Appendix. Critical Pathway of Brain Hypothermia Treatment978-4-431-53953-7/1.pdf · Appendix....
34
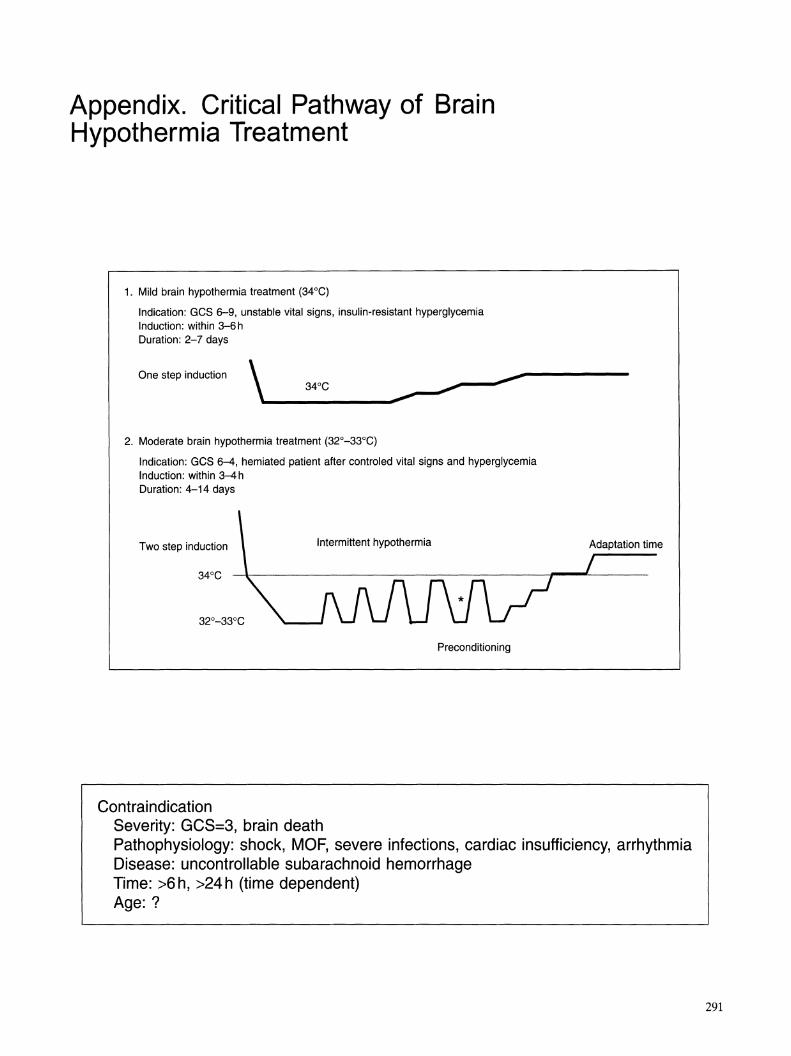
Appendix. Critical Pathway of Brain Hypothermia Treatment 1. Mild brain hypothermia treatment (34°C) Indication: GCS 6-9, unstable vital signs, insulin-resistant hyperglycemia Induction: within 3-6 h Duration: 2-7 days \ ,- One step induction 2. Moderate brain hypothermia treatment (32°-33°C) Indication: GCS 6-4, hemiated patient after controled vital signs and hyperglycemia Induction: within 3-4 h Duration: 4-14 days Two step induction Intermittent hypothermia Preconditioning Contraindication Severity: GCS=3, brain death Adaptation time Pathophysiology: shock, MOF, severe infections, cardiac insufficiency, arrhythmia Disease: uncontrollable subarachnoid hemorrhage Time: >6 h, >24 h (time dependent) Age: ? 291
-
Upload
phungquynh -
Category
Documents
-
view
213 -
download
0
Transcript of Appendix. Critical Pathway of Brain Hypothermia Treatment978-4-431-53953-7/1.pdf · Appendix....
Appendix. Critical Pathway of Brain Hypothermia Treatment
1. Mild brain hypothermia treatment (34°C)
Indication: GCS 6-9, unstable vital signs, insulin-resistant hyperglycemia Induction: within 3-6 h Duration: 2-7 days
\ ----~~ 3~C ,-
------~ One step induction
2. Moderate brain hypothermia treatment (32°-33°C)
Indication: GCS 6-4, hemiated patient after controled vital signs and hyperglycemia Induction: within 3-4 h Duration: 4-14 days
Two step induction Intermittent hypothermia
Preconditioning
Contraindication Severity: GCS=3, brain death
Adaptation time
Pathophysiology: shock, MOF, severe infections, cardiac insufficiency, arrhythmia Disease: uncontrollable subarachnoid hemorrhage Time: >6 h, >24 h (time dependent) Age: ?
291
N
\D
N >- "0
"0
(1)
~ ~ (")
Out
line
of t
he c
ritic
al p
ath
of b
rain
hyp
othe
rmia
tre
atm
ent
:J.
..... n·
Sta
ge
Sta
ge 1
S
tage
2
Sta
ge 3
S
tage
4
Sta
ge 5
S
tage
6
~
'"0
Indu
ctio
n 1
Indu
ctio
n 2
Coo
ling
Pre
cond
ition
ing
Rew
arm
ing
Pos
t hy
poth
erm
ia
~ So
:IE
Dur
atio
n 3
h
6h
3
-7 d
ays
1-2
day
s 1
-2 d
ays
3-4
wee
ks
~
'<
0 A
lgor
ithm
of
Ho
to
Man
agem
ent
Sta
biliz
e vi
tal s
igns
M
ild o
r m
oder
ate
Inte
rmitt
ent
Evi
denc
e of
neu
rona
l S
tep
by s
tep
rew
arm
A
10-
Dop
amin
e .... ~
Tar
gets
S
hive
ring
hypo
ther
mia
? hy
poth
erm
ia
reco
very
A
dapt
atio
n tim
e re
plac
emen
t th
erap
y S·
C
atec
hola
min
e S
erum
glu
cose
IC
P <
15
mm
Hg
N
o se
vere
inf
ectio
n S
erum
glu
cose
R
esto
ratio
n th
erap
y o
f ::r: '<
su
rge
<1
60
mg
/dl
Bra
in e
dem
a C
SF
/ser
um a
lbum
in
13
0-1
50
mg/
dl
vege
tatio
n "0
0
Neu
rona
l hy
poxi
a D
02
>70
0 m
Vm
in
AT
-III
>10
0%
<0.0
1 0
02
>7
00
ml/m
in
Neu
rore
habi
litat
ion
.....
::r-H
yper
glyc
emia
H
emog
lobi
n S
erum
alb
umin
S
erum
glu
cose
0
2 ER
23
-35
(1
) .... 34
°C b
rain
dy
sfun
ctio
n >
3.5
mg
/dl
12
0-1
40
mg/
dl
Pa
C0 2
32-
36 m
mH
g 8. ~
tem
pera
ture
A
T-III
>10
0%
Imm
une
Ent
eral
nut
ritio
n S
erum
pH
7.3
-7.4
::;l
D
opam
ine
rele
ase
Hyp
opot
asse
mia
dy
sfun
ctio
n R
ecov
er im
mun
e S
erum
Pho
spha
te
(1) ~
Rad
ical
rea
ctio
n S
BP
> 1
00
mm
Hg
P
reve
nt i
nfec
tion
func
tion
>3
mg
/dl
.....
S F
luid
res
usci
tatio
n A
ctiv
ate
lipid
A
ctiv
ate
lipid
S
erum
Mg
' >
1.3
mm
ol/d
l (1
) ~
met
abol
ism
m
etab
olis
m
Rep
lace
men
t vi
tam
in A
.....
I n
fect
ion
cont
rol
Sta
ndar
d M
anag
emen
t O
rder
B
asic
car
e pl
an
CD
CD
CD
CD
CD
CD
Car
e or
der
~
~
~
~
~
~
Inte
rven
tion
@
@
@
@
@
@
IV m
edic
atio
n @
) @
) @
) @
) @
) @
)
Mon
itor
Bra
in m
onito
r @
@
@
@
@
@
S
yste
mic
car
e ®
®
®
®
®
®
m
onito
r

Appendix. Critical Pathway of Brain Hypothermia Treatment 293
Stage 1.1.
Basic care plan:
• Start brain hypothermia within 3 h after insult. • Maintain the systolic blood pressure> 100 mmHg. • Evaluate GCS < 8 and surgical indication. • Rapid management of stress-associated hyperglycemia. • Maintain hemoglobin function with control of serum pH, phosphate, and magnesium. • Prevent catecholamine surge. • Neuronal oxygenation. • Prevent enterobacterial infection. • Suppress hypothalamus dopamine release.
Stage 1.2.
Care order:
• Systolic blood pressure (SBP): control at 120-160 mmHg by fluid resuscitation. • SBP > 170 mmHg hypertension: drip the antihypertensive drug, diltiazem hydrochlo-
ride (Helvesser), 250 mg, diluted with 100 ml saline at 2 ml/h. • Blood gases: Pa02> 100 mmHg, PaOiFi02 ratio> 350, PaC02 34-38 mmHg. • Urine: maintain at 0.5 ml/kg h-1•
• Serum glucose: control serum glucose at 120-140 mg/dl by drip of rapid - action insulin (Humarin R), 50 U diluted with 100 ml saline. * Administration speed: start from 2 ml/h and then slow down to 1 ml/hour after serum
glucose becomes lower than 200 mg/dl. • Serum potassium: control at 3.5-4.5 mEq/1 by drip of KCI 1 A, diluted with 80 ml saline.
* Replacement speed 40 ml/h for serum K+ < 2.0 mEq/1. * 20 mllh for serum K+ 1.2-2.5 mEq/1. * 15 ml/h for serum K+ 2.6-3.0 mEq/1. * 10 ml/h for serum K+ 23.1-3.05 mEq/1. * 5 ml/h for serum K+ 3.6-34.0 mEq/1.

294 Appendix. Critical Pathway of Brain Hypothermia Treatment
Stage 1.3.
Intervention:
• Bronchial intubation and ventilator care management. • Fluid resuscitation by central venous catheterization. • Catheter insertion for monitoring arterial blood gases. • Insertion of naso-gastric tube. • Insertion of Foley catheter for urinary drainage. • Monitoring of ECG. • Biochemical analysis. • Blood type. • X-ray examination. • Gastric lavage. • Digastrics decontamination.
* One shot enteral administration of nonabsorbable antibiotics: levofloxacin (Cravit, 200 mg) + amphotericin B, 100-300 mg.
Stage 1.4.
Intravenous medication:
• Fluid resuscitation: 7% Acetic acid Ringer solution (Veen F) and Saline Hess solution at induction stage, except hypoglycemia. The replacement of potassium phosphate, vitamin A, vitamin S, Mg++, 5% albumin, and AT-III are recommended.
• Crush induction of anesthesia: midazolam 0.15-0.25 mg/kg h-1 anesthesia, combined with pancuronium 0.05 mg/kg h-1 muscle relaxation, and buprenorphine 1.0-2.0 mg/kg h-1 analgesia. Propofol is much better for unstable cardiopulmonary function than midazolam. At the beginning of the induction stage, propopfol is preferred.
• Management of aspiration pneumonia: first choice is panipenem betamipron (Carbenin 500 mg x 2/day), second choice is ceftazidime (Modasin 1 9 x 2/day) or clindamycine (Dalacin, 150-300 mg per 6 h) + one-shot enteral administration of nonabsorbable antibiotics: levofloxacin (Cravit, 200 mg) + Amphotericin S, 100-300 mg to prevent Pseudomonas aspiration pneumonia and enteral bacterial translocation.

Appendix. Critical Pathway of Brain Hypothermia Treatment 295
Stage 1.5.
Brain monitoring and management:
• Computed brain monitoring: * Tympanic membrane temperature/core temperature> 1.0. * Internal jugular venous blood temperature/tympanic membrane temperature> 1.0. * Ventricular CSF temperature/internal jugular venous blood temperature> 1.0. * Ventricular CSF temperature/bladder temperature> 1.0.
• ICP < 20 mmHg. • Microdialysis monitoring. • Sj02> 60%. • CPP > 80 mmHg. • Trend EEG. • Auditory brain stem evoked response (ABER).
Stage 1.6.
Monitoring and management of systemic hemodynamic changes:
• SBP> 100mmHg • Monitoring of ECG for arrhythmia, ST changes, and QT interval < 450 mm/s. • Right flowing catheter monitoring of cardiac output (CO). • Cardiac index (CI). • Oxygen delivery> 700 ml/min. • Oxygen extraction ratio (02ER) 22%-26%. • Bladder pressure < 15 mmHg. • Gastric pHi> 7.3. • Intestinalluminar pressure < 15mmHg. • Serum glucose and hemoglobin A 1 C. • AT-III. • Hemoglobin. • Serum albumin. • Troponin I and CPK. • GOT and GPT.
• Ht. • Serum osmolarity. • Creatinine.

Sta
ge
1. A
lgo
rith
m m
anag
emen
t
• S
tabi
lize
vita
l si
gns:
ela
stic
ban
dagi
ng o
f ex
trem
ities
, no
rmal
vol
ume
repl
acem
ent,
med
icat
ion,
mai
ntai
n S
BP
>
10
0m
mH
g,
CP
P>
80
mm
Hg
, H
b>
12m
g/dl
, ox
ygen
de
live
ry>
800
ml/m
in.,
2,3
-DP
G >
13J
.lmol
/ml.
• S
erum
K+
> 3
mE
q/dl
, se
rum
glu
cose
12
0-1
40
mg
/dl.
• S
hive
ring:
mid
azol
am a
nest
hesi
a 0
.15
-0.2
5 m
g/kg
h-1
co
mbi
ned
with
pan
curo
nium
mus
cle
rela
xant
0.0
5 m
g/kg
h-1
,
and
bupr
enor
phin
e an
alge
sia
1.0
-2.0
mg/
kg h
-1•
• C
atec
hola
min
e su
rge:
con
trol
of
cate
chol
amin
e su
rge
by c
ontr
ol o
f br
ain
tissu
e te
mpe
ratu
re a
t 34
°C
, adm
inis
tra
tion
of m
etoc
lopr
amid
e.
• N
euro
nal
hypo
xia:
Pa
OiF
i02
ratio
> 3
50,
hem
oglo
bin
DP
G:
12-1
4J.lm
ol/m
l, ox
ygen
de
live
ry>
700
ml/m
in,
CP
P>
80
mm
Hg,
AT
-III
> 1
00%
. •
Hyp
ergl
ycem
ia:
adm
inis
trat
ion
of i
nsul
in w
ith c
ontr
ol o
f se
rum
pho
spha
te a
nd m
agne
sium
. •
7% a
ceta
te R
inge
r so
lutio
n.
• S
tero
id c
ontr
aind
icat
ed.
• A
ctiv
ate
resp
irato
ry m
uscl
e m
etab
olis
m w
ith a
lbut
amol
. •
Rap
id i
nduc
tion
of m
ild b
rain
hyp
othe
rmia
: co
mbi
natio
n of
bla
nket
coo
ling
met
hod
and
gast
ric l
avag
e w
ith c
hille
d sa
line,
alc
ohol
hea
t ev
apor
atio
n, c
ompl
ete
body
wra
ppin
g an
d in
sula
tion
from
roo
m a
ir, r
educ
e ro
om t
empe
ratu
re
to 1
8°C
, mai
ntai
n ro
om a
ir ou
tflow
circ
ulat
ion,
tw
o co
olin
g m
achi
nes,
rem
ove
heat
gen
erat
ing
med
ical
dev
ices
fro
m
the
beds
ide.
•
Dop
amin
e re
leas
e: e
arly
ind
uctio
n of
bra
in h
ypot
herm
ia a
nd a
dmin
istr
atio
n of
met
oclo
pram
ide.
•
Pre
vent
ion
of r
adic
al
reac
tion:
ear
ly i
nduc
tion
of m
ild b
rain
hyp
othe
rmia
and
con
tinue
to
mod
erat
e br
ain
hypo
th
erm
ia.
• C
ontr
ol o
f H
b >
11
mg/
dl,
adm
inis
trat
ion
of v
itam
ins
E a
nd C
.
tv
'D
0\ ~
"0
(1) ::::s &.
?< (J
::l. g. e:..
"'0
I'l ;.
~ ~ o '"" ttl .., I'
l Er ~ o .... p
(1
) §l s;.
~
(1)
I'l a (1) g

Appendix. Critical Pathway of Brain Hypothermia Treatment 297
Stage 2.1.
Basic care plan:
• Select mild or moderate brain hypothermia. • Monitor internal jugular venous temperature. • Monitor ventricular CSF temperature. • Monitor tympanic temperature. • Monitor core temperature. • Monitor bladder temperature. • Stabilize vital signs for induction to moderate brain hypothermia. • SSP> 100mmHg. • Treat hypokalemia. • Ensure no arrhythmia. • QT-interval < 450 mm/s on ECG. • Serum glucose 120-140 mmHg. • Brain monitoring, Sj02 65%-80%. • ICP < 20 mmHg.
Stage 2.2.
Care order:
• Systolic blood pressure (SBP): 120-160 mmHg by fluid resuscitation. • SBP> 170 mmHg hypertension: drip antihypertensive drug diltiazem hydrochloride (Helvesser), 250 mg,
diluted with 100 ml saline at 2 ml/h. • Complication of bradycardia (HR < 50 bpm): nicardipine hydrochloride (Perdipin) 2-5 ~g/kg min-1 .
• Blood gases: Pa02> 100 mmHg, PaOiFi02 ratio> 350, PaC02 35 mmHg. • Urine volume: more than 0.5 ml/kg h-1 .
• Serum glucose: 120-140 mg/dl by drip of rapid-action insulin (Humarin R) 50 U diluted with 100 ml saline. * Administration speed: start at 2 ml/h and slow to 1 ml/h after serum glucose falls below 200 mg/dl.
• Serum potassium: control at 3.5-4.5 mEq/1 by drip of KCI 1 A, diluted with 80 ml saline. * Replacement speed: 40ml/h for serum K+ < 2.0mEq/l.
20 ml/h for serum K+ 1.2-2.5 mEq/1. 15 ml/h for serum K+ 2.6-3.0 mEq/1. 10ml/h for serum K+ 23.1-3.05mEq/l. 5 ml/h for serum K+ 3.6-34.0 mEq/1.
298 Appendix. Critical Pathway of Brain Hypothermia Treatment
Stage 2.3.
Intervention:
• Ventilator management. • Ventricular drainage. • ICP monitoring. • Sj02 monitoring. • Monitoring cardiac output and 02ER. • Body weight. • Blood gases. • Microdialysis monitoring.
Stage 2.4.
Intravenous medication:
• Fluid resuscitation: 7% Acetic acid Ringer solution (Veen F) + H2 receptor antagonist (Zantac SOmg/A) + metoclopramide (Prinmperan) 1 A + panthenol (pantol SOO mg x 2).
• Maintenance fluid: actit solution SOO ml + carbazochrome sodium sulfonate (Adona) SO ml + tranexamic acid (Transamin S) 1A+ hemocoagulase (Reptilase-S 1A proteolysis enzyme) (drip).
• Enzyme inhibitor: ulinastatin (Miraclid) 300000 unit/day + maintenance fluid (T4-solution) 400ml (drip). • Proteolysis enzyme: gabexate mesilate (FOY) 1 SOO-2000mg + maintenance fluid (T4-solution) 200ml
(drip). • Antiepileptic phenytoin-phenobarbital (Aleviatin) 2S0mg + saline 20ml (i.v.), flush saline 20ml, Aleviatin
12S mg + saline 20 ml (i.v.). • Adsorbed tetanus toxoid O.S ml (i.m.) + human antitetanus immunoglobulin 2S0 IU (i.m.). • Anesthesia: midazola (20A) + maintenance fluid (T4-soution) 160ml drip 1 ml/h-1 combined drip with
pancuronium bromide (Myoblock) 20A + T4-solution 160ml, and buprenophine hydrochloride (Lepetan) 3-SA + saline 100 ml.
• Heparin calcium (Hepacarin) SOOO U + saline 100 ml drip, S ml/h to prevent complication of Sj02 monitoring.
• Blood transfusion for Hb < 10 mg/dl.

Appendix. Critical Pathway of Brain Hypothermia Treatment 299
Stage 2.5.
Brain monitoring and management:
• CPP > 80 mmHg. • ICP < 20 mmHg. • Sj02: 70%-80%. • Trend EEG. • ABER.
Care management of ICP (1) Prevent venous stasis by management of neck position, mediastinal pressure, abdominal hyperten-
sion, full stomach, and bladder pressure. (2) Diagnose the effectiveness of CSF drainage by changes in ICP during 3 min open/close drainage. (3) Continuous CSF drainage. (4) Manage hypercapnia. (S) Replacement of serum albumin to 3.S mg/dl. (6) Head-up position. (7) Management of hyperglycemia and serum electrolytes. (8) Control of blood pressure. (9) Administration of manitol 100 ml/30-60 min.
Stage 2.6.
Monitoring and management of systemic homodynamic changes: CI > 2.2, D021 > SOO, V021 > 12S, 02ER 22-26%, SVRI 1800-2S00, and PAWP > 8-12 mmHg.
• Management of cardiac disturbances: (1) Preload disturbances: administration of crystalloid, colloid, diuretics, and dopamine 1-3Ilg/ml min-1•
(2) Contraction disturbances: administration of dobutrex and/or PDE-III inhibitor. (3) After load disturbances: administration of noradrenalin and/or Ca blocker. (4) Electric imbalance: Na, K, Mg, IP, and Ca.
• Neuronal oxygenation: (1) Pa02/ Fi02> 300-3S0. (2) Manage neck position. (3) Check the correct position of intubation tube. (4) Control mechanical ventilation volume 10-1Sml/kg, PEEP 3-ScmH20, auto-sigh 20-2Sml/kg. (S) Management of red blood cells: Hb > 11 mg/dl, DPG 12-14Ilmol/ml, inorganic phosphate> 3.0 mg/dl.
• Laboratory examinations: blood gas analysis every 2 h, complete blood cell count, serum glucose, serum albumin, IP, Mg, AT-III, D-dimer, a2-PI, SFMC, PF1+2, APC, and platelet aggregation.
• MRSA bacterial analysis. • Gastrointestinal examination and management: gastric juice from N/G tube < 200 ml/day.

Sta
ge
2. A
lgo
rith
m m
anag
emen
t
• S
erum
glu
cose
< 1
60 m
g/dl
: 1.
E
arly
bra
in h
ypot
herm
ia (
33°
-34°
G) i
nduc
tion
with
in 3
h a
fte
r br
ain
dam
age.
Gat
echo
lam
ines
sur
ge-a
ssoc
iate
d hy
perg
lyce
mia
sho
uld
be m
inim
ized
. 2.
R
epla
cem
ent
of
insu
lin.
3.
No
adm
inis
trat
ion
of c
ortis
ol.
4.
Act
ivat
e pr
otei
n sy
nthe
sis
of m
uscl
e by
adm
inis
trat
ion
of a
rgin
ine,
sal
buta
mol
, cl
enbu
tero
l, gl
utam
ine.
5.
In
hibi
t pr
otei
n ca
tabo
lism
: am
urin
one.
6.
R
ehab
ilita
tion
and
kine
tic t
hera
py.
• 5
0 2 >
70
0 m
llmin
and
SS
P>
100
mm
Hg:
1.
F
luid
res
usci
tatio
n, a
dmin
istr
atio
n of
nor
epin
ephr
ine
+ d
opto
rex.
2.
E
last
ic b
anda
ging
of
extr
emiti
es.
3.
Tem
pora
ry i
nser
tion
of a
bdom
inal
bal
loon
cat
hete
r in
to t
he a
bdom
inal
aor
ta.
• H
emog
lobi
n dy
sfun
ctio
n:
1.
Con
trol
of
seru
m p
H>
7.3
. 2.
S
erum
glu
cose
12
0-1
40
mg/
dl.
3.
Ser
um i
norg
anic
pho
spha
te 3
-5 m
g/dl
and
mag
nesi
um 1
.4-1
.Bm
Eq/
1.
4.
Ser
um a
lbu
min
> 3
.5m
g/dl
, vi
tam
in A
50
-10
0m
g/d
l.
• A
T-I
II>
100
%:
repl
acem
ent
of s
erum
alb
umin
. •
Hyp
okal
emia
: co
ntro
l K+
at
3.5
-4.5
mE
q/1
by d
rip o
f K
GI
1 A,
dilu
ted
with
BO
ml
salin
e.
Rep
lace
men
t sp
eed:
40
mllh
for
ser
um K
+ <
2.0
mE
q/1.
20
ml/h
for
ser
um K
+: 1
.2-2
.5 m
Eq/
1.
15 m
l/h f
or s
erum
K+:
2.6
-3.0
mE
q/1.
10
ml/h
for
ser
um K
+: 2
3.1
-3.0
5 m
Eq/
1.
5 m
llh f
or s
erum
K+:
3.6
-34
.0 m
Eq/
1.
VJ 8 ;g ~ ~
0..
?<
" ()
;:l . .....
(S. a '"0
I>' So
~ ~ o """ tIl "' ~. ~ ~ o .....
::r
~ §. I>' ~
~
I>' S ~ ~

Appendix. Critical Pathway of Brain Hypothermia Treatment 301
Stage 3.1.
Basic care plan:
• Restoration of injured brain tissue. • Maintaining neuronal oxygenation. • Metabolic balance. • Maintaining lipid metabolism. • Management of ICP and brain edema. • Careful management of BBB function. • Control of immune dysfunction. • Maintaining neurohormonal function. • Nutritional consideration. • Prevention of infections.
The major target of leu management at the cooling stage are:
Stage 3.2.
Care order:
• Systolic blood pressure (SBP): control between at 120-160 mmHg by fluid resuscitation. • SBP> 170 mmHg hypertension: drip antihypertensive drug diltiazem hydrochloride (Helvesser). 250 mg.
diluted with 100 ml saline at 2 mllh. Complication of bradycardia (HR < 50 bpm): nicardipine hydrochloride (Perdipin) 2-5 ~g/kg min-1.
• Blood gases: Pa02 > 100 mmHg. Pa02/Fi02 ratio> 350. PaC02 35 mmHg. • Urine volume: more than 0.5 ml/kg h-1.
• Serum glucose: 12Q-140mg/dl by drip of rapid-action insulin (Humarin R): 50U diluted with 100ml saline. * Administration speed: start with 2 ml/h and slow to 1 ml/h after serum glucose becomes lower than
200mg/dl. • Serum potassium: control at 3.S-4.5 mEq/1 by drip of KCI 1 A. diluted with 80 ml saline.
* Replacement speed: 40 ml/h for serum K+ < 2.0 mEq/1. * 20 ml/h for serum K+ 1.2-2.5 mEq/1. * 15ml/h for serum K+ 2.6-3.0mEq/l. * 10ml/h for serum K+ 23.1-3.0SmEq/l. * 5 ml/h for serum K+ 3.6-34.0 mEq/1.

302 Appendix. Critical Pathway of Brain Hypothermia Treatment
Stage 3.3.
Intervention:
• Ventilator management. • Ventricular drainage. • ICP monitoring. • Sj02 monitoring. • Monitoring of cardiac output and 02ER. • Insert ileum gastric tube. • Kinetic therapy using dyna care bed. • Microdialysis monitoring.
Stage 3.4.
Intravenous medication:
• Fluid resuscitation: 7% Acetic acid Ringer solution (Veen F) + H2 receptor antagonist (Zantac SOmg/A) + metoclopramide (Prinmperan) 1 A + panthenol (pantol SOO mg x 2).
• Maintenance fluid: combination of physiosol-3 SOO ml, Amicaliq SOO ml, and Hicaliq SOO ml (drip). • Administration of vitamins C and E, and ZnCI2 •
• Enzyme inhibitor: ulinastatin (Miraclid) 300000U/day + maintenance fluid (T4-solution) 400ml (drip). • Proteolysis enzyme: gabexate mesilate (FOY) 1 SOO-2000mg + maintenance fluid (T4-solution) 200ml
(drip). • Vitamin kit: vitamin C SOOmg, vitamin B1 SOmg, vitamin B2 20mg, vitamin 6 20mg (i.v.). • Antiepileptic medicine: phenytoin-phenobarbital (Aleviatin) 2S0mg + saline 20ml (i.v.), flush saline
20 ml, Aleviatin 12S mg + saline 20 ml (i.v.). • Antibiotics: immipenem cilastain sodium (Tienam 1-2g/day x 3) > meropenem trihydrate (Meropn,
1.0-2.0g/day x 4) for enterobacteria, gram-negative bacteria, and pseudomonas. • Anesthesia: midazolam (20A) + maintenance fluid (T4-solution) 160ml drip 1 ml/h, combined drip with
pancuronium bromide (Myoblock) 20A + T 4-solution 160 ml, and buprenophine hydrochloride (Lepetan) 3-SA + saline 100 ml.
• Heparin calcium (Hepacarin) SOOO U + saline 100 ml drip, S ml/h to prevent complication of Sj02 monitoring.
• Blood transfusion for Hb > 10 mg/dl.
Appendix. Critical Pathway of Brain Hypothermia Treatment 303
Stage 3.5.
Brain monitoring and management:
• Cpp > 80 mmHg. • ICP < 20 mmHg. • Sj02 70%-80%. • Trend EEG. • ABER. • CT. • Brain tissue temperature.
Stage 3.6. - -
Monitoring and management of systemic homodynamic changes: CI > 2.2,0021> 500, V021 > 125, 02ER 22%-26%, SVRI 1800-2500, and PAWP > 8-12 mmHg.
• Management of cardiac disturbances: (1) Preload disturbances: administration of crystalloid, colloid, diuretics, and dopamine 1-3Ilg/ml min-1•
(2) Contraction disturbances: administration of dobutrex and/or POE-III inhibitor. (3) After load disturbances: administration of noradrenalin and/or Ca blocker. (4) Electric imbalance: Na, K, Mg, IP, and Ca.
• Neuronal oxygenation: (1) PaOiFi02 > 300-350. (2) Manage neck position. (3) Check the correct position of intubation tube. (4) Controlled mechanical ventilation volume 10-15 ml/kg, PEEP 3-5cmH20, auto-sigh 20-25ml/kg. (5) Management of red blood cells: Hb> 11 g/dl, OPG 12-14Ilmol/ml, inorganic phosphate >3.0mg/dl.
• Water balance: intake/output each 8 hours. • Laboratory examinations: blood gases analysis every 2 h, complete blood cell count, serum glucose, serum
albumin, IP, Mg, AT-III, D-dimer, a.2-PI, SFMC, PF1 + 2, APC, and platelet aggregation. • MRSA bacterial analysis. • Gastrointestinal examination and care management: gastric juice from N/G tubes <200 ml/day, abdominal X-ray,
nutritional consideration with management of BBB dysfunction (CSF/serum albumin ratio <0.01), and special enteral care management. Cetraxate hydrochloride (Neuer-S), L-glutamine (Glumin-S), Antibiotic-resistent lactic acid bacteria (Biofermin-R), potassium permanganate, and Oaiken Tyutou are enteral management drugs.
Sta
ge
3. A
lgo
rith
m m
anag
emen
t
1.
Inte
rmit
ten
t h
ypo
the
rmia
: pr
olon
ged
brai
n hy
poth
erm
ia,
belo
w 3
2°
-33
°C
, pro
duce
s a
redu
ctio
n of
pitu
itary
hor
mon
es.
Def
icie
ncy
of g
row
th h
orm
one
and
thyr
oid
horm
ones
cau
ses
an u
navo
idab
le d
eple
tion
of i
mm
une
func
tion.
To
prev
ent
this
com
plic
atio
n, i
nter
mitt
ent
cont
rol
of b
rain
tis
sue
tem
pera
tu
re b
etw
een
32°
C a
nd 3
4°C
is a
ver
y us
eful
man
agem
ent t
echn
ique
. T
he t
empo
rary
ele
vatio
n of
bra
in t
issu
e te
mpe
ratu
re is
rec
omm
ende
d at
18
00
-22
00
ho
urs
beca
use
phys
iolo
gica
l gr
owth
hor
mon
e is
nat
ural
ly r
elea
sed
at t
his
time.
The
det
aile
d te
chni
ques
are
des
crib
ed p
revi
ousl
y in
thi
s bo
ok.
2.
Bra
in e
de
ma
an
d c
on
tro
l o
f IC
P <
15
mm
Hg
: IC
P e
leva
tion
to m
ore
than
20
mm
Hg
prod
uces
ven
ous
stas
is a
nd d
istu
rban
ces
of m
icro
circ
ulat
ion.
To
prev
ent
mic
roci
rcul
atio
n, C
SF
dra
inag
e, h
ead-
up p
ositi
on,
redu
ctio
n of
abd
omin
al p
ress
ure
and
med
iast
inal
pre
ssur
e, p
reve
ntio
n of
hyp
o-al
bum
inem
ia,
adm
inis
trat
ion
of h
yper
-osm
otic
sol
utio
n, m
anito
l, an
d re
duct
ion
of C
SF
pro
duct
ion
by a
ceta
zola
mid
e (D
iam
ox)
are
pres
crib
ed m
anag
emen
t. 3.
A
T-I
II>
100
%:
perip
hera
l va
scul
ar s
tasi
s is
one
of t
he c
ompl
icat
ions
of
the
cool
ing
stag
e of
bra
in h
ypot
herm
ia.
Pro
long
ed b
ed r
est,
perip
hera
l va
scul
ar
cont
ract
ion,
sub
cuta
neou
s ed
ema
caus
ed b
y th
e co
mpl
icat
ion
of h
ypo-
albu
min
emia
, co
mpl
icat
ion
of i
nfec
tion,
and
con
sum
ptio
n on
of
AT
-III
by s
ever
e br
ain
dam
age
are
caus
es o
f re
duct
ed o
f AT-
III.
Low
er t
han
80
%-9
0%
of
AT-
III i
s cr
itica
l an
d pr
omot
es t
he s
yste
mic
dis
turb
ance
of
mic
roci
rcul
atio
n an
d de
velo
pmen
t of i
nfla
mm
atio
n of
vas
cula
r in
timae
. O
ur c
linic
al s
tudi
es s
ugge
st th
e m
anag
emen
t of A
T-III
affe
cts
to p
rogn
osis
and
suc
cess
of b
rain
hyp
othe
rm
ia t
reat
men
t. 4.
S
eru
m a
lbu
min
>3.
5 m
g/d
l: p
rolo
nged
hyp
othe
rmia
pro
mot
er s
ynth
esis
of
prot
ein
and
albu
min
. In
crea
sing
cyt
okin
es p
rodu
ces
hypo
-alb
umin
emia
. In
se
vere
ly b
rain
-inju
red
patie
nts,
rap
id d
evel
opm
ent
of h
ypo-
albu
min
emia
is a
big
clin
ical
iss
ue.
Pro
gres
sion
of
brai
n ed
ema,
ine
ffect
ive
man
itol
hype
ros
mot
ic d
iure
tics
for
brai
n ed
ema,
com
plic
atio
n of
pul
mon
ary
edem
a, i
ntes
tinal
muc
ous
edem
a pa
ncre
atic
duc
t obs
truc
tion
caus
ed b
y in
test
inal
wal
l ede
ma,
im
mun
e dy
sfun
ctio
n, b
acte
rial
tran
sloc
atio
n, u
nsta
ble
phar
mac
olog
ical
fun
ctio
n of
pro
tein
-bin
ding
dru
gs,
incr
ease
d fr
ee b
acte
ria a
nd e
ase
of i
nfec
tion
are
maj
or c
ompl
icat
ions
of
hypo
-alb
umin
emia
. T
here
fore
, re
plac
emen
t of
alb
umin
and
nut
ritio
nal c
onsi
dera
tion
for
hypo
-alb
umin
emia
are
impo
rtan
t m
an
agem
ent
stra
tegi
es d
urin
g th
e co
olin
g st
age
of b
rain
hyp
othe
rmia
tre
atm
ent.
5.
Imm
un
e d
ysfu
nct
ion
: re
duce
d gr
owth
hor
mon
e le
vels
and
ene
rgy
cris
is in
lym
phoc
ytes
are
maj
or c
ause
s of
imm
une
dysf
unct
ion
durin
g br
ain
hypo
ther
m
ia t
reat
men
t. T
he r
educ
tion
of g
row
th h
orm
one
is u
navo
idab
le w
ith p
rolo
nged
mod
erat
e br
ain
hypo
ther
mia
bec
ause
the
tem
pera
ture
of
the
pitu
itary
gl
and
is a
lso
low
ered
. G
luta
min
e is
the
ene
rgy
sour
ce f
or ly
mph
ocyt
es a
nd i
s pr
oduc
ed in
lun
g tis
sue
and
skel
etal
mus
cles
. T
his
glut
amin
e is
exp
ende
d by
lym
phoc
ytes
in
the
inte
stin
al d
iges
tive
orga
ns.
The
refo
re,
mus
cle
hypo
met
abol
ism
, pu
lmon
ary
infe
ctio
n, a
nd m
ucou
s ed
ema
in t
he d
iges
tive
orga
n ca
used
by
hypo
-alb
umin
emia
als
o pr
oduc
e im
mun
e dy
sfun
ctio
n. A
dmin
istr
atio
n of
arg
inin
e, s
albu
tam
ol,
and
grow
th h
orm
one
are
effe
ctiv
e in
mai
ntai
nin
g im
mun
e fu
nctio
n be
caus
e of
stim
ulat
ion
of p
rote
in s
ynth
esis
in
skel
etal
mus
cles
and
pro
mot
ion
of t
he l
ipid
met
abol
ism
whi
ch i
s th
e m
ain
met
abo
lism
und
er h
ypot
herm
ia.
6.
Pre
ven
tio
n o
f in
fect
ion
: co
mpl
icat
ion
with
sev
ere
infe
ctio
n du
ring
the
cool
ing
stag
e ca
uses
the
fai
lure
of
brai
n hy
poth
erm
ia t
reat
men
t. In
crea
sed
seru
m
proi
nfla
mm
ator
y cy
toki
nes
can
perm
eate
the
dam
aged
BB
B a
nd p
rodu
ce c
ytok
ine
ence
phal
itis
with
unc
ontr
olla
ble
incr
ease
s of
neu
roto
xic
glut
amat
e in
in
jure
d br
ain
tissu
e. T
here
fore
, as
man
agem
ent
of in
fect
ion
durin
g br
ain
hypo
ther
mia
trea
tmen
t, th
e ki
lling
of
bact
eria
, ac
tivat
ion
of im
mun
e fu
nctio
n, t
he
man
agem
ent
of B
BB
(C
SF
/ser
um a
lbum
in r
atio
<0.
01),
man
agem
ent
of s
erum
alb
umin
(>3
.5 g
/dl),
no
activ
atio
n of
vas
opre
ssin
rel
ease
by
neur
al c
ontr
ol
of t
he f
eedb
ack
mec
hani
sm t
o hy
perg
lyce
mia
, m
aint
enan
ce o
f pr
otei
n sy
nthe
sis
in s
kele
tal
mus
cles
, an
d ad
min
istr
atio
n of
bac
teria
-sen
sitiv
e no
n-pr
otei
nbi
ndin
g an
tibio
tics
are
indi
cate
d. T
he i
nter
mitt
ent
cont
rol
of b
rain
tis
sue
tem
pera
ture
at
32
°-3
3°
C, a
dmin
istr
atio
n of
arg
inin
e, a
nd r
ehab
ilita
tion
of s
kele
ta
l m
uscl
es a
re a
lso
effe
ctiv
e to
inc
reas
e th
e im
mun
e fu
nctio
n. T
he c
hoic
e of
sys
tem
ic a
dmin
istr
atio
n of
ant
ibio
tics
and
dige
stiv
e de
cont
amin
atio
n an
tibio
tics
ther
apy
was
des
crib
ed p
revi
ousl
y in
thi
s bo
ok.
7.
Act
iva
tio
n o
f lip
id m
eta
bo
lism
: br
ain
hypo
ther
mia
bel
ow 3
4°C
pro
duce
s m
etab
olic
shi
ft fr
om g
luco
se to
lipi
d m
etab
olis
m.
The
lipi
d m
etab
olis
m r
equi
res
vita
min
A a
nd a
dequ
ate
grow
th h
orm
one
for
ener
gy m
etab
olis
m w
ithou
t la
ctat
e pr
oduc
tion.
Exc
essi
ve r
epla
cem
ent
of g
row
th h
orm
one
prod
uces
hyp
er
glyc
emia
. T
here
fore
, ca
refu
l m
onito
ring
of s
erum
glu
cose
is
impo
rtan
t fo
r re
plac
emen
t th
erap
y of
gro
wth
hor
mon
e an
d ar
gini
ne.
w ss: ;J>
'0
'0
(1l ;:;
0.. ?<' ~ (S
. a '"0
Il:l So
~
~ o ....,
to .., Il:
l S· ::r: ~ o So
(1l S ;. ~
(1l
Il:l 8' (1l g

Appendix. Critical Pathway of Brain Hypothermia Treatment 305
Stage 4.1.
Basic care plan:
Rewarning can occur after exact diagnosis of some form of recovery. The recording of a 9 wave on the background of the 8 wave in trend EEG, no ICP elevation, Sj02 control at 60%-70%, and no brain swelling on CT scan are basic signs of neuronal recovery. To succeed in rewarming from brain hypothermia treatment, various preconditioning managements are needed.
Stage 4.2.
Care order:
Rewarming from brain hypothermia, especially prolonged treatment below 34°C, produces various physiological changes such as metabolic shift from lipid to glucose, vascular engorgement, increased of metabolic activity, activated cytokine production, increase in ·NO radicals, increased serum cytokines, uncoupling of bloodflow and metabolism in major organs, and oxygen demand in the brain tissue. Before rewarming, preconditioning management is recommended for adaptation or prevention of negative effects to the brain by these physiological changes. The major targets for preconditioning care are:
• No severe infection. • Lymphocytes> 1500/mm3. • T-H (CD4) lymph >55%. • Serum glucose 120-140 mg/dl. • Prealbumin >20 mg/dl. • Serum albumin >3.5 mg/dl. • Vitamin A >50 mg/dl. • Hb> 12mg/dl. • 02ER 23%-25%. • AT-III> 100%. • Gastric pHi> 7.35.
The success of management ensures no trouble during rewarming.

306 Appendix. Critical Pathway of Brain Hypothermia Treatment
Stage 4.3.
Intervention:
• EEG (recovery from () wave to 8 wave or recording of a wave ). • ABR. • Brain CT (no signs of brain swelling or severe brain edema). • ICP «20mmHg). • CPP (>70-80 mmHg). • Prevention of systemic infection by combined administration of antibiotics:
(1) Digestive decontamination: control of clostridium enteritis and MRSA by enteral administration of levofloxacin (Cravit, 200 mg) and Amphotericin B, 100-300 mg.
(2) Combined with vancomycin for (2-3g/day x 4-6 times i.v. drip) is useful prophylactic management for rewarming stage infection.
Stage 4.4.
Intravenous medication:
• Maintenance fluid: combination of physiosol-3 500 ml, amicaliq 500 ml, 7% acetic acid Ringer solution (Veen F) and hicaliq 500ml (drip). Calorie increases with monitoring of serum glucose.
• Administration of vitamins C and E, and ZnCI2. • Enzyme inhibitor: ulinastatin (Miraclid) 300000U/day+maintenance fluid (T4-solution) 400ml (drip). • Proteolysis enzyme: gabexate mesilate (FOY) 1500-2000 mg + maintenance fluid (T 4-solution)
200ml (drip). • Antiepileptic phenytoin-phenobarbital, Aleviatin 125mg + saline 20ml (i.v.), prepare the flush saline
20ml. • Antibiotics: arbekacin sulfate (Habekacin, 150-200 mg/day x 2) to prevent pseudomonal aerginosa and
MRSA infection, + cefozopran hydrochloride (Firstcin 1-2g/day x 2) for Tienam resistant Acinetobacter and xantomona + fluconazole (Diflucan 100-200 mg/day x 1) for Candida with evidence of B-D-Glucanpositive reactions).
• Anesthesia: midazola (20A) + maintenance fluid (T4-soution) 160ml drip 1 ml/h, combined drip with pancuronium bromide (Myoblock) 20A + T 4-solution 160 ml, and buprenophine hydrochloride (Lepetan) 3-5A + saline 100 ml.
• Heparin calcium (Hepacarin) 5000 U + saline 100 ml drip, 5 ml/h to prevent complication of Sj02 monitoring.
• Blood transfusion for Hb < 10 mg/dl.

Appendix. Critical Pathway of Brain Hypothermia Treatment 307
Stage 4.5.
Brain monitoring and management:
• CPP > 80 mmHg. • ICP > 20 mmHg. • Sj02 70%-80%. • Trend EEG (recovery from 8 wave to e wave or recording of a wave). • ABER. • Brain CT (no signs of brain swelling, severe brain edema or ICP elevation).
Stage 4.6.
Monitoring and management of systemic homodynamic changes: CI > 2.2,0021> SOO, \/021> 12S, 02ER 22%-26%, SVRI 1800-2S00, and PAWP > 8-12mmHg.
• Management of cardiac disturbances: (1) Preload disturbances: administration of crystalloid, colloid, diuretics, and dopamine 1-3Ilg/ml min-1•
(2) Contraction disturbances: administration of dobutrex and/or PDE·III inhibitor. (3) After load disturbances: administration of noradrenalin and/or Ca blocker. (4) Electric imbalance: Na, K, Mg, IP, and Ca.
• Neuronal oxygenation: (1) Pa02/Fi02> 300-3S0. (2) Manage neck position. (3) Check the correct position of intubation tube. (4) Controlled mechanical ventilation volume 10-1Sml/kg, PEEP 3-ScmH20, auto-sigh 20-2Sml/kg. (S) Management of red blood cells: Hb > 11 mg/dl, DPG 12-14Ilmol/ml, inorganic phosphate >3.0mg/dl.
• Water balance: intake/output every 8 hours. • Laboratory examinations: PaC02 32-36mmHg, serum glucose 120-1S0mmHg, serum albumin
>3.Smg/dl, IP > 3mg/dl, AT-III> 120%, D-dimer. • Gastrointestinal examination and management:
(1) Gastric juice from N/G tubes <200 ml/day. (2) Abdominal X-ray. (3) Nutritional consideration for management of BBB dysfunction (CSF/serum albumin ratio <0.01). (4) Special enteral care management.
* Cetraxate hydrochloride (Neuer-S), L-glutamine (Glumin-S), antibiotic-resistant lactic acid bacteria (Biofermin-R), potassium permanganate, and Daiken Tyutou are enteral management drugs.
* The management of digastrics decontamination with nonabsorbable and hypothermia-active antibiotics levofloxacin (Cravit, 200 mg) and amphotericin B, 100-300 mg, combined with intravenous drip administration of Vancomycin (2-3g/day x 4-6 times) are indicated for prevention of systemic infections.
Sta
ge
4.
Alg
ori
thm
ma
na
ge
me
nt
1.
Evi
de
nce
of
ne
uro
na
l re
cove
ry:
the
big
issu
e at
rew
arm
ing
is r
epro
gres
sion
of
brai
n in
jury
mec
hani
sm t
hat
was
sto
pped
at
the
cool
ing
stag
e. W
ithou
t ev
iden
ce o
f ne
uron
al r
ecov
ery
or a
t le
ast s
igns
of
reco
very
, re
war
min
g m
akes
the
cond
ition
muc
h w
orse
. If
neur
onal
rec
ov
ery
was
not
dia
gnos
ed b
y m
onito
ring
of I
CP
, S
j02,
EE
G,
and
CS
F b
ioch
emic
al c
hang
es,
the
cool
ing
stag
e sh
ould
be
exte
nded
for
a f
ew
mor
e da
ys.
Man
agem
ent
is s
ame
as S
tand
ard
Man
agem
ent,
Sta
ge 4
.1.
Bas
ic C
are
Pla
n, S
tage
4.2
. C
are
Ord
er,
Sta
ge 4
.3.
Inte
rven
tio
n, S
tage
4.4
. In
trav
enou
s M
edic
atio
n, S
tage
4.5
. B
rain
Mon
itorin
g, S
tage
4.6
. M
onito
ring
and
Man
agem
ent
of S
yste
mic
Hom
odyn
amic
C
hang
es,
and
Alg
orith
m M
anag
emen
t. N
o si
gns
of b
rain
ede
ma
or
othe
r co
mpl
icat
ions
on
the
CT
exa
min
atio
n ar
e al
so u
sefu
l to
dia
gno
se n
euro
nal
reco
very
. 2.
N
o s
eve
re i
nfe
ctio
n a
nd
CS
F/s
eru
m A
lbu
min
<0.
01:
the
elev
atio
n of
bod
y te
mpe
ratu
re b
y re
war
min
g st
imul
ates
the
act
ivity
of
seru
m
cyto
kine
s. I
ncre
ased
ser
um c
ytok
ines
can
eas
ily p
erm
eate
the
dam
aged
BB
B.
Thi
s se
rious
com
plic
atio
n ca
uses
the
fai
lure
of
the
brai
n hy
poth
erm
ia t
reat
men
t at
the
rew
arm
ing
stag
e. T
here
fore
, m
anag
emen
t of
sev
ere
pulm
onar
y in
fect
ion
and
man
agem
ent
of B
BB
dys
fu
nctio
n (C
SF
/ser
um a
lbum
in r
atio
low
er t
han
0.01
) m
ust
be a
chie
ved
befo
re r
ewar
min
g. T
he a
ctua
l m
anag
emen
t m
etho
d is
des
crib
ed
prev
ious
ly in
thi
s bo
ok.
3.
Se
rum
glu
cose
12
0-1
40
mg/
dl:
adm
inis
trat
ion
of i
nsul
in w
ith c
ontr
ol o
f se
rum
pho
spha
te a
nd m
agne
sium
, 7%
ace
tate
Rin
ger
solu
tion,
co
ntra
indi
cate
d st
eroi
d, a
ctiv
ate
resp
irato
ry m
uscl
e m
etab
olis
m b
y sa
lbut
amol
. 4.
E
nte
ral
nu
trit
ion
: th
e m
anag
emen
t of
nut
ritio
n at
the
rew
arm
ing
stag
e re
quire
s th
e re
plac
emen
t of
an
ener
gy s
ourc
e of
cal
orie
s, f
eed
to i
mm
une
cells
, st
abili
zatio
n of
the
int
estin
al d
iges
tive
orga
n, a
nd m
aint
enan
ce o
f nu
triti
onal
con
ditio
ns.
The
man
agem
ent
of B
BB
dys
fu
nctio
n is
als
o im
port
ant
beca
use
neur
otox
ic g
luta
mat
e in
crea
ses
abou
t tw
o to
thr
ee t
imes
with
ent
eral
and
par
ente
ral
amin
o ac
id n
utri
tion.
In
wel
l-or
gani
zed
BB
B w
ith C
SF
/ser
um a
lbum
in r
atio
low
er th
an 0
.01,
mic
rodi
alys
is s
tudi
es p
rovi
ded
no e
vide
nce
of s
erum
glu
tam
ate
pass
ing
into
the
bra
in t
issu
e an
d no
evi
denc
e of
wor
seni
ng b
rain
ede
ma.
P
relim
inar
y m
anag
emen
t of
BB
B d
ysfu
nctio
n w
ith r
epla
cem
ent
of s
erum
alb
umin
to
high
er th
an 3
.5 g
/dl,
anti-
infla
mm
ator
y m
edic
ine
for
the
vasc
ula
r w
all
such
as
AT-
III a
nd p
rote
in C
, an
d ra
dica
l sc
aven
ger
such
as
Rad
icut
are
use
ful
to a
void
nut
ritio
nal
com
plic
atio
ns a
t th
e re
war
min
g st
age.
The
rep
lace
men
t of
ser
um a
lbum
in i
s ve
ry e
ffec
tive
for
the
cont
rol
of i
ntes
tinal
muc
ous
mem
bran
e ed
ema
and
pre
vent
ion
of d
iarr
hea
caus
ed b
y en
tera
l nu
triti
on.
Pre
limin
ary
feed
ing
(with
glu
tam
ine
and
argi
nine
), c
orre
ct s
erum
ele
ctro
lyte
s, c
ontr
ol o
f th
e os
mot
ic g
ap (
seru
m O
sm -
2 (s
tool
Na
+ K
) >
100
mO
smkl
kg)
and
man
agem
ent
of m
esen
teri
c is
chem
ia a
re a
lso
usef
ul b
efor
e fe
edin
g m
anag
emen
t. T
wo
actu
al e
nter
al n
utrit
ion
cour
ses
are
prep
ared
. O
ne u
ses
salin
e im
mun
e nu
triti
on (
glut
amin
e +
arg
inin
e +
yea
st R
NA
) w
ith a
dmin
is
trat
ion
of h
oney
yog
urt,
and
cont
rol
of B
BB
fun
ctio
n at
CS
F/s
erum
alb
umin
rat
io l
ower
than
0.0
1. T
he o
ther
is t
wo-
step
ent
eral
nut
ritio
n w
ith C
SF
/ser
um a
lbum
in 0
.01
-0.0
2.
Firs
t st
ep:
salin
e 50
ml
to m
ax 1
50 m
l/4 h
, an
d re
mov
e re
tent
ion
fluid
rep
eat
for
3-4
day
s. S
econ
d st
age:
adm
inis
trat
ion
of h
oney
yog
urt
(50
ml
to m
ax 1
50 m
ll4 h
). T
he d
etai
l te
chni
ques
are
des
crib
ed e
arlie
r in
thi
s bo
ok.
The
com
bina
tio
n of
ent
eral
nut
ritio
n w
ith h
oney
yog
urt
and
argi
nine
is v
ery
effe
ctiv
e fo
r st
imul
atio
n of
lip
id m
etab
olis
m w
ithou
t pr
oduc
tion
of l
acta
te.
V)
o 00
~
'"d (1) ::l
0..
?<" Q
.... ri· e:..
'"d
~ ~ ~ '-<
: a to ... ~ Er :r: '-<
: '"
d o .... ::r
(1) §. ~ ~
(1) ~ 8' (1
) a
Appendix. Critical Pathway of Brain Hypothermia Treatment 309
Stage 5.1.
Basic care plan:
• Rewarming from mild brain hypothermia can be performed with increases of brain tissue temperature of 0.1 DC/h.
• However, rewarming from 32D-33DC requires an adaptation time for uncoupling between metabolic changes and blood flow at 34D-35DC for about 1-2 days.
Stage 5.2.
Care order:
• Systolic blood pressure (SBP): control between at 120-160 mmHg by fluid resuscitation. • SBP> 170mmHg hypertension: drip the antihypertensive drug, diltiazem hydrochloride (Helvesser),
250 mg, diluted with 100 ml saline at 2 ml/h. Complication of bradycardia (HR < 50 bpm): nicardipine hydrochloride (Perdipin) 2-5llg/kg min-'.
• Blood gases: Pa02 > 100 mmHg, PaOiFi02 ratio >350, PaC02 35 mmHg. • Urine volume: more than 0.5 ml/kg h-'. • Serum glucose: 120-140 mg/dl by drip of rapid-action insulin (Humarin R) 50 U diluted with 100 ml saline.
* Administration speed: start at 2 mllh and slow to 1 ml/h after serum glucose becomes lower than 200mg/dl.
• Serum potassium: control at 3.5-4.5 mEq/1 by drip of KCI 1 A, diluted with 80 ml saline. * Replacement speed: 40 ml/h for serum K+ < 2.0 mEq/1. * 20 ml/h for serum K+ 1.2-2.5 mEq/1. * 15 ml/h for serum K+ 2.6-3.0 mEq/1. * 10ml/h for serum K+ 23.1-3.05mEq/l. * 5 ml/h for serum K+ 3.6-34.0 mEq/1.

310 Appendix. Critical Pathway of Brain Hypothermia Treatment
Stage 5.3.
Intervention:
• Change ileus tube to ED tube. • Digestive decontamination for control of clostridium enteritis and MRSA by enteral
administration of levofloxacin (Cravit, 200 mg) and amphotericin B (100-300 mg). • Combine with vancomycin (2-3g/day x 4-6 times i.v. drip) is useful prophylactic man
agement of rewarming stage infections.
Stage 5.4.
Intravenous medication:
• Maintenance fluid: hicaliq-1 700 ml + amizet XS 300 ml + 10% NaCI 2A + zantac 20A + panrol 500 mg x 2 (drip).
• Administration of vitamins S, C, and E, and ZnCI2. • Proteolysis enzyme: gabexate mesilate (FOY) 1500-2000 mg + maintenance fluid (Solita T 4-solution)
200ml (drip). • Antiepileptic phenytoin-phenobarbital, Aleviatin 125 mg + saline 20 ml (i.v.) , prepare the flush saline
20ml. • Change the antibiotics: arbekacin sulfate (Habekacin, 150-200 mg/day x 2) to prevent pseudomonal
aerginosa and MRSA infection, + cefozopran hydrochloride (Firstcin 1-2g/day x 2) for Tienam-resistant Acinetobacter and xantomona + fluconazole (Diflucan 100-200 mg/day x 1) for Candida with evidence of ~-D-glucan positive reactions) .
• Anesthesia: midazolam (20A) + maintenance fluid (T 4-soution) 160 ml drip 1 ml/h, combined drip with pancuronium bromide (Myoblock) 20A + T4-solution 160ml, and buprenophine hydrochloride (Lepetan) 3-5A + saline 100 ml.
• Heparin calcium (Hepacarin) 5000 U + saline 100 ml drip, 5 ml/h for prevent to complication Sj02 monitoring.

Appendix. Critical Pathway of Brain Hypothermia Treatment 311
Stage 5.5.
Brain monitoring and managment:
• ICP < 25 mmHg. • Sj0 2 60%-75%. • CPP > 80 mmHg. • ABER. • CT.
Stage 5.6. - -
Monitoring and management of systemic homodynamic changes: CI > 2.2,0021> 500, V021 > 125, 02ER 22%-26%, SVRI 1800-2500, and PAWP> 8-12mmHg.
• Management of cardiac disturbances: (1) Preload disturbances: administration of crystalloid, colloid, diuretics, and dopamine 1-3Ilg/ml min-1.
(2) Contraction disturbances: administration of dobutrex and/or POE-III inhibitor. (3) After load disturbances: administration of noradrenalin and/or Ca blocker. (4) Electric imbalance: Na, K, Mg, IP, and Ca.
• Neuronal oxygenation: (1) PaOiFi02 > 300-350. (2) Manage neck position. (3) Check correct intubation tube position. (4) Controlled mechanical ventilation volume 10-15ml/kg, PEEP 3-5cmH20, auto-sigh 20-25ml/kg. (5) Management of red blood cells: Hb> 11 mg/dl, OPG 12-14IlmollmL, inorganic phosphate >3.0mg/dl.
• Water balance: intake/output every 8 hours (two times/day). • Laboratory examinations: PaC02: 32-36mmHg, serum glucose 120-150mg/dl, serum albumin >3.5mg/dl,
IP > 3mg/dl, AT-III> 120%, O-dimer, platelet. • Gastro-intestinal examination and care management:
(1) Gastric juice from N/G tube abdominal X-ray, nutritional consideration for management of BBB dysfunction (CSF/serum albumin ratio <0.01).
(2) Special enteric care management. Cetraxate hydrochloride (Neuer-S), L-glutamine (Glumin-S), antibioticresistant lactic acid bacteria (Biofermin-R), potassium permanganate, and Oaiken Tyutou are enteric management drugs.
(3) The management of digastrics decontamination with nonabsorbable and hypothermia-active antibiotics (combination of levofloxacin (Cravit, 200 mg) and amphotericin B, 100-300 mg).
(4) Combined intravenous drip of vancomycin (2-3g/day x 4-6 times) and administration of enteric nutrition are indicated to prevent systemic infections.

Sta
ge
5. A
lgo
rith
m m
anag
emen
t
• T
he
con
tro
l o
f b
rain
tis
sue
tem
per
atu
re:
rew
arm
ing
from
sho
rt-d
urat
ion
brai
n hy
poth
erm
ia is
not
diff
icul
t, ho
wev
er,
rew
arm
ing
from
pro
long
ed b
rain
hyp
othe
rmia
pro
duce
s m
any
nega
tive
effe
cts
on t
he i
njur
ed b
rain
tis
sue.
Ste
p w
ise
rew
arm
ing
to 3
4°C
and
the
n an
ada
ptat
ion
time
of 1
-2 d
ays
is v
ery
succ
essf
ul f
or r
ewar
min
g fr
om p
rolo
nged
mod
er
ate
brai
n hy
poth
erm
ia tr
eatm
ent.
Afte
r th
at,
the
cool
ing
blan
ket
is r
emov
e fr
om t
he b
ody
piec
e by
pie
ce o
ver
1-2
da
ys.
Thi
s ca
refu
l re
war
min
g te
chni
que
for
prol
onge
d br
ain
hypo
ther
mia
tre
atm
ent
is o
ne o
f th
e ke
y po
ints
for
su
cces
s of
bra
in h
ypot
herm
ia t
reat
men
t. •
Pre
ven
tio
n o
f h
yper
gly
cem
ia:
adm
inis
trat
ion
of i
nsul
in b
y dr
ip i
s us
eful
for
the
con
trol
of
hype
rgly
cem
ia.
In t
his
stag
e, g
row
th h
orm
one
to i
ncre
ase
the
imm
une
activ
ity is
not
rec
omm
ende
d, b
ecau
se t
his
mak
es c
ontr
ol o
f hy
per
glyc
emia
diff
icul
t be
caus
e of
incr
easi
ng s
erum
glu
cose
. M
icro
dial
ysis
stu
dies
sug
gest
tha
t co
ntro
l of
ser
um g
luco
se
at 1
30
-15
0 m
g/dl
is
effe
ctiv
e.
• O
xyg
en m
etab
oli
sm:
the
oxyg
en d
eman
d in
crea
ses
durin
g th
e re
war
min
g st
age.
The
con
trol
of
oxyg
en d
eliv
ery
over
700
ml/m
in,
Pa
OiF
i02
> 3
50,
and
02E
R 2
3%
-35
% a
re f
unda
men
tal.
To m
aint
ain
hem
oglo
bin
func
tion,
the
co
ntro
l of
Pa
C0
2 3
2-3
6m
mH
g,
seru
m p
H 7
.3-7
.4,
seru
m p
hosp
hate
>3m
g/dl
, an
d se
rum
Mg+
> 1
.3m
mol
/dl
are
also
im
port
ant.
The
maj
or p
itfal
l of
oxy
gen
man
agem
ent
at t
he r
ewar
min
g st
age
is t
he e
arly
man
agem
ent
of s
pon
tane
ous
brea
thin
g w
ithou
t su
ffici
ent
oxyg
en d
eliv
ery
and
cont
rol
of h
emog
lobi
n dy
sfun
ctio
n. S
pont
aneo
us b
reat
hin
g is
effe
ctiv
e to
avo
id p
ulm
onar
y at
elec
tasi
s, h
owev
er,
oxyg
en d
eman
d al
so i
ncre
ases
. S
pont
aneo
us b
reat
hing
ca
n ca
use
brai
n hy
poxi
a w
ith p
oor
oxyg
en d
eliv
ery
and
hem
oglo
bin
DP
G r
educ
tion.
Thi
s is
the
las
t pi
tfall
of u
nsuc
ce
ssfu
l br
ain
hypo
ther
mia
tre
atm
ent.
Ven
tilat
or b
reat
hing
m
anag
emen
t sh
ould
be
us
ed
until
the
end
sta
ge o
f re
war
min
g un
der
anes
thes
ia,
anal
gesi
a, a
nd m
uscl
e re
laxa
tion.
•
Infe
ctio
us
con
tro
l: t
he w
orse
ning
of
infe
ctio
n at
the
rew
arm
ing
stag
e is
rar
e w
ith g
ood
man
agem
ent
of p
reco
ndi
tioni
ng.
The
man
agem
ent
tech
niqu
e to
con
trol
inf
ectio
n is
ver
y di
ffere
nt a
s pr
evio
usly
des
crib
ed.
Infe
ctio
us c
ontr
ol
durin
g th
e co
olin
g st
age,
alg
orith
m m
anag
emen
t m
etho
d fo
r in
fect
ion
cont
rol,
and
man
agem
ent
at t
he p
reco
ndi
tioni
ng s
tage
hav
e re
duce
d th
e co
mpl
icat
ion
of p
neum
onia
to l
ess
than
10%
in o
ur IC
U.
The
com
plic
atio
n of
sev
ere
pulm
onar
y in
fect
ion
with
se
vere
B
BB
da
mag
e (C
SF
/ser
um
albu
min
>
0.0
1-0
.02
) pr
oduc
es
chem
ical
cy
toki
ne
ence
phal
itis.
The
com
plic
atio
n of
sev
ere
infe
ctio
n du
ring
brai
n hy
poth
erm
ia in
dica
tes
failu
re o
f the
trea
tmen
t. C
aref
ul
man
agem
ent
of i
nfec
tion
durin
g br
ain
hypo
ther
mia
tre
atm
ent
is i
mpo
rtan
t.
w
......
N ~
"0
(D
:::s
0..
?<" n a· o· e:..
"0
." s :E ~ o ....,
tc
"1
." s· ~ o s- (D S s;.
::;l
(D
." §' (D g

Appendix. Critical Pathway of Brain Hypothermia Treatment 313
Stage 6.1.
Basic care plan:
The basic treatments for the restoration of vegetative patients after brain hypothermia treatment are:
• The management techniques to prevent the release of dopamine at the acute stage was discussed in the algorithm care management section and earlier in this book.
• The major restoration therapy for vegetation is the management of the dopamine A 10 nervous system. The various neuronal injury patterns in the dopamine A 10 nervous system can be considered in vegetate patients: (1) No functioning of the dopamine A 10 nervous system, however, remaining dopamine very resistant
to the management of CBF and brain metabolism. (2) Synaptic confusion in the dopamine A 10 nervous system is caused by retention of neurotransmit
ters in interstitial space. (3) Reduced metabolic substrates for production of synaptic dopamine. (4) Feeble dopamine synapses.
• The replacement of metabolic substrates of dopamine neurotransmitters could be through: (1) Pharmacological replacement. (2) Electrophysiological stimulation of the dopamine A 10 nervous system. (3) Increasing activity of the dopamine A 10 nervous system by hormonal therapy, and monitoring of
the dopamine A 10 nervous system responsiveness.
Stage 6.2.
Care order:
• Systolic blood pressure (SBP): control between 120-160 mmHg by fluid resuscitation. • Blood gases: Pa02 > 100 mmHg, PaOiFi02 ratio >350, PaC02 35 mmHg. • Urine volume: more than 0.5 mllkg h-1 .
• Serum glucose: 120-140 mg/dl by drip of rapid-action insulin (Humarin R): 50 U diluted with 100 ml saline.
• Serum potassium: control at 3.5-4.5 mEq/1. • Serum magnesium: control> 1.0 mmol/I. • Serum inorganic phosphate: 2.5-4.5 mg/dl. • Prolactin: male 2-18ng/ml, female 2-30ng/ml. • T 4-throxin: free 0.8-1.8 ng/dl, total 4.5-12/lg/dl. • Estron: male 29-81 pg/mL, female 40-150pg/ml.

314 Appendix. Critical Pathway of Brain Hypothermia Treatment
Stage 6.3.
Intervention:
• Electrical median nerve stimulation for 3 weeks: 10-20mA, 20s on, 30s off, 30 pulse/s, duration time 300 ms.
• Emotional stimulation: music therapy and talking.
Stage 6.4.
Medication:
• Intracerebral dopamine replacement therapy: Levodopa (300-400 mg/day) Amantadine (100-200 mg/day) Parodel (10-15 mg/day).
• Estrogen (Estraderm TTS patch 2 mg/day) patch therapy. • Antiepileptic therapy. • Replacement of vitamin B.

Appendix. Critical Pathway of Brain Hypothermia Treatment 315
Stage 6.5.
Brain monitoring and management:
• CSF neurotransmitter analysis: dopamine, norepinephrine, and serotonin. • Responsiveness of dopamine A 10 nervous system: increasing of CSF dopamine/CSF
prolactin ratio after treatment. • EEG. • CT. • MRI. • Xe-CBF. • Somatosensory evoked potential (extend N20 position or disappearance of N20). • Visual evoked potential (extend the P300 300 msec positive wave).
Stage 6.6.
Monitoring and management of systemic homodynamic changes:
• SBP > 100 mmHg, 02ER 22%-26%. • Management of cardiac function. • Electric imbalance: Na, K, Mg, IP, and Ca. • Neuronal oxygenation:
PaOiFi02 > 300-350 Hb> 11 mg/dl DPG 12-14 ~mol/ml inorganic Phosphate >3.0 mg/dl.
• Water balance: Ht < 40. • Laboratory examinations:
Serum glucose 120-150 mmHg Serum albumin >3.5 mg/dl AT-III> 120%.
Sta
ge
6.
Alg
ori
thm
ma
na
ge
me
nt
• D
op
am
ine
re
pla
cem
en
t th
era
py:
do
pam
ine
repl
acem
ent
ther
apy
prov
ider
su
ppor
t fo
r th
e no
n-fu
nctio
ning
do
pam
ine
A 1
0 ne
rvou
s sy
stem
. T
he r
espo
nsiv
enes
s of
the
dop
amin
e A
10
nerv
ous
syst
em c
an b
e di
agno
sed
by
the
incr
ease
d C
SF
dop
amin
e/pr
olac
tin r
atio
eve
n w
ith n
o ne
urol
ogic
al r
espo
nse.
Ou
r cl
inic
al r
esea
rch
sugg
este
d th
at t
he C
SF
-dop
amin
e/pr
olac
tin r
atio
inc
reas
ed b
etw
een
3 an
d 14
day
s af
ter
mus
ic e
mot
iona
l st
imul
atio
n an
d re
cord
ed n
euro
nal
reco
very
fro
m v
eget
atio
n. N
o pa
tient
s re
cove
red
from
veg
etat
ion
with
out
resp
onse
of
the
CS
F
dopa
min
e/pr
olac
tin
ratio
. E
ffect
ive
stim
ulat
ion
of t
he d
opam
ine
A 1
0 ne
rvou
s sy
stem
in
clud
es p
harm
acol
ogic
al
dopa
min
e re
plac
emen
t th
erap
y, e
stro
gen
patc
h th
erap
y,
med
ian
nerv
e st
imul
atio
n, a
nd m
usic
the
rapy
. T
he b
ig
resp
onse
s of
the
CS
F d
opam
ine/
prol
actin
rat
io t
o em
otio
nal
body
con
tact
and
mus
ic t
hera
py w
ere
impr
essi
ve.
How
ever
, m
ore
effe
ctiv
e m
etho
ds o
f ac
tivat
ion
of t
he d
opam
ine
A 1
0 ne
rvou
s sy
stem
are
stil
l un
der
rese
arch
. •
Re
sto
rati
on
th
era
py
for
veg
eta
tio
n:
in t
he c
hron
ic s
tage
, re
spon
se o
f th
e do
pam
ine
A 1
0 ne
rvou
s sy
stem
sho
wn
as i
ncre
ased
of
CS
F d
opam
ine/
prol
actin
rat
io i
s an
ess
entia
l fa
ctor
fo
r su
cces
sful
neu
rona
l re
cove
ry f
rom
veg
eta
tion.
How
ever
, co
rtic
al n
euro
nal
resp
onse
is
also
im
port
ant
for
rest
orat
ion
from
veg
etat
ion.
Ou
r pr
elim
inar
y cl
inic
al
stud
ies
of n
euro
tran
smitt
er r
espo
nsiv
enes
s us
ing
mus
ic t
hera
py s
ugge
sted
tha
t in
crea
sed
CS
F e
pine
phrin
e an
d ho
mov
anill
ic
acid
, an
d sm
all
resp
onse
s of
C
SF
al
anin
e,
glut
amin
e,
and
5-hy
drox
yind
olea
cetic
ac
id
sugg
est
good
pro
gnos
is f
or
reco
very
fro
m t
he v
eget
ativ
e st
ate.
H
owev
er,
incr
ease
s of
CS
F a
lani
ne,
glut
amin
e, a
nd 5
-hy
drox
yind
olea
cetic
aci
d ar
e ne
gativ
e in
dica
tion
for
vege
tatio
n th
erap
y.
It w
as
surp
risin
g th
at t
he
rele
ase
of
neur
otox
ic n
euro
tran
smitt
ers
was
rec
orde
d in
res
pons
e to
em
otio
nal
mus
ic s
timul
atio
n in
cas
es o
f po
or p
rogn
osis
fo
r re
cove
ry f
rom
veg
etat
ion.
Res
pons
e of
the
dop
amin
e A
10
nerv
ous
syst
em a
nd d
opam
ine
and
nore
pine
phri
ne
rele
asin
g ne
uron
s,
and
slig
ht r
espo
nses
of
neur
otox
ic t
rans
mitt
er-r
elea
sing
ne
uron
s ar
e im
port
ant
fact
ors
for
reco
very
fro
m v
eget
atio
n. T
he m
echa
nism
of
prol
onge
d br
ain
dam
age
and
the
resp
onsi
vene
ss o
f ne
urot
oxic
tran
sm
itter
rel
ease
to
emot
iona
l st
imul
atio
n m
ust
be c
onsi
dere
d fu
rthe
r. I
ntra
cere
bral
dop
amin
e re
plac
emen
t th
erap
y an
d su
ppre
ssio
n of
the
neu
rona
l act
ivity
that
rel
ease
r gl
utam
ate,
ala
nine
, an
d 5-
hydr
oxyi
ndol
eace
tic a
cid
is a
n ar
ea
of f
utur
e tr
eatm
ent.
• N
eu
rore
ha
bili
tati
on
: th
e ea
rly p
lann
ing
of n
euro
reha
bilit
atio
n is
ver
y im
port
ant.
How
ever
, th
is b
ook
does
not
di
scus
s ne
uror
ehab
ilita
tion
ther
apy.
w
......
0'1 >
"0
"0
(J) t::l
0..
~. ~ "'"
~
'i:I
po So
:;:; ~ o """ t;O .., po S" ~ o So
(J) .., 3 ;"
~
(J)
po s (J
) a

Appendix. Critical Pathway of Brain Hypothermia Treatment 317
Management of dopamine A 10 nervous system in severely brain-injured patients
1. Acute stage: prevent dopamine release and use radical scavengers Prevent dopamine release in hypothalamus by administration of metoclopramide Brain hypothermia: 32°-34°C, prevent cerebral dopamine release and radical attack to the dopamine A 10 nervous system Replacement of prolactin and thyroid hormone Administration of radical scavengers
2. Chronic stage: activate dopamine A 10 nervous system Cerebral dopamine replacement therapy
Pharmacological treatment: Levodopa (300-400 mg/day), Amantadine (100-200 mg/day) Uptake of cerebral dopamine: Estrogen (Estraderm TIS Patch 2 mg/day) Median nerve stimulation: 1 0-20 mA 20s on 30s off, 30 pulse/s, duration time 30m/s
Music therapy

Subject Index
A A10 nervous system 75,82,83,89,90,106,237 abdominal hypertension 186 abdominal pressure 122,186,222 acute brain swelling 46, 78 acute onset of cerebral infarction 254 acute renal failure 214
-: basic management 213 -: complication 214 -: diagnosis 213 -: information 213 -: medication 213 -: pathophysiology 213 -: special consideration 214
adequate oxygenation 78, 106, 138 alcohol cooling 131 algorithm
- care management 278 - for ICP elevation 202 - for low blood pressure 202 - for malnutrition and diarrhea 211 - for pulmonary infection 202 - for renal insufficiency 211 - for unstable brain tissue temperature 199 - management 205,279,281,282,284,286,288
- of brain tissue temperature 200 - of hypotension: medication 203 - system 198
aluminum sheet 132 anaerobic brain metabolism 79,111 anaerobic metabolism 79 analgesic agents 145 anesthesia for surgery 141 antibiotics 112, 151,230 anti-Ca++ 171 anti-epieptic medicines 187 antimicrobial therapy 195 antipyretics medication 201 antithrombin III (AT-III) 71,122,150,152 apoptosis 30 arginin 116 aspiration pneumonia 173 atmospheric pressure 133, 159,228
automatic control device for hypothermia 127 autoregulation mechanism 46
B bacterial infection 193 bacterial translocation 194,231 basic care plan 278,279,281,283,285,287 beam balance 16 bed design for brain hypothermia 132 behavior 243
- disturbances 243 behavioral outcome 3 beta-amyloid precursor protein (beta-APP) 14 beyond indication and contraindication 98 biochemical CSF monitor 161,229 biochemical monitoring 229 biphasic effects of hypothalamus-pituitary-adrenal
(HPA) 56 bladder temperature 19,227 blood core temperature 77 blood gases 148 blood-borne exogenous neurotransmiter 25 blood-brain barrier (BBB) 3,25, 139, 190
- dysfunction 64,66,70,103,111,118,137,140, 172,220
- function 69 brain
- !bladder temperature ratio 223 - cooling technique 126 - damage by hypothalamus-pituitary-adrenal
neurohormonal excess reactions 68 - damage caused by hyperglycemia 62 - edema 44, 78 - hypoxia 79 - injury mechanism 48 - ischemia 47 - metabolism 47,71,143,161,162 - monitoring and management 279,280,282,284,
286,287 - oxygen metabolism 154 - stem infarction 255 - swelling 44
319

320 Subject Index
- temperature 49 - thermo-pooling 37,46,52,57,59,76,269 - thermo-regulation 136 - tissue glucose 66, 71, 86, 162, 179, 190 - tissue glutamate 84,139,162 - tissue glycerol 84 - tissue lactate 71,84, 179, 183 - tissue oxygen 161 - tissue pyruvate 72 - tissue temperature 57,58,96,120,125,137,225 - trauma 269
C Ca channel inhibitor 171 CAl hippocampal 10
- pathology 7 CAl hippocampus 9 cardiac arrest 7,9,250,268 cardiac index 155 cardiac muscle 152 cardiac output 96, 157 cardiopulmonary arrest 249 cardiopulmonary dysfunction 55 cardiopulmonary resuscitation 272 care management of systemic circulation 167 care map for sepsis 197 care order 278,280,281,283,285,287 catecholamine surge 55, 60, 64 CD4 immune functions 69 cerebral blood flow (CBF) 27, 77, 154
- and brain metabolism 136 - disturbance 57
- and brain metabolism 200 - thresholds for cell function 48
cerebral blood volume 46 cerebral dopamine replacement therapy 108 cerebral perfusion pressure (CPP) 59,112 cerebral resuscitation after cardiac arrest 251 cerebral thermal index (Cn) 154,155,226 cerebral vasospasm 260 c-fos 30 chronic histopathological and behavioral protection
10 coagulation 152 cognitive deficits 16, 243 cold water blanket technique 125, 128 coma 61 comparative indication 97 complete cerebrovascular obstruction (CVO) 254 complication of severe pulmonary infection 69 compromised patient 95 computed ICU management 199 computed tomography 147
concepts in brain tissue temperature control 120 continuous CSF drainage 262 continuous hemodiafiltration (CHDF) 129 contraction myocytolysis 64 contraindication 95, 97
- for brain hypothermia 173 cooling blanket 18, 165 cooling phase 196 cooling stage (Stage 3) 281 cooling suit 129
- technique 128 cooling water blanket 126 core temperature 18,142 cotton sheet 132 CPP and CBF 77 criteria for brain hypothermia 174 critical path management 277 critical path of brain hypothermia treatment 277 CSF
- cooling technique 129 - dopamine 162,246 - dopamine/prolactin ratio 89,241,242,245 - drainage 185 - epinephrine 162 - neurotransmitter 245 - /serum albumin ratio 69,88, 118 - -ILl 88 - -IL6 88
cyclic AMP 64 cytokine encephalitis 62,70,108,116,143 cytoskeletal pathology 14 cytotoxic brain edema 44
D debridement of necrotic contused brain tissue
143 decompressed semi-closed skull 159 delayed control of hyperglycemia 111 delayed HPA axis suppression by dopamine 81 delayed induction of brain hypothermia 103, 177 delayed vasospasm 259 design of the intensive care unit 133 diarrhea and nutrition
-: basic management 212 -: complications 212 -: diagnosis 211 -: information 211 -: medication 212 -: pathophysiology 211 -: special considerations 212
difference in brain injury mechanism in patients and experimental laboratory models 74
digastrics decontamination 108, 222

digestive organs 136 direct administration of oxygen 142 direct blood cooling hemodiafiltration technique
251 direct blood cooling system 130 direct brain injury 90 disseminated intravascular coagulability (DIe) 170,
195,197 - management 196
disturbances to memory 89 dobutrex 203 DOPAC 238 dopamine 203, 238
- A10 89 - central nervous system 237 - diagnosis of-nervous activity 241 - diagnostic method of responsiveness of the -
nervous system 89 - nervous 82, 83, 90
- system 75, 239 - -dominant systemic circulation 57 - metabolite 238 - nervous system 79 - replacement therapy 108,246
disphosphoglycerate (DPG) 63,114 - hemoglobin - 148,168,249,250
draining of subcutaneous CSF 143 duration of brain hypothermia 121, 124 dysoxia 156
E early induction of brain hypothermia 103,262 early induction of mild to moderate brain
hypothermia 85 early management of pulmonary infection 193 ebb phase 191 effectiveness of brain hypothermia 270 effectiveness of dopamine replacement therapy
246 efficacy of brain hypothermia 269 elastic bandage technique 148 electrocardiogram (ECG) 151 emergency cardiopulmonary bypass 251 emotional center 75,89,243 end tidal CO2 (ETC02) 167 enteral-intestinal 112 entry criteria 273 epinephrine 60 estrogen 237 excess release of vasopressin 74 excitatory amino acids 23 excitatory neurotransmitters 51 externally decompressed skull 46
F fibrinolysis 152 flow phase 191 fluid resuscitation 135
- at Induction Stage 170 fluid selection 188 fluorocarbon oxygen carrier 142 free radicals 24,83,103,182
Subject Index 321
fundamental technique of brain tissue temperature control 125
fungemia 197
G gastric lavage 154 gastric pHi 152, 170,231 gin reactions 48 glasgow outcome score 270 glucose metabolism 169 glutamate 23
- (IlmoIlL) 140 glycerol 140 glycogenesis of protein 81 growth hormone 69,195
H harmful stress stimulates the HPA axis 177 Hayashi catheter (H-catheter) 158,159 hazards of hypothermia 51 Hb-DPG 63,64,168,249,250 head position 148, 185 heat-generating medical devices 133 hemoglobin dysfunction 38,52,64,68,79,261 herniation 160 history of clinical trials of hypothermia 51 hsp70 30 hyperglycemia 61,64,111,149,178,219,255,262 hyper-metabolism 230 hyperthermia 18, 19,21 hypertonic crystalloid solutions 178 hypo-albuminemia 71,112,149,150 hypopituitarism 180 hypotension 21
-: basic management 203 -: complications 204 -: information 202 -: pathophysiology 203 -: special considerations 204
hypothalamus dysfunction 180 hypothalamus-pituitary-adrenal axis (HPA) 37,
55,250 - axis neurohormonal abnormality 254, 262 - axis stimulation 262

322 Subject Index
- dysfunction 90 - neurohormonal dysfunction 261 - stimulation 52
hypothermia anesthesia 51 hypoxia 21,156
I ICU management strategies 68 IL-10 32 immune dysfunction 69,117,191 immunocompromised host 193 improper management of brain hypothermia 110 inadequate brain temperature 71 inadequate nutrition 117 indication 97
- and criteria for dopamine replacement therapy 246
- of rewarming 214 - to stop hypothermia 198
indirect evaluation methods of monitoring 137 indirect method of brain hypothermia 125 indirect parameter of BBB dysfunction 139 induction of brain hypothermia treatment 165
- stage 1 278 - stage 2 279
ineffective oxygen inhalation 249 infection 192 infectious control 69,192-194 inflammatory cytokine 10 initial management 85 inner consciousness 235 inner cool by celsius control system 129 insertion of catheter 157 insulin resisted hyperglycemia 38, 60, 81, 104, 245,
249,261 intensive care management 108 interleukin-1 beta 30 internal jugular venous blood temperature 58, 77 intervention 278, 280, 281, 283, 285, 287 intestinal mucous membrane edema 112 intra-abdominal balloon catheter 80 intra-abdominal balloon pumping 251 intracranial hypertension 45 intracranial pressure (ICP) 112,137,184,228
- elevation 45 - at the rewarming stage 229 -: basic management 205 -: complications 206 -: diagnosis 205 -: information 205 -: medication 206 -: pathophysiology 205 -: special considerations 206
intravenous medication 279-281, 284, 285 irrigation of brain tissue 142 ischemic brain insults 99 ischemic duration 9
J jugular venous blood catecholamines 81 jugular venous blood temperature 160,225 jugular venous oxygen saturation (Sj02) 160 J-wave (Osborn wave) 152
L L-arginine 195 late induction of brain hypothermia 104 lipid metabolism 169 lipid peroxidation 24, 172 localized tissue temperature 225 long-term effects 12 low molecular weight heparin 184 lymphocytopenia 69
M macronutrient 71, 189
- feedback mechanism 65 - intake 87
maintenance of cerebral blood flow (CBF) 148 maintenance of microcirculation 138 major targets of brain hypothermia treatment 52 management
- care point at each stage 113 - choice 87 - during the cooling stage 175 - of BBB dysfunction 183 - of blanket water temperature 126, 127 - of brain tissue temperature 125 - of cardiopulmonary function 167
- during brain hypothermia 250 - of cerebral vasospasm 263 - of CPP 80 - of digestive organs 188 - of dopamine A10 nervous system 239 - of emotion 243 - of hemoglobin dysfunction 178 - of HPA axis neurophormone dysfunction
179 - of metabolic substrates and hyperglycemia
168 - of microcirculation and vascular inflammation
170 - of neurohormonal dysfunction 80 - of neuronal oxygenation 168

- of pulmonary infection 196 - at rewarming stage 230
- of rewarming 224 - of serum glucose 219 - of swan ganz catheter 157 - plans for brain tissue temperature 107
manito I and glycerol 110 masking neuronal hypoxia 37,52,62,63,104,113,
114 mechanism
- after severe subarachnoid hemorrhage 263 - of brain damage 43, 74, 90 - of emotional disturbance 243 - of hyperglycemia 60 - of vegetation 237
median nerve stimulation 244 medication 287 memory 243 metabolic ebb phase 189, 190 metabolic flow phase 189, 190 metabolic shift from glucose to lipid 169 metabolic substrate 78 metabolism of macronutrients 179 microdialysis 71
- catheter 143 - monitor 143,161
micro nutrients 189 microtubule-associated protein 2 (MAP-2) 14 midazolam 145 mild brain hypothermia 51, 120, 176
- management 166 - treatment 120, 122
moderate brain hypothermia 107,120,121,135, 176
- management 166 - treatment 120, 123
monitor 135, 157 - for ICU management 138,143
monitoring 147 - and management of systemic homodynamic
changes 279,280,282,284,286,287 - at the rewarming stage 225 - brain tissue temperature 225 - cardiac output 155, 158 - ICP 157 - of tympanic membrane temperature 226 - jugular venous blood temperature 158 - tympanic membrane temperature 226 - vital signs 147
muscle relaxants 145,185 muscle weakness 220, 221 music therapy 239,242 myelinated axons 19 myeloperoxidase (MPO) 28
Subject Index 323
N neurohormonal BBB dysfunction 79 neuroimmune function 200 neuron protection 76,141 neuronal damage 3 neuronal function 136 neuronal hormones 177 neuronal hypoxia 148,174,263 neuronal restoration 38 neuronal toxicity by glutamate 183 neuropeptide Y 88
- receptors 183 neuroprotection 44
- by glia 48 - therapy 181
neuroprotective agent 171 neurotoxic hydroxide radicals 75 new brain injury mechanism after subarachnoid
hemorrhage 260 new concept of brain hypothermia treatment 85,
269 new concept of unconsciousness 237 NF-kappaB 28 NIH stroke scale 256 nitric oxide synthase (cNOS) 26 N02/N03 163
- ratio 182 NO radicals 82, 163, 182 non-filling 155 nonfunctioning antibiotics 112 noninvasive monitoring 138
- of brain damage 137 nonperfusing ventricular tachycardia 272 nonspecific brain damage 90 normothermia treatment 269 normovolemic fluid resuscitation 167,184 nutritional considerations 191,221
- at the rewarming stage 231 nutritional management 189
o occlusive cerebral stroke 254 OH- radical 104 old-age patients 61 osmotic management 185 other treatment 186 outer consciousness 231 outline of the critical path 278 oxygen consumption 64, 156 oxygen delivery 64,80,114,156 oxygen extraction ratio (02ER) 155 oxygenation 138
324 Subject Index
p
PaC02 148,188 Pa02IFi02 168,251 parasagittal fiuidpercussion 12 parenteral nutrition 118 pathophysiology 22 PCPS 251,272 personality 89 pharmacological cooling 131 pharmacological neuroprotection 170 pharmacological treatment 178
-: levodopa 244 - of muscle weakness 221
phenobarbital 187 pitfall of brain hypoxia and ischemia 62 pitfalls of brain hypothermia treatment 108,111,113 pitfalls of rcp management 186 pituitary hypothermia 180 pituitary hormones 69 pituitary hypo-function 117,191 platelet 152
- count 122 pneumoma
-: basic management 208 -: complications 209 -: diagnosis 208 -: information 208 -: medication 208 -: pathophysiology 208 -: special considerations 210
polymorphonuclear leukocytes (PMNLs) 28 poor enteral care management 192 poor filling ischemia 155 posthypothermia stage (Stage 6) 287 preconditioning for rewarming 219
- (Stage 4) 283 preliminary refrigeration 165 presynaptic glutamate inhibition 171 prevention
- of acute brain swelling 229 - of brain edema 173, 184, 229 - of brain thermo-pooling 181 - of brain tissue lactate 87 - of convulsion 187 - of dopamine release 239 - of excess release of cerebral dopamine 182 - of excess release of cerebral glutamate 182 - of hypokalemia 198 - of immune crisis 190 - of infection 138, 192 - of nitrous oxide radical 172 - of pulmonary obstruction 186 - of rewarming stress 123 - of selective damage to the hippocumpus 83
- of systemic infections 222 - of vasopressin release 172 - of vegetation 106,245
prognosis - brain trauma 270 - cardiac arrest 237
proinfiammatory cytokines 69 prolonged anesthesia 145 prolonged moderate hypothermia 69 propofol 145 protection of BBB 195 protein binding type antibiotics 151 protein kinase C activity 30 protein synthesis 51 protocol for brain hypothermia 106 pseudomonas aeruginosa 197 PTCA 251 pulmonary infection 115,116,139,194
Q QT interval less 174
R rapid induction of brain hypothermia 87 rapid induction of moderate brain hypothermia
110 rapid progression of hyperglycemia 87 rapid rewarming 20 reactive oxygen species 24 rebleeding of a silent hematoma 147 reduced Hb-DPG 114 reduced immune function 116 regulation mechanism of brain tissue temperature
58, 76 rehabilitation of muscle weakness 221 release of dopamine 75 release of vasopressin 88 removal of infectious source 194 reperfusion 59 restoration therapy 68
- for injured neurons 176 reversibility of severe brain injury 98 reversibility of the vegetative state 241 rewarming 124
- clinical issues for management of- 217 - from mild brain hypothermia 224 - from moderate brain hypothermia 224 - phase 20,196 - stage (Stage 5) 285 - time 108, 123, 124, 217
rubber sheet 132

S sadation 185 safe induction of moderate brain hypothermia 127 selection of mild or moderate brain hypothermia
treatment 107 selective brain-cooling technique 125 selective OH- attack 82 selective radical damage of dopamine AlO 79,90,
106,237 semi-closed skull 157 sepsis 195 serum albumin 220 serum glucose 252, 261 serum magnesium 171,222 serum N02 and N02/N03 ratio 104 serum phosphate 222 shock patients 177 short duration of brain hypothermia 68, 115, 124 sick euthroid syndrome 238 Sj02 137 slow onset of cerebral infarction 255 slow rewarming 20 spatial memory performance 16 Spiel Berg ICP sensor 158 spinal cord ischemia 16 stabilize autonomic nerve reactions 201 stage care plan 277 standard care 278 standard management 279,281,283,285,287 staphylococcus aureus 197 steroid 79, 172
- administration 44 stimulation of the HPA axis 74 strategies for management of ischemic brain 256 stress-associated hyperglycemia 61,177,260
- after cardiac arrest 252 stress-induced catecholamine surge 37 stress reactions 56 stress to the HPA-axis 38 subarachnoid hemorrhage 258 supporting cooling method 130 surgical considerations 142 surgical position 141 suspected acute coronary syndrome 247 Swan Ganz catheter 136 systemic hemometabolism 153, 156 systemic metabolic shift 115
T target of treatment of severe brain injury 78 TBI complicated by secondary hypoxia 20
Subject Index 325
technique of H-catheter insertion 160 technique of rewarming 224 thrombolytic agents 10 thrombomodulin 152 time schedule for management of brain tissue
temperature 121,166,175 transient MCA occlusion 7 transluminal coronary angioplasty (PTCA) 272 triple H therapy 170, 171, 256 two-step induction of hypothermia 173 tympanic membrane temperature 58, 154, 226
U unconsciousness 231,237 uncontrollable hyperglycemia 95 uncontrolled hyperglycemia 115 unstable immune functions 201 unstable metabolic conditions 201 unsuccessful cooling of brain tissue temperature
200 unsuccessful hypothermia treatment 68 uptake of cerebral dopamine 244 urinary drainage 153
V vancomycin 150 vascular engorgement 43, 181 vasogenic brain edema 44 vasopressin 65,168,190,258
- release 64, 81, 261 vasospasm 258-260 vegetative state 73,235,238 venous stasis 45 ventricular fibrillation 272 ventricular tachycardia (VT) 249 vitamin A 122
W washing the clot of basal cistern 262 waterfall pressure 45 whole brain tissue temperature 77
y young children 61
Z ZnCI 116