
Aortic Stenosis Echo Clinical Conference March 10, 2010 Anne B. Riley.
42
Aortic Stenosis Echo Clinical Conference March 10, 2010 Anne B. Riley
-
Upload
mustafa-burroughs -
Category
Documents
-
view
221 -
download
0
Transcript of Aortic Stenosis Echo Clinical Conference March 10, 2010 Anne B. Riley.

Aortic Stenosis
Echo Clinical Conference
March 10, 2010
Anne B. Riley

Outline
• Epidemiology
• Etiology
• Disease Course
• Imaging evaluation
• Management
• New Technologies

Epidemiology
• Common disease: In a population-based echocardiographic study, 2% of persons 65 years of age or older had frank calcific AS, 29% exhibited age-related aortic valve sclerosis without stenosis
• Bicuspid valves present in 1-2% of population
• Calcific valve disease, even in the absence of valve obstruction, is associated with a 50% increased risk of CV death and MI
Braunwald’s Heart Disease.

Etiology
A. Normal Valve
B. Congenital Bicuspid valve
C. Rheumatic aortic stenosis
D. Calcific degenerative AS

Calcific Aortic Stenosis
Lipocalcific changes on aortic side of cusp
Sparing of commissures
Mechanical stress: highest at aortic side in the flexion area, near attachment to aortic root

Calcific Aortic Stenosis: PathologyCells, lipid and matrix in subendothelial location, elastic lamina displaced
Greater accumulation of cells, lipid and matrix in subendothelial location, elastic lamina fragmented
Freeman, et al. Spectrum of Calcific Aortic Valve Disease: Pathogenesis, Disease Progression, and Treatment Strategies. Circulation 2005.

Calcific AS: Pathogenesis
•Lipid accumulation
•Inflammation
•Calcification
Freeman, et al. Spectrum of Calcific Aortic Valve Disease: Pathogenesis, Disease Progression, and Treatment Strategies. Circulation 2005.

Bicuspid valvesExist in 1-2% of the populuation
More prevalent in men (70-80% of cases)
Subset of bicuspids have autosomal dominant inheritance with incomplete penetrance
Have associated dilatation of the ascending aorta (unrelated to degree of AS or AR), related to abnormalities of the media
Histopathology of calcific stenosis of a bicupsid valve is the same as that of a trileaflet valve
Increased turbulent flow and leaflet stress is felt to accelerate the changes-> earlier age of presentation (about 20 years earlier)

Roberts WC et al. Frequency by Decades of Unicuspid, Bicuspid, and Tricuspid Aortic Valves in Adults Having Isolated Aortic Valve Replacement for Aortic Stenosis, With or Without Associated Aortic Regurgitation. Circulation 2005.
Men No (%)
Unicuspid34 (6)
Bicuspid309 (53)
Tricuspid234 (40)
Uncertain7 (1)
Subtotal584 (100)
Women
Unicuspid12 (3)
Bicuspid149 (43)
Tricuspid183 (53)
Uncertain4 (1)
Subtotal348 (100)
Time period: January 1993 through June 2004, Baylor University
Procedure: AVR for isolated aortic stenosis
Exclusions: Mitral valve replacement or mitral stenosis, previous aortic valvoplasty
RESULTS:
Age <50 (7% of patients) 2/3 bicuspid, 1/3 unicuspid
Age 50-70 (40% of patients) 2/3 bicuspid, 1/3 tricuspid
Age >70 (53% of patients) 2/5 bicuspid, 3/5 tricuspid
Bicuspid Valves: Very Common reason for AVR

Rheumatic Heart Disease
• Fusion of commissures between the leaflets and leaflet vascularization-> leads to retraction and stiffening of free borders of the cusps
• Small round or triangular opening
• Calcific nodules develop on both surfaces
• Often have AI and AS• Usually involves the mitral
valve as well• Valve often regurgitant and
stenotic

Aortic Stenosis: Disease Course
Onset of symptoms to time of death
Heart failure: 2 years
Syncope: 3 years
Angina: 5 years

Hemodynamic progression
• Valve area 0.12 cm2/yr
• Aortic jet velocity 0.32 m/sec/yr
• Mean gradient increase 7 mm Hg/yr

Predicting Events
Rosenhek, R. et al. The Natural History of Very Severe Aortic Stenosis. Circulation 2010;121:151-156

Evaluation
• Echocardiography–M mode
– 2-D imaging
– Doppler
• Cardiac Catheterization

Echocardiography: M mode
Dense persistent echoes
Obscures normal leaflet motion

Two Dimensional Echocardiography
• Look for…– Extent of calcification of the leaflets and the aortic
root (including the aortic ring)
– Degree and pattern of leaflet motion• Doming pattern, asymmetric closure (? Bicuspid valve)
– Post-stenotic dilatation of the aortic root
– LVH

Doppler Echocardiography: Velocity
• Continuous wave doppler from multiple sites to sample flow across the valve
• To get highest velocity: need angle of interrogation to be as parallel with flow as possible
• Angles greater than 30 degrees result in major underestimation

From Velocity to Pressure:Bernoulli Equation
ΔP = ½ p (v22- v1
2) + p (dv/dt)dx + R(v)
ΔP Pressure gradient across valve (mm Hg)
p Mass density of blood (1.06 x 103 kg/m3)
v2 Velocity in stenotic jet
v1 Velocity proximal to stenosis
(dv/dt)dx Time-varying velocity at each distance along flowstream
R(v) Constant for viscous resistance

Modified Bernoulli
Simplified Bernoulli equation to obtain
peak instantaneous gradient
Peak pressure gradient= 4 x peak velocity²

Mean Pressure Gradient
ΔPmean = ΔPmax/1.45 + 2 mm Hg
Mean gradient is approximately 2/3 of the peak instantaneous gradient
Most often obtained by planimetry of the Doppler envelope

Doppler Echocardiography
Non-invasive assessment of aortic stenosis by Doppler Ultrasound. L Hatle et al. 1980; 43 284-292.
“In 57 of 63 patients with aortic stenosis, the aortic jet could be reached by the ultrasound beam and, in 37 of these, peak pressure drop by ultrasound was compared with that obtained at catheterization. In patients less than 50 years of age the aortic jet was easy to find, the measurement was reproducible, and underestimation of the pressure drop obtained at catheterization was within 25 per cent in 17 of 18 patients. In patients over 50 years Doppler signals from the aortic jet were more difficult to obtain, and pressure drop was significantly underestimated in one-third, but time of maximum velocity in systole could indicate whether moderate or severe aortic stenosis was present. “

Velocity and AVA
Vmax (m/s) Severity
>4 Severe
3-4 Moderate
1.6-3 Mild
<1.5 Normal
2006 AHA/ACC Guidelines

AVA: Continuity Equation
SV=Cross Sectional Area * TVIAVA= CSAot * TVI ot/TVI av
CSA = r²Simplified continuity equation: AVA= CSA ot * Vot/Vav
Stroke volume proximal to aortic valve must equal the stroke volume through the stenotic orifice
Bernoulli alone vs. Continuity Equation
• Increasing stroke volume increases the gradient– Coexisting AR
– Hyperdynamic LV function
• Decreasing stroke volume decreases the gradient even in presence of severe stenosis– Severe LV dysfunction
– Coexisting MR
• Continuity equation should not be affected

Case Example




Cardiac Catheterization
Otto. Textbook of Clinical Echocardiography.
Measures peak to peak gradients vs. Dopplers instantaneous gradients
Peak to peak gradients never actually exist
Mean gradients correlate better between cath and echo
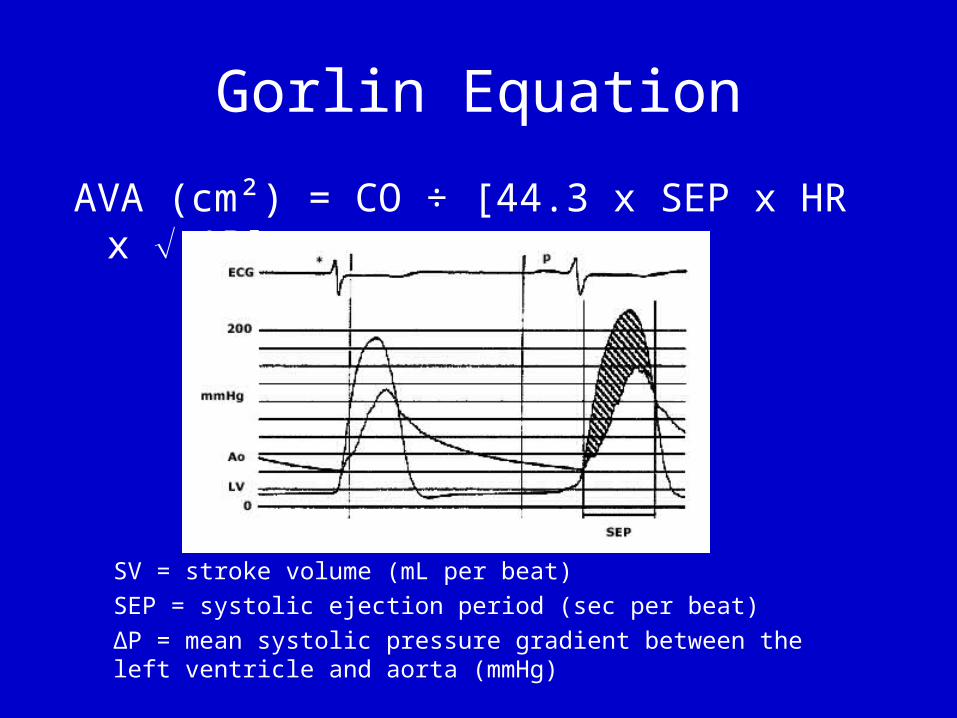
Gorlin Equation
AVA (cm²) = CO ÷ [44.3 x SEP x HR x ΔP]
SV = stroke volume (mL per beat)
SEP = systolic ejection period (sec per beat)
ΔP = mean systolic pressure gradient between the left ventricle and aorta (mmHg)

Echo challenges
The Aortic Jet• Search for the highest frequency signal- assumed
to present the nearest-parallel angle between the ultrasound in the direction of the jet
• Intercept angles within 15 degrees of parallel result in error of velocity of <5%
• Pitfalls: Inability to align the interrogation angle parallel to flow, mistakenly identify the jet (MR, TR, VSD, PA stenosis, Subaortic stenosis)
• Variability in velocity in irregular heart rhythms (afib, PVCs)

Echo Challenges (cont)
Outflow tract diameter• Measured in mid-systole, just proximal to and
parallel to the plane of the stenotic AV from the inner edge of the septal endocardial echo to the leading edge of the base of the anterior mitral leaflet
• Parasternal long axis view• This measurement shows the greatest intraoberver
and interobserver variability• Small errors in measurement lead to larger errors
in CSA

Echo Challenges (cont)
Outflow tract velocity• Measured using pulsed doppler echo
• Outflow tract diameter and velocity signals need to be recorded at the same anatomic site
• Measure both immediately adjacent to the valve
Therapy: Medical
The Statin Story
• SALTIRE Trial: Scottish Aortic Stenosis and Lipid Lowering Trial, Impact on Regression (NEJM 2005)– 155 calcific AS patients (aortic jet velocity>2.5 m/s, calcification seen on TTE, mean AVA
1.03 cm2)– Randomized to atorvastatin 80 mg vs. placebo– Endpoints: change in aortic jet velocity and aortic valve calcium score– 25 month follow up: no difference in progression of aortic valve calcification or rate of
increase in aortic jet velocity
• RAAVE Study: Rosuvastatin Affecting Aortic Valve Endothelium (JACC 2007)– 121 patients with moderate to severe AS
– Non-random assignment to rosuvastatin 20 mg if LDL > 130 mg/dL or to no statin if LDL < 130 mg/dL
– Endpoints: aortic valve area, aortic jet velocity
– 73 weeks follow up, patients treated with rosuvastatin had significantly slower rates of deterioration in mean aortic valve area and aortic jet velocity

Statins, continued
SEAS Trial: Simvastatin and Ezetimibe in Aortic Stenosis (NEJM 2008
• 1873 adults with mild to moderate aortic stenosis• Randomly assigned to treatment with simvastatin 40 mg plus ezetimibe 10 mg or
placebo• At 52 months follow up: no difference in the primary endpoint: CV death, AVR,
non-fatal MI, hospitalized unstable angina, CHF as a result of progression of AS, CABG, PCI, and non-hemorrhagic stroke.
• No difference in the rate of aortic valve replacement (28 versus 30 percent) or in the rate of hemodynamic progression of aortic stenosis
• Fewer ischemic events in the treatment group, due to a lower rate of CABG at the time of aortic valve surgery
• Higher rate of cancers in simvastatin-ezetimibe group

Therapy: Surgical
ACC/AHA 2006 guidelines
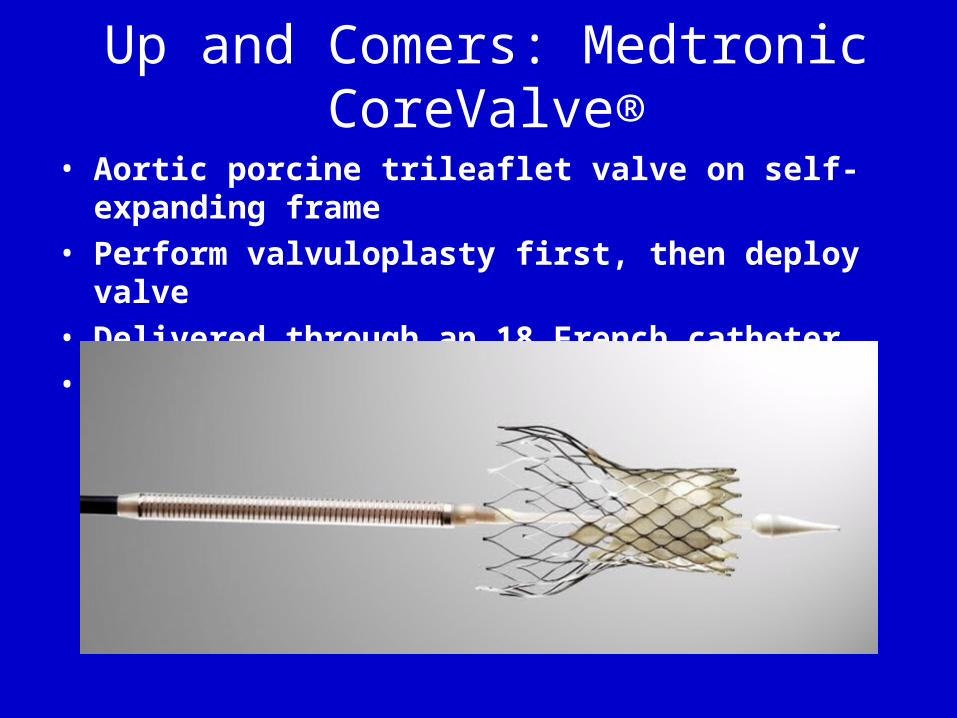
Up and Comers: Medtronic CoreValve®
• Aortic porcine trileaflet valve on self-expanding frame
• Perform valvuloplasty first, then deploy valve
• Delivered through an 18 French catheter
• US clinical trial scheduled to start Summer 2010

Medtronic CoreValve

Edwards SAPIENTM Percutaneous Valve
Equine pericardial trileaflet valve is sewn within a stainless steel frameDeployed via transfemoral or transapical approachBalloon inflation used to deploy the valvePARTNER trial underway



















