Sonoanatomy Scanning technique and basic pathology of the shoulder

a
Vascular Surgery Center
National Center for Cardiovascular Diseases.
Fuwai Hospital, CAMS & PUMC Beijing, China
Aortic Arch pathology options: Open,Hybrid,fenestration, Chimney or branched stent-graft?
Chang Shu, M.D., Ph.D
Email: [email protected]

Disclosure of Conflicts
None.

Total Volume of Aortic Surgery in
Fuwai Hospital(1997-2016)
1143 aortic operations in 2016:
1.9% of mortality.
573 open repair, 93 hybrid procedure, 477 endo-repair
1143 cases
Current Approaches for Arch
Open Repair
Total arch replacement
Hybrid TechniquesHybrid arch replacement
Debranching + TEVAR
Extra-anatomic bypass + TEVAR
Total Endo Techniques
Fenestrated stent-graft
Branched stent-graft
Chimney technique

OPEN REPAIR:
Total arch replacement
Suitable for arch anatomy, with or without elephant trunk implantation and ascending replacement.
Standard approach with credible long-term durability.

Standard option(2014 ESC, 2010 ACC/AHA/ACCF)
Circulatory arrest is mandatory
Peri-operative complications(cerebral, renal, spinal)
Risk arises in aged patient and co-morbidities
IRAD:Mortality 24.7%( Circulation 2004)
IRAD:Mortality 17%-26% (2016)
OPEN REPAIR:
Total arch replacement

Age Distribution in Treated Patients
in Fuwai Hospital
Percentage of aged patients increased every year, age is the first
risk factor of mortality and it limits open repair utilization.

Categories of Hybrid Procedure
RCCA – LCCA – LSARSA– LCCA RSA– LSA
De-branching:
Arch branch
transposition
Hybrid arch
replacement
Extra-anatomic bypass + TEVAR

Aortic arch pseudoaneurysm
Hybrid technique was adopted.
Ascending aorta – innominate artery – left carotid artery –
LSA bypass was achieved first.
Then TEVAR was used.
The patient recovered unevertfully.
Debranching ProcedureAscending - Supra Aortic Branches transposition
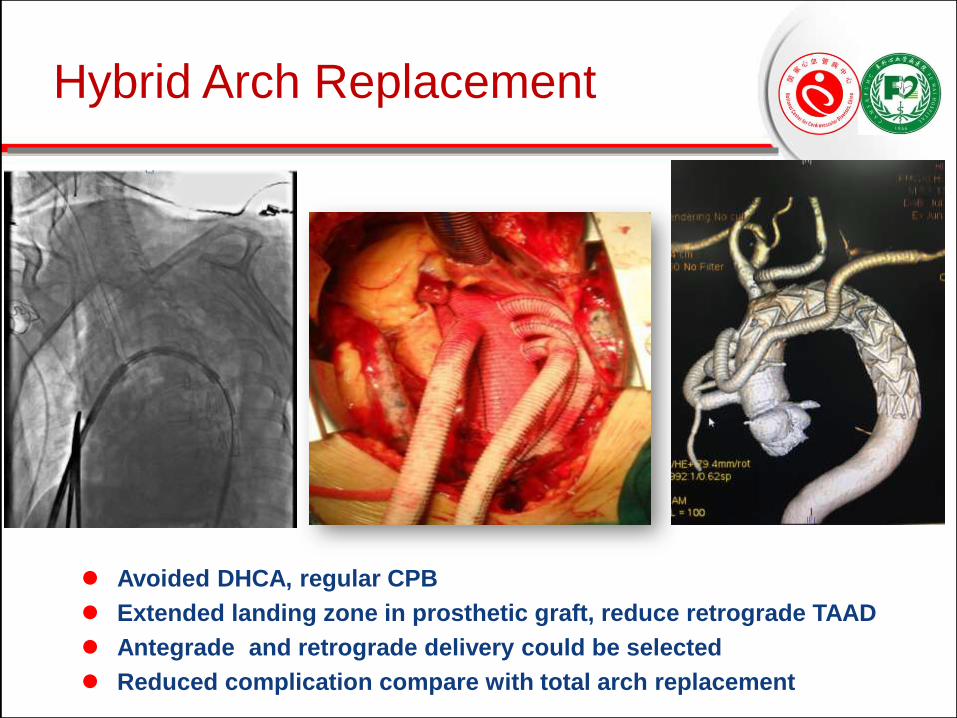
Avoided DHCA, regular CPB
Extended landing zone in prosthetic graft, reduce retrograde TAAD
Antegrade and retrograde delivery could be selected
Reduced complication compare with total arch replacement
Hybrid Arch Replacement

Hybrid procedure
Mata Analysis Results(2010)Overall 30-day mortality:8.3%
EL:9.2%
stroke:4.4%
paraplegia:3.9%
No affect between On or off-pump.
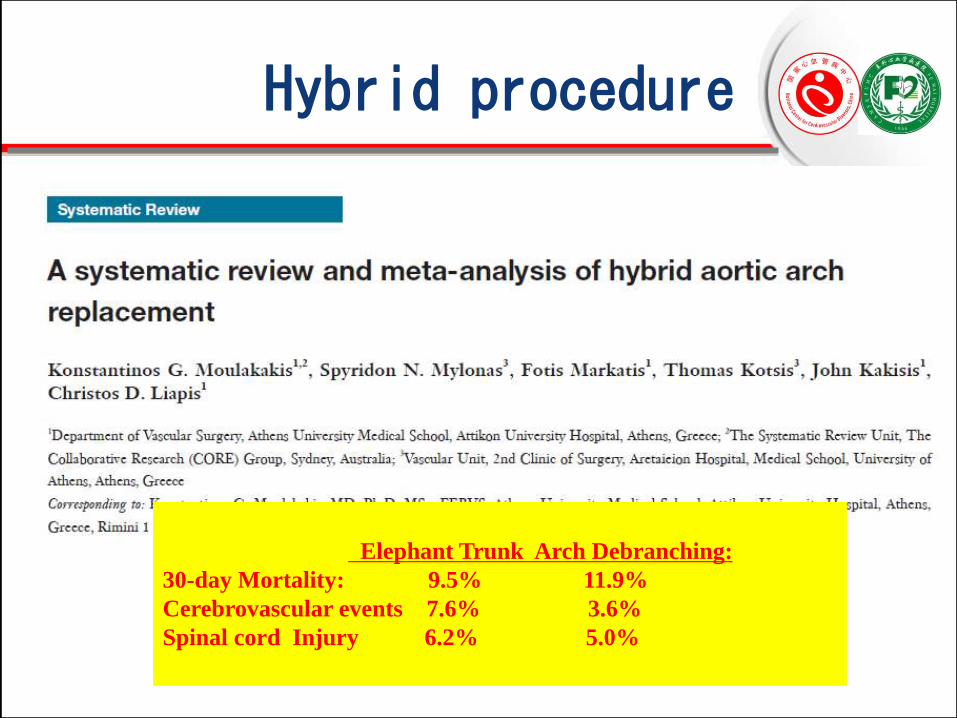
Elephant Trunk Arch Debranching:
30-day Mortality: 9.5% 11.9%
Cerebrovascular events 7.6% 3.6%
Spinal cord Injury 6.2% 5.0%
Hybrid procedure

For aortic arch pathology, minimal invasive
option is preferred in decision-making.
Adopted from Ivan Casserly MB
Massive
InvasiveLess
Invasive
Minimal
Invasive
Non-
invasiv
eOpen repair:
Better exposureHybrid:
InterimTotal-Endo
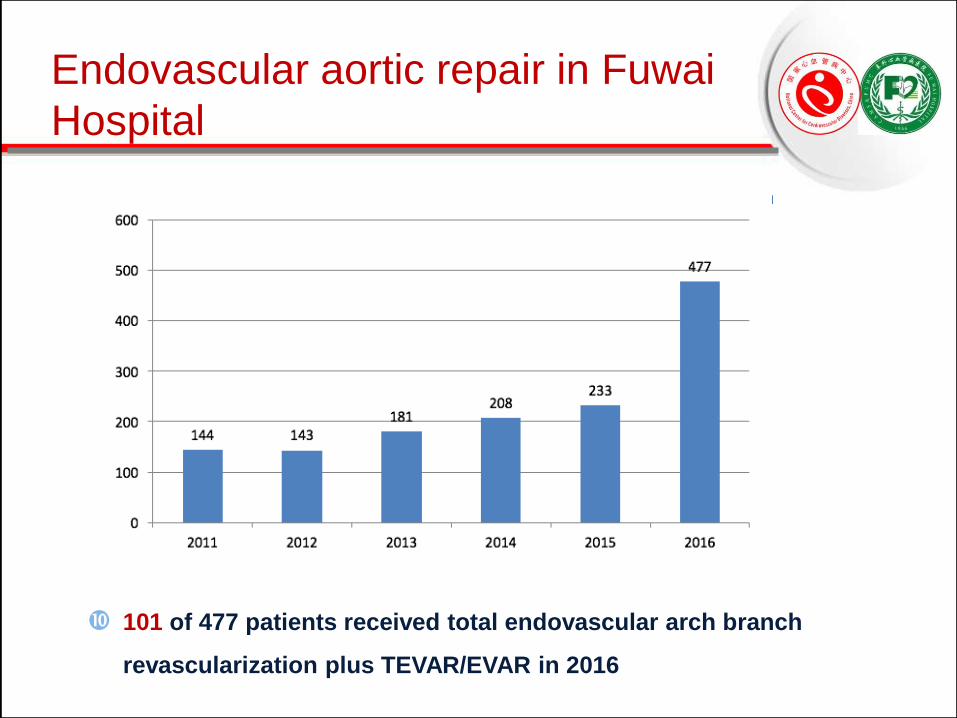
101 of 477 patients received total endovascular arch branch
revascularization plus TEVAR/EVAR in 2016
Endovascular aortic repair in Fuwai
Hospital

Endovascular aortic repair in Fuwai Hospital &
Second Xiangya Hospital(Nov2015-Nov2017)
Total TEVAR 1593
Arch branch
revascularization
354
Single Chimney 168
Double Chimney 16
Triple Chimney 2
Fenestration 92
Double Fenestration 8
Triple Fenestration 6
Snorkel 8
168
162
92
8 6 8
Single Chimney Double Chimney Triple Chimney
Fenestration Double Fenestration Triple Fenestration
Snorkel
Single
ChimneyFenestration

Fenestrated
Technique Branched
Stent-graftChimney Technique
Double Chimney
Technique
Total Endovascular Repair of
Supra-arch Branch

Nov, 2007
The 1st case of CSG
2008
CSG + PDA occluder
2009
Double CSG
2016
Triple CSG
Chimney Stent-graft (CSG)

During 1.5 years
follow up, no
complication
happened.
As a result, double
chimney technique
can be used for
retrograde type A
aortic dissection
with caution.
Double Chimney Technique

The patient, 84 years old, male,
received TEVAR for aortic aneurysm
in 2005, and suffered from chest pain
for 1 month.
With the development of
popularization of endovascular
technique and increasing of average
life span, more and more post-TEVAR
complications will happen and need
secondary intervention in the future.
Double Chimney Technique
Double chimney technique is a efficient and safe technique to
extend the proximal landing zone of aortic arch, especially for
aged patient.

• 3 months after TEVAR plus triple chimney procedure
• Double chimney with LSA snorkel stent
Triple Chimney Technique

Institutional outcomes in Fuwai TeamChimney Cohort
122 cases report from our center
Overall results:
Technical Success Rate:98.6%
84.2% free from any EL
80.6% free from any adverse events
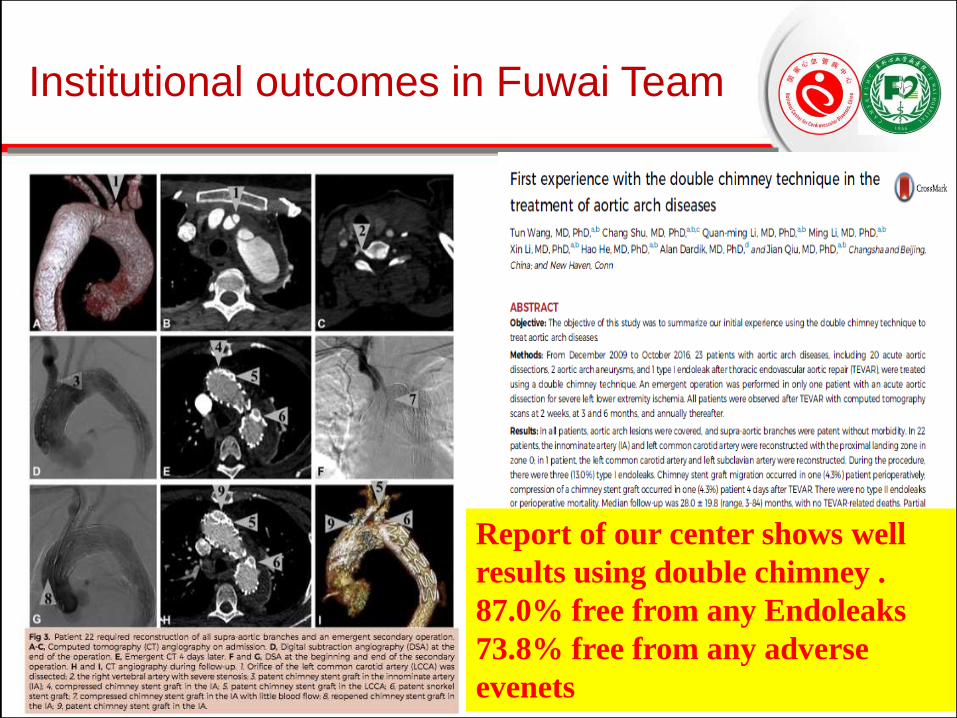
Report of our center shows well
results using double chimney .
87.0% free from any Endoleaks
73.8% free from any adverse
evenets
Institutional outcomes in Fuwai Team

Chimney Stent-graft (CSG)
2017 Meta-analysis report
373 patients and 387 CGs
Overall technical success :91.3%
Pooled 30-day mortality:7.9%
Overall early type Ia EL:9.4%
Early patency,:97.9%
Late patency:92.9%
Retrograde type A dissection:1.8%
Stroke, 2.6%

Fenestration Technique
Fenestration
In Vitro
Fenestration
In Situ
Fenestration
Off-the-shelf
Fenestration
Physician-modified
Fenestration
In Situ Needle
Fenestration
In Situ Laser
Fenestration

In Vitro Fenestration:
Physician-modified fenestration

Fenestration:Branch stent insertion
Pre-dilation and modelling of fenestration
Antegrade fashion:
Via femoral access
Retrograde fashion:
Via branchial access

On-the-table manner of In vitro fenestrationplus LSA branchstenting

LCCA + LSA: in vitro fenestration with Viabahn insertion
Inominate artery: Chimney with Fluency insertion
Double Fenestration plus chimney

Ballooned fenestration needle in facilitating in situs Fenestration
Fenestrated Graft:
In situs fenestration

In situ fenestration

In situ fenestration

Ann Thorac Surg 2016
In situs fenestration:
from single to multiple branch
• Total 3-Arch Repair Using In Situ Fenestration for Arch
Aneurysm, reported by Katada in 2016
• Success rate: 6/7 ------Ann Thorac Surg 2016

Physician-modified vs Off-the-shelf Fenestration
Overall clinical treatment success :
Physician-modified fenestration 91.4%
Off-the-shelf fenestration 95.0%

Branched stent-graft
Branched stent-graft
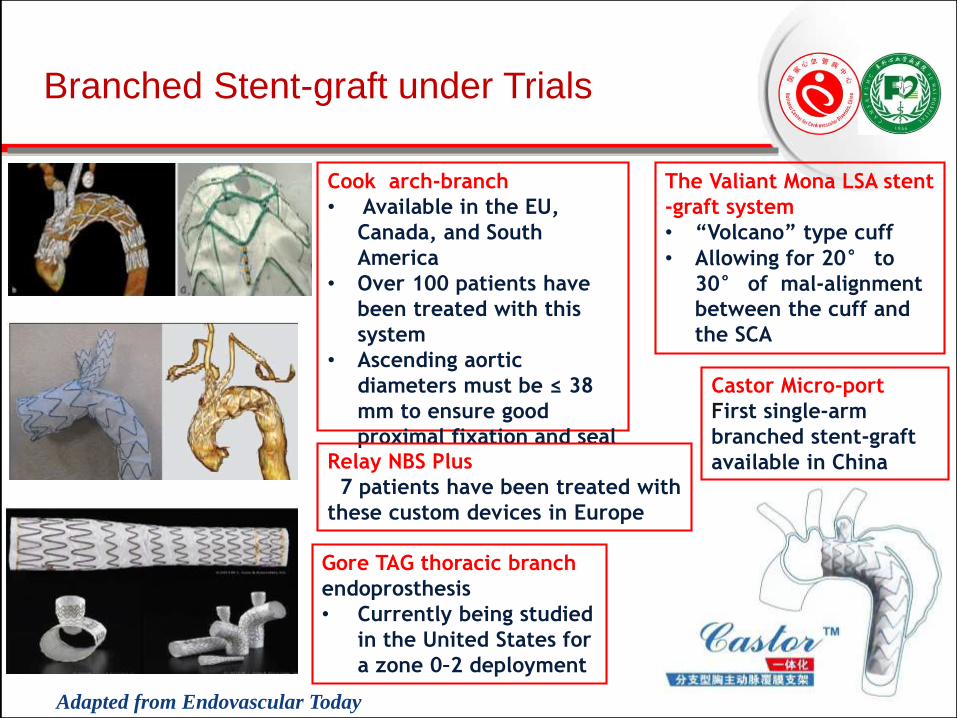
Branched Stent-graft under Trials
Gore TAG thoracic branch
endoprosthesis
• Currently being studied
in the United States for
a zone 0–2 deployment
Cook arch-branch
• Available in the EU,
Canada, and South
America
• Over 100 patients have
been treated with this
system
• Ascending aortic
diameters must be ≤ 38
mm to ensure good
proximal fixation and seal
The Valiant Mona LSA stent
-graft system
• “Volcano” type cuff
• Allowing for 20° to
30° of mal-alignment
between the cuff and
the SCA
Adapted from Endovascular Today
Castor Micro-port
First single-arm
branched stent-graft
available in ChinaRelay NBS Plus
47 patients have been treated with
these custom devices in Europe
Open portion procedure remains standard approach for aortic arch
pathology with long-term durability yet higher mortalities.
Hybrid and total endovascular procedure may substitute open repair
for patients with significant comorbidities.
Endo-techniques and devices, including fenestrated stent-graft/
branched stent-graft/ chimney technique are expected and should be
done individually according to the aortic arch pathology.
For total endo-technique(Fenestration and chimney approach, etc.),
long-term durability, efficacy and safety remains to be investigated in
larger patient cohorts before being widely adopted.
Conclusion and Prospective

Thank You!
2018 China Vascular Congress (CVC)
&
Annual Meeting of National Society of
Vascular Surgery, China (NSVS)
Welcome You!
August 2018, Beijing, China