,29 The authors note that elementsinclude knowledge creation and application through a prac-tice environment, with potential adopters, using an evidence-based innovation to transfer the evidence into practice toaffect the outcome during the process. Both the OMRU andthe KTA are classified as a process of knowledge translationphases applied through a systematic series of activities wherethe dynamic interaction between these elements.30 In theirseminal work, Logan and Graham29 describe OMRU as aninteractive model that takes place as different users of theinformation relate to the various elements. Specifically, ithas been directed toward the transfer of research-based knowl-edge into practice.31 OMRU is grounded in literature relatedto research utilization, the diffusion of innovations, physi-cian behavior change, and the development and implemen-tation of practice guidelines.31 The model, according to Loganand Graham,29 is a systematic assessment that encouragesresearchers and users to monitor and evaluate each elementprior to, during, and following any research transfer efforts.The KTA is a more “fluid and permeable” process of knowl-edge exchange with different stakeholders during differentphases at different points of the research process4 ~p. 18!.
Points of Intersection Linking Participatory ActionResearch, Ottawa Model of Research Use, andKnowledge to Action
Participatory action research is a methodology that gener-ates knowledge created and identified by the users as rele-vant to them, and the OMRU facilitates the translation ofknowledge that may be generated apart from, or in concertwith, the potential users of the research. The KTA frame-work highlights the complete knowledge-to-action process,including a range of stakeholders involved in translating re-search into practice and attempting to simplify the complexprocess of knowledge exchange. The intent of PAR is tococreate knowledge collaboratively and act on that knowl-edge to address an issue raised by the creators that mayresult in social change at the local level. The intent of OMRU0KTA is to implement evidenced informed knowledge andthen evaluate how that knowledge is adapted and adopted
Campbell
68 JOURNAL OF CONTINUING EDUCATION IN THE HEALTH PROFESSIONS—30(1), 2010DOI: 10.1002/chp
by those users. In essence, PAR may generate knowledgethat the OMRU and KTA may translate and disseminate. Bylinking PAR and OMRU theoretically in this study, it wasanticipated that a new knowledge translation framework forcommunity-based research might emerge ~see FIGURE 2!.During this linking process, the author endeavored to linkstrategies that applied the knowledge generated from PARtoward an action in the community with strategies to trans-late evidence-informed knowledge into action. Although someelements of the OMRU approach did inform PAR and viceversa, an overall merging of PAR and OMRU to assistcommunity-based researchers to translate their local knowl-edge into action was not accomplished because of time con-straints. However, it became clear that PAR, OMRU, andKTA share certain commonalities that might inform the ap-plication of these approaches in specific contexts with di-verse users of research; the divergent points became moreapparent.
During the original study of linking the processes of PARand OMRU in an effort to understand child health issues in
a rural community, a conceptual knowledge translation frame-work emerged. It depicted how these 2 approaches couldpotentially be used by health professionals to advance thetheory, method, and research of knowledge exchange, re-gardless of the context. It became apparent that some ofthe elements and strategies noted in OMRU to translate ex-isting knowledge did inform some aspects of PAR to gen-erate an action. The community participants reached a mutualunderstanding of the issues affecting their children andcollectively identified parenting as the priority issue. By voic-ing their concerns and openly sharing their experiences,the awareness of issues facing their children became public.Did that process make an immediate positive change in thehealth of their children? Unfortunately, the answer is no. Allparticipants confirmed that supporting families currently liv-ing in Souris will positively affect the next generation ofparents.
Further investigation to link the elements of PAR withOMRU ~as depicted in FIGURE 2! engaged the adopters0participants in a PAR approach to generate knowledge and
Note: There was no overlap or commonality of identified community strengths voiced by the 3 groups.
FIGURE 1. Similar and divergent perceptions of parents and youth.
Applying Knowledge to Generate Action
JOURNAL OF CONTINUING EDUCATION IN THE HEALTH PROFESSIONS—30(1), 2010 69DOI: 10.1002/chp

then used the OMRU to further understand how that knowl-edge when combined with research knowledge gets used.This original framework between PAR and OMRU was fur-ther explored using the more current KTA framework tosupport the notion that knowledge needs to be relevant, ap-propriate, applicable, timely, and reasonable to be useful tothose affected by the knowledge and to have an impact onchange. The practicality of PAR and the usefulness of OMRUand KTA were evident and they do at some level informeach other, making the distinctive characteristics of eachjust as salient as the collective qualities they convey. It iswith this acknowledgment that further application of thisemergent conceptual framework in knowledge translationmight be useful for rural or urban health professionals, intheir divergent settings, to assist them in translating researchwith other health care providers, policy makers, or userssuch as patients0clients. However, further research into andimplementation of both these approaches in a similar con-text would contribute to the emergent literature on knowl-edge translation theory and methods. For effective translationto occur, it is obvious from this study that the users of re-search must be involved at some level in its creation, im-plementation, and0or evaluation of the research, where allparticipants may contribute toward the most appropriate strat-
egy of translation, which is contextual and meets the spe-cific needs of either the community and0or its users.
Acknowledgments
The author acknowledges the support for the developmentof this framework from the University of Prince EdwardIsland’s knowledge translation team: Drs. Vianne Timmons,Kim Critchley, Jennifer Taylor, Sandy McAuley, and FionaWalton, her doctoral committee, Dr. Linda Ogilvie from theUniversity of Alberta, Dr. Dana Edge from Queen’s Uni-versity, Dr. Lorraine Watson from University of Calgary,and Rosalyn Adamowycz for her editorial assistance. Con-duct of the presently reported study was supported by Ca-nadian Institutes of Health Research ~CIHR!.
References
1. Choi BCK, McQueen DV, Rootman I. Bridging the gap between sci-entists and decision makers. J Epidemiol Commun Health. 2003;57~12!:918.
2. Birdsell JM, Atkinson-Grosjean J, Landry R. Knowledge translation intwo new programs: Achieving the Pasteur effect. http:00www.cihr-irsc.gc.ca0e07502.html. Accessed June 25, 2004.
3. Grunfeld E, Zitzelsberger L, Hayter C, Berman N, Cameron R, EvansWK, Stern H. The role of knowledge translation for cancer control inCanada. Chronic Dis Can. 2004;25~2!:1–5.
4. Graham ID, Logan J, Harrison MB, Straus SE, Tetroe J, Caswell W,Robinson N. Lost in knowledge translation: Time for a map? J ContinEduc Health Prof. 2006;26~1!:13–24.
5. Jacobson N, Butterill D, Goering P. Development of a framework forknowledge translation: Understanding user context. J Health Serv ResPolicy. 2003;8~2!:94–99.
6. Harrison M, Logan J, Joseph L, Graham ID. Quality improvements,research and evidence-based practice: 5 years’ experience with pres-sure ulcers. Evid Based Nurs. 1998;1~4!:108–110.
7. Bender S, Fish A. The transfer of knowledge and the retention of ex-pertise: The continuing need for global assignments. J Knowl Manag.2008;4~2!:125–137.
FIGURE 2. A community-based knowledge translation conceptualframework.
Lessons for Practice
• Translating research knowledge into actioneffectively requires all participants to be in-volved throughout the process.
• The “applying knowledge to generate ac-tion” framework emerged when rural com-munity members and researchers workedcollaboratively around children’s healthissues.
• To result in an action, the knowledge beingtranslated needs to be relevant, appropri-ate, applicable, timely, and reasonable tothe needs of the intended users.
Campbell
70 JOURNAL OF CONTINUING EDUCATION IN THE HEALTH PROFESSIONS—30(1), 2010DOI: 10.1002/chp

8. Berwick DM. Disseminating innovations in health care. J Am MedAssoc. 2003;289~15!:1969–1975.
9. Dobbins M, Ciliska D, Cockerill R, Barnsley J, DiCenso A. A frame-work for the dissemination and utilization of research for health-carepolicy and practice. Online J. Knowl Synth Nurs. 2002;9~7!:1–12.
10. Farnsworth P, Hagens D. Developing a Process for Translating andIncorporating Traditional and Ecological Knowledge (TEK) Into theScenario Planning Process. Enhanced Aboriginal Initiative of McGre-gor Model Forest Web site. http:00www.mcgregor.bc.ca0publications0TEKReport.pdf. Accessed May 7, 2004.
11. Haig-Brown C. Continuing collaborative knowledge production: Know-ing when, where, how and why. J Intercult Stud. 2001;22~1!:19–32.
12. Landry R, Amara N, Lamari M. Climbing the ladder of research uti-lization: Evidence from social science research. Sci Commun. 2001;22~4!:396–422.
13. Lomas J. Connecting research and policy. ISUMA: Can J Policy Res.2000;1~1!:140–144.
14. Rynes SL, Bartunek JM, Daft RL. Across the great divide: Knowledgecreation and transfer between practitioners and academics. Acad ManagJ. 2001;44~2!:340–355.
15. Stetler CB. Research utilization: Defining the concept. IMAGE: J NursSchol. 1985;17~2!:40–44.
16. Volet S. Learning across cultures: Appropriateness of knowledge trans-fer. Int J Educ Res. 1999;31~7!:625–643.
17. Straus S, Graham ID, Taylor M, Lockyer J. Development of a men-torship strategy: A knowledge translation case study. J Contin EducHealth Prof. 2008;28~3!:117–122.
18. Canadian Institutes for Health Research. Knowledge Translation Strat-egy 2004–2009: Innovation in Action. http:00www.cihr-irsc.gc.cae08505.html. Accessed January 13, 2004,
19. Canadian Health Services Research Foundation. Glossary of Knowl-edge Exchange Terms as Used by the Foundation. http:00www.chsrf.ca0keys0glossary_e.php. Accessed November 29, 2005.
20. Canadian Institutes for Health Research. About Knowledge Transla-tion. http:00www.cihr-irsc.gc.ca0e029418.html. Accessed July 26,2008.
21. Nutley S, Walter I, Davies HTO. From knowing to doing: A frameworkfor understanding the evidence-into-practice agenda. Evaluation. 2003;9~2!:125–148.
22. Rogers EM. Diffusion of Innovations. 3rd ed. New York, NY: FreePress; 1983.
23. Huberman M. Steps toward an integrated model of research utilization.Knowl. Creation Diffusion Util. 1987;8~4!:586–611.
24. Huberman M. Predicting conceptual effects in research utilization:Looking with both eyes. Knowl Soc Int J Knowl Transf. 1989;2~3!:6–24.
25. Huberman M. Linkage between researchers and practitioners: A qual-itative study. Am Educ Res J. 1990;27~2!:363–391.
26. Cousins J, Leithwood K. Enhancing knowledge utilization as a strat-egy for school improvement. Knowl Creation Diffusion Util. 1993;14~3!:305–333.
27. Rogers EM. Diffusion of Innovations. 4th ed. New York, NY: FreePress; 1995.
28. Best A, Stokols D, Green LW, Leichow S, Holmes B, Buchholz K. Anintegrative framework for community partnering to translate theoryinto effective health promotion strategy. Am J Health Promot. 2003;18~2!:168–178.
29. Logan J, Graham I. Toward a comprehensive interdisciplinary modelof health care research use. Sci Commun. 1998;20~2!:227–246.
30. Graham I, Logan J. Translating research: Innovations in knowl-edge transfer and continuity of care. Can J Nurs Res. 2004;36~2!:89–103.
31. Graham ID, Harrison MB, Brouwers N, Davies BL, Dunn S. Facili-tating the use of evidence in practice: Evaluating and adapting clinicalpractice guidelines for local use in health care organizations. J ObstetGynecol Neonatal Nurs. 2002;31:599–611.
Applying Knowledge to Generate Action
JOURNAL OF CONTINUING EDUCATION IN THE HEALTH PROFESSIONS—30(1), 2010 71DOI: 10.1002/chp