Applied Epidemiology
22
1 PREVENTIVE MEDICINE III APPLIED EPIDEMIOLOGY Dr. PHILIPP U. PO DR. Antonio E. CHAN Learning objectives 1. Define epidemiology and outline its scope 2. Differentiate epidemiology from clinical epidemiology 3. Describe approaches to establishing “normality” 4. Describe criteria and measures of disease occurrence commonly used in epidemiology 5. Enumerate some routinely available data use in epidemiology 6. Understand diagnostic test in relation to disease 7. Describe the main types of epidemiological studies 8. Enumerate the advantages and disadvantages of observational studies compared with experimental studies 9. Explain cause of disease 10. Outline the steps necessary to establish the cause of disease 11. Appreciate the differing approaches used in epidemiology to compare the occurrence of disease 12. Outline the role of epidemiology in describing the natural history of a disease and prognosis 13. Understand the role of epidemiology in the prevention and control of disease through identification of the causes of disease 14. Relate the different stages of the development of a disease to the phases of prevention What is Epidemiology? The study of the distribution and determinants of health-related states or events in specified populations, and the application of this study to control of health problems AIMS OF EPIDEMIOLOGY To understand the course of the disease (natural history of the disease) To identify the causes or risk factors To provide effective measures of treatment and prevention USES OF EPIDEMIOLOGY APPLIED EPIDEMIOLOGY Clinical epidemiology Communicable disease epidemiology Environmental and occupational epidemiology Molecular epidemiology CLINICAL EPIDEMIOLOGY Definition is the application of epidemiological principles and methods to the practice of clinical medicine is the science of making predictions about individual patients by counting clinical events in similar patients, using scientific methods for studies of groups of patients to ensure that the predictions are accurate Purpose: to develop and apply methods of clinical observations that will lead to valid conclusions by avoiding being misled by systematic error and chance to make good decisions in the care of patients Clinical Question Issue Question Abnormality Is the patient sick or well? Diagnosis How accurate is tests used to diagnose disease? Frequency How often does a disease occur? Risk What factors are associated with an increased risk of disease? Prognosis What are the consequences of having a disease? Treatment How does treatment change the course of disease? Prevention Does an intervention on well people keep disease from arising? Does early detection and treatment improve the course of disease? Cause What conditions lead to disease? What are the pathogenetic mechanisms of disease? Cost How much will care for an illness cost? Confounding variable: Male has higher risk factor for MI Female have lower prognostic factor - They have smaller coronary vessels - The real reason is the coronary vessels and not the fact that they are female. - Being a female is the confounding variable but it is not the real risk factor. We always have to consider the cause. Sources of data useful for epidemiology studies Data on vital events – birth and death Morbidity or disease statistics Data on physiologic and or pathologic condition Statistics on health resources and services Statistics pertaining to the environment
-
Upload
jerrica-charlene-galope -
Category
Documents
-
view
2 -
download
0
description
Applied Epidemiology
Transcript of Applied Epidemiology

1
PREVENTIVE MEDICINE III
APPLIED EPIDEMIOLOGY Dr. PHILIPP U. PO
DR. Antonio E. CHAN
Learning objectives 1. Define epidemiology and outline its scope 2. Differentiate epidemiology from clinical epidemiology 3. Describe approaches to establishing “normality” 4. Describe criteria and measures of disease occurrence commonly
used in epidemiology 5. Enumerate some routinely available data use in epidemiology 6. Understand diagnostic test in relation to disease 7. Describe the main types of epidemiological studies 8. Enumerate the advantages and disadvantages of observational
studies compared with experimental studies 9. Explain cause of disease 10. Outline the steps necessary to establish the cause of disease 11. Appreciate the differing approaches used in epidemiology to
compare the occurrence of disease 12. Outline the role of epidemiology in describing the natural history
of a disease and prognosis 13. Understand the role of epidemiology in the prevention and
control of disease through identification of the causes of disease 14. Relate the different stages of the development of a disease to the
phases of prevention
What is Epidemiology? The study of the distribution and determinants of health-related states or events in specified populations, and the application of this study to control of health problems AIMS OF EPIDEMIOLOGY
To understand the course of the disease (natural history of the disease)
To identify the causes or risk factors
To provide effective measures of treatment and prevention
USES OF EPIDEMIOLOGY
APPLIED EPIDEMIOLOGY
Clinical epidemiology Communicable disease epidemiology Environmental and occupational epidemiology Molecular epidemiology
CLINICAL EPIDEMIOLOGY Definition
is the application of epidemiological principles and methods to the practice of clinical medicine
is the science of making predictions about individual patients by counting clinical events in similar patients, using scientific methods for studies of groups of patients to ensure that the predictions are accurate
Purpose: to develop and apply methods of clinical observations that
will lead to valid conclusions by avoiding being misled by systematic error and chance
to make good decisions in the care of patients
Clinical Question Issue Question Abnormality Is the patient sick or well? Diagnosis How accurate is tests used to diagnose disease? Frequency How often does a disease occur? Risk What factors are associated with an increased
risk of disease? Prognosis What are the consequences of having a disease? Treatment How does treatment change the course of
disease? Prevention Does an intervention on well people keep
disease from arising? Does early detection and treatment improve the course of disease?
Cause What conditions lead to disease? What are the pathogenetic mechanisms of disease?
Cost How much will care for an illness cost? Confounding variable:
Male has higher risk factor for MI Female have lower prognostic factor
- They have smaller coronary vessels - The real reason is the coronary vessels and not
the fact that they are female. - Being a female is the confounding variable but it
is not the real risk factor. We always have to consider the cause. Sources of data useful for epidemiology studies
Data on vital events – birth and death Morbidity or disease statistics Data on physiologic and or pathologic condition Statistics on health resources and services Statistics pertaining to the environment

2
Demographic data Socio-cultural data
Make your own analysis, cross-tabulate or etc. to discover something that may be relevant
MEASURING HEALTH AND DISEASE
Clinical question: Is the patient sick or well? Health is defined as “a state of complete physical, mental, and social well-being and not merely the absence of disease or infirmity.” –WHO Epidemiologist’s definition of health states “disease present” or “disease absent” Diagnostic tests
Qualitative diagnostic test (+) or (-) results Quantitative diagnostic test Values are present Normal (Gaussian) distribution method Percentile method Therapeutic method Predictive value method Diagnostic criteria are usually based on symptoms, signs and test results 1. Hepatitis
Presence of antibodies in the blood 2. Asbestosis
Symptoms and signs of specific changes in lung function Radiographic demonstration of fibrosis of the lung tissue
or pleural thickening History of exposure to asbestos fibers
Respirable dust Asbestos fiber is long (> 5 microns) but is still considered respirable? Because the diameter will not reach 5mm.
The Jones Criteria (revised) for Guidance in the Diagnosis of Acute Rheumatic Fever
A high probability of rheumatic fever is indicated by the presence of two major or one major and two minor, manifestations, if supported by evidence of a preceding Group A streptococcal infection Major Manifestations Minor Manifestations Carditis Clinical: Polyarthritis fever Chorea athralgia (joint pains) Erythema marginatum previous rheumatic fever or Subcutaneous nodules rheumatic heart disease Laboratory Acute phase reactants: Abnormal ESR, CRP, leukocytosis Prolonged P-R interval WHO CASE-DEFINITION FOR AIDS The presence of disseminated Kaposis sarcoma or cryptococcal meningitis or Two major signs in association with at least one minor sign MAJOR SIGNS MINOR SIGNS Weight loss > 10% Persistent cough > 1 month Fever > 1 month General pruritic dermatitis Chronic diarrhea > 1 month Recurrent herpes zoster General lymphadenopathy Chronic herpes simplex Oral candidiasis
Measuring Health and Disease
Diagnostic criteria must be clearly stated, easy to use and easy to measure in a standard manner under a wide variety of circumstances by different people
Diagnostic criteria may change quite rapidly as knowledge or techniques improve.
Definitions used in clinical practice are less rigidly specified and clinical judgment is more important in diagnosis
The development of criteria to establish the presence of disease requires definition of normality and abnormality
Difficult to define what is normal
No clear distinction between normal and abnormal
APPROACHES IN ESTABLISHING “NORMALITY”
Clinical question: Is the patient sick or well?
Problem (misclassification) Clinical measurements
Nominal asymptomatic Ordinal cut-off point Interval or ratio Any biologic parameter can be measured. Mild moderate… Clinical measurements have skewed distributions Percentile method (same prevalence rates) Normal Abnormal Common or usual being unusual Well being sick Not being treatable being treatable

3
MEASURES OF DISEASE FREQUENCY
Clinical question: How often does a disease occur?
PREVALENCE
Prevalence of a disease is the number of cases in a defined population at a specified point in time
- Point prevalence - Period prevalence
Prevalence studies do not usually provide strong evidence of causality
It is helpful in assessing the need for health care and the planning of health services
Prevalence rates are often used to measure the occurrence of conditions for which the onset of disease may be gradual
You measured the causes and the effects at the same time.
The prevalence rate (P) for a disease is calculated as follows: Number of people with the disease or condition P = ----------------------------------------------------------------- (x factor) Number of people in the population at risk at the specified time (Cross-sectional)
Factors influencing observed prevalence rate Increased by: Decreased by: Longer duration of the disease Shorter duration of disease Prolongation of life of patient High case-fatality rate from disease without cure Increase in new case Decrease in new cases (increase in incidence) (decrease in incidence) In-migration of cases In-migration of healthy people Out-migration of healthy people Out-migration of cases In-migration of susceptible people Improved cure rate of cases Improved diagnostic facilities (better reporting)
(Longer duration, they are still included in the numerator.)
INCIDENCE
Incidence is the number of new cases arising in a given period in a specified population
Incidence you need a base line before you can determine this
Incidence rate (I) Number of people who get a disease in a specified period I = ---------------------------------------------------- X (factor) Sum of the length of time during which each person in the population is at risk (Longitudinal) Incidence rate
The numerator is the number of new events that occur in a defined time period
The denominator is the population at risk of experiencing the event during this period
The most accurate way of calculating incidence rate is to calculate the person-time incidence rate (Incidence density)
Cumulative incidence rate or risk (CI) Number of people who get a disease during a specified period CI = ---------------------------------------------------- X (factor) Number of people free of the disease in the population at risk at the beginning of the period (Not the person time in the denominator)
At the beginning of 1992, there are 4 cases, prevalence is 4/100; at the beginning of 1993, the prevalence is 5/100; 7/100 in 1994 and 5/100 in 1995 Incidence rate, we consider only the 96 individuals free of the disease at the beginning of 1992; 5 new cases in 1992; 6 new cases in 1993; 5 new cases in 1994; The 3-year incidence of the disease 16/96; but the annual incidence is 5/96 in 1992; 6/91 in 1993; and 5/85 in 1994
Incidence rate is 3/33 person-years or 9.1 cases per 100 person-years; cumulative incidence is 3/7 or 43 case per 100 persons; the average duration of disease is 10/3 or 3.3 years Prevalence at year 4 = 2/6 or 33 cases per 100 persons but the average prevalence is duration of disease x incidence rate = 3.3 X 9.1 = 30 cases per 100 population

4
Cumulative incidence rate
Unlike incidence rate, it measures the denominator only at the beginning of a study
This rate has a simplicity that makes it suitable for the communication of health information to decision makers
Easy to interpret and provide a useful summary measure
It is useful approximation of incidence rate when the rate is low or when the study period is short
Case-fatality rate a measure of the severity of a disease No. of deaths from a disease in a specified period Case fatality rate = ------------------------------------------ X 100 (CFR) No. of diagnosed cases of the disease in the same period USE OF AVAILABLE INFORMATION (Mortality) Number of deaths in a specified period Crude mortality rate = --------------------------------------------------------- X F (CMR) Average total population during that period
This mortality can be made specific as to age, sex or cause
Not appropriate to use for comparison because death varies according age, sex, race, socio-economic class and other factors
Comparison of mortality rates between groups of diverse age structure are usually based on age-standardized rates
Standardization of rates (Adjustment of rates) 1. Direct adjustment of rates
This requires the selection of some population, called a standard population, to which the age-specific rates for each population can be applied.
2. Indirect adjustment of rates
Standardization is based on age-specific rates rather than age composition
The population whose rates form the basis for comparison is referred to as the “standard population”
The larger of the two populations is usually chosen as standard because its rates tend to be more stable
If developed and an undeveloped country are compared, the developed country would probably be taken as the standard
A common way of carrying out indirect age-adjustment is to relate the total expected deaths thus obtained to observed deaths through a formula known as the Standardized Mortality Ratio (SMR)
Total observed deaths in a population SMR = ------------------------------------------------------- Total expected deaths in that population Interpretation:
If this mortality ratio is greater than 1, it means that more deaths are observed in the smaller or comparison population than would be expected on the basis of rates in the larger (standard) population
If the ratio is less than 1, fewer deaths are observed than expected
The CDR is higher in the A. Considering that the population composition is not the same. Mas maraming ams matanda. Kaya, hindi reliable ang CDR in this case.

5
Mortality No. of deaths in a year of children
less than 1 year of age Infant mortality rate = ------------------------------------------------------ X F No. of live births in the same year
(July 1 of the preceeding year to June 30 for the current year)
A measure of overall health status for a given population
It is based on the assumption that it is particularly sensitive to socio-economic changes and to health care intervention
Other measures of mortality in early childhood are : 1. Fetal death rate 2. Stillbirth or late fetal death rate 3. Perinatal mortality rate 4. Neonatal mortality rate 5. Postneonatal mortality rate Child mortality rate is based on deaths of children aged 1 – 4 years and is important because accidental injuries, malnutrition and infectious diseases are common in this age group Maternal pregnancy-related deaths in a year Maternal mortality rate = ------------------------------------- Total births in the same year (MMR = 28 in the Philippines) Life expectancy is the average number of years an individual of a given age is expected to live if current mortality rates continue
DIAGNOSIS
Clinical question: How accurate are tests used to diagnose disease? Diagnostic test – the objective is to diagnose any treatable disease present Characteristics of a diagnostic test
Reliable – gives the same measurement when repeated more than once
Valid - measures what it intends to measure
Accurate – correctly determines those with disease and those without
Easy to use – can be performed by other people without difficulty
Not expensive – affordable
Safe and acceptable Gold standard
a sounder indication of truth or a standard of accuracy
a new diagnostic test is compared elusive (not available)
expensive and risky – biopsy, surgical exploration, autopsy
sometimes simple – throat swab culture
(Predictive value method)
Validity of a diagnostic test a = no. of true positives, b = no. of false positives c = no. of false negatives, d = no. of true negatives Sensitivity = probability of a positive test in people with the disease = a/ (a + c) Specificity = probability of a negative test in people without the disease Positive predictive value = probability of the person having the disease when the test is positive = a / (a + b) Negative predictive value = probability of the person not having the disease when the test is negative = d / (c + d)

6
DISEASE
Clinical question: How accurate are tests to diagnose disease? Use of multiple diagnostic tests
Use of imperfect diagnostic tests, with less than 100% sensitivity and specificity, a single test frequently results in a probability of disease that is neither very high or very low
Parallel tests (all at once)
Used when rapid assessment is necessary as in hospitalized or emergency patients, or for ambulatory patients who cannot return easily for evaluation because they have come from a long distance
Parallel tests generally increase the sensitivity and, therefore, the negative predictive value for a given disease prevalence above those of each individual test. On the other hand, specificity and positive predictive value are lowered
Parallel testing is useful when the clinician is faced with the need for a very sensitive test but has available only two or more relatively insensitive ones
Serial testing (consecutively, based on previous test result)
Used when rapid assessment is not required
Used when some of the tests are expensive or risky Maximizes specificity and positive predictive value but
lowers sensitivity and the negative predictive value.
The process is more efficient if the test with the highest specificity is used first.
Statements about validity test
Sensitivity and specificity are inversely related.
A sensitive test can pick up most cases of the disease but it will erroneously label as positive many persons who do not have the disease.
A highly specific test will correctly label as negative those who do not have the disease but it will miss many cases
A very sensitive test gives a low positive predictive value since it produces many false positive. Conversely, a very specific test gives a high positive predictive value.
Sensitivity and specificity are unaffected by the prevalence of the disease or condition. Since sensitivity depends only on those with the disease or condition and specificity only on those without the disease or condition.
The positive predictive value of a test increases with the prevalence of the disease.
Uses of sensitive tests - A sensitive test should be chosen when there is an
important penalty for missing a disease (dangerous but treatable condition)
- A sensitive test is most helpful to the clinician when the test result is negative (to rule out disease)
Uses of specific tests - Highly specific tests are needed when false-positive
results can harm the patient physically, emotionally, or financially.
- A specific test is most helpful when the test result is positive (to confirm or “rule in” the disease

7
Receiver operator characteristic curve Tests that discriminate well crowd toward the upper left corner of the ROC curve;Tests that perform less well have curves that fall closer to the diagonal running from left lower to upper right. The diagonal line shows the relationship between true-positive and false positive rates that would occur for a test yielding no information.
LIKELIHOOD RATIO
Alternative way of describing the performance of a diagnostic test
Summarize the same kind of information as sensitivity and specificity
Used to calculate the probability of disease after a positive or negative test (positive or negative predictive value)
Advantage – can be used at multiple level of test results. Use of likelihood ratios depends on odds
Probability - Used to express sensitivity, specificity and predictive
value - Is the proportion of people in whom a particular
characteristic, such as a positive test, is present
Odds - Is the ratio of two probabilities (the probability of an
event to that of 1 – probability of event Odds and probability contain the same information, but
they express it differently The two can be interconverted using simple formulas:
Probability of event Odds = ------------------------------- 1 – Probability of event Odds Probability = ------------------------- 1 + Odds
Express how many times more (or less) likely a test is to be
found in diseased, compared with non-diseased, people.
If a test yields dichotomous results (both positive and negative)
Two types of likelihood ratios described its ability to discriminate between diseased and non-diseased people
1. Test’s positive likelihood ratio (LR+) – the ratio of the proportion of diseased people
with a positive test result (sensitivity) to the proportion of non-diseased with a positive test result
(1 – specificity) 2. Test’s negative likelihood ratio (LR-)
– the proportion of diseased people with a negative test result (1 – sensitivity) divided by the proportion of non-diseased people with a negative test result (specificity)
INTERPRETATION OF LIKELIHOOD RATIOS
Likelihood Ratio is the probability of a particular test result for a person with the disease of interest divided by the probability of that test result for a person without the disease of interest
An LR+ of one indicates a test with no value in sorting out persons with and without the disease of interest, since the probability of a positive test result is equally likely for affected and unaffected persons.
The larger the value of the LR+, the stronger the association between having a positive test result and having the disease of interest
The larger the size of the LR+ the better the diagnostic value of the test. Although somewhat arbitrary, an LR+ value of 10 or greater is often perceived as in indication of a test of high diagnostic value
An LR- with a value of one indicates a test with no value in sorting out persons with and without the disease of interest as the probability of a negative test result is equally likely among persons affected and unaffected.
The smaller the value of the LR-, the stronger the association between having a negative test result and not having the disease of interest.
The smaller the size of the LR-, the better the diagnostic value of the test. On somewhat arbitrary grounds, an LR- value of 0.1 or less is often perceived as an indication of a test with high diagnostic value
TECHNIQUES FOR USING LIKELIHOOD RATIOS
A. Mathematical approach B. Using a likelihood ratio nomogram C. Simple “Rule of Thumb” for determining effect of
likelihood ratios on disease probability

8
Mathematical Approach 1. Convert Pretest Probability (Prevalence) to Pretest odds
Pretest odds = Prevalence / (1 – Prevalence) 2. Multiply Pretest odds by Likelihood ratio to obtain
Posttest odds Pretest odds X Likelihood ratio = Posttest odds
3. Convert Posttest odds to Posttest probability (predictive value) Posttest probability = Posttest odds / (1 + Posttest odds)
Using a likelihood ratio nomogram
Place a straight edge at the correct prevalence and likelihood ratio values and read off the posttest probability where the straight edge crosses the line
Simple “Rule of Thumb”
Mnemonic
- Likelihood ratio of 2, 5, 10 increases the probability of disease approximately 15%, 30% and 45% respectively, and the inverse of these likelihood ratios of 0.5, 0.2, and 0.1 decrease the probability of disease similarly 15%, 30%, and 45%
LIKELIHOOD RATIOS (con’d)
Likelihood ratios must be used with odds, not probability
The main advantage of likelihood ratios is that they make it possible to go beyond the simple and clumsy classification of a test result as either abnormal or normal, as is usually done when describing the accuracy of a diagnostic test only I terms of sensitivity and specificity at a single cutoff point.
Disease is more likely in the presence of an extremely abnormal test result than it is for a marginal one
With likelihood ratios, it is possible to summarize information contained in a test result at different levels
In computing likelihood ratios across range of test results, a limitation of sensitivity and specificity is overcome.
Can accommodate the common and reasonable, clinical practice of putting more weight on extremely high (or low)
test results than on borderline ones when estimating the probability (or odds) that a particular disease is present.
Likelihood ratio for hypothyroidism were highest for low levels of T4 and lowest for high levels. The lowest values in the distribution of T4 (<4.0 mg/dL) were only seen in patients with hypothyroidism (these levels ruled in the diagnosis). The highest levels (>8.) mg/dL) were not seen in patients with hypothyroidism (the presence of these levels ruled out the disease)
PROBLEMS
Lack of information on negative tests Lack of information on test results in the nondiseased Lack of objective standards for disease Consequences of imperfect standards
If a new test is compared with an old (but inaccurate) standard test, the new test may seem worse even when it is actually better Reliability and validity Measurement error Instrument The means of making the measurement Observer The person making the measurement Biologic variation Within individuals Changes in people with time and situation Among individuals Biologic differences from person to person
An instrument can be valid (accurate) on the average but not be reliable; because the measures obtained are widely scattered about the true value. On the otherhand, an instrument can be very reliable but be systematically off the mark (inaccurate); A single measurement with poor reliability has low validity because it is likely to be off the mark simply because of chance alone.
EARLY DIAGNOSIS
Strategies - Screening test (uni- or multi-phasic) - Periodic health examination - Case finding
Objectives - Early detection of asymptomatic disease - Identification of predictors or risk factors of
disease

9
NATURAL HISTORY OF DISEASE (FOUR STAGES) 1. Biologic onset
- initial interaction between man, causal factors, and the rest of the environment
- cannot detect the presence of disease 2. Early diagnosis possible
- mechanisms of disease produce structural or functional changes
- individual remains free of any symptoms 3. Usual clinical diagnosis
- disease progresses to the point where symptoms appear and affected individual becomes ill
4. Outcome - recovery, permanent disability or
death
(In between there are critical points)
Another assumption underlies attempts at early diagnosis. This element was described by Hutchison in 1960 and consists of a “critical point” in the natural history of a disease, before which therapy is either more effective or easier to apply than afterward. A disease may have several critical points (pulmonary tuberculosis) or may have none (several cancers), and the location of these critical points along its natural history is crucial to the value of early diagnosis. CP = Critical Point CRITICAL POINTS IN THE NATURAL HISTORY OF DISEASE Position 1
The screening test and case finding would be too late to be of help in early detection of disease
Position 2
The test will have a promise of improving the outcomes of those who have the target disorder
Position 3
Early detection of the disease is a waste of time “How do we tell a disease has a critical point at position 2 and its detection is worth our critical effort?”
No benefit could be confirmed among women under age 50, but striking reductions in breast cancer mortality were observed at age 50 and beyond (the mortality from other causes of death was identical, confirming that randomization had produced comparable groups of experimental and control women). This landmark randomized trial (confirmed by additional subsequent trials) demonstrated that a critical point does, in fact, exist in the natural history of breast cancer and that it is located between the point where early diagnosis is possible and the time of usual clinical diagnosis.
HOW TO DECIDE WHEN TO SEEK AN EARLY DIAGNOSIS
1. Does early diagnosis really lead to improved clinical outcomes (in terms of survival, function, and quality of life)?
2. Can you manage the additional clinical time required to confirm the diagnosis and provide long-term care for those screen positive?
3. Will the patients in whom an early diagnosis is achieved comply with your subsequent recommendations and treatment regimen
4. Has the effectiveness of individual components of a periodic health examination or multiphasic screening program been demonstrated prior to their combination?
5. Does the burden of disability from the target disease warrant action?
6. Are the cost, accuracy, and acceptability of the screening test adequate for your purpose?
Effectiveness versus efficacy Effectiveness – Does offering treatment work in ordinary condition? Efficacy – Dose giving the treatment work in ideal condition?
Does early diagnosis really lead to improved clinical outcomes (in terms of survival, function, and quality of life)?
Claims for therapeutic benefit must withstand close scrutiny and experimental evidence from randomized trials is a prerequisite.
Long-term beneficial effects of therapy outweigh the long-term detrimental effects of the treatment regimen and labeling of patients as diseased.
Can you manage the additional clinical time required to confirm the diagnosis and provide long-term care for those screen positive?
Increased demands on your time start with early diagnosis and you need to be sure that you have enough of it.
Large numbers of labeled but untreated hypertensive attest to the size of this problem
Will the patients in whom an early diagnosis is achieved comply with your subsequent recommendations and treatment regimens
If patients will not take their medicine, all the screening and diagnosis made are nullified.
Labeled patient Have the effectiveness of individual components of a periodic health examination or multiphasic screening program been demonstrated prior to their combination?
The appropriateness of a mix of tests must consider whether differences in the distributions of two diseases render the combination of their respective screening tests nonsensical.
It was this consideration that led the Canadian Task Force on the Periodic Health Examination to propose quite different “health protection packages” for patients of different age, sex, and social status.

10
Does the burden of disability from the target disease warrant action?
The disease you are searching for should be either so common or so awful as to warrant all the work and expense of detecting it in its presymptomatic state
TYPES OF EPIDEMIOLOGICAL STUDIES
Observational studies allow nature to take its course: the investigator measures but does not intervene. In an experiment the investigator studies the impact of varying some factor that he controls. For example, he may take a litter of rats, expose one of two randomly selected halves to a supposedly carcinogenic agent, and then record the frequency with which cancer develops in the two groups. In the more usual approach the investigator can only observe the occurrence of disease in people who are already segregated into groups on the basis of some experience or exposure. In this kind of study, allocation into groups on the basis of exposure to a factor is not under the control of the investigator.
DESCRIPTIVE STUDIES 1) Case reports
detailed presentations of a single case or a handful of cases
means of describing rare clinical events describe unusual manifestations of disease elucidate the mechanisms of disease and treatment place issues before medical community and often trigger
more decisive studies susceptible to bias
2) Case-series
a simple descriptive account of interesting characteristics observed in a group of patients
study larger group of patients (e.g. 10 or more) with particular disease
describe the clinical manifestations of disease and treatments in a group of patients assembled at one point in time
absence of a comparison group, not conclusive
hypothesis-generating
selection bias
OBSERVATIONAL STUDIES 1) Ecological studies
aggregate risk studies units of analysis are populations or groups of people rather
than individuals rely on data collected for other purposes; data on different
exposures and on socioeconomic factors may not be available
ecological fallacy (bias) useful in raising hypothesis
An ecological fallacy results if inappropriate conclusions are drawn on the basis of ecological data. The association observed between variables at the group level does not necessarily represent the association that exists at the individual level Increase in alcohol consumption and increase in liver cirrhosis but we don’t know if there are other factors. 1:1 comparison
2) Cross-sectional studies (Prevalence studies)
measure the prevalence of disease measurements of exposure and effect are made at the
same time useful for investigating exposures that are fixed
characteristics of individuals, such as ethnicity, socio-economic status and blood group, or chronic diseases or stable conditions
in sudden outbreaks of disease it is the most convenient first step in an investigation into the cause
Rare disease, conditions of short duration or diseases with high case fatality are often not detected
short-term and therefore less costly provide no direct estimate of risk prone to bias from selective survival estimates of prevalence may be biased by the exclusion of
cases in which death or recovery are rapid Uncertainty about the temporal sequence and biases associated with the study of cases of longer duration (old cases) Clinicians use incidence and prevalence for predicting future course of the disease, assigning a probability to a patient, and making comparisons. Clinicians use measures of frequency as the ingredients in comparative measures of the association between a factor and the disease or disease outcome. Cohort – Relative Risk Case Control – Odds Ratio Cross Sectional – Rates BUT NO RISKSSSS 3) Case-control studies
longitudinal studies (looking backward from the disease to
a possible cause)
use new (incident) cases
used to investigate cause (etiology) of disease, esp. rare diseases
used odds ratio
relatively efficient, requiring smaller sample than cohort study
completed faster and more economical earliest practical observational strategy for determining an
association
antecedent-consequence uncertainty

11
Odds ratio – measure of the strength association Interpretation of Odds ratio
Odds ratio is the ratio of the odds of exposure among cases to the odds in favor of exposure among the controls.
The odds of having the disease in question are OR times greater among those exposed than those with no exposure
The larger the value of OR, the stronger the association between the disease in question and exposure to the risk factor
When the value of OR is close to 1, the disease and the exposure to the risk factor are unrelated
Interpretation of Odds ratio
Value of OR less than 1 indicates a negative association (i.e., protective effect) between the risk factor and the disease
For rare disease (e.g., most chronic diseases with disease prevalence of less than 10%), OR approximates RR
4) Cohort studies
Concurrent cohort is better than historical due to recall bias
longitudinal studies (forward)
provide the best information about the causation of disease
most direct measurement of the risk of developing disease provide the possibility of estimating the attributable risks
use relative risk (Attributable risk refers to the magnitude of disease attributable to a risk factor)
most closely resemble experimental studies Long-term, not always feasible
Sample size required for the study extremely large
Attrition is most serious problem
Relative risk of a disease is the ratio of incidence in exposed persons to incidence in non-exposed persons
Interpretation of relative risk (RR)
The disease (or other health related outcome) is RR times more likely to occur among those exposed than among those with no exposure
The larger the value of RR, the stronger the association between the disease in question and exposure to the risk factor
Value of RR close to 1 indicates that the disease and exposure to the risk factor are unrelated
Value of RR less than 1 indicates a negative association between the risk factor and the disease (i.e., protective rather than detrimental)
Example of cohort study Problem: A county school system provides lunch to 10,000 school children. During the first week of school, 2,500 of these children ate chicken salad later shown to be contaminated with salmonella. The entire population of 10,000 students was subsequently followed for one month to determine whether exposure to salmonella increased the risk of diarrhea.

12
EXPERIMENTAL STUDIES 1) Randomized controlled trials (RCTs)
Treatment and control groups have the same characteristics.
Gold standard or reference in medicine
Provide the greatest justification for concluding causality Subject to the least number of problems or biases
Best study design to establish the efficacy of a treatment or a procedure
Expensive and time-consuming
Difficult to obtain approval to perform properly designed clinical trials
Bias in Clinical Observation
Selection bias occurs when comparisons are made between groups of patients that differ in determinants of outcome other than the one under study
Measurement bias occurs when the methods of measurement are dissimilar among groups of patients
Confounding bias occurs when two factors are associated (“travel together”) and the effect of one is confused with or distorted by the effect of the other
Selection bias occurs when there is a systematic difference between the characteristics of the people selected for a study and the characteristics of those who are not. (when participants select themselves for a study, either because they are unwell or because they are particularly worried about an exposure.) Confounding can occur when another exposure exists in the study population and is associated both with the disease and the exposure being studied. Example : Coffee drinking, cigarette smoking, and coronary heart disease. CONFOUNDING BIAS RISK FACTORS AND MI
Males have a higher risk to have myocardial infarction prognostic factor. Observe that female has a poor prognosis after an MI (they are more prone to have another MI, CVE or cardiac death) The smaller coronary vessel the worse the prognosis. Females usually have a small coronary vessel. The female is confounding. The real variable is small coronary vessels.
Best case/worst case analysis – A cohort of 123 morbidly obese patients was studied 19-47 months after surgery. Success was defined as having lost more than 30% of excess weight. Only 103 patients (84%) could be located. In these, the success rate of surgery was 60/103 (58%). Best case success rate (60+20)/123 or 65%; Worse case success rate 60/123 or 49% Thus the true rate must have been between 49 and 65%.
CAUSE
Clinical question: What conditions lead to disease? What are the pathogenetic mechanisms of disease?
Webster’s definition: “something that brings about an effect or a result”
“A factor is a cause of an event if its operation increases the frequency of an event”
In medicine : “etiology” “pathogenesis” “mechanisms” or “risk factors”
Importance: prevention, diagnosis and treatment of disease
Concepts of Cause Single causation (Koch’s postulates) a particular disease has one cause and a particular cause results in one disease
1. The organism must be present in every case of the disease 2. The organism must be isolated and grown in pure culture 3. The organism must cause a specific disease when
inoculated into an animals and 4. The organism must then be recovered from the animal and
identified

13
Multiple causation (Web of causation)
Effects never depend on single isolated causes, but rather develop as the result of chains of causation in which each link itself is the result of “a complex genealogy of antecedents.”
Many factors act together to cause disease Concept of Cause
A cause must precede a disease A cause is termed sufficient when it inevitably produces or
initiates a disease A cause is termed necessary if a disease cannot develop in
its absence A sufficient cause is not usually a single factor, but often
comprises several components It is not necessary to identify all the components of a
sufficient cause before effective prevention can take place Each sufficient cause has a necessary cause as a
component A causal factor on its own is often neither necessary nor
sufficient Proximity of cause to effect Disease is also determined by less specific, more remote
causes or risk factors, such as people’s behavior or characteristics of their environment.
Tuberculosis as an example: Check for the modifiable risk factors, try to modify them.
A schematic diagram of sufficient causes in a hypothetical individual. Each constellation of component causes is minimally sufficient to produce disease; that is, there is no redundant or extraneous component cause – each one is a necessary part of that specific causal mechanism. A specific component cause may play a role in one, several, or all of the causal mechanism. It can facilitate an understanding of some key concepts such as 1. strength of effect 2 interaction
Causation
Causal relationship in the physical sciences are often simple, as in Boyle’s law relating pressure and volume of a gas, or the effect of heat on a metal bar. The causal agent is sufficient, the time relationship is short, and replication is easy.
In the Boyle’s law situation, a change in pressure was both necessary and sufficient for a change in volume, given that the other circumstances were fixed.
In the metal bar example, heat was sufficient but not a necessary cause; there are other ways of lengthening a metal bar
Causal relationship in human health and disease are rarely simple
In human health and disease not all causal agents are sufficient.
In the disease tuberculosis, infection by the tubercle bacillus does not invariably lead to clinical tuberculosis.
Only a small proportion of those who are infected by the bacillus develop clinical tuberculosis
Most situations in health and disease do not fulfill the criteria either necessary or for sufficient causation.
An healthy man is admitted to hospital with multiple fractures, having been hit by a bus just outside the hospital
We can conclude that there was a causal relationship between being hit by the bus and having multiple fractures
But the relationship implies neither that the cause is sufficient nor that it is necessary.
Not all people hit by buses have multiple fractures. Not all patients with multiple fractures have been hit by buses.
Where the time relation is not clear, and the concepts of necessary and sufficient cause do not hold, we need a quantitative assessment of the relationship, based on observations not on one individual but on a number of individuals. Hence, the definition of causation is quantitative
A direct test of the quantitative definition of causation is by randomized trial approach
Proximity of cause to effect
Disease is also determined by less specific, more remote causes or risk factors, such as people’s behavior or characteristics of their environment.
These factors may be even more important causes of disease than are pathogenetic mechanisms
If the pathogenetic mechanism is not clear, knowledge of risk factors may still lead to very effective treatments and prevention
Don’t need to know mechanisms of the disease we know the sufficient cause and we can already control disease.
Interplay of multiple causes Synergism – the joint effect is greater than the sum of the
effects of the individual causes Antagonism – the joint effect is lesser Effect Modification – a special type of interaction A substantial impact on a patient’s health by changing only
one or a small number of the causes When more than one cause act together, the resulting risk may be greater than or less than would be expected by simply combining the effects of the separate causes Effect modification is present when the strength of the relationship between two variables is different according to the level of some third variable, called an effect modifier. Thiazide diuretics at 25, 50, 100 mg – sudden death – potassium sparing therapy
Cause as a risk factor
Risk refers to the probability of some untoward event
Risk indicates the likelihood that people who are exposed to certain factors (risk factors) will subsequently develop a particular disease
Risk factor refers to condition, physical characteristic, or behavior that increases the probability (i.e., risk) that a currently healthy individual will develop a particular disease.
Exposure to risk factor can occur at a single point in time or over a period of time
ever exposed current dose largest dose taken total cumulative dose years of exposure years since first contact

14
Recognizing risk
Large risks associated with effects that occur rapidly after exposure are easy for anyone to recognize
Most morbidity and mortality are caused by chronic diseases. The relationship between exposure and disease are far less obvious – latency period
It is not difficult to appreciate the relationship between exposure and disease for conditions such as chicken pox, sunburn, and aspirin overdose, IF RR is high, easy to recognize the cause of disease.
Comparing disease occurrence among exposed and unexposed 1) Absolute comparison
Risk difference, also called attributable risk (exposed), excess risk or absolute risk
Attibutable fraction (exposed) or etiological fraction (exposed)
Population attributable risk or attributable fraction (population)
2) Relative comparison Risk ratio
Standardized mortality ratio The larger the risk Difference, the higher the association Being exposed to the disease leads to a higher risk.
Person being observed for 5 years - 1 person for 5 years – 1 person years.
Risk difference is the difference in rates of occurrence between exposed and unexposed groups; useful measure of the extent of the public health problem caused by the exposure Example:
49.6 – 17.7 = 31.9 per 100,000 person-years Attributable fraction (exposed) is the proportion of the disease in the specific population that would be eliminated in the absence of exposure determined by dividing the risk difference by the rate of occurrence among the exposed population DENOMINATOR IS THE ONE EXPOSED
Example: [(49.6 – 17.7) / 49.6] x 100 = 64% Interpretation: One would expect to achieve a 64% reduction in the risk of stroke among the women smokers if smoking were stopped, on the assumption that smoking is both causal and preventable Population attributable risk [attributable fraction (population)] is a measure of the excess rate of disease in a total study population which is attributable to an exposure; useful for determining the relative importance of exposures for the entire population and is the proportion by which the incidence rate of the outcome in the entire population would be reduced if exposure were eliminated.
Ip = Incidence rate of the disease in the total population; Iu = Incidence rate of the disease among the unexposed group Risk ratio or relative risk
the ratio of the risk of occurrence of a disease among exposed people to that among the unexposed
better indicator of the strength of an association than the risk difference
used in assessing the likelihood that an association represents a causal relationship
Example: RR = 49.6 / 17.7 = 2.8 The higher the RR: If one is exposed, this is how much you will get the disease. Less than 1 protective
Uses of risk factor
1. predict the occurrence of disease 2. marker of disease outcome 3. improve the positive predictive value of a diagnostic test 4. prevent disease
A risk factor that is not a cause of disease is called marker because it “marks” the increased probability of disease Knowledge of risk can be used in the diagnostic process, since the presence of a risk factor increased the prevalence of disease among patients – one way of improving the positive predictive value of a diagnostic test. If a risk factor is also a cause of disease, its removal can be used to prevent disease whether or not the mechanism by which the disease takes place is known.
Establishing cause
In clinical medicine, it is not possible to prove causal relationship beyond any doubt. It is only possible to increase one’s conviction of a cause and effect relationship, by means of empiric evidence, cause is established.
Factors that are considered causes at one time are sometimes found to be indirectly related to disease later, when more evidences are available
Two factors – the suspected cause and the effect – obviously must appear to be associated if they are to be considered as cause and effect
However, not all associations are causal
Two factors may be associated but not causal due to the presence of selection and measurement biases, chance and confounder
Guidelines for Causation Temporal Does the cause precede the effect? (essential) Plausibility Is the association consistent with other
knowledge? (mechanism of action; evidence from experimental animals)
Consistency Have similar results been shown in other studies?
Strength What is the strength of the association between
the cause and the effect? (relative risk) Dose-response Is increased exposure to the possible cause relationship associated with increased effect? Dose-response relationship Alcohol

15
Reversibility Does the removal of a possible cause lead to reduction of disease risk?
There are a lot of diseases that are irreversible. Thus, it is not necessary in all cases.
Study design Is the evidence based on a strong study design? Judging the How many lines of evidence lead to the evidence conclusion?
NATURAL HISTORY OF A DISEASE AND PROGNOSIS
Clinical question: What are the consequences of having a disease? Prognosis is a prediction of the future course of disease following its onset. Natural history of disease refers to the stages of a disease.
Be familiar with this slide! Primary - Use of seatbelts, helmets and protective gears Secondary – Detection
Prognostic factors are conditions that are associated with a given outcome of the disease Risk factors Prognostic factors events being counted are a variety of consequences the onset of disease of disease are counted predict low probability describe relatively frequent events events E.g. Risk factors of Myocardial infarction
Multiple prognostic factors and prediction rules
A combination of factors may give a more precise prognosis than each of the same factors taken one at a time
Clinical prediction rules estimate the probability of outcomes according to a set of patient characteristics
Prognostic staging of AIDS – once patients with HIV infection develop AIDS, the prognosis is poor and survival time is short.- with 1 point for the presence of each of 7 factors – severe diarrhea or a serum albumin <2.0 gm/dL, any neurologic deficit, Po2 less than or equal to 50 mm Hg, hematocirti <30%. ;lymphocyte count <150/mL, white count <2500/mL, and platelet count <140,000/mL – Stage I, 0 point; II, 1 point; III, greater than or equal to 2 points
TUBERCULOUS MENINGITIS (STAGING) STAGE I Characterized by non-specific symptoms such as fever, headache, irritability, drowsiness and body malaise. Focal neurologic signs are absent STAGE II Characterized by lethargy nuchal rigidity, seizures, positive Kernig or Brudzinski signs, hypertonia, vomiting, cranial nerve palsies and other focal neurologic signs STAGE III Characterized by coma, hemiplegia or paraplegia, hypertension, decerebrate posturing, deterioration of vital signs and eventually death Coma alone may not be specific but if you have all the following, then it would be most likely.
Survival analysis (Kaplan-Meir analysis) more common manner
- a way of estimating the survival of a cohort over time
Life table analysis MAKING A PROGNOSIS
1. What do we tell the patient? Should we keep mum, reassure him that his illness is trivial, or advise him to make out his will?
2. What do we do for the patient? Should we reassure him and leave him alone, simply watch and wait, or treat him as soon as possible?
The answers to these questions depend on our understanding of the natural history of the disease
- time course of the interactions between the patient, the causal factors for his disease, and the rest of his environment

16
- beginning with the biologic onset of disease and ending with his recovery, death, or arrival at some other physical, social, and emotional state
In deciding what to tell and what to do for the patient, we will be extrapolating from what we know about the likely clinical course of the patient’s disease in order to make judgments about the patient’s prognosis
In some situations, making a prognosis is clear cut and easy but in some it is difficult
(Sample cases)
1. Suppose that you discover a symptom-less subcutaneous lipoma on the back of an anxious steelworker who has come to you for insomnia and dyspepsia, which began after being laid off by the mill.
2. Suppose the biopsy of a mass discovered on rectal examination of an otherwise robust 62-year-old waitress with recent rectal bleeding reveals a well-differentiated carcinoma.
1. Aware of the benign clinical course of such lumps and alert to the potential dangers of labeling the patient as having a “tumor” you probably will decide to tell him nothing, at least until his current problem is resolved and simply will make a note to check the lipoma at a subsequent visit to confirm its innocence. 2. Aware of the serious prognosis and alert to the potential benefit of prompt surgical evaluation, you will inform the patient of her condition and arrange an early referral. The main problem is the patient is anxious which causes insomnia and dyspepsia and not necessarily the cancer.
3. Suppose you detect 10-15 degrees of scoliosis in an
otherwise healthy 12-year-old student who has come for her preschool examination. Do you tell her and her parents, refer her to an “orthopod” or what?
4. Suppose you have finally controlled a 37-year-old accountant’s left-sided ulcerative colitis that had troubled him since he was 32. Should you now recommend a prophylactic colectomy to obviate the risk of subsequent cancer?
What to do for difficult situations
Seek an expert opinion
Read up on clinical literature about clinical course and prognosis
Prognosticate based on your own clinical experience GUIDES FOR READING ARTICLES TO LEARN THE CLINICAL COURSE AND PROGNOSIS OF DISEASE
1. Was an “inception cohort” assembled? 2. Was the referral pattern described? 3. Was complete follow-up achieved? 4. Were objective outcome criteria developed and used? 5. Was the outcome assessment “blind”? 6. Was adjustment for extraneous prognostic factors carried
out? Inception cohort serotype Problem with study of prognostication = hard to assemble patients with the same serotype at the same stage of the disease.
WAS AN “INCEPTION COHORT” ASSEMBLED?
Patients should have been identified at an early and uniform point (inception) in the course of their disease (e.g. onset of symptoms, time of diagnosis or beginning of treatment), so that those who succumbed or completely recovered are included with those whose disease persisted.
- The starting point is called zero time
Descriptions of prognosis should include the full range of manifestations that would be considered important to patients
In most cases, the effect would be to make prognosis appear gloomier than it really is. However, distortion in the opposite direction also can occur
Failure to start a study of clinical course and prognosis with an inception cohort has an unpredictable effect on its results
Failure to assemble a proper inception cohort of patients constitutes a fatal flaw in studies of prognosis.
Several studies of the risk of stone recurrence ask currently symptomatic patients if they have had stones previously, failing to realize that recurrent stone formers (with positive past histories) have multiple chances to be included in such studies, but patients without recurrences (with negative past histories) have only one chance of being included; no wonder recurrence rates vary all over the map. Like Diagnosis, if there is no use of gold standard, the information are not valid. There should be an inception cohort in prognostication. All possible cases are included in the analysis.
WAS THE REFERRAL PATTERN DESCRIBED?
The pathways by which patients entered the study sample should be described.
- Did they come from a primary care center or were they assembled in a tertiary care center?
It is in the assembly of patients that studies of the course and prognosis of disease often flounder
WAS THE REFERRAL PATTERN DESCRIBED? (Different forms of bias)
A major clinical center’s reputation results in part from its particular expertise in a specialized area of clinical medicine, it will be referred problem cases likely to benefit from this expertise (Centripetal bias)
And its experts may preferentially admit and keep track of these cases over other, less challenging or less interesting ones (popularity bias)
The selection that occurs at each stage of the referral process can generate patient samples at tertiary care centers that are much different from those found in the general population (referral filter bias)
Patients differ in their financial and geographic access to the clinical technology that identifies them as eligible for studies of the course and prognosis of disease (diagnostic access bias)
These biases will distort the conclusions of the study
WAS COMPLETE FOLLOW-UP ACHIEVED?
All members of the inception cohort should be accounted for at the end of the follow-up period, and their clinical status should be known.
This is because patients do not disappear from a study for trivial reasons (refuse therapy or recover or die or retire or simply grow tired of being followed.)
Difficult for the authors to achieve perfection, they are bound to lose a few members of their inception cohort
Best case and Worse case approach
WERE OBJECTIVE OUTCOME CRITERIA DEVELOPED AND USED?
The prognostic outcomes should be stated in explicit, objective terms so that you, as the reader of the subsequent report, will be able to relate them to your own practice
These criteria are applied in a consistent manner. An article about the prognosis of patients with transient ischemic attack. If the article describes the risk of “subsequent stroke” without presenting the explicit, objective critieria for what constituted a “stroke”, you are in a quandary. Are these “strokes” limited to severe derangements of sensation or motor power? Or, are the majority of these “strokes” merely transient or trivial changes in sensation or in deep or superficial reflexes? The implications of these different definitions for counseling patients or initiating therapy are whopping
WAS THE OUTCOME ASSESSMENT “BLIND”? The examination for important prognostic outcomes
should have been carried out by clinicians who were “blind” to the other features of these patients.
The clinician who knows that a patient possesses a prognostic factor of presumed importance may carry out more frequent or more detailed searches for the relevant prognostic outcome (diagnostic-suspicion bias)
Pathologists and others who interpret diagnostic specimens can have their judgments dramatically influenced by prior knowledge of the clinical features of the case (expectation bias)
This is essential to avoid the two following biases.

17
WAS ADJUSTMENT FOR EXTRANEOUS PROGNOSTIC FACTORS CARRIED OUT?
Is there mathematical adjustment for extraneous prognostic factors mentioned in the article?
Clinicians may not be familiar “Rules of thumb” to apply to the “predictive model”.
FIRST RULE OF THUMB
If the article concludes that some constellation of symptoms, signs, and laboratory results accurately predicts a certain prognosis, demand evidence that the authors have confirmed the constellation’s predictive power in a second independent sample of patients (the test sample)
The multivariate approaches used will fail to distinguish important prognostic factors from unimportant idiosyncracies of the particular patient sample (the training sample) to which they are applied.
SECOND RULE OF THUMB It has to do with the numbers of patients that should have
been included in the training and test samples. There should at least be 10 patients for every prognostic
factor the authors studied. Increases the number of study subjects
TREATMENT
Clinical question: How does treatment change the course of disease? DECIDING ON THE BEST THERAPY THREE PRINCIPAL DECISIONS THAT DETERMINE THE RATIONAL TREATMENT OF ANY PATIENT
1. IS THE ULTIMATE OBJECTIVE TO ACHIEVE CURE, PALLIATION, SYMPTOMATIC RELIEF, OR WHAT?
2. DOES THE PATIENT REQUIRE ANY TREATMENT AT ALL? WHAT SORTS OF EVIDENCE, FROM WHAT SOURCES, SHOULD DETERMINE THE CHOICE OF THE SPECIFIC TREATMENT TO BE USED TO REACH THIS GOAL
3. HOW WILL YOU KNOW WHEN TO STOP TREATMENT, CHANGE ITS INTENSITY, OR SWITCH TO SOME OTHER TREATMENT?
Example A PATIENT WITH SYMPTOMLESS BUT MODERATELY SEVERE ESSENTIAL HYPERTENSION (FIFTH-PHASE DIASTOLIC BLOOD PRESSURE 110 mm Hg).
1. ULTIMATE OBJECTIVE OF TREATMENT To prevent (further) target organ damage to the brain, eye, heart, kidney, and large vessels that would cause disability or untimely death.
2. CHOICE OF SPECIFIC TREATMENT On the basis of randomized clinical trials of active agents versus placebo, antihypertensive drugs
3. TREATMENT TARGET A fifth-phase diastolic blood pressure of less than 90 mm Hg, or as close to that as tolerable in the face of drug side effects.
SIX OBJECTIVES OF TREATMENT
1. Cure (e.g. kill the microbe, cut out the tumor, desensitize the phobic patient)
2. Prevent a recurrence (e.g. give prophylactic antibiotics following recovery from acute rheumatic fever, or major tranquilizers following discharge for schizophrenia)
3. Limit structural or functional deterioration (e.g. reconstruct, rehabilitate)
4. Prevent the later complication (e.g. give diuretics to symptomless hypertensives and aspirin to threatened strokes).
5. Relieve the current distress (e.g. replace the hormone, provide emotional support or counseling, give painkillers, anti-depressants and anti-inflammatory drugs)
6. Deliver reassurance (e.g. “un-label” the misdiagnosed, transmit the truly favorable prognosis)
Allow to die with comfort and dignity (e.g. cancel further diagnostic testing and focus on the relief of current symptoms and the preservation of self-esteem). E.g. Post menopausal women replace hormones.
THREE ELEMENTS OF A SICKNESS
1. THE DISEASE OR TARGET DISORDER THE ANATOMIC, BIOCHEMICAL, PHYSIOLOGIC, OR PSYCHOLOGIC DERANGEMENT
2. THE ILLNESS THE SIGNS, SYMPTOMS, AND BEHAVIORS EXHIBITED BY THE PATIENT AS A RESULT OF, AND RESPONDING TO, THE TARGET DISORDER
3. THE PREDICAMENT THE SOCIAL, PSYCHOLOGICAL, AND ECONOMIC FASHION IN WHICH THE PATIENT IS SITUATED IN THE ENVIRONMENT
Need to know exactly what is being treated - Its prognosis when treated and untreated - Its risk of relapse and recurrence - Its permanent disabilities - Its ultimate outcomes
Need for the correct and accurate assessment of illness as this is the key to setting treatment objectives (symptomatic relief)
Need to assess the patient’s predicament in order to identify the limits of one’s treatment options
SELECTING THE SPECIFIC TREATMENT The first element of selecting the specific treatment is to decide first whether any treatment is required. Modern manufacturers have introduced exotic machines that can select, punch, drill, bend, fit, and weld raw materials into finished goods all by themselves, they sharpen their own tools when they become dull, replace bits of themselves when they wear out, and even sense and correct their own mistakes. One problem they have not been able to overcome, however, is the almost irresistable temptation they present to their human attendants to adjust, reset, and otherwise tinker with them, even when they are functioning fine. The results are often disastrous. In desperation, some plant managers have installed prominent notices along their automated assembly lines: IF IT AIN’T BROKE, DON’T FIX IT! There are two circumstances in which patients “ain’t broke” and ought not attempt to “fix” them
1. False-positive diagnostic errors that label patients as diseased.
2. When either the treatment is worse than the disease or when their illness is trivial, self-limited, or well within the recuperative and reparative powers of the patient’s body and mind
DR. CLIFTON MEADOR NICELY SUMMARIZED THESE “NON-DISEASES”
MIMICKING SYNDROMES (round-faced fat women with hairy upper lips but normal steroids have non-Cushing’s disease)
UPPER-LOWER LIMIT SYNDROMES (borderline laboratory values)
NORMAL VARIATION SYNDROMES (Short children of short parents have non-dwarfism)
LABORATORY ERROR SYNDROMES
ROENTGENOLOGIC-OVERINTERPRETATION SYNDROMES
CONGENITALLY ABSENT-ORGAN SYNDROMES (“Non-functioning” kidneys and gall bladders that are not there)
OVERINTERPRETATION-OF-PHYSICAL FINDINGS SYNDROMES

18
Conditions among patients who “ain’t broke, so don’t fix them” 1. Adie’s pupil 2. Café au lait spots 3. Campbell de Morgan spots 4. Non-dwarfism 5. Pregnancy 6. Pityriasis rosea 7. Silent gallstones 8. Ptosis of the kidney (in normotensive) 9. “Letter-reversal” in a 4-year old 10. Umbilical hernia in infancy 11. Symptomless hypotension 12. Symptomless hiatus hernia 13. Symptomless hyperuricemia 14. Symptomless colonic diverticulae 15. Small degrees of stable scoliosis 16. Non-Cushing’s disease 17. Symptomless hypokalemia in thiazide-treated
hypertensives who are not taking digitalis THREE WAYS OF PICKING UP THERAPY
1. YOUR OWN UNCONTROLLED CLINICAL EXPERIENCE (INDUCTION METHOD)
2. FORMAL RANDOMIZED CLINICAL TRIALS (DEDUCTION METHOD)
3. RECOMMENDATIONS OF OTHERS (ABDICATION OR SEDUCTION METHOD)
SELECTING SPECIFIC TREATMENT
THE HYPOTHETICO-DEDUCTIVE METHOD IS PREFERRED FOR SELECTING SPECIFIC TREATMENTS
THE BEST INFORMATION ON WHETHER A GIVEN TREATMENT DOES MORE GOOD THAN HARM TO PATIENTS WITH A GIVEN DISORDER IS THE
RESULTS OF A RANDOMIZED CLINICAL TRIAL SIX GUIDES TO DISTINGUISH USEFUL FROM USELESS OR EVEN HARMFUL THERAPY
1. Was the assignment of patients to treatments really randomized?
2. Were all clinically relevant outcomes reported? 3. Were the study patients recognizably similar to your own? 4. Were both clinical and statistical significance considered? 5. Is the therapeutic maneuver feasible in your practice? 6. Were all the patients who entered the study accounted for
at its conclusion
- Guides 1 & 6 deal mostly with validity (Are the article’s conclusions true?)
- Guides 2, 3, & 5 deal mostly with applicability (Are the article’s conclusions relevant to your own patients?)
- Guide 4 deals with both validity (statistical significance) and applicability (clinical significance)
WERE THE STUDY PATIENTS RECOGNIZABLY SIMILAR TO YOUR OWN?
The clinical and socio-demographic status of study patients must be described in sufficient detail
The study patients should be at least roughly similar to patients in your practice.
WERE BOTH CLINICAL AND STATISTICAL SIGNIFICANCE CONSIDERED ?
CLINICAL SIGNIFICANCE - refers to the importance of a difference in clinical
outcomes between treated and control patients. - usually described in terms of the magnitude of a
result. STATISTICAL SIGNIFICANCE
- tells us whether the conclusions the authors have drawn are likely to be true (regardless of whether or not they are clinically important).
If the difference is statistically significant, is it clinically significant as well ?
If the difference is not statistically significant, was the trial big enough to show a clinically important difference if it had occurred ?
“CLINICAL SIGNIFICANCE” GOES BEYOND ARITHMETIC AND IS DETERMINED BY CLINICAL JUDGMENT.
If the difference of study variables being considered is small, there is a need to have a larger sample size. Vice versa.
An article that reports on a randomized double-blind clinical trial comparing a new drug (Drug A) with an identical appearing placebo (Drug B) for the control of an important clinical disorder.
Based on the results, the authors of the article will have drawn one of two conclusions: either Drug A is better than Drug B or Drug A is no better than Drug B.
Alpha and Beta is balanced. Alternate hypotheses were used. Ho is true and Ho is false
The relationships between Type I and Type II errors are used in both planning and interpreting randomized trials.
In planning such a trial, investigators can decide beforehand just how great a risk they are willing to run of drawing erroneous conclusions of both sorts
Most authors decide to set the false-positive () risk at .05
and the false-negative () risk at .20 – conventional levels of statistical significance.
In other clinical situations, esp. in the growing number of cases in which clinicians want to find out whether a new treatment is not better than, but as good as; a standard treatment of higher toxicity or cost, the false-negative risk may be set lower.

19
IF THE DIFFERENCE IS STATISTICALLY SIGNIFICANT, IS IT CLINICALLY SIGNIFICANT AS WELL?
One of the landmark U.S. Veterans Administration trials of whether treating hypertension would prevent fatal and nonfatal target organ damage.
In this trial, patients with and without prior target organ damage (to the heart, brain, eye, kidney, or major vessels) at entry were randomized to receive either active anti-hypertensive drugs or identical appearing placebos, and the clinical course were observed over the next 3 years for the subset of men who entered before the age of 50 with diastolic blood pressures between 90 and 114
YARDSTICK FOR Relative Risk Reduction (RRR)
- Relative risk reductions of 50% almost
- always, and of 25% often, are - considered to be clinically significant. - A quick and useful measure of clinical - significance.
For easy interpretation of absolute risk reduction, we take
the reciprocal of it. The reciprocal of the absolute risk reduction is the number
of patients we need to treat in order to prevent one complication of their disease
This measure of clinical significance is called the number needed to treat (NNT)
If the baseline risk without treatment is high, you stil have to treat. The higher the RRReduction, If the baseline is already high, no a mount of Rrreduction can make a difference in the MMT. If it is low, then there is a huge dfference. Example for tumors, the baselin risk is high, so you stil have to remove. Despite that.
Conclusions: When the absolute baseline risk of the bad clinical
outcome is high, even modest relative risk reductions generate gratifyingly small NNT.
Small changes in the absolute baseline risk of a rare clinical event lead to big changes in the numbers of patients we need to treat in order to prevent one.
IF THE DIFFERENCE IS NOT STATISTICALLY SIGNIFICANT, WAS THE TRIAL BIG ENOUGH TO SHOW A CLINICALLY IMPORTANT DIFFERENCE IF IT HAD OCCURRED? Sample case
When Hill and his colleagues performed their randomized trial of home-versus-hospital care for patients with suspected myocardial infarction (in the days before thrombolytic therapy), they observed a 6-week case- fatality rate of 20% among the 132 patients who were randomized to be treated at home. This rate was not statistically significantly different from the 6-week case- fatality rate of 18% they documented among the other 132 patients who were randomized to treatment in hospital
Can we conclude that it was safe in those days to treat such coronary patients at home ?
Was this trial big enough to show a clinically significant difference (say a 25% or 50% better among hospitalized coronaries) if it did occur ?

20
IF THE DIFFERENCE IS NOT STATISTICALLY SIGNIFICANT, WAS THE TRIAL BIG ENOUGH TO SHOW A CLINICALLY IMPORTANT DIFFERENCE IF IT HAD OCCURRED?
The trial needed 261 patients per group to be confident that it had not missed a risk reduction of 25% in the 6-week case-fatality rate of coronary patients treated in hospital
The trial needed 45 patients per group (50%) The trial was too small to reject a 25% improvement, but
large enough to reject a 50% improvement in the 6-week case-fatality rates of coronary patients treated in hospital
95% CONFIDENCE INTERVAL OR CONFIDENCE LIMIT ON RISK REDUCTION, NNT OR OTHER MEASURE OF EFFICACY
C
E
EE
C
CCEC
p
n
pp
n
pppp
)1()1(96.1)(
This is a Swedish Co-operative Stroke Study carried out to determine whether patients with cerebral infarcts might have fewer subsequent strokes if they took aspirin. Placebos were given to 252 controls patients (nC), and 18 of these (pC = 18 / 252 = .07) had a subsequent nonfatal stroke. Aspirin was given to 253 experimental patients (nE), of whom 23 (pE = 23 / 253 = .09) had a recurrent nonfatal stroke. The results certainly did not favor aspirin. There was an absolute increase of .02 between the two groups, generating a relative risk increase (rather than reduction) of 29%.
The result appears quite definitive in terms of excluding
any possible benefit from aspirin
Based on confidence interval analysis - (- .02 - .05 =) - .07, generating a relative risk
increase of recurrent stroke from aspirin of (- .07 / .07 =) – 100%, support the prior suspicion that aspirin cannot be beneficial in this situation.
- (-.02 + .05 =) + .03, generating a relative risk reduction of recurrent stroke from aspirin of (.03 / .07 =) + 43%
- If we believe that a risk reduction of 30% or more would be clinically significant, we cannot regard the Swedish study as definitively excluding a benefit of aspirin.
In summary, when an article draws a negative conclusion about a
treatment (because P .05), you can focus on the upper end of the confidence interval for the relative risk reduction, for this place the treatment in the most favorable light. If this upper boundary lies below what you’d consider to be the smallest clinically significant risk reduction, you are reading about a definitively negative trial. If, on the otherhand, this upper end of the confidence interval includes clinically important relative risk reductions, the trial hasn’t ruled them out and cannot be regarded as definitively negative. IS THE THERAPEUTIC MANEUVER FEASIBLE IN YOUR PRACTICE
The therapeutic maneuver has to be described in sufficient detail for readers to replicate it with precision.
Must be clinically sensible Must be available Must note whether the authors avoid two specific biases
in its application Contamination (in which control patients accidentally
receive the experimental treatment Cointervention ( the performance of additional diagnostic
or therapeutic acts on experimental but not the control patients)
WERE ALL PATIENTS WHO ENTERED THE STUDY ACCOUNTED FOR AT ITS CONCLUSION What can a reader do when outcomes are not reported for missing subjects ?
Best case/worse case approach - Arbitrarily assign a bad outcome to all missing
members of the group which fared better, and good outcome to all missing members of the group that fared worse.
- If this maneuver fails to cancel the statistical or clinical significance of the results, the reader can accept the study’s conclusions
Example A cohort of 123 morbidly obese patients was studied 19 – 47 months after surgery. Success was defined as having lost more than 30% of excess weight. Only 103 patients (84%) could be located. In these, the success rate of surgery was 60/103 (58%) Solution
Best case success rate = (60 + 20) / 123 = 65% Worse case success rate = 60 / 123 = 49% Thus the true rate must have been 49 and 65% Interval is bigger if many lost to follow up and vice versa
TREATMENT (cont’d) Clinical question: How does treatment change the course of disease?
Usually the effects of treatment are much less obvious and most interventions require research to establish their value
Specific interventions must do more good than harm among patients who use them (efficacious and effective)
The most desirable method for measuring efficacy and effectiveness is that of the randomized controlled trial
Efficacious treatment is one that has the desired effects among those who receive it. Effective if it does more good than harm in those to whom it is offered.
Intervention studies
Clinical trials Controlled trials Uncontrolled trials Concurrent control
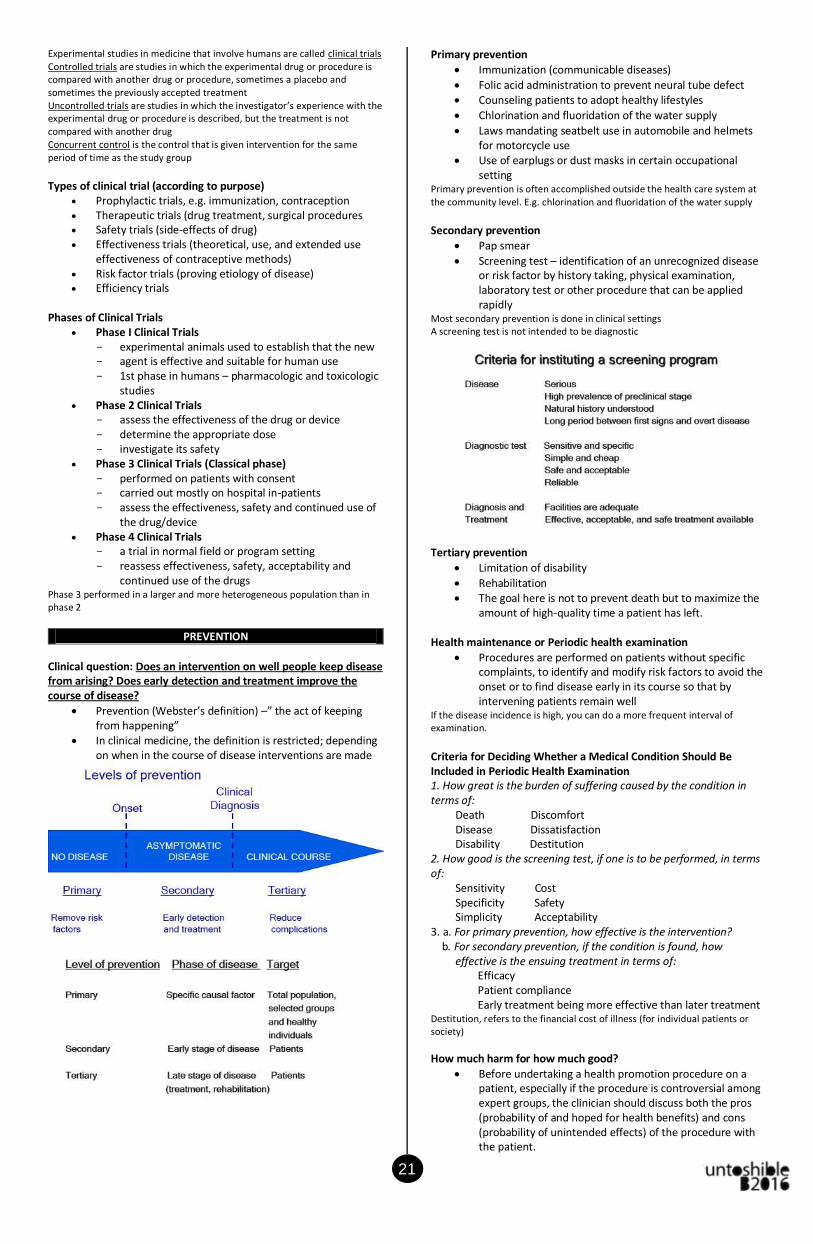
21
Experimental studies in medicine that involve humans are called clinical trials Controlled trials are studies in which the experimental drug or procedure is compared with another drug or procedure, sometimes a placebo and sometimes the previously accepted treatment Uncontrolled trials are studies in which the investigator’s experience with the experimental drug or procedure is described, but the treatment is not compared with another drug Concurrent control is the control that is given intervention for the same period of time as the study group
Types of clinical trial (according to purpose)
Prophylactic trials, e.g. immunization, contraception Therapeutic trials (drug treatment, surgical procedures Safety trials (side-effects of drug) Effectiveness trials (theoretical, use, and extended use
effectiveness of contraceptive methods) Risk factor trials (proving etiology of disease) Efficiency trials
Phases of Clinical Trials
Phase I Clinical Trials - experimental animals used to establish that the new - agent is effective and suitable for human use - 1st phase in humans – pharmacologic and toxicologic
studies Phase 2 Clinical Trials
- assess the effectiveness of the drug or device - determine the appropriate dose - investigate its safety
Phase 3 Clinical Trials (Classical phase) - performed on patients with consent - carried out mostly on hospital in-patients - assess the effectiveness, safety and continued use of
the drug/device Phase 4 Clinical Trials
- a trial in normal field or program setting - reassess effectiveness, safety, acceptability and
continued use of the drugs Phase 3 performed in a larger and more heterogeneous population than in phase 2
PREVENTION
Clinical question: Does an intervention on well people keep disease from arising? Does early detection and treatment improve the course of disease?
Prevention (Webster’s definition) –” the act of keeping from happening”
In clinical medicine, the definition is restricted; depending on when in the course of disease interventions are made
Primary prevention
Immunization (communicable diseases)
Folic acid administration to prevent neural tube defect Counseling patients to adopt healthy lifestyles
Chlorination and fluoridation of the water supply
Laws mandating seatbelt use in automobile and helmets for motorcycle use
Use of earplugs or dust masks in certain occupational setting
Primary prevention is often accomplished outside the health care system at the community level. E.g. chlorination and fluoridation of the water supply
Secondary prevention
Pap smear
Screening test – identification of an unrecognized disease or risk factor by history taking, physical examination, laboratory test or other procedure that can be applied rapidly
Most secondary prevention is done in clinical settings A screening test is not intended to be diagnostic
Tertiary prevention
Limitation of disability
Rehabilitation The goal here is not to prevent death but to maximize the
amount of high-quality time a patient has left. Health maintenance or Periodic health examination
Procedures are performed on patients without specific complaints, to identify and modify risk factors to avoid the onset or to find disease early in its course so that by intervening patients remain well
If the disease incidence is high, you can do a more frequent interval of examination.
Criteria for Deciding Whether a Medical Condition Should Be Included in Periodic Health Examination 1. How great is the burden of suffering caused by the condition in terms of: Death Discomfort Disease Dissatisfaction Disability Destitution 2. How good is the screening test, if one is to be performed, in terms of: Sensitivity Cost Specificity Safety Simplicity Acceptability 3. a. For primary prevention, how effective is the intervention? b. For secondary prevention, if the condition is found, how effective is the ensuing treatment in terms of: Efficacy Patient compliance Early treatment being more effective than later treatment Destitution, refers to the financial cost of illness (for individual patients or society)
How much harm for how much good?
Before undertaking a health promotion procedure on a patient, especially if the procedure is controversial among expert groups, the clinician should discuss both the pros (probability of and hoped for health benefits) and cons (probability of unintended effects) of the procedure with the patient.

22
APPENDIX
Origin
Over 2,000 years ago, Hippocrates “environmental factors can influence the occurrence of disease”
In the early 19th century, the distribution of disease in
specific human population groups was measured
“Miasma” dirty cloud Most likely a water contamination of the diseases
ACHIEVEMENTS IN EPIDEMIOLOGY
Eradication of Smallpox Identification of methyl mercury – “Minamata Disease” Identification of factors causing Rheumatic fever and
Rheumatic heart disease Iodine deficiency disease AIDS, SARS
PROGNOSIS
Survival curve 1. Actuarial or life table analysis
(Cutler-Ederer method) 2. Kaplan-Meier curve
Source: Dr. Chan’s PPT