
Applications of Robotic Surgery- Gynecology Tommaso Falcone, M.D. Professor & Chair Department of...
77
Applications of Robotic Surgery-Gynecology Tommaso Falcone, M.D. Professor & Chair Department of Obstetrics & Gynecology
-
Upload
shonda-lloyd -
Category
Documents
-
view
216 -
download
0
Transcript of Applications of Robotic Surgery- Gynecology Tommaso Falcone, M.D. Professor & Chair Department of...

Applications of Robotic Surgery-GynecologyTommaso Falcone, M.D.Professor & ChairDepartment of Obstetrics & Gynecology

Financial Disclosure
I receive no grants/ honoraria / or other financial support from any robotics company

LEARNING OBJECTIVESAt the conclusion of this presentation, the
participant should be able to:Describe the current robotic system that is commercially available and describe the safe strategy for deploymentReview the limitations and advantages of using a robot for a surgical procedureAssess the current clinical data in gynecology for the use of the robotPredict potential future applications of robotics when newer prototypes become available

Robots
Active robots (autonomous)System completes a preprogrammed task with minimal human supervision
Passive robotsComputer-assisted surgery

Cyberknife

Cyberknife

Cyberknife

Navigational devices
Determine the surgical pathComplex technologyRobust and reliable

Target Guidance

Computer-assisted surgical planning
Contrast-enhanced CT or MRI data to reconstruct a model (Fusion technology)Ex. veins and arteries around a tumor


Robot: Surgical Assistant
Laparoscope holderAutomated Endoscopic System for Optimal Positioning (AESOP) 1994Voice activation

Robotics & Medicine-Cleveland Clinic
Neurosurgery (Navigational)General Surgery (Morbid Obesity surgery)
NOT USED AT ALL
Urology ( Radical Prostatectomy)Cardiac surgery ( Coronary bypass surgery & mitral valve surgery)Gynecology
Robot hardwareSurgical Cart
Three-Four robotic arms: one holds the laparoscope; three robotic arms are instrument holders or tissue retractors
Console for the surgeonTwo handles that controls the robot arms


Robot advantages
3 D view of the operative fieldManipulation of the robotic handles is transmitted to a computer that filters, scales and then translates the surgeon’s movements to the robotic arms

Advantages of robotic assistance
Increases dexterityScales surgeon’s movementsFilters natural tremor

Advantages of robotic assistance
Movement can be scaledExample: scaling ratio of 10:1 means that for every 1 cm the surgeon moves the handles at the console, the robotic instruments move 1 mm

Motion scaling:2:1 to 5:12:1 to 5:1
5 cm 1 cm

EndoWristTM Instrumentation
Modeled after the human wrist. Full range of motion
High-strength cable system
Transpose fingers to instrument tips

7 Degrees of freedom instruments

Robotics & Gynecology
Laparoscopic microsuturingMajor challengePrinciple is different from conventional microsurgeryOptically magnified tremorLong operating times results in fatigue for the surgeon & laparoscope holder

First gynecologic procedure: Tubal Reversal using Robotic (Zeus) Assistance
10 mm laparoscopeThree 5 mm portsTwo ends were prepared conventionally6-0 polygalactin for the mesosalpinxTwo layered closure with 8-0 polygalactin7 stitches per side


Results: Fertility & Sterility 2000;73:1040-2
Safe, no injuries occurredEBL 70 mLPatency in all tubes anastomosedHSG 6 weeks post-op 17/19 tubes still patent5/10 patients after follow-up time of 12 months


The da Vinci™ Surgical System


Patient side surgical cartPatient side surgical cart


da Vinci 4th Arm-previous da Vinci 4th Arm-previous modelmodel












Limitations
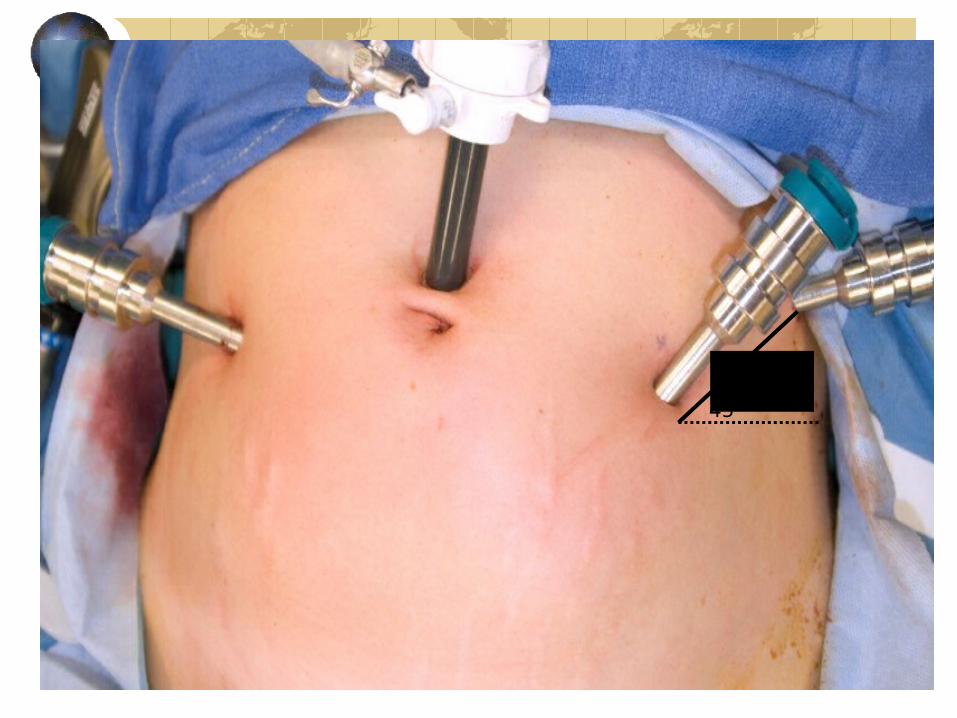
Requires trainingMost important learning step is port placement
Especially if using the fourth arm
Angle of access may be difficultNeed to adjust the port placementIf convert to traditional laparoscopy ports may be inappropriate

Da Vinci: Limitations
Hard to access the abdomen for accessory portsAssistants have difficulty moving aroundDisengage the system if changing patient position


Laparoscopic Tubal Anastomosis without robotic assistance
Goldberg & Falcone Hum Reprod (2003;)No robot: Procedure time: 190 minutes
– LOS:222 minutes
Zeus robot: Procedure time:284 minutes– LOS:198 minutes
Da Vinci ( Degueldre et al Fertil Steril 2000): Procedure time:181 minutes

Comparative Trial
Compared Robot assisted laparoscopic Tubal reversal surgery with outpatient “mini-laparotomy” using traditional microsurgery techniques (published
Obstetrics & Gynecology 2007)No difference in pregnancy rates or ectopic pregnancy ratesMain differences:
OR time longer with robotReturn to work time shorter with the robot

Robotic(N=26)
Laparotomy(N=41)
P Value
EBL <100cc 19 (73%) 31 (80%) 0.48
Surgical time (min.) 226 ± 45 186 ± 49 0.001
Anesthesia time (min.) 279 ± 42 209 ± 51 <0.001
Hospitalization (min.) 274 ± 412 381 ± 478 0.14
Costs (difference in median values)
$1446 greater for Robotic95% CI: ($1112 , $1812)
<0.001
Weeks to go back to work 1.5 ± 1.3 2.5 ± 1.5 0.013

Myomectomy
Closure of the uterine defect critical to prevent rupture during laborAdvincula et al ( University of Michigan) JAAGL 2004-35 casesThe mean weight of leiomyomata removed was 223 grams; mean number 1.6; mean diameter 7.9 cmThe mean operative time was 230+ 83 minutes.

Myomectomy
Conversion to laparotomy-3Pneumonia-1Port site infection-1Cardiogenic shock (from vasopressin)-1Length of stay-median=1 day (0-5 days)

Robot versus Laparotomy
Advincula et al 2007N=58 (29 in each group)2 conversionsUterine weight: robot (227+247g) and laparotomy (223+228 g )OR time: Robot (231+85 minutes) and laparotomy (154+43 minutes)LOS: robot (1.5 days) and laparotomy (3.6 days)

Technical considerationsUterine manipulator8-10 cm between the endoscope and the top of the elevated uterusAccurate myoma “mapping”
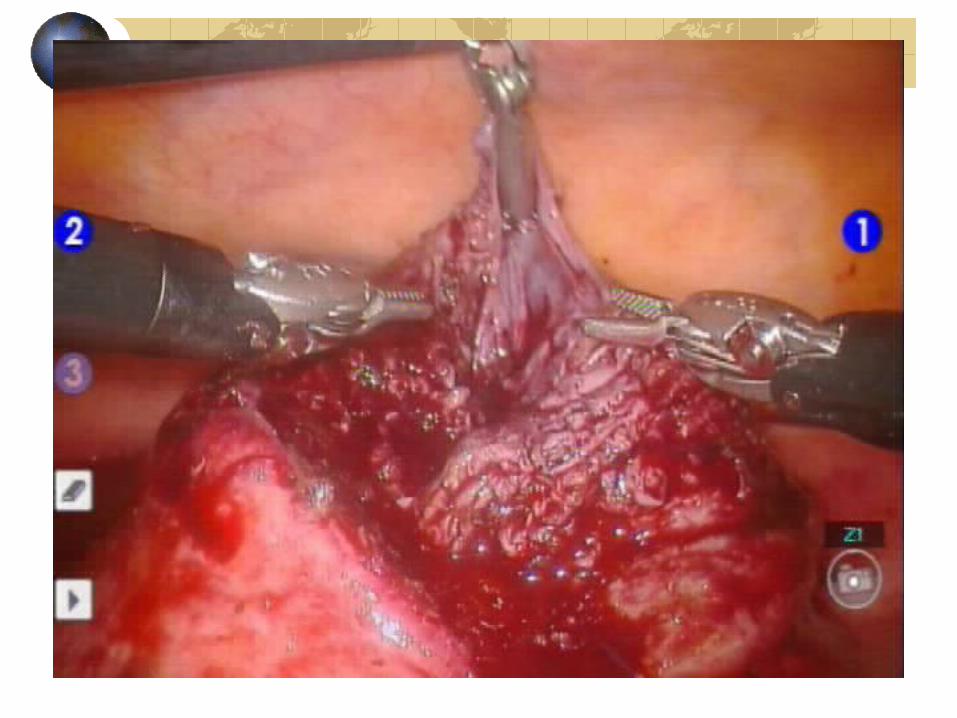
No tactile feedback
Keep your instruments in viewYou may have 2 energy sources at one time
Use your wrist often


15°
10 cm
45°
8-10 cm
Hysterectomy video




Robot-assisted laparoscopic hysterectomy
7 case series reported 2002-2007Total-94 patients in 6 case series & 91 cases in 1 ( Mayo clinic-Arizona)Age-median 38-55BMI-26-28Indications-Mostly non-malignant conditions (uterine weights-30-327 g)

Robot-assisted laparoscopic hysterectomy: Operative Time
1. 270-600 minutes2. 148-277 minutes3. 170-368 minutes (Median=254 min)4. 43-315 minutes (Median=185 min)5. 170-432 min ( Median= 242 minutes )6. 110-290 min (Median= 192 minutes )

Robot-assisted laparoscopic hysterectomy
Hospital stay-US study=1-2 daysFrench study=8 days

Robot-assisted laparoscopic hysterectomy: Operative Time
Mayo Clinic experienceUterine weight 135 g (67)53 % menometrorrhagia or pelvic painSurgery time 127 + 35 minutes



Ochsner Clinic Experience (Baton Rouge, Louisiana)
AAGL-2007 Washington) abstract“Robotic equivalence to laparoscopic skin to skin times was achieved after 75 cases”

Robot-assisted laparoscopic hysterectomy: Complications
Conversion to open surgery- 5 cases12 operative/postoperative
Hemorrhage-3Vaginal cuff/pelvic hematoma-3Cystotomy-1Thermal bowel injury-1Pneumonia/UTI/Venous phlebitis/lymph collection

Robot-assisted cancer procedures
2005-Reynolds et al JSLS 7 patients ( 4 endometrial/2 ovarian/1 tubal cancer)• Mean OR time 257 minutes, median lymph
node count 15/ EBL 50 mL/LOS 2 days
Kim et al Gynecol Oncol 200710 patients-radical hyst 1A2-1B1 cervix• Mean OR time 207 minutes
Robot-assisted cancer procedures
Sert & Abeler Int J Med Robotics & Computer Assisted Surgery 2007
7 patients-robotic (Stage 1A & 1 B cases)• 3 robotic & 2 conventional ports• Mean console time 241 (160-445) minutes• Docking time was 25 minutes
7 patients-laparoscopic• Mean OR time 300 ( 225-375) minutes

Robot-assisted cancer procedures
Boggess JF Am J Obstet Gynecol 2008Robotic versus open radical hysterectomy
Boggess JF Obstet Gynecol 2008Robotic versus conventional laparoscopy for cervix cancer
Boggess JF Obstetr Gynecol 2008Robotic versus conventional laparoscopy for endometrial cancer

Sacrocolpopexy
Suture of a mesh to the vagina and sacral promontoryMultiple interrupted 1.0 Gore-Tex sutures were used to secure the mesh to the vagina and sacral promontory. The average operative time was 3 hours 42 minutes.

Ovarian Transposition:Molpus et al JSLS 2003
Ovarian Transplantation
Autologous transplant to orthotopic site
Small ovarian tissue piecesSutured with 6-0 PDS to ovarian bed

Next phase in computer aided surgery
Tactile & Force feedback (Science of Haptics)Automation of surgical Tasks

Autonomous knot tying ( Bauerschmitt et al Germany)



















