Aphasia and Brain Organization

of 204
-
Upload
raisita-salas-castaneda -
Category
Documents
-
view
224 -
download
0
Transcript of Aphasia and Brain Organization
-
8/10/2019 Aphasia and Brain Organization
1/204
-
8/10/2019 Aphasia and Brain Organization
2/204
PH SI and
BR IN
ORG NIZ TION
-
8/10/2019 Aphasia and Brain Organization
3/204
-
8/10/2019 Aphasia and Brain Organization
4/204
P
H
S
I
n
d
B
R
I
N
O
R
G
N
I
Z
T
IO
N
lvarReinvang
Sum
ums
Hos
pital
m
ul
lustil
ulc of
Psy
cholo
gy
of
O
slo
Os
lo
mwa
y
S
PR
ING
ER
S
CIE
NC
E
BU
SIN
ES
SM
E
DIA
, L
LC
-
8/10/2019 Aphasia and Brain Organization
5/204
Library o
f Congress Ca
taloging
in
Pub
lication Data
Re
invang, lvar.
Aphasia and b
rain organizati
on.
A ppl
ied psycholing
uistics and com
municat ion di
sorders)
Bibliograph
y: p
Includes inde
x.
I
Aphasia.
2 Cogni t ive dis
orders.
3.B
ra in-
Woun
ds
an
d injuri
es-Complicati
ons
an
d sequelae.
4 Neuropsychol
ogy.
I
Title.
II Series.
R
C424.7.R45
1985
6 6.
85'52
85-9545
IS
BN 978-1-4757
-9216-4 ISB
N 978-1-4757-9
214-0 eBook)
DOI 10.1
007/978-1-4757
-9214-0
1985 Sp
ringer Science+
Business Media
New York
Originall
y published by P
lenum Press, Ne
w York in 1985
Softcov
er reprint
of
the
hardcover Ist ed
ition 198 5
All rights rese
rved
N o p
art of this b
ook may bc rep
roduced, store
d in a retrieval
system,
or
tr a
nsmitted,
in any form
or by any m
eans, electronic
, mechanical, p
hotocopying,
microfilming,
recording, o
r otherwise,
without wri t ten
permission fro
m the Publishe
r
-
8/10/2019 Aphasia and Brain Organization
6/204
PR
EF CE
This book
presents
t
he
work on aphas ia c
oming
out of
the
Ins t
i tute
for A ph
as ia a
nd
S
troke
in orw
ay during its
10
y
ears of exis
tence.
R ath
er
than
rev
iewing pre
vious ly
presen
ted
w o
rk, it
was my des ire
to give a
unified an
alysis
and discussion
of our acc
umula ted
data.
T heem
pirical bas i
s for
the
ana
lysis is a fa
irly lar ge
group 2
49
pa
tients)
inve
stigated
with
a s tand a
rd , com pre
hens ive
set
of proced
ures .
Tests of language functions
must
be developed
anew
for each
langua
ge,
but
com
parison o
f my findin
gs
withother recen t c
ompre-
h
ens ive s tu
dies of aph
asi a is facil
iated
by
clo
se parallels
i
n
tes tm e
th -
ods
C ha
pt er 2). The
classificat
ion sys tem
used is cur
rent ly
the m
ost
a
cceptedneu
rological sy
stem, b
ut
I
have opera
tionalized
it for resear
ch
purpo
ses
C
hapte r3).
The analy
ses
presented
are
based
on the view t
hat aphas ia is
an aspe
ct o f a m ul
t id imen s ion
al dis tu rba
nce of bra i
n function.
Find-
ings o
f associated
dis turban
ces and
vari
at ions
in the aphasic c
ondi t ion
over t ime
h
ave
b
een dismissed
b
y
some a
s irrelevan
t to
thestud
y
of
ap
has ia as a
languag e d
eficit. M y v
iew is
that this rich
and com ple
x
set of fin
dings give
s im
portant clues to
the
organiz
a t ion of b
ra in
func
tions
inhumans I
presen
t
analys
es of
the
re
la t ionship
of aphasia
to neuro
psychologi
cal disorde
rs
in
conce
ptual organ
ization,m e
mory ,
v
isuospatial
abilities
an
d
apraxia
C ha p ters
4 5,
and
6)
, and Is
tudy
the variat ions
wi
th
tim e o
f t
he
aphas
ic cond itio
n C hapte r
8).
N
o studyof
aphas ia is
complete
withou
t an
a
nalysisof
its clin-
ic
oanatom ic
al basis. Te
sting
the a
ssumptions
of the cl
assical mode
l
of a
phas ia , I c
an only pa
rt ly confirm
them. M
y analyses
reveal
that
-
8/10/2019 Aphasia and Brain Organization
7/204
vi
PREFACE
in many cases
interach ans
be
tween sev
erallesion
sites are
im
portant
in
deter
min ingd ef
icits
that
ar
e of ten
thought tohav
e a mo re c
ircum-
scribed clinicoanatomicalbasis.
In ta k
ing such a
broad v iew
of aphasia,
my
theoret
ical fram ew
ork
h
as been influenc
ed
by
conc
epts from g
enera l sy s
tems theor
y. The
theoretical
chaptersof
the book C
hapters1
and 9 presen
t and deve
lop
this
type of ap
proach suf
ficiently to
account fo
r the main
aspects of
my findings
an
d
to sugg
es t some
new lines o
f investiga
tion for
the
future.
I sh
ould l ike to
acknow le
dge the he
lp
and
su
pport of sev
eral
friends
and
colleagues. First of all, K
Sundet
perform ed the statistical
ana
lyses
an
d di
scussed all
th
e
st
atistical pr
oblems
with
m
e
P. B
arens te in ex
amined
my CT scans
and scored
the
m in
a s
tandard-
ized sys
tem.
K
W i
llmes
made available to
me
the
sy
s tem for an
alysis
of
CT
scan
s used
in the Aa c h en
aphas ia lab
oratory.
He also adv i
sed
me on problem
s of choos
ing app rop
riate s tatist
ical m odels
. My w ife,
T. Bjorg, d id
the
ar tw or
k for
the
bo
ok. A spec
ial w
ard
o
f thanks to
M. Tay
lor Sarno ,
who read
an earlier ve
rs ion of th
is mon
ograph an
d
gave m e every he lp
and
encouragementto deve lop i t for publication.
F
inally, Im
ust th
ank
the
N o r w egian
Nat ional H
eal th Asso
ciation
f
or theirs
upport of
my work d
uring several y
ears, inc lu
d ing
the
t im
e
period
during
w hic
h the bo ok
w
as w ritte
n .
IVAR
REINV NG
-
8/10/2019 Aphasia and Brain Organization
8/204
-
8/10/2019 Aphasia and Brain Organization
9/204
-
8/10/2019 Aphasia and Brain Organization
10/204
CONTEN
TS
ix
Chapter
5 M
emoryand Lea
rning Defi
cits
5 1
Normal
M em or y
71
5 1 1
Verbal Me
m ory
7
2
5 1 2 Ve
rbal Learni
ng
73
5 1 3 Th
e Relation
of Verbal Memo
ry
and
Lear
ning to La
nguage Fun
ct ion
73
52 Verb
alM e m o ry
and
Learn
ing in A ph
asics
74
5
2 1 Verbal
M em or y
74
5
2 2 Verba
l Learning
76
5 3
N onverba l
M em or y
a
nd
Learnin
g
77
5 4
Conc lus
ion
78
5 5 P
resent S
tudy
79
5 5 1 Te
sts
80
5 5
2 The S t
ructure of Memo
ry
in
A phas ia
~
55 3 Rel
ations of M
em ory to A
phas ia
Group
89
5
5 4 Discu
ssion
93
55 5 Con
clus ion
95
Chapter 6
Defe
cts
o
f Vi
sualNonv
erbal bilities
61 Visua
l Nonverba
l Funct ion
s in A p h a s
ia
97
6 1 1
Apraxia
99
6 2 Th
e
Prese
nt
Study
101
6 2 1 Test
s of Nonve
rbal Abiliti
es
1
01
6 2 2
Tests of
M otor Func
tion
103
6 2
3 Apraxi
a
103
6
2 4 Resu
lts
104
6 2 5
Discussio
n
1
06
Chapt
er
7
Localiza
tion of
Le
sion in
p
hasia
7 1
S tatus of
theLocaliza
tion Model
7 2
ew
an
didates
for Statu
s as
1
09
Langua
ge Areas
110
-
8/10/2019 Aphasia and Brain Organization
11/204
x
CO N TEN
TS
70201
T h
e Limbic
Sys tem 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0
0 110
7
2 2
T he Len
ticular Zon
e
0
0 0 0 0 0 0 0 0 0 0
0 0 0 0 111
7 2 3
Medial Struc tures
0 00 0 0 0 0 0 0 0 0 00 0 0 0 0 0 0 11 2
7 3
T he Pres
en t S tudy 0 0 0 0
0 0 0 0 0 0 0 0 0
00 0 0 0 0 0 0 0 0
0 113
70301
M e
thod 0 0 0 0 0 0 0 0
00 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0
115
7 3 2
Results 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0
00 0 0 7
7 3
3 A
nalysis of T
est Pa ram
eters 0 0 0 0 0 0 0 0
00 119
7
03 40
Lesions and
Their C
ontext 0 0 0 0 0 0
0 0 0 0 0 121
7 40
C onclu
s ion 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0
00 0 0 0 0 0 0 0 0
00 0 28
Chapter
Rec
overy an
d Pr
ognosis
801 T h
e Recovery
Process 0 0 0 0
00 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 12
9
8 2
Reco
veryof No
nverbal Fu
nct ions 0 0 0 0 0 0
0 0 0 0 0 131
8 3 P
rognosis 0 0 0 0
0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0
00 0 0 0 0 0 0 0 1
31
8
40 M e
chan isms
of Recovery
0
00 0 0 0 0 0 0 0 0
00 0 0 0 0 0 13
3
8 401
R elearnin
g
or
Facili
tation 0 0 0 0 0 0 0
0 0 0 0 0 133
84020
R eorganization of Function
0 0 0 0 0 0 0 00 0 134
8 4030
Release
of Vicario
us N eura l
S tr
uctures
and
Functiona
l Relocaliz
ation 34
8 40
40
C om
plem enta ry
R edifferen
tiation of
Funct io
n 00 0 0 0 0 0 0 0 0
00 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 13
5
8 5
ThePrese
n t S tudy 0 0 0 0
0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0
0 136
8050
1
Recov
ery P at tern
0 0
00 0 0 0 0 0 0 0 0
00 0 0 0 0 0 0 36
8 5 2
P
rognosis 0 0 0 0
00 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0
0 0 141
8 53
Relations
between
Fundionsin
A cute
an
d
Chronic Pa
tients 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 4
4
805 40
C onclu
sions 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 14 5
C
hapter
The
rganized
R
esponse
of the
rain to
Injury
901
Evidence
for O rgan iz
ed C omple
xity 0 0 0 0 0 0 0 0
148
9
2
A Prop ose d System icMode l
0 0
0 0 0 0 0 0 0 0 0
00 0 0 149
9
0201
A
bstrac t Mo
del 0 0 0 0 0 0 0 0 0
00 0 0 0 0 0 0 0 0
00 49
-
8/10/2019 Aphasia and Brain Organization
12/204
CONTENTS
xi
9.2.2. Neural Model
151
9.2.3. Clinical Evidence on Hemispheric
Relationships . . . . . . . . . . . . . . . . . . . . . . . 152
9.2.4. Within Hemispheric Specialization
and
Differentiation in umans . . . . . . . . . . 154
9.2.5. The Effect of Lesions and the Systemic
Basis of Recovery . . . . . . . . . . . . . . . . . . . 155
9.3. Testing the Model
158
9.3.1. Application of the Model to the Present
Findings . . . . . . . . . . . . . . . . . . . . . . . . . . .
159
9.3.2. General Applications of the Model 16
9.4. Concluding Remarks
161
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 165
ppendix
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
181
ndex 193
-
8/10/2019 Aphasia and Brain Organization
13/204
PPRO CHES TO THE
STUDY OF PH SI
1 1 Clinical and
Theoretical
pproaches
The study of aphasia
may
be motivated by clinical as weil as theoretical
considerations.
t
has been
estimated
that about
1 million people suffer
from aphasia
in the
United States (Sarno, 1980). In
Sweden the
inci-
dence of aphasia
has
been estimated
at
60
per
100,000 inhabitants
per
year (Broman, Lindholm, Melin, 1967), and in
Norway Petlund
(1970) estimated the prevalence at .09 . The most frequent cause of
aphasia is strake, which is itself a common disease in an elderly
population. Whereas the risk of strake in the fifth decade of life is
.2 , the corresponding risk in the seventh decade is 2.0 (Mar-
quardsen
1969).
Add
the
fact
that
20 to 25 of
strake
patients
are
initially aphasic (Brust, Schafer, Richter, Bruun, 1976), and the
magnitude of the clinical problems becomes striking. In this context,
the need for practical and reliable methods of testing is apparent. A
classification system with knowledge of associated neurological and
neuropsychological deficits, prognosis, and
underlying
pathology is
a prerequisite for
sound
treatment.
From a theoretical point of view,
aphasia
has, since the time of
the founding papers of Broca
(1861)
and Wernicke (1874), presented
a unique
opportunity
to study
the
relationship of
the
brain to
higher
mental functions.
The
theoretical
problern may
however be
1
-
8/10/2019 Aphasia and Brain Organization
14/204
2
CHAPTER 1
fonnulated in different ways,
and
different methodological approaches
may be chosen.
A clinically
based
research strategy includes the following steps:
1.
Observing naturally occurring associations and dissociations
of symptoms. These groupings are referred to as syndromes, with
the
understanding that
they are clinically useful fictions.
2.
Distinguishing between theoretically meaningful associations
phenomena associated because they reflect the same function)
and
theoretically meaningless associations (associations
produced
by the
oretically uninteresting combinations of functions). The
methods used
include psychometric analysis,
post
ho
control of
the
lesion variable
(as the size of the lesion is believed to be the
most
significant factor
in producing spurious associations of symptoms), and experimental
control of the task variable. The result is a structural analysis of the
function involved.
An
alternative research strategy is based on
assumptions
about
the
nature
of language in the normal case.
t is fair to say that, recently, theoretically oriented efforts have
had
the
goal of analyzing (decomposing)
the
cognitive-linguistic proc
ess into constituent subfunctions and assigning
neural
correlates to
these subfunctions. In order to attain the goal of accounting for proc
essing, the internal computational steps of subfunctions and their
ordering must be specified for a given type of task.
Progress in linguistics has led to models of the
subcomponents
of the language function, and to possible rules for relating linguistic
symbols to each other. The structural school of linguistics has influ
enced
aphasiology
through
the works of Jakobsan (1971), whereas in
more recent times the transformational generative model of linguistics
presented
by Chomsky
1965) has
been
influential.
The tenn
neurolinguisti s
(Hecaen Dubois, 1971; Whitaker, 1971)
stands for
an
interdisciplinary
study
of aphasia
based on
neurology
and linguistics.
In
an
influential paper, Arbib and Caplan 1979)
argued
that
neurolinguistics must make an effort to give a computational account
of processing and that this can be approached by converging efforts
of
neurolinguistics, psycholinguistics,
artificial intelligence,
and
neurophysiology.
In the summary of Caplan (1982), the first steps are
-
8/10/2019 Aphasia and Brain Organization
15/204
APPROACHES TO THE STUDY OF APHASIA
1 The Ievel at which the nature of computation is expressed. With
respect to human language, Marshall suggests that generative transfor-
mational theories of grammar provide a characterization of
the
structures
relevant to language,
that
is, a characterization of the features of the
mental object attained.
2.
The Ievel
at
which algorithms
that implement
a computation are
characterized. Marshall suggests
that
work
on
parsing strategies,
both
implemented
and
based
on
the results of psychological experimentation,
provides
an
example of the beginnings of a characterization of the psy-
chological steps which are operative in the
attainment
of
the
linguistic
structures of Level 1
3. The Ievel at which an algorithm is committed to particular mech-
anisms, which has been
the
traditional preserve within psycholinguistics
of the aphasiologist. (p.
423
3
Clinical and theoretical motivations have been closely wedded
in the history of the
study
of aphasia. t
has been assumed that
theoretical inferences could be drawn with confidence on the basis
of clinical observation of the association
and
dissociation of phenom-
ena,
and
that the
syndrome
is a significant
unit
for theoretical analysis.
Only recently has the closeness or fruitfulness of this alliance been
questioned. According
toMarshall
(1982),
there will be some models
ofbrain
organization within which the
demands
of clinical diagnosis
and
theoretical
understanding
pull in diametrically
opposed
directions. (p.
404
For the neurolinguist, the unit of analysis is language, and
assumptions about a language function are
independently
motivated
from studies in linguistics and psycholinguistics. t
does
not follow,
however, that aphasia
n
toto
or
subsets of aphasia phenomena are
wholly interpretable as a failure in
subfundians or
processing stages
of the language function. l t is interesting to follow the increasing
divisions of clinical and neurolinguistic studies. In
the
1970s
there
was
optimism that the major clinical
syndromes
of aphasia could be
given a neurolinguistic analysis referring to breakdown in major blocks
of linguistic subfunctions (Caramazza Bemdt, 1978 . The more recent
attitude is that only selected aphasic symptoms, including agram-
matism and some forms of dyslexia and agraphia, can be usefully
studied,
and
then
preferably in selected cases
with
'
1
pure defects.
Taking the
stand that
there are only
two
approaches
to
aphasi(l-
the clinical, which takes the patient as
an
unanalyzed whole as its
unit of study, and the theoretical, which takes the language function
-
8/10/2019 Aphasia and Brain Organization
16/204
4
CHAPTER 1
and nonclinical models of it as its units of study-grossly disregards
a third approach.
This
approach
may
be
termed
neuropsychological
and
takes
the
syndrome as its unit of analysis. t follows the step of the clinical
research procedure as outlined above. When the outlines and divi
sions of a functional domain have been established with gross neu
rological correlates, then one of two options may be chosen.
One
is
to say that this is as far as one can get in clinical group studies, and
selected patients with more specific deficits offer the only opportunity
to advance the study by clinical material or methods. Another option,
however, is to say
that syndromes
are meaningful indicators of
the
multidimensional response of the brain to localized injury. They are
indications of the organizing principles at work in the efforts of
the
whole brain to maintain optimal functioning, as
much
as they are
indications of
the
contributions of the missing parts.
Although neurolinguistic analysis is strong on detailed func
tional analysis and specification of processing, it has difficulty justi
fying its selection of study
material
and
its notion of relevant
case
We
have no
theoretical metric for
measuring
the pureness
of functional
deficits, and it
may
well be
that
sharply delineated behavioral
symp
toms are the consequence of highly complex functional interactions.
The findings from analyses of
pure
deficits can be applied to more
complex cases only if one
assumes
that pure deficits can be conca
tenated
without giving rise to
strong
interaction effects. See Shallice,
1979, for a discussion of the problems
and
advantages of single-case
studies.)
Neuropsychological analysis is weak on detailed
function-and
process analysis. The existence of
some
alleged syndromes may be
questioned on empirical
grounds
e.g., the criticism of Benton, 1961,
of the Gerstman syndrome). Neuropsychological analysis has the
advantage of not requiring an independently motivated theoretical
model
and
provides much of the necessary framework for more
sophisticated analysis by giving a normative background for gradation
of performances.
f
the phenomena under study are interactive, then
syndromes
may reflect the emergent properties of factors combined
in
a larger system,
and
a description of the relationship of
the
variables
for different parametric values is a necessary part of a complete the
oretical analysis.
-
8/10/2019 Aphasia and Brain Organization
17/204
APPROACHES TO THE STUDY OF APHASIA 5
1.2.
Historical Approaches
The
present
conceptions of aphasia date back to
the
continental
European neurological tradition before and
around
the
turn
of the
century. This tradition has a main stream,
represented by
Wernicke
1874) and Lichtheim 1885) and several tributaries with supplemen-
tary approaches (Marie, 1906; Jackson, as summarized
by
Head, 1915,
1926; Goldstein, 1948; Luria, 1970; Jakobson, 1971; Hecaen Dubois,
1971). To a surprising degree,
the
mainstream of thinking
around the
turn
of the century is still a dominant
mode
of
thought
(Benson
Geschwind, 1977). Because all classical thories are centered
on
con-
cepts of localization of function, it is useful to give a more general
characteristic of localization theory before discussing the controversies.
1.2 .1. Localization Theory
of
Language to Brain
elation
No
author can be taken as the foremost representative of local-
ization theory. The following is
the
present author's summary of the
essential features of
the
theory implied
by authors
who
use
terms
like
language area or speech center to describe
the
neurological basis
of the language functions:
1.
The brain contains areas with specialized functions, beyond
the sensory
and
motor areas. Normally, one cerebral
hemisphere
contains all
the
structures necessary
and
sufficient for language. This
hemisphere
is said
tobe
dominant (for language). Normally,
the
left
hemisphere
is dominant,
but
in some instances,
these
structures may
be distributed
between the hemispheres
or
may
be located entirely
in the right hemisphere.
2.
Within the dominant hemisphere, there is also specialization,
so
that
some areas are of critical importance to the language function
and some are not. The structures necessary for language (language
areas) are commonly believed tobe cortical, and
tobe
located in the
temporal
and
frontal Iobes. There are, however, different theories
and formulations of which specific areas are important and how far
their functions are differentiated.
3.
Different parts of
the
language areas are specialized for dif-
ferent functions. Differently localized lesions in the language areas
give rise to varied clinical syndromes.
By
focusing
on the
features
-
8/10/2019 Aphasia and Brain Organization
18/204
6
CHAPTER 1
that
show
the most consistent relationships to the locus of injury, a
definition of types of aphasia can be given. t is
not assumed
that all
pathological performances in aphasia
show
a lawful relationship to
the locus of injury. Alternative classifications built
on
principles other
than clinicopathological correlation may be chosen but would have
to prove their advantage for special purposes. Again, there are dif-
ferent alternative formulations of which are the major
and
minor
aphasic syndromes and what is their specific relationship to the locus
of injury.
4
Language areas have fiber connections with one another and
with
other
areas. In the classicallocalization theories, these Connec-
tions are believed to have very simple functions of transmitting stim-
uli, thereby triggering the activity characteristic of the area receiving
the stimulus. More complex information on the results of previous
stages of analysis may also be transmitted, thereby
adding
or inte-
grating the activity of several connected areas before a motor response
is emitted. This simple conception of the functioning of connecting
fibers has led to their being
named
association
fibers
and to their areas
of convergence being called
association
areas Although it
has
not been
done
in classical localization theory, it is entirely possible,
without
abandoning localization theory altogether, to explore the hypothesis
that association fibers have more complex functions than believed.
The localization theory
has
been criticized both on general
conceptual grounds and with respect to some of its more specific
statements about the nature of aphasia
and
the types of aphasic
disturbances.
t is worthwhile to pause and note that none of these criticisms
question the existence of a correlation between the type of aphasia
and the locus of the lesion. Even authors often identified as antilo-
calizationalists, like Jackson see Head, 1915), Marie 1906), Head
1926), and Goldstein 1948), never denied the existence of clinico-
pathological correlation.
1 2 2
Criticism
of Basic Premises
The criticisms most often advanced may be summarized
under
three points:
-
8/10/2019 Aphasia and Brain Organization
19/204
APPROACHES TO THE STUDY OF APHASIA
7
1. t is impossible or unacceptable to try to localize normallan-
guage, a criticism stated forcefully by Jackson (see Head, 1915 .
2.
The mixture of behavioral
and
neurological
terms
of classi
fications is ill-conceived
and
confusing. This criticism, too, is
closely connected
with the work of Jackson (see Head, 1915).
3. The general form of
the theory
(connectionism
or
associa
tionism) is
outdated and has been shown
tobe
inadequate.
Both Head (1926)
and
Pribram (1971) have stated this argu
ment forcefully.
Regarding the alleged nonlocalizability of
normallanguage,
it is
appropriate to stress
the
difficulty of using observational clinical data
as a basis for inference about normal processes. In particular it is
unwise
to
name
centers on
the
direct basis of lesion locus
and
symptom
description. This is
no more than
to
say that phrenology
is
outdatedas
a model of neuropsychological research.
On
the basis of
observation
that
patients
with
certain lesions have difficulty
in
naming
objects, we would be unwise in inferring that the locus of the lesion
is normally
the
locus of object
names.
But
assume
that
characteristics
of this naming
difficulty can be
teased out further by
experimental
variation of conditions
and
can
be shown
to deviate from
normal
performance by certain parameters. We
would have
then a basis for
hypothesizing an underlying process, which can then, again hypo-
thetically,
be
related to a given neurological structure.
The hypotheses
may
very well have implications that could also
be tested
on
normal
individuals by
means
of behavioral measures.
The criticism is correct if it is reformulated to
say that
no
hypoth-
esis assigning normal processes to given neurological structures should
be accepted on clinical evidence alone. The declaration that
language
cannot be
localized, however,
seems
to
be
an arbitrary conceptual
decision
that any
function
with
a definite relation to a
neural
locus
cannot be called language
Mixing behavioral
and
neurological classification was called
psychoneurology
by
Jackson (see
Head,
1915). There is danger of
tautological reasoning if concepts from one category are used to define
those from another. f
frontal
aphasia
is
defined
as
the type of aphasia
resulting from frontal injury, then the question of the frontal locali
zation of this
syndrome has
already
been
settled
by
definition.
-
8/10/2019 Aphasia and Brain Organization
20/204
8
CHAPTER I
However, if care is taken to define behavioral categories in behavior
terms and neurological categories in anatomical terms,
then
there
should
be
no
objection to
studying
the relationships
between
the two.
With the
advent
of more sophisticated statistical techniques, the
question of the behavioral validity of aphasia types can be raised: Are
there naturally occurring clusters of aphasia symptoms,
and if so, do
they correspond to the classically described types of aphasia?
t
must
be recognized that the answer to this question depends on the patient
group studied. The agent of injury
may
be
such
as to
produce
diffuse
lesions, as in metabolic or anoxic lesions.
t
may also produce discrete
lesions,
but
of several anatomically distinct structures
not
known
to
have a common function. This combination of lesions
may
weil occur
in
cerebrovascular disease, where structures may be damaged together
by
virtue of having a common blood supply. In
penetrating
head
injuries, again, the lesion may be discrete and weil defined but may
not follow the demarcation lines drawn by anatomy. Rather than
injuring one well-defined anatomical structure completely, it
may
incompletely injure three.
odern
statistical studies started
with
Weisenburg
and
McBride
1935) and continued with Jones and Wepman 1961) and Schuell,
Jenkins, and Carroll (1962). All these studies rejected classical clas
sification schemes but are open to the criticism of Iack of control of
localization of the
lesion. Recent studies
by
Goodglass
and
Kaplan
1972) and Kertesz and
Phipps
1977) indicate that
an
extension and
refinement of classificatory schemes within the framework of a clas
sical clinicopathological model are a likely development.
I agree wholeheartedly with the critics of classical localization
theory that associationism is an inadequate theory for explaining the
complex activity of the nervous system. Hughlings Jackson was aware
of this point. From his studies of epilepsy, he described a certain dass
of symptoms as release symptoms, that is, symptoms caused
by
a
loss of inhibition. In his hierarchial model, the alleged loss of the
propositionallevel of function and the emergence of autornahe speech
are the primary example ofthistype of deficit in aphasia. In modern
times, several authors, among them Pribram (1971), have rejected
associationism
and
have
proposed
more complex theoretical models.
As noted above (p. 6), localization theory does not presuppose
associationism, although the two theories have been closely linked
-
8/10/2019 Aphasia and Brain Organization
21/204
APPROACHES TO THE STUDY OF APHASIA 9
historically. The inadequacy of
an
associationist model of
the
brain,
tagether
with
the
criticisms discussed above,
should not
lead to aban
doning the
concept of localization of function. Localization
theory
should,
however, be modified and modernized. The specific content
of an adequate theory is largely unknown.
t
is, however, of some
interest to discuss
what
general features
an adequate
theory
must
have.
1 2 3 Criticisms of Assumptions Regarding
the
Nature of phasia
or
the
Types
of phasie
Disturbances
The following criticisms will be discussed:
1
Language
cannot
be distinguished from intelligence. Aphasia
is symptomatic of a more general intellectual disturbance
(Marie, 1906; Bay, 1962).
2. Different forms of aphasia do not exist; only
aphasia
with
different additional disturbances exists (Bay, 1962; Schuell,
Jenkins Jimenez-Pabon, 1965).
Jackson (see Head, 1915) proposed that language is
integrated
in
several levels of mental functioning. Aphasia is
not
a disturbance
of an anatomically localized language mechanism or process; rather,
it reflects mental regression from a propositional
11
Ievel of functioning
to lower levels. Speech
in
emotional context is preserved,
but prop-
ositional speech is lost. Other influential thinkers
supported
this posi
tion.
l t
was adopted
by
Head (1926),
who echoed
Jackson's statement
that an aphasic is in a certain sense lame in his thinking, and by
P. Marie 1906}, who said that aphasia is a special sort of intelligence
defect. In modern times Bay
1962) has
been a strong advocate of
the view that a conceptual disturbance is inherent in aphasia.
The position of Wernicke (1874) on this issue was clear:
The spoken and written narne of an object is not a
new
attribute of
the object. t is
thus
clearly different frorn the actual sensory rnemory
irnages of the object. Only the latter make up
the
concept of the object.
Disturbance of the concepts of things with which
we
deal in the process
of thinking are always disturbances of intelligence. Disturbances of speech,
on the contrary, cause difficulties only in the use of the conventional
means of representation of the concepts. (p.63)
-
8/10/2019 Aphasia and Brain Organization
22/204
10
CHAPT
ER 1
Th
e con
sequ
enceo
f th is
issue
for r
esear
ch see
m s to
be to
que
s
tion
whet
her a
cons
isten
t defe
ct in
inte
lligen
ce c
an be
foun
d in
aphasics.
f
so, it is necessaryto postulate
n
inherent l ink be tw een
tho
ught
nd
langu
age b
eyond
thep
lausi
ble as
sum p
tiont
h t th
e lan
g
uage
distur
bance
m ak
es n
ins tru
m en
t for th
ough
t le ss
avail
able.
A
w
ay o
f dem
onstr
ating
a def
ect of
intel
ligenc
e is t
o sho
w tha
t, giv
en
a def
ect in
perf
o rmin
g a ta
sk w i
th lan
guag
e mat
erial,
it is p
ossib
le to
dem
onstra
te th
e def
ect ev
en if
the v
erbal
elem
ents
of the
task
are
rem
oved.
The
availa
ble re
searc
h on
hem i
spher
ic asy
m m e
try o
nly pa
rtly
supportsthe notion of material-specific functions of the tw o hemi
sph
eres(
Milne
r,
197
4;
Ga
zzani
ga
Ledo
ux 19
78), nd
dif
feren
ces in
th
e cog
nitive
m od
e of
opera
tion
of the
two
hem
isphe
res mus
t b
e
con
sidere
d. (Fo
r revi
ew, s
ee Bra
dsha
w
n
d
N ettl
eton,
1981.
) Rese
arch
on
in t
ellige
nce in
apha
sia, s
um m
arized
in L
ebrun
nd
H oop
s (197
4),
indic
ates s
om e
reduc
tioni
n spe
cific n
onve
rbal t
asks, but
t
he ro
le of
the
size o
f the
injur
y in
expla
ining
such
defec
ts is
uncer
tain .
The
evid
ence
on th
e issu
e is n
ot str
onge
noug
h to l
ead us
to ab
ando
n the
theoryof localized language function. The facts nd their in terp re
ta
tiona
re d i
scusse
d fur
ther i
n C h
apter
6.
The s
econd
c hall
enge
to loc
alizat
ion th
eory nd
th
e clin
icopa
th
ologic
al m o
del i
s the
quest
ion o
f w he
therd
iffere
nt ty
pes o
f apha
sia
exist
. The
posit
ion ta
ken
by an
tiloca
lizatio
nists
is tha
t diff
erent
syn
drom e
s exi
st afte
r diff
erent
ly loc
alized
lesio
ns, but
the
y sho
u ldn
ot
be
calle
d diff
erent
form
s of a
phasi
a. Th
ey sh
ould
r the
rbe s
een a
s
aph
asia w
ith d
iffere
nt, dd
ed d
isturb
ance
s. Ma
rie
1
906)
s
tated
tha t
Bro
ca aph
asia
is the
comb
inatio
n ofa
phas
ia nd
anar
thria.
This
is the
holis
tic in
terpre
tation
of a
phasi
a , w h
ich h
as al
so be
en po
pula
r in
m
odern
time
s th r
ough
the w
ork o
f Sch
uell t al
1965
).
Ther
e is no
dou
bt tha
t, ina
phasi
a, var
iations
in pe
rform
ance
can of
ten be
obse
rved,
so
thats
om ep
atien
ts hav
e dis
propo
rtiona
te dif
ficulti
es w i
th spe
aking
,
w
riting
, read
ing,
o r au
ditory
ana
lysis.
Som
etim e
s suc
h var
iation
s
dete
rm in
e the
classi
ficati
on of
the t
ype o
f aph
asia.
W het
her o
r not
such
distur
banc
es of
perfo
rm an
ce sh
ould
be ca
lled d
istur
bance
of
la
ngua
ge is
partl
y a c
oncep
tual
questi
on. B
enso
n nd
G es
chw in
d
1977)
defin
ed lan
guag
e as
perce
ption
of ver
bal se
nsory
stim
uli, in
te
gratio
n oft
hese
stim u
li w ith
prio
r know
ledg
e, nd
activ
ation
of ve
rbal
-
8/10/2019 Aphasia and Brain Organization
23/204
-
8/10/2019 Aphasia and Brain Organization
24/204
-
8/10/2019 Aphasia and Brain Organization
25/204
APP
ROAC
HESTO
THE
STUDY
OF A
PHAS
IA
13
d
ifficu
lty of
deriv
ing te
stabl
e pred
ictio
ns. G
enera
l syst
em s t
h eory
is
no t
a testa
ble th
eory
but on
ly a f
ramew
ork f
or de
velopi
ng m
ore de
tailed
theorieswi th in a specific field.
13
1 App
licati
ons of
Syste
ms The
oryCo
ncepts
in
N
europ
sychol
ogy
A
com p
rehen
sive r
eview
of th
is top
ic is
be
yond
t
he scope
of th i
s
ch
apter
.Few
a
utho
rs re
fer ex
plicitl
yto sy
s tem
s theo
ry its
elf,
and ver
y
many
u s
e con
cepts
t
hat
a
re re
lated
to sy
s t ems
theo
ry in
one
way
or
anoth
er . H
ere I
focu
s esp
eciall
y
on
s ta te
m e n t
s em
phas i
z ing
th
e
dynamic, interactive
nature
of b rain funct ion
and
the nature
of sy m p
to
m s a
s an
organ
ized r
espon
se o f
the w
ho le
brain
after
injur
y .
O
ne
cont
ext i
n w
hich
the
dynam
ic
n
ature
of fun
ction
-to
loca
lizatio
n rel
a t ions
hips h
as
bee
n muc
h
d
ebate
d is
the
s
tudy
o
f t
he
on to
g en y
of th
e cere
bral l
a teral
izat io
n of
the
lan
guag
e fun
ction.
Len
neb
erg
1967)
s u m m
arize
d
theevide
nce
and co
nclud
ed t
hat lan
guag
e
is
gradu
al ly
latera
lized
after
bein
g init
ially b
ilater
ally
rep res
en ted
.
Sinc
e the
n it h
as
been
re
cogni
zed
tha
t
th i
s v iew
is o
versta
ted. T
here
is ev idence ofearlyspecialization ofthe left hemisphere for lan g u age
(D
enni
s W
hitak
er, 19
77),
and fo
r seve
ral as
pects
of lan
guag
e,
ther
e
are
no
in
dicat
ions
of co
n t inui
ng la
terali
zation
. As
p
ointe
d ou
t
b
y
M osc
owitc
h (197
7), c
u r ren
t test
smay
t
ap only
very
low
levels
o f
lin
guist
ic pro
cessin
g ,
and
w
heth
er h igh
e r
ord
er
li
nguis
tic pro
cesse
s
do
inde
ed
b
ecom
e pro
gress
ively
m ore
latera
lized
wit
h age is
open
to
de
bate
(p. 2
04).
Se
ines 1
974)
gave
an ex
tensiv
e rev
iew o
f t
he role o
f the
corpu
s
ca l losum
inestablishing hemispheric
spec ial iza t ion.
With poorly
devel
oped
c
o rt ico
-cor t
ical C
o n n e
ct ion
s ,
recip
rocal
sp
ecial
izatio
n
deve
lops o
nly s
o far
as st
ructu
ral as
ym m e
tries
allow
. Wit
h cal
losal
a
genes
is, th
ere is
an in
dicat
ion o
fgrea
ter l ik
eliho
od of
b
ilater
allan
guage
repr
esen t
a t ion
a
nd a h ig
h er in
ciden
ce of
retar
dat io
n in
l
an
guag
e dev
elopm
ent .
The d
evelo
pme
nt of h
emi s
pher i
cspec
ializa
tion
fo
r lan
guage
in no
rmal s
may
b
e
re
la ted
to rela
tively
late
m yeli
n izat i
on
of
callosa
l fibe
rs (Ya
kovlev
Le
cours
,
1
967).
Sein
es 1
974) co
m m e
nted:
The evidence in support of the view that CC (corp us cal losum ) m ay
b
e respo
nsible
for th e
e stabl
ishm en
t o fla n
guage
laterali
zation
is th
us
no
t
str o
ng,
but
at
leas
t it has
thead
van tag
e o fbei
ng rel a
tively e
asyto
confirm
o
r disco
nfi rm .
This v
ie w di
ffers fr
om the
trad i
t ional
in hibi
tory th
eory
-
8/10/2019 Aphasia and Brain Organization
26/204
-
8/10/2019 Aphasia and Brain Organization
27/204
-
8/10/2019 Aphasia and Brain Organization
28/204
1
6
C
HAPTER 1
T he insiste
nce on
the
interactive
, dyn
amic proper t ies
of
neural
fu
nctions is
in agreeme
nt with
a
sys tems
theo ry app
roach. Th
is
approach
is
furtherdevelopedin
an
eloquent statement
of h is p osi t ion
by
Kinsbo
urne 1982
):
There ar
e no discontin
uitie s in the
brain. No independent
ch
anne ls
traverse it, nor
is its territ
ory divisible i
n to areas that house auton
omaus
processes No
Simula
tion of
h
uman
behaviour , howe
ver impre
ssively
successful
in im personat
ing its model
, is capable o
f revealing how
the
human
mind arrive
s
at
the s ame
outcome , un l
ess i t
i
s based
on
a ne twork
mech
anism. p. 412
1.3.2 Localizat
ion
of Function in Ligh
t of
Systems T
heory
t is possi
ble to class
ify neurop
sychologic
al theories
according
to
thei r posi t
ion on
the
two
dicho
tom ies of l
ocalization
ve
rsus non-
loc
alization
and systemi
c vers
us
no
nsystemic .
I will first
describe
the
d icho
tom y
betwe
en
nonloc
alizat ion and
localiza
tion views
and
then
show how
these v iews a re
m odified
by
in
troducing
the
co
ncept of
systemi
c functioni
ng.
1. Nonloc
alization
nonsy
stemic
T
he t
heory
s
ays tha
t
fun
ctions a re
diffuse
ly represen
tedin a str
ucturally re
latively un
differentiate
d brain.
eural net
works have
been
d
escr ibed a
s analtern
at ive to lo
calized
functional
cente rs . Th
e alternativ
e , h o w e v e
r , se
ems hard
to recon
cile
w
iththe
h ig
h ly specifi
c str
uctures
and patt
erns
of conn
ec t ions
foun
d
in modern neurosc
ience .
T he origina
l ideaof the neuron
network
as acontinuum
of nerve c
ells
of
Standard sha
pe
a
nd isotr
opic random
or
geometric
ally determin
ed)
connectivity propert ies has all
but
disappeared from
our
im age of the
centers of
the higher an
imals . Szent
agothai Ar
bib, 1975, p. 43
T h
erefore , be
cause
of th
e
kn
own
sp
ecif ity
and diversi ty o
f ana tomica
l
s t ruc tu re s
i
n the
brain
, th is
theor
y cannot be m
aintained for
the
fu
nc-
t ioning of t
he bra in a
s a w hole .
t m ay, how
ever ,
be
c
o n s ide red
for
ce
rta in func t
ions
in
re la
t ion to lim
ited bra in r
egions . Th
e thesis
that
lesion
s
within t
he
la
nguage areas g i
ve rise to
apha
sias
o
f v ary ing
severi t
y , bu
t not
o
f varying
type , exem
plifies this
p roposi t ion
.
2.
Localization
nonsyste
mic
Thi
s th
eory
s t
a tes th
at th
e
br
ain h
as
highl
y specific
and diversif
ied ana tomi
cal s t ruc tu
re s
with
eq
uallyspe -
cific
and diversifi
ed function
s. T he ext r
em e exam
ple is
phrenology
-
8/10/2019 Aphasia and Brain Organization
29/204
APPROACHES TO THE STUDY OF APHASIA 17
which says that the brain is a collection of
independently
working
organs.
The advantage of classical clinicopathological theory over
phren-
ology is that it
adds
the possibility of integrative action
by
postulating
connections between neural centers, as weil as the building
up
of
more complex functions
by
association. The theory is still nonsys
temic, so long as the presence of connection does not modify the
operations of localized functional centers. The Wernicke-Lichtheim
model uses the concept of localized functions to describe
and
explain
loss of function but
adds
aphasia syndromes (conduction aphasia,
transcortical aphasias) caused
by
isolation
or
disconnection of lan
guage areas.
An even more sophisticated step in analysis is taken when local
ized centers are connected in temporal sequence
and
shifting com
binations. These functional systems (see Luria, 1973) are
seen as
underlying normal performances. They arestill
not
systemically orga
nized in the sense of the
present
discussion, because the functioning
of a component is not modified by other components, barring the
special case of disconnection.
3. Nonlocalization systemic
Although acknowledging the highly
interconnected
nature of neural tissue, I have already rejected the
neural net as a sufficient model of the human nervaus system. As an
alternative to neural nets, Szentagothai
and
Arbib
1975)
described
more
modern
concepts,
based on
the idea of modules of
neuronal
organization. Although recognizing anatomical specificity, still
the
similarity of neuronal building blocks, called
modules throughout
the
cortex is stressed.
To make such a model systemic, it
would be
necessary to
assume
that
the pattern of interaction between neural elements (modules)
determines function, whereas this
pattern
can be set up
anywhere in
the brain, or at least
in
the cortex. Although such formulations are
more theoretically acceptable than simpler concepts in
the
nonsys
temic version of nonlocalization theory,
the
problern is to
show how
localized injury to a brain thus organized could result in a differential
deficit in the language function, with relative sparing of
other
func
tions. Hence, the introduction of a systemic dimension does
not
make
nonlocalization theories better able to explain the empirical findings.
Although rejecting this alternative as a model for the brain as a whole,
-
8/10/2019 Aphasia and Brain Organization
30/204
-
8/10/2019 Aphasia and Brain Organization
31/204
APPROACHES TO THE STUDY OF APHASIA 9
is the
main
clue to the systemic organization of cerebral representa
tion. In nonsystemic organization
the
additivity of effects is pre
served
but not
in
systemic organizations. Finally
the
degree of
changeability in the performance-to-structure relationship in recovery
can be used as additional relevant information.
1 4
The
resent Study
What
one undertakes as a research project is determined by
one
s
interests practicallimitations
and,
most
important
what
one
regards
as reasonably well established.
During the period of time in which the material for this study
was
collected
the
general services offered aphasic individuals in Nor
way
were unsatisfactory. Speech
therapy
services
were not
organized
and were available only in large cities or communities. No counseling
social
support,
or information pertaining specifically to the problems
connected with aphasia were given to families
and no
training in the
care
and
treatment
of aphasia patients
was
offered to hospital per
sonnel. As a first step to improve this situation the Institute for
Aphasia and Stroke
was
established in 1973 by a donation from the
National Health Association a private organization with the fight
against coronary
and
other vascular diseases as one of its goals.
The Institute for Aphasia and Stroke is a test laboratory located
in the
Sunnaas
Rehabilitation Hospital which is one of the municipal
hospitals of Oslo Norway. The staff of the institute consists of one
neuropsychologist
one
technician
and one
research associate. The
hospital has 226
beds and
admits patients with several kinds of func
tional disturbance with organic etiology offering physiotherapy
occupational therapy speech therapy and, in addition social and
medical services. Patients
may
be
admitted
for evaluation only or for
full treatment. The hospital offers only
inpatient
services; thus, the
patients
admitted
for treatment have severe physical handicaps
whereas patients with lighter physical defects are referred to other
institutions with outpatient services.
Because of its
unique
position
the
institution received appli
cations for admission from the entire country during the period of
this study. An attempt
was
made to see as
many
as possible of the
-
8/10/2019 Aphasia and Brain Organization
32/204
20
CH
APTER 1
pa t
ients for ev
aluat ion a
nd testing,
so as to ge
t a survey
of
t
he pop-
ulatio
n referred f
or treatmen
t . A l thoug
h no exact
figure can b
e given,
it
can
safely be sta ted that m ore
than
90
of thepat ients referred
wer
e teste
d .
The decisi
on to create
an aphas ia
registry w
as mot iva t
ed by the
des
ire for a sy
stematic r
egistration
of all avail
able inform
ation perti
nent
to the des
cription an
d evaluat io
n of the pa
t ien t g roup
. Th e regis
try shoul
d serve
primarily
as an ins
trument fo
r clinical r
esearch,
c
oncentra t in
g
o
n the co
nnect ion of
aphas ia with
other symp
toms and
on the d
evelopmen
t of ap
has ia with
t ime. The
results of
tests per
formed at the Institu te for A phas ia
and
Stroke form the
main
content
of the
registry, w
i th medica
l
an
d gen
eral
b
ackground
info
rmat ion
added.
As re
viewed abo
ve, a summ
ary of
theconsensus
in
1978, when
this
study s tar ted,
runs as fo
llows:
The clini
cally defin
ed
sy
ndromes
of apha
sia are s ta
ble enti t ies
wit
h a wel
l-def ined p
athological
substrate.
Because a
phasia is a
lin
gui
stic deficit,
a more refi
ned l inguis
tic analy sis
of langu ag
e per form
ances in the major syndromes will allow us to replace the static
tradi
tional
descriptio
ns of functio
ns as un
analyzed
wholes
wit
h
dy
nam ic pro
cess ing con
cepts
approachin
g
the
ideal of co
mplete com
puta t ion
al specifica
tion with n
eural corre
lates.
My d ifficul
ties with ac
cepting the
pos i t ion just
sum
marized were
b
ased
on
both m e
thodologic
al and con
ceptual wo
rries. First
of all, I
wor r ied abou
t the lo
osely d ef in
ed procedu
res for test
ing
a
nd def
ining
apha
s ic syndrom
es . A nec
essary first
step for cl
inical research
and
a step t
hat
m
ust be
taken anew
n each di
fferent lan g
uage
com
munity-
is to def
ine strict and
quantif i
able proced
ures for te
s t ing and
classi
ficatio
n. The sy
stem of m
yself and
my colleag
ues is desc
r ibed in
Cha p te
rs 2 and 3.
Sec
ond, I wor
r ied about the
seemin
gly i
nnocuous assump
tion
that
a
ph asia is a
lingu istic d
eficit. Rem
ernhering t
he papers by
Teuber
a
nd Weins te
in 1956),
by Weins t
ein 1964),
and by o th
ers showing
an assoc
iation of a
phas ia w i t
h some v is
ual reason
ing
a
nd le
a rn ing
tests,
as well as t
he many ex
iting papers by
Kimur
a see Kimu
ra, 1979)
on
the close a
ssociation o
f langua ge
and
h ighe
r
or
der
motor function
s,
I thoug
ht i t more a
ppropr ia te
to def ine
aphas ia at
the outset
as a
linguistic-c
ognitive de
fect.
lthough I in
no way wish t
o ques t ion the
-
8/10/2019 Aphasia and Brain Organization
33/204
APPROACHES TO THE STUDY OF APHASIA
21
reality of a language function separate from other cognitive functions,
it
may
still be the case that aphasia does
not
reflect
an
isolated dis
turbance of this function.
f
it
turnsout
that
only a few selected cases
demonstrate
pure
disturbances of language,
then
a scientific approach
to the great majority is needed. Maybe these cases can be viewed as
just mixed and can be explained as additions of defects observed
in isolation in the
pure
cases. But it may also be
that
important inter
actions are at work, so that mixe
syn romes
becomes a misnomer for
unanalyzed complexity.
Third, I worried about the generally simplistic approach to
the
effect of brain injuries evident in a deficit-oriented analysis.
t
seemed
to me that the multidimensional response of the brain to injury, as
weil as the variations over time of this response, was what
had
to be
described
and
accounted for. I was (and am) disturbed by
the
tend-
ency to stress regularity and to dismiss variability in the response of
the brain to injury as noise. Commenting on the relative success
of syndrome classification, Wernicke 1874) stated:
Only a particular period in the course of the disease should be con
sidered if
one
is to diagnose aphasia correctly.
On
the one hand the
general
phenomena
which accompany the onset of aphasia, as
they
do
that of most localized lesions of the brain, must have disappeared. On
the
other hand
however, the conditions ought not to have Iasted so long
that
the
possibility of compensation by the
other hemisphere
is already
present. (p.
69)
Here, the motivation of the neurological diagnostician to ignore infor
mation not pointing to the locus of the injury is clearly seen.
Poeck (1983b) echoed the same opinion:
l t
cannot be denied that a certain
number
of vascular aphasias (approx
imately 15%) cannot be classified in terms of
standard
or nonstandard
syndromes. The main reason, in
our
experience, is that the examination
is
done
too early, prior to the establishment of a weil defined syndrome
or at
the
late stage of recovery, with or
without the
effects of speech
therapy. (p. 80)
On the basis of these reflections, and having standardized the
necessary tools for measuring and classifying aphasic phenomena
(Chapters 2 and 3), I have therefore
undertaken
a broadly conceived
program of testing aphasics with neuropsychological tests. Informa
tion on lesions with CT -scans has been recorded when possible, and
repeated testing has been performed in order to chart as far as possible
-
8/10/2019 Aphasia and Brain Organization
34/204
CH
APTER
the e
xtrem
es of
para
metri
c valu
es in
apha
sia
conce
ived
of as
n
ex
perim
ent o
fnatu
re. I
will a
ttem p
t to gi
ve a s
ystem
s-the
ory-o
riente
d
account of the complexity of the aphasic condition.
t
m u st be rec
ogniz
ed th
a t th
e acco
unt f
alls s
hort o
f the
goal
of
n expe
rim e
ntal
analy
sis of
causa
lly si
gnific
ant fa
ctors
if suc
h n a
nalys
is can
be giv
en.
t
also
falls s
hort o
fthe
ideal
of a sp
ecific
ation
of the
actu
al pro
cessin
g
stag
es be
h ind
the p
erform
ance
sobs
erved
. I w o
uld s
till cla
im th
at at
th
e ver
y leas
t thi
s type
of a
nalys
is of
the or
ganiz
ed co
mple
xity o
f
lingui
stic-co
gniti
ve ph
enom
ena
und
er a set
of ex
treme
cond
itions
is
a valu
able
com p
lem e
nt to
other
sour
ces o
f info
rm at
ion a
bout
the
underly ing system.
-
8/10/2019 Aphasia and Brain Organization
35/204
OPER TION LIZ TION
OF MODEL
2 1 The odel
2
The goal is to select a model that, tothebest of
our
current knowledge,
captures
the
significant dimensions of clinical
syndromes
t
should
also account for the associations of
parameters
that are useful for
defining syndromes while leaving reasonable space for
within-
syndrome
variations.
The Wernicke-Lichtheim model underlies
the
terminology
and
the clinical classification systems most frequently used today.
t
is a
model within the localizationist tradition (Wernicke, 1874; Lichtheim,
1885), and it identifies
two
cortical areas
important
to
the
language
function,
the
Broca
and
Wernicke areas. The fibers associating
these
areas are assumed to run in the arcuate fasciculus. In addition, Lich
theim
assumed that transcortical fibers, via a hypothetical concept
center, can mediate information between the language areas. Dif
ferent forms of aphasia follow from lesions of different neurological
structures.
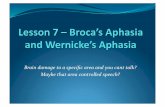
The localization of language areas is
shown in
Figure 2.1, and
the
types of aphasia resulting from differently located lesions are
shown
in Table 2.1.
A more detailed review of brain regions and the associated aphasia
types is given below. The review does not limit itself to statements
3
-
8/10/2019 Aphasia and Brain Organization
36/204
4
C
HAPT
ER 2
Fig
ure 2.
1. Loca
lization
of lan
guage
areas.
Legend
: 1)
an
ter ior
languag
e area
Broca
);
2) W ernic
ke area
; 3)
su
prama
rginal
gyrus;
4) ang
ular gy
rus.
by cla ss
ical
u
thors
but in
tends
to
sketc
h the
p res
en t -d
ay st
tuso
f
th is
m ode
l.
2
1 1
Broca
re
a
T
he Br
oca ar
ea is
locate
d in
th
e
th
i rd tr
an sv e
rse fr
ontal
conv
o
l
ution
, w hi
ch ca
n b e d
iv id e
d in t
o th re
e par
ts: th
e orb
ital, t
he tri
an
gular
,
nd th e o
percu
lar.
t
is th
e o pe
rcu la
r p r
t of
the
con
volu
tion
Table
2 1
Assumptions of
the
Wernicke Lichthe
im
Model
Typ
eof ap
has ia
B
roca
W e
rn icke
Globa
l
C
onduc t
ion
Ano
m ic
Is o
la tion syn
drome
Tr
anscort
ical mo
tor
Tr
anscor
ti cal se
n sory
Broca
area
W
ernick
earea
Locus
of lesi
on
Bro
ca nd
W ernic
ke area
s
A rcuat
e fasci
culus
A n g u
lar gyr
us
Exte
nsive n
eocorti
cal, sp
a ring B
roca
nd
W ernickeareas
Frontal
, spari
ng the
Broca a
rea
Pariet
o-occip
ital, sp
ar ing t
he Wer
nicke
area
-
8/10/2019 Aphasia and Brain Organization
37/204
-
8/10/2019 Aphasia and Brain Organization
38/204
6
CH
APTER 2
1977; M
ohr , 1976;
K erschens
te iner , Poe
ck, Huber,
Stachowia
ck,
W eniger , 1
975).
2.1.2. Poste
rior Languag
e rea
The p
os te r ior
language area
is compose
d ofparts
o
f
th
ete
mporal
neocorte
x,
th
e gyru
s su p r a m a r
g inal is , and th
e g
yrus an gular is
. The
Wernic
ke
area
is
defined in th
is
mo
nograph
as the t
e m p ora l part
o fthe
pos
terior languag
e
a
rea.
T here
seems to be a
gene
ral
ag
reement abou
t the pr
actical
rule
of
thumb fo
llow ed by ne
urosurgeon
s that the
an
terior
part
o f
the
tem
porallobe
up to
Labbe ' s ve
in can be e
xcised without
dire c
on-
sequenc
es
f
or
t
he
language func
t ion. In
neuroa
natomical t e rms
,
Heschl
s
g
yri a re
often g iven as
the
anterior Iimit of
the
W e r n i
cke
are
a . In reg
ard to the p o
ster ior, i t i
s general ly
agreed that
th is
area
is
continuou
s
wi
th the
supramarg
inal and
ang
ular gyri
. The main
disp ar i ty betw
een d iv
erse statem
entsand
diagrams
seems to be that
some
reg
ard
o
nly the
superior tem
pora l c o n v
olut ion as
re levant to
lang
uage, whereas
others
include
t
he
middle, and
some
a
uthors even
the inf
er ior, t emp
ora l gyr
us
(
Bogen B
ogen, 1976)
. Theresul t
s based
on
electric
al cortical s
t imula t ion in
local
anaesthesia
vary
am
ong e
ar ly
report
s (Penfield
R oberts,
1959), w
hich seem to
in dicate a
more
extens
ive area,
and la ter re
ports (
Rasmussen
M
ilner, 1975
; Fed io
van
B uren, 19
75), whi
ch f ind a more
restr icted
area. I have
adopte
d
the
def ini t ion
tha
tthe W
ernicke are
a consists o
f the
posterior
par
t of
the sup
erior and
middle
temporal gyri.
In the opinion of Galaburda (1982), the W ernicke area shows a
degree of ana
t o m ic diffe
rent iat ion, judge
d
by architecton
ic criteria,
closely sim
ilar to
th
at
of the Broc
a area. He
noted :
In fact, arch
itectonic simil
arities between anterior
and
posterior la
n-
guage
areas
and
the
over lap
in
their
conn
ect ional o rgan
izat ion make
it a
somewhat surprisi
ng
finding
tha
t le
sions in
e
ither
region produ
ce su ch
different
aphasic
sy
ndromes.
(p. 443
)
t should
be n
oted
however, that the
studi
es re fer red
to have
been performed
on
rhesus m onkeys Th
e
p o
ster io r l
anguage
area
has
evolved
out of pro
isocortex
located in the
tem
poral and p o
s-
terio
r insula
r
re
gion. t co n
tain s regio
n s o f
varying cytoarch
i tectonic
-
8/10/2019 Aphasia and Brain Organization
39/204
OPERATIONALIZATION OF A MODEL
27
differentiation, from primary auditory sensory cortex to more gen
eralized neocortex, found in
the
inferior parietal lobule
and the
temporo-occipital junction.
Wernicke
1874)
believed
that the
Wernicke area is a store of
auditory
ward
images
Klangbilder).
The condition after injury is there
fore characterized
by
difficulties
with
auditory language perception
(total or partial
ward
deafness) and disturbances of speech (because
the appropriate auditory images for stimulating motor representations
are disturbed).
Geschwind
1979)
stated:
Much
new
information has been
added
in
the past
100 years,
but
the
general principles Wernicke elaborated still seem valid. In this model the
underlying structure of an utterance arises in Wernicke s area. t is
then
transferred through the arcuate fasciculus to Broca s area where it evokes
a detailed and coordinated program for vocalization. (p.
187)
Wernicke aphasia is characterized by fluent, paraphasic speech
and
reduced auditory comprehension. Speech is
produced
without
effort and has complex grammatical structure. Informational content
is deficient (Goodglass Kaplan, 1972;
Huber
Stachowiack, Poeck,
Kerschensteiner, 1975). The term jargon aphasia is sometimes used
for cases in which speech is totally incomprehensible,
but
jargon is
not confined toWernicke aphasia (Benson Geschwind, 1977). Rep
etition is usually disturbed to the same degree as auditory compre
hension, whereas naming performances may vary. Reading and writing
are usually severely disturbed,
but in
some cases,
they
are preserved
(Lecours Rouillon, 1976).
The
supramarginal yrus
is continuous
with the
superiortemporal
gyrus. Wernicke
1874)
regarded the supramarginal gyrus as part of
a continuous perisylvian gyrus, anatomically and functionally contin
uaus
with
the superior temporal convolution. The stimulation
data
seem to
support
this view (Penfield Roberts, 1959; Rasmussen
Milner, 1975). The reason for giving special consideration to this gyrus
isthat the
probability of
an
auditory-language-comprehension defect
is markedly lower with a lesion of the supramarginal gyrus alone than
with a lesion of the superior temporal gyrus (Luria, 1970), whereas
the
probability of
reduced
fluency of speech
with
misarticulation
and
phoneme substitutions increases, possibly because of
the
proximity
to the primary somatosensory cortex. The possibility of finding a
-
8/10/2019 Aphasia and Brain Organization
40/204
28
CHAPTE
R 2
sy
ndrome corre
sponding to
co
nduction
aph
asia may
therefore
exist with
lesions o
f the supra
m arginal g
yrus . Cytoa
rchitectoni
c s tudies
by Gal-
aburda, LeM ay, Kem per,
and
G eschw ind
1978)
indicatethat thepart
of the su
p ramargina
l gyrus imm
ediate ly a
d jacent to
the
sup
erior
tem -
poral g
y rus may
be long to t
he audi tory
associatio
n cortex,
whereas
m or e p
er ipheral p
o r t ions
do not.
The an
gular yrus is c
onvent iona
lly def ined
and is ana
tomically
co
n tinuous w
ith the mid
d le tempor
al gyrus. A
ccording t
o Hensche
n
1922),
only five c
ases wit
h
s
elective inv
o lvem en t o
f the
a
ngular
gyrus
had bee
n publ i shed
up tothat
time. The
pat ients
wereall alexic
and
agraphic
but
had
no
aud i tory
comprehension
defect. Lesions of the
a
ngula r gyr
us occur o
ften wi
th more exten
sive involv
em ent of
the
poster ior
language a
rea.
A
uthors
who use
an extende
dconcept
ofthe
Wernick
e area usu
ally includ
e the angul
a r gyrus e
.g . , Marie,
1906;
D
ejerine, 1
914; Penfie
ld Rober
ts, 1959). W
ernicke
1874) accord
ed
no s
ta tus to
the
angu
lar gy
rus in conn
ect ion w
ith read ing an
dwrit ing
butassumed
that asso
ciation fib
ers from
the occipita
l lobe to
the
Werni
cke area we
renecessar
y for rea din
g . The ass
umption of
a special
im por tance of the
angular
gyrus for reading
and
w riting is widely
adopted
today. So
m e autho
rs also acco
rded it a sp
ecial funct
ion in
w or d
retrieval n
aming) Ge
schwind,
1967
b;
Luria,
1970).
Anomic
apha
sia
is ch
aracter ized
by f luent
speech
with m ar ked
shor tage o
f conte
nt
w
ords . Ther
e is little p
a raphas ia
as such,
but there are
attemp
ts to
subst i t
u te circuml
ocutions an
dvague d
escr iptions
for con
tent w ords .
C
omprehen
sion and repet
ition are g
ood , but
th
ere are sev
ere prob-
le
m s in read
ing an
d
w
riting Goo
dglass K
aplan, 197
2; Kertesz
,
1
979).
les
ion encom
pass ing
bothBroca an
dWernicke
areas produces
a global
aphasia Thi
s
may
be r e
garded as
a composi te
form of ap
has ia
th
at shou
ld not be clas
sified as a
n indep
endent type,
butclinically
it
has d
istinct feat
ures.
t
is c
haracter ize
d by severe
loss in
allla
nguage
modalit i
es , but t
he pa tien t is u
sual ly not mute
Ofte
n ,he or
she has
v
erbal s tereo
types , con
sist ing of c
onvent iona
l phrases
sw earing) or
m eaningle
sssyllabic c
ombinat ion
s. In audi t
o ry com pr e
hension , th
e re
is
also some a
bility to re
act to con cr
ete words ,
particularl
y if they ar
e
em otionall
y significan
t for the pa t
ient Stach
owiak, Hub
er , Kersch
en-
stein
er, Poeck,
Wenige
r, 1977).
-
8/10/2019 Aphasia and Brain Organization
41/204
OPERATIONALIZATION OF A MODEL
29
2
1 3 Arcuate
Fasciculus
Very precise descriptions of this cortico-cortical fiber
bundle
are
hard
to find. t has a compact middle
portion
sweeping around the insula
parallel to the circular sulcus. The
ends
fanout
and connect the infe
rior
and
middle frontal convolutions
with
large parts of the convexity
of the temporal lobe. The existence of a direct projection from
auditory
areas to a homologue of the Broca area has been confirmed in rhesus
monkeys
by
Pandya
and Galaburda (1980).
This fiber
bundle
is
one among
several structures
assumed
to
be of functional importance
in
connecting
the
posterior language area
with the Broca area. Wernicke believed
the
insula to have this func
tion, but this possibility is now considered unlikely, and in the neo
classical literature, the
arcuate fasciculus is accepted as the major
functional connection. Lesions of the fascicle result in a conduction
aphasia
with relatively fluent speech and
good comprehension,
but
repetition difficulty. Fluency may be less than
in
Wernicke aphasia,
because the patient makes frequent attempts to correct literal para
phasias
phoneme
substitution errors).
He
or
she may
go
through
a
series of approximations in attempting to correct his or her production
( zeroing in ). In addition to
good
auditory
comprehension,
there is
also often
good
reading comprehension (Benson, Sheremata, Bou
chard, Segarra, Price, Geschwind, 1973;
Green
Howes, 1977;
Benson Geschwind, 1977).
Lesions outside the language areas
mentioned
above may pro
duce
aphasia. This means not that the areas injured have language
functions,
but
that
the language areas normally interact
with
sur
rounding areas when language is integrated in complex behaviors.
The essential feature of
such
lesions producing aphasia is
that they
disconnect or isolate parts of the entire language areas from the sur
rounding
cortex.
Total isolation produces an isolated speech area syndrome. The
patient
has no
spontaneaus
speech but responds to questions. The
response is afmost f i l ~ w a y s a direct repetition of the question. Speech
is weil aiticulated ~ d tb:e patient repeats even long sentences 'He or