
APPLICATION INSTRUCTIONS FOR NURSE LICENSUREibn.idaho.gov/IBNPortal/IBN/UPDATED FORMS...
14
APPLICATION FOR RN or LPN LICENSURE BY ENDORSEMENT Use this application if: The applicant has never held an Idaho license. (and you do NOT live in a Compact State) Criminal Background checks – All applicants are required to submit to a fingerprint-based criminal background check by the Idaho Central Criminal Database and Federal Bureau of Investigation criminal history database. Fingerprint cards are available from the Board office by calling (208) 334-3110 ext 2476. Total Fees to be submitted: RN/LPN Endorsement Fee - $110.00 Fingerprint Processing Fee - $ 30.00 TOTAL FEE: $140.00 or Temporary License Fee - $ 25.00 (if requested) TOTAL FEE: $165.00 PLEASE NOTE: Effective October 1, 2012, the Fingerprint Processing Fee will be increased to $34.00. Applications post-marked on or after October 1, 2012, must include the increased fee. (Total fee to submit - $144.00 OR $169.00 with a temporary license) Effective July 1, 2013, the Fingerprint Processing Fee will be increased to: $42.00. Applications post-marked on or after July 1, 2013, must include the increased fee. (Total fee to submit - $152.00 OR $177.00 with a temporary license)
Transcript of APPLICATION INSTRUCTIONS FOR NURSE LICENSUREibn.idaho.gov/IBNPortal/IBN/UPDATED FORMS...
APPLICATION FOR RN or LPN LICENSURE
BY ENDORSEMENT Use this application if: The applicant has never held an Idaho license.
(and you do NOT live in a Compact State)
Criminal Background checks – All applicants are required to submit to a fingerprint-based criminal background check by the Idaho Central Criminal Database and Federal Bureau of Investigation criminal history database. Fingerprint cards are available from the Board office by calling (208) 334-3110 ext 2476.
Total Fees to be submitted: RN/LPN Endorsement Fee - $110.00 Fingerprint Processing Fee - $ 30.00 TOTAL FEE: $140.00 or Temporary License Fee - $ 25.00 (if requested) TOTAL FEE: $165.00 PLEASE NOTE: Effective October 1, 2012, the Fingerprint Processing Fee will be increased to $34.00. Applications post-marked on or after October 1, 2012, must include the increased fee. (Total fee to submit - $144.00 OR $169.00 with a temporary license) Effective July 1, 2013, the Fingerprint Processing Fee will be increased to: $42.00. Applications post-marked on or after July 1, 2013, must include the increased fee. (Total fee to submit - $152.00 OR $177.00 with a temporary license)

Idaho Board of Nursing - PO Box 83720, Boise, Idaho 83720-0061 Voice - (208) 334-3110 - TDD Relay - (800) 377-3529
APPLICATION INSTRUCTIONS FOR NURSE LICENSURE
This application may be used by nurses applying for:
Licensed practical nurse licensure (LPN).
Licensed professional nurse licensure (RN).
Advanced practice professional nurse licensure (CNM, CNS, NP, RNA). If you are applying for APPN licensure and are not currently licensed to practice in Idaho as a professional nurse (RN), you must apply for professional and advanced practice professional nurse licensure and pay both licensure fees. Temporary licensure. Idaho has a mandatory nurse licensure law requiring nurses to be licensed to practice in Idaho at the time of employment. A temporary license may be issued for an interim period of ninety (90) days while the application for renewable licensure is being processed. Instructions for temporary licensure are included on the reverse side. The following must be on file with the Board of Nursing to determine your eligibility for licensure in Idaho. (All documents become the property of the Board and may be destroyed, without further notification, if the application is not completed within one year.) Documents requiring notarization may NOT be received by FAX. The following items are required for all applications: 1. APPLICATION FORM: Only application forms provided by the Board, completed in ink and notarized will be accepted. Photocopies or Faxed copies of application forms will not be accepted.
1) If all information requested is not supplied, provide an explanation for the omission. 2) Sign the affidavit with your usual signature and have it notarized. 3) Attach a 2 x 2 identification photograph, taken within the last year. Electronically scanned photos are not acceptable; features must be clearly identifiable. Black & white or color photos are acceptable.
2. FEE: Enclose the appropriate fee for all categories of licensure for which you are applying (personal checks are accepted): Licensed Practical Nurse (LPN)/Licensed Professional Nurse (RN):
Endorsement Fee - $110.00 Reinstatement Fee - $125.00 RN/PN Temporary License Fee – additional $25.00 3. CENSUS QUESTIONNAIRE: Complete the enclosed Census Questionnaire and return with your completed application. (If you have not been licensed in Idaho previously, leave the box requesting your license number blank.) 4. VERIFICATION FORM: Send the verification of licensure form to the state in which you were licensed by examination (complete the enclosed “Verification of Licensure” form) OR if you were ever licensed in one of the states on the enclosed “NOTICE To Nurses Seeking Licensure in Idaho”, you will need to complete only the enclosed NURSYS form and submit it to the National Council of State Boards of Nursing for processing (see attached information). Do not request both verifications. The temporary license can be issued prior to the receipt of either of these forms. 5. EMPLOYMENT REFERENCE: A satisfactory nursing employment reference from the three-year period immediately preceding the application is required. The employment reference may be faxed to (208) 334-3262 or mailed directly to the Board of Nursing by the employer. References will not be accepted from the applicant. This form is not required to be on file in order to issue the temporary license. If you have not been employed in nursing within the last three years, do not complete the reference form. You may be required to obtain a conditional temporary license in order to update your nursing knowledge to qualify for Idaho licensure. 6. DECLARATION OF STATE OF RESIDENCE: Complete the enclosed form attesting to your primary residence. You may be requested to submit supporting documentation. 7. AFFIDAVIT: The affidavit on page 2 of the application must be completed and notarized in order for your application to be valid. 8. FINGERPRINT CARD Complete the required Fingerprint card and submit to the Board for processing. Only cards from the Board office are acceptable - fee for processing - $30.00. Effective October 1, 2012, the fee for processing of fingerprint cards shall be increased to: $34.00. Applications post-marked on or after October 1, 2012, must include the increased fee. Effective July 1, 2013, the Fingerprint Processing Fee will be increased to: $42.00. Applications post-marked on or after July 1, 2013, must include the increased fee. 9. PRIVACY STATEMENT: You must complete and return the enclosed “NonCriminal Justice Applicant Privacy Statement” to the Board office before your license can be issued. To obtain and challenge your FBI Identification Record – go to: www.fbi.gov/hq/cjisd/fprequest.htm. PLEASE BE ADVISED: Licensed professional nurses and advanced practice professional nurses must renew their license(s) by August 31
st of every odd-numbered year. Licensed practical nurses must renew their license by August 31
st of every even-numbered year. A
nurse who applies for licensure on or after March 1st
of the year in which the license would ordinarily be renewed, will be issued a license valid until the next renewal period.
Continued on Page 2

Page 2 INSTRUCTIONS FOR APPLYING FOR TEMPORARY LICENSURE FOR RN/LPN APPLICANTS
Applicants requesting temporary licensure as an RN/LPN must submit completed application pages 1 & 2 with these additional materials:
1) Licensure fee, plus the additional temporary licensure fee of $25.00. 2) Evidence that you are currently licensed in good standing in another state. Submit a photocopy of a current licensure
certificate (wallet-sized card) accompanied by the enclosed “Affidavit Attesting to Validity of Copies”. The licensure certificate must indicate the expiration date. Temporary licenses CANNOT be issued on expired, inactive, non-practicing certificates; temporary licenses from other states; or certificates not issued in your current name unless accompanied by a Change of Name Affidavit (available from this office) or a copy of your marriage license, divorce decree or other legal document indicating name change.
Applicants who have not been employed in nursing within the last three years may be required to obtain a conditional temporary license in order to update nursing knowledge and skills. The conditional temporary license may be issued by submitting completed application pages 1 & 2 with these additional materials:
1) Licensure fee, plus the additional temporary licensure fee of $25.00. 2) Evidence of previous licensure or a copy of your lapsed license is acceptable, pending receipt of a verification form from
original state of licensure (or NURSYS). (Please contact the Board office ext. 34 if you have questions.)
ADVANCED PRACTICE PROFESSIONAL NURSE
In addition to submitting the competed application pages 1 & 2, the following items are required for Advanced Practice Professional Nurse Licensure: 1. APPLICATION FORM: Complete the information requested on page 3. 2. FEE: Enclose the appropriate fee: Advanced Practice Professional Nurse (CNM, CNS, NP, RNA) - $90.00 APPN Temporary License - No Fee Fingerprint Processing Fee (if not also applying for RN license) - $30.00*
*Effective October 1, 2012, the fee for processing of fingerprint cards shall be increased to: $34.00. Applications post-marked on or after October 1, 2012, must include the increased fee. Effective July 1, 2013, the Fingerprint Processing Fee will be increased to: $42.00. Applications post-marked on or after July 1, 2013, must include the increased fee.
3. OFFICIAL TRANSCRIPT: Request an OFFICIAL TRANSCRIPT indicating program completion from the advanced practice professional nursing program, to be mailed directly to the Board of Nursing office.
4. ADVANCED PRACTICE PROFESSIONAL NURSE NATIONAL CERTIFICATION: Submit a copy of your current national certification
attached to the enclosed affidavit. 5. RN LICENSURE. If you are currently licensed to practice as an RN in Idaho, do not submit items 2, 3, 4, or 5 on page 1 of these instructions.
TEMPORARY LICENSURE FOR ADVANCED PRACTICE PROFESSIONAL NURSE APPLICANTS
Advanced practice professional nurse applicants (CNM, CNS, NP, RNA) applying for APPN temporary licensure, who are currently authorized to practice in Idaho under temporary or renewable professional (RN) licensure must submit the completed application form and the “Affidavit Attesting to Validity of Copy”, attached to one of the following documents:
1) If you hold national certification, submit a copy of your current certificate showing the expiration date; or 2) If you have not yet taken the certification examination, submit a copy of the document which verifies acceptance to take the
examination. In addition, evidence of completion of an Advanced Practice Professional Nursing education program is required. If a final transcript is not yet available, submission of one of the following documents is acceptable:
a. Correspondence received directly (by FAX or mail) from the director of the educational program attesting to completion of all graduation requirements; or
b. Notarized copy of diploma. 3) If your national certification has lapsed, submit a copy of your lapsed certificate. The Board will consider issuance of a
conditional temporary license in order for you to meet specified practice requirements under supervision for re-entry into advanced practice professional nursing.
8/12
THE IDAHO BOARD OF NURSING DOES NOT DISCRIMINATE OR DENY SERVICES ON THE BASIS OF AGE, RACE, RELIGION, COLOR, NATIONAL ORIGIN, SEX AND/OR DISABILITY
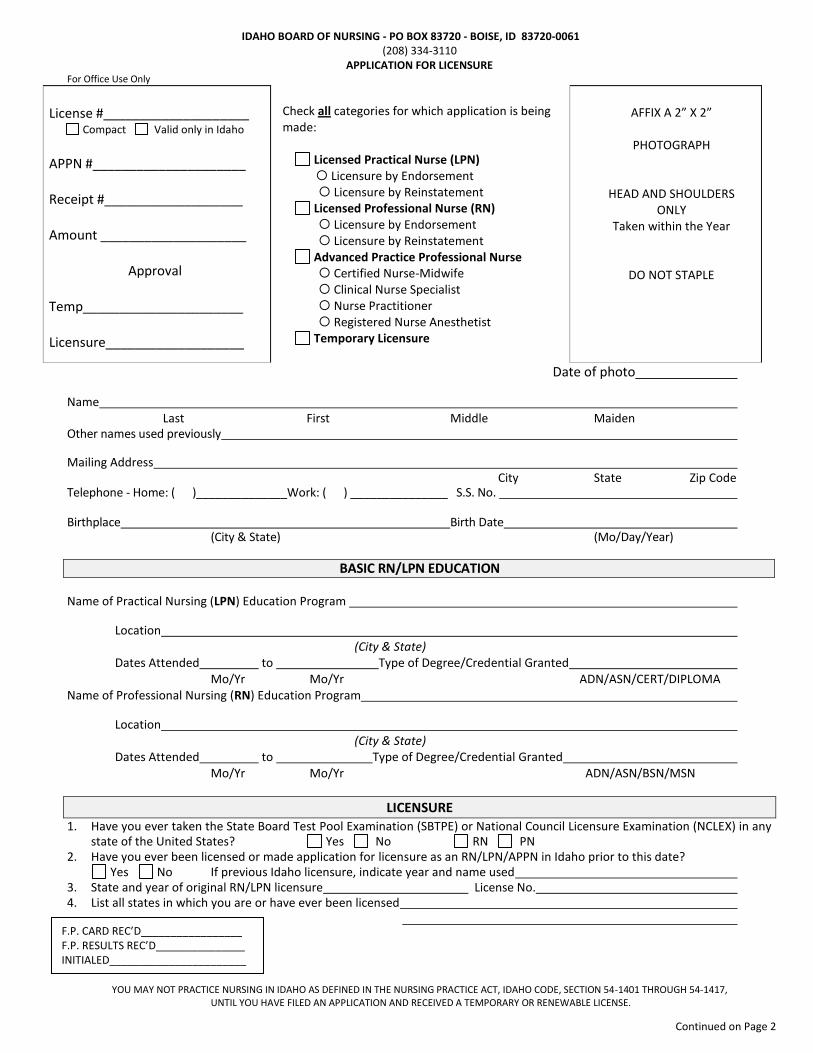
IDAHO BOARD OF NURSING - PO BOX 83720 - BOISE, ID 83720-0061 (208) 334-3110
APPLICATION FOR LICENSURE For Office Use Only
License #____________________ Compact Valid only in Idaho
APPN #_____________________ Receipt #___________________ Amount ____________________
Approval
Temp______________________ Licensure___________________
Check all categories for which application is being made:
Licensed Practical Nurse (LPN)
Licensure by Endorsement Licensure by Reinstatement
Licensed Professional Nurse (RN) Licensure by Endorsement Licensure by Reinstatement
Advanced Practice Professional Nurse Certified Nurse-Midwife Clinical Nurse Specialist Nurse Practitioner Registered Nurse Anesthetist
Temporary Licensure
AFFIX A 2” X 2”
PHOTOGRAPH
HEAD AND SHOULDERS ONLY
Taken within the Year
DO NOT STAPLE
Date of photo
Name Last First Middle Maiden Other names used previously
Mailing Address City State Zip Code Telephone - Home: ( )______________Work: ( ) _______________ S.S. No.
Birthplace Birth Date (City & State) (Mo/Day/Year)
BASIC RN/LPN EDUCATION
Name of Practical Nursing (LPN) Education Program
Location (City & State) Dates Attended to Type of Degree/Credential Granted Mo/Yr Mo/Yr ADN/ASN/CERT/DIPLOMA Name of Professional Nursing (RN) Education Program
Location (City & State) Dates Attended to Type of Degree/Credential Granted Mo/Yr Mo/Yr ADN/ASN/BSN/MSN
LICENSURE 1. Have you ever taken the State Board Test Pool Examination (SBTPE) or National Council Licensure Examination (NCLEX) in any
state of the United States? Yes No RN PN 2. Have you ever been licensed or made application for licensure as an RN/LPN/APPN in Idaho prior to this date? Yes No If previous Idaho licensure, indicate year and name used 3. State and year of original RN/LPN licensure License No. 4. List all states in which you are or have ever been licensed
YOU MAY NOT PRACTICE NURSING IN IDAHO AS DEFINED IN THE NURSING PRACTICE ACT, IDAHO CODE, SECTION 54-1401 THROUGH 54-1417,
UNTIL YOU HAVE FILED AN APPLICATION AND RECEIVED A TEMPORARY OR RENEWABLE LICENSE.
F.P. CARD REC’D_________________ F.P. RESULTS REC’D_______________ INITIALED_______________________
Continued on Page 2

Page 2
EMPLOYMENT INFORMATION
LIST LAST THREE (3) YEARS OF NURSING EMPLOYMENT: (Additional information may be listed on a separate sheet.)
Name & Complete Address of Employer
Position
Employment From To
If you have not been employed in nursing within the last three years, or if there are gaps in employment, indicate your last year of nursing employment and explain the reason. (Supervised practice and a content update may be required if you have not engaged in nursing practice during the last three years.) IT IS THE DUTY OF EACH APPLICANT TO MAKE INQUIRY OF THE INDIVIDUAL LICENSING BOARDS REGARDING THE STATUS OF LICENSURE IN THAT STATE BEFORE RESPONDING TO THE QUESTIONS BELOW. Ignorance of license status or disciplinary information will not constitute an excuse for incorrect information. In addition, failure to disclose all licenses may result in denial of your application or other appropriate action.
SCREENING QUESTIONS PLEASE ANSWER ALL QUESTIONS (For all “yes” answers, attach a complete explanation including dates, circumstances and supporting documents if necessary.) 1. Has your nursing license ever been disciplined in any state (e.g., revoked, suspended, placed
on probation, formally reprimanded, or otherwise encumbered)?
Yes
No
2. Is any action pending against your nursing license in any state? Yes No 3. Have you ever had approval to practice in an advanced role denied, limited, suspended,
revoked or otherwise disciplined? NA Yes No
4. Have you ever had an application for nursing license denied? Yes No 5. Have you ever been denied admission to take a nursing examination by any state? Yes No 6. Do you have, or have you been diagnosed as having, or have you been treated for having
a physical or mental condition, including drug or alcohol addiction during the past five (5) years, which may impair your ability to practice nursing with reasonable skill and safety?
Yes
No
7. If yes, do you require special accommodations in order to practice? NA Yes No 8. Do you currently have any felony or misdemeanor charges pending against you in any
jurisdiction? Yes No
9. Have you ever pled guilty, entered a plea of nolo contendre, been convicted of, or received a withheld judgment for a misdemeanor or felony in any jurisdiction?
Yes No
THE AFFIDAVIT BELOW MUST BE COMPLETED IN ORDER FOR YOUR APPLICATION TO BE VALID.
A F F I D A V I T State of ) ) s.s. County of ) I, being duly sworn, declare that I understand the instructions and terms as set forth in this application form, that I am the person referred to in the foregoing application and this affidavit, and that I have personally completed this form, and that the information given in this application is true, correct and complete. I declare that I have no mental or physical disabilities (except as otherwise noted above) that presently interfere with my ability to competently and safely practice nursing and that I have read and understand this affidavit. Signature of Applicant On this day of , in the year of before me , a notary public, personally appeared known or identified to me to be the person whose name is subscribed to the within instrument, and acknowledged to me that he/she executed the same. Notary Public WITNESS my hand and official seal. My Commission expires 8/2012

Professional Nurse (RN) CENSUS QUESTIONNAIRE
Please Print NAME :
ADDRESS :
CITY & STATE : Zip Code
Idaho License No. Birth Date Social Security No. Gender* (Optional)
County Name
/ /
- -
Residence:
Employment:
Ethnicity* (Optional) Caucasian (1) African American/Black (2) Hispanic (3) Am. Indian/Alaska Native (4)
Asian/Pacific Islander (5) Multi-Racial (6) Other (99)
(*Voluntary disclosure information – response optional) Please choose only one answer for each question, write the appropriate number in the box to the left.
EMPLOYMENT STATUS 1. Employed in nursing full-time 5. Not Employed/Student 9. Retired 2. Employed in nursing part-time 6. Not Employed/Not Seeking 3. Employed outside nursing 7. Volunteer 4. Not Employed/Seeking Employment 8. Emeritus
PRIMARY EMPLOYER
Employer Address
PRIMARY EMPLOYMENT 1. Hospital 7. Assisted Living 99. Other (specify) 2. Nursing Home 8. Nursing Education 3. Home Health/Hospice 9. Insurance Company 4. Public Health 10. Jail/Prison 5. Occupational Health 11. School Health 6. Medical Office/Clinic 12. Outpatient Facility
TYPE OF POSITION 1. Staff or General Duty 6. Quality Assurance/Outcomes Management 2. Case Manager/Discharge Planner 7. Consultant/Researcher 3. Administrator/Supervisor 8. Charge/Lead Nurse/ Team Leader 4. Educator 99. Other (specify) 5. Advanced Practice (not RN Specialty)
MAJOR CLINICAL AREA 1. Geriatric 5. Psychiatric/Mental Health 99. Other (specify) 2. Gynecologic/Obstetric 6. Emergency 3. Medical/Surgical 7. Community/Public Health 4. Pediatric 8. Rehabilitation/Restorative
BASIC EDUCATION 1. Diploma 3. Baccalaureate Degree or Higher 2. Associate Degree 4. Other (specify)
HIGHEST DEGREE 1. Diploma/RN 6. Masters in Other Field 10. PN Associate Degree 2. Associate Degree/RN (specify) 99. Other (specify) 3. Baccalaureate Degree/RN 7. Doctorate in Nursing 4. Baccalaureate Degree in Other Field 8. Doctorate in Other Field (specify) (specify) 5. Masters in Nursing 9. PN Certificate/Diploma
Year Advanced Degree was Granted
I am currently taking courses toward an additional/advanced degree in nursing? Yes No
I intend to leave/retire from the practice of nursing in the next two years? Yes No States other than Idaho in which I am practicing:
Information provided is for statistical purposes only.
IDAHO BOARD OF NURSING
Cert # Rec’t # Amt Date Issued
□ Reinstatement □ Endorsement
For Office Use Only

IDAHO BOARD OF NURSING, 280 NORTH 8TH STREET, SUITE 210, BOISE, ID 83720-0061
Mailing: P.O. Box 83720 FAX: (208) 334-3262
VERIFICATION OF LICENSURE
APPLICANT: Complete the requested information and forward to the Board of Nursing in the state in which you were licensed by examination. Board addresses are located on the back of this form. (A fee may be required.)
NAME: (Last, First, Middle, Maiden)
PREVIOUS NAMES: SOCIAL SECURITY NO:
CURRENT ADDRESS: (Street, City, State, Zip Code)
ORIGINAL LICENSE NUMBER:
TYPE OF LICENSE ( ) Professional (RN) ( ) Practical
DATE ISSUED:
NURSING EDUCATION PROGRAM COMPLETED: YEAR OF GRADUATION: Name: Location:
I hereby authorize the Board of Nursing to release the information requested below to the Idaho Board of Nursing. Date: Signature:
LICENSING AGENCY
This is to certify that the above-named individual was issued: LICENSE NUMBER: DATE ISSUED: ( ) Licensed Professional Nurse (RN) ( ) Licensed Practical Nurse
LICENSED BY: ( ) Examination ( ) Endorsement
LICENSURE STATUS: ( ) Current ( ) Lapsed
EXPIRATION DATE:
Has this license ever been encumbered in any way (revoked, suspended, restricted, limited, placed on probation)? ( ) YES* ( ) NO Under current investigation ( ) YES* ( ) NO Action Pending ( ) YES* ( ) NO * If YES, please attach an explanation, documents, etc.
NURSING EDUCATION PROGRAM: Location: Year of Graduation: Approved/Accredited by Board of Nursing at time of graduation: ( ) YES ( ) NO
Examination Information
Registered Nurse NCLEX
Registered Nurse SBTPE
Practical Nurse NCLEX/ SBTPE MEDICAL
NURSING PSYCH NURSING
OB NURSING
SURG NURSING
NURSING OF CHILD
Standard Scores
Series/Form
This form may be FAXED if the Board seal is an inked imprint. JURISDICTION: SIGNATURE: DATE: TITLE: (BOARD SEAL) 8/12

ADDRESSES OF STATE BOARDS OF NURSING
ALABAMA, 770 WASHINGTON AVENUE, RSA PLAZA, STE 250, MONTGOMERY, AL 36130-3900 (334/242-4060) ALASKA, 550 WEST SEVENTH AVENUE, SUITE 1500, ANCHORAGE, ALASKA 99501-3567 (907/ 269-8161) AMERICAN SAMOA, LBJ TROPICAL MEDICAL CENTER, PAGO PAGO, AS 96799 (684/633-1222) ARIZONA, 4747 N. 7
TH STREET, SUITE 200, PHOENIX, AZ 85014-3653 (602/889-5150)
ARKANSAS, UNIVERSITY TOWER BLDG, 1123 S. UNIVERSITY, SUITE 800, LITTLE ROCK, AR 72204-1619 (501/686-2700) CALIFORNIA-RN, 1625 N. MARKET BLVD, STE N-217, SACRAMENTO, CA 95834-1924 (916/322-3350) CALIFORNIA-PN, 2535 CAPITOL OAKS DRIVE, SUITE 205, SACRAMENTO, CA 95833 (916/263-7800) COLORADO, 1560 BROADWAY, SUITE 880, DENVER, CO 80202 (303/894-2430) CONNECTICUT, 410 CAPITOL AVENUE, MS# 13PHO, P.O. BOX 340308, HARTFORD, CT 06134-0328 (860/509-7624) DELAWARE, 861 SILVER LAKE BLVD, CANNON BUILDING, SUITE 203, DOVER, DE 19904 (302/739-4522) DIST. OF COLUMBIA, 717 14
TH STREET NW, STE 600, WASHINGTON, DC 20005 (202/724-4900)
FLORIDA, 4052 BALD CYPRESS WAY, BIN C02, TALLAHASSEE, FL 32399-3252 (850/245-4125) GEORGIA-PN, 237 COLISEUM DRIVE, MACON, GA 31217-3858 (478/207-1640) GEORGIA-RN, 237 COLISEUM DRIVE, MACON, GA 31217-3858 (478/207-1640) GUAM, P.O. BOX 2816, HAGATNA, GUAM 96932 (671/735-7406) HAWAII, KING KALAKAUA BUILDING, 335 MERCHANT STREET, 3RD FLOOR, HONOLULU, HI 96813 (808/586-3000) IDAHO, P.O. BOX 83720, BOISE, ID 83720-0061 (208/334-3110) ILLINOIS, 320 W. WASHINGTON STREET, 3
RD FLOOR, SPRINGFIELD, IL 62786 (217/782-8556)
INDIANA, 402 W. WASHINGTON STREET, ROOM W072, INDIANAPOLIS, IN 46204 (317/234-2043) IOWA, RIVERPOINT BUSINESS PARK, 400 S.W. 8TH STREET, SUITE B, DES MOINES, IA 50309-4685 (515/281-3255) KANSAS, LANDON STATE OFFICE BUILDING, 900 S.W. JACKSON, SUITE 1051, TOPEKA, KS 66612 (785/296-4929) KENTUCKY, 312 WHITTINGTON PARKWAY, SUITE 300, LOUISVILLE, KY 40222 (502/429-3300) LOUISIANA-PN, 3421 N. CAUSEWAY BOULEVARD, SUITE 505, METAIRIE, LA 70002 (504/838-5791) LOUISIANA-RN, 5207 ESSEN LANE, SUITE 6, BATON ROUGE, LA 70809 (225/763-3570) MAINE, 158 STATE HOUSE STATION, AUGUSTA, ME 04333 (207/287-1133) MARYLAND, 4140 PATTERSON AVENUE, BALTIMORE, MD 21215 (410/585-1900) MASSACHUSETTS, 239 CAUSEWAY STREET, 2
ND FLOOR, BOSTON, MA 02114 (617/973-0800)
MICHIGAN, OTTAWA TOWERS NORTH, 611 W. OTTAWA, 1ST FLOOR, LANSING, MI 48933 (517/335-0918) MINNESOTA, 2829 UNIVERSITY AVENUE SE, MINNEAPOLIS, MN 55414 (612/617-2270) MISSISSIPPI, 1935 LAKELAND DRIVE, SUITE B, JACKSON, MS 39216-5014 (601/987-4188) MISSOURI, 3605 MISSOURI BLVD. P.O. BOX 656, JEFFERSON CITY, MO 65102-0656 (573/751-0681) MONTANA, 301 SOUTH PARK, PO BOX 200513, HELENA, MT 59620-0513 (406/841-2340) NEBRASKA, 301 CENTENNIAL MALL SOUTH, LINCOLN, NE 68509-4986 (402/471-4376) NEVADA, 5011 MEADOWOOD MALL #201, RENO, NV 89502-6547 (775/688-2620) NEW HAMPSHIRE, 21 SOUTH FRUIT STREET, SUITE 16, CONCORD, NH 03301-2341 (603/271-2323) NEW JERSEY, P.O. BOX 45010, 124 HALSEY STREET, 6TH FLOOR, NEWARK, NJ 07101 (973/504-6586) NEW MEXICO, 6301 INDIAN SCHOOL ROAD, NE, SUITE 710, ALBUQUERQUE, NM 87110 (505/841-8340) NEW YORK, EDUCATION BLDG, 89 WASHINGTON AVE, 2ND FLOOR WEST WING, ALBANY, NY 12234 (518/474-3817) NORTH CAROLINA, 3724 NATIONAL DRIVE, SUITE 201, RALEIGH, NC 27602 (919/782-3211) NORTH DAKOTA, 919 SOUTH 7TH STREET, SUITE 504, BISMARCK, ND 58504 (701/328-9777) NORTHERN MARIANA ISLANDS, PO BOX 501458, SAIPAN, MP 96950 (670/664-4812) OHIO, 17 SOUTH HIGH STREET, SUITE 400, COLUMBUS, OH 43215-3413 (614/466-3947) OKLAHOMA, 2915 N. CLASSEN BOULEVARD, SUITE 524, OKLAHOMA CITY, OK 73106 (405/962-1800) OREGON, 17938 SW UPPER BOONES FERRY RD, PORTLAND, OR 97224-7012 (971/673-0685) PENNSYLVANIA, PO 2649, HARRISBURG, PA 17105-2649 (717/783-7142) PUERTO RICO, PO BOX 10200, SANTURCE, PR 00908-0200 (787/725-7506) RHODE ISLAND, 105 CANNON BUILDING, THREE CAPITOL HILL, PROVIDENCE, RI 02908 (401/222-5700) SOUTH CAROLINA, 110 CENTERVIEW DRIVE, SUITE 202, COLUMBIA, SC 29210 (803/896-4550) SOUTH DAKOTA, 4305 SOUTH LOUISE AVE., SUITE 201, SIOUX FALLS, SD 57106-3115 (605/362-2760) TENNESSEE, 425 FIFTH AVE NORTH, 1ST FLOOR - CORDELL HULL BUILDING, NASHVILLE, TN 37247 (615/532-5166) TEXAS, 333 GUADALUPE, SUITE 3-460, AUSTIN, TX 78701 (512/305-7400) UTAH, HEBER M. WELLS BLDG., 4TH FLOOR, 160 EAST 300 SOUTH, SALT LAKE CITY, UT 84111 (801/530-6628) VERMONT, NATIONAL LIFE BLDG NORTH F1-2, MONTPELIER, VT 05620-3402 (802/828-2396) VIRGIN ISLANDS, VETERANS DRIVE STATION, ST. THOMAS, VI 00803 (340/776-7397) VIRGINIA, PERIMETER CNTR, 9960 MARYLAND DR., STE. 300, RICHMOND, VA 23233 (804/662-9909) WASHINGTON, HPQA #6, 310 ISRAEL RD SE, TUMWATER, WA 98501-7864 (360/236-4700) WEST VIRGINIA-PN, 101 DEE DRIVE, CHARLESTON, WV 25311 (304/558-3572) WEST VIRGINIA-RN, 101 DEE DRIVE, CHARLESTON, WV 25311 (304/558-3596) WISCONSIN, 1400 E. WASHINGTON AVENUE, RM 173, MADISON, WI 53708 (608/266-0145) WYOMING, 1810 PIONEER AVENUE, CHEYENNE, WY 82001 (307/777-7601) 0309

Idaho Board of Nursing
PO Box 83720 – Boise, Idaho 83720-0061 Voice: (208) 334-3110 ext. 2476
TDD – (800) 377-3529 Fax: (208) 334-3262
To Nurses Seeking Licensure in Idaho
If you are or were ever licensed in Alaska, Arizona, Arkansas, Colorado, Delaware, District of Columbia, Florida, Indiana, Iowa, Kentucky, Maine, Maryland, Massachusetts, Minnesota, Mississippi, Missouri, Montana, Nebraska, Nevada, New Hampshire, New Jersey, New Mexico, North Carolina, North Dakota, Ohio, Oregon, Rhode Island, South Carolina, South Dakota, Tennessee, Texas, Utah, Vermont, Virgin Islands, Virginia, Washington, West Virginia (PN), Wisconsin or Wyoming, you must obtain a Nursys LICENSE VERIFICATION by accessing the Nursys website at https://www.nursys.com and completing the request form. You may pay the $30.00 fee by MasterCard or Visa. DO NOT COMPLETE THE ENCLOSED IDAHO VERIFICATION OF LICENSURE FORM. Your verification will be completed by the NURSYS system and provided to the Idaho Board of Nursing electronically. This verification form is valid for ninety days only and may only be extended by submitting an additional fee. If you submit your application after the expiration date of the Verification, you will be requested to pay an additional $30.00 fee. Note: If you are NOT licensed in Alaska, Arizona, Arkansas, Colorado, Delaware, District of Columbia, Florida, Indiana, Iowa, Kentucky, Maine, Maryland, Massachusetts, Minnesota, Mississippi, Missouri, Montana, Nebraska, Nevada, New Hampshire, New Jersey, New Mexico, North Carolina, North Dakota, Ohio, Oregon, Rhode Island, South Carolina, South Dakota, Tennessee, Texas, Utah, Vermont, Virgin Islands, Virginia, Washington, West Virginia (PN), Wisconsin or Wyoming, please complete the enclosed Verification of Licensure form (Idaho form) and forward this form to your original state of licensure. DO NOT COMPLETE THE NURSYS FORM. Please contact the Board office (208) 334-3110 ext. 2476 if you have questions concerning the Verification form. 8/12

NURSING EMPLOYMENT REFERENCE FORM
LICENSURE APPLICANT:
1. If you have been employed as a nurse at some time within the last three years for a minimum of 80 hours, complete the release information at the top of this form and send to a registered nurse/supervisor from your current or most recent place of employment for completion of the bottom section. The form must be returned directly to the Board by the nursing employer.
2. If you graduated from a nursing education program less than one year ago AND you have not been employed as a nurse for a minimum of 80 hours, complete the release information at the top of this form and send to a faculty member at your nursing education program for completion of the bottom section. The form must be returned directly to the Board office by the faculty.
TO: PLACE OF EMPLOYMENT (OR NURSING SCHOOL) SUPERVISOR (OR FACULTY CHAIR) I,________________________________________, Social Security # ___________________________ have applied to the (Name of Nurse Applicant) the Idaho Board of Nursing for licensure as an _______________________ nurse. I stated on my licensure application (RN/LPN/APPN) that I was employed/enrolled at your institution as a for the following (circle one) (RN, LPN, RNA, NP, CNM, CNS, other) period: to . I hereby authorize you to release to the Idaho Board of Nursing for licensure purposes, the information requested below.
DATE SIGNATURE OF APPLICANT
ATTENTION: THIS FORM WILL NOT BE ACCEPTED DIRECTLY FROM THE APPLICANT.
NURSING EMPLOYER (OR FACULTY MEMBER): The above named person has applied for licensure as a nurse in the State of Idaho and has given your name as a reference. Please furnish the information requested below and return the completed form by mail or FAX to: IDAHO BOARD OF NURSING, P.O. BOX 83720, BOISE, ID 83720-0061 - FAX: (208) 334-3262 (If returning this form by FAX, please do not follow up with a hard copy.)
1. The applicant was employed/enrolled from to .
(circle one) as a(n): RN CNM NP
LPN CNS RNA OTHER*
*If OTHER is checked, please specify job title in the blank and list job duties on the reverse side of this form. 2. GENERAL HISTORY: ** Met performance requirements
Performance NOT satisfactory (If NOT satisfactory, please explain on reverse.)
** If unable to release this information, please initial here , sign and return this form.
DATE SIGNATURE AND TITLE EMPLOYER OR SCHOOL: MAILING ADDRESS: PHONE and FAX NUMBERS: 8/12

DECLARATION OF PRIMARY STATE OF RESIDENCE
NURSING LICENSURE INTERSTATE COMPACT
Dear Applicant for Licensure by Interstate Endorsement or Reinstatement: On July 1, 2001, Idaho became a member of the Nurse Licensure Compact. Other states include Arizona, Arkansas, Colorado, Delaware, Iowa, Kentucky, Maine, Maryland, Mississippi, Missouri, Nebraska, New Hampshire, New Mexico, North Carolina, North Dakota, Rhode Island, South Carolina, South Dakota, Tennessee, Texas, Utah, Virginia, and Wisconsin. Under terms of the Nurse Licensure Compact, nurses may hold a license to practice issued by their state of residence, if that state is a Compact state, and are granted the privilege to practice in other Compact states without holding separate licenses in those other states. If you reside in a Compact state, you may hold a Compact state license only in your declared state of residence; you may not be licensed in any other Compact state. If you reside in a state that is not a member of the Compact and you apply for licensure to practice in any Compact state, you will be issued a license by the individual Compact state that will be designated as valid for practice only in that state. If you are applying for licensure in Idaho and indicating a mailing address in another Compact state, it is imperative that you inform the Idaho Board as to which scenario best suits your particular situation, to ensure that appropriate procedures are followed in issuing your Idaho license or in directing you to contact the appropriate state(s) to apply for and receive a license. Please note, if you are in the process of moving to Idaho and declaring Idaho as your state of residence, you must provide the Idaho Board with an Idaho address within 30 days of relocating to this state. Upon notice of address change, licenses held in any other Compact state will become invalid. More information regarding the Nurse Licensure Compact is available on the National Council of State Boards of Nursing web site at http://www.ncsbn.org. If you have questions about your application, please contact the Board at (208) 334-3110 ext. 21.
-------------------------------------------------------------Tear off and return-----------------------------------------------------------------
DECLARATION OF STATE OF RESIDENCE
Name Address: Primary state of residence is defined as “the state of a person’s declared fixed permanent and principal home for legal purposes; domicile. Documentation of state of residence includes a valid driver’s license with a home address, voter registration card with a home address, and/or the state declared as the state of residency on the last federal tax return. Based on the definition above, my primary state of residence is I am currently practicing nursing (including telenursing) in the following states:
Check one:
I am declaring Idaho as my state of residence, even though my mailing address is in another Compact state – enclose
evidence.
I am declaring Idaho as my state of residence; my mailing address is listed below.
I am practicing in Idaho, but am declaring another Compact state as my state of residence - enclose evidence.
I am practicing in Idaho, but am declaring a Non-Compact state ________________________ as my state of residence.
I am a member of the armed forces and am declaring Idaho as my state of residence.
I am in the process of moving to Idaho, but do not yet have an Idaho mailing address. * Estimated move date__________
*Notify the Board office of Idaho address as soon as possible.
Signature Date Address: 8/12

Idaho State Police Bureau of Criminal Identification
NONCRIMINAL JUSTICE APPLICANT PRIVACY STATEMENT
As an applicant who is the subject of a national fingerprint-based criminal history record check for a non-criminal justice purpose you have certain rights which are discussed below. This serves as notification from the Idaho Board of Nursing that your fingerprints will be used to check the criminal history records of the State of Idaho and the FBI and that those records will be used solely for the purpose requested and may not be disseminated outside the receiving department, related agency or other authorized entity. The collection of applicant fingerprints in Idaho is authorized by Idaho Code §67-3008.
• If you have a criminal history record, the officials making a determination of your suitability for the job, license, or other benefit must provide you the opportunity to complete or challenge the accuracy of the information in the record.
• Procedures for obtaining a change, correction, or updating of your criminal history record are set forth at Title 28, Code of Federal Regulations (CFR), Section 16.34.
• If you have a criminal history record, you should be afforded a reasonable amount of time to correct or complete the record , or decline to do so, before being denied the job, license, or other benefit based on information in the criminal history record.
• Disclosure of your Social Security number is voluntary and is solicited pursuant to the Federal Privacy Act and Idaho Code §67-3012 to aid the processing of an interstate background check request for noncriminal justice purposes allowed by federal statute, federal executive order or a state statute that has been approved by the attorney general. The fingerprints and information reported from this request may be disclosed pursuant to your consent, and may also be disclosed by the FBI without your consent as permitted by the Federal Privacy Act of 1974 (5 USC 552a(h)). Routine uses include, but are not limited to, disclosures to appropriate governmental authorities responsible for civil or criminal law enforcement, counterintelligence, national security or public safety matters to which the information may be relevant; to State and local governmental agencies and nongovernmental entities or application processing as authorized by Federal and State legislation, executive order, or regulation, including employment, security, licensing, and adoption checks. Depending on the nature of your application, other authorities may include numerous Federal or State statutes pursuant to Public Law 92-544 or other authorized authorities. According to Idaho state law and if agency policy permits, you may be provided a copy of your FBI criminal history record for review and possible challenge upon submission of a written request. If agency policy does not permit it to provide you a copy of the record, you may obtain a copy of the record by submitting fingerprints and a fee to the FBI. Information regarding this process may be obtained at http://www.fbi.gov/about-us/cjis/background-checks. If you decide to challenge the accuracy or completeness of your FBI criminal history record, you should send your challenge to the agency that contributed the questioned information to the FBI. Alternatively, you may send your challenge directly to the FBI at the same website address as provided above. The FBI will then forward your challenge to the agency that contributed the questioned information and request the agency to verify or correct the challenged entry. Upon receipt of an official communication from that agency, the FBI will make any necessary changes/corrections to your record in accordance with the information supplied by that agency. (See 28 CFR 16.30-16.34) If a change, correction or update needs to be made to an Idaho criminal history record, that process information is available on the Idaho State Police website. http://www.isp.idaho.gov/identification/crime_history/FrequentlyAskedQuestions-CriminalRepository.html. Your signature below acknowledges this agency has informed you of your privacy rights for fingerprint-based background check requests used by the agency for non-criminal justice purposes.
I do I do not want a copy of the Privacy Act Statement. Printed Name Signature of Applicant Date
Idaho Board of Nursing – PO Box 83720 – Boise, ID 83720-0061

AFFIDAVIT ATTESTING TO VALIDITY OF COPY
I hereby certify that the attached is a direct photocopy of: Please appropriate box (es). RN/LPN: The certificate which shows proof of current licensure as a licensed professional nurse (RN)
or licensed practical nurse (LPN) APPN: The certificate which shows advanced practice professional nurse national certification The document which verifies acceptance to take the certification examination The diploma from my Advanced Practice Professional Nurse educational program
Total number of documents Signature of Applicant On this day of , in the year of , before me , a notary public, personally appeared , known or identified to me to be the person whose name is subscribed to the within instrument, and acknowledged to me that he/she executed the same. (Notary Seal) Notary Public My Commission Expires
2012
Check List
The following items must be submitted when you file your application for LPN/RN licensure: Completed, notarized application – pages 1 and 2 Fee(s) Census Questionnaire Declaration Form Fingerprint Card Privacy Statement Affidavit attesting to the Validity of Copies – if applying for a temporary license, this form must be
accompanied by a copy of your current licensure certificate or lapsed licensure certificate if you are applying for a conditional temporary license
Be sure that you have requested your employer to complete the Employment Reference form and that you have requested your Verification of Licensure form be submitted directly to the Board of Nursing.
The following items must be submitted when you file your application for APPN licensure: Completed, notarized application – pages 1, 2 and 3. Fee – for Advanced Practice Professional Nurse licensure Fee – for Professional Nurse (RN) licensure if NOT currently licensed to practice in Idaho as an RN and NOT
residing in a Compact State Declaration Form Fingerprint Card – if NOT also applying for RN licensure Affidavit attesting to the Validity of Copies – attach a copy of your APPN Certification card
Be sure that you have requested that an OFFICIAL TRANSCRIPT of your advanced practice professional nursing program be submitted directly to the Board office.
It is not necessary to return this form with your application Check List.doc 2012


















