“Recommended but unfunded · •Ajit Johal BSc (Pharm) RPh BCPP CDE CTH •Community Pharmacist...
90
“Recommended but unfunded vaccines” Creating health equity amongst those vulnerable to vaccine preventable diseases Ajit Johal Director of Immunize.io initiative
Transcript of “Recommended but unfunded · •Ajit Johal BSc (Pharm) RPh BCPP CDE CTH •Community Pharmacist...

“Recommended but unfunded vaccines”
Creating health equity amongst those vulnerable to vaccine preventable diseases
Ajit Johal Director of Immunize.io initiative

Outline of Today’s Workshop
• Introduction: Vaccine preventable diseases how far have we come, where do we need to go?
• Seasonal Influenza • Influenza Quiz (Kahoot!)• Pneumococcal Disease • PD Quiz (Kahoot!)• Herpes Zoster Virus • HSV Quiz (Kahoot!)• Conclusion: Improving Access to Recommended
Vaccines for Seniors

Instructions to use Kahoot!
• Go to the website: https://kahoot.com/welcomeback/
• Login: Username= TravelRx and Password: TravelRx
• Click on the “Kahoots” button on the top left side of the screen: There it will show all 3 quizzes (Influenza, Pneumonia and Shingles)
• Select the quiz you would like to play

References: 1.Smallpox | CDC [Internet]. Cdc.gov. 2018 [cited 9 November 2018]. Available from: https://www.cdc.gov/smallpox/index.html

References: 1.History of Smallpox | Smallpox | CDC [Internet]. Cdc.gov. 2018 [cited 9 November 2018]. Available from: https://www.cdc.gov/smallpox/history/history.html

References: 1.Smallpox | CDC [Internet]. Cdc.gov. 2018 [cited 9 November 2018]. Available from: https://www.cdc.gov/smallpox/index.html

References: 1.Smallpox | CDC [Internet]. Cdc.gov. 2018 [cited 9 November 2018]. Available from: https://www.cdc.gov/smallpox/index.html



References: 1.Smallpox | CDC [Internet]. Cdc.gov. 2018 [cited 9 November 2018]. Available from: https://www.cdc.gov/smallpox/index.html

References: 1.Smallpox | CDC [Internet]. Cdc.gov. 2018 [cited 9 November 2018]. Available from: https://www.cdc.gov/smallpox/index.html

References: 1.Smallpox | CDC [Internet]. Cdc.gov. 2018 [cited 9 November 2018]. Available from: https://www.cdc.gov/smallpox/index.html

References: 1.Smallpox | CDC [Internet]. Cdc.gov. 2018 [cited 9 November 2018]. Available from: https://www.cdc.gov/smallpox/index.html

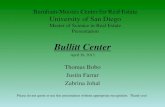
The Success of Vaccines in the 20th century
Centers for Disease Control and Prevention. The Pink Book: Course Textbook – 13th Edition (2015). Appendix E: Impact of Vaccines in the 20th and 21st Centuries. Available at: http://www.cdc.gov/vaccines/pubs/pinkbook/downloads/appendices/E/impact.pdf
JAMA. 2007;298(18):2155-2163. ; CDC. MMWR August 15, 2014;63(32);702-715.
Disease20th Century Annual
Morbidity2013 Reported
Cases% Decreases
Smallpox 29,005 0 100%
Diphtheria 21,053 0 100%
Pertussis 200,752 28,639 86%
Tetanus 580 26 96%
Polio (paralytic) 16,316 1 >99%
Measles 530,217 187 >99%
Mumps 162,344 584 >99%
Rubella 47,745 9 >99%
Congenital Rubella Syndrome (CRS)
152 1 99%
Haemophilus influenzae (B)
20,000 (est.) 31§ >99%
14

Life Expectancy at Birth(US)
Age
(Yrs)
Year

Add “Life to Years”
“For the first time in human history, the world will soon have more older people than children. The human race is ageing and we are unprepared. Unless we change the way we think and act about ageing, we will miss the opportunity to age in good health and to build a society where older people are respected and valued members of society.”
WHO March 28, 2018 - Add "life to years" through healthy ageing

BC Seniors Guide – 11th Edition Published 2016 http://www2.gov.bc.ca/gov/content/family-social-supports/seniors/about-seniorsbc/seniors-
related-initiatives/bc-seniors-guide
BC Overview: Seniors
17

Aging Population




About Me
• Ajit Johal BSc (Pharm) RPh BCPP CDE CTH
• Community Pharmacist
• Clinical Instructor and Course Coordinator at UBC Faculty of Pharmaceutical Sciences
• Area’s of interest - Infectious Disease, Immunology, Vaccines

Influenza
in·flu·en·zaˌinfləˈwenzə/nouna highly contagious viral infection of the respiratory passages causing fever, severe aching, and catarrh, and often occurring in epidemics.

Older Canadians suffer disproportionately from
influenza-related morbidity and mortality
...they experience:
• 70% of influenza-related hospitalizations AND
• >90% of influenza-related death2
While adults over 65 represent just 15% of the Canadian
population…1
References:1. Statistics Canada Population projections: Canada, the provinces and territories, 2013 to 2063. Available at: http://www.statcan.gc.ca/dailyquotidien/140917/dq140917aeng.htm. Accessed on October 8, 2015.2. Public Health Agency of Canada (PHAC). FluWatch. May 3 to May 9, 2015.

Influenza and Seniors: Worse than you Think!
• https://www.youtube.com/watch?v=nmQN4JRVkUs&t=1s

Influenza Worsens Comorbidities1-3
Among those without comorbidities, influenza can lead to new infections such as
secondary bacterial pneumonia, increase the risk of cardiac complications, etc.
References:
1. CDC. http://www.cdc.gov/flu/about/disease/us_flu-related_deaths.htm. Accessed January 17, 2013.
2. CDC. http://www.cdc.gov/flu/keyfacts.htm. Accessed January 16, 2013.
3. Capua I, et al. J Virology 2013;87(1):597-610.
Among those with comorbidities, influenza often aggravates existing
chronic illness, such as:
Congestive heart failure
Chronic Obstructive Pulmonary Disease (COPD)
Asthma
Diabetes
Deaths from influenza-related complications are typically attributed to
these underlying or secondary illnesses
26

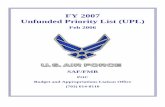
Comorbidities Increase Mortality from Influenza
amongst Older Adults
References:
1. Barker WH, Mullooly JP. Arch Intern Med. 1982;142(1):85-89.
9
217
797
0
225
450
675
900
None 1 ≥2
Death
s p
er
10
0,0
00
po
pu
lati
on
Number of high-risk conditions
Chart Title
Death rates from influenza and pneumonia among persons
≥65 years of age: Epidemics in 1968-1969, 1972-1973
27

Co-morbidities Associated with Influenza-attributed mortality
For adults aged 65 years and over, the risk for influenza-attributed death was1:
Greater among those with both chronic heart and lung conditions
20x
Greater among those with chronic lung diseases12x
Greater among those with chronic heart diseases
5x
1.An Advisory Committee Statement (ACS)/National Advisory Committee on Immunization (NACI): Canadian Immunization
Guide Chapter on Influenza and Statement on Seasonal Influenza Vaccine for 2016–2017.
2.Schanzer DL, et al. Co-morbidities associated with influenza-attributed mortality, 1994–2000, Canada. Vaccine. 26 (2008)
4697–4703.

In 2014–2015, hospitalizations caused by influenza A and B
were highest among adults over 65…1
Cumulative number of hospitalizations with influenza reported by the participating provinces and territories, Canada, 2014–2015
…but influenza A, especially H3N2, was by far the leading cause of hospitalization among seniors.
Adapted from Public Health Agency of Canada (PHAC). FluWatch 2014—2015.
Reference:1. Public Health Agency of Canada (PHAC). FluWatch. August 16 to August 29, 2015.

Immunosenescence, Imflammaging, and Influenza
Influenza A vs Influenza B
• Influenza B strain - Influenza B viruses circulate widely only among humans
• Influenza A strain - influenza A viruses circulate among both humans and many animal populations. The primary reservoir for influenza A viruses is wild waterfowl and other wild birds, but viruses are common in swine populations as well. Influenza A viruses can also infect other animal species, such as poultry, cats, dogs, horses, sea lions, and bats.
30

Secondary Bacterial Infection with Pneumonia
• Up to 65% of influenza infections have resulted in secondary bacterial infection
• Most common bacteria associated with secondary infection during influenza are:
• S. pneumonia
• H. influenzae
• S aureus
• High risk populations are young children and elderly
• Prevention: Get vaccinated with Pneumococcal vaccine and Flu shot!!
References: 1.Morris DE, Cleary DW, Clarke SC. Secondary bacterial infections associated with influenza pandemics. Frontiers in microbiology. 2017 Jun 23;8:1041.

High-risk Plaque Formation
Infections like influenza may result in exacerbation of underlying inflammatory processes of athlerosclerosis
References: 1.Madjid M. Eur Heart J. 2007;28 (10):1205-1210. 2. Ross R. Nature. 1993;362(6423): 801-809. 3. Warren-Gash C, et al. Lancet Infect Dis. 2009;9(10):601-610. 4. Harskamp
RE, van Ginkel MW. Ann Med. 2008;40(2):121-128. 5. Phrommintikul A, et al. Eur Heart J. 2011;32(14):1730-1735.
Severe inflammation during acute infection
Inflammation → Plaque Rupture → Coagulation Cascade → Acute Coronary Syndrome
“The influenza virus has extensive effects on inflammatory and coagulationpathways, which might lead to destabilization of vulnerable atheroscleroticplaques and thus coronary artery occlusion – the major cause of acutemyocardial infarction (AMI)”3
1 2
34
Influenza→ Inflammation→ Potential AMI1-5

AMI after Influenza
• Of 277k respiratory virus tests, 19k influenza
• 499 of these hospitalized for AMI
• Of these, 332 unique patients and had flu in week before AMI– Risk AMI (incidence ratio) 6-fold
higher in week after flu
• Risk also increased for AMI following RSV and other viruses by about 3-fold
Kwong JC, et al, N Engl J Med 2018; 378:345-353

Influenza hits Nursing homes hard
• BC Flu watch - To date this season, 1,508 influenza/ILI outbreaks have been reported, of which 917 (61%) occurred in LTC facilities.
Does this sound FAMILIAR TO YOU?
• This leads to strict infection control measures to deal with a number of influenza outbreaks.

Welcome to…..
u·to·pi·ayoo͞ˈtōpēə/nounan imagined place or state of things in which everything is perfect.

Utopia in LTC

Quality of Life
• Meals delivered to client rooms
• Family visitations limited
• Emotional Impact
• Decreased staffing
• Decreased services
• Bed closures
• Decreased Admissions

Influenza Negatively Affects Functional Status in Nursing Home Residents
Reference: 1. Gozalo PL, et al. J Am Geriatr Soc. 2012;60(7):1260-1267.
Quarterly pattern of the rate of decline of activities of daily living [ADL ( )] vs influenza city-level mortality ( ) for long-stay (>90 days) nursing home residents in 122 CDC-monitored cities in the US, 1999-2005.
WORSE
BETTER
38
FunctionDressingBathingEatingToiletingTransferringBed mobilityLocomotion

What is the most effective method of preventing flu??

Are all Influenza Vaccines Equal?

Why are Adults 65+ at Greater Risk of Influenza and
Related Complications?
References1. FLUZONE® High-Dose vaccine. Product Monograph. Sanofi Pasteur Inc.; September 2015.2. Public Health Agency of Canada (PHAC). Canadian Immunization Guide. General Guidelines. 2013. http://www.phac-aspc.gc.ca/publicat/cig-gci/assets/pdf/p01-eng.pdf. Accessed December 4, 2015.
This results in:
• Higher risk and severity of infectious diseases
• Lower responsiveness to vaccines2
Immunosenescence is the natural and progressive weakening of the immune system over time.1
Immunosenescence renders vaccines less effective for seniors, making seniors more vulnerable to influenza
41

Standard-Dose Influenza Vaccine
Effectiveness by Age1
Reference: 1. Monto AS, Ansaldi F, Aspinall R, et al. Influenza control in the 21st century: optimizing protection of older
adults. Vaccine. 2009;27:5043-5053.
During the influenza seasons shown, the range of vaccine effectiveness was
62% to 76% in persons 15-64 years of age and 26% to 52% in those ≥65 years of age
42

Evolution of Influenza Vaccines:
High-Dose Influenza Vaccine: A new option for adults over 65
43

FLUZONE® High-Dose Vaccine1
• Developed in response to requests for a more immunogenic/effective vaccine for seniors
• 60 mcg hemagglutinin (HA) of each influenza strain per 0.5 mL dose (4 times that of standard-dose influenza vaccines) (15 mcg HA/strain)
• Trivalent, inactivated, split-virus influenza vaccine
• No adjuvant, antibiotic, gelatin, or preservative
• Format:
– Single-dose, 0.5 mL, prefilled syringe
– Supplied in packages of 5 prefilled syringes
• Available in Canada as of 2016-2017.
Reference: 1. Fluzone High-Dose vaccine Canadian product monograph44

45
Relative Efficacy against Confirmeda Influenza of FLUZONE High-Dose to Standard Dose FLUZONE Vaccine:
By Study Year
| 38
Year 1 Year 2
HD
N=7253
n (%)
SD
N=7244
n (%)
Relative
Efficacy
% (95% CI)
HD
N=8737
n (%)
SD
N=8749
n (%)
Relative
Efficacy
% (95% CI)
Associated with PD ILIb 32 (0.32) 42 (0.58)
45.31 (6.95 – 68.60)
205 (2.35) 259 (2.96)20.74
(4.43– 34.33)
Low Activity; High Match High-Activity; Low Match
a. PD-ILI: Protocol-Defined Influenza-like Illness
References: 1. DiazGranados CA, et al. N Engl J Med. 2014;371(7):635-645.
The authors concluded that this, “finding provides reassurance that the benefit of [High-Dose vaccine] persists despite varying seasonal conditions.”1

Izurieta et al: Effectiveness of Fluzone High-Dose Vaccine Among US Medicare Recipients, 2012-20131
1. Izurieta HS et al. Lancet Infect Dis 2015;15:293-300, Figure 3
22% more effective in
preventing probable
influenza, based on
rapid influenza test and
oseltamivir Rx
22% more effective in
preventing influenza
inpatient hospital
admission or emergency
department visit
FDA, CDC, and CMS Study: Identified Medicare beneficiaries ≥ 65 years of age who were immunized at community pharmacies during the 2012-2013 season
The study included 929,730 Fluzone High-Dose recipients and 1,615,545 standard-dose influenza vaccine recipients

INFLUENZA SEASON 2013-2014
47

Number Needed to Vaccinate(for All Causes, Ever Hospitalized)
NNT = 1/ARR where ARR = CER – EER a
69, FFS sample
To prevent 1 hospitalization, 69 long-stay NH residents 65+ years of age need to be vaccinated with high-dose influenza vaccine compared to standard dose vaccine.
a NNT (or NNV) = number needed to treat; ARR = absolute risk reduction; CER = control event rate (i.e., probability of hospitalization for the SD group); EER = experimental event rate (i.e., probability of hospitalization for the HD group)
48Gravenstein et al, Lancet Respir Med 2017

NACI’s 2018/2019 Seasonal Influenza Vaccine Recommendations
Recipient by Age
Group
Vaccine Types
Available for Use†Comments
Adults 65+ years of
age
TIVQIV
ATIV
High dose TIV
At the programmatic level, NACI recommends that any of the four influenza vaccines available for use in adults 65 years of age and older
should be used: standard-dose TIV, high-dose TIV, MF59-adjuvanted TIV, and QIV. High-dose TIV is expected to provide superior protection
compared to standard-dose TIV; however, with cost-effectiveness assessments having been outside the scope of the evidence review and
without data on the relative efficacy/effectiveness between high-dose TIV, MF59-adjuvanted TIV, and QIV, there is insufficient evidence to make
a comparative recommendation on the use of these vaccines at the programmatic level (Grade I).
At the individual level, NACI recommends that high-dose TIV should be offered over standard-dose TIV to persons 65 years of age and older.
NACI concludes that, given the burden of disease associated with influenza A(H3N2) and the good evidence of better efficacy compared to
standard-dose TIV in this age group, high-dose TIV should be offered over standard-dose TIV to persons 65 years of age and older (Grade A).
There is insufficient evidence to make comparative recommendations on the use of MF59-adjuvanted TIV and QIV over standard-dose
TIV.
NACI’s 2018/2019 Seasonal Influenza Vaccine Recommendations for Adults 65+
There is good evidence that Fluzone® High-Dose provides superior protection(e.g., decrease in ILI, influenza-related death and all-cause hospitalization) compared with standard-dose TIV in the elderly (Grade A Evidence)

What is the Current Program in BC?
In B.C., influenza vaccines are provided free to people who are at high risk of serious illness from influenza
• Young children
• Pregnant women
• The elderly
• People with certain medical conditions
• Those able to transmit or spread influenza to those at high risk
• People who provide essential community services.

Funded Vaccines for 65+
2016-2017 Influenza Season• TIIV (standard dose) trivalent inactive influenza vaccine, or
• ATIIV (adjuvanted standard dose) trivalent inactive influenza vaccine
2017-2018 Influenza Season• TIIV (standard dose) trivalent inactive influenza vaccine.
(ATIIV program discontinued by public health)

Available Vaccines for 65+
2016-2017 Influenza Season• TIIV (standard dose) trivalent inactive influenza vaccine• ATIIV (adjuvanted standard dose)• HD TIIV (High dose)
2017-2018 Influenza Season• TIIV (standard dose) trivalent inactive influenza vaccine• ATIIV discontinued for seniors by public health due to
limited data on effectiveness • HD TIIV (High Dose)

What is happening in Canada?
• Manitoba provides TIIV HD to LTC facilities
• Ontario has a publicly funded program – part of Seniors action plan
• Nova Scotia providing TIIV HD to LTC facilities
• NWT offering HD to LTC facilities

Manitoba First Province to adopt High Dose Vaccine
• High dose vaccine available for seniors at LTC facilities at no charge
• Results:
• Fewer outbreaks in LTC facilities of Influenza A
• Fewer cases of influenza in LTC facilities
• Decreased risk of getting influenza A
• Fewer deaths in immunized seniors
References1. Long-term facility residents urged to get special high-dose seasonal flu vaccine [Internet]. Mysteinbach.ca. 2018 [cited 9 November 2018]. Available from:
https://www.mysteinbach.ca/news/3643/long-term-facility-residents-urged-to-get-special-high-dose-seasonal-flu-vaccine/

Now BC seniors are faced with a choice….
Publicly funded Standard Dose TIIV
OR
Private pay High Dose TIIV

It’s Quiz Time!
• Time to Test Your Knowledge on Seasonal Influenza

But…. Are there other recommended but unfunded vaccines????
What is out there?

Approved But Non Funded Vaccines
“ The greatest need is to change the widespread perception that vaccines should be publicly funded or ignored. The long-standing and total dominance of population over individual considerations for vaccines needs to end or the potential benefits of some vaccines will not be realized, to the detriment of those at risk. It is a form of discrimination against vaccines compared with (preventive) drugs that urgently needs to be corrected”1

The National Committee on Immunization (NACI) Recommendations
• 1. Fluzone High Dose Influenza Vaccine (high-dose TIV should be offered over standard-dose TIV to persons 65 years of age and older for protection against seasonal influenza vaccine.
• 2. Prevnar 13 (Pneumococcal Conjugate Vaccine) Recommended for adults over 65 for protection against invasive pneumococcal disease
• 3. Shingrix (Recombinant Zoster Vaccine) –Recommended for adults over the age of 50, for protection against herpes zoster virus.

Pneumococcal Vaccine
• Protects against “Invasive PnuemococcalDisease” – caused by the infectious agent Streptococcus pneumoniae
• Each year, approximately 3,000 cases of IPD are reported in Canada. Most are among the very young (those under the age of 5) or the elderly (those 65 and older).

“Invasive Pneumococcal Disease”
• An infection confirmed by the isolation of S pneumoniae from a normally sterile site, such as blood or CSF
• Sinusitis, Acute otitis media, and community acquired pneumonia (not in the blood) = non-invasive (muscosal) disease
• Meningitis, bacteremia, and IPD are invasive disease

Pneumococcal Vaccines Licensed for Adults in Canada
1. Pneumococcal Polysaccharide vaccine (PPSV23) –Pneumovax 23 ***PROVIDED FREE IN BC**
• Serotypes – 1,3,4,5,6B,7F,9V, 14, 18C, 19A, 19F, 23F, 2,8,9N, 10A, 11A 12F, 15B, 17F, 20, 22F, 33F
2. Pneumococcal Conjugate Vaccine (PCV) - PCV13 (Prevnar 13) ***PRIVATE PAY IN BC****
• Serotypes – 1,3,4,5,6B, 7F, 9V, 14, 18C, 19A, 19F, 23F, 6A

Polysacchride Vaccine (PPSV23)
• Contains polysaccharide antigens
• Stimulates B Cells to produce antibodies
• T-cell independent immune response
• Covers more serotypes
• Not effective at preventing CAP that is not in the blood
• Limited Herd Effect
• Hyporesponsiveness on reimmunization

Conjugate Vaccine (PVC13)
• Contains polysaccharide antigens covalently linked to a carrier protien
• Stimulates T cells to help B cells produce antibodies and generate immune memory (IgG)
• T-cell dependent immune response
• Herd effect
• Protects against fewer serotypes but effective against CAP and IPD (10% of CAP caused by PCV-13 serotypes)

NACI 2016 Statement
Immunocompetent adults over 65 years of age
• PCV13 followed by PPSV23 – In Individuals not previously immunized against PD (grade A recommendation)
• PPSV23 – In all individuals aged 65 or older (grade B recommendation)

Current Recommendation on PCV13
• In 2010 PCV13 was approved for use in adults >50 years old to prevent pneumonia and invasive disease
• In 2014 they recommended routine use PCV 13 in seniors (>65 years old)
• FDA defined "meaningful therapeutic benefit over existing treatments”
• Efficacy of PCV13 against IPD is 75%
• More importantly the additional efficacy against CAP
References1. Use of 13-Valent Pneumococcal Conjugate Vaccine and 23-Valent Pneumococcal Polysaccharide Vaccine Among Adults Aged ≥65 Years: Recommendations of
the Advisory Committee on Immunization Practices (ACIP) [Internet]. Cdc.gov. 2018 [cited 9 November 2018]. Available from: https://www.cdc.gov/mmwr/preview/mmwrhtml/mm6337a4.htm

PCV13 Efficacy against CAP
• Effectiveness against 3.7% of CAP – over 5 years represents 137 000 cases of hospitalized CAP potentially preventable with PCV13 in the US (1)
• In Canada – The proportion of hospitalized CAP cases in adults caused by PCV13-type S. pneumoniae ranged between 7% and 14.8% among cases (2)

Implications of Adding PCV 13 to the routine schedule
• Reduction in Vaccine Preventable CAP and IPD causing morbidity and mortality in hospitalized Canadian adults
• Reduction in antibiotic use to treat Vaccine Preventable CAP and IPD


It’s Quiz Time!
• Time to Test Your Knowledge on Pneumococcal Disease!

Shingles• Also known as herpes
zoster
• Its a painful rash
• Occurs when virus that causes chickenpox gets activated
• Symptoms: itching, tingling, pain, rash and blisters
References1. Shingles [Internet]. HealthLink BC. 2018 [cited 9 November 2018]. Available from: https://www.healthlinkbc.ca/health-topics/hw75433

Shingles
• Am I at risk for shingles?Although any person who has had chickenpox before can get shingles, most who do so are older than 50 or have a weakened immune system
• According to the BCCDC, it is estimated that 15-28% of people will develop shingles at some point in their life
• Additionally, one in five people with shingles go on to develop post-herpetic neuralgia, or PHN, which is nerve pain that can linger for months or even years

Post-Herpetic Neuralgia
• Presentation: pain, headache and nerve problems
• Duration: at least 30 days and can last months to years
• Location: Forehead and Chest
• Risk Factors: Age greater than 50 years and severe pain and rash during shingles
• Pain may impact:
• sleep
• appetite
• daily activities
• increases risk of depression
• Treatment: Anticonvulsants, Antidepressants and Opioids to relieve pain
References1. Shingles [Internet]. HealthLink BC. 2018 [cited 9 November 2018]. Available from: https://www.healthlinkbc.ca/health-topics/hw75433

PHN: The Burden of Disease

PHN: The Burden of Disease

What Vaccines are available?
• Shingrix (2 doses IM that are 2-6 months apart) *this is the newest shingles vaccine to be approved*
• Zostavax (1 dose SC)

Zostavax
• It reduces the chance of shingles by only 51%and post-herpetic neuralgia by only 67% and is recommended for those ages 60 and older.3
• Its effects were thought to last only up to 5 years, with new research saying that the effects might wane after only 3 years.5

Shingrix
• The Shingrix vaccine, although two doses are needed, offers 90% protection against shingles according to clinical trials in people aged 50 years and above.4
• As well, its effectiveness remained high throughout the 4 year study period.4

NACI Statement
• RZV (Shingrix®) should be offered to persons >50 years of age without contraindications including:
• Individuals previously vaccinated with LZV. Re-vaccinate with two doses of RZV at least one year after receiving LZV.
• Individuals with a previous episode of herpes zoster disease. Provide two doses of RZV at least one year after herpes zoster episode.
• Immunocompromised individuals, may be considered on a case-by-case assessment of the benefits vs risks.
• LZV (Zostavax®II) may be considered for immunocompetentindividuals >50 years of age without contraindications when RZV is contraindicated, unavailable or inaccessible.

It’s Quiz Time!
• Time to Test Your Knowledge on HZV!

Issues….
• No special consideration for seniors
• Lack of education about the burden of influenza, IPD, and HZV and vaccine options
• Lack of awareness amongst the public, and health care providers
• Lack of education from the public sector on non-publicly funded vaccines…

Missed opportunity
If the government is NOT going to offer recommended but unfunded vaccines through the public program, it is up to front-line immunization providers to inform their patients about the OPTION
Immunization Administration
Discussion about the influenza vaccine options, and benefits based on age, medical conditions, risk.
Discussion about price, funded vs non-funded vaccines, individual vs population protection

Missed opportunity
• If the government is NOT going to offer recommended but unfunded vaccines through the public program, it is up to front-line immunization providers to inform their patients about the OPTION
Immunization Administration
Discussion about the influenza vaccine options, and benefits based on age, medical conditions, risk.
Discussion about price, funded vs non-funded vaccines, individual vs population protection

Unfortunately information given to HCP is “confusing”
BCCDC Q & A Statement August 2017:
“Given the lack of an explicit recommendation for preferential use of high dose TIIV by NACI and/or endorsement of superiority by provincial advisory committees, providers are under no greater obligation to inform patients of the high dose TIIV option than any other TIIV product approved for seniors in Canada.

Just because there is a publicly funded alternative, does that mean our patients should not be informed that they have a choice?

Lack of Public Awareness of approved but non-funded vaccines2
• Need to change widespread perception that approved vaccines should be publically funded or ignored
• Recognition that individuals have a prerogative to take advantage of a vaccine of potential benefit
• Provincial Health Programs should recommend and promote both funded and private vaccines
• Pharmacists are key players in making unfunded vaccines locally available

But also we should look into funding these vaccines for Seniors!
• Aging Demographic
• Health Equity
• Healthcare Sustainability – Hospitalizations from Influenza, PD, HZV, and PHN
• Antimicrobial Resistance

WHO: Global Vaccine Action Plan
• “The introduction of new vaccines represents an opportunity to strengthen immunization systems and to act as a catalyst to implement many of the required reforms”.
• “As national immunization investments increase, so must government oversight and accountability”.
• “Vaccination has made the greatest contribution to global health of any human intervention apart from the introduction of clean water and sanitation.”
• “There is no better way in which national revenue could be spent.”Greenwood, B “The Contribution of Vaccination to Global Health: Past, Present and Future” PhilosTrans R SocLondB Biol Sci. 2014 Jun 19; 369(1645): 20130433.

Thank You!