Application of artificial neural networks in the diagnosis of urological dysfunctions
7
Review Application of artificial neural networks in the diagnosis of urological dysfunctions David Gil a, * , Magnus Johnsson b , Juan Manuel Garcia Chamizo a , Antonio Soriano Paya a , Daniel Ruiz Fernandez a a Computing Technology and Data Processing, University of Alicante, Alicante, Spain b Lund University Cognitive Science, Department of Computer Science, Lund University, Lund, Sweden article info Keywords: Artificial neural networks Urology Expert systems in medicine Artificial intelligence Decision support systems abstract In this article, we evaluate the work out of some artificial neural network models as tools for support in the medical diagnosis of urological dysfunctions. We develop two types of unsupervised and one super- vised neural network. This scheme is meant to help the urologists in obtaining a diagnosis for complex multi-variable diseases and to reduce painful and costly medical treatments since neurological dysfunc- tions are difficult to diagnose. The clinical study has been carried out using medical registers of patients with urological dysfunctions. The proposal is able to distinguish and classify between ill and healthy patients. Ó 2008 Elsevier Ltd. All rights reserved. 1. Introduction Currently, urologists have different tools available to obtain urodynamical data. However, it still remains very complicated to make a correct diagnosis: the knowledge concerning the origin of the detected dysfunctions depends mainly on acquired experi- ence and on the research, which is regularly carried out within the field of urology. The specialists in urology are quite often dealing with situations that are poorly described or that are not described in the medical literature. In addition there are too many dysfunctions whose precise diagnoses are complicated. This is a consequence of the interaction with the neurological system and the limited knowledge available on how this operates. For the purpose of diagnosing dysfunctions of the lower urinary tract (LUT) there are several techniques, which entail different de- grees of invasiveness toward the patient (Abrams, 2005). A urolog- ical study of a patient consists of carrying out a variety of costly neurological examination as well as physical tests like flowmetry and cystometry examinations with high degrees of complexity and invasiveness. The medical diagnosis is by nature a complex and fuzzy cognitive process, therefore soft computing methods, such as neural networks, have shown great capacity to be applied in the development of medical decision support systems of dis- eases. This project is intended to aid the specialist in obtaining a reliable diagnosis while decreasing the number of tests. To this objective we propose the use of artificial neural networks (ANNs) since these present good results for classification problems which are either weakly formalized or suffer from quite limited knowl- edge (Begg, Kamruzzaman, & Sarkar, 2006). In that way, major ben- efits will be obtained both for the patient, by avoiding painful tests, and for the medical institutions by avoiding expensive urodynam- ical tests, by increasing the reliability of the diagnoses and reduc- ing waiting lists. Although the use of ANNs in medicine is a rather recent phe- nomenon, there are many applications deployed as in the field of diagnosis, imaging, pharmacology, pathology and prognosis. ANNs have been used in the diagnosis of appendicitis, back pain, dementia, myocardial infraction (Green et al., 2006), psychiatric disorders (Peled, 2005; Politi, Balduzzi, Bussi, & Bellodi, 1999), acute pulmonary embolism (Suzuki, Shiraishi, Abe, MacMahon, & Doi, 2005). In Urology, prostate cancer serves as a good exam- ple for working out with ANNs (Batuello et al., 2001; Remzi et al., 2003; Remzi & Djavan, 2004) but there are no studies related with urological tests. Regarding this subject, our work is more re- lated with the neurological part which is less explored in the uro- logical field (Gil, Soriano, Ruiz, García, & Flórez, 2005; Gil, Soriano, Ruiz, & Montejo, 2006; Gil, Johnsson, Soriano, & Ruiz, 2008; Ruiz, García, Macía, & Soriano, 2005). In this paper we demonstrate that such a complex system for helping to diagnose dysfunctions of the LUT can be implemented by means of ANNs. The remaining part of the paper is organized as follows: first, we give a brief description of the network setting for each ANN. Next we describe the design of our proposal and the training of the ANNs by the available data. Then, we describe the subsequent testing carried out in order to analyze the results. Fi- nally we draw the relevant conclusions. 0957-4174/$ - see front matter Ó 2008 Elsevier Ltd. All rights reserved. doi:10.1016/j.eswa.2008.06.065 * Corresponding author. E-mail address: [email protected] (D. Gil). Expert Systems with Applications 36 (2009) 5754–5760 Contents lists available at ScienceDirect Expert Systems with Applications journal homepage: www.elsevier.com/locate/eswa
Transcript of Application of artificial neural networks in the diagnosis of urological dysfunctions

Expert Systems with Applications 36 (2009) 5754–5760
Contents lists available at ScienceDirect
Expert Systems with Applications
journal homepage: www.elsevier .com/locate /eswa
Review
Application of artificial neural networks in the diagnosis of urological dysfunctions
David Gil a,*, Magnus Johnsson b, Juan Manuel Garcia Chamizo a, Antonio Soriano Paya a,Daniel Ruiz Fernandez a
a Computing Technology and Data Processing, University of Alicante, Alicante, Spainb Lund University Cognitive Science, Department of Computer Science, Lund University, Lund, Sweden
a r t i c l e i n f o a b s t r a c t
Keywords:
Artificial neural networksUrologyExpert systems in medicineArtificial intelligenceDecision support systems0957-4174/$ - see front matter � 2008 Elsevier Ltd. Adoi:10.1016/j.eswa.2008.06.065
* Corresponding author.E-mail address: [email protected] (D. Gil).
In this article, we evaluate the work out of some artificial neural network models as tools for support inthe medical diagnosis of urological dysfunctions. We develop two types of unsupervised and one super-vised neural network. This scheme is meant to help the urologists in obtaining a diagnosis for complexmulti-variable diseases and to reduce painful and costly medical treatments since neurological dysfunc-tions are difficult to diagnose. The clinical study has been carried out using medical registers of patientswith urological dysfunctions. The proposal is able to distinguish and classify between ill and healthypatients.
� 2008 Elsevier Ltd. All rights reserved.
1. Introduction
Currently, urologists have different tools available to obtainurodynamical data. However, it still remains very complicatedto make a correct diagnosis: the knowledge concerning the originof the detected dysfunctions depends mainly on acquired experi-ence and on the research, which is regularly carried out withinthe field of urology. The specialists in urology are quite oftendealing with situations that are poorly described or that arenot described in the medical literature. In addition there aretoo many dysfunctions whose precise diagnoses are complicated.This is a consequence of the interaction with the neurologicalsystem and the limited knowledge available on how thisoperates.
For the purpose of diagnosing dysfunctions of the lower urinarytract (LUT) there are several techniques, which entail different de-grees of invasiveness toward the patient (Abrams, 2005). A urolog-ical study of a patient consists of carrying out a variety of costlyneurological examination as well as physical tests like flowmetryand cystometry examinations with high degrees of complexityand invasiveness. The medical diagnosis is by nature a complexand fuzzy cognitive process, therefore soft computing methods,such as neural networks, have shown great capacity to be appliedin the development of medical decision support systems of dis-eases. This project is intended to aid the specialist in obtaining areliable diagnosis while decreasing the number of tests. To thisobjective we propose the use of artificial neural networks (ANNs)
ll rights reserved.
since these present good results for classification problems whichare either weakly formalized or suffer from quite limited knowl-edge (Begg, Kamruzzaman, & Sarkar, 2006). In that way, major ben-efits will be obtained both for the patient, by avoiding painful tests,and for the medical institutions by avoiding expensive urodynam-ical tests, by increasing the reliability of the diagnoses and reduc-ing waiting lists.
Although the use of ANNs in medicine is a rather recent phe-nomenon, there are many applications deployed as in the field ofdiagnosis, imaging, pharmacology, pathology and prognosis. ANNshave been used in the diagnosis of appendicitis, back pain,dementia, myocardial infraction (Green et al., 2006), psychiatricdisorders (Peled, 2005; Politi, Balduzzi, Bussi, & Bellodi, 1999),acute pulmonary embolism (Suzuki, Shiraishi, Abe, MacMahon,& Doi, 2005). In Urology, prostate cancer serves as a good exam-ple for working out with ANNs (Batuello et al., 2001; Remzi et al.,2003; Remzi & Djavan, 2004) but there are no studies relatedwith urological tests. Regarding this subject, our work is more re-lated with the neurological part which is less explored in the uro-logical field (Gil, Soriano, Ruiz, García, & Flórez, 2005; Gil, Soriano,Ruiz, & Montejo, 2006; Gil, Johnsson, Soriano, & Ruiz, 2008; Ruiz,García, Macía, & Soriano, 2005).
In this paper we demonstrate that such a complex system forhelping to diagnose dysfunctions of the LUT can be implementedby means of ANNs. The remaining part of the paper is organizedas follows: first, we give a brief description of the network settingfor each ANN. Next we describe the design of our proposal and thetraining of the ANNs by the available data. Then, we describe thesubsequent testing carried out in order to analyze the results. Fi-nally we draw the relevant conclusions.

D. Gil et al. / Expert Systems with Applications 36 (2009) 5754–5760 5755
2. Neural network architectures
In the last few years the development of techniques of artificialintelligence (AI) applied to numerous industrial fields has achievedsignificant improvements. Medicine and the diagnosis of diseasesare not an exception. Thus, there are several candidate methodsto be used as decision support systems (DSS) for medical diagnosis.However, we decided to apply ANNs instead of others because theknowledge of the architecture, setup parameters and more techni-cal details is above and far more thorough with ANNs than the oth-ers. Moreover, they can be trained with appropriate data learningin order to improve their knowledge of the system. Consequently,they will achieve a higher level of generalization for the diagnosisin a similar way that the physician reaches a diagnosis by using hisexperience. ANNs are more suitable for medical diagnosis if theyare compared with other techniques or other (more classical) ap-proaches such as rule based systems or systems based on probabi-listic methods. One of the main disadvantages of ANNs is that theytrend toward overfitting and this situation will be avoided by usingthe cross validation method to determine when to stop the trainingof the ANN. Therefore, in medical diagnosis, we use the advantagesof ANNs, which are considered as a method of disease classifica-tion. This classification has two meanings. We can have a set ofregisters, vectors or data with the aim of establishing the existenceof classes or clusters. In contrast, we can know with certainty thatthere exist some classes, and the aim is to establish a rule able toclassify a new register into one of these classes. The first type isknown as Unsupervised Learning (or Clustering) and the secondone is known as Supervised Learning.
In this section, we will describe the architecture of three differ-ent ANNs, two unsupervised and one supervised. The goal is to ob-tain a system that supports the diagnoses of dysfunctions of theLUT. The classification in maps of the unsupervised ANNs and theoutput from the supervised ANN will be of assistance to the urolo-gist in their medical decisions.
2.1. Unsupervised ANN – Kohonen’s self-organizing maps
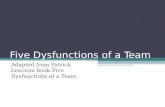
Kohonen’s self-organizing maps (SOM) are composed of neu-rons located in a two-dimensional matrix (Kohonen, 1988, 1990,2001). There is a reference vector, mi = (mi1, . . . ,min) associated withevery neuron in the SOM, where n is the dimension of the inputvectors. In our case they are the n fields of each observation of apattern or a patient in the register. The SOM is used as a classifierand is organized as indicated in Fig. 1.
In the fully trained network each neuron is associated with avector in the input space. The SOM is a soft competitive neural net-
Input Vector{x1...xn}
Reference Vector{mi1...min}
Fig. 1. The Kohonen SOM.
work, which means the winner neuron, i.e. the neuron with the ref-erence vector that is closest to the current input vector accordingto some measure (dot product in our implementation), gets its ref-erence vector updated so that it becomes more similar to the inputvector. The neurons in the vicinity of the winner neuron also gettheir reference vectors updated but to a lesser extent. Usually aGaussian function of the distance to the winner neuron is used tomodify the updating of the reference vectors. The trained SOM isa projection of the input space, which preserves the topologicalrelationships of the input space. The training of the SOM worksas follows.
At time step t an input signal x 2 Rn activates a winner node c forwhich the following is valid:
xTðtÞmcðtÞP xTðtÞmiðtÞ 8i: ð1Þ
The weights are updated according to
miðt þ 1Þ ¼½miðtÞ þ aðtÞxðtÞ�=kmiðtÞ þ aðtÞxðtÞk if i 2 NcðtÞmiðtÞ if i R NcðtÞ
�
ð2Þ
where Nc(t) is the neighbourhood of the node c at time t and0 < a(t) <1.
The training parameters employed in the architecture areshowed in Table 1.
2.2. Unsupervised ANN – growing cell structures
It has been pointed out that the predefined structure and size ofKohonen’s SOM bring limitations to the resulting mapping. One at-tempt to solve this problem is the growing cell structures (Fritzke,1993a, 1997), which have a flexible and compact structure, a var-iable number of elements and a k-dimensional topology where kcan be arbitrarily chosen.
By definition, the adaptation of a reference vector in the grow-ing cell structures (GCS) is done as described in the previous sec-tion (SOM), i.e. determine the best matching unit, adjust itsreference vector and the reference vectors of its topological neigh-bours. However, there are two important differences when com-pared to Kohonen’s model, namely that the adaptation strengthis constant over time, and that only the best matching unit andits direct topological units are adapted.
The probability density function P(x) of the input space is notexplicitly known, but with a local signal counter it is possible toestimate it by the relative frequency of input signals gathered byeach unit. In the end, all units should have the same relative fre-quency. Therefore, a high value of the local signal counter indicatesa good position to insert a new unit, since then the new unit willprobably reduce this high value to some extent.
Simulations have indicated (Fritzke, 1993a) that under a widerange of parameter settings the model will approach a state wherethe probabilities that each unit is the best matching unit for thenext input signal x is approximately equal. Therefore, accordingto Fritzke (Fritzke, 1993a, 1993b) the growing cell structures esti-mate the unknown probability distribution significantly betterthan Kohonen’s feature map. Other advantages are that the param-eters are constant over time, and the size of the network can be
Table 1SOM training parameters
Parameters Value
Learning rate 0.02Neighbourhood distance 1Epochs 1000

5756 D. Gil et al. / Expert Systems with Applications 36 (2009) 5754–5760
automatically determined, i.e. the algorithm stops when a certainperformance criterion is met.
It is worth mentioning that already early in simulations withthe growing cell structures, the network has reached its finalshape, only with fewer units. This behaviour can be described as‘‘fractal growth”. An important implication of this is that the pro-cess can be stopped whenever and there will anyway be a well-shaped structure.
The growing cell structures algorithm is rather similar to theGrowing Gas algorithm (Fritzke, 1995). The main difference is thatthe network topology is constrained to only k-dimensional sim-plexes. The basic building block and also the initial configurationof every network is a k-dimensional simplex. Such a simplex isfor k = 1 a line, for k = 2 a triangle, and for k = 3 a tetrahedron.
For a given network configuration a number of adaptation stepsare used in order to update the reference vectors for the neurons,and to gather local error information at each neuron. This errorinformation is used to decide where new neurons will be inserted.
In some cases, especially when P(x) consists of several separateregions of positive probability density, an even better modellingcan be obtained by removing superfluous units. A unit can be con-sidered superfluous if it has a position, i.e. has a reference vector, ina region of the input space with very low probability density. Gen-erally, P(x) is unknown, but the relative signal frequency of a unitcan be related to the size of its receptive field (Voronoid field) toobtain a local estimation. The training parameters employed inthe GCS’s architecture are showed in Table 2. The training of theGCS works as follows.
The network is initialized to contain k + 1 neurons with refer-ence vectors mi 2 Rn randomly chosen. The neurons are connectedso that a k-dimensional simplex is formed. In our experiment thedimensionality k = 2, but it can be set to any integer value greaterthan 0.
At time step t an input signal x 2 Rn activates a winner node c forwhich the following is valid:
kx�mck < kx�mik 8i; ð3Þ
and the squared distance between the input signal and the winner cis added to a local error variable Ec:
DEc ¼ kx�mck2: ð4Þ
The reference vectors are updated by fractions eb and en, respec-tively according to
Dmc ¼ ebðx�mcÞ; ð5ÞDmi ¼ enðx�miÞ8i 2 Nc; ð6Þ
where Nc is the set of direct topological neighbours of c.A neuron is inserted if the number of input signals that have
been generated so far is an integer multiple of a parameter k. Thisis done by dividing the longest edge between the neuron q with thelargest accumulated error and its connected neighbour f, and thenremoving the earlier connection (q, f) and connect r to all neigh-bours that are common for q and f. The reference vector for r isinterpolated from the reference vectors for q and f:
Table 2GCS training parameters
Parameters Value
k 2eb 0.1en 0.03k 19a 0.5b 0.3
mr ¼ ðmq þmf Þ=2: ð7Þ
The error variables for all neighbours to r are decreased by a fractiona that depends on the number of neighbours of r:
DEi ¼ ð�a=jNr jÞ � Ei; ð8i 2 NrÞ: ð8Þ
The error variable for r is set to the average of its neighbours:
Er ¼ ð1=jNrjÞ �Xi2Nr
Ei; ð9Þ
and then the error variables of all neurons are decreased:
DEi ¼ �bEi 8i: ð10Þ
2.3. Supervised ANN – multilayer perceptron
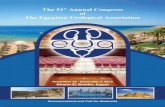
A typical Multilayer Perceptron (MLP) network consists of threelayers of neurons: an input layer that receives external inputs, onehidden layer, and an output layer which generates the classifica-tion results (Bishop, 1995; Hand, 1997; Haykin, 1998; Ripley,1996) as it is showed in the Fig. 2. Note that unlike other layers,no computation is involved in the input layer. The principle ofthe network is that when data are presented at the input layer,the network neurons run calculations in the consecutive layers un-til an output value is obtained at each of the output neurons. Thisoutput will indicate the appropriate class for the input data.
The architecture of the MLP consists of layer 1, with the inputsthat correspond to the input vector, the layer 2, with the hiddenlayer and the layer 3 which is the output (healthy or illness).
The learning used is backpropagation algorithm with the adap-tive learning rate, the momentum constant and an optimized algo-rithm based on the gradients method (the backpropagationtraining parameters are showed in Table 3). This improved learningalgorithm runs as follows.
All the reference vectors m are initialized with small randomvalues from a pseudorandom sequence generator. Then (i.e. whenthe error E is below a preset value) the three basic steps are re-peated until to converge:
� The reference vectors mi are updated by
mðt þ 1Þ ¼ mðtÞ þ DmðtÞ; ð11Þ
� where
DmðtÞ ¼ �hoEðtÞ=om: ð12Þ
� Compute the error E(t+1), where t is the iteration number, m isthe reference vector, and h is the learning rate. The error E canbe chosen as the mean square error function between the actualoutput yj and the desired output dj:
E ¼ 12
Xnj
j¼1
ðdj � yjÞ2: ð13Þ
InputHidden
OutputAge
Anal Tone
Micturition time
IllnessHealthy
Fig. 2. The architecture of the artificial neural network, MLP (input layer, hiddenlayer and output layer).

Table 3Backpropagation training parameters
Parameters Value
Learning rate 0.01Adaptive learning rate 0.1Momentum constant 0.2Epochs 50Minimum performance gradient 1
e�10
D. Gil et al. / Expert Systems with Applications 36 (2009) 5754–5760 5757
The adaptive learning rate can be adapted to speed up the conver-gence of the algorithm. For batch training strategy, the learning ratecan be adjusted as follows:
gðtÞ ¼bgðt � 1Þ if EðtÞ < Eðt � 1Þhgðt � 1Þ if EðtÞ > kEðt � 1Þgðt � 1Þ otherwise
8><>: ð14Þ
where g(t) is the learning rate at the ith iteration, and b, h and k arechosen as such that b > 1, 0 < h < 1, and k > 1 and the learning ratecan be updated using g(t) = g 0 + k E(t + 1), where g0 is a presetlearning rate and k > 0.
For the construction of the architecture of MLP we proceed asfollows:
(a) Layer 1 with the inputs that correspond to the input vector,that is, all the parameters/fields of the patient’s record.
(b) Layer 2 with the hidden layer. The number of hidden neu-rons for this layer is the most elaborated question in the net-work’s architecture. This number represents a trade ofbetween performance and risk of overfitting. In fact, thenumber of neurons in a hidden layer will significantly influ-ence the ability of the network to generalize from the train-ing data to the unknown examples (Kavzoglu, 2001). Fig. 3shows several tests. In this graphics of the MLP training/val-idation it can be appreciated how they evolve with differentvalues of hidden neurons. The best solution for this hiddenlayer has been found with 20 neurons. Moreover, these tests
0 5 10
10-1
0
23 Ep
TrainingValidation
Performance is 0
10-2
0 5 10 15 20
10-1
0
23 Epochs
TrainingValidation
10-2
Performance is 0.0752903, Goal is 0
1
25 hidden
20 hid
Fig. 3. The training of a MLP in order to find out the
provide the optimal number of training iterations. For thisissue the process is to stop training when the test error stopsdecrease and it increase again.
(c) Layer 3 with the output (ill and healthy patients).
3. Experiments
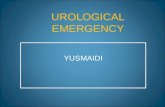
The input data in the system starts when a patient reports to aphysician. Then, a large number of information to be considered dur-ing the diagnosis will be saved in a database. In this study, anexhaustive urological exploration with 20 different measurementshas been carried out by using 300 patients with dysfunctions ofthe LUT. The 20 input variables (Fig. 4) that are essential to the diag-nosis of the LUT diseases of interest are extracted from the urologicaldatabase. Fig. 4 helps us to understand the dimension of the problemto deal with (different types of data, ranges and incomplete fields).
These variables can be divided into five classes:
(a) Basic information of a patient, in our case only the age, nor-mally the sex is also included but we use only femalepatients (the urological service is specialized in femaleincontinence).
(b) Neurological physical examination (three features in total).(c) Free flowmetry analysis (five features in total).(d) Cystometry (three features in total) and(e) Test pressure/flow (eight features in total).
Moreover, the 20 input variables (categorized into three groupsor classes) are prearranged using the following structures:
(a) Numerical variables such as age, volume of urine and mictu-rition time are normalized on to the interval (0,1). Forinstance, the patients’ ages may span from 0 to 100 yearsold. However, in practice the oldest is 86, and thereby theage of a 86-year-old patient can be normalized to the valueof 86/86 = 1 whereas a 63-year-old patient can be normal-ized to the value of 63/86 = 0.73.
15 20ochs
.023377, Goal is 0
0 5 10 15 20
10-1
0
23 Epochs
TrainingValidation
0-2
Performance is 0.0752903, Goal is 0
15 hidden
den
best solution performance without overfitting.

{ (0,1)
( 1, 0, 1)
General Information A- ge
- Perineal and perianal sensitivity Neurological
- Anal tonePhysical
Examination
−
( 0, 1)
( 1, 0, 1)
( 0, 1)- Volume of urine
- Post void residual
- Voluntary control of the anal sphincter
- Free Flowmetry
−
( 0, 1)
( 0, 1)
( 0, 1)
( 0
- Maximum flow rate
- Average flow rate
- Micturition time , 1)
( 0, 1)
( 0, 1)
- Bladder storage
- Detrusor pressure during filling- Cystometry
- First sensation of bladder filling ( 0, 1)
( 1, 0, 1)
( 1, 0, 1)
- Detrusor contraction
- Abdominal pressure
- Volume of urine in micturition
- Test pressure / flow
−
−
( 0, 1)
( 0, 1)
( 0, 1)
( 0, 1)
- Post void residual
- Maximum pressure detrusor
- Maximum flow rate
- Average flow rate ( 0, 1)
( 0, 1)- Micturition time
Fig. 4. Fields of the urological database and their consequent values normalized onto the interval between parenthesis.
Table 4Information of the variables
Input variables Times withmissing data
Mean of thevariable
General Information Age 8 0.68Neurological physical
examinationPerineal and perianalsensitivity
7 0.2
Anal tone 7 0.96Voluntary control of theanal sphincter
16 �0.8
Free flowmetry Volume of urine 12 0.27Post void residual 17 0.1Maximum flow rate 15 0.21Average flow rate 15 0.26Micturition time 18 0.19
Cystometry Bladder storage 0 0.49Detrusor pressure filling 1 0.13First sensation ofbladder filling
8 0.49
Test pressure/flow Detrusor contraction 4 �0.56Abdominal pressure 0 0.55Volume of urine inmicturition
4 0.41
Post void residual 109 0.11Maximum pressuredetrusor
64 0.28
Maximum flow rate 25 0.27Average flow rate 32 0.35Micturition time 139 0.26
Missing data and mean value of each variable.
5758 D. Gil et al. / Expert Systems with Applications 36 (2009) 5754–5760
(b) The variables with only two independent attributes are pre-arranged with binary values (0, 1). We only have the repre-sentation of anal tone where 1 means normal and 0 denoterelaxed.
(c) The variables with three independent attributes, such as Per-ineal and perianal sensitivity, detrusor contraction orabdominal pressure are prearranged using the ternary values(�1, 0, 1). For example, the abdominal pressure will take �1for the absence, 0 represents weak and 1 represents normal.
ANNs usually operate with complete input data. However, anusual problem in medical databases is the deficient of informationand consequently the missing data values. Sometimes, some exam-inations can not be appropriated for certain patients or the doctorrecorded some data unsuccessfully. Numerous methods have beenrecommended to deal with this missing data problem (Doyle,Parmanto, Marino, Aldrighetti, & Doria, 1995; Heckerling, Elstein,Terzian, & Kushner, 1991). The simplest method is to ignore thecases with missing data. A more complex approach may involvecomputing a complex structure like an ANN (Erkki, Matti, & Matti,1998). In our work, the substituting means method is adopted. Inother words, the missing data values of the incomplete input datacases are substituted with the mean values computed from the in-put data. Concerning to the accuracy, it has been revealed that thissubstituting means method has a corresponding performance asthe ANN-based approach, while requiring less computing effort.Table 4 presents the classification of every variable with theirnumber of cases with missing data values and the correspondingmean. The realization of evaluation is critically important for theproposed system, since ANNs systems are strongly dependent onthe selected training set (Embrechts, Arciniegas, Breneman,Bennett, & Lockwood, 2001), in particular for small data sets. Thecross validation method will be used to evaluate the accuracy inorder to avoid this dependency with the data sets and, obtainingthen, a higher level of generalization with new data.
Frequently, the complete data set is divided into two subsets:the training set and the test set. Here, the training set is used todetermine the system parameters, and the test set is used to eval-uate the diagnosis accuracy and the network generalization. Cross-
validation has been widely used to assess the generalization of anetwork. The cross-validation estimation of the accuracy is deter-mined by the overall number of correct classifications divided bythe total number of examples in the dataset (Kohavi, 1995).
Acccv ¼1n
Xðxi ;yiÞ2S
dðIðSi; xiÞ; yiÞ; ð15Þ
where n is the size of the dataset S, xi is the example of S, yi is thetarget of xi, and Si is the probable target of xi by the classifier.Therefore
dði; jÞ ¼1 if i ¼ j;
0 otherwise:
�ð16Þ
Specifically, for this study we have applied a five-fold cross-valida-tion method for the performance assessment. The data has been di-vided in five sets (S1, S2, S3, S4, S5) and the five experimentsperformed were
Experiment 1 – Training: S1, S2, S3, S4; Test: S5Experiment 2 – Training: S1, S2, S3, S5; Test: S4Experiment 3 – Training: S1, S2, S4, S5; Test: S3Experiment 4 – Training: S1, S3, S4, S5; Test: S2Experiment 5 – Training: S2, S3, S4, S5; Test: S1
Therefore, the sets of data used for the process of constructingthe model (the training data) were of 240 registers. The other setof data used to validate the model (the test data) was of 60registers.
The measurement of the accuracy of the MLP is simple since it isa supervised network and we can know the correct output andthus verify whether the result obtained by the network is corrector not. For the measurement of the accuracy of the unsupervisednetworks there exist, in general, greater problems. Nevertheless,in our case, as we have the correct value that the network mustpredict, this factor is not so vital. Moreover, as a fundamental

Fig. 5. Classification by using unsupervised ANNs.
Table 5Result of accuracy with cross-validation
MLP SOM GCS
Experiment 1 53 52 54Experiment 2 54 51 51Experiment 3 51 50 52Experiment 4 56 56 51Experiment 5 54 51 53Mean Acc (%) 89.30 82.00 83.60
D. Gil et al. / Expert Systems with Applications 36 (2009) 5754–5760 5759
characteristic of the unsupervised ANNs, they also inform of thedegree of membership to the categorized area. This is a big advan-tage of using unsupervised ANNs, as we can see in Fig. 5, the visualperception of the proximities between illness and health patients.In this experimentation the degree of membership has been settleddown with five values:
(a) 100%: When the test element is between elements of itssame class and it does not have neighbours of a differentone.
(b) 75%: When the test element has only one neighbour ofanother class.
(c) 50%: When the element has two neighbours of another class.(d) 25%: When the test element has three neighbours of another
class.(e) 0%: When the test element is referenced to the same posi-
tion of another class.
This results are represented in Table 5.The accuracy of the cross-validation classification is determined
by the expression:
53þ 54þ 51þ 56þ 54300
¼ 268300
¼ 89:3% ð17Þ
for each ANN. This value belong to MLP’s experiment and the sameexpression has been done for the others ANNs.
From the results detailed in Table 5 we can observe that theproposed system by using ANNs is quite suitable since it presentsa robust capability of accuracy to distinguish the illness andhealthy patients. The accuracy of the supervised method is slightlyhigher. However, a big advantage of using unsupervised ANNs, aswe can see in Fig. 5, is the visual perception of the proximities ofthe different dysfunctions (their membership functions) catego-rized in areas to find out relations between similar inputs. The per-centage of negative false is minimal, of around 10%. This fact makesit highly reliable amongst the urologists.
4. Conclusions and future work
In this paper we have evaluated the performance of three differ-ent kinds of artificial neural networks, the Kohonen self-organizing
map, the Growing Cell Structures and the Multilayer Perceptrontrained with the backpropagation algorithm, when applied to thecategorization of urological dysfunctions. The ANNs were trainedwith data from a database with registers of patients with urologicaldysfunctions.
The experiment starts with a preprocessing of the urodynamicalmeasures from every patient. After that, data are provided to theANN and they determine whether there is a dysfunction of theLUT or not. Data preprocessing is the stage in which the most timeof the experimentation is spent. However, it is worth it because theaccuracy has been especially if we compare it to other techniquessuch as discretization (Duda, Hart, & Stork, 2000).
The human expert is able to generalize by using his experience.This big advantage is simulated for ANNs by using graphs offering avisual perception. The frontiers between health and illness help theurologist to discover resemblances and maybe to make more testsfor these patients (possibly some of the parameters are near thedysfunction’s threshold). They can also help detecting similaritiesbetween fields or urodynamical samples.
In this work, we obtained valuable comments from the urolo-gists after using the system. They remarked its advantages to givea more precise diagnosis and, therefore, to save time and money tohealth sector institutions. Their comments encourage us to con-tinue our work to develop a system that uses the diagnosis ob-tained as a result of the combined use of different neuralnetworks. This gives an even more accurate diagnosis.
Once the accuracy of the ANNs has been tested and they show ahigh degree of certainty above 80% and in some cases close to 90%,they will be used in order to distinguish and classify among themost common dysfunctions by using the fuzzy logic theory. Conse-quently, since ANNs are suitable for this matter, we will propose ahybrid system such as the’Adaptive Network based Fuzzy InferenceSystems’ (ANFIS) to take advantage of both methods ANNs and ofthe fuzzy systems.
Acknowledgements
We want to express our acknowledgement to Christian Balke-nius for helpful comments on the manuscript. The data used inthe development of this system is the result of several years of col-laboration with urologists of the Hospital of San Juan (Alicante-Spain). The work has been supported by the Office of Science andTechnology as part of the research project ‘‘Cooperative diagnosissystems for Urological dysfunctions (2005–2006)”.
References
Abrams, P. (2005). Urodynamics (3rd ed.). Springer. pp. 20–39.Batuello, J. T., Gamito, E. J., Crawford, E. D., Han, M., Partin, A. W., McLeod, D. G., et al.
(2001). Artificial neural network model for the assessment of lymph nodespread in patients with clinically localized prostate cancer. Urology, 57,481–485.

5760 D. Gil et al. / Expert Systems with Applications 36 (2009) 5754–5760
Begg, R., Kamruzzaman, J., & Sarkar, R. (2006). Neural Networks in Healthcare:Potential and Challenges.
Bishop, C. M. (1995). Neural networks for pattern recognition. Oxford: OxfordUniversity Press.
Doyle, H., Parmanto, B., Marino, I., Aldrighetti, L., & Doria, C. (1995). Building clinicalclassifiers using incomplete observations-a neural network ensemble forhepatoma detection in patients with cirrhosis. Methods of Information inMedicine, 34, 253–258.
Duda, R., Hart, P., & Stork, D. (2000). Pattern classification (2nd ed.). Wiley-Interscience.
Embrechts, M. J., Arciniegas, F. A., Breneman, C. M., Bennett, K. P., & Lockwood, L.(2001). Bagging neural network sensitivity analysis for feature reduction for In-Silico drug design. In Proceedings of INNSIEEEinternational joint conference onneural networks (Vol. 2478, p. 2482).
Erkki, P., Matti, E., & Matti, J. (1998). Treatment of missing data values in a neuralnetwork based decision support system for acute abdominal pain. ArtificialIntelligence in Medicine, 13, 139–164.
Fritzke, B. (tul=0?>Fritzke, 1993a). Growing Cell Structures – A Self-organizingNetwork for Unsupervised and Supervised Learning, 93–126.
Fritzke, B. (1993b). Kohonen Feature maps and growing cell structures aperformance comparison, NIPS 1992. Denver.
Fritzke, B. (1995). A Growing Neural Gas Network Learns Topologies.Fritzke, B. (1997). Unsupervised ontogenic networks. In Fiesler & Beale (Eds.),
Handbook of neural computation. IOP Publishing Ltd. and Oxford UniversityPress.
Gil, D., Soriano, A., Ruiz, D., García, J., & Flórez, F. (2005). Decision support system fordiagnosing dysfunctions in the lower urinary tract. In 3rd European medical andbiological engineering conference. IFMBE European Conference on BiomedicalEngineering.
Gil, D., Soriano, A., Ruiz, D., & Montejo, C. A. (2006). Development of an artificialneural network for helping to diagnose diseases in urology. In Proceedings ofthe bio-inspired models of network, Information and Computing Systems(BIONETICS’06).
Gil, D., Johnsson, M., Soriano, A., & Ruiz, D. (2008). Artificial neural networks fordiagnoses of dysfunctions in urology. In International conference on healthinformatics.
Green, M., Bjork, J., Forberg, J., Ekelund, U., Edenbrandt, L., & Ohlsson, M. (2006).Comparison between neural networks and multiple logistic regression to
predict acute coronary syndrome in the emergency room. Artificial Intelligencein Medicine, 38, 305–318.
Hand, D. J. (1997). Construction and assessment of classification rules. New York:Wiley.
Haykin, S. (1998). Neural networks: A comprehensive foundation (Vol. 2). PrenticeHall.
Heckerling, P., Elstein, A., Terzian, C., & Kushner, M. (1991). The effect of incompleteknowledge on diagnoses of a computer consultant system. Medical Informatics,16, 363–370.
Kavzoglu, T. (2001). An investigation of the design and use of feedforward artificialneural networks in the classification of remotely sensed images, PhD thesis,School of Geography, University of Nottingham.
Kohavi, R. (1995). A study of cross-validation and bootstrap for accuracy estimationand model selection. In Proceedings of international joint conference onartificial intelligence.
Kohonen, T. (1988). Self-organization and associative memory. Berlin Heidelberg:Springer-Verlag.
Kohonen, T. (1990). The self-organizing map. Proceedings of the IEEE, 78(9),1464–1480.
Kohonen, T. (2001). Self-organizing maps. Berlin Heidelberg: Springer-Verlag.Peled, A. (2005). Plasticity imbalance in mental disorders the neuroscience of
psychiatry: Implications for diagnosis and research. Medical Hypotheses, 65,947–952.
Politi, E., Balduzzi, C., Bussi, R., & Bellodi, L. (1999). Artificial neural networks: Astudy in clinical psychopharmacology. Psychiatry Research, 87, 203–215.
Remzi, M., & Djavan, B. (2004). Artificial neural networks in urology. EuropeanUrology, 33–38.
Remzi, M., Anagnostou, T., Ravery, V., Zlotta, A., Stephan, C., Marberger, M., et al.(2003). An artificial neural network to predict the outcome of repeat prostatebiopsies. Urology, 62, 456–460.
Ripley, B. D. (1996). Pattern recognition and neural networks. Cambridge: CambridgeUniversity Press.
Ruiz, D., García, J. M., Macía, F., & Soriano, A. (2005). Robust modelling of biologicalneuroregulators. IEEE Engineering in Medicine and Biology Society.
Suzuki, K., Shiraishi, J., Abe, H., MacMahon, H., & Doi, K. (2005). False-positivereduction in computer-aided diagnostic scheme for detecting nodules in chestradiographs by means of massive training artificial neural network. AcademicRadiology, 12, 191–201.