AOA Cardiology Review High Yield USMLE FACTS 2009 Patrick Brine & Brian Katz.
59
AOA Cardiology AOA Cardiology Review Review High Yield USMLE High Yield USMLE FACTS FACTS 2009 2009 Patrick Brine Patrick Brine & & Brian Katz Brian Katz
-
Upload
diana-waters -
Category
Documents
-
view
231 -
download
1
Transcript of AOA Cardiology Review High Yield USMLE FACTS 2009 Patrick Brine & Brian Katz.

AOA Cardiology AOA Cardiology ReviewReview
High Yield USMLE FACTSHigh Yield USMLE FACTS20092009
Patrick BrinePatrick Brine
&&
Brian KatzBrian Katz

Case #1 HTNCase #1 HTN
A 34 year-old man undergoing a routine physical A 34 year-old man undergoing a routine physical examination is found to have a blood pressure of 165/105 examination is found to have a blood pressure of 165/105 mm Hg. The physician asks the patient to return the next mm Hg. The physician asks the patient to return the next week and the week following, and each time repeats the week and the week following, and each time repeats the evaluation yielding the following results: 170/102, 168/107, evaluation yielding the following results: 170/102, 168/107, 175/108, 167/102 mm Hg.175/108, 167/102 mm Hg.
Patient’s BP should be classified as which?Patient’s BP should be classified as which?– A. OptimalA. Optimal– B. NormalB. Normal– C. High-NormalC. High-Normal– D. Stage 1 HTND. Stage 1 HTN– E. Stage 2 HTNE. Stage 2 HTN– F. Stage 3 HTNF. Stage 3 HTN

Case # 1Case # 1 ANSWER: EANSWER: E
– Pre-HTN: 120-139/80-89Pre-HTN: 120-139/80-89– Stage I: 140-159/90-99Stage I: 140-159/90-99– Stage II: >160/>100Stage II: >160/>100– Dx with 2 or more BP or 2 subsequent visitsDx with 2 or more BP or 2 subsequent visits
What % of these patients have essential HTN?What % of these patients have essential HTN?– A. Less than 5%A. Less than 5%– B. 10-15%B. 10-15%– C. 40-50%C. 40-50%– D. 70-80%D. 70-80%– E. 90-95%E. 90-95%

Case # 1Case # 1
ANSWER: EANSWER: E– RF for Essential HTNRF for Essential HTN
Cardiovascular DzCardiovascular Dz High CholesterolHigh Cholesterol DiabetesDiabetes Family HxFamily Hx SmokingSmoking High Salt DietHigh Salt Diet Alcohol UseAlcohol Use Race and Sex: African Americans and MalesRace and Sex: African Americans and Males

Case # 1Case # 1
HTN Complications: High Yield USMLEHTN Complications: High Yield USMLE– Kidney: Hyaline ArteriosclerosisKidney: Hyaline Arteriosclerosis– Cardiac: Left Ventricular HypertrophyCardiac: Left Ventricular Hypertrophy– Eye: Cotton wool spots from Retinal IschemiaEye: Cotton wool spots from Retinal Ischemia– Large and Small Vessel DamageLarge and Small Vessel Damage
Aneursyms, Strokes, AtherosclerosisAneursyms, Strokes, Atherosclerosis
TreatmentTreatment– Lifestyle modifications: decrease Na, exercise, diet, decrease Lifestyle modifications: decrease Na, exercise, diet, decrease
smoking and alcohol intakesmoking and alcohol intake– ThiazidesThiazides– ACEI in DM and Post MIACEI in DM and Post MI– B Blocker in Post MIB Blocker in Post MI

Case # 2 HTNCase # 2 HTN A 35 year-old man has hypertension, which has been difficult to control with A 35 year-old man has hypertension, which has been difficult to control with
medication. Periodically, he experiences periods when he develops intense medication. Periodically, he experiences periods when he develops intense symptoms including racing heart, lightheadedness, flushing, diaphoresis, clammy symptoms including racing heart, lightheadedness, flushing, diaphoresis, clammy skin, headache, and a sense of impending doom. He has gone to the emergency skin, headache, and a sense of impending doom. He has gone to the emergency department of a local hospital several times during these episodes, but by the time department of a local hospital several times during these episodes, but by the time he is seen several hours later, symptoms have long passed, and nothing can be he is seen several hours later, symptoms have long passed, and nothing can be found on physical examination or serum chemistry studies.found on physical examination or serum chemistry studies.
The patient’s physician orders a 24 hour urine to be collected, The patient’s physician orders a 24 hour urine to be collected, which is found to contain significantly elevated levels of VMA. which is found to contain significantly elevated levels of VMA. This compound is a degradation product of which of the This compound is a degradation product of which of the following?following?– A: AcetylcholineA: Acetylcholine– B: CholesterolB: Cholesterol– C: EpinephrineC: Epinephrine– D: SerotoninD: Serotonin– E: TestosteroneE: Testosterone

Case # 2Case # 2
ANSWER: CANSWER: C– VMA: degradation product of Epinephrine and VMA: degradation product of Epinephrine and
NorepinephrineNorepinephrine
– Serotonin: produced by carcinoid tumors: Serotonin: produced by carcinoid tumors: measured directly or by 5HIAAmeasured directly or by 5HIAA
– Testosterone: measured directly in serum or Testosterone: measured directly in serum or precursors: DHEA, DHT, androstiendioneprecursors: DHEA, DHT, androstiendione

Case # 2Case # 2
Q2: What is the most likely Diagnosis?Q2: What is the most likely Diagnosis?– A: LeiomyosarcomaA: Leiomyosarcoma– B: LymphomaB: Lymphoma– C: NeuroblastomaC: Neuroblastoma– D: PheochromocytomaD: Pheochromocytoma– E: Small Cell CarcinomaE: Small Cell Carcinoma

Case # 2Case # 2
ANSWER: DANSWER: D– PHEO is commonly tested on USMLEPHEO is commonly tested on USMLE
Rare cause of 2Rare cause of 2ndnd HTN HTN RULE OF TENs: RULE OF TENs:
– 10% bilat, 10% bilat, – 10% outside of the Adrenal medulla10% outside of the Adrenal medulla– 10% malignant10% malignant

Case # 2Case # 2
Q3: The patient’s lesion has been Q3: The patient’s lesion has been associated with which of the following associated with which of the following thyroid lesions?thyroid lesions?– A: Follicular CarcinomaA: Follicular Carcinoma– B: Graves DiseaseB: Graves Disease– C: Hashimoto’s DiseaseC: Hashimoto’s Disease– D: Medullary CarcinomaD: Medullary Carcinoma– E: Papillary CarcinomaE: Papillary Carcinoma

Case # 2Case # 2
Answer: DAnswer: D– MEN Syndromes:MEN Syndromes:
MEN I: 3 P’s: Pituitary, Parathyroid, PancreasMEN I: 3 P’s: Pituitary, Parathyroid, Pancreas– Parathyroid hyperplasia, Zollinger-Ellison SyndromeParathyroid hyperplasia, Zollinger-Ellison Syndrome
MEN IIa: Thyroid, Pheochromocytoma, ParathyroidMEN IIa: Thyroid, Pheochromocytoma, Parathyroid MEN IIb: Thyroid, Pheochromocytoma, Mucosal MEN IIb: Thyroid, Pheochromocytoma, Mucosal
Neuronal TumorsNeuronal Tumors

Case # 2Case # 2
Final Q: The patient is scheduled for Final Q: The patient is scheduled for surgical removal of the tumor. Which of the surgical removal of the tumor. Which of the following agents should be administered?following agents should be administered?– A: IodideA: Iodide– B: LorazepamB: Lorazepam– C: PhenoxybenzamineC: Phenoxybenzamine– D: PropylthiuricilD: Propylthiuricil– E: SpirinolactoneE: Spirinolactone

CASE # 2CASE # 2
ANSWER: CANSWER: C– alpha blockers used: prevents constriction of peripheral blood alpha blockers used: prevents constriction of peripheral blood
vesselsvessels EPINEPHRINE REVERSAL: Blocking alpha receptors forces EPINEPHRINE REVERSAL: Blocking alpha receptors forces
epinephrine to bind to beta receptors and decrease blood pressureepinephrine to bind to beta receptors and decrease blood pressure
Other causes of 2Other causes of 2ndnd HTN: HTN: – Renal Artery Stenosis: ABD BRUIT, fibromuscular dysplasiaRenal Artery Stenosis: ABD BRUIT, fibromuscular dysplasia– Hyperaldosteronism: Conn Syn: R/A ratio, decreased K, increased Hyperaldosteronism: Conn Syn: R/A ratio, decreased K, increased
Na, metabolic alkalosis- ADRENAL ADENOMANa, metabolic alkalosis- ADRENAL ADENOMA– Cushing’s: Elevated Cortisol levelCushing’s: Elevated Cortisol level– Thyroid: Hyperthyroidism: elevated T4, suppressed TSHThyroid: Hyperthyroidism: elevated T4, suppressed TSH– Coarctation of the Aorta: unequal ext. blood pressuresCoarctation of the Aorta: unequal ext. blood pressures

Case # 3 Ht FailureCase # 3 Ht Failure A 45 year-old woman presents to her primary care physician A 45 year-old woman presents to her primary care physician
complaining of fatigue, weight gain, and shortness of breath. She has complaining of fatigue, weight gain, and shortness of breath. She has always been an active athlete, but in the past 2 weeks, has found it always been an active athlete, but in the past 2 weeks, has found it impossible to jog for more than a few minutes, after which she feels impossible to jog for more than a few minutes, after which she feels tired and winded. She feels her appetite is normal or has even tired and winded. She feels her appetite is normal or has even declined, but she noticed she has gained 15 lbs and her pants and declined, but she noticed she has gained 15 lbs and her pants and shoes no longer fit. She appears fatigued, but in NAD. Expiratory shoes no longer fit. She appears fatigued, but in NAD. Expiratory wheezes at both bases. Normal S1, S2 with a II/IV soft holosystolic wheezes at both bases. Normal S1, S2 with a II/IV soft holosystolic murmur heard best at the apex. Distended abdomen. CXR reveals murmur heard best at the apex. Distended abdomen. CXR reveals cardiomegaly and increased vascular markings.cardiomegaly and increased vascular markings.
Which of the following is the most likely diagnosis?Which of the following is the most likely diagnosis?– A. Acute LeukemiaA. Acute Leukemia– B. CardiomyopathyB. Cardiomyopathy– C. FibromyalgiaC. Fibromyalgia– D. HypothyroidismD. Hypothyroidism– E. Major Depressive DisorderE. Major Depressive Disorder

Case # 3Case # 3 Answer: BAnswer: B
– Heart FailureHeart Failure Poor Cardiac OutputPoor Cardiac Output SX: SOBSX: SOB FatigueFatigue poor appetitepoor appetite EdemaEdema AscitesAscites cardiomegalycardiomegaly
– Which of the following is the most likely cause of the patient’s Which of the following is the most likely cause of the patient’s murmur?murmur? A. Aortic InsufficiencyA. Aortic Insufficiency B. Aortic StenosisB. Aortic Stenosis C. High-Output flow murmurC. High-Output flow murmur D. Mitral RegurgitationD. Mitral Regurgitation E. Mitral StenosisE. Mitral Stenosis F. Pulmonic InsufficiencyF. Pulmonic Insufficiency G. Pulmonic StenosisG. Pulmonic Stenosis H. Tricuspid RegurgitationH. Tricuspid Regurgitation

Case # 3Case # 3
Answer: DAnswer: D– Mitral Regurg- holosystolic heard best at apexMitral Regurg- holosystolic heard best at apex– Aortic Stenosis- crescendo/decrescendo systolic murmur 2Aortic Stenosis- crescendo/decrescendo systolic murmur 2ndnd Rt Rt
intercostal and radiation to carotidsintercostal and radiation to carotids– Aortic Regurg- diastolic murmur flowAortic Regurg- diastolic murmur flow– Mitral Stenosis- soft diastolic at apexMitral Stenosis- soft diastolic at apex
Blood in the pulmonary vein is at the same pressure as Blood in the pulmonary vein is at the same pressure as blood in which of the following?blood in which of the following?– A: AortaA: Aorta– B. Lt AtriumB. Lt Atrium– C. Lt VentricleC. Lt Ventricle– D. Rt. AtriumD. Rt. Atrium– E. Rt. VentricleE. Rt. Ventricle

Case # 3Case # 3 Answer: B High Yield Cardio PhysiologyAnswer: B High Yield Cardio Physiology
– Closed vs. Open circulationClosed vs. Open circulation

Case # 3Case # 3
What impt. Physiologic effect will starting this patient on an What impt. Physiologic effect will starting this patient on an ACEI achieve?ACEI achieve?– A. Decrease in arteriolar resistance, resulting in less resistance to A. Decrease in arteriolar resistance, resulting in less resistance to
forward cardiac outpt.forward cardiac outpt.– B. Decrease in cardiac filling pressures, resulting in less pulm. B. Decrease in cardiac filling pressures, resulting in less pulm.
CongestionCongestion– C. Increase in arteriolar resistance, resulting in improved blood C. Increase in arteriolar resistance, resulting in improved blood
pressurepressure– D. Increase in Lt. Ventricular End-Diastolic Volume, improving in D. Increase in Lt. Ventricular End-Diastolic Volume, improving in
stroke volume via starling Forcesstroke volume via starling Forces– E. Increase in Myocardial Contractility, resulting in improved stroke E. Increase in Myocardial Contractility, resulting in improved stroke
volumevolume– F. Stabilization of myocardial membranes, resulting in reduced risk F. Stabilization of myocardial membranes, resulting in reduced risk
of arrythmiaof arrythmia

Case # 3Case # 3 Answer: A High Yield R-A-A Answer: A High Yield R-A-A
systemsystem– Heart failure promotes an Heart failure promotes an
elevated SVR due to poor elevated SVR due to poor cardiac outptcardiac outpt
– ACEI decrease the resistance ACEI decrease the resistance against the heart pumping to against the heart pumping to increase volume in the poor increase volume in the poor outpt state. AFTERLOAD outpt state. AFTERLOAD REDUCTIONREDUCTION
– Decrease PreloadDecrease Preload Aldosterone and ADH Aldosterone and ADH
elevate LV End Diastolic elevate LV End Diastolic VolumeVolume
Leads to Vascular Leads to Vascular CongestionCongestion
NITRATES AND NITRATES AND DIURETICS REDUCE DIURETICS REDUCE PRELOADPRELOAD
– Increase ContractilityIncrease Contractility Inotropic DrugsInotropic Drugs

Case # 3Case # 3

Case # 3Case # 3

Case # 4 Heart FailureCase # 4 Heart Failure A 40 year-old man presents to the emergency department complaining A 40 year-old man presents to the emergency department complaining
of severe SOB. The SOB has been worsening over the past few of severe SOB. The SOB has been worsening over the past few years, and the patient reports growing tachypneic with mild exertion, years, and the patient reports growing tachypneic with mild exertion, and sometimes even at night. On exam, he has generalized edema, and sometimes even at night. On exam, he has generalized edema, JVD, and hepatic distention. Cardiac exam shows Rt. Ventricular JVD, and hepatic distention. Cardiac exam shows Rt. Ventricular Heave, a rt. Sided S3, and S4 with a pulm. Ejection click. A CXR Heave, a rt. Sided S3, and S4 with a pulm. Ejection click. A CXR shows Cardiomegaly and a widening of the hilar vessels, including shows Cardiomegaly and a widening of the hilar vessels, including pulm. Arteries. EKG shows tall Peaked P waves in II, III, and aVF, rt pulm. Arteries. EKG shows tall Peaked P waves in II, III, and aVF, rt axis deviation, and RVH.axis deviation, and RVH.
Which of the following is the most likely Diagnosis?Which of the following is the most likely Diagnosis?– A. Cor PulmonaleA. Cor Pulmonale– B. Hypertrophic CardiomyopathyB. Hypertrophic Cardiomyopathy– C. Lt Ventricular Ht FailureC. Lt Ventricular Ht Failure– D. MID. MI– E. PE (acute)E. PE (acute)

Case # 4Case # 4 ANSWER: A High yield Ht FailureANSWER: A High yield Ht Failure
– Enlargement of Rt. Ventricle 2Enlargement of Rt. Ventricle 2ndnd to diseases of to diseases of LUNGS, THORAX, or PULM. LUNGS, THORAX, or PULM. CIRCULATION.CIRCULATION.
– Rt. Atrial Enlargement- EKG: Tall, peaked P waves in leads II, III, aVFRt. Atrial Enlargement- EKG: Tall, peaked P waves in leads II, III, aVF– MOST COMMON Cause of Rt. Ht FailureMOST COMMON Cause of Rt. Ht Failure
LT SIDED HT FAILURELT SIDED HT FAILURE
Pulm. HTN is suspected in the pt. and a Swan Ganz Catheter is placed. Pulm. HTN is suspected in the pt. and a Swan Ganz Catheter is placed. Which of the following denotes the correct anatomic sequence of vessels Which of the following denotes the correct anatomic sequence of vessels that would be traversed by the catheter if it was introduced into the Lt. that would be traversed by the catheter if it was introduced into the Lt. Subclavian vein?Subclavian vein?– A. Lt. Subclavian vein, Lt. Brachiocephalic vein, SVC, Rt. Atrium, RV, Pulm A. Lt. Subclavian vein, Lt. Brachiocephalic vein, SVC, Rt. Atrium, RV, Pulm
ArteryArtery– B. Lt. Subclavian vein, Lt Common Carotid, SVC, Rt. Atrium, RV, Pulm Artery.B. Lt. Subclavian vein, Lt Common Carotid, SVC, Rt. Atrium, RV, Pulm Artery.– C. Lt. Subclavian Vein, Lt. Jugular Vein, Lt. Atrium, Lt. Ventricle, AortaC. Lt. Subclavian Vein, Lt. Jugular Vein, Lt. Atrium, Lt. Ventricle, Aorta– D. Lt. Subclavian Vein, Lt. Jugular Vein, SVC, Rt. Atrium, Rt. Ventricle, Pulm D. Lt. Subclavian Vein, Lt. Jugular Vein, SVC, Rt. Atrium, Rt. Ventricle, Pulm
ArteryArtery– E. Lt. Subclavian Vein, SVC, Rt. Atrium, Rt. Ventricle, Pulm. ArteryE. Lt. Subclavian Vein, SVC, Rt. Atrium, Rt. Ventricle, Pulm. Artery

Case # 4Case # 4 Answer: A HIGH YIELD Cardio AnatomyAnswer: A HIGH YIELD Cardio Anatomy

Case # 4Case # 4
Which of the following physiologic stimuli will Which of the following physiologic stimuli will result in decreased Pulmonary Vascular result in decreased Pulmonary Vascular Resistance?Resistance?– A. Decreased Cardiac OutputA. Decreased Cardiac Output– B. Increased Cardiac OutputB. Increased Cardiac Output– C. Low O2 TensionC. Low O2 Tension– D. Lung Volumes near Residual Volume (RV)D. Lung Volumes near Residual Volume (RV)– E. Lung Volumes near Total Lung Capacity E. Lung Volumes near Total Lung Capacity
(TLC)(TLC)
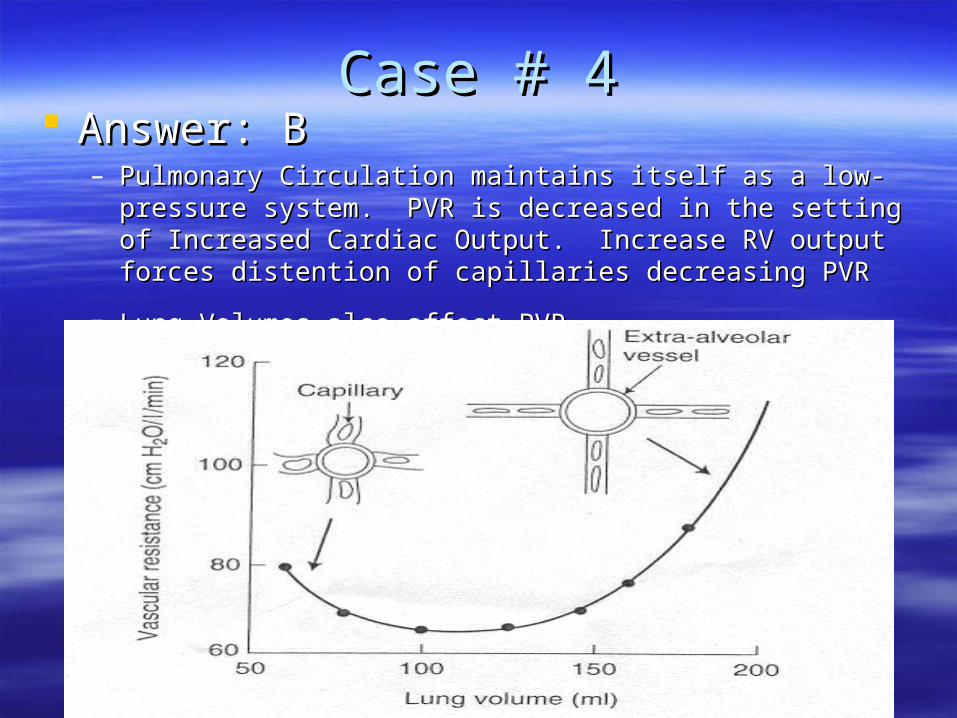
Case # 4Case # 4 Answer: BAnswer: B
– Pulmonary Circulation maintains itself as a low-pressure system. Pulmonary Circulation maintains itself as a low-pressure system. PVR is decreased in the setting of Increased Cardiac Output. PVR is decreased in the setting of Increased Cardiac Output. Increase RV output forces distention of capillaries decreasing PVRIncrease RV output forces distention of capillaries decreasing PVR
– Lung Volumes also affect PVR.Lung Volumes also affect PVR.

Case # 4Case # 4
Some of the exam findings include HEPATIC Some of the exam findings include HEPATIC congestion. Which of the following terms is congestion. Which of the following terms is commonly used to identify the macroscopic commonly used to identify the macroscopic pattern of red, depressed hepatic nodules with pattern of red, depressed hepatic nodules with pale periphery that accompanies the chronic pale periphery that accompanies the chronic hepatic congestion seen in this condition?hepatic congestion seen in this condition?– A. Centrilobular HemorrhageA. Centrilobular Hemorrhage– B. CirrhosisB. Cirrhosis– C. Fatty ChangeC. Fatty Change– D. Nutmeg LiverD. Nutmeg Liver– E. Piecemeal necrosisE. Piecemeal necrosis

Case # 4Case # 4 Answer: DAnswer: D
– Nutmeg Liver is due to Nutmeg Liver is due to CHRONICCHRONIC passive passive congestion in centrilobular region with hypoxia congestion in centrilobular region with hypoxia and fatty changes- and fatty changes- NUTMEGNUTMEG

Case # 4Case # 4 RT. Sided Ht FailureRT. Sided Ht Failure

Case # 5 Chest PainCase # 5 Chest Pain 45 year-old man presents to ER with chest pain began 20 minutes 45 year-old man presents to ER with chest pain began 20 minutes
prior while pumping gas. He describes the pain as substernal, intense, prior while pumping gas. He describes the pain as substernal, intense, dull, and squeezing. It does not change with respiration. He also dull, and squeezing. It does not change with respiration. He also complains that he is nauseated. He has never experienced anything complains that he is nauseated. He has never experienced anything like this before. His temp is 99.5, BP 124/76, P 80, RR 22, O2 Sat of like this before. His temp is 99.5, BP 124/76, P 80, RR 22, O2 Sat of 95% on RA. On exam, he is diaphoretic, CTA, RRR. JVP is elevated 95% on RA. On exam, he is diaphoretic, CTA, RRR. JVP is elevated to level of jaw. His abd is nontender with normal bowel sounds. An to level of jaw. His abd is nontender with normal bowel sounds. An EKG shows normal sinus rhythm, normal intervals, and ST elevation in EKG shows normal sinus rhythm, normal intervals, and ST elevation in leads II, III, and aVF. CXR reveals no cardiac and pulmonary leads II, III, and aVF. CXR reveals no cardiac and pulmonary abnormalities.abnormalities.
Which of the following is the most likely diagnosis?Which of the following is the most likely diagnosis?– A. Acute MIA. Acute MI– B. Aortic DissectionB. Aortic Dissection– C. Gastroesophageal refluxC. Gastroesophageal reflux– D. PericarditisD. Pericarditis– E. PEE. PE

Case # 5Case # 5
Answer: A High Yield Diff Dx of Chest PainAnswer: A High Yield Diff Dx of Chest Pain– CARDIAC VS NONCARDIAC CAUSESCARDIAC VS NONCARDIAC CAUSES
RULE OUT WITH SX, EKG, CXR, Cardiac EnzymesRULE OUT WITH SX, EKG, CXR, Cardiac Enzymes
– EKG Findings in Acute ST Elevation MIEKG Findings in Acute ST Elevation MI II, III, avF- inferior wallII, III, avF- inferior wall V1-V2- Posterior WallV1-V2- Posterior Wall V2-V4- Anterior WallV2-V4- Anterior Wall V5-V6- Lateral WallV5-V6- Lateral Wall

Case # 5Case # 5

Case # 5Case # 5
What is the pathophysiologic process most likely What is the pathophysiologic process most likely to be responsible for this patient’s presentation?to be responsible for this patient’s presentation?– A. Atherosclerotic plaque rupture resulting in thrombus A. Atherosclerotic plaque rupture resulting in thrombus
formationformation– B. Buildup of atherosclerotic stenosis to produce high-B. Buildup of atherosclerotic stenosis to produce high-
grade obstruction of the arterygrade obstruction of the artery– C. Dissection of the vesselC. Dissection of the vessel– D. Embolization of the clot, air, or foreign materialD. Embolization of the clot, air, or foreign material– E. Myocardial Hypertrophy resulting in vessel narrowingE. Myocardial Hypertrophy resulting in vessel narrowing

Case # 5Case # 5
Answer: AAnswer: A– ACS: rupture of plaque often of one that is not ACS: rupture of plaque often of one that is not
producing high grade stenosisproducing high grade stenosis– HIGH GRADE STENOSIS CAUSES ANGINAHIGH GRADE STENOSIS CAUSES ANGINA
Which of the following is most likely to be diseased Which of the following is most likely to be diseased in this patient?in this patient?– A. Coronary SinusA. Coronary Sinus– B. Lt Anterior Descending arteryB. Lt Anterior Descending artery– C. Lt. Circumflex coronary arteryC. Lt. Circumflex coronary artery– D. Lt. Main Coronary arteryD. Lt. Main Coronary artery– E. Rt. Coronary arteryE. Rt. Coronary artery

Case # 5Case # 5 Answer: EAnswer: E
– Rt coronary arteryRt coronary artery Gives off branches to the RV, the SA nodal Artery, AV nodal artery, and 85% of people the Gives off branches to the RV, the SA nodal Artery, AV nodal artery, and 85% of people the
Posterior Descending ArteryPosterior Descending Artery– Posterior supplies inferior wall of the RV and LV and 1/3 of the interventricular septum (II, III, aVF)Posterior supplies inferior wall of the RV and LV and 1/3 of the interventricular septum (II, III, aVF)
– Lt main coronary artery (I, aVL, V2-V6)Lt main coronary artery (I, aVL, V2-V6) Divides into the Lt anterior Descending and the CircumflexDivides into the Lt anterior Descending and the Circumflex Ant Descending supplies the anterior and anteroseptal portions of the LV- (V2 to V6)Ant Descending supplies the anterior and anteroseptal portions of the LV- (V2 to V6) Circumflex supplies Lateral Wall of LV (I, aVL, V5, V6)Circumflex supplies Lateral Wall of LV (I, aVL, V5, V6)
Aspirin is given in ER. Decreased Production of which mediator is Aspirin is given in ER. Decreased Production of which mediator is responsible for the beneficial effects of aspirin?responsible for the beneficial effects of aspirin?– A. cAMPA. cAMP– B. Platelet glycoprotein IIb/IIIaB. Platelet glycoprotein IIb/IIIa– C. ProstacyclinC. Prostacyclin– D. Thromboxane A2D. Thromboxane A2– E. Ubiquinone (coenzyme Q)E. Ubiquinone (coenzyme Q)

Case # 5Case # 5
Answer: DAnswer: D– Inhibits cyclooxygenase which produces prostaglandins from Inhibits cyclooxygenase which produces prostaglandins from
arachadonic acidarachadonic acid– Cyclooxygenase produces Thromboxane A2 which is a platelet Cyclooxygenase produces Thromboxane A2 which is a platelet
aggregator and potent vasoconstrictoraggregator and potent vasoconstrictor– IIb/IIIa: promotes aggregation (clodipidogrel)IIb/IIIa: promotes aggregation (clodipidogrel)
Elevation of which of the following enzymes is the most Elevation of which of the following enzymes is the most specific for this patient’s condition?specific for this patient’s condition?– A. Alanine aminotransferaseA. Alanine aminotransferase– B. Creatinine PhosphokinaseB. Creatinine Phosphokinase– C. Lactate DehydrogenaseC. Lactate Dehydrogenase– D. TransferrinD. Transferrin– E. TroponinE. Troponin

Case # 5Case # 5 Answer: EAnswer: E
– Troponins : most sensitive elevate in 3-12 hrs and peak Troponins : most sensitive elevate in 3-12 hrs and peak at 24 hours. Last 5-14 daysat 24 hours. Last 5-14 days
– CPK: most sensitive is CKMB elevated in 8-24 hours CPK: most sensitive is CKMB elevated in 8-24 hours and last 48-72 hoursand last 48-72 hours
3 days after admission, patient becomes SOB and hypotensive. 3 days after admission, patient becomes SOB and hypotensive. HR is 100 and normal EKG. BP 75/50, RR 38, O2 sat is 60% on 2 L HR is 100 and normal EKG. BP 75/50, RR 38, O2 sat is 60% on 2 L NC. CXR reveals bilateral fluffy infiltrates. Which of the following NC. CXR reveals bilateral fluffy infiltrates. Which of the following complications has occurred?complications has occurred?– A. Dilation of the Lt VentricleA. Dilation of the Lt Ventricle– B. Dressler Syn.B. Dressler Syn.– C. Rupture of the Lt. Ventricular Free WallC. Rupture of the Lt. Ventricular Free Wall– D. Rupture of papillary muscleD. Rupture of papillary muscle– E. VTACHE. VTACH

Case # 5Case # 5
Answer: D High Yield MI complicationsAnswer: D High Yield MI complications– Cardiogenic Shock with Severe Pulm EdemaCardiogenic Shock with Severe Pulm Edema– THINK: Arrhythmia, Cardiac Tamponade, or LV valvular THINK: Arrhythmia, Cardiac Tamponade, or LV valvular
dysfnxdysfnx INFERIOR MI like papillary dysfnxINFERIOR MI like papillary dysfnx Dilation of LV- ST elevation in Ant Leads and MRDilation of LV- ST elevation in Ant Leads and MR Dressler Syn- Autoimmune Pericarditis 6-8 weeks after MI- Dressler Syn- Autoimmune Pericarditis 6-8 weeks after MI-
Pleuritc Pain, SOB, Friction RubPleuritc Pain, SOB, Friction Rub LV free wall rupture would cause Cardiac Tamponade- 3-5 days LV free wall rupture would cause Cardiac Tamponade- 3-5 days
after MI think more extensive MIafter MI think more extensive MI Arrhythmias in the first 24 hours of MIArrhythmias in the first 24 hours of MI
– DD

Case # 5Case # 5
Other Causes of Chest PainOther Causes of Chest Pain– Aortic Dissection: tearing painAortic Dissection: tearing pain
Know ascending vs. descending and tx differenceKnow ascending vs. descending and tx difference Promptly lower BP to prevent further dissectionPromptly lower BP to prevent further dissection Marfan Syn asstd- other causes such as Syphilis that cause an aortic Marfan Syn asstd- other causes such as Syphilis that cause an aortic
root dilatationroot dilatation
– PEPE– PericarditisPericarditis– PneumothoraxPneumothorax– PneumoPneumo– MusculoskeletalMusculoskeletal– GIGI– PsychogenicPsychogenic

Case # 6Case # 6
19 year-old referred to physician for abn. Heart sound on 19 year-old referred to physician for abn. Heart sound on Physical Exam. Denies SOB, chest pain but does have Physical Exam. Denies SOB, chest pain but does have Palpitations. He is adopted. 79 inches tall and 160 lb with Palpitations. He is adopted. 79 inches tall and 160 lb with long arms and legs. On exam, has a mid-systolic click, long arms and legs. On exam, has a mid-systolic click, heard best at the apex. The click is heard better with heard best at the apex. The click is heard better with standing or valsalva.standing or valsalva.
Which of the following cardiac abnormalities does this Which of the following cardiac abnormalities does this patient most likely have?patient most likely have?– A. Aortic RegurgitationA. Aortic Regurgitation– B. Aortic StenosisB. Aortic Stenosis– C. Mitral StenosisC. Mitral Stenosis– D. Mitral valve prolapseD. Mitral valve prolapse– E. Tricuspid Regurgitation E. Tricuspid Regurgitation

Case # 6Case # 6
Answer: DAnswer: D– MVP can cause Palpitations, SOB, Chest PainMVP can cause Palpitations, SOB, Chest Pain
Classic Midsystolic Click that is sometimes followed by murmur – at apex, Classic Midsystolic Click that is sometimes followed by murmur – at apex, increase with valsalva and standingincrease with valsalva and standing
– AR blowing diastolic murmur Lt 2AR blowing diastolic murmur Lt 2ndnd intercostal border intercostal border– AS crescendo-decrescendo systolic murmur Rt 2AS crescendo-decrescendo systolic murmur Rt 2ndnd intercostal space that intercostal space that
radiates to carotidsradiates to carotids– MS low-pitched diastolic murmur at apexMS low-pitched diastolic murmur at apex
Preceded by opening snapPreceded by opening snap– TR blowing systolic murmur at Lt. Lower sternal borderTR blowing systolic murmur at Lt. Lower sternal border
An echocardiogram is performed. Which of the following would An echocardiogram is performed. Which of the following would likely be observed during the study?likely be observed during the study?– A. Ballooning of the aortic valve into the ventricle during diastoleA. Ballooning of the aortic valve into the ventricle during diastole– B. Ballooning of the mitral valve into the atrium during diastoleB. Ballooning of the mitral valve into the atrium during diastole– C. Rupture of the aortic valveC. Rupture of the aortic valve– D. Rupture of the tricuspid valveD. Rupture of the tricuspid valve– E. Stenotic mitral valveE. Stenotic mitral valve

Case # 6Case # 6 Answer: B USMLE HIGH YIELDAnswer: B USMLE HIGH YIELD
– Marfan Syndrome and MVP commonly related to same Marfan Syndrome and MVP commonly related to same questionquestion
Over the next year, patient develops Chest Pain, SOB, and Over the next year, patient develops Chest Pain, SOB, and progressive fatigue. On auscultation, he has a midsystolic progressive fatigue. On auscultation, he has a midsystolic click which is now followed by high pitched blowing systolic click which is now followed by high pitched blowing systolic murmur. Which of the following is the most likely cause of murmur. Which of the following is the most likely cause of this new development?this new development?– A. Aortic AneurysmA. Aortic Aneurysm– B. Aortic StenosisB. Aortic Stenosis– C. Mitral RegurgitationC. Mitral Regurgitation– D. Mitral StenosisD. Mitral Stenosis– E. MIE. MI

Case # 6Case # 6
Answer: CAnswer: C– Severe cases MVP develops into MRSevere cases MVP develops into MR– Mitral Stenosis 2Mitral Stenosis 2ndnd to Rheumatic Fever to Rheumatic Fever– Aortic Aneurysm is asstd with Marfan SyndomeAortic Aneurysm is asstd with Marfan Syndome

Diastolic MurmursDiastolic Murmurs

Systolic MurmursSystolic Murmurs
Case # 7Case # 7 A pediatrician sees a 4 month old boy for the first time. He A pediatrician sees a 4 month old boy for the first time. He
had been delivered at home by his grandmother, who had had been delivered at home by his grandmother, who had been a midwife in SE Asia. Baby had been born on time been a midwife in SE Asia. Baby had been born on time and weighed 7 lbs at birth. Exam shows continuous and weighed 7 lbs at birth. Exam shows continuous murmur heard best at the Lt. upper Sternal Border. A thrill, murmur heard best at the Lt. upper Sternal Border. A thrill, analagous to kitten’s purring, can be felt over the left side analagous to kitten’s purring, can be felt over the left side of the baby’s chest.of the baby’s chest.
The infant’s murmur is suggestive of which of the The infant’s murmur is suggestive of which of the following diagnoses?following diagnoses?– A. Coarctation of the AortaA. Coarctation of the Aorta– B. Hypoplastic Left VentricleB. Hypoplastic Left Ventricle– C. Mitral Valve StenosisC. Mitral Valve Stenosis– D. PDAD. PDA– E. Tricuspid Valve StenosisE. Tricuspid Valve Stenosis

Case # 7Case # 7 Answer: D High Yield USMLEAnswer: D High Yield USMLE
– PDA- machine-like murmurPDA- machine-like murmur– Treated with Treated with IndomethacinIndomethacin– To keep open- add To keep open- add ProstaglandinsProstaglandins– Coarctation of the Aorta soft BruitCoarctation of the Aorta soft Bruit
Patients with syncope cannot maintain sufficient Patients with syncope cannot maintain sufficient cardiac output to meet peripheral perfusion demands. cardiac output to meet peripheral perfusion demands. Which of the following best describes cardiac output?Which of the following best describes cardiac output?– A. CO= End Diastolic Volume- End Systolic VolumeA. CO= End Diastolic Volume- End Systolic Volume– B. CO= HR x MAPB. CO= HR x MAP– C. CO= HR x SVC. CO= HR x SV– D. CO= SV x MAPD. CO= SV x MAP– E. CO= SVR x MAPE. CO= SVR x MAP

Case # 7Case # 7
Answer: CAnswer: C– Stroke Volume = End Diastolic – End SystolicStroke Volume = End Diastolic – End Systolic
In a patient with Aortic Stenosis, which of the following sets In a patient with Aortic Stenosis, which of the following sets of changes depict the MAP, Pulm Wedge Pressure, Lt of changes depict the MAP, Pulm Wedge Pressure, Lt Atrial Pressure, and Lt Ventricular Peak Systolic Pressure Atrial Pressure, and Lt Ventricular Peak Systolic Pressure compared to a healthy individual?compared to a healthy individual?– MAPMAP LVPSPLVPSP PWPPWP LAPLAP– A. normalA. normal increasedincreased increasedincreased increasedincreased– B. normalB. normal increasedincreased normalnormal increasedincreased– C. normalC. normal increasedincreased normalnormal normalnormal– D. decreasedD. decreased normalnormal increasedincreased increasedincreased

Case # 7Case # 7
Answer: AAnswer: A– In AS:In AS:
Blood is ejected through smaller than normal opening Blood is ejected through smaller than normal opening Increases Resistance to flow which increases LVPSPIncreases Resistance to flow which increases LVPSP LVPSP increase causes increase in LAP as well as Pulmonary Wedge LVPSP increase causes increase in LAP as well as Pulmonary Wedge
Pressure( which clinically measures LAP)Pressure( which clinically measures LAP)
With a patient with MR, which of the following sets of changes With a patient with MR, which of the following sets of changes depict LAP at the end of ventricular systole and at the end of depict LAP at the end of ventricular systole and at the end of ventricular diastole of this patient compared to a healthy ventricular diastole of this patient compared to a healthy individualindividual
End Systolic LAPEnd Systolic LAP End Diastolic LAPEnd Diastolic LAP A.A. normalnormal IncreasedIncreased B.B. increasedincreased normalnormal C.C. increasedincreased increasedincreased D.D. decreaseddecreased decreaseddecreased E.E. decreaseddecreased normalnormal

Case # 7Case # 7
Answer: BAnswer: B– MR has elevated LAP toward the end of systoleMR has elevated LAP toward the end of systole

Endocarditis:Endocarditis:High Yield Subacute vs. AcuteHigh Yield Subacute vs. Acute


Case # 8Case # 8
54 year old man presents to ER with palpitations and SOB. 54 year old man presents to ER with palpitations and SOB. Temp of 98.6, BP 102/68, P 130, R 26. Elevated JVP, Temp of 98.6, BP 102/68, P 130, R 26. Elevated JVP, cardiac exam reveals irregular rate and rhythm, with a low cardiac exam reveals irregular rate and rhythm, with a low pitched diastolic murmur preceded by an opening snap pitched diastolic murmur preceded by an opening snap over the apex. Lung exam revealed bibasilar crackles. 2+ over the apex. Lung exam revealed bibasilar crackles. 2+ bilateral pitting edema. EKG shows an irregular undulation bilateral pitting edema. EKG shows an irregular undulation of the baseline, absence of P waves, and a narrow QRS of the baseline, absence of P waves, and a narrow QRS complex that are irregularly irregular?complex that are irregularly irregular?
What is the following preliminary diagnosis?What is the following preliminary diagnosis?– A. Atrial ArrythmiaA. Atrial Arrythmia– B. 1B. 1stst degree AV block degree AV block– C. Normal sinus rhythmC. Normal sinus rhythm– D. 3D. 3rdrd degree AV block degree AV block– E. Ventricular arrhythmiaE. Ventricular arrhythmia

Case # 8Case # 8 Answer: A High Yield ArrhythmiasAnswer: A High Yield Arrhythmias
– Narrow Complex QRS means it is Supraventricular Narrow Complex QRS means it is Supraventricular source- atrialsource- atrial
– Ventricular arrythmias wide QRS complexVentricular arrythmias wide QRS complex– AV block- conduction delayAV block- conduction delay
PR interval delayPR interval delay
Which of the following best describes the Which of the following best describes the patient’s cardiac rhythm?patient’s cardiac rhythm?– A. Atrial FibrillationA. Atrial Fibrillation– B. Atrial FlutterB. Atrial Flutter– C. Multifocal Atrial TachycardiaC. Multifocal Atrial Tachycardia– D. Sinus BradycardiaD. Sinus Bradycardia– E. Sinus TachycardiaE. Sinus Tachycardia

Case # 8Case # 8
Answer: AAnswer: A
What is the underlying cause of the What is the underlying cause of the arrhythmia?arrhythmia?– A. Aortic StenosisA. Aortic Stenosis– B. HyperthyroidismB. Hyperthyroidism– C. HypothyroidismC. Hypothyroidism– D. Mitral StenosisD. Mitral Stenosis

Case # 8Case # 8
Answer: DAnswer: D– Murmur diastolic and causing lt atrial dilatation Murmur diastolic and causing lt atrial dilatation
which promotes arrhythmiaswhich promotes arrhythmias– Think of mitral stenois and rheumatic feverThink of mitral stenois and rheumatic fever
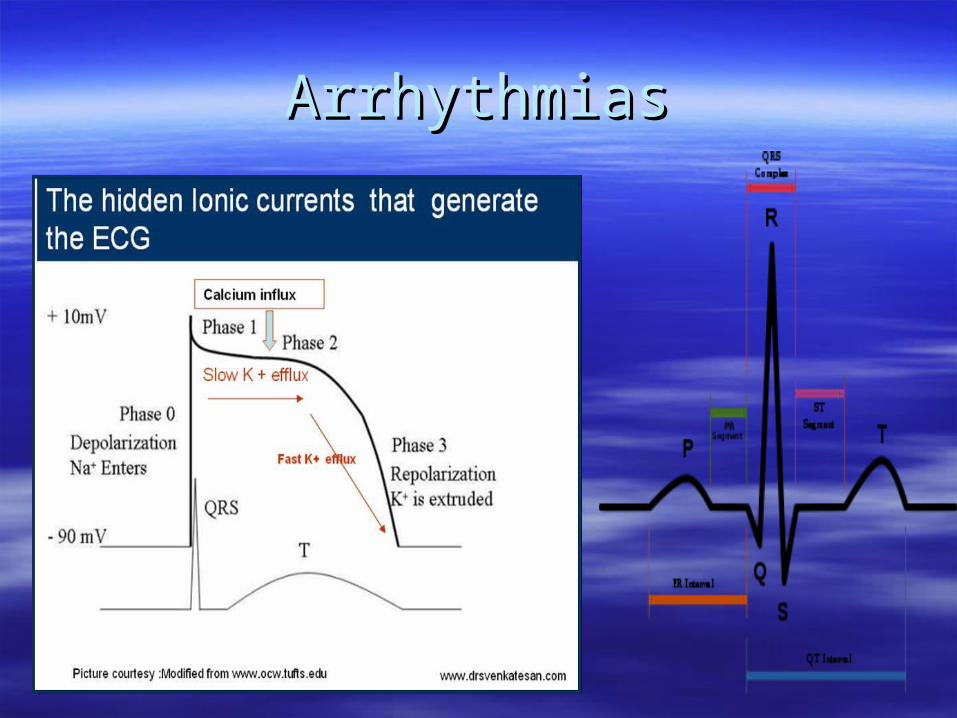
ArrhythmiasArrhythmias

Heart FailureHeart FailureNYHA GUIDELINESNYHA GUIDELINES

Heart FailureHeart FailureDrugsDrugs