
Melanotic Schwannoma of Adrenal Gland - A Rare Entity/ Diagnostic Dilemma

Appendicolithiasis causing diagnostic dilemma: a rare cause of acute appendicitis (report of a case)
Tanısal ikileme neden olan apandikolitiyazis: Akut apandisitin nadir görülen bir sebebi (Olgu sunumu)
Zafer TEKE,1 Burhan KABAY,1 Halil ERB‹fi,1 Ömer Levent TUNCAY2
323
C o r r e s p o n d e n c e (‹ l e t i fl i m) : Zafer Teke, M.D. Kuflp›nar Ma h ., Emek Cad., Öykü Sitesi A-Blok No: 12 1 , K: 4 D: 1 0, 2 0 0 2 0 D e n i z l i, T u r k e y.Tel: +90 - 258 - 2 6 4 8 9 91 Fax ( F ak s): +90 - 258 - 213 49 22 e -m a i l ( e -p o s t a) : z t e k e _ m d @ y a h o o . c o m
Pamukkale Üniversitesi T›p Fakültesi, 1Genel Cerrahi A n abilim Dal›,2Üroloji A n abilim Dal›, Denizli.
D e p a r t m e n tsof 1General Surgery and 2U r o l o g y ,Medicine Faculty of Pamukkale University, Denizli, Turkey.
Apandikolitiyazis, apandis içerisinde tafllaflma meydana gel-mesi fleklinde tanımlanan bir durumdur. Apandis taflları, akutapandisitli hastalarda %10 oran›nda bulunur, fakat dahasıklıkla perfore apandisitte ve apse oluflumunda görülür. Bizburada genitoüriner sistemin akut hastalıklarını taklit eden vetanısal karıflıklı¤a neden olan apandikolitiyazise ba¤lı bir akutapandisit olgusu sunuyoruz. Otuz sekiz yaflındaki bir erkekhasta fliddetli, ani bafllangıçlı, tekrarlayan, sa¤ kasık bölgesinedo¤ru yayılan, bulantının efllik etti¤i kramp tarzı karın sa¤ altkadran a¤rısı ile acil servise baflvurdu. Fiziksel incelemedekarın sa¤ alt kadranda defans muskuler ve ribaund hassasiye-ti, sa¤ üreter trasesinde hassasiyet ve sa¤ kostovertebral açıhassasiyeti saptand›. Direkt grafide, sa¤ böbrek taflı ve karınsa¤ alt kadranda 3 cm çapında insidental opasite oldu¤u görül-dü. Hastaya apandektomi yapıldı. Tanı operasyonla ve apandi-kolitiyazisi gösteren apandektomi materyalinin direkt grafi-siyle konuldu. Akut apandisit, çeflitli genitoüriner hastalıklarfleklinde ortaya çıkabilir. Akut apandisitle birlikte veya birlik-te olmadan bir apandis taflı olasılı¤ı, akut alt karın ve pelvikhastalıkların ayırıcı tanısında ve sık görülen akut ürolojik has-talıklardan dolayı her zaman düflünülmelidir.
Anahtar Sözcükler: Akut apandisit; apandis taflı; apandikolitiyazis;ürolitiyazis.
Appendicolithiasis is a condition characterized by a concretionin the vermiform appendix. Appendicoliths are found in 10% ofpatients with acute appendicitis, but they are seen more frequent-ly in perforated appendicitis and in abscess formation. We here-in report a case of acute appendicitis due to appendicolithiasis,which mimics acute disorders of the genitourinary tract andcauses diagnostic confusion. A 3 8 - y e a r-old man presented to oure m e rgency department with a history of intense, acute, recurrent,crampy right lower quadrant pain radiating to the right groinregion, accompanied by nausea. Physical examination revealedmuscular defense and rebound tenderness in the right lowerquadrant, tenderness in the line of the right ureter and right cos-tovertebral angle tenderness. On X-ray examination, a right kid-ney stone was identified as was an incidental 3-cm density in theright lower quadrant. The patient underwent appendectomy. T h ediagnosis was made by operation and also X-ray examination ofthe appendectomy material showing appendicolithiasis. A c u t eappendicitis may manifest as a variety of genitourinary disor-ders. The possibility of an appendicolith with or without acuteappendicitis must always be considered in the differential diag-nosis of acute lower abdominal and pelvic disorders, and in theconsideration of common acute urological disorders.Key Words: Acute appendicitis; appendicolith; appendicolithiasis;urolithiasis.
Turkish Journal of Trauma & Emergency Surgery Ulus Travma Acil Cerrahi Derg 2008;14(4):323-325
Case Report Olgu Sunumu
Appendicolithiasis is a condition characterized bya concretion in the vermiform appendix. Most appen-dicoliths are fecaliths, stones composed of tightlypacked stool. A small minority are actual calculi,stones containing mineral deposits. It is believed thatby causing obstruction of the appendiceal lumen andsubsequent accumulation of mucus, appendicolithia-sis may favor the development of appendicitis.
Appendicoliths are found in 10% of patients withacute appendicitis, but they are seen more frequentlyin perforated appendicitis and in abscess formation.The appendix contains all the elements capable ofreproducing a colicky pain. Clinically, it has beennoted that pathological states that commonly aff e c tthis organ do not present as an acute intensive col-icky pain as may occur in urolithiasis.
Ulus Travma Acil Cerrahi Derg
Ekim - October 2008324
CASE REPORT
A 38-year-old man presented unaccompanied toour emergency department with a history ofintense, acute, recurrent, crampy right lower quad-rant pain radiating to the right groin region, accom-panied by nausea. The patient denied any anorexia,vomiting, fever, or urinary tract symptoms. Thepatient’s medical history revealed that he had aright kidney stone about 1.5 cm in diameter anddysuria due to nephrolithiasis 10 years before.Physical examination of the abdomen revealedmuscular defense and rebound tenderness in theright lower quadrant and tenderness in the line ofthe right ureter. Examination of the right flankrevealed right costovertebral angle tenderness.There was no palpable mass in the abdomen. Bowelsounds were hypoactive. Digital rectal examinationdid not elicit any pain or tenderness. The patient’stemperature was 38 °C and rectal temperature was39.3 °C. Laboratory tests included a white bloodcount of 22.800 cells per mm3 with 93.6% neu-
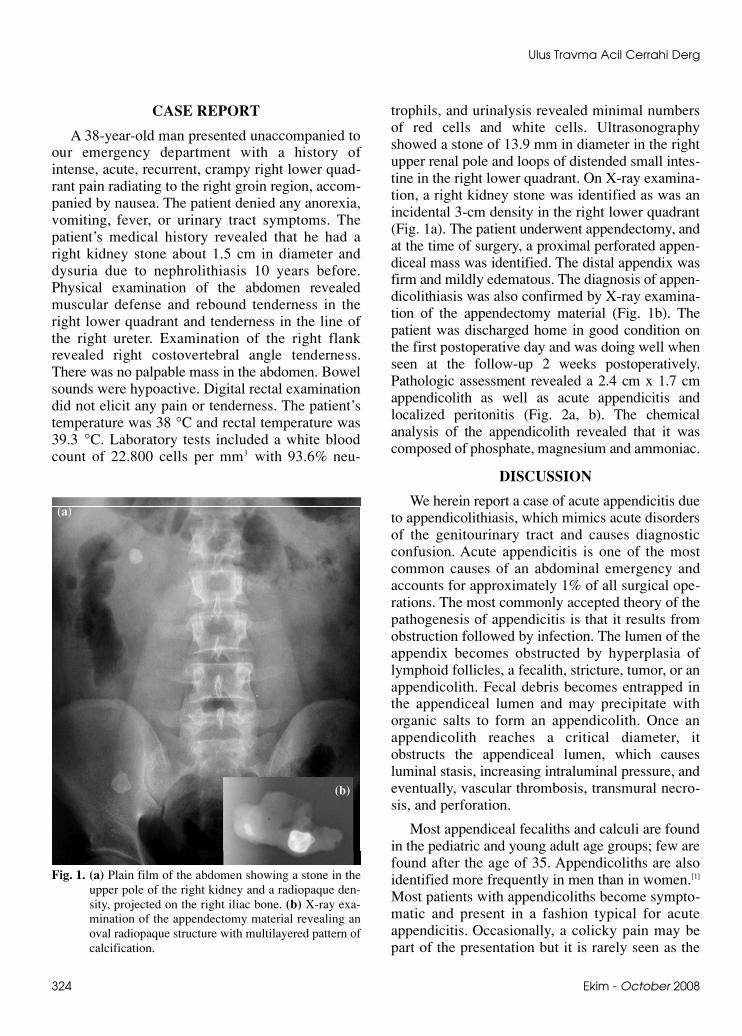
trophils, and urinalysis revealed minimal numbersof red cells and white cells. Ultrasonographyshowed a stone of 13.9 mm in diameter in the rightupper renal pole and loops of distended small intes-tine in the right lower quadrant. On X-ray examina-tion, a right kidney stone was identified as was anincidental 3-cm density in the right lower quadrant(Fig. 1a). The patient underwent appendectomy, andat the time of surg e r y, a proximal perforated appen-diceal mass was identified. The distal appendix wasfirm and mildly edematous. The diagnosis of appen-dicolithiasis was also confirmed by X-ray examina-tion of the appendectomy material (Fig. 1b). T h epatient was discharged home in good condition onthe first postoperative day and was doing well whenseen at the follow-up 2 weeks postoperatively.Pathologic assessment revealed a 2.4 cm x 1.7 cmappendicolith as well as acute appendicitis andlocalized peritonitis (Fig. 2a, b). The chemicalanalysis of the appendicolith revealed that it wascomposed of phosphate, magnesium and ammoniac.
DISCUSSION
We herein report a case of acute appendicitis dueto appendicolithiasis, which mimics acute disordersof the genitourinary tract and causes diagnosticconfusion. Acute appendicitis is one of the mostcommon causes of an abdominal emergency andaccounts for approximately 1% of all surgical ope-rations. The most commonly accepted theory of thepathogenesis of appendicitis is that it results fromobstruction followed by infection. The lumen of theappendix becomes obstructed by hyperplasia oflymphoid follicles, a fecalith, stricture, tumor, or anappendicolith. Fecal debris becomes entrapped inthe appendiceal lumen and may precipitate withorganic salts to form an appendicolith. Once anappendicolith reaches a critical diameter, itobstructs the appendiceal lumen, which causesluminal stasis, increasing intraluminal pressure, andeventually, vascular thrombosis, transmural necro-sis, and perforation.
Most appendiceal fecaliths and calculi are foundin the pediatric and young adult age groups; few arefound after the age of 35. Appendicoliths are alsoidentified more frequently in men than in women.[1]
Most patients with appendicoliths become sympto-matic and present in a fashion typical for acuteappendicitis. Occasionally, a colicky pain may bepart of the presentation but it is rarely seen as the
Fig. 1. (a) Plain film of the abdomen showing a stone in theupper pole of the right kidney and a radiopaque den-sity, projected on the right iliac bone. (b) X-ray exa-mination of the appendectomy material revealing anoval radiopaque structure with multilayered pattern ofcalcification.
(a)
(b)

Cilt - Vol. 14 Say› - No. 4 325
Appendicolithiasis causing diagnostic dilemma: a rare cause of acute appendicitis
main presenting complaint.[2,3] What was impressivein the present case was the presence of the colickypain caused by appendicolithiasis. The occurrenceof the appendiceal colic can be seen as arising fromthe contraction of an involuntary muscular tube thatis normally painless. The violence of the contrac-tion is usually produced in an effort to overcomesome obstacles that prevent the passage of normalexcretion or secretion. The pain is due to thestretching or distention of the tube such as typical-ly seen in cases of urolithiasis, which may presentwith or without microscopic or gross hematuria.Renal or ureteral colic in males does not alwaysradiate to the testis, and appendicitis can sometimesbe felt in the testicle and present as acute scrotum.[4]
There are some radiographic characteristics ofappendicoliths. Appendiceal calculi are solitary andlaminated. Although they are typically located inthe right lower quadrant, the location can vary withthe anatomy of the appendix. These characteristicshelp to differentiate them from other possible diag-noses, including ureteral stones, calcified pelvicphleboliths, and calcified mesenteric lymphnodes.[2,5,6] Stones must be sufficiently calcified toappear on plain films. In the present case, X-rayexamination of the abdomen revealed a right kid-ney stone and an incidental 3-cm density in theright lower quadrant. On ultrasound, appendicolithsare visible as bright echogenic foci with distalacoustic shadowing, but in this case, the appendi-colith could not be seen due to loops of the distend-ed small intestine in the right lower quadrant.
Acute appendicitis may manifest as a variety ofgenitourinary disorders, including gross hematuria,acute prostatitis and ureteral obstruction. T h eabove-presented case revealed more urological thanappendiceal characteristics clinically. This case ofappendicitis presented with a colicky pain suggest-ing a renal or ureteral stone, without microscopichematuria but with clinical evidence supportive ofa calculus and with his medical history. The possi-bility of an appendicolith with or without acuteappendicitis must always be considered in the dif-ferential diagnosis of acute lower abdominal andpelvic disorders, and in the consideration of com-mon acute urological disorders. As a result, we rec-ommend appendectomy for all patients with a radi-ographically confirmed appendicolith regardless ofthe symptomatology.
REFERENCES
1. Nitecki S, Karmeli R, Sarr MG. Appendiceal calculi andfecaliths as indications for appendectomy. Surg GynecolObstet 1990;171:185-8.
2. Cohen MS, Norris MA, Gruber MB, Warren MM. Caseprofile: appendicitis and appendicolithiasis presenting asureteral stone and colic. Urology 1981;18:623-4.
3. Haynes AL, Woodside JR. Periappendicitis presenting asleft renal colic. Urology 1980;16:611-3.
4. Ahmann TM. Appendicitis simulating torsion of the sper-matic cord: a case report. J Urol 1976;116:827.
5. Copeland EM, Long JM 3rd. Elective appendectomy forappendiceal calculus. Surg Gynecol Obstet1970;130:439-42.
6. Shin MS, Ho KJ. Appendicolith. Significance in acuteappendicitis and demonstration by computed tomogra-phy. Dig Dis Sci 1985;30:184-7.
Fig. 2. (a) Appendix delivered onto the surgical field at thetime of appendectomy demonstrates the proximalappendiceal mass. (b) Appendicolith and edematousdistal appendix.
(a)
(b)


















